Embed Size (px)
Citation preview

JOURNAL OF ENDOUROLOGYVolume 3, Number 3, 1989Mary Ann Liebert, Inc., Publishers
Pédiatrie ESWL: Long-Term Resultsand Effects on Renal Growth
MARK C. ADAMS, M.D.,* DANIEL M. NEWMAN, M.D.,fand JAMES E. LINGEMAN, M.D.f
ABSTRACT
The Dornier HM3 lithotripter was used to treat 55 stone events in 44 pédiatrie patients.The mean patient age at treatment was 11.3 years, with the youngest patient being 13months of age. Sixty-two extracorporeal shock wave lithotripsy (ESWL) treatments were
necessary for the 55 stone events at a mean of 1186 shock waves (range 250 to 2100) at19.6 kV (range 16 to 26 kV). Follow-up was available for 95% of the treated stoneevents; 79% of patients were stone free at 3 months, and 83% eventually became stonefree. Risk factors for retained fragments in the pédiatrie population appear to be similarto those for adults. Renal growth of 14 treated renal units in 12 patients has beenunimpaired after ESWL treatment as judged by intravenous urography or sonography.
INTRODUCTION
With the virtual disappearance of endemic bladder calculi, the prevalence of pédiatriecalculous disease has progressively declined in industrialized societies.1 Several recent
reports suggest a prevalence of one calculous case per 1060 to one per 1380 general pédiatriehospital admissions,2-5 and 1% to 3% of urolithiasis cases still occur in the pédiatrie popula-tion.6-9
The majority of uroliths in children are now renal. Approximately one-third of pédiatriepatients with such stones will have an anatomic abnormality potentially predisposing to stones,5a higher percentage than in adults with calculi. Only one-third of children with stones have anidentifiable underlying metabolic disorder,5 although this percentage would likely be higher if afull metabolic evaluation were performed on each patient.4 Calcium salts are the most commonstone compositions found in North American children. Previously, hypercalciuria was thought tobe relatively uncommon in children with calcium urolithiasis;710 however, more recent studieshave demonstrated hypercalciuria to be present in as many as 53% of pédiatrie patients with
Resident in Urology, Indiana University School of Medicine.fMethodist Hospital Institute for Kidney Stone Disease, Indianapolis, IN
245
ADAMS ET AL.
calcium stones.4-"-13 There are many well-recognized causes of hypercalciuria, with or withouthypercalcemia, in children; however, idiopathic hypercalciuria is probably the most common
cause in children.12 Infection stones (magnesium ammonium phosphate/carbonate apatite) are thesecond most common stone composition in North American and the most common stones foundin European children.5 Such patients require thorough anatomic and metabolic evaluations.Approximately one-third of pédiatrie patients with struvite urolithiasis will have underlyingcongenital anomalies and another third have been reported to have vesicoureteral reflux.1214Significant underlying metabolic disorders may also coexist.41516 Uric acid lithiasis constitutes a
smaller percentage of stones in children than in adults,57 whereas cystinuria is associated with a
higher percentage of stones in children.5With the successful use of extracorporeal shock wave lithotripsy (ESWL) in adults, there has
been a natural evolution to the application of ESWL in the treatment of pédiatrie urolithiasis.Because of the relatively low prevalence of pédiatrie stone disease, experience with pédiatrieESWL at any single center has been limited.917-20 Herein is reported the experience with ESWLin the treatment of pédiatrie urolithiasis at the Methodist Hospital of Indiana.
PATIENTS AND METHODS
At the Methodist Hospital of Indiana, ESWL has been used in the treatment of 44 pédiatriepatients with stone disease. Fifty-five stone events were treated in these 44 patients. Bilateralrenal calculi treated in the same patient were considered to be separate stone events, whereasmultiple unilateral renal calculi were considered a single treatment event. Ureteral calculi were
counted as a separate stone event only if treated in situ and clearly away from any renal calculi.Preoperative evaluation of each patient included a thorough history and physical examination,
routine blood tests, urinalysis, and urine culture. Intravenous urography (and other radiographietests as indicated) was used to assess function, anatomy, and the presence or absence ofobstruction.
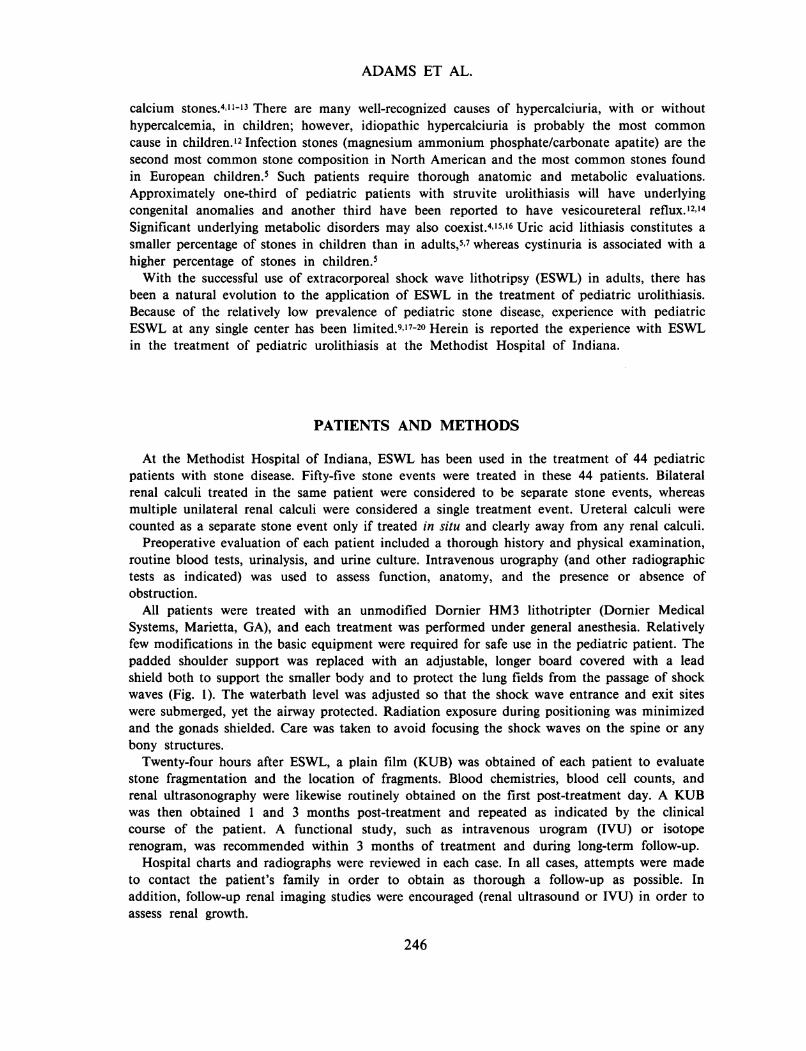
All patients were treated with an unmodified Dornier HM3 lithotripter (Dornier MedicalSystems, Marietta, GA), and each treatment was performed under general anesthesia. Relativelyfew modifications in the basic equipment were required for safe use in the pédiatrie patient. Thepadded shoulder support was replaced with an adjustable, longer board covered with a leadshield both to support the smaller body and to protect the lung fields from the passage of shockwaves (Fig. 1). The waterbath level was adjusted so that the shock wave entrance and exit siteswere submerged, yet the airway protected. Radiation exposure during positioning was minimizedand the gonads shielded. Care was taken to avoid focusing the shock waves on the spine or anybony structures.
Twenty-four hours after ESWL, a plain film (KUB) was obtained of each patient to evaluatestone fragmentation and the location of fragments. Blood chemistries, blood cell counts, andrenal ultrasonography were likewise routinely obtained on the first post-treatment day. A KUBwas then obtained 1 and 3 months post-treatment and repeated as indicated by the clinicalcourse of the patient. A functional study, such as intravenous urogram (IVU) or isotoperenogram, was recommended within 3 months of treatment and during long-term follow-up.
Hospital charts and radiographs were reviewed in each case. In all cases, attempts were madeto contact the patient's family in order to obtain as thorough a follow-up as possible. Inaddition, follow-up renal imaging studies were encouraged (renal ultrasound or IVU) in order toassess renal growth.
246
PEDIATRIC ESWL
FIG. 1. Gantry modification. Padded lead shield (shaded) used to support body and protect lung fieldsfrom shock waves.
RESULTS
Sixty-two ESWL treatments were necessary for the 55 stone events. The mean patient age attreatment was 11.3 years, with the youngest patient being 13 months old. The group was
comprised of 24 female and 20 male patients. Eighteen patients (41%) had histories of stonedisease and 15 previously had required open surgery for stone removal. Thirteen patients (30%)had anatomic abnormalities potentially predisposing to calculus formation, the most common
being neurogenic bladder dysfunction secondary to myelodysplasia, while sixteen (36%) had a
known metabolic risk factor for the stone disease under treatment. Urinary tract infection was
part of the clinical presentation in 21 patients (48%).The 55 treated stone events included right renal calculi in 22 patients, left renal calculi in 12,
and bilateral renal calculi in eight. Five ureteral calculi were treated in situ. Twenty-three of thetreated renal stone events involved only stones in the renal pelvis, with all but two being singlestones. Nineteen of the stone events involved only caliceal stones, of which ten were singlestones and nine multiple stones. Multiple pelvic and caliceal stones accounted for eight of thetreated stone events. All five ureteral calculi treated in situ were single stones. Table 1 showsstone events stratified by size and number. Stone size was the diameter of a single calculus or
the diameter of the largest of the multiple calculi. Stone composition was documented byanalysis of fragments in 64% of the patients and consisted of calcium oxalate in 36%,struvite/apatite in 18%, uric acid in 5%, and cystine in 5%.
Treatments consisted of a mean of 1186 shock waves (range 250 to 2100) at a mean 19.6 kV(range 16 to 26). Of the 62 treatments, less than 1000 total shock waves were applied in 24,between 1000 and 2000 shock waves in 37, and more than 2000 (2100) shock waves only once.
The maximum voltage applied was 20 kV or less for 50 treatments and more than 20 kV foronly 12 treatments. Pre-ESWL cystoscopy and placement of a ureteral catheter to assist inimaging of calculi during treatment was performed for ten stone events in nine patients. These
Table 1. Stone Events Stratified by Size (Cm) and Number
<1 1-2 >2
Single 18 13 4Multiple 13 7 0
247
ADAMS ET AL.
catheters were removed immediately after treatment in most instances. Indwelling ureteral stentswere utilized with six treated stone events in five patients. Five patients underwent retrogradeureteral stone displacement prior to ESWL, and two patients had unsuccessful stone manipula-tion prior to having ureteral stones treated in situ. One patient underwent ureteroscopy andultrasonic lithotripsy of a lower ureteral calculus, and another patient underwent cystolitholapaxyimmediately prior to ESWL of renal calculi. Two patients had percutaneous debulking ofstaghorn calculi prior to ESWL treatment of retained fragments, and three patients underwentsecondary nephrostolithotomy through established percutaneous tracts after ESWL. Three pa-tients were treated with hemiacidrin irrigations after ESWL.
The overall retreatment rate was 11% in this series (62 treatments in 55 stone events). Fivepatients required two ESWL treatments, and one patient three. Five of the patients requiringretreatment had large stone burdens, as all had multiple stones of at least 1 to 1.5 cm, includingone patient whose multiple 1-cm cystine stones were treated. The sixth patient requiredretreatment after initially receiving only 250 shock waves at 18 kV for a single 0.8-cm calculus.Fragmentation appeared adequate by fluoroscopy at the time of her initial treatment; however, a
KUB the next day revealed a 0.4-cm fragment, which was then retreated.Successful fragmentation of stones was achieved with ESWL in all patients except one. That
particular patient presented with a staghorn calculus composed of cystine. Residual 1-cm calicealstones from primary nephrostolithotomy were treated twice with ESWL prior to a secondarypercutaneous procedure, as fragmentation was still incomplete despite two sessions of ESWL.The patient was rendered stone free but required several additional nephrostomy tracts duringthe secondary percutaneous procedure.
No complications related to the many associated procedures were noted. Skin bruising at theentrance and exit sites of the shock waves was pronounced in many children immediately aftertreatment but resolved without sequelae. No patient suffered any pulmonary complications. Sixpatients developed low-grade temperature elevations after ESWL treatment, but no patientbecame septic. Three patients did develop obstructing distal-ureteral columns of fragments{Steinstrasse) of stone fragments after ESWL. Two Steinstrassen developed after treatment ofsingle 1.5-cm renal pelvic stones in two females (ages 5 and 6). The third column developedafter treatment of a 16-year-old patient for three calculi (0.5 to 1.2 cm). All Steinstrassenresolved spontaneously within 48 hours of treatment without intervention, and no patientrequired post-treatment manipulation for obstructing ureteral fragments. One small, asymptomat-ic perirenal hematoma was found on routine ultrasonography after treatment of a 15-year-oldfemale. Her 8-mm stone had been treated in the renal pelvis with 300 shock waves at 24 kVafter atraumatic retrograde displacement from the proximal ureter. The hematoma has resolvedwithout sequelae to date. The mean post-treatment hospital stay for the entire group was 2.9days (range 1 to 12 days).
Three patients have been lost to follow-up, whereas radiographie follow-up is complete on 41patients (93%) representing 52 of 55 stone events treated (95%). Mean follow-up for this group isnow 34 months (range 11 to 54 months). Forty-one of the 52 treated stone events with adequatefollow-up (79%) were stone free 3 months after treatment, while 83% eventually became stonefree. One-half of the patients had a stone-free state demonstrated by KUB, and the other halfwere confirmed to be stone free by tomography, ultrasonography, or computed axial tomographyin addition to KUB.
Retained fragments remain after nine of the treated stone events (17%). Three patients'fragments are clinically insignificant, as the fragments are smaller than 3 mm, asymptomatic, notinfectious stones and have demonstrated no regrowth. Clinically significant fragments remainedfollowing six treated stone events ( 11 %) and represent true failures of ESWL. All but two ofthese fragments are smaller than 3 mm; however, four of the fragments are infection stones, andthe other two have demonstrated significant regrowth and have required retreatment elsewhere.
248
PEDIATRIC ESWL
Of these nine treated stone events with retained fragments, the initial stone burden was quitelarge in three, one being a 35-mm partial staghorn calculus and the other two consisting ofmultiple stones (0.5 to 1.5 cm). Four of the remaining stone-bearing kidneys treated notachieving a stone-free state were hydronephrotic. In two of these kidneys, stones were located inthe lower-pole calix, as was the treated stone in another patient with a retained fragment. Anunsuccessful outcome occurred in only one patient with none of the above risk factors.
On routine survey of the spine on the follow-up radiographs, no patient demonstrated any new
scoliosis or other spinal deformity. Several of the older myelomeningocele patients in the serieshad severe preexisting scoliosis, which remained unchanged.
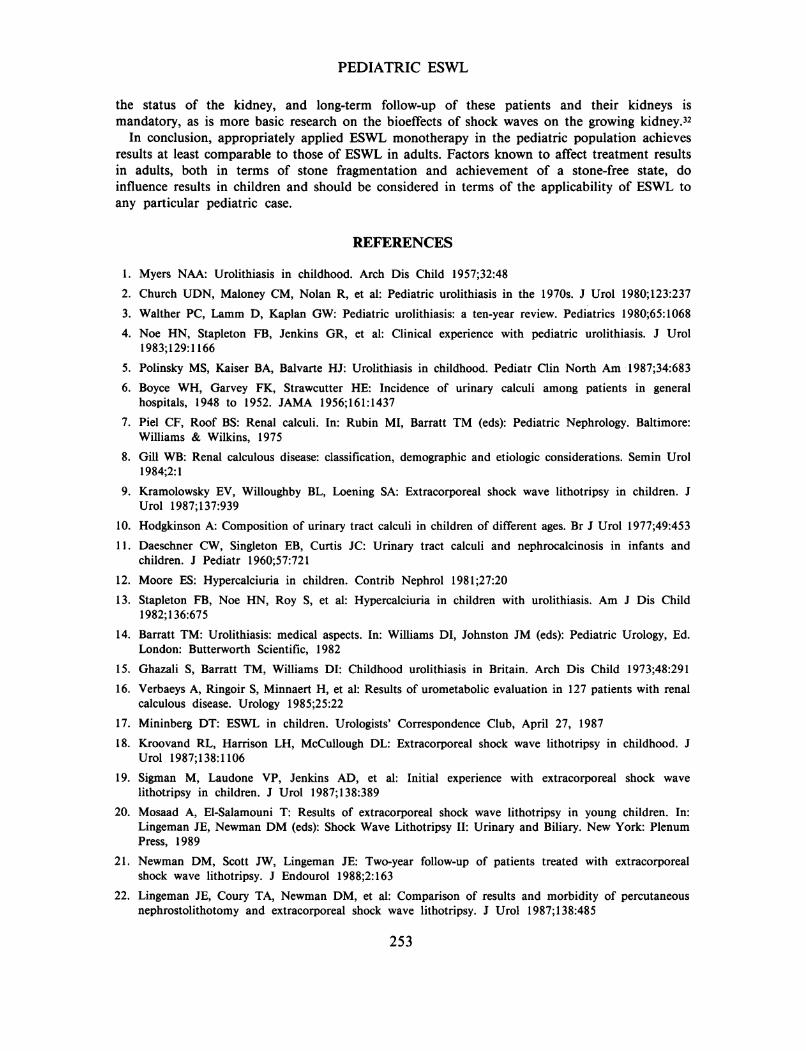
For 12 of these young patients, adequate measurements of renal size (renal length) was
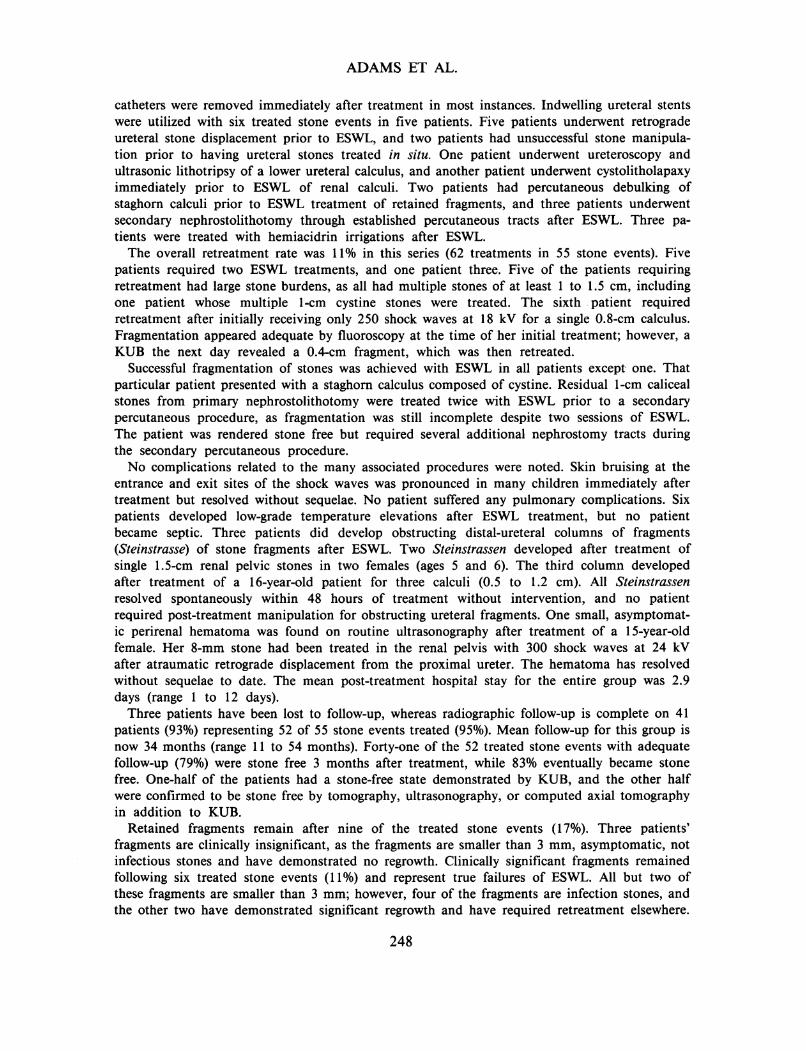
available both immediately prior to ESWL and at least 1 year (average 23 months) followingtreatment, representing measurements of 14 renal units in which stone events were treated.Measurements were made by IVU both initially and in follow-up in ten patients (12 renal units),whereas the pretreatment and posttreatment measurements were made by ultrasonography in twopatients. Measurements were included only when the renal outlines could be seen distinctlyduring an IVU (performed with standard techniques) to avoid significant differences inmagnification or when the ultrasonographer clearly marked and measured renal length. In Figure2, renal growth after ESWL is plotted against a normal renal growth curve (as measured byIVU). In each case, to date, there has been growth that at least parallels expected renal growth.
DISCUSSION
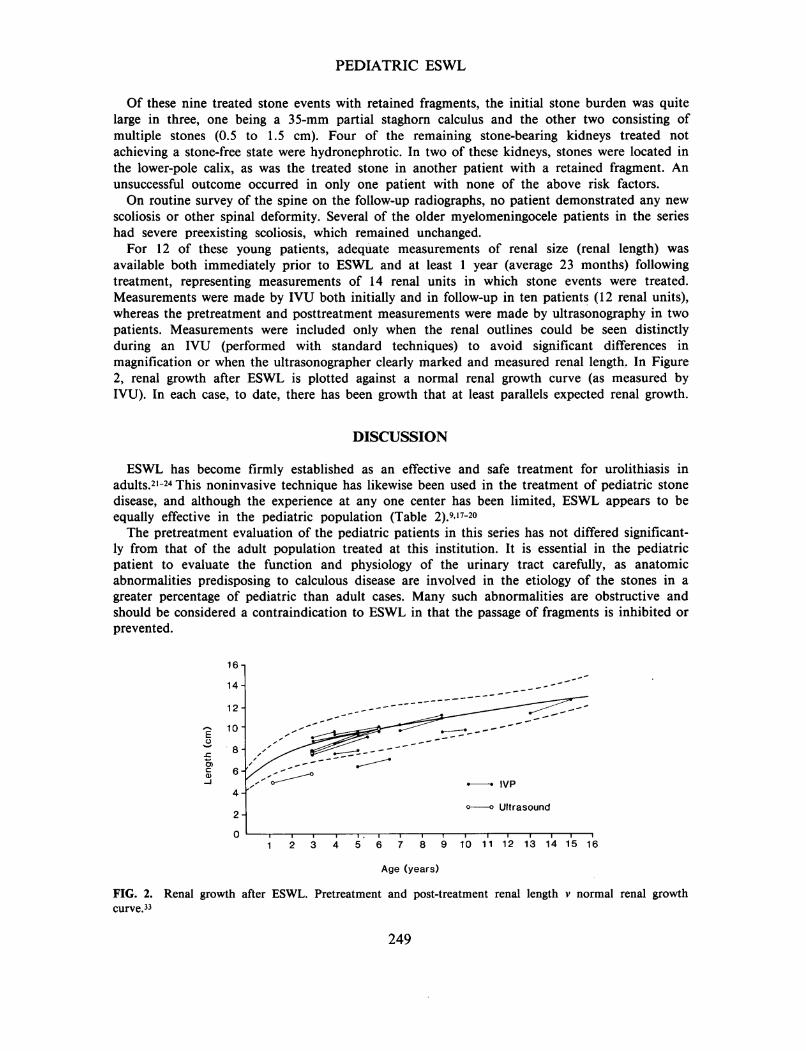
ESWL has become firmly established as an effective and safe treatment for urolithiasis inadults.21-24 This noninvasive technique has likewise been used in the treatment of pédiatrie stonedisease, and although the experience at any one center has been limited, ESWL appears to beequally effective in the pédiatrie population (Table 2).917-20
The pretreatment evaluation of the pédiatrie patients in this series has not differed significant-ly from that of the adult population treated at this institution. It is essential in the pédiatriepatient to evaluate the function and physiology of the urinary tract carefully, as anatomicabnormalities predisposing to calculous disease are involved in the etiology of the stones in a
greater percentage of pédiatrie than adult cases. Many such abnormalities are obstructive andshould be considered a contraindication to ESWL in that the passage of fragments is inhibited or
prevented.
16-,
0 '-1-1-1-1-r~.-1-1-1-1-1-1-1-1-1-1-11 2 3 4 5 6 7 8 9 10 1 1 12 13 14 15 16
Age (years)
FIG. 2. Renal growth after ESWL. Pretreatment and post-treatment renal length v normal renal growthcurve.33
249
ADAMS ET AL.
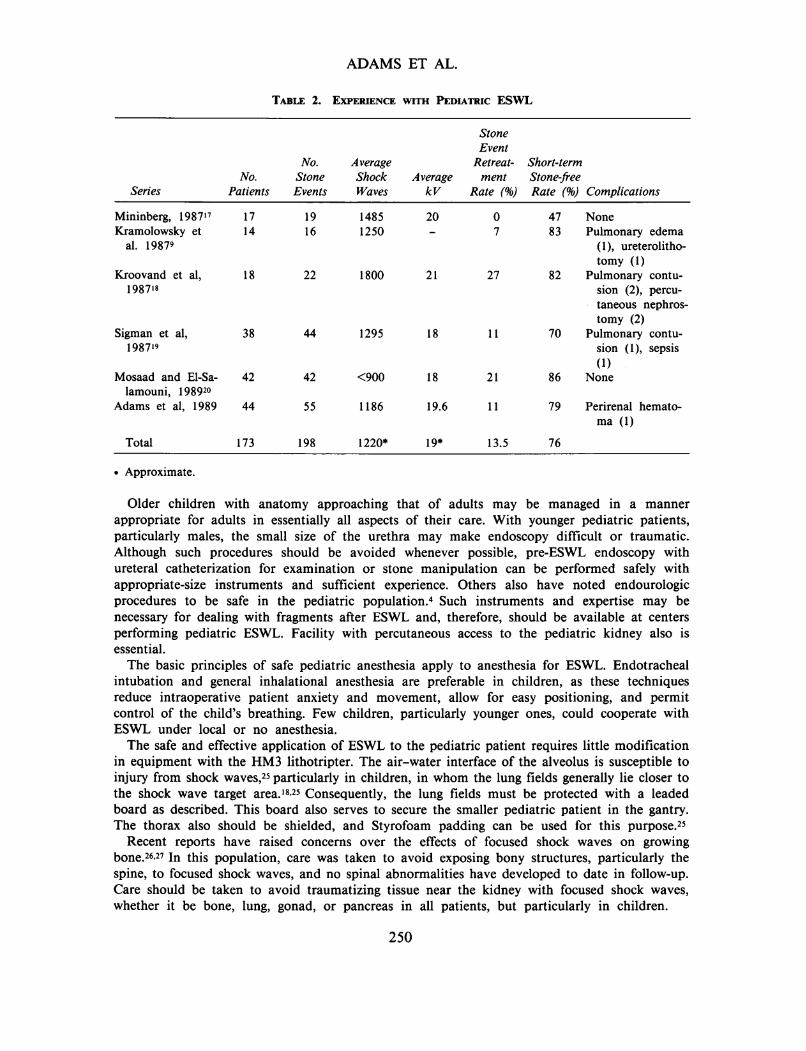
Table 2. Experience with Pediatric ESWL
SeriesNo.
Patients
No.StoneEvents
AverageShockWaves
AveragekV
StoneEvent
Retreat- Short-termment Stone-free
Rate (%) Rate (%) ComplicationsMininberg, 198717 17 19Kramolowsky et 14 16
al. 19879
Kroovand et al, 18 22198718
Sigman et al, 38 44198719
Mosaad and Ei-Sa- 42 42lamouni, 198920
Adams et al, 1989 44 55
Total 173 198
14851250
1800
1295
<900
1186
1220*
20
21
19.6
19*
27
11
21
11
13.5
4783
82
70
86
79
76
NonePulmonary edema
(1), ureterolitho-tomy (1)
Pulmonary contu-sion (2), percu-taneous nephros-tomy (2)
Pulmonary contu-sion (1), sepsis(1)
None
Perirenal hemato-ma (1)
• Approximate.
Older children with anatomy approaching that of adults may be managed in a manner
appropriate for adults in essentially all aspects of their care. With younger pediatric patients,particularly males, the small size of the urethra may make endoscopy difficult or traumatic.Although such procedures should be avoided whenever possible, pre-ESWL endoscopy withureteral catheterization for examination or stone manipulation can be performed safely withappropriate-size instruments and sufficient experience. Others also have noted endourologicprocedures to be safe in the pediatric population.4 Such instruments and expertise may benecessary for dealing with fragments after ESWL and, therefore, should be available at centersperforming pediatric ESWL. Facility with percutaneous access to the pediatric kidney also isessential.
The basic principles of safe pediatric anesthesia apply to anesthesia for ESWL. Endotrachealintubation and general inhalational anesthesia are preferable in children, as these techniquesreduce intraoperative patient anxiety and movement, allow for easy positioning, and permitcontrol of the child's breathing. Few children, particularly younger ones, could cooperate withESWL under local or no anesthesia.
The safe and effective application of ESWL to the pediatric patient requires little modificationin equipment with the HM3 lithotripter. The air-water interface of the alveolus is susceptible toinjury from shock waves,25 particularly in children, in whom the lung fields generally lie closer tothe shock wave target area.1825 Consequently, the lung fields must be protected with a leadedboard as described. This board also serves to secure the smaller pediatric patient in the gantry.The thorax also should be shielded, and Styrofoam padding can be used for this purpose.25
Recent reports have raised concerns over the effects of focused shock waves on growingbone.26-27 In this population, care was taken to avoid exposing bony structures, particularly thespine, to focused shock waves, and no spinal abnormalities have developed to date in follow-up.Care should be taken to avoid traumatizing tissue near the kidney with focused shock waves,whether it be bone, lung, gonad, or pancreas in all patients, but particularly in children.
250
PEDIATRIC ESWL
The number and energy level of shock waves that can safely be applied to a kidney,particularly a growing kidney, are unknown. Therefore, the number of shock waves andkilovoltage applied should be kept to the absolute minimum required for effective fragmentationof the stone in pédiatrie patients. Such conservative application of ESWL, although responsiblefor one possibly avoidable retreatment in this series, did result in effective stone fragmentationin these patients and should minimize trauma to the growing kidney. Skin bruising is more
pronounced in children because the shock wave is generally more focused at the point at whichit passes through the skin. Likewise, there is less soft tissue between the waterbath and stone,which, at least in theory, might serve to reduce the dissipation of shock wave energy and impartsome enhanced efficacy in terms of stone fragmentation. It should be noted, however, that thefactors that affect stone fragmentation in adults22 will influence fragmentation in children. Of thepatients requiring retreatment in this series, all but one demonstrated risk factors for incompletefragmentation such as a large stone burden or cystine stone composition.
Treatment with ESWL was well tolerated by these patients. In spite of the small diameter ofthe pédiatrie ureter, children discharge fragments created by ESWL with little morbidity.Although indwelling stents were used only sparingly, few patients developed symptoms orevidence of obstruction during the passage of gravel. No patient required a secondary procedurepost-ESWL because of obstructing fragments. The ability of the pédiatrie ureter to handle a
relatively large stone burden may explain why typical colic is rare among children presentingwith stones.412.28.29
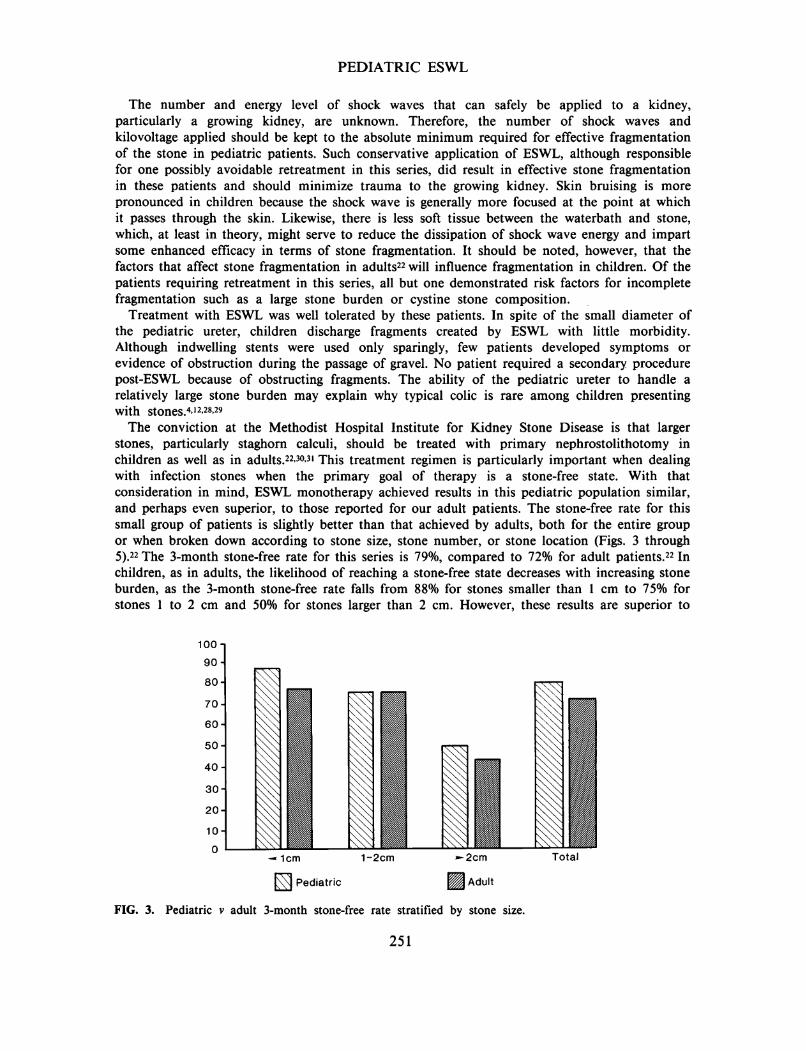
The conviction at the Methodist Hospital Institute for Kidney Stone Disease is that largerstones, particularly staghorn calculi, should be treated with primary nephrostolithotomy inchildren as well as in adults.22'30.31 This treatment regimen is particularly important when dealingwith infection stones when the primary goal of therapy is a stone-free state. With thatconsideration in mind, ESWL monotherapy achieved results in this pédiatrie population similar,and perhaps even superior, to those reported for our adult patients. The stone-free rate for thissmall group of patients is slightly better than that achieved by adults, both for the entire groupor when broken down according to stone size, stone number, or stone location (Figs. 3 through5).22 The 3-month stone-free rate for this series is 79%, compared to 72% for adult patients.22 Inchildren, as in adults, the likelihood of reaching a stone-free state decreases with increasing stoneburden, as the 3-month stone-free rate falls from 88% for stones smaller than 1 cm to 75% forstones 1 to 2 cm and 50% for stones larger than 2 cm. However, these results are superior to
Pédiatrie ¡Ü Adult
FIG. 3. Pédiatrie v adult 3-month stone-free rate stratified by stone size.
251
ADAMS ET AL.
100 o.
=> 90 1 80-
£ 70-co2 60-coa 50
CD
I 40.a
I 30"55« 20-Ig 10-a.
0One Stone Multiple Stones
Pédiatrie Adult
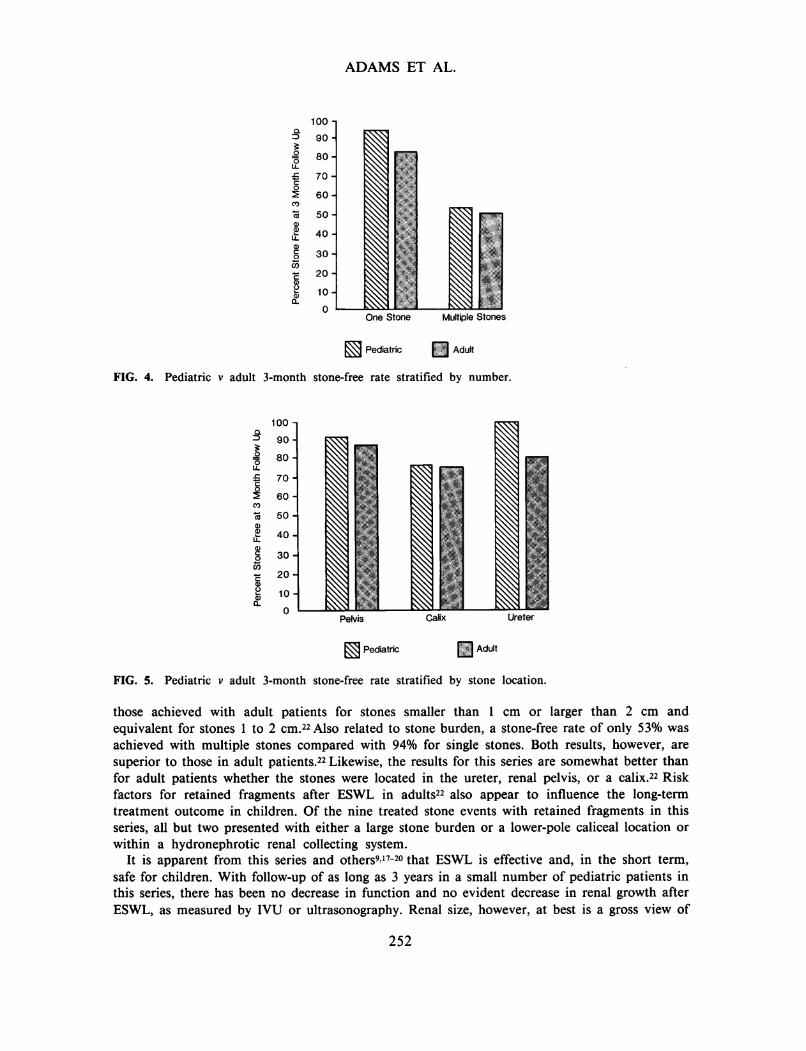
FIG. 4. Pédiatrie v adult 3-month stone-free rate stratified by number.
100a3 90
I 80
£ 70co5 60CO
2LL
50 H40
30
_ 20Si io
CL0
Pelvis Calix Ureter
R^| Pédiatrie ~J Adult
FIG. 5. Pédiatrie v adult 3-month stone-free rate stratified by stone location.
those achieved with adult patients for stones smaller than 1 cm or larger than 2 cm andequivalent for stones 1 to 2 cm.22 Also related to stone burden, a stone-free rate of only 53% was
achieved with multiple stones compared with 94% for single stones. Both results, however, are
superior to those in adult patients.22 Likewise, the results for this series are somewhat better thanfor adult patients whether the stones were located in the ureter, renal pelvis, or a calix.22 Riskfactors for retained fragments after ESWL in adults22 also appear to influence the long-termtreatment outcome in children. Of the nine treated stone events with retained fragments in thisseries, all but two presented with either a large stone burden or a lower-pole caliceal location or
within a hydronephrotic renal collecting system.It is apparent from this series and others917-20 that ESWL is effective and, in the short term,
safe for children. With follow-up of as long as 3 years in a small number of pédiatrie patients inthis series, there has been no decrease in function and no evident decrease in renal growth afterESWL, as measured by IVU or ultrasonography. Renal size, however, at best is a gross view of
252
PEDIATRIC ESWL
the status of the kidney, and long-term follow-up of these patients and their kidneys ismandatory, as is more basic research on the bioeffects of shock waves on the growing kidney.32
In conclusion, appropriately applied ESWL monotherapy in the pédiatrie population achievesresults at least comparable to those of ESWL in adults. Factors known to affect treatment resultsin adults, both in terms of stone fragmentation and achievement of a stone-free state, doinfluence results in children and should be considered in terms of the applicability of ESWL toany particular pédiatrie case.
REFERENCES
1. Myers NAA: Urolithiasis in childhood. Arch Dis Child 1957;32:482. Church UDN, Maloney CM, Nolan R, et al: Pédiatrie urolithiasis in the 1970s. J Urol 1980;123:2373. Walther PC, Lamm D, Kaplan GW: Pédiatrie urolithiasis: a ten-year review. Pediatrics 1980;65:10684. Noe HN, Stapleton FB, Jenkins GR, et al: Clinical experience with pédiatrie urolithiasis. J Urol
1983;129:11665. Polinsky MS, Kaiser BA, Balvarte HJ: Urolithiasis in childhood. Pediatr Clin North Am 1987;34:6836. Boyce WH, Garvey FK, Strawcutter HE: Incidence of urinary calculi among patients in general
hospitals, 1948 to 1952. JAMA 1956; 161:14377. Piel CF, Roof BS: Renal calculi. In: Rubin MI, Barratt TM (eds): Pédiatrie Nephrology. Baltimore:
Williams & Wilkins, 19758. Gill WB: Renal calculous disease: classification, demographic and etiologic considerations. Semin Urol
1984;2:19. Kramolowsky EV, Willoughby BL, Loening SA: Extracorporeal shock wave lithotripsy in children. J
Urol 1987;137:93910. Hodgkinson A: Composition of urinary tract calculi in children of different ages. Br J Urol 1977;49:45311. Daeschner CW, Singleton EB, Curtis JC: Urinary tract calculi and nephrocalcinosis in infants and
children. J Pediatr 1960;57:72112. Moore ES: Hypercalciuria in children. Contrib Nephrol 1981;27:2013. Stapleton FB, Noe HN, Roy S, et al: Hypercalciuria in children with urolithiasis. Am J Dis Child
1982;136:67514. Barratt TM: Urolithiasis: medical aspects. In: Williams DI, Johnston JM (eds): Pédiatrie Urology, Ed.
London: Butterworth Scientific, 198215. Ghazali S, Barratt TM, Williams DI: Childhood urolithiasis in Britain. Arch Dis Child 1973;48:29116. Verbaeys A, Ringoir S, Minnaert H, et al: Results of urometabolic evaluation in 127 patients with renal
calculous disease. Urology 1985;25:2217. Mininberg DT: ESWL in children. Urologists' Correspondence Club, April 27, 198718. Kroovand RL, Harrison LH, McCullough DL: Extracorporeal shock wave lithotripsy in childhood. J
Urol 1987;138:110619. Sigman M, Laudone VP, Jenkins AD, et al: Initial experience with extracorporeal shock wave
lithotripsy in children. J Urol 1987;138:38920. Mosaad A, El-Salamouni T: Results of extracorporeal shock wave lithotripsy in young children. In:
Lingeman JE, Newman DM (eds): Shock Wave Lithotripsy II: Urinary and Biliary. New York: PlenumPress, 1989
21. Newman DM, Scott JW, Lingeman JE: Two-year follow-up of patients treated with extracorporealshock wave lithotripsy. J Endourol 1988;2:163
22. Lingeman JE, Coury TA, Newman DM, et al: Comparison of results and morbidity of percutaneousnephrostolithotomy and extracorporeal shock wave lithotripsy. J Urol 1987;138:485
253
ADAMS ET AL.
23. Lingeman JE, Newman DM, Mertz JHO, et al: Extracorporeal shock wave lithotripsy: the MethodistHospital of Indiana experience. J Urol 1986;135:1134
24. Drach GW, Dretler SP, Fair WR, et al: Report of the United States cooperative study of extracorporealshock wave lithotripsy. J Urol 1986;135:1127
25. Chaussy C: Extracorporeal Shock Wave Lithotripsy: Technical Concept, Experimental Research, andClinical Application. Basel; S Karger, 1986
26. Graff J, Pastor J, Senge T, et al: The effect of high energy shock waves on bony tissue: an experimentalstudy [abstract]. J Urol 1987;137:278A
27. Yeaman LD, Jerome CP, McCullough DL: Effects of shock waves on the structure and growth ofimmature rat epiphysis. J Urol 1989; 141:670
28. Bass HN, Emanuel B: Nephrolithiasis in childhood. J Urol 1966;95:74929. Sinno K, Boyce WH, Resnick MI: Childhood urolithiasis. J Urol 1979,121:66230. Kahnoski RJ, Lingeman JE, Coury TA, et al: Combined percutaneous and extracorporeal shock wave
lithotripsy for staghorn calculi: an alternative to anatrophic nephrolithotomy. J Urol 1986;135:67931. Lingeman JE, Smith LH, Woods JR, et al: Staghorn calculi. In: Lingeman JE, Smith LH, Woods JR, et
al (eds): Urinary Calculi: ESWL, Endourology, and Medical Therapy. Philadelphia: Lea & Febiger, 198932. Lingeman JE, McAteer JL, Kempson SA, et al: Bioeffects of extracorporeal shock wave lithotripsy:
strategy for research and treatment. Urol Clin North Am 1988;15:50733. Stolpe Y, King LR, White H: The normal range of renal size in children. Invest Urol 1967;4:600
Address reprint requestsJames E. Lingeman, M.D.
1801 N. Senate Blvd., No. 655Indianapolis, IN 46202
254





























