Embed Size (px)
Citation preview
Abstract:Infants and children are commonvictims of disaster or mass casualtysituations. Prehospital providersprovide the initial care andstabilization at the scene of a masscasualty event. There are a numberof challenges the prehospitalprovider faces when caring forchildren in a mass casualty event,among them are the following: thephysiology of children differs fromadults, children are particularlyvulnerable in a disaster, separationfrom parents or caregiversmay occur,and protocols developed for adultsmay not work well for children. Thisarticle reviews the planning andtriage considerations for prehospitalproviders caring for children in amass casualty event.
Keywords:disaster; triage; pediatrics;
emergency medical services;
planning; mass casualty;
prehospital
Department of Pediatrics, University of
Arkansas for Medical Sciences, Little
Rock, AR.
Reprint requests and correspondence:
James Graham, MD, Arkansas
Children’s Hospital, #1 Children’s Way,
Little Rock, AR 72202-3591.
1522-8401/$ - see front matter
© 2009 Published by Elsevier Inc.
PE
Pediatric MassCasualty: Triageand Planning forthe Prehospital
Provider
DIATRIC MASS CASUALTY / LYLE, T
Kristin Lyle, MD, Tonya Thompson, MD,James Graham, MD
mass casualty event (MCE) involving a large number ofchildren is a prospect that many prehospital providers
Amight consider to be their worst nightmare. Unfortu-nately, children may be involved in any mass casualtyresponse. In one recent study of Disaster Medical Assistance Team(DMAT) deployment, almost one third of the patients seen inDMAT field clinics were children.1 Some disasters have adisproportionate number of pediatric victims, such as schoolshootings. Children have higher morbidity and mortality during adisaster than adults. Age is inversely related to increasedmorbidity and mortality in disaster scenarios.2 The needs and,henceforth, the care required by children in an MCE are different.Therefore, consideration and planning for the needs of children inthe event of a MCE are imperative.
Difficulties in the prehospital care of children in non–masscasualty emergency situations have been well documented,including the lack of proper equipment, the relative lack ofpractice for technical skills, and lack of pediatric-specificcontinuing education.3-5 These pediatric-specific shortcomingsin our day-to-day emergency care system are likely to beexacerbated in an MCE.
Several recent studies have demonstrated deficiencies in thepreparedness of the emergency medical system for the care ofchildren in disaster or mass casualty situations. One study notedsignificant deficiencies in pediatric training and equipmentamong DMATs.6 A recent study of pediatricians in Michigan
HOMPSON AND GRAHAM • VOL. 10, NO. 3 173

174 VOL. 10, NO. 3 • PEDIATRIC MASS CASUALTY / LYLE, THOMPSON AND GRAHAM
found that 38% had never attended a lecture onbioterrorism and 85% had never participated in abioterrorism drill. The authors concluded thatpediatricians are “overwhelmingly underpreparedto deal with an event” of bioterrorism.7 A nationalsurvey of ambulance services found deficiencies inthe preparedness of many services for the care ofchildren in MCEs.8
PREHOSPITAL CHALLENGES IN THECARE OF CHILDREN
There are several physiologic vulnerabilities inchildren that pose a challenge in an MCE.9-11
Figure 1 gives a partial list of the physiologicdifferences between children and adults that areimportant in the management of mass casualties.Children are physiologically and psychologicallyless fit than adults to survive the acute, subacute,and chronic stresses of a disaster. Children have alarger body surface/mass ratio than adults; predis-posing them to heat loss and increased vulner-ability to contact toxins. Infants have a particularlylarger head to body ratio predisposing to headinjury. Depending on the developmental stage ofthe child, there may be limited communication andself-protection abilities. For example, a young childmay not have the motor skills to escape adangerous situation. Even if they have the motorability, they may lack the cognitive ability torecognize the danger.
Because children are typically dependent on theirparents or caregivers, identification and separationare important difficulties during a disaster. Theremay be children whose adult caregivers have beenincapacitated or injured. Reunification of childrenand parents can take months or years or may not bepossible at all in some cases. Patient tracking of
FIGURE 1. Physiologic differen
pediatric victims who require transport is especiallyimportant to ensure future reunification of thosechildren with their families.12-14
First responders and emergency medical services(EMS) providers are faced with the additionalchallenge of securing the scene of a disaster andensuring the safety of the victims as well as their ownstaff. Protecting unsupervised or orphaned childrenat a disaster scene can be more of a challenge thanadults but should be given a high priority.
One of the biggest pediatric care challenges facingprehospital care providers is airway management.There are several anatomic factors that impact themaintenance of a pediatric airway. The child's headis disproportionately large, with a prominent occi-put. When lying in a supine position, the chin istucked and the head is pitched forward, makingproper positioning of the airway difficult to achieveand maintain. A child's airway is smaller and moreanterior, making it more difficult to visualize andintubate. The smaller diameter makes the airwaymore prone to occlusion, with secretions or smallamounts of debris.
It is important for the prehospital provider to beaware that the most common cause of cardiacarrest in a child is the inability to establish ormaintain a patent airway or the inability tooxygenate or ventilate a child. In a child with adepressed level of consciousness, the airway maysimply become occluded from malpositioning of thehead. Studies have shown that attempts at intuba-tion by EMS providers in the pediatric patient areoften unsuccessful, even in a relatively controlledsetting.15 Given the difficulties of pediatric fieldintubation in controlled circumstances, successfulintubation in an MCE may be even less likely. Thefocus for prehospital airway management in thedisaster situation should be on positioning andbag valve mask ventilation rather than on invasive
ces in children in disasters.

PEDIATRIC MASS CASUALTY / LYLE, THOMPSON AND GRAHAM • VOL. 10, NO. 3 175
techniques. Positioning the child's airway appro-priately can be a lifesaving intervention. Anotherimportant intervention that is often overlooked inthe prehospital setting is appropriate suctioning ofthe child's airway. Because of the smaller diameterof the airway, it can easily be compromised (oreven occluded) by secretions, especially in theevent of chemical exposure.
Blast injury can be seen in certain MCEs. Injurypatterns in children after a blast injury also differfrom their adult counterparts and from nonblastpediatric injuries.16,17 These different injury pat-terns must be recognized by the prehospitalprovider because explosives remain a weapon ofchoice among terrorist organizations. Because thehead of a child is proportionately larger, there is ahigher frequency of blunt traumatic brain injuries.17
Children's smaller body mass, less subcutaneous fat,more pliable skeletons, and close proximity oforgans mean that the energy imparted from theblast or flying debris can result in a greater forceapplied per unit of body area. Children are morelikely to sustain multisystem injury rather thanisolated injuries. Because of the pliability of thepediatric skeleton, there may be internal organinjury without overlying bony fracture. Identifica-tion of shock in a pediatric victim of a blast injurycan be difficult for the prehospital provider. Thechild's ability to maintain blood pressure andcardiac output with increasing heart rate can bean important protective mechanism; but thesemechanisms mean that the signs of early shockdiffer in children and adults. Tachycardia, poordistal pulse quality, and poor skin perfusion areearly signs of shock in children, which must berecognized in the field.
Any incident involving a toxic chemical exposureposes special challenges to the EMS provider.9
Children live closer to the ground, and therefore,are often the first to become symptomatic from achemical agent. They have higher baseline respira-tory rates and are at higher risk for airborne toxinexposure. Nerve gas antidote kits available foradults are not yet available for children in theUnited States. Management of the airway is still ofutmost importance in the chemically exposed childand can be even more challenging due to increasedairway secretions that may be caused by thechemical. Children are at increased risk for dermalabsorption of toxins due to their thinner skin.Children have a greater body surface/mass ratio, soa smaller total amount of exposed skin can stillprovide significant absorption.9,18
One of the most important steps in the initialmanagement of any victim of a chemical exposure
is decontamination. The thin skin and largesurface area/mass ratio of pediatric patients alsoplaces them at risk for hypothermia during thedecontamination process. Warm water decontami-nation may prevent hypothermia in children butmay not be available to the prehospital provider inthe field. The ideal pediatric decontaminationsystem would use large-volume, low-pressurewarm water. In addition, infants and childrenmay need a parent or adult to accompany themin the decontamination process, requiring evenmore warm water and a facility large enough toaccommodate family units. Prehospital providersshould plan for active rewarming measures afterdecontamination. These measures might includeblankets, radiant warmers, and warm postdeconta-mination clothing.19,20
Biological agent exposure in children also posesspecial challenges.9,21,22 Children have a relativelyimmature immune system and therefore may have ahigher mortality rate than adults from any seriousinfection. Children dehydrate more easily thanadults from any toxin producing gastroenteritis.Most young children have poor hygiene habits, sotransmission rates of biological agents amongchildren can be very rapid. This rapid transmissionmeans that outbreaks of infectious agents may befirst detected in daycare or school settings.
Unfortunately, some of the recommended treat-ments for biological terrorism agents have beenpoorly studied, rarely used, or are relatively contra-indicated in children.14,22
Nuclear and radiologic exposures in children willalso produce higher levels of morbidity and mortalitythan in adults.23,24 Again, the greater surface area/mass ratio and thinner skin leave children moresusceptible to these exposures. Likewise, their shortstature and higher baseline respiratory rate leadsthem to receive higher particulate exposure of inhaledradioactive fallout. Lower total intravascular volumereserves in children leave them more susceptible todehydration from the gastrointestinal losses encoun-tered from acute radiation syndrome.23,24
In addition to the anatomic and physiologicvulnerabilities, there are several pediatric treatmentconsiderations that may pose special challenges inan MCE.8-11,25 For many medications, a single adultdosage form is adequate. There is no “one size fitsall” dosing of medications or fluids in children—most medications involve kilogram dosing andcalculations. Medication calculation and adminis-tration for children can be problematic in routineclinical prehospital situations but especially so forproviders faced with multiple pediatric victims.Children require a broad range of equipment sizes,

176 VOL. 10, NO. 3 • PEDIATRIC MASS CASUALTY / LYLE, THOMPSON AND GRAHAM
and maintaining adequate stocks of this equipmentis a preparedness challenge.
Children, and particularly infants, are especiallyvulnerable to heat loss. Thus, temperature control isparticularly important and may be a substantialchallenge in shelter situations. Because childrenmay not be able to effectively communicate theirmedical history and needs, separation from parentsor caregivers presents a special treatment problem,which is exacerbated in the MCE situation.12
The other treatment dimension that becomes achallenge in a mass casualty situation is therelatively limited availability of pediatric specialtycare and lack of pediatric surge capacity.25 Incomparison to adult care, the care of critically illor injured children occurs in a smaller number ofspecialized centers, and some general hospitals lackthe resources necessary for the care of ill or injuredchildren. A study by the Centers for Disease Controlfound that only 5.5% of US hospital emergencydepartments had all the pediatric equipmentrecommended by the American Academy of Pedia-trics and American College of Emergency Physi-cians and that only half had 85% or more of therecommended equipment.26 Another study of emer-gency department preparedness found substantialdeficiencies in necessary pediatric equipment andmedications.27 Thus, the availability of pediatricspecialty care or even pediatric inpatient beds in anMCE may be limited in a given area. Transport ofsuch children to other centers away from thedisaster site may be necessary, and planning forsuch mass pediatric transport is important.
PLANNING CONSIDERATIONS FORPEDIATRIC PREHOSPITAL CARE IN MCES
MostMCEs involve children. Table 1 includes a listof several sentinel events from around the globe thathave included children over the past 2 decades.28-58
Lessons learned from these events emphasize thechallenges faced at the scene by prehospital provi-ders. These lessons help focus efforts and prioritiesin the planning stages for future MCEs. Managing anMCE in the field requires a systematic approach thatencompasses elements of command structure, scenesafety, communication, assessment and triage ofpatients, and finally treatment, transport to local ortertiary facilities, and disposition.59
Command Structure
The most important management aspect of anyMCE is the presence of a unified and organized
command structure. The type and composition of thiscommand structure should be organized in thepreplanning stage. The Oklahoma City bombingprovides an example of the need for preplannedcoordination among local, community, state, andfederal agencies as well as nontraditional agenciessuch as public utilities. This MCE involved thecoordination of more than 75 fire departments andmore than 100 law enforcement agencies. TheFederal Emergency Management Agency dispatched11 urban search and rescue task forces. Telephoneand electric utilities were involved in the response.The incident command was coordinated by theOklahoma City Fire Department.37 Problems facedby the incident command included a flood ofvolunteers who came to the site of the explosion.Although well intentioned, this became a logisticalproblem.60 One of the advantages the respondingagencies had was previous participation in a course atthe Emergency Management Institute.37 Multiagencypreplanning and coordination help establish a coor-dinated incident command structure during an MCE.
Incident command should be flexible and ready torespond to any type of disaster in the “all-hazardmode.” Tactical decisions made by first arrivingcommanders should be flexible, tempered by incom-ing and frequently changing information. The needfor flexibility and altering the response to changinginformation were vividly demonstrated in the WorldTrade Center attacks of September 11, 2001.61
Responding personnel to the 9/11 attacks initiallyassumed that a small plane or light aircraft hadveered off course and struck the building. Therefore,initial decision making planned for the triage area tobe established on the first floor of Tower 1. Before thearea could be established, the second tower was hitand subsequently collapsed. Incident command wasthen reestablished at a nearby undamaged hotel, andthe search and rescue operation continued.61 Thisevent illustrates the scope of planning needed, forexample, to prepare for the possibility that theestablished Incident Command itself may be injeopardy and that alternate sites and contingencyplans need to be secured.
Scene Safety and Control
Disaster scene safety and control are important toprevent further injury to victims or initial injuryto rescue workers. The importance of scene safetyis dramatically demonstrated in recent terroristbombings, where secondary devices were set toexplode after the arrival of prehospital providers.This situation is well illustrated by the ColumbineHigh School shooting events in Littleton, CO, on
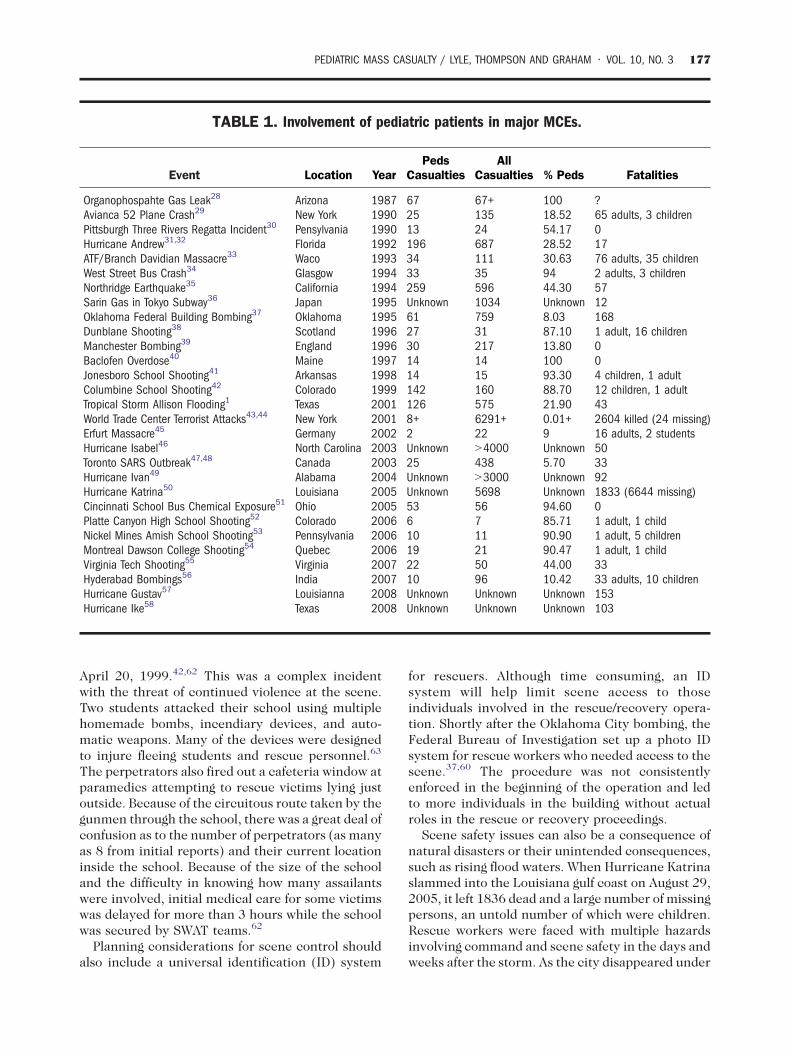
TABLE 1. Involvement of pediatric patients in major MCEs.
Event Location YearPeds
CasualtiesAll
Casualties % Peds Fatalities
Organophospahte Gas Leak28 Arizona 1987 67 67+ 100 ?Avianca 52 Plane Crash29 New York 1990 25 135 18.52 65 adults, 3 childrenPittsburgh Three Rivers Regatta Incident30 Pensylvania 1990 13 24 54.17 0Hurricane Andrew31,32 Florida 1992 196 687 28.52 17ATF/Branch Davidian Massacre33 Waco 1993 34 111 30.63 76 adults, 35 childrenWest Street Bus Crash34 Glasgow 1994 33 35 94 2 adults, 3 childrenNorthridge Earthquake35 California 1994 259 596 44.30 57Sarin Gas in Tokyo Subway36 Japan 1995 Unknown 1034 Unknown 12Oklahoma Federal Building Bombing37 Oklahoma 1995 61 759 8.03 168Dunblane Shooting38 Scotland 1996 27 31 87.10 1 adult, 16 childrenManchester Bombing39 England 1996 30 217 13.80 0Baclofen Overdose40 Maine 1997 14 14 100 0Jonesboro School Shooting41 Arkansas 1998 14 15 93.30 4 children, 1 adultColumbine School Shooting42 Colorado 1999 142 160 88.70 12 children, 1 adultTropical Storm Allison Flooding1 Texas 2001 126 575 21.90 43World Trade Center Terrorist Attacks43,44 New York 2001 8+ 6291+ 0.01+ 2604 killed (24 missing)Erfurt Massacre45 Germany 2002 2 22 9 16 adults, 2 studentsHurricane Isabel46 North Carolina 2003 Unknown N4000 Unknown 50Toronto SARS Outbreak47,48 Canada 2003 25 438 5.70 33Hurricane Ivan49 Alabama 2004 Unknown N3000 Unknown 92Hurricane Katrina50 Louisiana 2005 Unknown 5698 Unknown 1833 (6644 missing)Cincinnati School Bus Chemical Exposure51 Ohio 2005 53 56 94.60 0Platte Canyon High School Shooting52 Colorado 2006 6 7 85.71 1 adult, 1 childNickel Mines Amish School Shooting53 Pennsylvania 2006 10 11 90.90 1 adult, 5 childrenMontreal Dawson College Shooting54 Quebec 2006 19 21 90.47 1 adult, 1 childVirginia Tech Shooting55 Virginia 2007 22 50 44.00 33Hyderabad Bombings56 India 2007 10 96 10.42 33 adults, 10 childrenHurricane Gustav57 Louisianna 2008 Unknown Unknown Unknown 153Hurricane Ike58 Texas 2008 Unknown Unknown Unknown 103
PEDIATRIC MASS CASUALTY / LYLE, THOMPSON AND GRAHAM • VOL. 10, NO. 3 177
April 20, 1999.42,62 This was a complex incidentwith the threat of continued violence at the scene.Two students attacked their school using multiplehomemade bombs, incendiary devices, and auto-matic weapons. Many of the devices were designedto injure fleeing students and rescue personnel.63
The perpetrators also fired out a cafeteria window atparamedics attempting to rescue victims lying justoutside. Because of the circuitous route taken by thegunmen through the school, there was a great deal ofconfusion as to the number of perpetrators (as manyas 8 from initial reports) and their current locationinside the school. Because of the size of the schooland the difficulty in knowing how many assailantswere involved, initial medical care for some victimswas delayed for more than 3 hours while the schoolwas secured by SWAT teams.62
Planning considerations for scene control shouldalso include a universal identification (ID) system
for rescuers. Although time consuming, an IDsystem will help limit scene access to thoseindividuals involved in the rescue/recovery opera-tion. Shortly after the Oklahoma City bombing, theFederal Bureau of Investigation set up a photo IDsystem for rescue workers who needed access to thescene.37,60 The procedure was not consistentlyenforced in the beginning of the operation and ledto more individuals in the building without actualroles in the rescue or recovery proceedings.
Scene safety issues can also be a consequence ofnatural disasters or their unintended consequences,such as rising flood waters. When Hurricane Katrinaslammed into the Louisiana gulf coast on August 29,2005, it left 1836 dead and a large number of missingpersons, an untold number of which were children.Rescue workers were faced with multiple hazardsinvolving command and scene safety in the days andweeks after the storm. As the city disappeared under

178 VOL. 10, NO. 3 • PEDIATRIC MASS CASUALTY / LYLE, THOMPSON AND GRAHAM
water, multiple individuals who did not evacuatewere left stranded on rooftops for days, requiringwater rescue. These victims were stranded withlittle food or water, no working toilets, and no powerfor lights or air-conditioning for several days. Risingtide waters polluted with sewage and decayingbodies disrupted the freshwater supply lines andincreased the risk of dehydration and disease. It isestimated that 56 000 pregnant women and 75 000infants were affected by Hurricane Katrina. Disrup-tion in the supply of safe drinking water, food,crowded shelter conditions, and exposure to envir-onmental toxins put these vulnerable populations atrisk.64 Looting and violence among citizensstranded in their homes and at shelters increasedas police were outnumbered and overwhelmed.Until the arrival of the National Guard, the personalsafety of prehospital workers was frequently at riskfrom violence.65
Communication
Communication among responding providers isan essential part of the response at all MCEs.Multiagency responses can be especially proble-matic, with varying channel assignments andavailable radio frequencies between agencies.Unless a regional interagency communication planhas been developed and tested, there may not becommunication compatibility among those in-volved. At the Columbine scene, not all respondingunits had access to the Fire Emergency ResponseNetwork as had been previously assumed. The lackof frequency coordination between various respon-ders' radio systems created delays in allocation ofresources.62 In addition, numerous 911 cell phonecalls from students inside the school began toquickly overwhelm the telephone communicationsystem. Telephone system overload is common inMCEs. Another event that demonstrated the impor-tance of interagency and interoperable communi-cation capability was the Virginia Tech MCE.Medics from the scene reported several “deadzones” in Norris Hall dormitory, which resultedin “a tough time with radio communicationstraffic.” There was a significant degree of noiseand chatter on the EMS radio frequency, whichfurther complicated communication. A separatecommand frequency was available and was used,but information needed to be transmitted back tofirst-line responders on the EMS channel. Radiosused by other responding agencies consisted of acombination of very high frequency, ultra highfrequency, and hospital emergency ambulanceradio frequencies.66
Another significant communications gap was thelack of credible information available to give to areahospitals concerning the number of patients theymight receive. One hospital learned of the incidentonly when a call requesting a medical examiner atthe scene was received. In several instances, on-scene providers called hospitals or other providersdirectly instead of going through incident com-mand, thus increasing confusion. Upon review, thiswas determined to have occurred secondary to thelack of an Emergency Operations Center located atthe university proper.55 The lack of standardizedon-scene communications can lead to serioussafety issues for providers and a hamperedresponse for victims. Preplanning considerationsmust include interoperability of communicationservices between incident command, dispatch,providers, and area hospitals.
Triage
Mass casualty triage (MCT) was first describedand developed by British Naval surgeon JohnWilson. Wilson postulated that in order for medicalcare to be lifesaving in mass injury, it should beprovided to those most in need.67 Mass casualtytriage is intended to distinguish between thoserequiring immediate lifesaving care and those whocan receive delayed care. In an MCE, triage isessential because the need for care can easilyoverwhelm available resources. Mass casualty triagediffers from the triage processes normally per-formed in an emergency department. Most tradi-tional emergency department triage protocolsrequire several minutes per patient and take avariety of objective and subjective information intoaccount but are appropriate under normal stan-dards when the resources available meet or exceedthe needs of the patients presenting for care.
However, during an MCE, the triage objectiveschange.68,69 Mass casualty triage systems have beendeveloped to address situations in which thenumber of casualties is greater than the availableresources. In this paradigm shift, the prioritybecomes maximizing the number of lives saved.The focus changes from the needs of everyindividual patient to doing the best for the entiregroup of patients. Resources are allocated, andattention is directed to the most reasonably salvage-able patients and not necessarily to the mostcritically ill or injured. Immediate treatment isdirectly only to those for whom lifesaving proce-dures may make the difference. Everyone else hasdelayed treatment. The aim of MCT is to provide thegreatest good to the greatest number.
PEDIATRIC MASS CASUALTY / LYLE, THOMPSON AND GRAHAM • VOL. 10, NO. 3 179
Altered standards and focus of care in MCT areindeed a grim reality. Many medical ethicists havewritten about it, and most agree that the utilitarianrule is in play. Using limited resources to obtainthe greatest benefit, whether it is given to thosemost in need or not is the utilitarian concept usedin most Western MCT schemes.69,70
Mass casualty triage is performed only in the caseof a true MCE. There is no set number of victimsthat qualify a specific incident as an MCE. It isinstead a function of the resources available andthe severity of injuries of the victims. When thenumber of patients overwhelms the locally avail-able resources, either in the field or at the treat-ment center, it is generally considered a masscasualty situation.
Triage is a dynamic process. Primary triage is therapid patient assessment, assignment, and taggingusually done at the scene of an incident. Theseassignments can change during the secondary triageprocess. Secondary triage typically occurs at thehealth care facility where the patient is transported.There are often more resources available to thepatient by the time they reach secondary triage.
Primary MCT is performed by EMS and otherfirst responders at the scene. The goal of any MCTscheme is to assign the patient a triage categorybased on a rapid assessment of the severity oftheir injury and their physiologic parameters.71,72
Primary MCT should be accomplished veryquickly, requiring about 30 seconds per patient,and should be based solely on the patient'sphysiology. The goal of primary disaster triage isto assess how well the patient is able to use theirown resources to compensate for their injuries—itshould be as objective as possible. It also allowsthe field provider to determine which patients willbenefit the most from the expenditure of theirlimited resources.
Most MCT systems use 4 color-coded categories:red, yellow, green, and black. Patients categorized asred are believed to have immediate or life-threaten-ing injuries. Persons with these injuries are believedto be salvageable with immediate medical attention.Examples of these conditions include airwayobstruction, significant external hemorrhage,shock, sucking chest wounds, or burns to the faceand neck. The yellow category represents poten-tially serious injuries in patients who are stableenough to wait a short period for medical attention.Examples might include patients with an openthoracic wound, penetrating abdominal wound,severe eye injury, long-bone fractures, an avascularlimb, or significant burns other than to the faceor neck.
The green category represents patients withminor injuries, often termed “the walkingwounded.” These injuries can wait longer periodsfor treatment. Examples include minor lacerations,contusions, sprains, superficial burns, partial thick-ness burns, and ambulatory fractures.72
The black category in MCT algorithms representspatients who have either died or are expected to die.This includes patients that are alive but haveinjuries that are not compatible with survivalunder the current conditions. Assigning a patientwho is still alive to the black category requires aclear understanding of available resources andconditions. Examples include those with no vitalsigns but also those with signs of impending death,those who do not respond to airway positioning,multisystem trauma with hemodynamic instability,and massive head injury.73,74
Two common types of triage models used arethe sieve or sort methods. The sieve requiresrescuers to initiate little or no treatment andprimarily distribute those individuals into groups.This approach can lead to the overtriage ofnonwalking casualties (ie, simple foot fracture)and children (infants and toddlers) and theundertriage of individuals with life-threateninginjuries such as burns or head injuries.59
The sorting style triage tools are more timeconsuming and complex, for example, using amethod based on the revised trauma score.74 Thisapproach is hypothesized to undertriage casualtieswho are gravely injured but have stable vital signsdue to compensation.59 These systems are fre-quently not used for these reasons.
A number of MCT tools or protocols have beendeveloped. The START (simple triage and rapidtreatment) protocol was developed in California in1983 in response to a school bus accident.75 Itrelies on rapid assessment of ambulation, airway,circulation, and neurologic function. It is reportedthat START can be rapidly performed with adultvictims and can be readily taught to first respon-ders. The START triage protocol has been criti-cized for a lack of objective evidence of itseffectiveness, a deficiency of most MCT tools.76 In1996, Benson et al77 developed an extension of theSTART with the “secondary assessment of victimend point” protocol. In this scheme, disasterpatients are sorted into 3 categories: those whowill survive regardless, those who will die even withmaximal effort, and those who would benefit fromimmediate intervention.77 The “secondary assess-ment of victim end point” protocol is particularlyintended for situations in which transport todefinitive care may be substantially delayed. The

180 VOL. 10, NO. 3 • PEDIATRIC MASS CASUALTY / LYLE, THOMPSON AND GRAHAM
triage sieve protocol, used by the British militaryfor primary triage, uses the parameters assessed inthe START protocol, with the exception of mentalstatus.72 The French use a diagnosis-based MCTsystem, in which the triage officer makes a rapidassessment of field diagnosis and the patient iscategorized based on that assessment.68 The ItalianEMS system uses a protocol titled CESIRA (Cos-ciente, Emorrhagia, Shock, Insufficienza, Rotture,Altre), which triages patients into red, yellow, andgreen categories. Italian law prevents paramedicsfrom certifying death; thus, the protocol will notallow the use of a black category.68
Because many of the MCT protocols that havebeen developed are based on adults and there areclear anatomic, physiologic, and developmentaldifferences in children, there is a need for a reliablepediatric mass casualty tool. Figure 1 highlightssome of the many physiologic differences inchildren that make it difficult to categorize themusing the standard mass casualty tools. The mostimportant of these physiologic differences is thechild's amazing ability to compensate for mild-to-moderate injuries. Infants and children can increasetheir heart rate significantly, thereby maintainingtheir cardiac output in the early phases of shock.This can serve them well in terms of survivabilitybut makes appropriate triage difficult.
As previously discussed, maintenance of anadequate airway and appropriate oxygenation andventilation in a child is of paramount importance.Circulation may be maintained for a short time afterrespirations have ceased in a child. The child is stillsalvageable in this period. If a pediatric victim of anMCE is encountered by a triage officer during thistime when their respirations have ceased butcirculation is still intact, then that child's life maybe saved with a quick airway intervention.
The 3 objective and physiologic areas measuredand assessed in most mass casualty triage algo-rithms are respirations, perfusion, and mentalstatus. All 3 of these areas can be significantlydifferent at baseline in children vs adults. In a childwho is injured, these differences need to beappreciated when assigning a triage category.Heart rate and respiratory rate vary across thepediatric age spectrum. Capillary refill time inchildren may be effected by ambient temperature,and thus may not be reliable in austere conditions.78
Any degree of hypothermia can cause a significantdelay in capillary refill, which may not necessarilyreflect a shock state in a child. Many children arenot developmentally capable of following commandsat a baseline, so assessing their mental status bytheir ability to follow commands is not a reliable
indicator of central nervous system function. Mostchildren are also developmentally reliant on adultsand therefore may not independently self-evacuateto a safe area. Even if they are a child of ambulatoryage, they will wait for their parent before moving tothe safe zone.
First responders and EMS providers admit theyoften overtriage a child based solely on their age,even in day-to-day emergency care. Few EMSagencies have specific provisions for children intheir MCE response plans.8 Most EMS agencies donot interact with local schools or daycare centers topractice mass casualty incident drills. In a nationalsurvey, fewer than 20% of EMS agencies were foundto use a pediatric-specific triage protocol, and lessthan 15% involved a pediatrician in their medicalcontrol.8 The presence of an objective pediatrictriage tool would serve to greatly ease the emotionalstress upon the triage officer in this situation.
In answer to these needs, pediatric-specific MCTprotocols have been devised. Perhaps the mostwell known and widely adopted is the JumpSTARTalgorithm authored by Romig in 2002. Jump-START uses the existing START algorithm butincorporates pediatric physiologic parameters.79 Itallows for an additional intervention in the apneicchild who is found to have a pulse, 5 rescuebreaths, given the significance of airway interven-tion for such children.
The JumpSTART algorithm, combined withSTART, is depicted in Figure 2. It is designed tobe used on any victim who appears to be less than8 years of age (with START used for olderchildren). The JumpSTART algorithm uses breath-ing, circulation, and mental status as physiologicparameters, just as in START. The airway is firstassessed. If it is not functional, then the airwayshould be positioned. If this results in sponta-neous resumption of respirations, then the patientis tagged red. If the child remains apneic afterpositioning the airway, then the pulse is assessed.If there is no palpable pulse, then the patient istagged black. If they still have a palpable pulse butremain apneic, then 5 rescue breaths are admi-nistered by the triage officer. If the child remainsapneic after this intervention, then they aretagged black and considered deceased. If the5 rescue breaths results in spontaneous resump-tion of respirations, then they are tagged red.This delivery of 5 rescue breaths is termedthe “JumpSTART.”
The JumpSTART algorithm allows for the age-dependant physiologic parameters of a child interms of respiratory rate, circulation, and mentalstatus assessment.
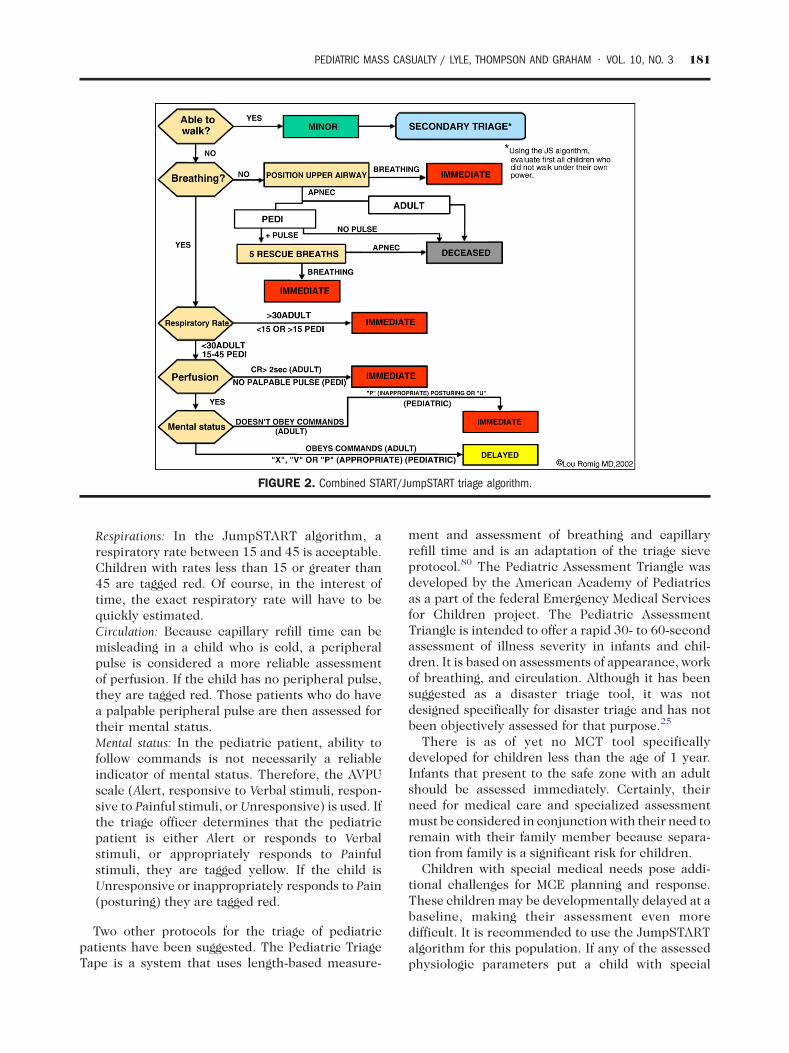
FIGURE 2. Combined START/JumpSTART triage algorithm.
PEDIATRIC MASS CASUALTY / LYLE, THOMPSON AND GRAHAM • VOL. 10, NO. 3 181
Respirations: In the JumpSTART algorithm, arespiratory rate between 15 and 45 is acceptable.Children with rates less than 15 or greater than45 are tagged red. Of course, in the interest oftime, the exact respiratory rate will have to bequickly estimated.Circulation: Because capillary refill time can bemisleading in a child who is cold, a peripheralpulse is considered a more reliable assessmentof perfusion. If the child has no peripheral pulse,they are tagged red. Those patients who do havea palpable peripheral pulse are then assessed fortheir mental status.Mental status: In the pediatric patient, ability tofollow commands is not necessarily a reliableindicator of mental status. Therefore, the AVPUscale (Alert, responsive to Verbal stimuli, respon-sive to Painful stimuli, or Unresponsive) is used. Ifthe triage officer determines that the pediatricpatient is either Alert or responds to Verbalstimuli, or appropriately responds to Painfulstimuli, they are tagged yellow. If the child isUnresponsive or inappropriately responds to Pain(posturing) they are tagged red.
Two other protocols for the triage of pediatricpatients have been suggested. The Pediatric TriageTape is a system that uses length-based measure-
ment and assessment of breathing and capillaryrefill time and is an adaptation of the triage sieveprotocol.80 The Pediatric Assessment Triangle wasdeveloped by the American Academy of Pediatricsas a part of the federal Emergency Medical Servicesfor Children project. The Pediatric AssessmentTriangle is intended to offer a rapid 30- to 60-secondassessment of illness severity in infants and chil-dren. It is based on assessments of appearance, workof breathing, and circulation. Although it has beensuggested as a disaster triage tool, it was notdesigned specifically for disaster triage and has notbeen objectively assessed for that purpose.25
There is as of yet no MCT tool specificallydeveloped for children less than the age of 1 year.Infants that present to the safe zone with an adultshould be assessed immediately. Certainly, theirneed for medical care and specialized assessmentmust be considered in conjunction with their need toremain with their family member because separa-tion from family is a significant risk for children.
Children with special medical needs pose addi-tional challenges for MCE planning and response.These children may be developmentally delayed at abaseline, making their assessment even moredifficult. It is recommended to use the JumpSTARTalgorithm for this population. If any of the assessedphysiologic parameters put a child with special

182 VOL. 10, NO. 3 • PEDIATRIC MASS CASUALTY / LYLE, THOMPSON AND GRAHAM
needs into the immediate category, then they shouldbe tagged red. If at the completion of the Jump-START triage algorithm they meet criteria for ayellow tag, then the triage officer must look forsignificant external injuries. They should be taggedyellow if they have significant external signs ofinjury such as deep penetrating wounds, severebleeding, severe burns, or an amputation. If theymeet criteria for a yellow tag but have no significantexternal injury, then they are tagged green.
All MCT tools have limitations. None have beenwell validated by outcomes data; this makes it verydifficult to endorse any single tool.68,69,72,76 Anothersignificant limitation of all MCT algorithms is thatthey are not as simple as they appear. They requirerepetitive practice. Even for providers who are usedto doing standard triage under normal standards ofcare, MCT can be very difficult. It requires aconscious shift in thinking and priorities. Perhapsthe most obvious limitation of pediatric-specificalgorithms is that they require diligent attention todetail. Most EMS providers do not get enough hands-on experience with pediatric victims to remember adisaster triage algorithm instinctively—it requires agreat amount of training and practice to perfect.
Perhaps the most significant issue with currentMCTsystems is that there is considerable variabilityin the type of tool used. There is presently nonational standard disaster triage protocol. Differentjurisdictions use different protocols; yet masscasualty patients frequently cross jurisdictionallines. A common language or universally acceptedtool for mass casualties would serve our country wellin the face of large-scale disasters that requirecommunication and cooperation between multiplestate, local, and federal agencies.
To address some of these limitations, a consensusstatement has recently been endorsed by multipleprofessional organizations. In July of 2008, a panelof experts issued a proposition entitled SALT (Sort,Assess, Life-saving interventions, and Transport/Treatment), which is intended to simplify triage ofall victims, ensure that lifesaving interventions areprovided before a severity category is assigned, andhopefully provide some uniformity among the toolscurrently practiced.69 It attempts to incorporate themost effective parts of all currently available toolsand could potentially be taught to those trained inother methods. SALT offers 5 levels of severity. Inaddition to the red, yellow, green, and blackcategories seen in most 4-level systems, SALTallowsfor a gray category. Patients in the gray categoryhave severe injuries or signs of impending death butare not dead at the time of primary triage. It mayserve the triage officer well to be able to easily
identify those patients who deserve and wouldbenefit from more resources as they becomeavailable. SALT is intended to be used for bothpediatric and adult victims.
Treatment, Transport, and Disposition
The limits of pediatric surge capacity andcapabilities as previously discussed are likely to bean important issue in determining the transport ofpediatric victims to definitive care. Adult facilitiesmay need to accept low-acuity pediatric patients;although this may more readily overwhelm thefacility than the same number of adult patients dueto scarce pediatric supplies or limited pediatric careexperience. Tertiary pediatric facilities may be ableto provide receiving facilities with needed resourcessuch as anesthesia and pediatric resuscitationteams. Local EMS services need to be aware of thepediatric surge capabilities in the region so thatchildren can be taken to the facilities best capable ofcaring for them without overwhelming a singlehospital. Pediatric patients requiring tertiary caremay require transports of long distances to reachspecialized facilities with available bed capacity.Plans for the care of children in MCEs shouldinclude provisions for long-distance transport.81 Inaddition, pediatric planning should include provi-sions for mental health services because childrenare particularly vulnerable. Understanding themental health and social work capabilities in aparticular region is an important part of developinga community or regional disaster plan.
Some of the care for pediatric patients in adisaster situation may occur in a DMAT field clinic.DMATs are mobilized by the federal government toassist local entities in a large-scale disaster.Currently, there are no universal requirements forpediatric personnel, training, medication, or equip-ment within DMATs. There are presently 2 pedia-tric specialty DMATs.82 Assessments of pediatricreadiness have called for the developmentof additional pediatric capability in the presentDMAT system.1
Where Do We Go From Here?
The outcomes for pediatric victims of a disastercan likely best be improved by focusing on the day-to-day readiness of our emergency care system forthe management of pediatric victims. Many EMSproviders openly admit to being uncomfortable withpediatric patients in their daily practice. Increasedfocus on education and training of EMS providers inthe emergency care of children will pay dividends in
PEDIATRIC MASS CASUALTY / LYLE, THOMPSON AND GRAHAM • VOL. 10, NO. 3 183
better care for day-to-day concerns and betterdisaster preparedness.
First responders and EMS providers need to haveaccess to the appropriate pediatric equipment aswell as the opportunity to practice using thatequipment on a frequent basis. There are sometools available to the EMS provider, such as length-based resuscitation tapes that make the dosing offluids and resuscitation medications a simpler task.This equipment is not always available to EMSproviders and does require some familiarity toenable effective use.
Some treatment adjuncts, such as intraosseousneedles, can be lifesaving for a pediatric patient. Theuse of new drills for intraosseous needle placementmay make that procedure more successful but,again, requires some training of the EMS profes-sional and availability of the correct equipment.
Another opportunity for improvement is in mak-ing decontamination facilities more child and familyfriendly. These facilities should have warm wateravailable whenever possible and have a plan forchildren who require some adult supervision inthe process.
A nationally standardized disaster triage protocolwould provide the advantage of cross jurisdictionalcompatibility. In addition, research should focus onthe validation of disaster triage protocols to ensurethat they accomplish their stated purpose.
Perhaps the greatest opportunity for improve-ment in the prehospital care of pediatric patients isin interagency planning and collaboration, as mightbe achieved in more frequent and effective commu-nity-wide disaster drills. Very few EMS providersparticipate in drills with local schools or daycarecenters. Community-wide disaster drills often donot include pediatric victims in the scenario.8
Encouraging community-wide drills that wouldallow first responders and EMS providers to interactwith children would increase their comfort level incaring for them and allow the practice of pediatric-specific triage algorithms. Such a drill would alsoencourage better communication between thedifferent agencies involved in a mass casualtyincident and typically generates a productivedialogue. This kind of dialogue is the best forumfor communities to find solutions to the many taxingissues of pediatric care in MCEs.
REFERENCES1. Gnauck KA, Nufer KE, LaValley JM, et al. Do pediatric and
adult disaster victims differ? A descriptive analysis of clinicalencounters from four natural disaster DMAT deployments.Prehosp Disaster Med 2007;22:67-73.
2. Becker, Bruce M. In: Ciottone G, Anderson P, Auf DerHeide E, et al, editors. “Children and Disaster.” Disastermedicine. 3rd ed. Philadelphia, PA: Elsevier Mosby; 2006.p. 51-8.
3. Graham CJ, Stuemky J, Lera TA. Emergency medicalservices preparedness for pediatric emergencies. PediatrEmerg Care 1993;9:329-31.
4. Zaritsky A, French JP, Schafermeyer R, et al. A statewideevaluation of pediatric prehospital and hospital emergencyservices. Arch Pediatr Adolesc Med 1994;148:76-81.
5. Youngquist ST, Henderson DP, Gausche-Hill M, et al.Paramedic self-efficacy and skill retention in pediatric airwaymanagement. Acad Emerg Med 2008;15:1295-303.
6. Mace SE, Bern AI. Needs assessment: are Disaster MedicalAssistance Teams up to the challenge of a pediatric disaster?Am J Emerg Med 2007;25:762-9.
7. Stankovic C, Mahajan P, Ye H, et al. Bioterrorism: evaluatingthe preparedness of pediatricians in Michigan. Pediatr EmergCare 2009;25:88-92.
8. Shirm S, Liggin R, Dick R, et al. Prehospital preparednessfor pediatric mass casualty events. Pediatrics 2007;120:e756-61.
9. Markenson D, Redlener I. Pediatric terrorism preparednessnational guidelines and recommendations: findings of anevidence-based consensus process. Biosecur Bioterror 2004;2:301-19.
10. Cicero MX, Baum CR. Pediatric disaster preparedness: bestplanning for the worst case scenario. Pediatr Emerg Care2008;24:478-82.
11. Carley SD, Mackway-Jones K, Donnan S. Delphi study intoplanning for care of children in major incidents. Arch DisChild 1999;80:406-9.
12. Chung S, Shannon M. Reuniting children with their familiesduring disasters: a proposed plan for greater success. Am JDisaster Med 2007;2:113-7.
13. Brandenburg MA, Watkins SM, Brandenburg KL, et al.Operation Child-ID: reunifying children with their legalguardians after Hurricane Katrina. Disasters 2007;31:277-87.
14. Brandenburg MA, Arneson WL. Pediatric disaster response indeveloped countries: ten guiding principles. Am J DisasterMed 2007;2:151-62.
15. Gausche-Hill M. Ensuring quality in prehospital airwaymanagement. Curr Opin Anaesthesiol 2003;16:173-81.
16. Aharonson-Daniel L, Waisman Y, Dannon YL, et al. Epide-miology of terror-related versus non–terror-related traumaticinjury in children. Pediatrics 2003;112:e280.
17. Quintana DA, Parker JR, Jordan FB, et al. The spectrum ofpediatric injuries after a bomb blast. J Pediatr Surg 1997;32:307-10.
18. Bernardo LM. Pediatric implications in bioterrorism part 1:physiological and psychosocial differences. Int J Trauma Nurs2001;7:14-6.
19. Allen GM, Parrillo SJ, Will J, et al. Principles of disasterplanning for the pediatric population. Prehosp Disaster Med2007;22(6):537-40.
20. Freyberg CW, Arguilla B, Fertel BS, et al. Disaster prepared-ness: hospital decontamination and the pediatric patient:guidelines for hospitals and emergency planners. PrehospDisaster Med 2008;23:166-73.
21. Teran-Maciver M, Larson K. Implications of chemicalbiological terrorist events for children and pregnantwomen. MCN Am J Matern Child Nurs 2008;33:224-32.
22. Committee on Environmental Health and Committee onInfectious Disease. Chemical-biological terrorism and itsimpact on children. Pediatrics 2006;118:1267-78.

184 VOL. 10, NO. 3 • PEDIATRIC MASS CASUALTY / LYLE, THOMPSON AND GRAHAM
23. Skorga P, Persell DJ, Arangie P, et al. Caring for victims ofnuclear and radiological terrorism. Nurse Pract 2003;28:24-41.
24. American Academy of Pediatrics. Committee on Environ-mental Health. Radiation disasters and children. Pediatrics2003;111(6 Pt 1):1455-66.
25. Hohenhaus SM. Practical considerations for providing pedia-tric care in a mass casualty incident. Nurs Clin N Am 2005;40:523-33.
26. Middleton KR, Burt CW. Availability of pediatric services andequipment in emergency departments: United States, 2002-03. Adv Data 2006;367:1-16.
27. Gausche-Hill M, Schmitz C, Lewis RJ. Pediatric preparednessof U.S. emergency departments: a 2003 survey. Pediatrics2007;120:1229-37.
28. Cyr C. Multivictim emergency care: a case study oforganophosphate poisoning in 67 children. J Emerg Nurse1988;14:277.
29. Van Amerongen RH, Fine JS, Talbert JL. The Avianca planecrash: an emergency medical system's response to pediatricsurvivors of the disaster. Pediatrics 1993;92:105-10.
30. Vukmir RB, Paris PM. The three rivers regatta incident: anEMS perspective. Am J Emerg Med 1991;81:64-71.
31. Quinn B, Baker R, Pratt J. Hurricane Andrew and apediatric emergency department. Ann Emerg Med 1994;23:737-41.
32. McNabb SJN, Kelso KY, Wilson SA, et al. Hurricane Andrew–related injuries and illnesses, Louisiana, 1992. Southern MedJ 1995;88:615-8.
33. Ammerman NT. Report to the Justice and Treasury Depart-ments regarding law enforcement interaction with theBranch Davidians in Waco, Texas Recommendations ofExperts for Improvements in Federal Law EnforcementAfter Waco. Washington (DC): U.S. Department of Justiceand U.S. Department of the Treasury; 1993.
34. Wass AR, Williams MJ, Gibson MT. A review of the manage-ment of a major incident involving predominantly pediatriccasualties. Injury 1994;25:371-4.
35. Peek-Asa C, Kraus JF, Bourque LB, et al. Fatal andhospitalized injuries resulting from the 1994 Northridgeearthquake. Int J Epidemiol 1998;27:459-65.
36. Okamura T, Takasu N, Ishimatsu S, et al. Report on 640victims of the Tokyo subway sarin attack. Ann Emerg Med1996;28:129-35.
37. Alfred P. The City of Oklahoma City. Murrah Federal Buildingbombing April 19, 1995 final report. Stillwater, OK: FireProtection Publications; 1996.
38. Sampson P, Crow A. Dunblane: our year of tears. Edinburgh:Mainstream Publishing Co. Ltd.; 1997.
39. Carley SD, Mackway-Jones K, Donnan S. Major incidents inBritain over the last 28 years: the case for centralisedreporting of major incidents. J Epidemiol Community Health1998;52:392-8.
40. Perry H, Wright R, Shannon M, et al. Baclofen overdose: drugexperimentation in a group of adolescents. Pediatrics 1998;101:1045-8.
41. Stolinsky DC, Barham M, Needles CF, et al. Private arsenalsand public peril. N Engl J Med 1998;339:565-6.
42. Nordberg M. When kids kill: Columbine High Schoolshooting. Emerg Med Serv 1999;28:38-50.
43. Fairbrother G, Stuber J, Galea S, et al. Unmet need forcounseling services by children in New York City after theSeptember 11 attacks on the World Trade Center: implica-tions for pediatricians. Pediatrics 2004;113:1367-74.
44. Brackbill RM, Thorpe LE, DiGrande L, et al. Surveillance forWorld Trade Center disaster health effects among survivors of
collapsed and damaged buildings. MMWR SurveillanceSummaries, April 7 2006;55(SS02):1-18.
45. BBCWorld News, 18 dead in German school shooting, Friday,26 April, 2002. Available at: http://news.bbc.co.uk/2/hi/europe/1952869.stm.
46. Centers for Disease Control. Rapid community health andneeds assessments after Hurricane Isabel and Charley—North Carolina 2003-2004. MMWR 2004;53:840-2.
47. Varia M, Wilson S, Sarwal S. Investigation of a nosocomialoutbreak of severe acute respiratory syndrome (SARS) inToronto, Canada. Canadian Med J 2003;169:65-9.
48. Poutanen S, Low D, Henry B, et al. Identification of severeacute respiratory syndrome in Canada. N Engl J Med 2003;348:1995-2005.
49. Stewart S. Tropical Cyclone Report—Hurricane Ivan 2-24 September 2004. National Hurricane Center, Decem-ber 16, 2004. Available at: http://www.nhc.noaa.gov/pdf/TCR-AL092004_Ivan.pdf.
50. Thomas DE, Gordon ST, Melton JA, et al. Pediatricians'experiences 80 miles up the river: Baton Rouge pediatricians'experiences meeting the health needs of evacuated children.Pediatrics 2006;117:s396-s401.
51. Timm N, Reeves S. A mass casualty incident involvingchildren and chemical decontamination. Disast ManagResponse 2007;5:49-55.
52. BBC World News. US school siege ends in bloodshed,September 28, 2006. Available at: http://news.bbc.co.uk/2/hi/americas/5387062.stm.
53. Ressel R, Reihart M, Brown S, et al. West Nickel Mines schoolshooting—how a rural MCI was successfully managed. JEMS2008;33:48-56.
54. Raphael Cohen-Almagor R, Haleva-Amir S. Bloody wednes-day in Dawson College - the Story of Kimveer Gill, or whyshould we monitor certain websites to prevent murder. StudEthics Law Technol 2008;2:5-8.
55. The Commonwealth of Virginia. Mass shootings atVirginia Tech: report of the Virginia Tech Review Panel;2007. Richmond, VA. Available at: http://www.governor.virginia.gov/TempContent/techPanelReport.cfm.
56. IBN Live Network News. Death toll in Hyderabad serial blastsrises to 44, August 25, 2007. Available at: http://ibnlive.in.com/news/death-toll-in-hyderabad-serial-blasts-rises-to-41/47450-3.html.
57. Beven JL, Kimberlain TB. National Hurricane Center,Tropical Cyclone Report—Hurricane Gustav (AL072008),25 August–4 September 2008 January 22, 2009. Available at:http://www.nhc.noaa.gov/pdf/TCR-AL072008_Gustav.pdf.
58. Berg R. National Hurricane Center, Tropical Cyclone Report—Hurricane Ike (AL092008), 1-14 September 2008, Jan-uary 23, 2009. Available at: http://www.nhc.noaa.gov/pdf/TCR-AL092008_Ike.pdf.
59. Castle N. Triage and transport decisions after mass casualtyincidents. Emerg Nurse 2006;14:22-5.
60. Maningas PA, Robison M, Mallonee S. The EMS response tothe Oklahoma City bombing. Prehosp Disaster Med 1997;12:80-5.
61. Cook L. The World Trade Center attack: the paramedicresponse: an insider's view. Crit Care 2001;5:301-3.
62. State of Colorado Columbine Review Commission. Thereport of Governor Bill Owen's Columbine Review Commis-sion. Denver: State of Colorado; 2001.
63. Mell H, Sztajnkrycer MEMS. Response to Columbine. LessonsLearned. Internet J Rescue Disaster Med 2005;5:1.
64. Callaghan WM, Rasmussen SA, Jamieson DJ, et al. Healthconcerns of women and infants in times of natural disasters:

PEDIATRIC MASS CASUALTY / LYLE, THOMPSON AND GRAHAM • VOL. 10, NO. 3 185
lessons learned from Hurricane Katrina. Matern Child HealthJ 2007;11:307-11.
65. McCain C, Davis R. Devastation in Katrina's wake. JEMS2005;30:20-6.
66. Armstrong JH, Frykberg ER. Lessons from the response to theVirginia Tech shootings. Disaster Med Pub Health Prep 2007;1(1 Suppl):S7-S8.
67. Sztajnkrycer MD, Madsen BE, Alejandro BA. Unstable ethicalplateaus and disaster triage. Emerg Med Clin North Am 2006;24:749-68.
68. Cone DC, Koenig KL. Mass casualty triage in the chemical,biological, radiological, or nuclear environment. Eur J EmergMed 2005;12:287-302.
69. Lerner EB, Schwartz RB, Coule PL, et al. Mass casualty triage:an evaluation of the data and development of a proposednational guideline. Disaster Med Pub Health Prep 2008;2:S25-S34.
70. Holt GR. Making difficult ethical decisions in patient careduring natural disasters and other mass casualty events.Otolaryngol Head Neck Surg 2008;139:181-6.
71. Veatch RM. Disaster preparedness and triage. Mt Sinai J Med2005;72:236-41.
72. Garner A, Lee A, Harrison K, et al. Comparative analysis ofmultiple-casualty incident triage algorithms. Ann Emerg Med2001;38:541-8.
73. Reisner A. Triage. In: Ciottone GR, editor. Disaster medicine.3rd ed. Philadelphia, PA: Elsevier Mosby; 2006. p. 283-9.
74. Hodgetts T, Mackway-Jones K. Major incident medicalmanagement and support: the practical approach at thescene. 2nd ed. London: BMJ Books; 2002.
75. Super G, Groth S, Hook R, et al. START: simple triage andrapid treatment plan. Newport Beach, CA: Hoag MemorialPresbyterian Hospital; 1994.
76. Kahn CA, Schultz CH, Miller KT, et al. Does START triagework? An outcomes assessment after a disaster. Ann EmergMed 2009 [Epub ahead of print].
77. Benson M, Koenig KL, Schultz CH. Disaster triage: START,then SAVE—a new method of dynamic triage for victims of acatastrophic earthquake. Prehosp Disaster Med 1996;11:117-24.
78. Gorelick MH, Shaw KN, Baker MD. Effect of ambienttemperature on capillary refill time in healthy children.Pediatrics 1993;92:699-702.
79. Romig LE. Pediatric triage—a system to JumpSTART yourtriage of young patients at MCIs. JEMS 2002;37:52-63.
80. Hodgetts T, Hall J, Maconochie I, et al. Paediatric triage tape.Prehosp Immediate Care 1998;2:155-9.
81. Baldwin S, Robinson A, Barlow P, et al. Moving hospitalizedchildren all over the southeast: interstate transfer ofpediatric patients during Hurricane Katrina. Pediatrics2006;117(5 pt 3):s416-20.
82. Weiner DL, Manzi SF, Waltzman ML, et al. The nationaldisaster medical system: a pediatric perspective. Pediatrics2006;117:S405-11.