Embed Size (px)
Citation preview
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 1 of 50 Revised as of 9-4-14
MEDICAL REFERRAL GUIDELINES
Referral guidelines are indexed by specialty and in alphabetical order.
1. Access Clinic ........................................................................................................................................................................................ 2
2. Cardiac Clinic ....................................................................................................................................................................................... 2
3. Dermatology Clinic ................................................................................................................................................................................. 4
4. Diabetes Clinic ....................................................................................................................................................................................... 7
5. Endocrinology Clinic .............................................................................................................................................................................. 7
6. Family Care Clinic (FCC) ........................................................................................................................................................................... 8
7. Gastroenterology (GI) Clinic ................................................................................................................................................................. 10
8. Geriatric Assessment Clinic ................................................................................................................................................................. 12
9. Hematology/Oncology Clinic ................................................................................................................................................................ 13
10. Hepatology Clinic .................................................................................................................................................................................. 21
11. HIV and Infectious Disease Clinic ........................................................................................................................................................ 22
12. Internal Medicine: Procedure Clinic ...................................................................................................................................................... 24
13. Neurology ............................................................................................................................................................................................ 24
14. Obstetrics and Gynecology ....................................................................................................................................................................... 25
15. Ophthalmology Clinic ........................................................................................................................................................................... 26
16. Orthopedics Spine Clinic ........................................................................................................................................................................... 27
17. Pediatric Sub Specialties .................................................................................................................................................................... 27
18. Pulmonary/Chest Clinic ........................................................................................................................................................................ 32
19. Renal Clinic .......................................................................................................................................................................................... 33
20. Rheumatology Clinic ............................................................................................................................................................................ 34
21. Smoking Cessation Clinic ......................................................................................................................................................................... 36
22. Surgery: ENT Surgery Clinic ............................................................................................................................................................... 37
23. Surgery: General Surgery Clinic .......................................................................................................................................................... 38
24. Surgery: Neurosurgery Clinic .............................................................................................................................................................. 39
25. Surgery: Orthopaedic Surgery Clinic ................................................................................................................................................... 41
26. Surgery: Plastic Surgery Clinic ............................................................................................................................................................. 45
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 2 of 50 Revised as of 9-4-14
27. Surgery: Vascular ................................................................................................................................................................................. 45
28. Urology Clinic ....................................................................................................................................................................................... 47
29. Wound Clinic ........................................................................................................................................................................................ 49
MEDICAL REFERRAL GUIDELINES
Referral guidelines are indexed by specialty and in alphabetical order.
1. Access Clinic Return
Criteria Comments
Located in Family Care Clinic 2,The Access Clinic is a medical home designed to provide coordinated primary care for adults with chronic physical or mental disabilities, including: adults with chronic disabilities, mental or physical (including but not limited to developmental delay, Down’s syndrome, Autism, paraplegia, quadriplegia, schizophrenia, bipolar disorder) with complex care needs who might benefit from improved case coordination from a multi-disciplinary team specializing in care of the disabled.
1. Covered by IEHP. Requires Prior-Authorization.
2. Chronically disabled due to a medical or psychiatric condition
3. On SSI or SDI
4. 18 years or older
Phone: 951-486-5573
The Access Clinic does not do disability determinations. The clinic is designed for patients with well established disabilities who have complex care needs.
2. Cardiac Clinic Return
Diagnosis Supporting Documents/Tests
Chest Pain Referrals a. EKG
b. Exercise or pharmacological stress test with results
c. Previous coronary angiogram reports (if done)
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 3 of 50 Revised as of 9-4-14
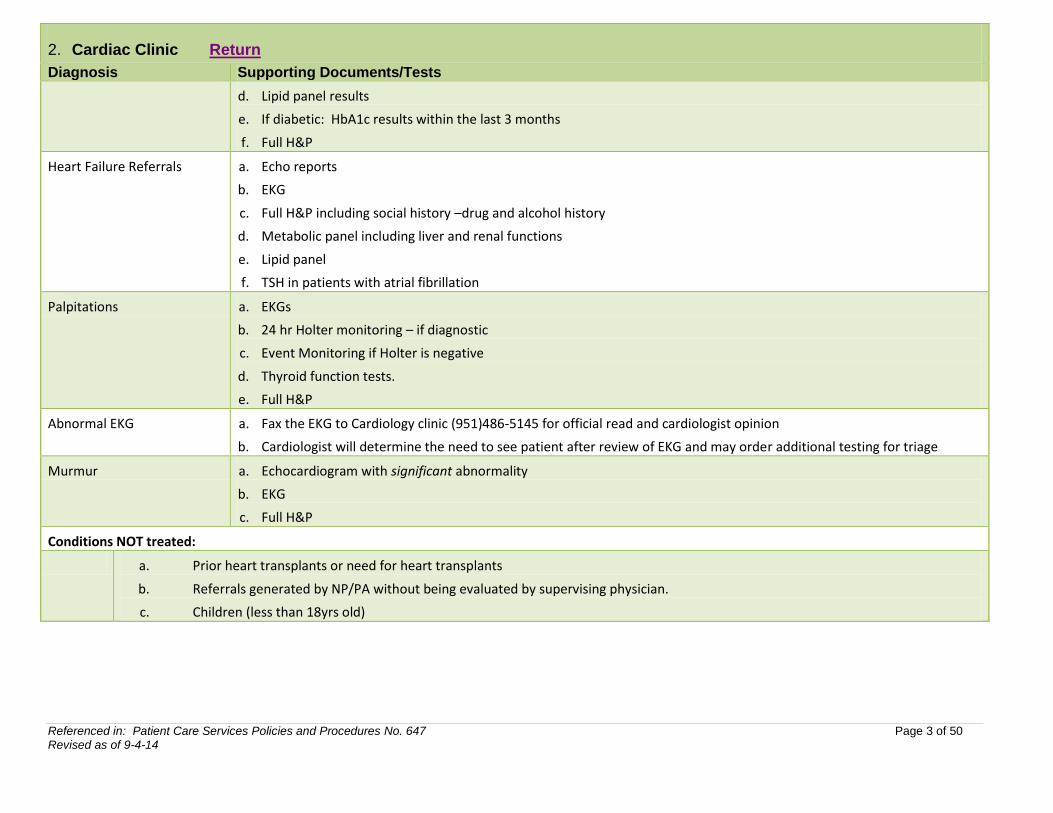
2. Cardiac Clinic Return
Diagnosis Supporting Documents/Tests
d. Lipid panel results
e. If diabetic: HbA1c results within the last 3 months
f. Full H&P
Heart Failure Referrals a. Echo reports
b. EKG
c. Full H&P including social history –drug and alcohol history
d. Metabolic panel including liver and renal functions
e. Lipid panel
f. TSH in patients with atrial fibrillation
Palpitations a. EKGs
b. 24 hr Holter monitoring – if diagnostic
c. Event Monitoring if Holter is negative
d. Thyroid function tests.
e. Full H&P
Abnormal EKG a. Fax the EKG to Cardiology clinic (951)486-5145 for official read and cardiologist opinion
b. Cardiologist will determine the need to see patient after review of EKG and may order additional testing for triage
Murmur a. Echocardiogram with significant abnormality
b. EKG
c. Full H&P
Conditions NOT treated:
a. Prior heart transplants or need for heart transplants
b. Referrals generated by NP/PA without being evaluated by supervising physician.
c. Children (less than 18yrs old)
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 4 of 50 Revised as of 9-4-14
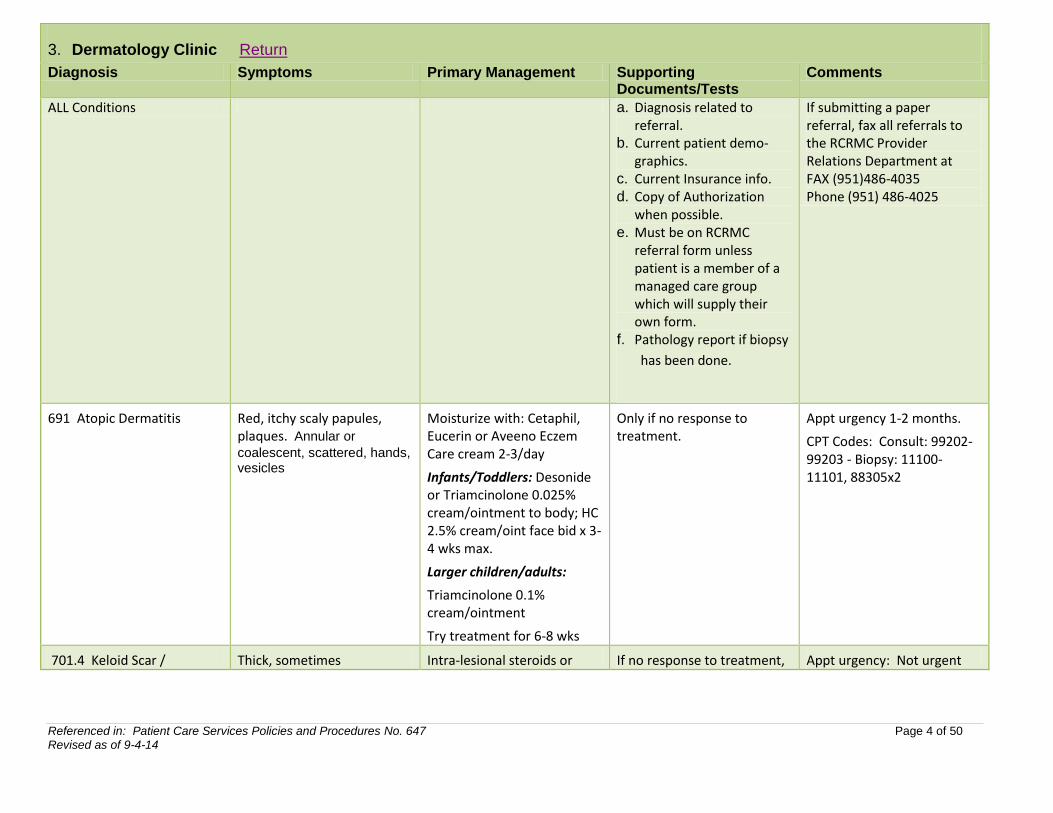
3. Dermatology Clinic Return
Diagnosis Symptoms Primary Management Supporting Documents/Tests
Comments
ALL Conditions a. Diagnosis related to referral.
b. Current patient demo-graphics.
c. Current Insurance info. d. Copy of Authorization
when possible. e. Must be on RCRMC
referral form unless patient is a member of a managed care group which will supply their own form.
f. Pathology report if biopsy
has been done.
If submitting a paper referral, fax all referrals to the RCRMC Provider Relations Department at FAX (951)486-4035 Phone (951) 486-4025
691 Atopic Dermatitis Red, itchy scaly papules, plaques. Annular or
coalescent, scattered, hands, vesicles
Moisturize with: Cetaphil, Eucerin or Aveeno Eczem Care cream 2-3/day
Infants/Toddlers: Desonide or Triamcinolone 0.025% cream/ointment to body; HC 2.5% cream/oint face bid x 3-4 wks max.
Larger children/adults:
Triamcinolone 0.1% cream/ointment
Try treatment for 6-8 wks
Only if no response to treatment.
Appt urgency 1-2 months.
CPT Codes: Consult: 99202- 99203 - Biopsy: 11100-11101, 88305x2
701.4 Keloid Scar / Thick, sometimes Intra-lesional steroids or If no response to treatment, Appt urgency: Not urgent
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 5 of 50 Revised as of 9-4-14
3. Dermatology Clinic Return
Diagnosis Symptoms Primary Management Supporting Documents/Tests
Comments
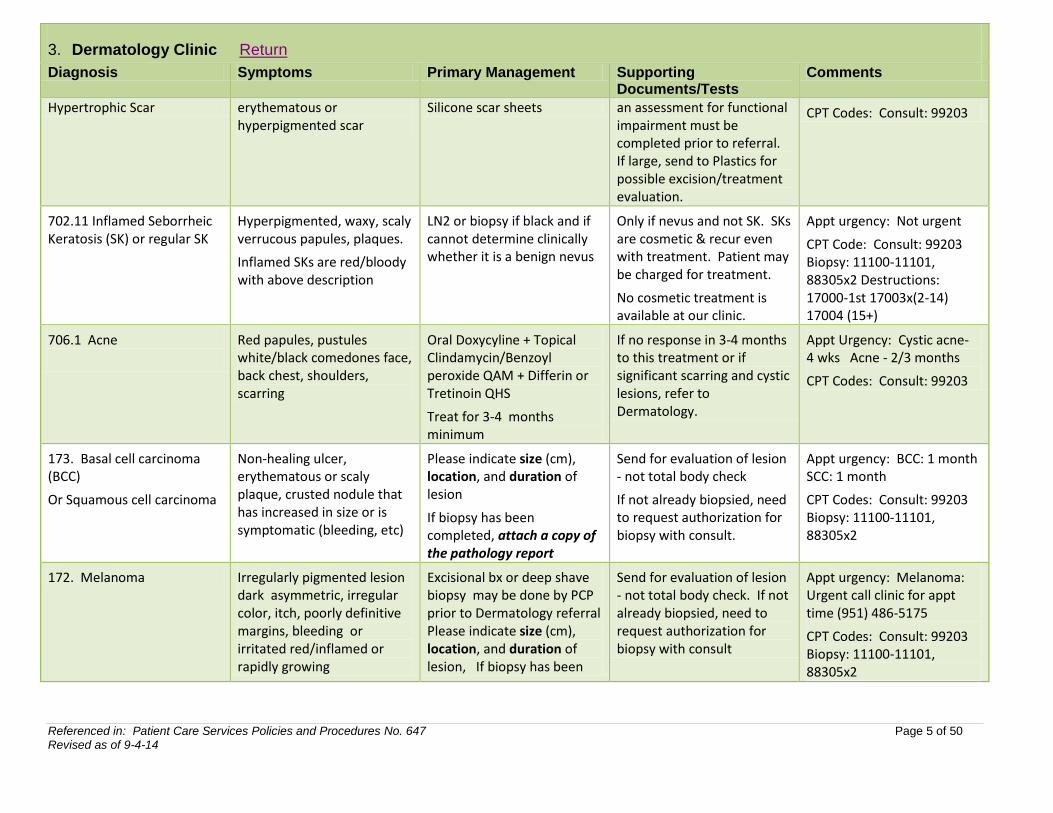
Hypertrophic Scar erythematous or hyperpigmented scar
Silicone scar sheets an assessment for functional impairment must be completed prior to referral. If large, send to Plastics for possible excision/treatment evaluation.
CPT Codes: Consult: 99203
702.11 Inflamed Seborrheic Keratosis (SK) or regular SK
Hyperpigmented, waxy, scaly verrucous papules, plaques.
Inflamed SKs are red/bloody with above description
LN2 or biopsy if black and if cannot determine clinically whether it is a benign nevus
Only if nevus and not SK. SKs are cosmetic & recur even with treatment. Patient may be charged for treatment.
No cosmetic treatment is available at our clinic.
Appt urgency: Not urgent
CPT Code: Consult: 99203 Biopsy: 11100-11101, 88305x2 Destructions: 17000-1st 17003x(2-14) 17004 (15+)
706.1 Acne
Red papules, pustules white/black comedones face, back chest, shoulders, scarring
Oral Doxycyline + Topical Clindamycin/Benzoyl peroxide QAM + Differin or Tretinoin QHS
Treat for 3-4 months minimum
If no response in 3-4 months to this treatment or if significant scarring and cystic lesions, refer to Dermatology.
Appt Urgency: Cystic acne- 4 wks Acne - 2/3 months
CPT Codes: Consult: 99203
173. Basal cell carcinoma (BCC)
Or Squamous cell carcinoma
Non-healing ulcer, erythematous or scaly plaque, crusted nodule that has increased in size or is symptomatic (bleeding, etc)
Please indicate size (cm), location, and duration of lesion
If biopsy has been completed, attach a copy of the pathology report
Send for evaluation of lesion - not total body check
If not already biopsied, need to request authorization for biopsy with consult.
Appt urgency: BCC: 1 month SCC: 1 month
CPT Codes: Consult: 99203 Biopsy: 11100-11101, 88305x2
172. Melanoma Irregularly pigmented lesion dark asymmetric, irregular color, itch, poorly definitive margins, bleeding or irritated red/inflamed or rapidly growing
Excisional bx or deep shave biopsy may be done by PCP prior to Dermatology referral Please indicate size (cm), location, and duration of lesion, If biopsy has been
Send for evaluation of lesion - not total body check. If not already biopsied, need to request authorization for biopsy with consult
Appt urgency: Melanoma: Urgent call clinic for appt time (951) 486-5175
CPT Codes: Consult: 99203 Biopsy: 11100-11101, 88305x2
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 6 of 50 Revised as of 9-4-14
3. Dermatology Clinic Return
Diagnosis Symptoms Primary Management Supporting Documents/Tests
Comments
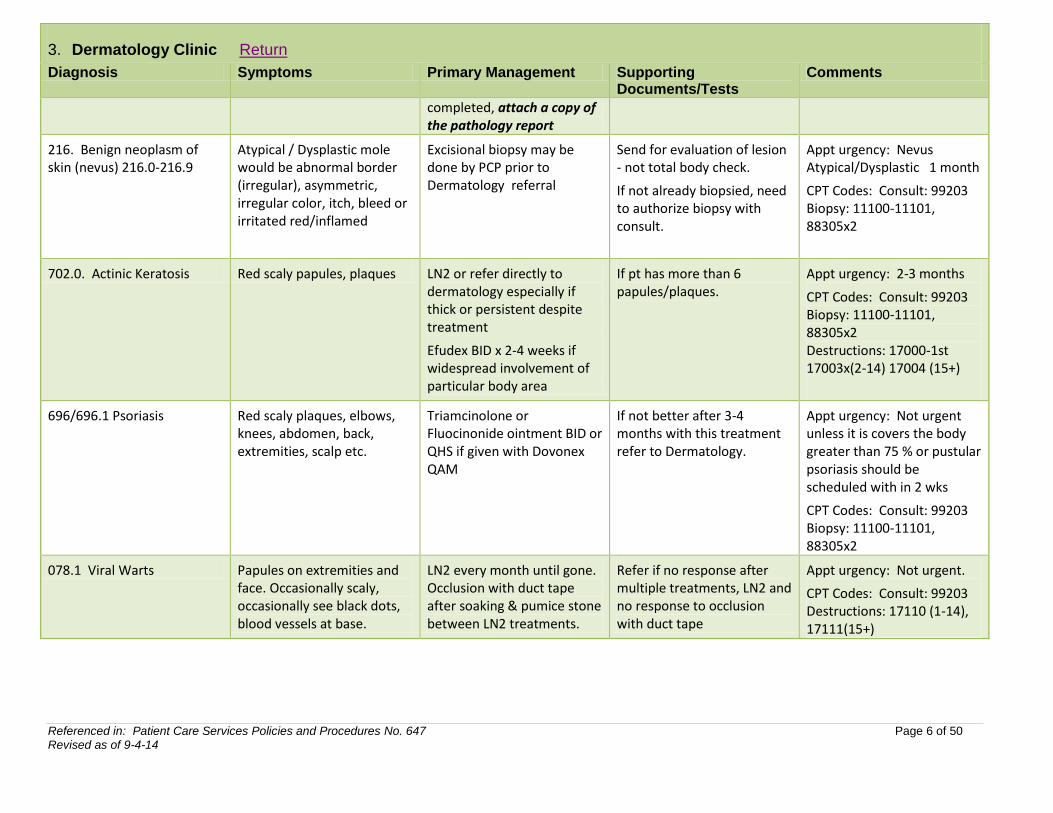
completed, attach a copy of the pathology report
216. Benign neoplasm of skin (nevus) 216.0-216.9
Atypical / Dysplastic mole would be abnormal border (irregular), asymmetric, irregular color, itch, bleed or irritated red/inflamed
Excisional biopsy may be done by PCP prior to Dermatology referral
Send for evaluation of lesion - not total body check.
If not already biopsied, need to authorize biopsy with consult.
Appt urgency: Nevus Atypical/Dysplastic 1 month
CPT Codes: Consult: 99203 Biopsy: 11100-11101, 88305x2
702.0. Actinic Keratosis Red scaly papules, plaques LN2 or refer directly to dermatology especially if thick or persistent despite treatment
Efudex BID x 2-4 weeks if widespread involvement of particular body area
If pt has more than 6 papules/plaques.
Appt urgency: 2-3 months
CPT Codes: Consult: 99203 Biopsy: 11100-11101, 88305x2 Destructions: 17000-1st 17003x(2-14) 17004 (15+)
696/696.1 Psoriasis
Red scaly plaques, elbows, knees, abdomen, back, extremities, scalp etc.
Triamcinolone or Fluocinonide ointment BID or QHS if given with Dovonex QAM
If not better after 3-4 months with this treatment refer to Dermatology.
Appt urgency: Not urgent unless it is covers the body greater than 75 % or pustular psoriasis should be scheduled with in 2 wks
CPT Codes: Consult: 99203 Biopsy: 11100-11101, 88305x2
078.1 Viral Warts Papules on extremities and face. Occasionally scaly, occasionally see black dots, blood vessels at base.
LN2 every month until gone. Occlusion with duct tape after soaking & pumice stone between LN2 treatments.
Refer if no response after multiple treatments, LN2 and no response to occlusion with duct tape
Appt urgency: Not urgent.
CPT Codes: Consult: 99203 Destructions: 17110 (1-14), 17111(15+)
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 7 of 50 Revised as of 9-4-14
4. Diabetes Clinic Return
Diagnosis Supporting Documents/Tests
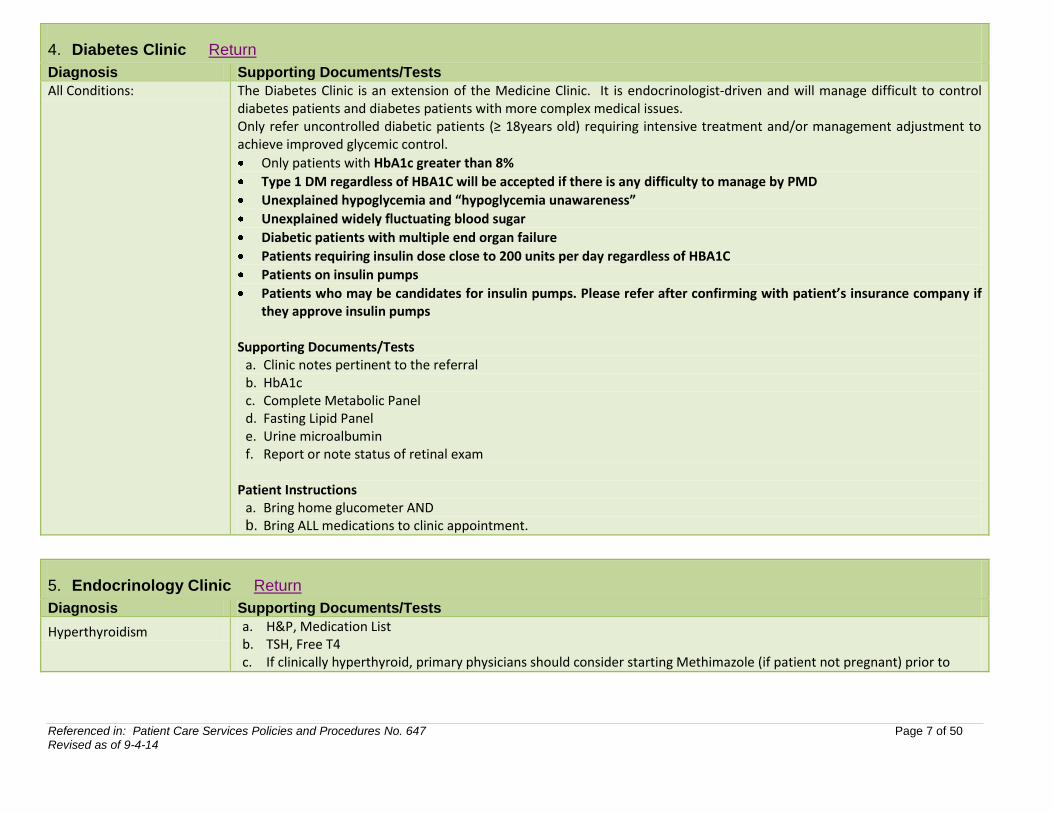
All Conditions: The Diabetes Clinic is an extension of the Medicine Clinic. It is endocrinologist-driven and will manage difficult to control diabetes patients and diabetes patients with more complex medical issues. Only refer uncontrolled diabetic patients (≥ 18years old) requiring intensive treatment and/or management adjustment to achieve improved glycemic control.
Only patients with HbA1c greater than 8%
Type 1 DM regardless of HBA1C will be accepted if there is any difficulty to manage by PMD
Unexplained hypoglycemia and “hypoglycemia unawareness”
Unexplained widely fluctuating blood sugar
Diabetic patients with multiple end organ failure
Patients requiring insulin dose close to 200 units per day regardless of HBA1C
Patients on insulin pumps
Patients who may be candidates for insulin pumps. Please refer after confirming with patient’s insurance company if they approve insulin pumps
Supporting Documents/Tests a. Clinic notes pertinent to the referral b. HbA1c c. Complete Metabolic Panel d. Fasting Lipid Panel e. Urine microalbumin f. Report or note status of retinal exam
Patient Instructions
a. Bring home glucometer AND b. Bring ALL medications to clinic appointment.
5. Endocrinology Clinic Return
Diagnosis Supporting Documents/Tests
Hyperthyroidism a. H&P, Medication List b. TSH, Free T4 c. If clinically hyperthyroid, primary physicians should consider starting Methimazole (if patient not pregnant) prior to
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 8 of 50 Revised as of 9-4-14
5. Endocrinology Clinic Return
Diagnosis Supporting Documents/Tests
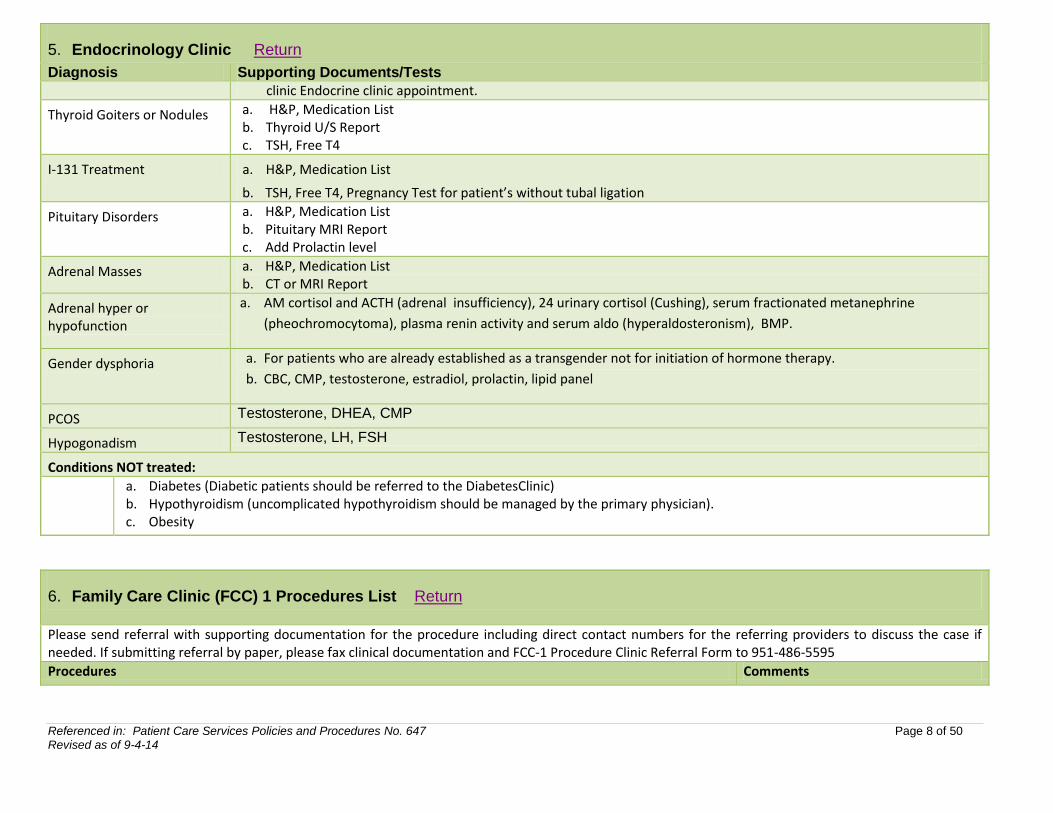
clinic Endocrine clinic appointment.
Thyroid Goiters or Nodules a. H&P, Medication List b. Thyroid U/S Report c. TSH, Free T4
I-131 Treatment a. H&P, Medication List
b. TSH, Free T4, Pregnancy Test for patient’s without tubal ligation
Pituitary Disorders a. H&P, Medication List b. Pituitary MRI Report c. Add Prolactin level
Adrenal Masses a. H&P, Medication List b. CT or MRI Report
Adrenal hyper or hypofunction
a. AM cortisol and ACTH (adrenal insufficiency), 24 urinary cortisol (Cushing), serum fractionated metanephrine
(pheochromocytoma), plasma renin activity and serum aldo (hyperaldosteronism), BMP.
Gender dysphoria a. For patients who are already established as a transgender not for initiation of hormone therapy.
b. CBC, CMP, testosterone, estradiol, prolactin, lipid panel
PCOS Testosterone, DHEA, CMP
Hypogonadism Testosterone, LH, FSH
Conditions NOT treated:
a. Diabetes (Diabetic patients should be referred to the DiabetesClinic) b. Hypothyroidism (uncomplicated hypothyroidism should be managed by the primary physician). c. Obesity
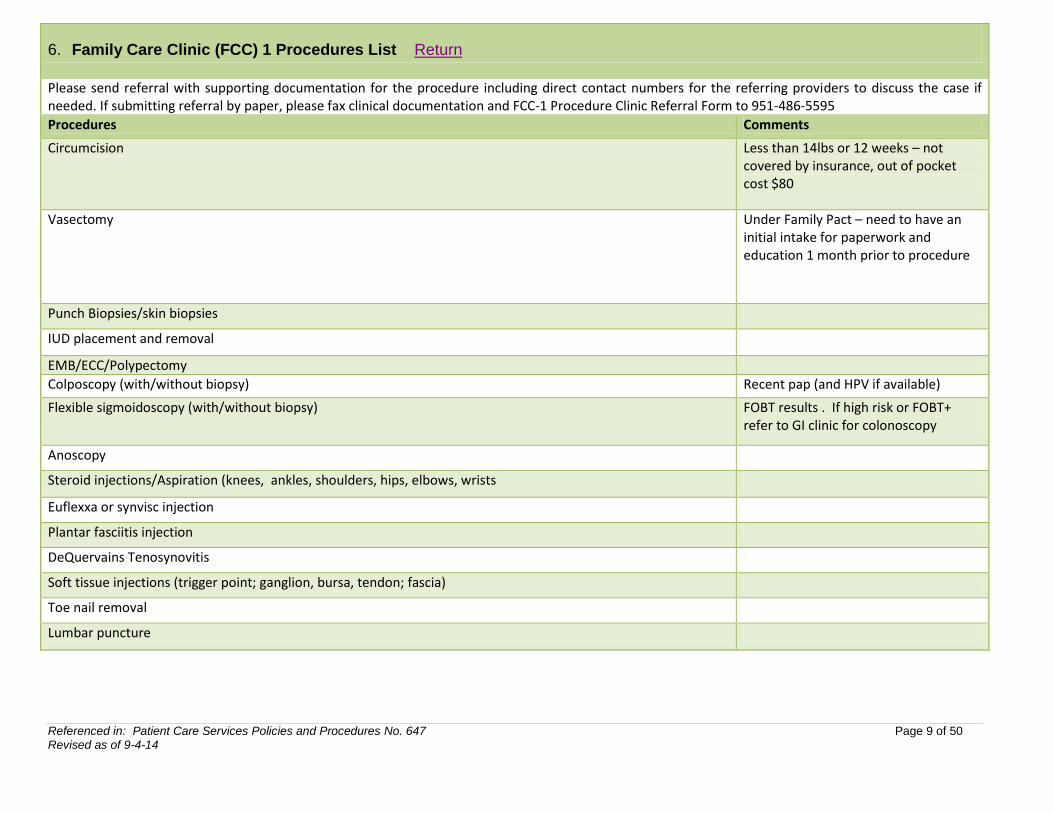
6. Family Care Clinic (FCC) 1 Procedures List Return
Please send referral with supporting documentation for the procedure including direct contact numbers for the referring providers to discuss the case if needed. If submitting referral by paper, please fax clinical documentation and FCC-1 Procedure Clinic Referral Form to 951-486-5595
Procedures Comments
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 9 of 50 Revised as of 9-4-14
6. Family Care Clinic (FCC) 1 Procedures List Return
Please send referral with supporting documentation for the procedure including direct contact numbers for the referring providers to discuss the case if needed. If submitting referral by paper, please fax clinical documentation and FCC-1 Procedure Clinic Referral Form to 951-486-5595
Procedures Comments
Circumcision Less than 14lbs or 12 weeks – not covered by insurance, out of pocket cost $80
Vasectomy Under Family Pact – need to have an initial intake for paperwork and education 1 month prior to procedure
Punch Biopsies/skin biopsies
IUD placement and removal
EMB/ECC/Polypectomy
Colposcopy (with/without biopsy) Recent pap (and HPV if available)
Flexible sigmoidoscopy (with/without biopsy) FOBT results . If high risk or FOBT+ refer to GI clinic for colonoscopy
Anoscopy
Steroid injections/Aspiration (knees, ankles, shoulders, hips, elbows, wrists
Euflexxa or synvisc injection
Plantar fasciitis injection
DeQuervains Tenosynovitis
Soft tissue injections (trigger point; ganglion, bursa, tendon; fascia)
Toe nail removal
Lumbar puncture

Referenced in: Patient Care Services Policies and Procedures No. 647 Page 10 of 50 Revised as of 9-4-14
6. Family Care Clinic (FCC) 1 Procedures List Return
Please send referral with supporting documentation for the procedure including direct contact numbers for the referring providers to discuss the case if needed. If submitting referral by paper, please fax clinical documentation and FCC-1 Procedure Clinic Referral Form to 951-486-5595
Procedures Comments
Lump/bumps/Cysts - excisions If >4cm, or on face/neck call to discuss (see below)
Fine needle aspiration
I&D
Cryotherapy
Injection of Chalazion-eye (if failed conservative measures)
Paracentesis
Thoracentesis**
** Please call Dr. Jukaku to review these cases for approval/advice.
Hospital cell: 951 232 4856.
Email at [email protected]
Bone marrow biopsy**
Lymph node, muscle biopsy**
Nasolaryngoscopy**
Insertion of word catheter for bartholin cyst**
Long term catheter removal (dialysis cath, etc.)**
Removal of peg tube**
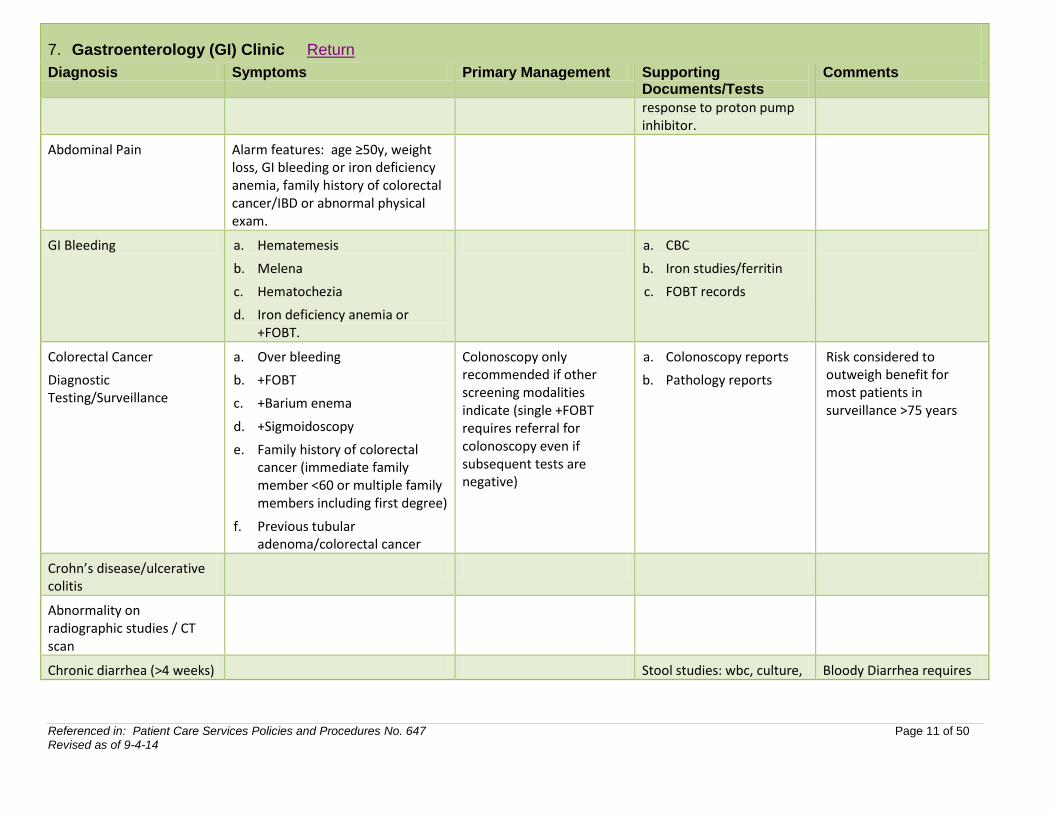
7. Gastroenterology (GI) Clinic Return
Diagnosis Symptoms Primary Management Supporting Documents/Tests
Comments
Dyspepsia
Alarm features: age≥50y, family history of upper GI malignancy, weight loss, GI bleeding or iron deficiency anemia, dysphagia, odynophagia, or vomiting.
Documentation of evaluation and/or treatment of Helicobacter pylori infection (stool antigen preferred) and
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 11 of 50 Revised as of 9-4-14
7. Gastroenterology (GI) Clinic Return
Diagnosis Symptoms Primary Management Supporting Documents/Tests
Comments
response to proton pump inhibitor.
Abdominal Pain Alarm features: age ≥50y, weight loss, GI bleeding or iron deficiency anemia, family history of colorectal cancer/IBD or abnormal physical exam.
GI Bleeding a. Hematemesis
b. Melena
c. Hematochezia
d. Iron deficiency anemia or +FOBT.
a. CBC
b. Iron studies/ferritin
c. FOBT records
Colorectal Cancer
Diagnostic Testing/Surveillance
a. Over bleeding
b. +FOBT
c. +Barium enema
d. +Sigmoidoscopy
e. Family history of colorectal cancer (immediate family member <60 or multiple family members including first degree)
f. Previous tubular adenoma/colorectal cancer
Colonoscopy only recommended if other screening modalities indicate (single +FOBT requires referral for colonoscopy even if subsequent tests are negative)
a. Colonoscopy reports
b. Pathology reports
Risk considered to outweigh benefit for most patients in surveillance >75 years
Crohn’s disease/ulcerative colitis
Abnormality on radiographic studies / CT scan
Chronic diarrhea (>4 weeks) Stool studies: wbc, culture, Bloody Diarrhea requires
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 12 of 50 Revised as of 9-4-14
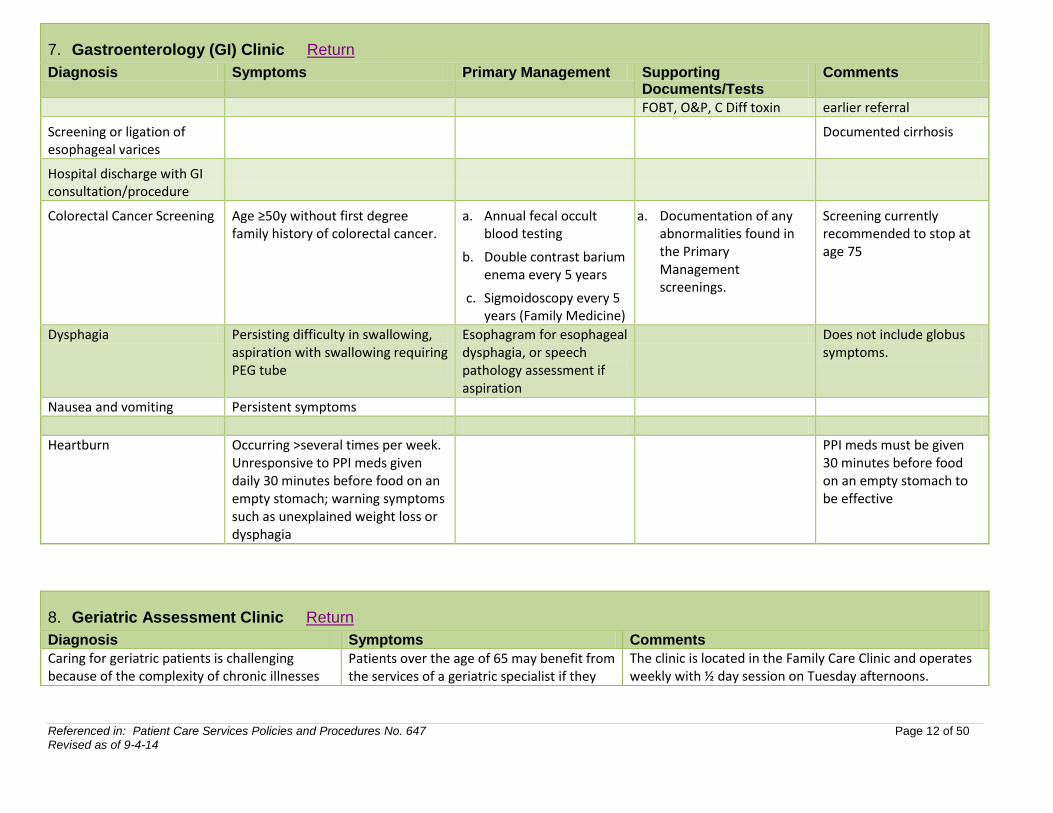
7. Gastroenterology (GI) Clinic Return
Diagnosis Symptoms Primary Management Supporting Documents/Tests
Comments
FOBT, O&P, C Diff toxin earlier referral
Screening or ligation of esophageal varices
Documented cirrhosis
Hospital discharge with GI consultation/procedure
Colorectal Cancer Screening Age ≥50y without first degree family history of colorectal cancer.
a. Annual fecal occult blood testing
b. Double contrast barium enema every 5 years
c. Sigmoidoscopy every 5 years (Family Medicine)
a. Documentation of any abnormalities found in the Primary Management screenings.
Screening currently recommended to stop at age 75
Dysphagia Persisting difficulty in swallowing, aspiration with swallowing requiring PEG tube
Esophagram for esophageal dysphagia, or speech pathology assessment if aspiration
Does not include globus symptoms.
Nausea and vomiting Persistent symptoms
Heartburn Occurring >several times per week. Unresponsive to PPI meds given daily 30 minutes before food on an empty stomach; warning symptoms such as unexplained weight loss or dysphagia
PPI meds must be given 30 minutes before food on an empty stomach to be effective
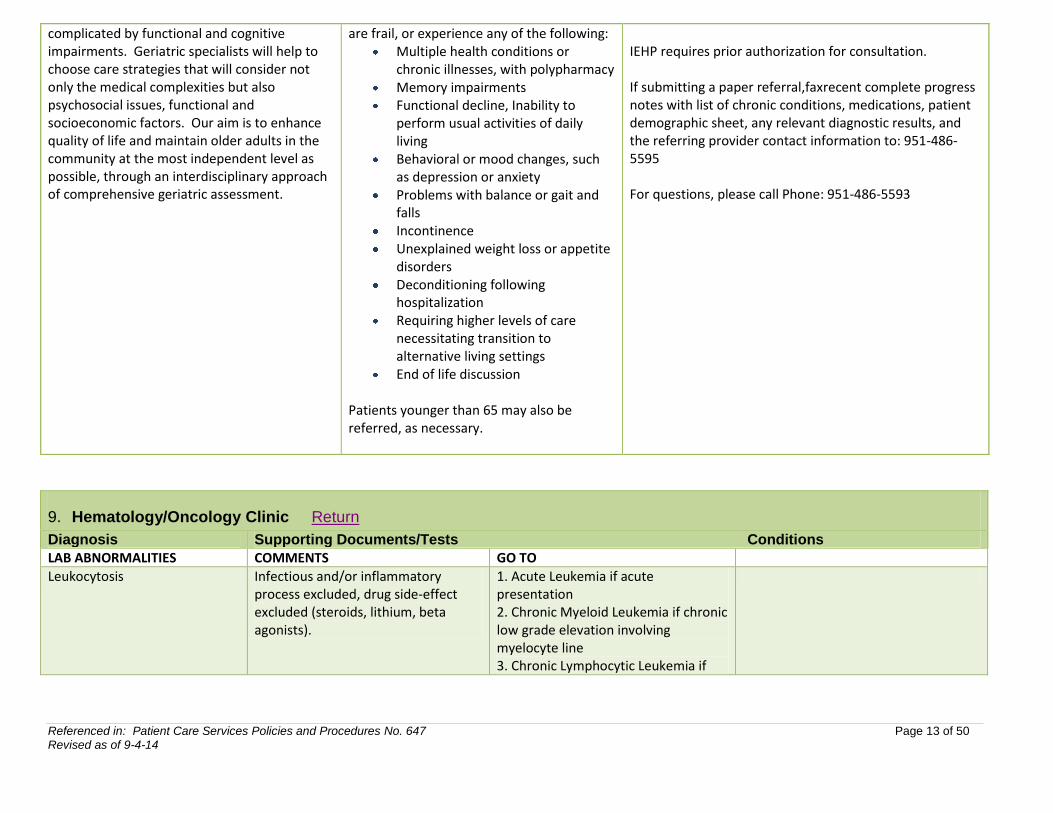
8. Geriatric Assessment Clinic Return
Diagnosis Symptoms Comments
Caring for geriatric patients is challenging because of the complexity of chronic illnesses
Patients over the age of 65 may benefit from the services of a geriatric specialist if they
The clinic is located in the Family Care Clinic and operates weekly with ½ day session on Tuesday afternoons.
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 13 of 50 Revised as of 9-4-14
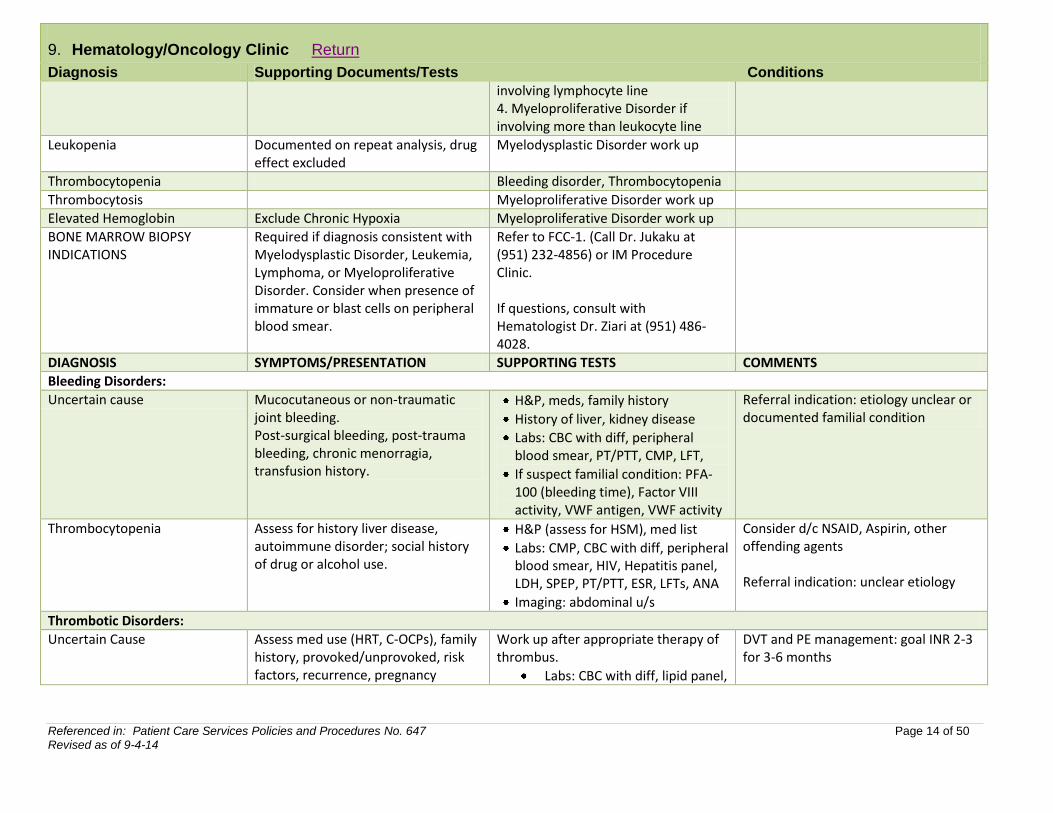
9. Hematology/Oncology Clinic Return
Diagnosis Supporting Documents/Tests Conditions
LAB ABNORMALITIES COMMENTS GO TO
Leukocytosis Infectious and/or inflammatory process excluded, drug side-effect excluded (steroids, lithium, beta agonists).
1. Acute Leukemia if acute presentation 2. Chronic Myeloid Leukemia if chronic low grade elevation involving myelocyte line 3. Chronic Lymphocytic Leukemia if
complicated by functional and cognitive impairments. Geriatric specialists will help to choose care strategies that will consider not only the medical complexities but also psychosocial issues, functional and socioeconomic factors. Our aim is to enhance quality of life and maintain older adults in the community at the most independent level as possible, through an interdisciplinary approach of comprehensive geriatric assessment.
are frail, or experience any of the following: Multiple health conditions or
chronic illnesses, with polypharmacy Memory impairments Functional decline, Inability to
perform usual activities of daily living
Behavioral or mood changes, such as depression or anxiety
Problems with balance or gait and falls
Incontinence Unexplained weight loss or appetite
disorders Deconditioning following
hospitalization Requiring higher levels of care
necessitating transition to alternative living settings
End of life discussion
Patients younger than 65 may also be referred, as necessary.
IEHP requires prior authorization for consultation. If submitting a paper referral,faxrecent complete progress notes with list of chronic conditions, medications, patient demographic sheet, any relevant diagnostic results, and the referring provider contact information to: 951-486-5595 For questions, please call Phone: 951-486-5593
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 14 of 50 Revised as of 9-4-14
9. Hematology/Oncology Clinic Return
Diagnosis Supporting Documents/Tests Conditions
involving lymphocyte line 4. Myeloproliferative Disorder if involving more than leukocyte line
Leukopenia Documented on repeat analysis, drug effect excluded
Myelodysplastic Disorder work up
Thrombocytopenia Bleeding disorder, Thrombocytopenia
Thrombocytosis Myeloproliferative Disorder work up
Elevated Hemoglobin Exclude Chronic Hypoxia Myeloproliferative Disorder work up
BONE MARROW BIOPSY INDICATIONS
Required if diagnosis consistent with Myelodysplastic Disorder, Leukemia, Lymphoma, or Myeloproliferative Disorder. Consider when presence of immature or blast cells on peripheral blood smear.
Refer to FCC-1. (Call Dr. Jukaku at (951) 232-4856) or IM Procedure Clinic. If questions, consult with Hematologist Dr. Ziari at (951) 486-4028.
DIAGNOSIS SYMPTOMS/PRESENTATION SUPPORTING TESTS COMMENTS
Bleeding Disorders:
Uncertain cause Mucocutaneous or non-traumatic joint bleeding. Post-surgical bleeding, post-trauma bleeding, chronic menorragia, transfusion history.
H&P, meds, family history
History of liver, kidney disease
Labs: CBC with diff, peripheral blood smear, PT/PTT, CMP, LFT,
If suspect familial condition: PFA-100 (bleeding time), Factor VIII activity, VWF antigen, VWF activity
Referral indication: etiology unclear or documented familial condition
Thrombocytopenia Assess for history liver disease, autoimmune disorder; social history of drug or alcohol use.
H&P (assess for HSM), med list
Labs: CMP, CBC with diff, peripheral blood smear, HIV, Hepatitis panel, LDH, SPEP, PT/PTT, ESR, LFTs, ANA
Imaging: abdominal u/s
Consider d/c NSAID, Aspirin, other offending agents Referral indication: unclear etiology
Thrombotic Disorders:
Uncertain Cause Assess med use (HRT, C-OCPs), family history, provoked/unprovoked, risk factors, recurrence, pregnancy
Work up after appropriate therapy of thrombus.
Labs: CBC with diff, lipid panel,
DVT and PE management: goal INR 2-3 for 3-6 months
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 15 of 50 Revised as of 9-4-14
9. Hematology/Oncology Clinic Return
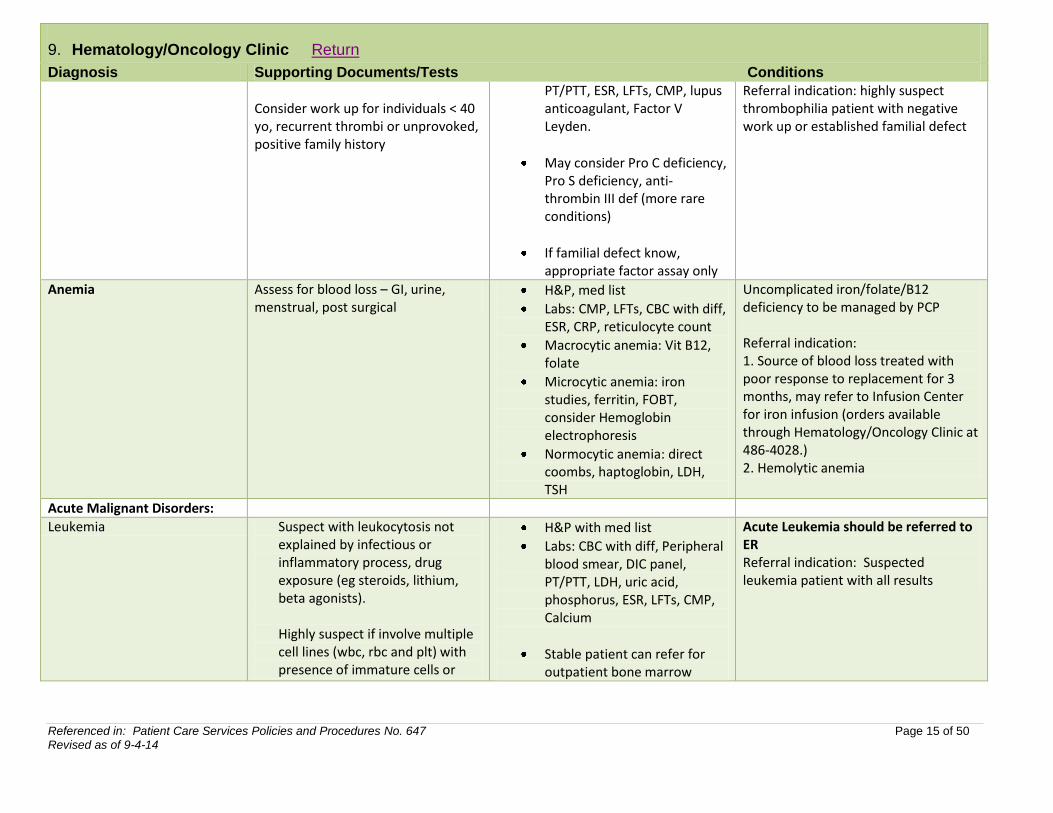
Diagnosis Supporting Documents/Tests Conditions
Consider work up for individuals < 40 yo, recurrent thrombi or unprovoked, positive family history
PT/PTT, ESR, LFTs, CMP, lupus anticoagulant, Factor V Leyden.
May consider Pro C deficiency, Pro S deficiency, anti-thrombin III def (more rare conditions)
If familial defect know, appropriate factor assay only
Referral indication: highly suspect thrombophilia patient with negative work up or established familial defect
Anemia Assess for blood loss – GI, urine, menstrual, post surgical
H&P, med list
Labs: CMP, LFTs, CBC with diff, ESR, CRP, reticulocyte count
Macrocytic anemia: Vit B12, folate
Microcytic anemia: iron studies, ferritin, FOBT, consider Hemoglobin electrophoresis
Normocytic anemia: direct coombs, haptoglobin, LDH, TSH
Uncomplicated iron/folate/B12 deficiency to be managed by PCP Referral indication: 1. Source of blood loss treated with poor response to replacement for 3 months, may refer to Infusion Center for iron infusion (orders available through Hematology/Oncology Clinic at 486-4028.) 2. Hemolytic anemia
Acute Malignant Disorders:
Leukemia Suspect with leukocytosis not explained by infectious or inflammatory process, drug exposure (eg steroids, lithium, beta agonists). Highly suspect if involve multiple cell lines (wbc, rbc and plt) with presence of immature cells or
H&P with med list
Labs: CBC with diff, Peripheral blood smear, DIC panel, PT/PTT, LDH, uric acid, phosphorus, ESR, LFTs, CMP, Calcium
Stable patient can refer for outpatient bone marrow
Acute Leukemia should be referred to ER Referral indication: Suspected leukemia patient with all results
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 16 of 50 Revised as of 9-4-14
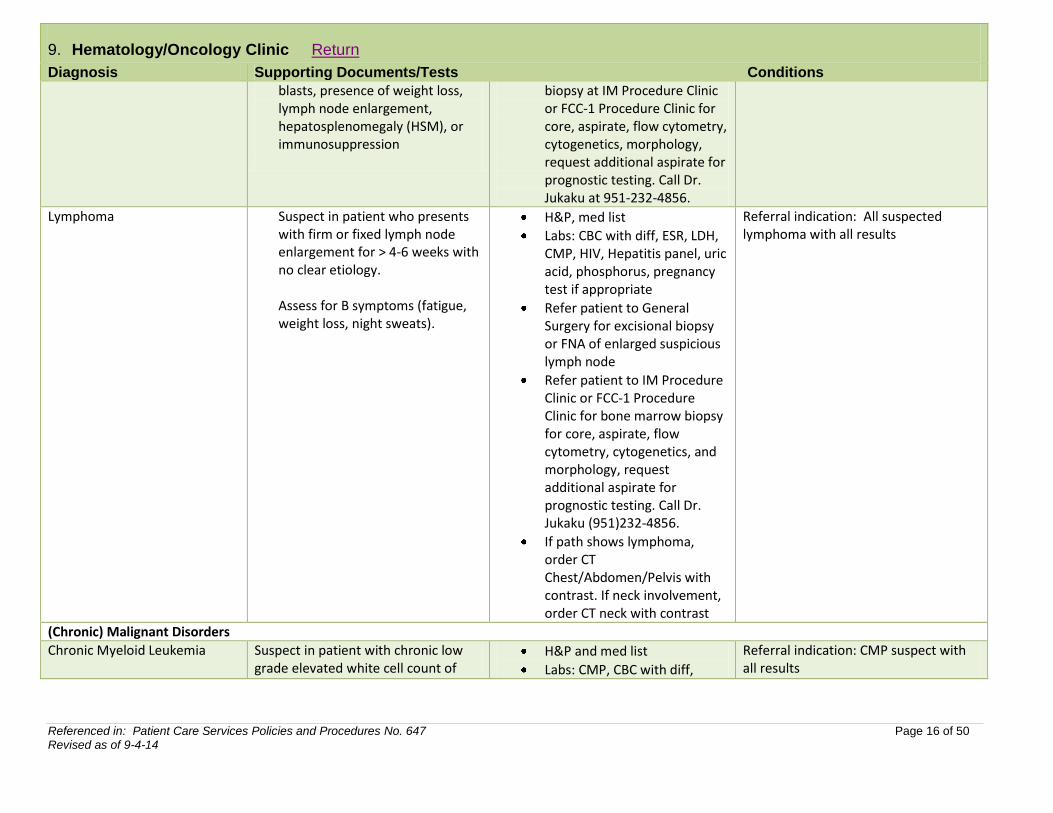
9. Hematology/Oncology Clinic Return
Diagnosis Supporting Documents/Tests Conditions
blasts, presence of weight loss, lymph node enlargement, hepatosplenomegaly (HSM), or immunosuppression
biopsy at IM Procedure Clinic or FCC-1 Procedure Clinic for core, aspirate, flow cytometry, cytogenetics, morphology, request additional aspirate for prognostic testing. Call Dr. Jukaku at 951-232-4856.
Lymphoma Suspect in patient who presents with firm or fixed lymph node enlargement for > 4-6 weeks with no clear etiology. Assess for B symptoms (fatigue, weight loss, night sweats).
H&P, med list
Labs: CBC with diff, ESR, LDH, CMP, HIV, Hepatitis panel, uric acid, phosphorus, pregnancy test if appropriate
Refer patient to General Surgery for excisional biopsy or FNA of enlarged suspicious lymph node
Refer patient to IM Procedure Clinic or FCC-1 Procedure Clinic for bone marrow biopsy for core, aspirate, flow cytometry, cytogenetics, and morphology, request additional aspirate for prognostic testing. Call Dr. Jukaku (951)232-4856.
If path shows lymphoma, order CT Chest/Abdomen/Pelvis with contrast. If neck involvement, order CT neck with contrast
Referral indication: All suspected lymphoma with all results
(Chronic) Malignant Disorders
Chronic Myeloid Leukemia Suspect in patient with chronic low grade elevated white cell count of
H&P and med list
Labs: CMP, CBC with diff,
Referral indication: CMP suspect with all results
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 17 of 50 Revised as of 9-4-14
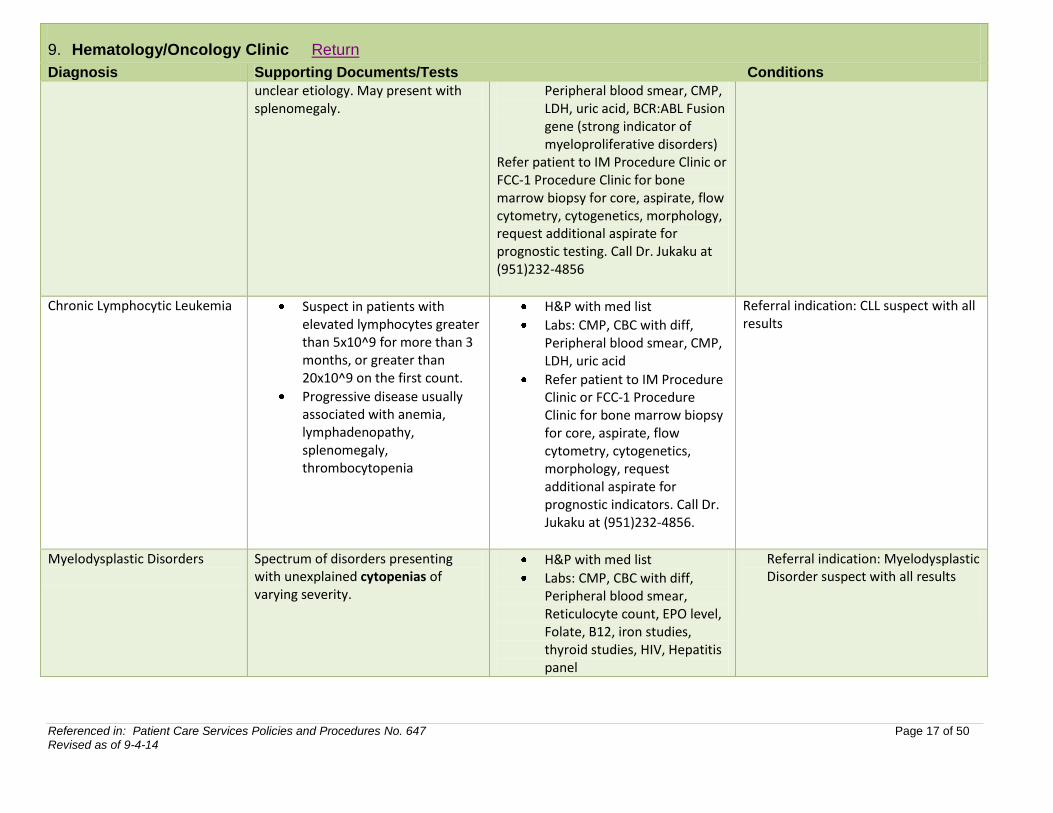
9. Hematology/Oncology Clinic Return
Diagnosis Supporting Documents/Tests Conditions
unclear etiology. May present with splenomegaly.
Peripheral blood smear, CMP, LDH, uric acid, BCR:ABL Fusion gene (strong indicator of myeloproliferative disorders)
Refer patient to IM Procedure Clinic or FCC-1 Procedure Clinic for bone marrow biopsy for core, aspirate, flow cytometry, cytogenetics, morphology, request additional aspirate for prognostic testing. Call Dr. Jukaku at (951)232-4856
Chronic Lymphocytic Leukemia Suspect in patients with elevated lymphocytes greater than 5x10^9 for more than 3 months, or greater than 20x10^9 on the first count.
Progressive disease usually associated with anemia, lymphadenopathy, splenomegaly, thrombocytopenia
H&P with med list
Labs: CMP, CBC with diff, Peripheral blood smear, CMP, LDH, uric acid
Refer patient to IM Procedure Clinic or FCC-1 Procedure Clinic for bone marrow biopsy for core, aspirate, flow cytometry, cytogenetics, morphology, request additional aspirate for prognostic indicators. Call Dr. Jukaku at (951)232-4856.
Referral indication: CLL suspect with all results
Myelodysplastic Disorders
Spectrum of disorders presenting with unexplained cytopenias of varying severity.
H&P with med list
Labs: CMP, CBC with diff, Peripheral blood smear, Reticulocyte count, EPO level, Folate, B12, iron studies, thyroid studies, HIV, Hepatitis panel
Referral indication: Myelodysplastic Disorder suspect with all results
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 18 of 50 Revised as of 9-4-14
9. Hematology/Oncology Clinic Return
Diagnosis Supporting Documents/Tests Conditions
If abnormal LFTs or Hepatitis, obtain abdominal u/s
Refer patient to IM Procedure Clinic or FCC-1 Procedure Clinic for bone marrow biopsy for core, aspirate, flow cytometry, cytogenetics, morphology, request additional aspirate for prognostic indicators. Call Dr. Jukaku at (951) 232-4856
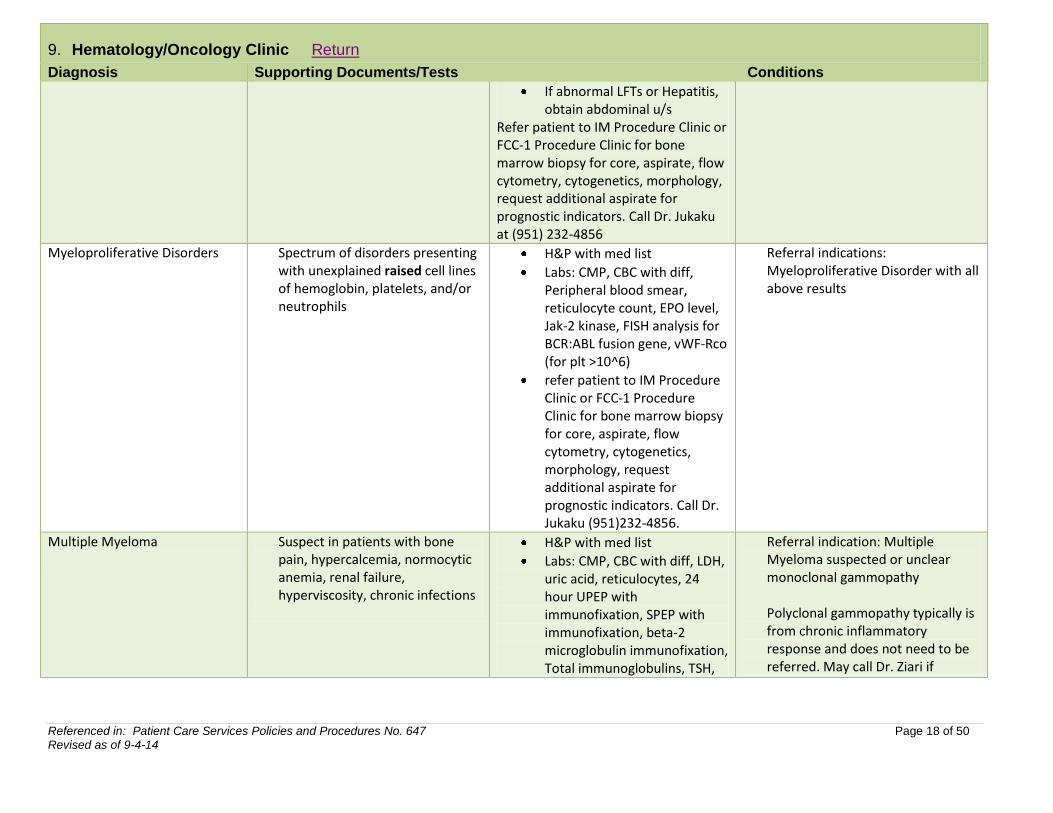
Myeloproliferative Disorders
Spectrum of disorders presenting with unexplained raised cell lines of hemoglobin, platelets, and/or neutrophils
H&P with med list
Labs: CMP, CBC with diff, Peripheral blood smear, reticulocyte count, EPO level, Jak-2 kinase, FISH analysis for BCR:ABL fusion gene, vWF-Rco (for plt >10^6)
refer patient to IM Procedure Clinic or FCC-1 Procedure Clinic for bone marrow biopsy for core, aspirate, flow cytometry, cytogenetics, morphology, request additional aspirate for prognostic indicators. Call Dr. Jukaku (951)232-4856.
Referral indications: Myeloproliferative Disorder with all above results
Multiple Myeloma
Suspect in patients with bone pain, hypercalcemia, normocytic anemia, renal failure, hyperviscosity, chronic infections
H&P with med list
Labs: CMP, CBC with diff, LDH, uric acid, reticulocytes, 24 hour UPEP with immunofixation, SPEP with immunofixation, beta-2 microglobulin immunofixation, Total immunoglobulins, TSH,
Referral indication: Multiple Myeloma suspected or unclear monoclonal gammopathy Polyclonal gammopathy typically is from chronic inflammatory response and does not need to be referred. May call Dr. Ziari if
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 19 of 50 Revised as of 9-4-14
9. Hematology/Oncology Clinic Return
Diagnosis Supporting Documents/Tests Conditions
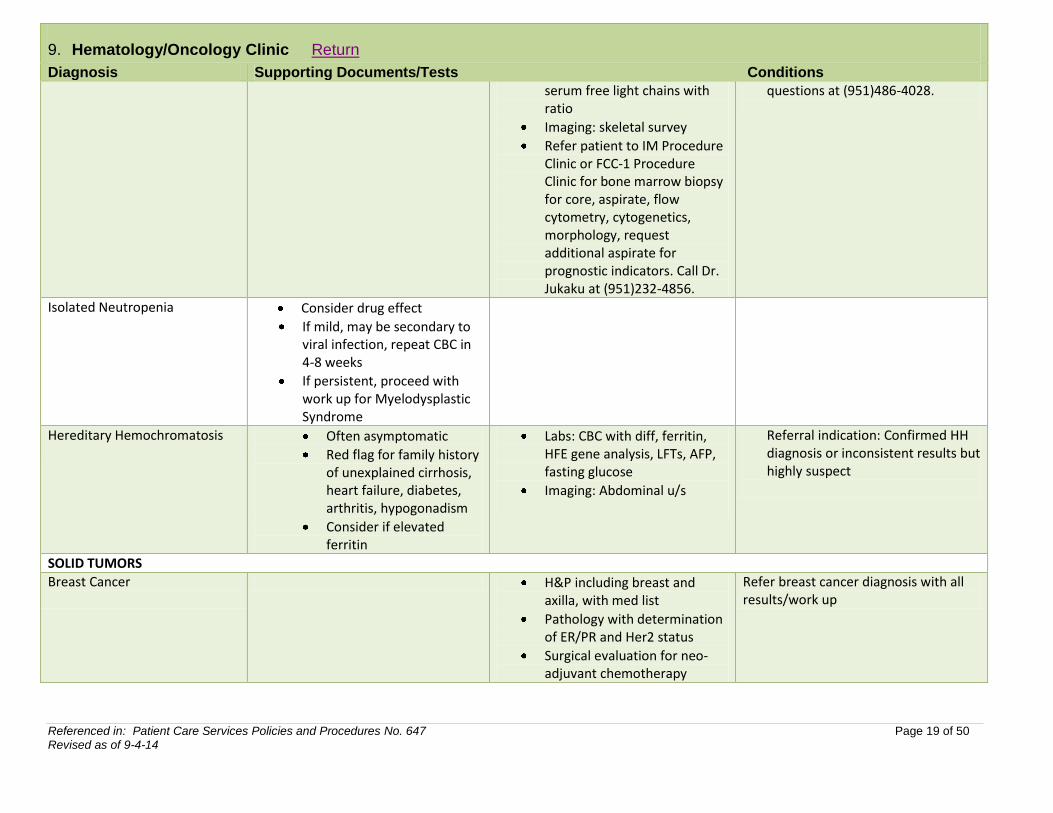
serum free light chains with ratio
Imaging: skeletal survey
Refer patient to IM Procedure Clinic or FCC-1 Procedure Clinic for bone marrow biopsy for core, aspirate, flow cytometry, cytogenetics, morphology, request additional aspirate for prognostic indicators. Call Dr. Jukaku at (951)232-4856.
questions at (951)486-4028.
Isolated Neutropenia
Consider drug effect
If mild, may be secondary to viral infection, repeat CBC in 4-8 weeks
If persistent, proceed with work up for Myelodysplastic Syndrome
Hereditary Hemochromatosis
Often asymptomatic
Red flag for family history of unexplained cirrhosis, heart failure, diabetes, arthritis, hypogonadism
Consider if elevated ferritin
Labs: CBC with diff, ferritin, HFE gene analysis, LFTs, AFP, fasting glucose
Imaging: Abdominal u/s
Referral indication: Confirmed HH diagnosis or inconsistent results but highly suspect
SOLID TUMORS
Breast Cancer
H&P including breast and axilla, with med list
Pathology with determination of ER/PR and Her2 status
Surgical evaluation for neo-adjuvant chemotherapy
Refer breast cancer diagnosis with all results/work up
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 20 of 50 Revised as of 9-4-14
9. Hematology/Oncology Clinic Return
Diagnosis Supporting Documents/Tests Conditions
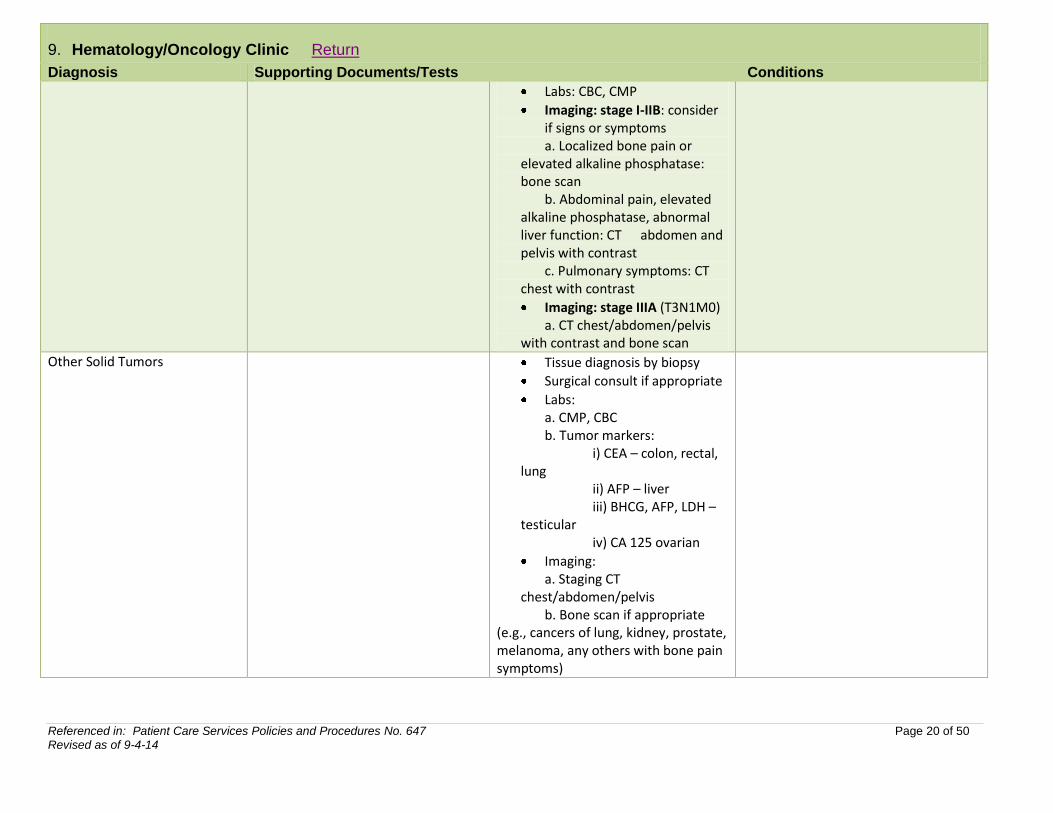
Labs: CBC, CMP
Imaging: stage I-IIB: consider if signs or symptoms
a. Localized bone pain or elevated alkaline phosphatase: bone scan b. Abdominal pain, elevated alkaline phosphatase, abnormal liver function: CT abdomen and pelvis with contrast c. Pulmonary symptoms: CT chest with contrast
Imaging: stage IIIA (T3N1M0) a. CT chest/abdomen/pelvis with contrast and bone scan
Other Solid Tumors
Tissue diagnosis by biopsy
Surgical consult if appropriate
Labs: a. CMP, CBC b. Tumor markers: i) CEA – colon, rectal, lung ii) AFP – liver iii) BHCG, AFP, LDH – testicular iv) CA 125 ovarian
Imaging: a. Staging CT chest/abdomen/pelvis
b. Bone scan if appropriate (e.g., cancers of lung, kidney, prostate, melanoma, any others with bone pain symptoms)
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 21 of 50 Revised as of 9-4-14
9. Hematology/Oncology Clinic Return
Diagnosis Supporting Documents/Tests Conditions
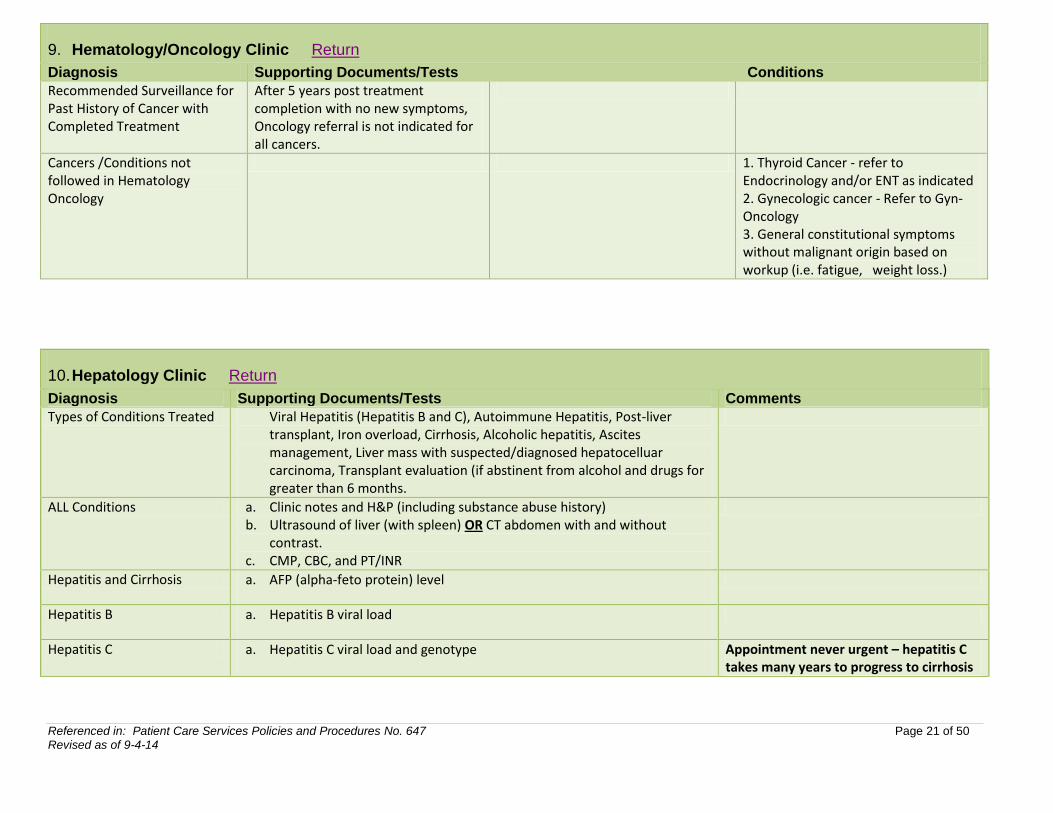
Recommended Surveillance for Past History of Cancer with Completed Treatment
After 5 years post treatment completion with no new symptoms, Oncology referral is not indicated for all cancers.
Cancers /Conditions not followed in Hematology Oncology
1. Thyroid Cancer - refer to Endocrinology and/or ENT as indicated 2. Gynecologic cancer - Refer to Gyn-Oncology 3. General constitutional symptoms without malignant origin based on workup (i.e. fatigue, weight loss.)
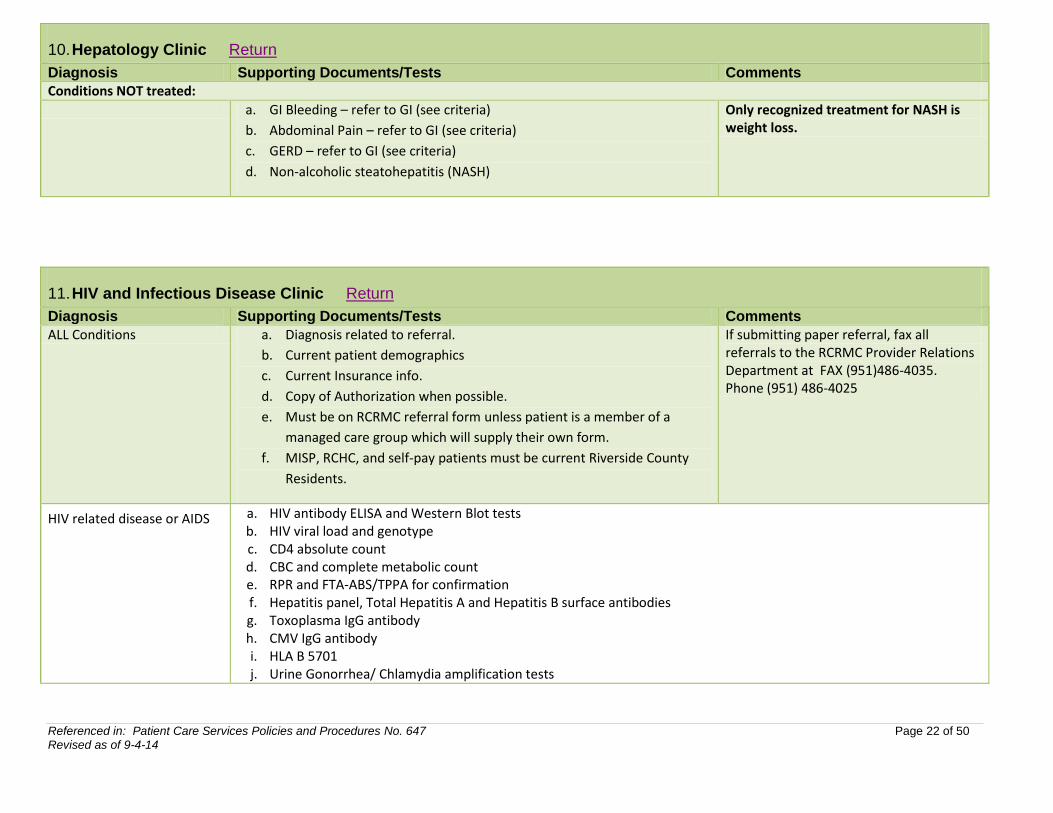
10. Hepatology Clinic Return
Diagnosis Supporting Documents/Tests Comments
Types of Conditions Treated Viral Hepatitis (Hepatitis B and C), Autoimmune Hepatitis, Post-liver transplant, Iron overload, Cirrhosis, Alcoholic hepatitis, Ascites management, Liver mass with suspected/diagnosed hepatocelluar carcinoma, Transplant evaluation (if abstinent from alcohol and drugs for greater than 6 months.
ALL Conditions a. Clinic notes and H&P (including substance abuse history) b. Ultrasound of liver (with spleen) OR CT abdomen with and without
contrast. c. CMP, CBC, and PT/INR
Hepatitis and Cirrhosis a. AFP (alpha-feto protein) level
Hepatitis B a. Hepatitis B viral load
Hepatitis C a. Hepatitis C viral load and genotype Appointment never urgent – hepatitis C takes many years to progress to cirrhosis
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 22 of 50 Revised as of 9-4-14
10. Hepatology Clinic Return
Diagnosis Supporting Documents/Tests Comments
Conditions NOT treated:
a. GI Bleeding – refer to GI (see criteria)
b. Abdominal Pain – refer to GI (see criteria)
c. GERD – refer to GI (see criteria)
d. Non-alcoholic steatohepatitis (NASH)
Only recognized treatment for NASH is weight loss.
11. HIV and Infectious Disease Clinic Return
Diagnosis Supporting Documents/Tests Comments
ALL Conditions a. Diagnosis related to referral.
b. Current patient demographics
c. Current Insurance info.
d. Copy of Authorization when possible.
e. Must be on RCRMC referral form unless patient is a member of a
managed care group which will supply their own form.
f. MISP, RCHC, and self-pay patients must be current Riverside County
Residents.
If submitting paper referral, fax all referrals to the RCRMC Provider Relations Department at FAX (951)486-4035. Phone (951) 486-4025
HIV related disease or AIDS a. HIV antibody ELISA and Western Blot tests b. HIV viral load and genotype c. CD4 absolute count d. CBC and complete metabolic count e. RPR and FTA-ABS/TPPA for confirmation f. Hepatitis panel, Total Hepatitis A and Hepatitis B surface antibodies g. Toxoplasma IgG antibody h. CMV IgG antibody i. HLA B 5701 j. Urine Gonorrhea/ Chlamydia amplification tests
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 23 of 50 Revised as of 9-4-14
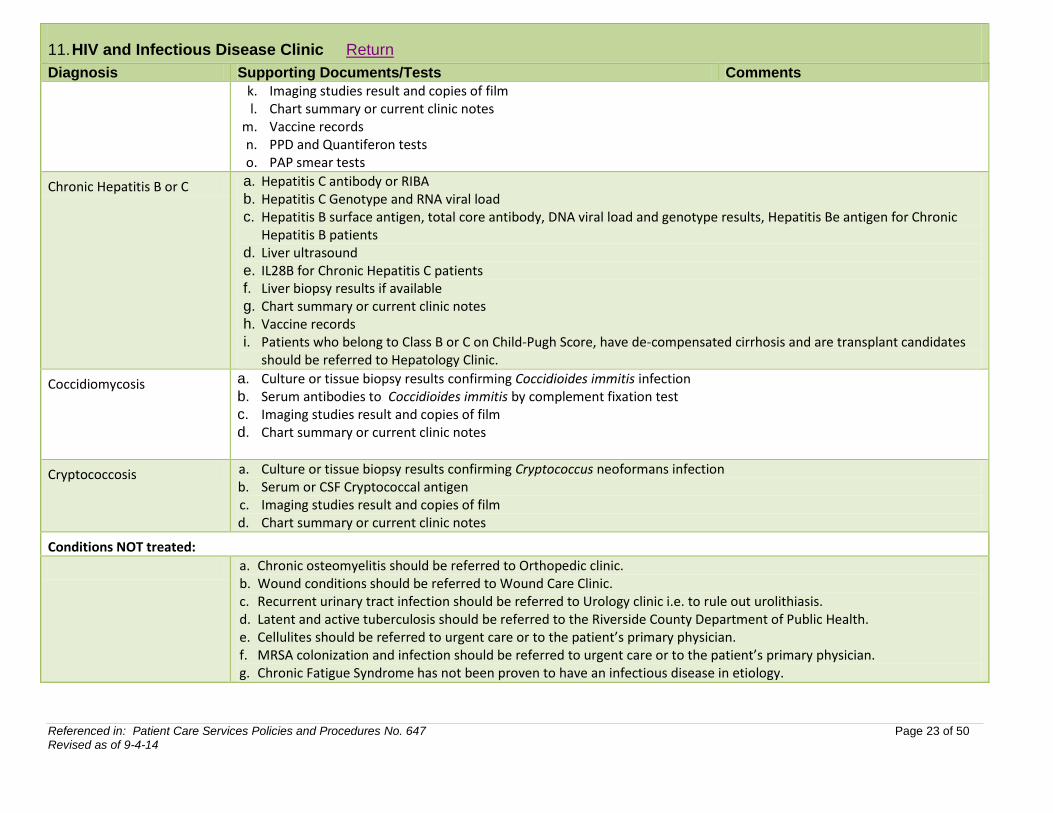
11. HIV and Infectious Disease Clinic Return
Diagnosis Supporting Documents/Tests Comments
k. Imaging studies result and copies of film l. Chart summary or current clinic notes
m. Vaccine records n. PPD and Quantiferon tests o. PAP smear tests
Chronic Hepatitis B or C a. Hepatitis C antibody or RIBA b. Hepatitis C Genotype and RNA viral load c. Hepatitis B surface antigen, total core antibody, DNA viral load and genotype results, Hepatitis Be antigen for Chronic
Hepatitis B patients d. Liver ultrasound e. IL28B for Chronic Hepatitis C patients f. Liver biopsy results if available g. Chart summary or current clinic notes h. Vaccine records i. Patients who belong to Class B or C on Child-Pugh Score, have de-compensated cirrhosis and are transplant candidates
should be referred to Hepatology Clinic.
Coccidiomycosis a. Culture or tissue biopsy results confirming Coccidioides immitis infection b. Serum antibodies to Coccidioides immitis by complement fixation test c. Imaging studies result and copies of film d. Chart summary or current clinic notes
Cryptococcosis a. Culture or tissue biopsy results confirming Cryptococcus neoformans infection b. Serum or CSF Cryptococcal antigen c. Imaging studies result and copies of film d. Chart summary or current clinic notes
Conditions NOT treated:
a. Chronic osteomyelitis should be referred to Orthopedic clinic. b. Wound conditions should be referred to Wound Care Clinic. c. Recurrent urinary tract infection should be referred to Urology clinic i.e. to rule out urolithiasis. d. Latent and active tuberculosis should be referred to the Riverside County Department of Public Health. e. Cellulites should be referred to urgent care or to the patient’s primary physician. f. MRSA colonization and infection should be referred to urgent care or to the patient’s primary physician. g. Chronic Fatigue Syndrome has not been proven to have an infectious disease in etiology.
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 24 of 50 Revised as of 9-4-14
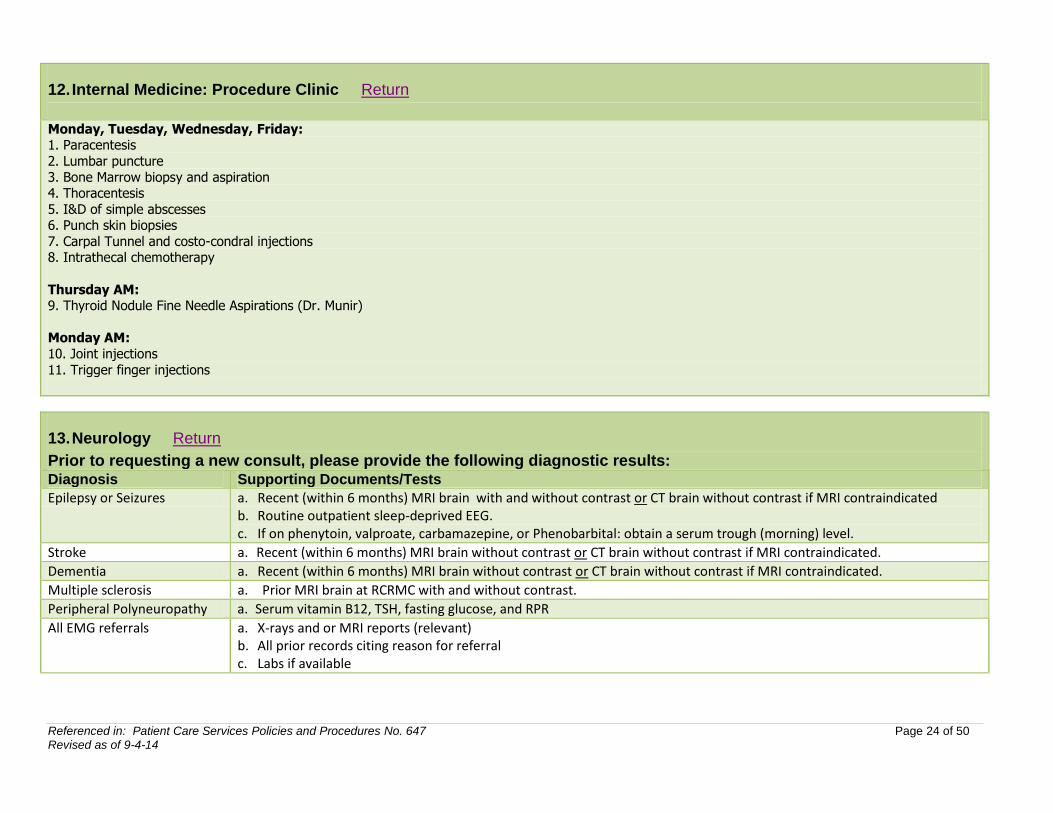
12. Internal Medicine: Procedure Clinic Return
Monday, Tuesday, Wednesday, Friday: 1. Paracentesis
2. Lumbar puncture
3. Bone Marrow biopsy and aspiration 4. Thoracentesis
5. I&D of simple abscesses 6. Punch skin biopsies
7. Carpal Tunnel and costo-condral injections 8. Intrathecal chemotherapy
Thursday AM: 9. Thyroid Nodule Fine Needle Aspirations (Dr. Munir)
Monday AM:
10. Joint injections
11. Trigger finger injections
13. Neurology Return
Prior to requesting a new consult, please provide the following diagnostic results: Diagnosis Supporting Documents/Tests
Epilepsy or Seizures a. Recent (within 6 months) MRI brain with and without contrast or CT brain without contrast if MRI contraindicated b. Routine outpatient sleep-deprived EEG. c. If on phenytoin, valproate, carbamazepine, or Phenobarbital: obtain a serum trough (morning) level.
Stroke a. Recent (within 6 months) MRI brain without contrast or CT brain without contrast if MRI contraindicated.
Dementia a. Recent (within 6 months) MRI brain without contrast or CT brain without contrast if MRI contraindicated.
Multiple sclerosis a. Prior MRI brain at RCRMC with and without contrast.
Peripheral Polyneuropathy a. Serum vitamin B12, TSH, fasting glucose, and RPR
All EMG referrals a. X-rays and or MRI reports (relevant) b. All prior records citing reason for referral c. Labs if available
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 25 of 50 Revised as of 9-4-14
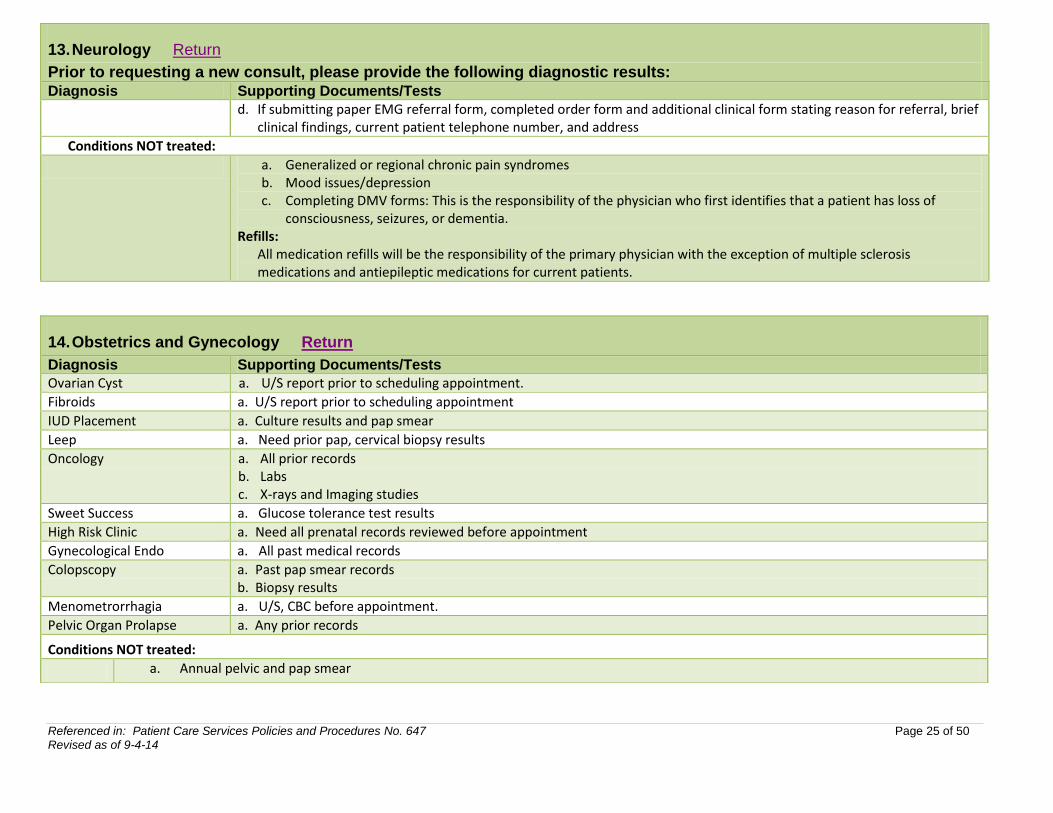
13. Neurology Return
Prior to requesting a new consult, please provide the following diagnostic results: Diagnosis Supporting Documents/Tests
d. If submitting paper EMG referral form, completed order form and additional clinical form stating reason for referral, brief clinical findings, current patient telephone number, and address
Conditions NOT treated:
a. Generalized or regional chronic pain syndromes b. Mood issues/depression c. Completing DMV forms: This is the responsibility of the physician who first identifies that a patient has loss of
consciousness, seizures, or dementia. Refills:
All medication refills will be the responsibility of the primary physician with the exception of multiple sclerosis medications and antiepileptic medications for current patients.
14. Obstetrics and Gynecology Return
Diagnosis Supporting Documents/Tests
Ovarian Cyst a. U/S report prior to scheduling appointment.
Fibroids a. U/S report prior to scheduling appointment
IUD Placement a. Culture results and pap smear
Leep a. Need prior pap, cervical biopsy results
Oncology a. All prior records b. Labs c. X-rays and Imaging studies
Sweet Success a. Glucose tolerance test results
High Risk Clinic a. Need all prenatal records reviewed before appointment
Gynecological Endo a. All past medical records
Colopscopy a. Past pap smear records b. Biopsy results
Menometrorrhagia a. U/S, CBC before appointment.
Pelvic Organ Prolapse a. Any prior records
Conditions NOT treated:
a. Annual pelvic and pap smear
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 26 of 50 Revised as of 9-4-14
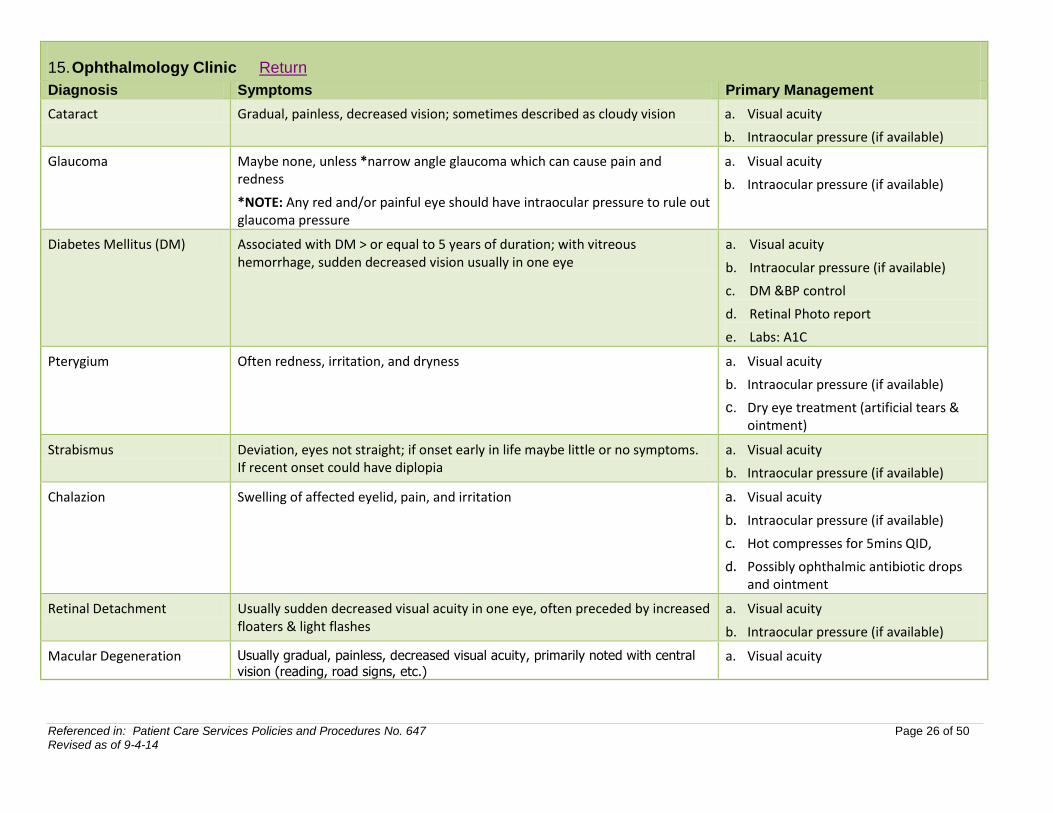
15. Ophthalmology Clinic Return
Diagnosis Symptoms Primary Management
Cataract Gradual, painless, decreased vision; sometimes described as cloudy vision a. Visual acuity
b. Intraocular pressure (if available)
Glaucoma Maybe none, unless *narrow angle glaucoma which can cause pain and redness
*NOTE: Any red and/or painful eye should have intraocular pressure to rule out glaucoma pressure
a. Visual acuity
b. Intraocular pressure (if available)
Diabetes Mellitus (DM) Associated with DM > or equal to 5 years of duration; with vitreous hemorrhage, sudden decreased vision usually in one eye
a. Visual acuity
b. Intraocular pressure (if available)
c. DM &BP control
d. Retinal Photo report
e. Labs: A1C
Pterygium Often redness, irritation, and dryness a. Visual acuity
b. Intraocular pressure (if available)
c. Dry eye treatment (artificial tears & ointment)
Strabismus Deviation, eyes not straight; if onset early in life maybe little or no symptoms. If recent onset could have diplopia
a. Visual acuity
b. Intraocular pressure (if available)
Chalazion Swelling of affected eyelid, pain, and irritation a. Visual acuity
b. Intraocular pressure (if available)
c. Hot compresses for 5mins QID,
d. Possibly ophthalmic antibiotic drops and ointment
Retinal Detachment Usually sudden decreased visual acuity in one eye, often preceded by increased floaters & light flashes
a. Visual acuity
b. Intraocular pressure (if available)
Macular Degeneration Usually gradual, painless, decreased visual acuity, primarily noted with central
vision (reading, road signs, etc.) a. Visual acuity
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 27 of 50 Revised as of 9-4-14
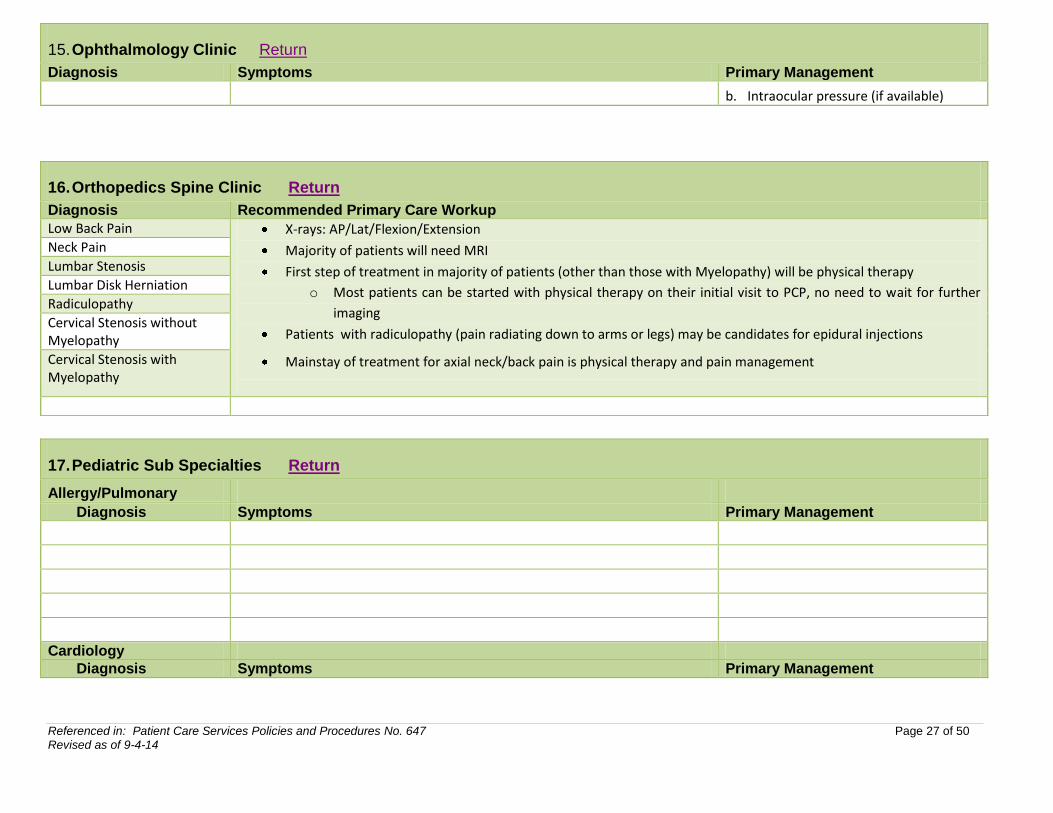
15. Ophthalmology Clinic Return
Diagnosis Symptoms Primary Management
b. Intraocular pressure (if available)
17. Pediatric Sub Specialties Return
Allergy/Pulmonary
Diagnosis Symptoms Primary Management
Cardiology
Diagnosis Symptoms Primary Management
16. Orthopedics Spine Clinic Return
Diagnosis Recommended Primary Care Workup
Low Back Pain X-rays: AP/Lat/Flexion/Extension
Majority of patients will need MRI
First step of treatment in majority of patients (other than those with Myelopathy) will be physical therapy
o Most patients can be started with physical therapy on their initial visit to PCP, no need to wait for further
imaging
Patients with radiculopathy (pain radiating down to arms or legs) may be candidates for epidural injections
Mainstay of treatment for axial neck/back pain is physical therapy and pain management
Neck Pain
Lumbar Stenosis
Lumbar Disk Herniation
Radiculopathy
Cervical Stenosis without Myelopathy
Cervical Stenosis with Myelopathy
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 28 of 50 Revised as of 9-4-14
17. Pediatric Sub Specialties Return
Dermatology
Diagnosis Symptoms Primary Management
Endocrinology
Diagnosis Symptoms Primary Management
ENT
Diagnosis Symptoms Primary Management
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 29 of 50 Revised as of 9-4-14
17. Pediatric Sub Specialties Return
Gastroenterology
Diagnosis Symptoms Primary Management
General Surgery
Diagnosis Symptoms Primary Management
Infectious Disease
Diagnosis Symptoms Primary Management
Nephrology
Diagnosis Symptoms Primary Management
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 30 of 50 Revised as of 9-4-14
17. Pediatric Sub Specialties Return
Neurology
Diagnosis Symptoms Primary Management
NICU High Risk Follow Up Clinic
Diagnosis Symptoms Primary Management
Ophthalmology – Preemie/Newborn Screens
Diagnosis Symptoms Primary Management
Orthopedics
Diagnosis Symptoms Primary Management
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 31 of 50 Revised as of 9-4-14
17. Pediatric Sub Specialties Return
Plastic Surgery
Diagnosis Symptoms Primary Management
Spine Clinic -Scoliosis
Diagnosis Symptoms Primary Management
Urology
Diagnosis Symptoms Primary Management
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 32 of 50 Revised as of 9-4-14
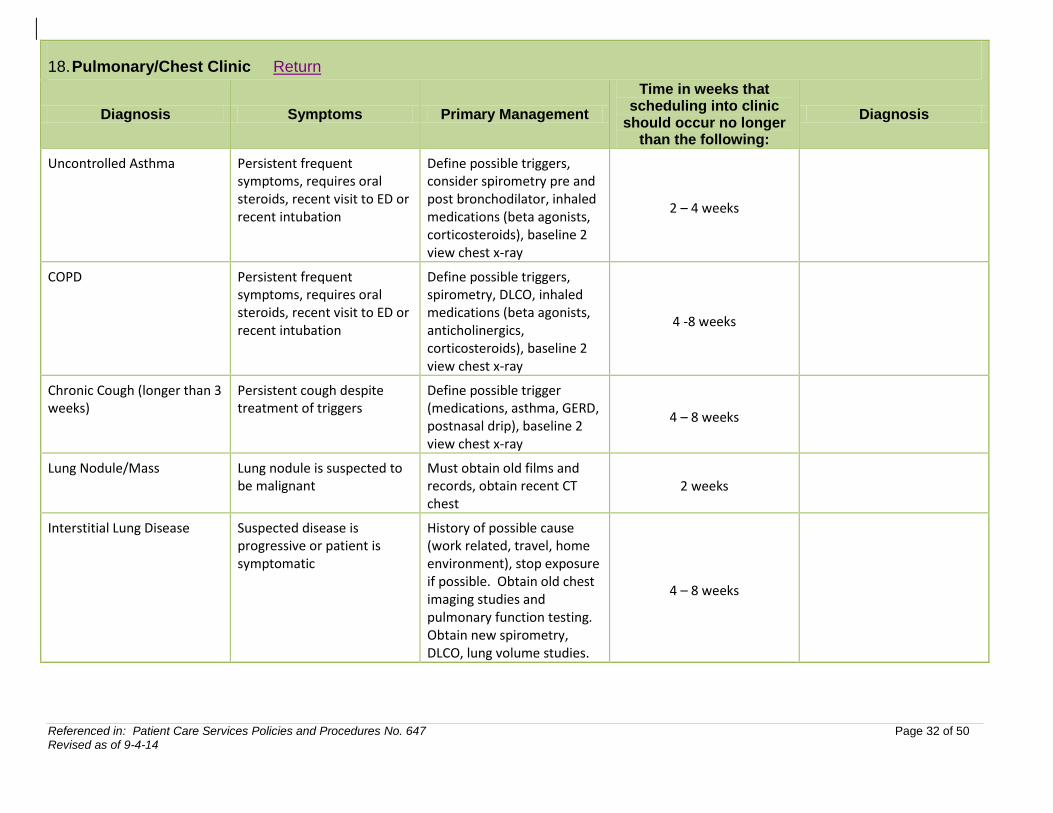
18. Pulmonary/Chest Clinic Return
Diagnosis Symptoms Primary Management
Time in weeks that scheduling into clinic
should occur no longer than the following:
Diagnosis
Uncontrolled Asthma Persistent frequent symptoms, requires oral steroids, recent visit to ED or recent intubation
Define possible triggers, consider spirometry pre and post bronchodilator, inhaled medications (beta agonists, corticosteroids), baseline 2 view chest x-ray
2 – 4 weeks
COPD Persistent frequent symptoms, requires oral steroids, recent visit to ED or recent intubation
Define possible triggers, spirometry, DLCO, inhaled medications (beta agonists, anticholinergics, corticosteroids), baseline 2 view chest x-ray
4 -8 weeks
Chronic Cough (longer than 3 weeks)
Persistent cough despite treatment of triggers
Define possible trigger (medications, asthma, GERD, postnasal drip), baseline 2 view chest x-ray
4 – 8 weeks
Lung Nodule/Mass Lung nodule is suspected to be malignant
Must obtain old films and records, obtain recent CT chest
2 weeks
Interstitial Lung Disease Suspected disease is progressive or patient is symptomatic
History of possible cause (work related, travel, home environment), stop exposure if possible. Obtain old chest imaging studies and pulmonary function testing. Obtain new spirometry, DLCO, lung volume studies.
4 – 8 weeks
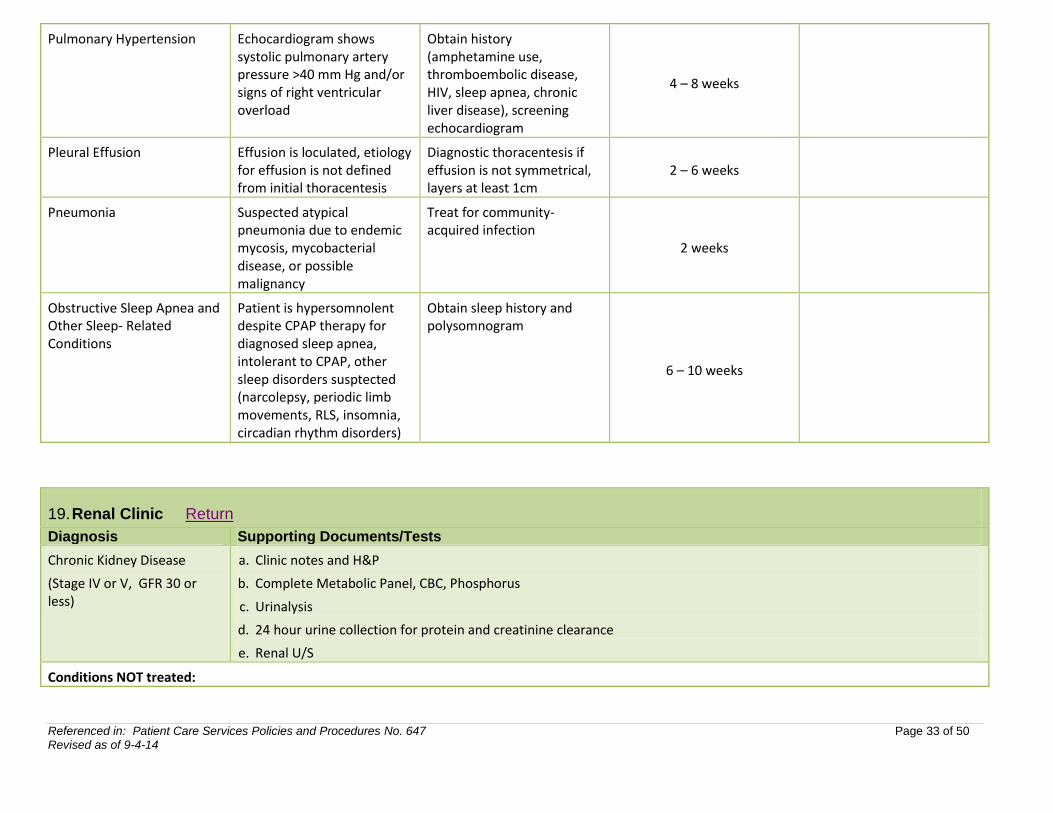
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 33 of 50 Revised as of 9-4-14
Pulmonary Hypertension Echocardiogram shows systolic pulmonary artery pressure >40 mm Hg and/or signs of right ventricular overload
Obtain history (amphetamine use, thromboembolic disease, HIV, sleep apnea, chronic liver disease), screening echocardiogram
4 – 8 weeks
Pleural Effusion Effusion is loculated, etiology for effusion is not defined from initial thoracentesis
Diagnostic thoracentesis if effusion is not symmetrical, layers at least 1cm
2 – 6 weeks
Pneumonia Suspected atypical pneumonia due to endemic mycosis, mycobacterial disease, or possible malignancy
Treat for community- acquired infection
2 weeks
Obstructive Sleep Apnea and Other Sleep- Related Conditions
Patient is hypersomnolent despite CPAP therapy for diagnosed sleep apnea, intolerant to CPAP, other sleep disorders susptected (narcolepsy, periodic limb movements, RLS, insomnia, circadian rhythm disorders)
Obtain sleep history and polysomnogram
6 – 10 weeks
19. Renal Clinic Return
Diagnosis Supporting Documents/Tests
Chronic Kidney Disease
(Stage IV or V, GFR 30 or less)
a. Clinic notes and H&P
b. Complete Metabolic Panel, CBC, Phosphorus
c. Urinalysis
d. 24 hour urine collection for protein and creatinine clearance
e. Renal U/S
Conditions NOT treated:
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 34 of 50 Revised as of 9-4-14
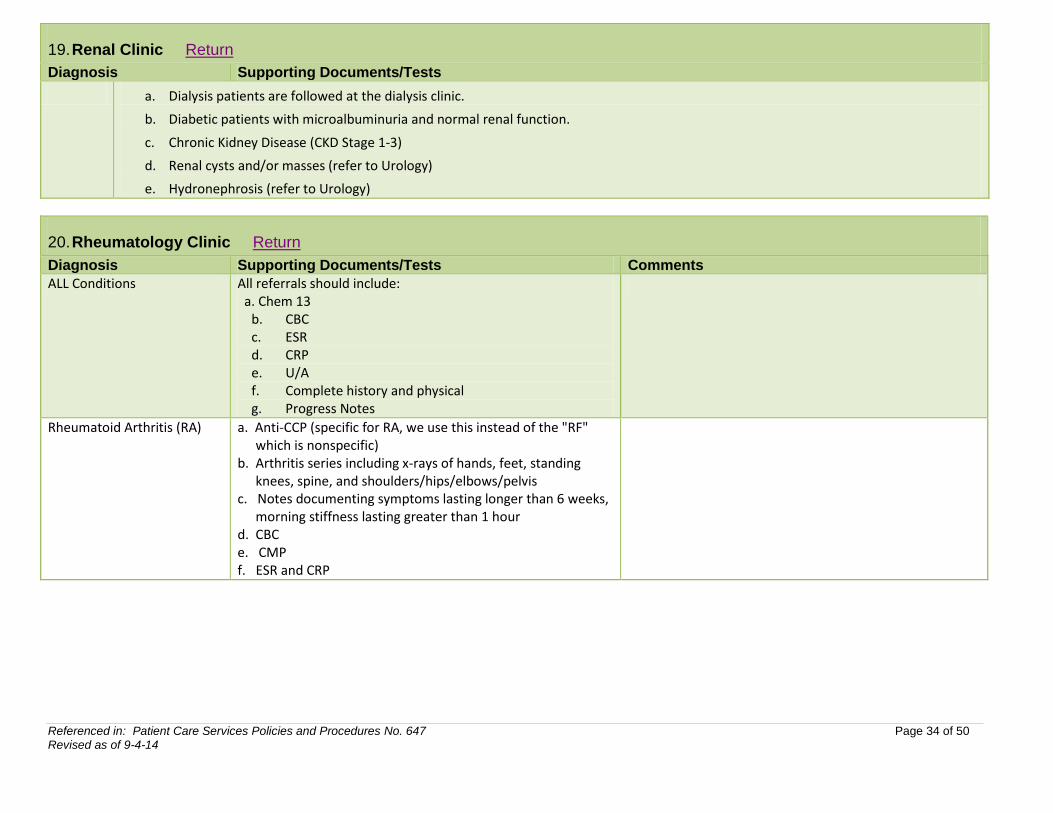
19. Renal Clinic Return
Diagnosis Supporting Documents/Tests
a. Dialysis patients are followed at the dialysis clinic.
b. Diabetic patients with microalbuminuria and normal renal function.
c. Chronic Kidney Disease (CKD Stage 1-3)
d. Renal cysts and/or masses (refer to Urology)
e. Hydronephrosis (refer to Urology)
20. Rheumatology Clinic Return
Diagnosis Supporting Documents/Tests Comments
ALL Conditions All referrals should include: a. Chem 13
b. CBC c. ESR d. CRP e. U/A f. Complete history and physical g. Progress Notes
Rheumatoid Arthritis (RA) a. Anti-CCP (specific for RA, we use this instead of the "RF" which is nonspecific)
b. Arthritis series including x-rays of hands, feet, standing knees, spine, and shoulders/hips/elbows/pelvis
c. Notes documenting symptoms lasting longer than 6 weeks, morning stiffness lasting greater than 1 hour
d. CBC e. CMP f. ESR and CRP
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 35 of 50 Revised as of 9-4-14
20. Rheumatology Clinic Return
Diagnosis Supporting Documents/Tests Comments
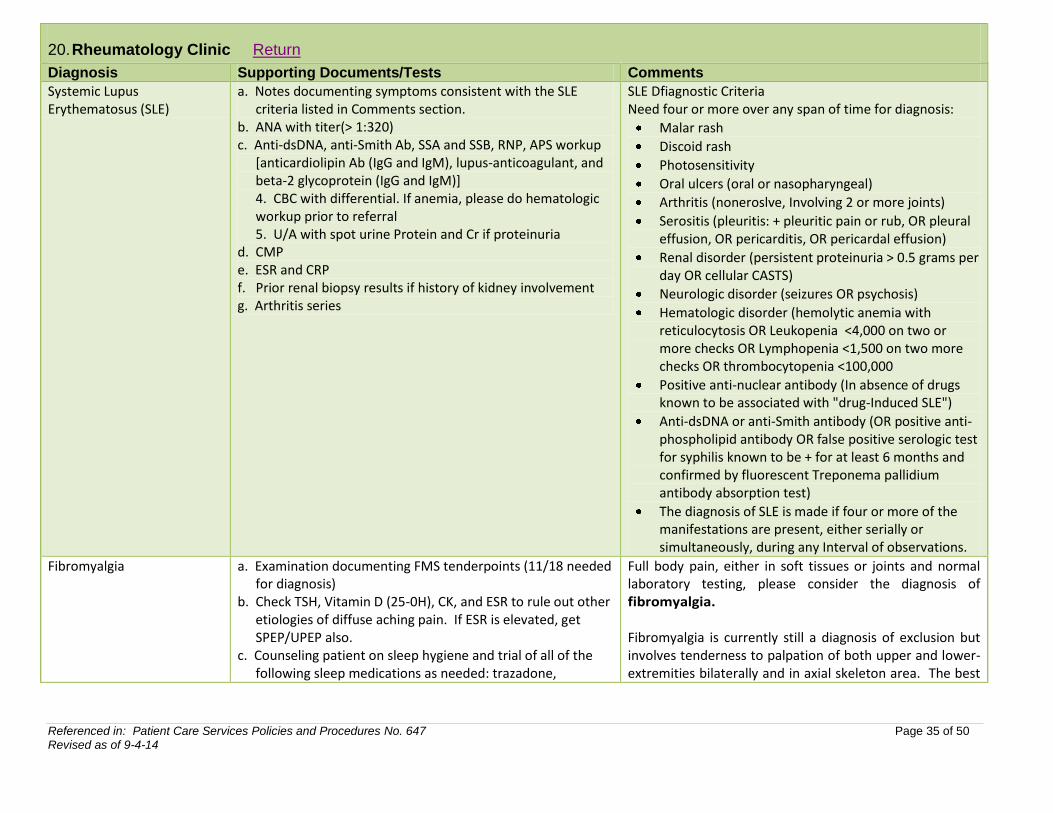
Systemic Lupus Erythematosus (SLE)
a. Notes documenting symptoms consistent with the SLE criteria listed in Comments section.
b. ANA with titer(> 1:320) c. Anti-dsDNA, anti-Smith Ab, SSA and SSB, RNP, APS workup
[anticardiolipin Ab (IgG and IgM), lupus-anticoagulant, and beta-2 glycoprotein (IgG and IgM)] 4. CBC with differential. If anemia, please do hematologic workup prior to referral 5. U/A with spot urine Protein and Cr if proteinuria
d. CMP e. ESR and CRP f. Prior renal biopsy results if history of kidney involvement g. Arthritis series
SLE Dfiagnostic Criteria Need four or more over any span of time for diagnosis:
Malar rash
Discoid rash
Photosensitivity
Oral ulcers (oral or nasopharyngeal)
Arthritis (noneroslve, Involving 2 or more joints)
Serositis (pleuritis: + pleuritic pain or rub, OR pleural effusion, OR pericarditis, OR pericardal effusion)
Renal disorder (persistent proteinuria > 0.5 grams per day OR cellular CASTS)
Neurologic disorder (seizures OR psychosis)
Hematologic disorder (hemolytic anemia with reticulocytosis OR Leukopenia <4,000 on two or more checks OR Lymphopenia <1,500 on two more checks OR thrombocytopenia <100,000
Positive anti-nuclear antibody (In absence of drugs known to be associated with "drug-Induced SLE")
Anti-dsDNA or anti-Smith antibody (OR positive anti-phospholipid antibody OR false positive serologic test for syphilis known to be + for at least 6 months and confirmed by fluorescent Treponema pallidium antibody absorption test)
The diagnosis of SLE is made if four or more of the manifestations are present, either serially or simultaneously, during any Interval of observations.
Fibromyalgia a. Examination documenting FMS tenderpoints (11/18 needed for diagnosis)
b. Check TSH, Vitamin D (25-0H), CK, and ESR to rule out other etiologies of diffuse aching pain. If ESR is elevated, get SPEP/UPEP also.
c. Counseling patient on sleep hygiene and trial of all of the following sleep medications as needed: trazadone,
Full body pain, either in soft tissues or joints and normal laboratory testing, please consider the diagnosis of fibromyalgia. Fibromyalgia is currently still a diagnosis of exclusion but involves tenderness to palpation of both upper and lower-extremities bilaterally and in axial skeleton area. The best
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 36 of 50 Revised as of 9-4-14
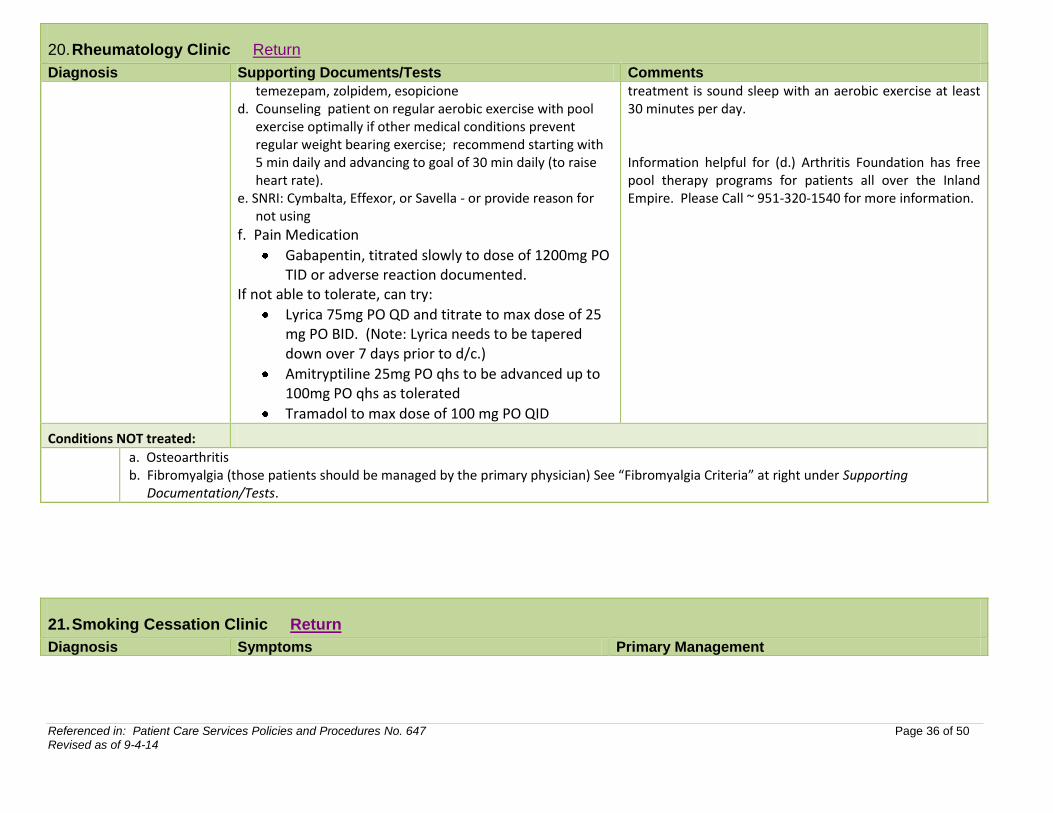
20. Rheumatology Clinic Return
Diagnosis Supporting Documents/Tests Comments
temezepam, zolpidem, esopicione d. Counseling patient on regular aerobic exercise with pool
exercise optimally if other medical conditions prevent regular weight bearing exercise; recommend starting with 5 min daily and advancing to goal of 30 min daily (to raise heart rate).
e. SNRI: Cymbalta, Effexor, or Savella - or provide reason for not using
f. Pain Medication
Gabapentin, titrated slowly to dose of 1200mg PO TID or adverse reaction documented.
If not able to tolerate, can try:
Lyrica 75mg PO QD and titrate to max dose of 25 mg PO BID. (Note: Lyrica needs to be tapered down over 7 days prior to d/c.)
Amitryptiline 25mg PO qhs to be advanced up to 100mg PO qhs as tolerated
Tramadol to max dose of 100 mg PO QID
treatment is sound sleep with an aerobic exercise at least 30 minutes per day. Information helpful for (d.) Arthritis Foundation has free pool therapy programs for patients all over the Inland Empire. Please Call ~ 951-320-1540 for more information.
Conditions NOT treated:
a. Osteoarthritis b. Fibromyalgia (those patients should be managed by the primary physician) See “Fibromyalgia Criteria” at right under Supporting
Documentation/Tests.
21. Smoking Cessation Clinic Return
Diagnosis Symptoms Primary Management
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 37 of 50 Revised as of 9-4-14
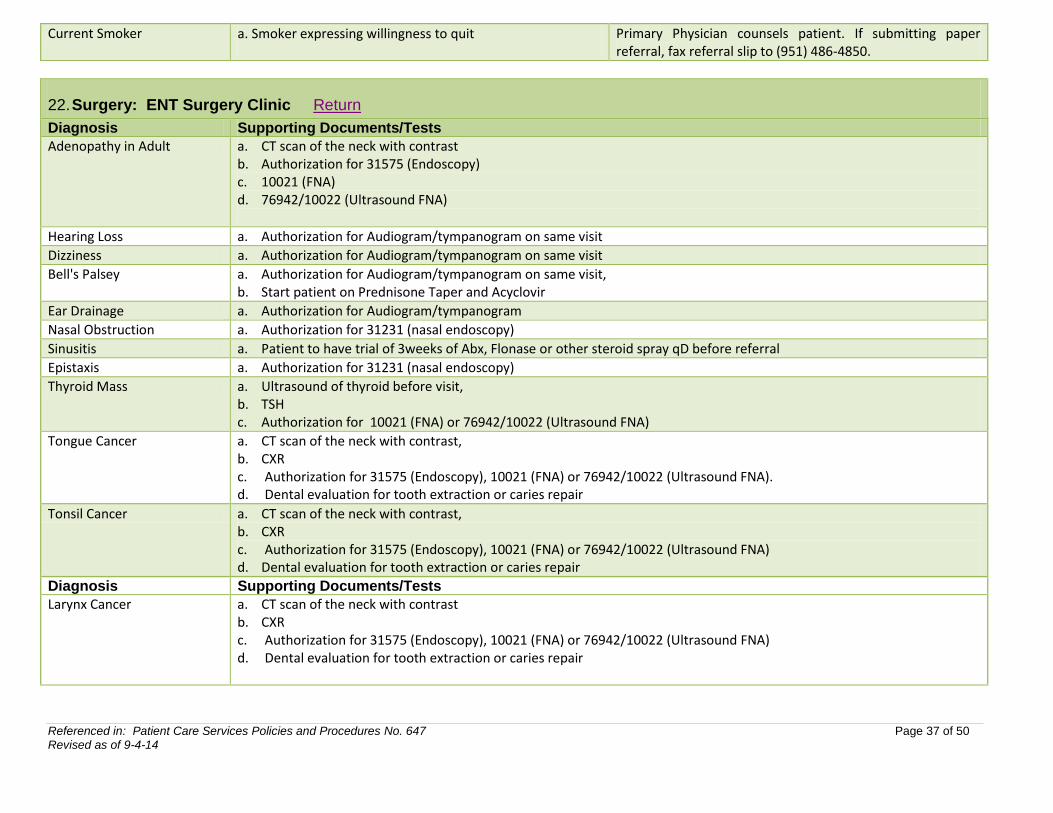
22. Surgery: ENT Surgery Clinic Return
Diagnosis Supporting Documents/Tests
Adenopathy in Adult a. CT scan of the neck with contrast b. Authorization for 31575 (Endoscopy) c. 10021 (FNA) d. 76942/10022 (Ultrasound FNA)
Hearing Loss a. Authorization for Audiogram/tympanogram on same visit
Dizziness a. Authorization for Audiogram/tympanogram on same visit
Bell's Palsey a. Authorization for Audiogram/tympanogram on same visit, b. Start patient on Prednisone Taper and Acyclovir
Ear Drainage a. Authorization for Audiogram/tympanogram
Nasal Obstruction a. Authorization for 31231 (nasal endoscopy)
Sinusitis a. Patient to have trial of 3weeks of Abx, Flonase or other steroid spray qD before referral
Epistaxis a. Authorization for 31231 (nasal endoscopy)
Thyroid Mass a. Ultrasound of thyroid before visit, b. TSH c. Authorization for 10021 (FNA) or 76942/10022 (Ultrasound FNA)
Tongue Cancer a. CT scan of the neck with contrast, b. CXR c. Authorization for 31575 (Endoscopy), 10021 (FNA) or 76942/10022 (Ultrasound FNA). d. Dental evaluation for tooth extraction or caries repair
Tonsil Cancer a. CT scan of the neck with contrast, b. CXR c. Authorization for 31575 (Endoscopy), 10021 (FNA) or 76942/10022 (Ultrasound FNA) d. Dental evaluation for tooth extraction or caries repair
Diagnosis Supporting Documents/Tests
Larynx Cancer a. CT scan of the neck with contrast b. CXR c. Authorization for 31575 (Endoscopy), 10021 (FNA) or 76942/10022 (Ultrasound FNA) d. Dental evaluation for tooth extraction or caries repair
Current Smoker a. Smoker expressing willingness to quit Primary Physician counsels patient. If submitting paper referral, fax referral slip to (951) 486-4850.
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 38 of 50 Revised as of 9-4-14
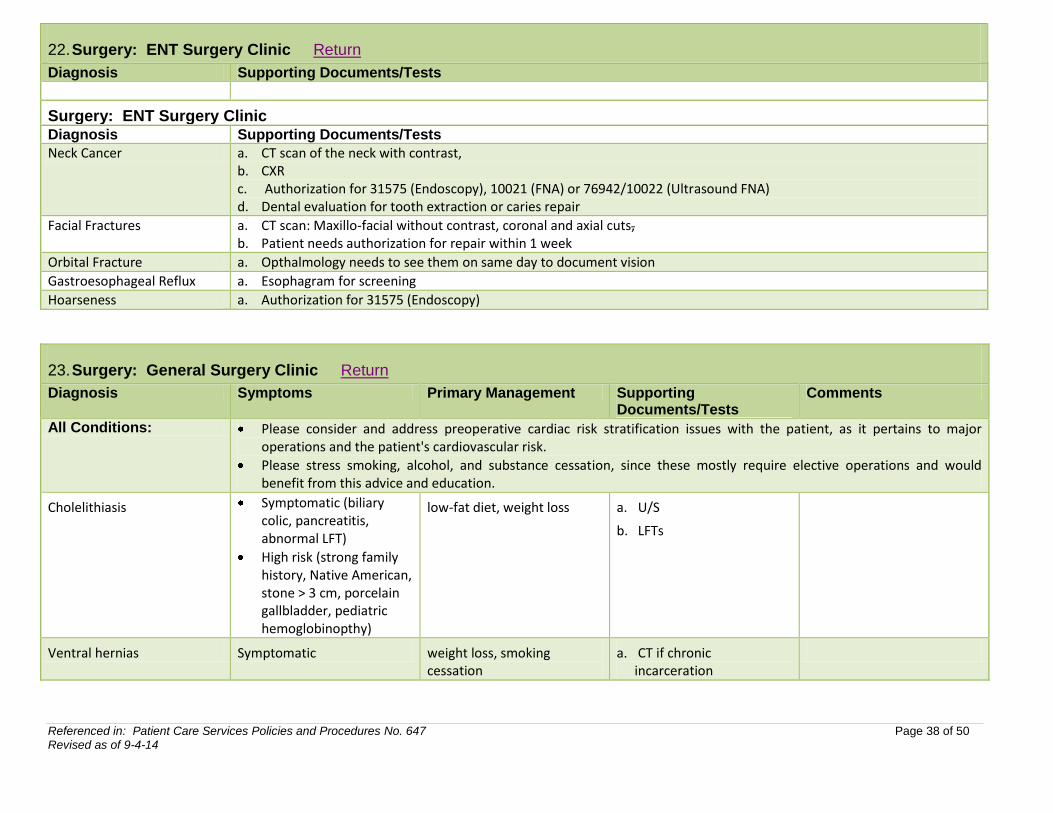
22. Surgery: ENT Surgery Clinic Return
Diagnosis Supporting Documents/Tests
Surgery: ENT Surgery Clinic
Diagnosis Supporting Documents/Tests
Neck Cancer a. CT scan of the neck with contrast, b. CXR c. Authorization for 31575 (Endoscopy), 10021 (FNA) or 76942/10022 (Ultrasound FNA) d. Dental evaluation for tooth extraction or caries repair
Facial Fractures a. CT scan: Maxillo-facial without contrast, coronal and axial cuts, b. Patient needs authorization for repair within 1 week
Orbital Fracture a. Opthalmology needs to see them on same day to document vision
Gastroesophageal Reflux a. Esophagram for screening
Hoarseness a. Authorization for 31575 (Endoscopy)
23. Surgery: General Surgery Clinic Return
Diagnosis Symptoms Primary Management Supporting Documents/Tests
Comments
All Conditions: Please consider and address preoperative cardiac risk stratification issues with the patient, as it pertains to major operations and the patient's cardiovascular risk.
Please stress smoking, alcohol, and substance cessation, since these mostly require elective operations and would benefit from this advice and education.
Cholelithiasis Symptomatic (biliary colic, pancreatitis, abnormal LFT)
High risk (strong family history, Native American, stone > 3 cm, porcelain gallbladder, pediatric hemoglobinopthy)
low-fat diet, weight loss a. U/S
b. LFTs
Ventral hernias Symptomatic weight loss, smoking cessation
a. CT if chronic incarceration
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 39 of 50 Revised as of 9-4-14
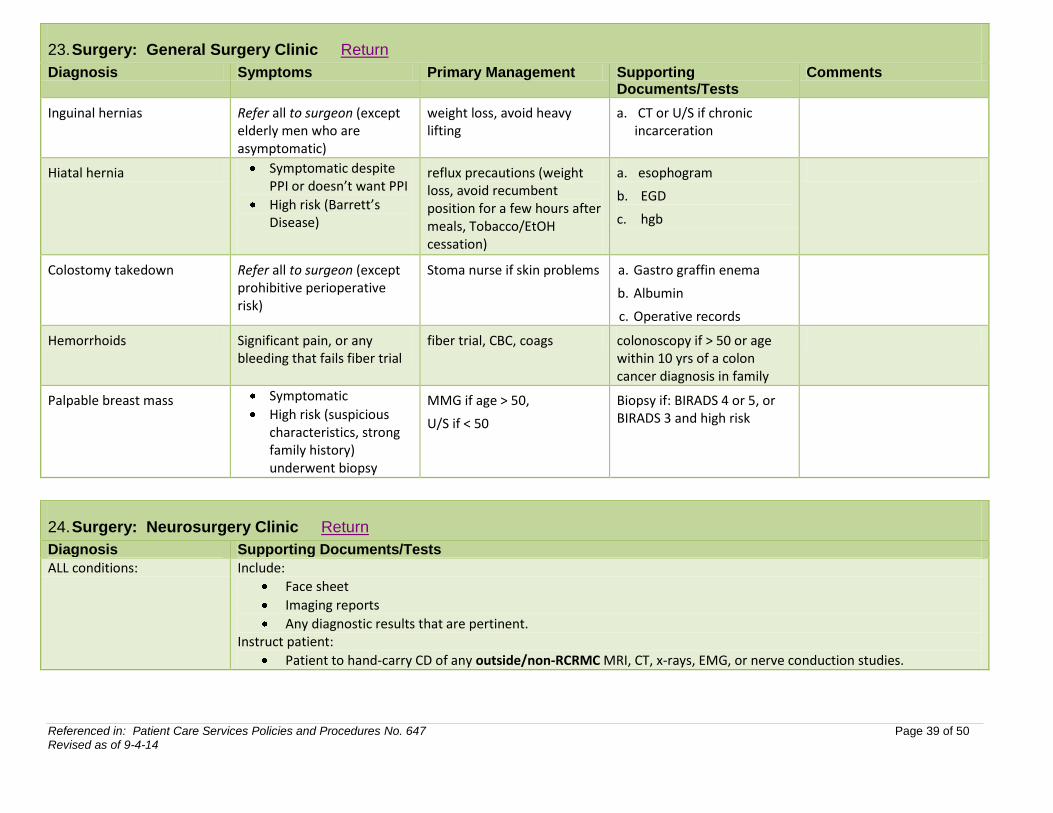
23. Surgery: General Surgery Clinic Return
Diagnosis Symptoms Primary Management Supporting Documents/Tests
Comments
Inguinal hernias Refer all to surgeon (except elderly men who are asymptomatic)
weight loss, avoid heavy lifting
a. CT or U/S if chronic incarceration
Hiatal hernia Symptomatic despite PPI or doesn’t want PPI
High risk (Barrett’s Disease)
reflux precautions (weight loss, avoid recumbent position for a few hours after meals, Tobacco/EtOH cessation)
a. esophogram
b. EGD
c. hgb
Colostomy takedown Refer all to surgeon (except prohibitive perioperative risk)
Stoma nurse if skin problems a. Gastro graffin enema
b. Albumin
c. Operative records
Hemorrhoids Significant pain, or any bleeding that fails fiber trial
fiber trial, CBC, coags colonoscopy if > 50 or age within 10 yrs of a colon cancer diagnosis in family
Palpable breast mass Symptomatic
High risk (suspicious characteristics, strong family history) underwent biopsy
MMG if age > 50,
U/S if < 50
Biopsy if: BIRADS 4 or 5, or BIRADS 3 and high risk
24. Surgery: Neurosurgery Clinic Return
Diagnosis Supporting Documents/Tests
ALL conditions: Include:
Face sheet
Imaging reports
Any diagnostic results that are pertinent. Instruct patient:
Patient to hand-carry CD of any outside/non-RCRMC MRI, CT, x-rays, EMG, or nerve conduction studies.
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 40 of 50 Revised as of 9-4-14
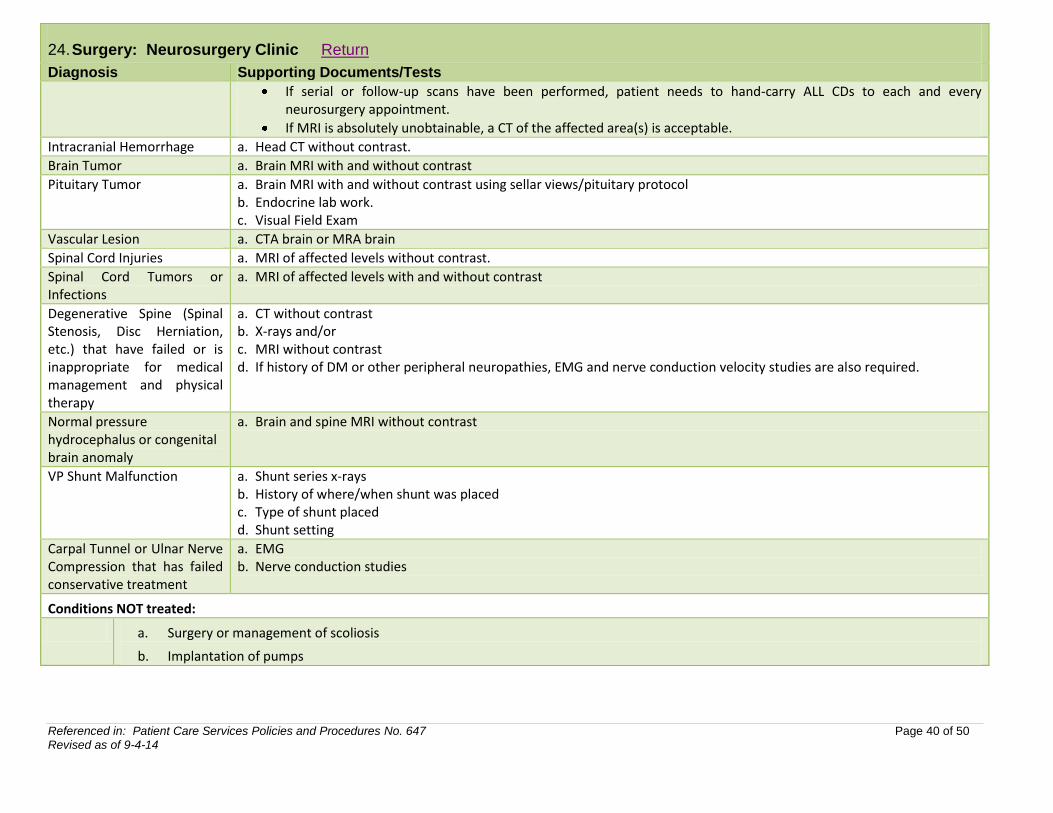
24. Surgery: Neurosurgery Clinic Return
Diagnosis Supporting Documents/Tests
If serial or follow-up scans have been performed, patient needs to hand-carry ALL CDs to each and every neurosurgery appointment.
If MRI is absolutely unobtainable, a CT of the affected area(s) is acceptable.
Intracranial Hemorrhage a. Head CT without contrast.
Brain Tumor a. Brain MRI with and without contrast
Pituitary Tumor a. Brain MRI with and without contrast using sellar views/pituitary protocol b. Endocrine lab work. c. Visual Field Exam
Vascular Lesion a. CTA brain or MRA brain
Spinal Cord Injuries a. MRI of affected levels without contrast.
Spinal Cord Tumors or Infections
a. MRI of affected levels with and without contrast
Degenerative Spine (Spinal Stenosis, Disc Herniation, etc.) that have failed or is inappropriate for medical management and physical therapy
a. CT without contrast b. X-rays and/or c. MRI without contrast d. If history of DM or other peripheral neuropathies, EMG and nerve conduction velocity studies are also required.
Normal pressure hydrocephalus or congenital brain anomaly
a. Brain and spine MRI without contrast
VP Shunt Malfunction a. Shunt series x-rays b. History of where/when shunt was placed c. Type of shunt placed d. Shunt setting
Carpal Tunnel or Ulnar Nerve Compression that has failed conservative treatment
a. EMG b. Nerve conduction studies
Conditions NOT treated:
a. Surgery or management of scoliosis
b. Implantation of pumps
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 41 of 50 Revised as of 9-4-14
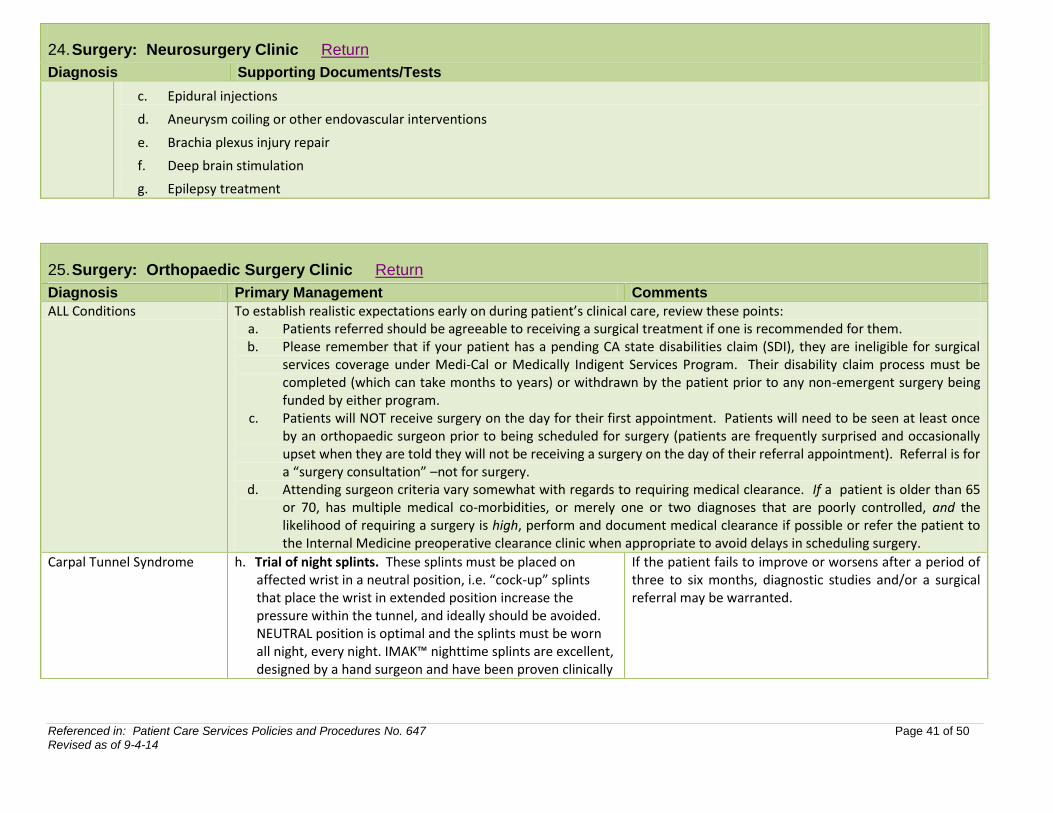
24. Surgery: Neurosurgery Clinic Return
Diagnosis Supporting Documents/Tests
c. Epidural injections
d. Aneurysm coiling or other endovascular interventions
e. Brachia plexus injury repair
f. Deep brain stimulation
g. Epilepsy treatment
25. Surgery: Orthopaedic Surgery Clinic Return
Diagnosis Primary Management Comments
ALL Conditions To establish realistic expectations early on during patient’s clinical care, review these points: a. Patients referred should be agreeable to receiving a surgical treatment if one is recommended for them. b. Please remember that if your patient has a pending CA state disabilities claim (SDI), they are ineligible for surgical
services coverage under Medi-Cal or Medically Indigent Services Program. Their disability claim process must be completed (which can take months to years) or withdrawn by the patient prior to any non-emergent surgery being funded by either program.
c. Patients will NOT receive surgery on the day for their first appointment. Patients will need to be seen at least once by an orthopaedic surgeon prior to being scheduled for surgery (patients are frequently surprised and occasionally upset when they are told they will not be receiving a surgery on the day of their referral appointment). Referral is for a “surgery consultation” –not for surgery.
d. Attending surgeon criteria vary somewhat with regards to requiring medical clearance. If a patient is older than 65 or 70, has multiple medical co-morbidities, or merely one or two diagnoses that are poorly controlled, and the likelihood of requiring a surgery is high, perform and document medical clearance if possible or refer the patient to the Internal Medicine preoperative clearance clinic when appropriate to avoid delays in scheduling surgery.
Carpal Tunnel Syndrome h. Trial of night splints. These splints must be placed on affected wrist in a neutral position, i.e. “cock-up” splints that place the wrist in extended position increase the pressure within the tunnel, and ideally should be avoided. NEUTRAL position is optimal and the splints must be worn all night, every night. IMAK™ nighttime splints are excellent, designed by a hand surgeon and have been proven clinically
If the patient fails to improve or worsens after a period of three to six months, diagnostic studies and/or a surgical referral may be warranted.
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 42 of 50 Revised as of 9-4-14
25. Surgery: Orthopaedic Surgery Clinic Return
Diagnosis Primary Management Comments
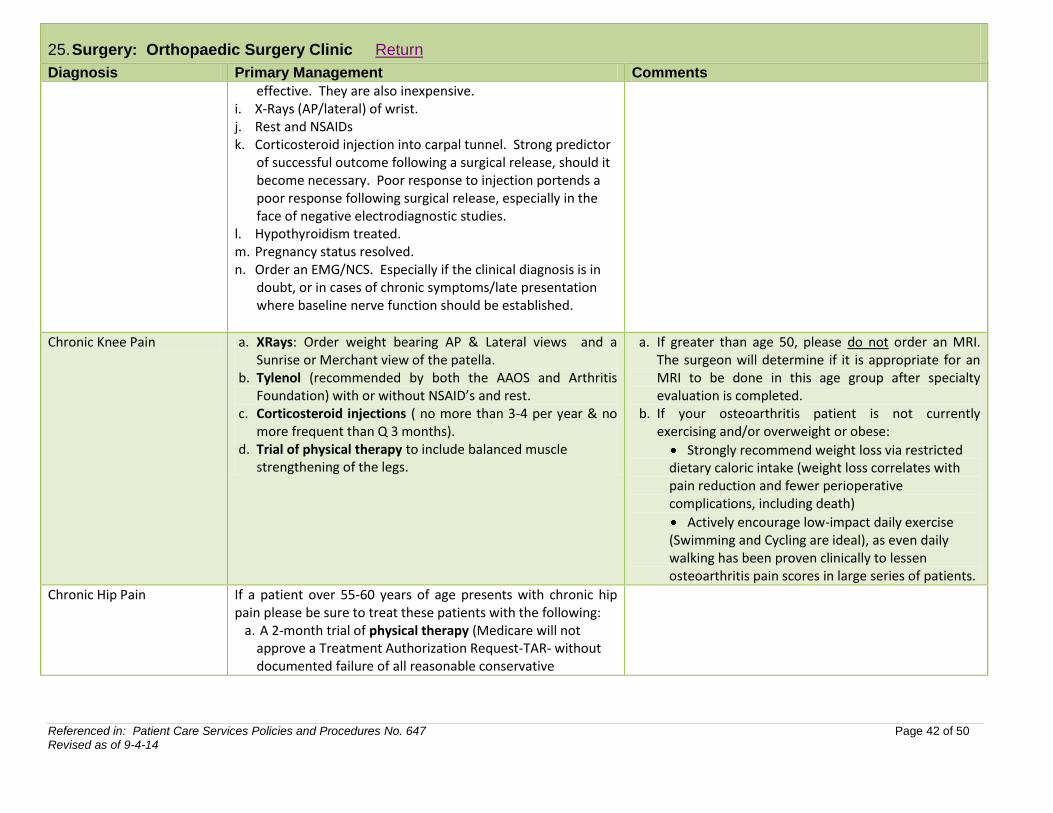
effective. They are also inexpensive. i. X-Rays (AP/lateral) of wrist. j. Rest and NSAIDs k. Corticosteroid injection into carpal tunnel. Strong predictor
of successful outcome following a surgical release, should it become necessary. Poor response to injection portends a poor response following surgical release, especially in the face of negative electrodiagnostic studies.
l. Hypothyroidism treated. m. Pregnancy status resolved. n. Order an EMG/NCS. Especially if the clinical diagnosis is in
doubt, or in cases of chronic symptoms/late presentation where baseline nerve function should be established.
Chronic Knee Pain a. XRays: Order weight bearing AP & Lateral views and a Sunrise or Merchant view of the patella.
b. Tylenol (recommended by both the AAOS and Arthritis Foundation) with or without NSAID’s and rest.
c. Corticosteroid injections ( no more than 3-4 per year & no more frequent than Q 3 months).
d. Trial of physical therapy to include balanced muscle strengthening of the legs.
a. If greater than age 50, please do not order an MRI. The surgeon will determine if it is appropriate for an MRI to be done in this age group after specialty evaluation is completed.
b. If your osteoarthritis patient is not currently exercising and/or overweight or obese:
Strongly recommend weight loss via restricted dietary caloric intake (weight loss correlates with pain reduction and fewer perioperative complications, including death)
Actively encourage low-impact daily exercise (Swimming and Cycling are ideal), as even daily walking has been proven clinically to lessen osteoarthritis pain scores in large series of patients.
Chronic Hip Pain If a patient over 55-60 years of age presents with chronic hip pain please be sure to treat these patients with the following:
a. A 2-month trial of physical therapy (Medicare will not approve a Treatment Authorization Request-TAR- without documented failure of all reasonable conservative
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 43 of 50 Revised as of 9-4-14
25. Surgery: Orthopaedic Surgery Clinic Return
Diagnosis Primary Management Comments
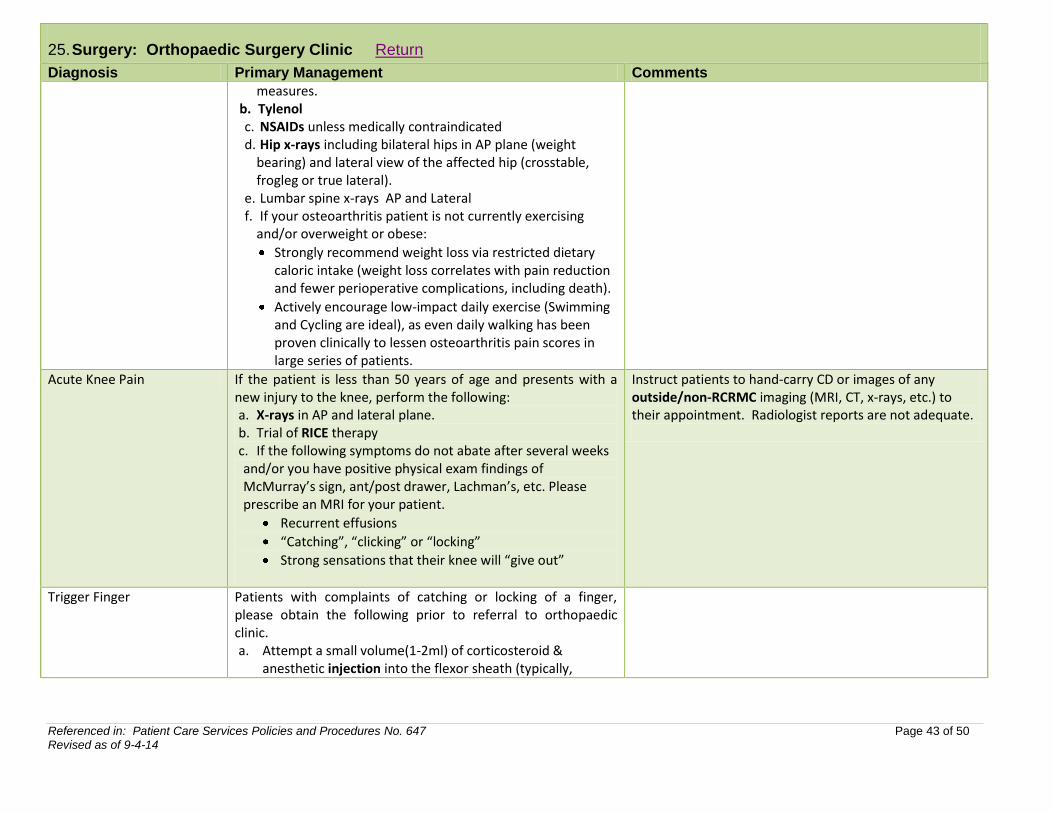
measures. b. Tylenol c. NSAIDs unless medically contraindicated d. Hip x-rays including bilateral hips in AP plane (weight
bearing) and lateral view of the affected hip (crosstable, frogleg or true lateral).
e. Lumbar spine x-rays AP and Lateral f. If your osteoarthritis patient is not currently exercising
and/or overweight or obese:
Strongly recommend weight loss via restricted dietary caloric intake (weight loss correlates with pain reduction and fewer perioperative complications, including death).
Actively encourage low-impact daily exercise (Swimming and Cycling are ideal), as even daily walking has been proven clinically to lessen osteoarthritis pain scores in large series of patients.
Acute Knee Pain If the patient is less than 50 years of age and presents with a new injury to the knee, perform the following: a. X-rays in AP and lateral plane. b. Trial of RICE therapy c. If the following symptoms do not abate after several weeks and/or you have positive physical exam findings of McMurray’s sign, ant/post drawer, Lachman’s, etc. Please prescribe an MRI for your patient.
Recurrent effusions
“Catching”, “clicking” or “locking”
Strong sensations that their knee will “give out”
Instruct patients to hand-carry CD or images of any outside/non-RCRMC imaging (MRI, CT, x-rays, etc.) to their appointment. Radiologist reports are not adequate.
Trigger Finger Patients with complaints of catching or locking of a finger, please obtain the following prior to referral to orthopaedic clinic. a. Attempt a small volume(1-2ml) of corticosteroid &
anesthetic injection into the flexor sheath (typically,
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 44 of 50 Revised as of 9-4-14
25. Surgery: Orthopaedic Surgery Clinic Return
Diagnosis Primary Management Comments
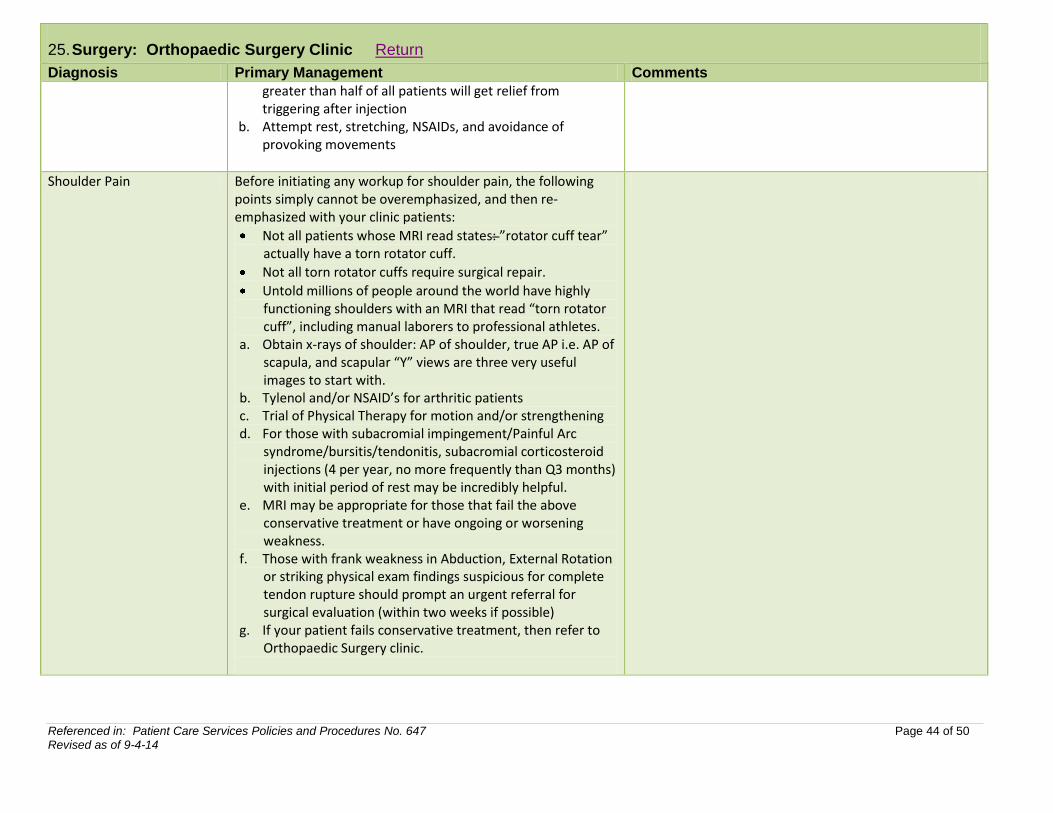
greater than half of all patients will get relief from triggering after injection
b. Attempt rest, stretching, NSAIDs, and avoidance of provoking movements
Shoulder Pain Before initiating any workup for shoulder pain, the following points simply cannot be overemphasized, and then re-emphasized with your clinic patients:
Not all patients whose MRI read states: ”rotator cuff tear” actually have a torn rotator cuff.
Not all torn rotator cuffs require surgical repair.
Untold millions of people around the world have highly functioning shoulders with an MRI that read “torn rotator cuff”, including manual laborers to professional athletes.
a. Obtain x-rays of shoulder: AP of shoulder, true AP i.e. AP of scapula, and scapular “Y” views are three very useful images to start with.
b. Tylenol and/or NSAID’s for arthritic patients c. Trial of Physical Therapy for motion and/or strengthening d. For those with subacromial impingement/Painful Arc
syndrome/bursitis/tendonitis, subacromial corticosteroid injections (4 per year, no more frequently than Q3 months) with initial period of rest may be incredibly helpful.
e. MRI may be appropriate for those that fail the above conservative treatment or have ongoing or worsening weakness.
f. Those with frank weakness in Abduction, External Rotation or striking physical exam findings suspicious for complete tendon rupture should prompt an urgent referral for surgical evaluation (within two weeks if possible)
g. If your patient fails conservative treatment, then refer to Orthopaedic Surgery clinic.
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 45 of 50 Revised as of 9-4-14
25. Surgery: Orthopaedic Surgery Clinic Return
Diagnosis Primary Management Comments
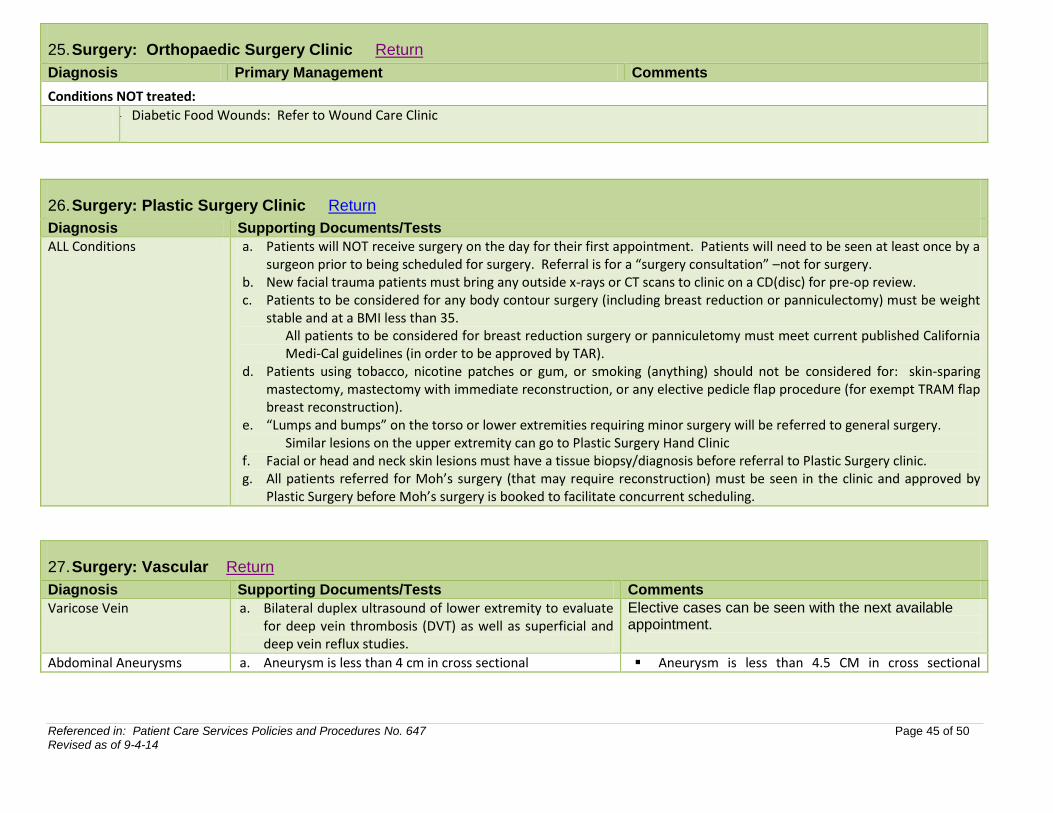
Conditions NOT treated:
a. Diabetic Food Wounds: Refer to Wound Care Clinic
26. Surgery: Plastic Surgery Clinic Return
Diagnosis Supporting Documents/Tests
ALL Conditions a. Patients will NOT receive surgery on the day for their first appointment. Patients will need to be seen at least once by a surgeon prior to being scheduled for surgery. Referral is for a “surgery consultation” –not for surgery.
b. New facial trauma patients must bring any outside x-rays or CT scans to clinic on a CD(disc) for pre-op review. c. Patients to be considered for any body contour surgery (including breast reduction or panniculectomy) must be weight
stable and at a BMI less than 35. All patients to be considered for breast reduction surgery or panniculetomy must meet current published California Medi-Cal guidelines (in order to be approved by TAR).
d. Patients using tobacco, nicotine patches or gum, or smoking (anything) should not be considered for: skin-sparing mastectomy, mastectomy with immediate reconstruction, or any elective pedicle flap procedure (for exempt TRAM flap breast reconstruction).
e. “Lumps and bumps” on the torso or lower extremities requiring minor surgery will be referred to general surgery. Similar lesions on the upper extremity can go to Plastic Surgery Hand Clinic
f. Facial or head and neck skin lesions must have a tissue biopsy/diagnosis before referral to Plastic Surgery clinic. g. All patients referred for Moh’s surgery (that may require reconstruction) must be seen in the clinic and approved by
Plastic Surgery before Moh’s surgery is booked to facilitate concurrent scheduling.
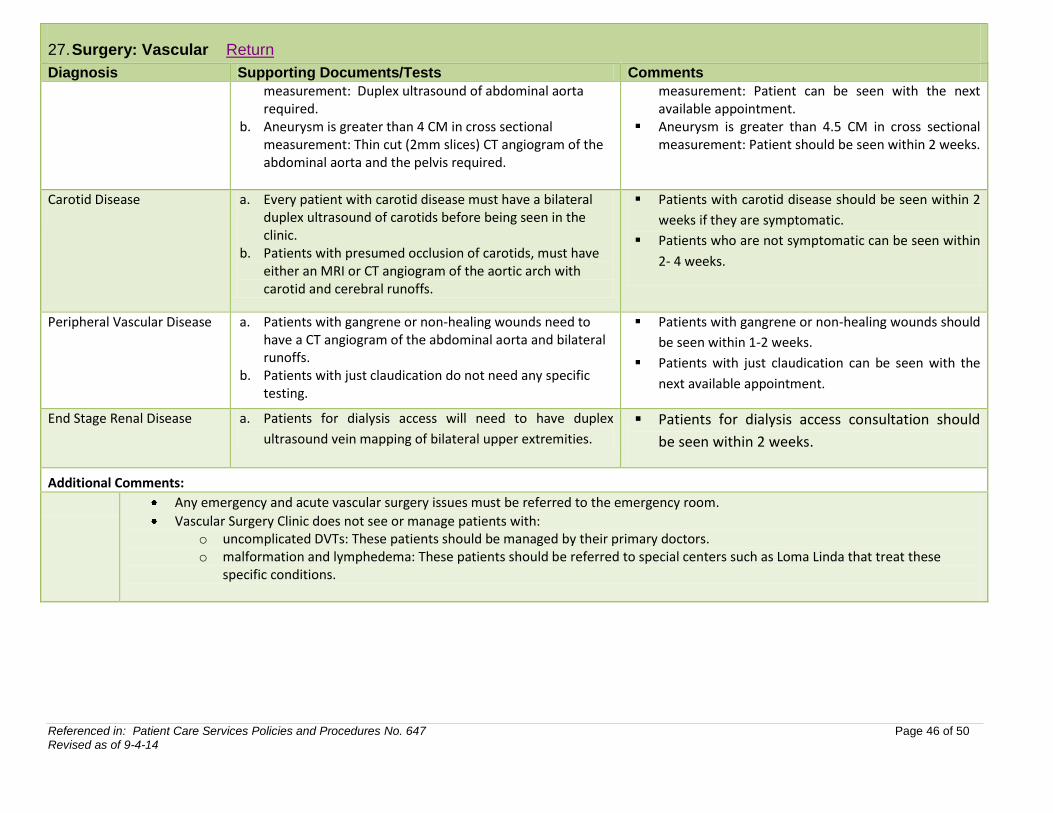
27. Surgery: Vascular Return
Diagnosis Supporting Documents/Tests Comments
Varicose Vein a. Bilateral duplex ultrasound of lower extremity to evaluate for deep vein thrombosis (DVT) as well as superficial and deep vein reflux studies.
Elective cases can be seen with the next available appointment.
Abdominal Aneurysms a. Aneurysm is less than 4 cm in cross sectional Aneurysm is less than 4.5 CM in cross sectional
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 46 of 50 Revised as of 9-4-14
27. Surgery: Vascular Return
Diagnosis Supporting Documents/Tests Comments
measurement: Duplex ultrasound of abdominal aorta required.
b. Aneurysm is greater than 4 CM in cross sectional measurement: Thin cut (2mm slices) CT angiogram of the abdominal aorta and the pelvis required.
measurement: Patient can be seen with the next available appointment.
Aneurysm is greater than 4.5 CM in cross sectional measurement: Patient should be seen within 2 weeks.
Carotid Disease
a. Every patient with carotid disease must have a bilateral duplex ultrasound of carotids before being seen in the clinic.
b. Patients with presumed occlusion of carotids, must have either an MRI or CT angiogram of the aortic arch with carotid and cerebral runoffs.
Patients with carotid disease should be seen within 2
weeks if they are symptomatic.
Patients who are not symptomatic can be seen within
2- 4 weeks.
Peripheral Vascular Disease
a. Patients with gangrene or non-healing wounds need to have a CT angiogram of the abdominal aorta and bilateral runoffs.
b. Patients with just claudication do not need any specific testing.
Patients with gangrene or non-healing wounds should
be seen within 1-2 weeks.
Patients with just claudication can be seen with the
next available appointment.
End Stage Renal Disease
a. Patients for dialysis access will need to have duplex
ultrasound vein mapping of bilateral upper extremities.
Patients for dialysis access consultation should
be seen within 2 weeks.
Additional Comments:
Any emergency and acute vascular surgery issues must be referred to the emergency room.
Vascular Surgery Clinic does not see or manage patients with: o uncomplicated DVTs: These patients should be managed by their primary doctors. o malformation and lymphedema: These patients should be referred to special centers such as Loma Linda that treat these
specific conditions.
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 47 of 50 Revised as of 9-4-14
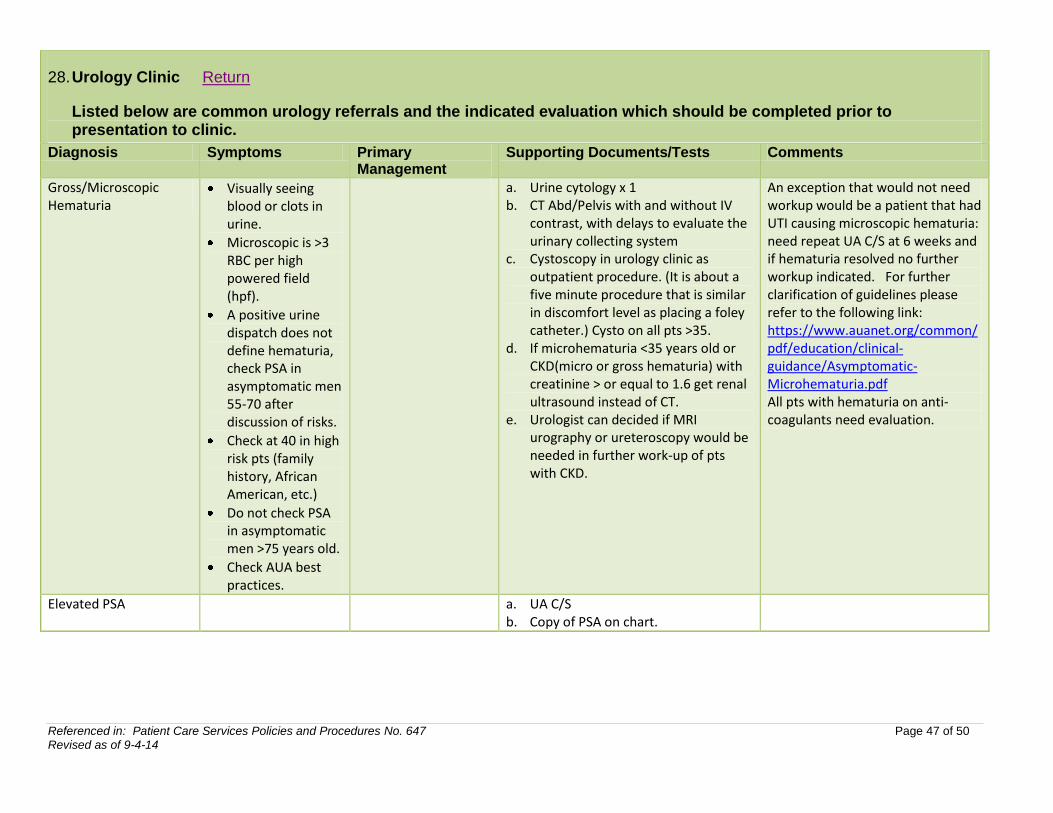
28. Urology Clinic Return
Listed below are common urology referrals and the indicated evaluation which should be completed prior to presentation to clinic.
Diagnosis Symptoms Primary Management
Supporting Documents/Tests Comments
Gross/Microscopic Hematuria
Visually seeing blood or clots in urine.
Microscopic is >3 RBC per high powered field (hpf).
A positive urine dispatch does not define hematuria, check PSA in asymptomatic men 55-70 after discussion of risks.
Check at 40 in high risk pts (family history, African American, etc.)
Do not check PSA in asymptomatic men >75 years old.
Check AUA best practices.
a. Urine cytology x 1 b. CT Abd/Pelvis with and without IV
contrast, with delays to evaluate the urinary collecting system
c. Cystoscopy in urology clinic as outpatient procedure. (It is about a five minute procedure that is similar in discomfort level as placing a foley catheter.) Cysto on all pts >35.
d. If microhematuria <35 years old or CKD(micro or gross hematuria) with creatinine > or equal to 1.6 get renal ultrasound instead of CT.
e. Urologist can decided if MRI urography or ureteroscopy would be needed in further work-up of pts with CKD.
An exception that would not need workup would be a patient that had UTI causing microscopic hematuria: need repeat UA C/S at 6 weeks and if hematuria resolved no further workup indicated. For further clarification of guidelines please refer to the following link: https://www.auanet.org/common/pdf/education/clinical-guidance/Asymptomatic-Microhematuria.pdf All pts with hematuria on anti-coagulants need evaluation.
Elevated PSA a. UA C/S b. Copy of PSA on chart.
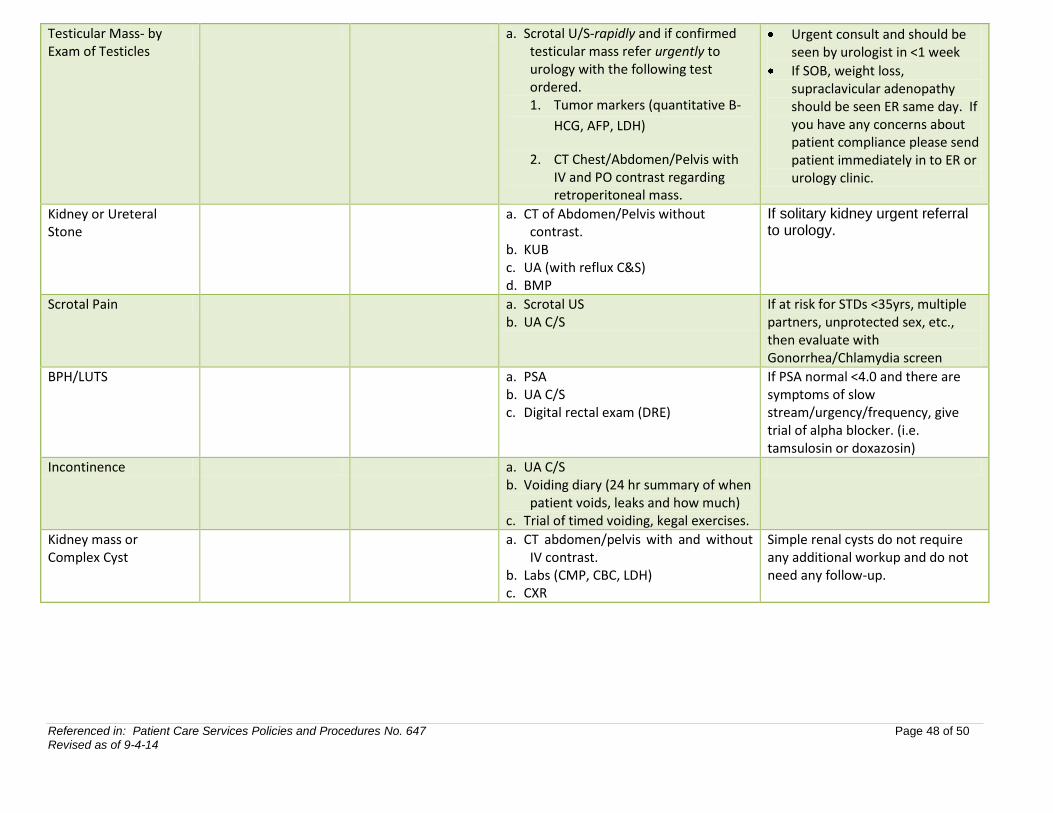
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 48 of 50 Revised as of 9-4-14
Testicular Mass- by Exam of Testicles
a. Scrotal U/S-rapidly and if confirmed testicular mass refer urgently to urology with the following test ordered. 1. Tumor markers (quantitative B-
HCG, AFP, LDH)
2. CT Chest/Abdomen/Pelvis with IV and PO contrast regarding retroperitoneal mass.
Urgent consult and should be seen by urologist in <1 week
If SOB, weight loss, supraclavicular adenopathy should be seen ER same day. If you have any concerns about patient compliance please send patient immediately in to ER or urology clinic.
Kidney or Ureteral Stone
a. CT of Abdomen/Pelvis without contrast.
b. KUB c. UA (with reflux C&S) d. BMP
If solitary kidney urgent referral to urology.
Scrotal Pain a. Scrotal US b. UA C/S
If at risk for STDs <35yrs, multiple partners, unprotected sex, etc., then evaluate with Gonorrhea/Chlamydia screen
BPH/LUTS a. PSA b. UA C/S c. Digital rectal exam (DRE)
If PSA normal <4.0 and there are symptoms of slow stream/urgency/frequency, give trial of alpha blocker. (i.e. tamsulosin or doxazosin)
Incontinence a. UA C/S b. Voiding diary (24 hr summary of when
patient voids, leaks and how much) c. Trial of timed voiding, kegal exercises.
Kidney mass or Complex Cyst
a. CT abdomen/pelvis with and without IV contrast.
b. Labs (CMP, CBC, LDH) c. CXR
Simple renal cysts do not require any additional workup and do not need any follow-up.
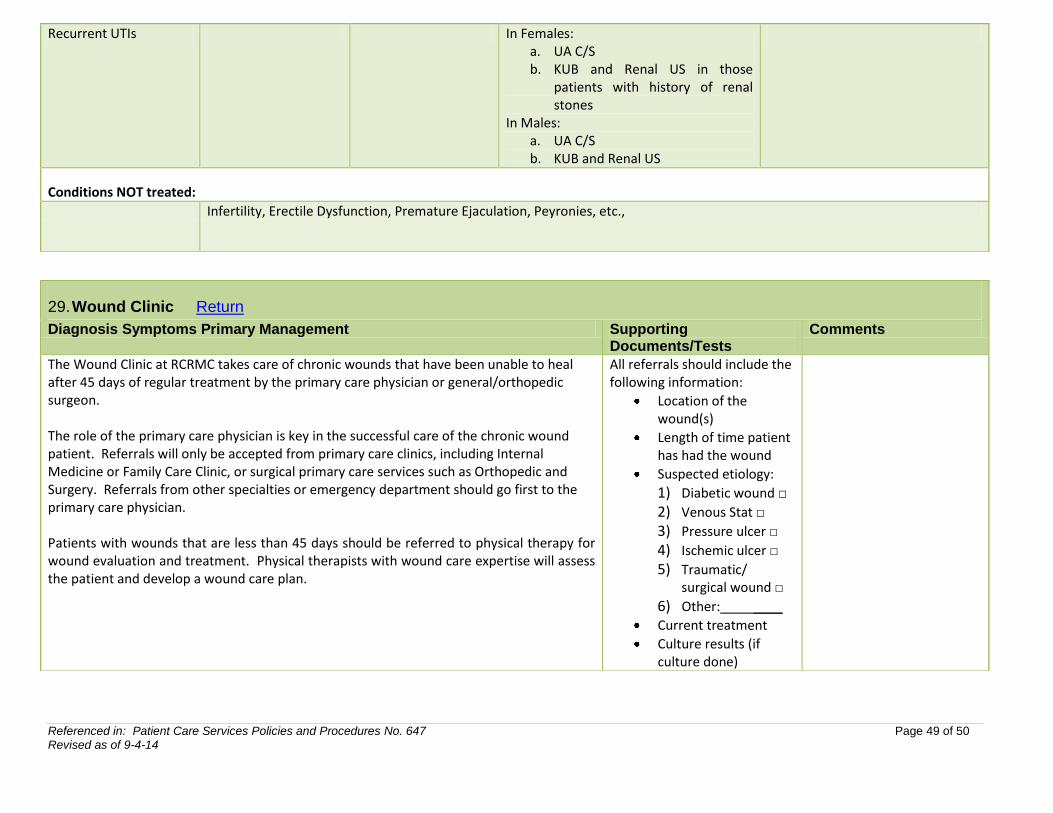
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 49 of 50 Revised as of 9-4-14
Recurrent UTIs In Females: a. UA C/S b. KUB and Renal US in those
patients with history of renal stones
In Males: a. UA C/S b. KUB and Renal US
Conditions NOT treated:
Infertility, Erectile Dysfunction, Premature Ejaculation, Peyronies, etc.,
29. Wound Clinic Return
Diagnosis Symptoms Primary Management Supporting Documents/Tests
Comments
The Wound Clinic at RCRMC takes care of chronic wounds that have been unable to heal after 45 days of regular treatment by the primary care physician or general/orthopedic surgeon. The role of the primary care physician is key in the successful care of the chronic wound patient. Referrals will only be accepted from primary care clinics, including Internal Medicine or Family Care Clinic, or surgical primary care services such as Orthopedic and Surgery. Referrals from other specialties or emergency department should go first to the primary care physician. Patients with wounds that are less than 45 days should be referred to physical therapy for wound evaluation and treatment. Physical therapists with wound care expertise will assess the patient and develop a wound care plan.
All referrals should include the following information:
Location of the wound(s)
Length of time patient has had the wound
Suspected etiology:
1) Diabetic wound □
2) Venous Stat □
3) Pressure ulcer □
4) Ischemic ulcer □
5) Traumatic/ surgical wound □
6) Other: ____
Current treatment
Culture results (if culture done)
Referenced in: Patient Care Services Policies and Procedures No. 647 Page 50 of 50 Revised as of 9-4-14
Recent antibiotic therapy
If patient is a diabetic, include HbA1c results within the last three months (submit results if outside lab used)





























