-
7/23/2019 Pediatric Nephrotic Nephritic Syndromes
1/18
1
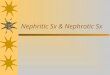
THE GLOMERULAR FILTRATION BARRIER
The human kidney is a complex and vital organ
system that even in full term infants, the normal renal
function is incomplete until about 2 years of age. It
consist
of about 1 million nephrons which at the tip is composed of
the glomerulus. In the glomerulus, blood from the afferent
arteriole is circulated in the glomerular capillaries which
becomes the source of the filtrate into the Bowmans space.
It is taken away from the Bowmans capsule via the
efferentarterioles. Parietal epithelial cells line the Bowmans
capsule.
The glomerular filtration barrier consist of the
podocyte, glomerular basement membrane, and the
glomerular capillary. Podocytes, or visceral epithelial cells,
separate the capillaries and the urinary space.
They have cellular extensions called foot processes, which
interdigitate to form slit diaphragms. The
glomerular basement membrane (GBM) is a trilaminar (lamina rara
externa, lamina densa, lamina rara
interna) structure beneath the podocytes. It is mainly made up
of type IV collagen, laminin, and heparin
sulfate proteoglycans. Found beneath the GBM, the endothelial
layer contains pores called endothelial
fenestrations.
The structure and the composition of the glomerular basement
allows it to have size, shape, and
charge selectivity. Size and shape selectivity are determined by
the 50100 nm diameter pores in the
endothelial layer, the ~40nm slit diaphragm distance, and the
network of proteins in the GBM. Charge
selectivity is determined by the negatively charged
sialoglycoproteins in the luminal aspect of the
podocyte membrane and the slit diaphragm. The negatively charged
glycocalyx lining the endothelium
also confers a negative charge to the structure. The properties
of the glomerular filtration barrier allows
it to produce an ultrafiltrate, which is cell free and contains
all of the substances in plasma (electrolytes,
glucose, phosphate, urea, creatinine, peptides, low
molecular weight proteins) except proteins having a
molecular weight of 68 kd (such as albumin and globulins).
Normally only a few red blood cells (RBCs) may be passed
out in the urine [
-
7/23/2019 Pediatric Nephrotic Nephritic Syndromes
2/18
2
HEMATURIA AND PROTEINURIA
Hematuria and proteinuria are common manifestations of
glomerular diseases. Hematuria isdefined as the presence of at
least 5 RBCs per microliter of urine or per high power field (hpf)
in a spun
urine sample (although different sources will vary from 2 12
RBCs/hpf in a spun freshly voided urine) .
The etiology of which must first be narrowed down to either from
the upper or from the lower urinary
tract. Hematuria form the glomerulus is usually described as
brown, cola or tea-colored, or burgundy urine
with proteinuria >100 mg/dL via dipstick and urinary
microscopic findings of RBC casts, and deformed or
dysmorphic urinary RBCs (particularly acanthocytes). Gross
hematuria is the term used when evidence of
blood in the urine is visible to the naked eye. Persistent
microscopic hematuria is hematuria demonstrated
via 23 urinalysis over a 23 week period. Urinary tract infection
is the most common cause of hematuria
but in some it may be associated with more serious diseases such
as glomerulonephritis. Proteinuria
should also be quantified in all patients with hematuria.
Proteinuria could either be glomerular proteinuria, tubular
proteinuria, or overflow proteinuria.
Glomerular proteinuria can be detected using the dipstick
method. Urine protein electrophoresis will
show that the albumin the dominant fraction; the same as with
the serum analysis. The normal rate of
protein excretion in the urine is less than 4 mg/m2/h or less
than 150mg/1.73m2/day during childhood.
Abnormal proteinuria is defined as 4 to 40 mg/m2/h. Nephrotic
range proteinuria is when protein
excretion exceeds 40 mg/m2/h. Excretion of protein in the urine
however varies in different age groups
(Table 9.5 from Clinical Pediatric Nephrology).
-
7/23/2019 Pediatric Nephrotic Nephritic Syndromes
3/18
3
Often hematuria and proteinuria are used
to differentiate between nephrotic and nephritic
glomerular syndromes; however the symptoms of
nephrotic syndromes and nephritic syndromes
may overlap and both may occur at the same
time.
NEPHROTIC & NEPHRITIC SYNDROMES
Nephrotic and nephritic syndromes differ in the way fluid is
handled by the body. In nephrotic
syndrome, the excretion of protein depletes the albumin in the
intravascular space leading to decrease in
oncotic pressure and subsequently fluid extravasation. In
nephritic syndromes, the decrease in glomerular
filtration rate causes volume expansion in both intravascular
space and extracellular space.
The incidence of nephrotic and nephritic syndromes vary in
different age groups. According to the
Department of Health, nephrotic and nephritic syndromes place
10thin the leading causes of mortality for
children 10 to 14 years of age in 2010.
NEPHROTIC SYNDROMES
Nephrotic syndrome is characterized by massive proteinuria,
hypoalbuminemia, and edema,
although additional clinical features such as hyperlipidemia are
usually also present. Children with this
condition often present with sudden development of periorbital
swelling, with or without generalized
edema.
-
7/23/2019 Pediatric Nephrotic Nephritic Syndromes
4/18
4
Epidemiology
The annual incidence of nephrotic syndrome ranges from 2 - 7 new
cases per 100 000 children
and the prevalence is about 16 cases per 100 000 children, or 1
in 6000 children. Boys are about 2x as
likely as girls to develop nephrotic syndrome during the younger
years but nearing adolescence and
adulthood, the disparity in incidence disappears. The
presentation of nephrotic syndrome also differs
among different races. Idiopathic nephrotic syndrome is 6x more
common among Asian children than inCaucasian children in the United
Kingdom, with an incidence of 16 new cases per 100 000 children
per
year. In a study involving children with nephrotic syndrome,
African-Americans (47%) have more chance
of having a less favorable diagnosis than Caucasians (18%) or
Hispanics (11%). In a community with various
ethnicities such as in Texas, the racial distribution of
nephrotic syndrome was 49% Caucasian, 20% African-
American, and 24% Hispanics.
The peak age of presentation is 2 years but 70-80% of nephrotic
syndromes occur in children less
than 6 years old.
Etiology
Primary or idiopathic nephrotic syndrome (INS) is the most
common form of nephrotic syndromein children. Glomerular lesions
associated with idiopathic nephrotic syndrome include minimal
change
disease (MNCS), focal segmental glomerulosclerosis (FSGS),
membranoproliferative glomerulonephritis,
membranous nephropathy, and diffuse mesangial proliferation.
Nephrotic syndrome may also be secondary to systemic diseases
such as systemic lupus
erythematosus, Henoch-Schonlein purpura, malignancy (lymphoma
and leukemia), and infections
(hepatitis, HIV, and malaria).
Hereditary nephrotic syndromes also occur in patients possessing
mutations in genes encoding
critical proteins in the glomerular filtration barrier.
Nephrotic syndrome appearing in the first 3 months of age are
referred to as congenital nephroticsyndrome (CNS). These are mostly
due to genetic causes especially those involved in encoding
nephrin
and podocin. In one series mutations in the podocin gene (NPHS2)
were shown to be responsible for up
to 40% of all cases of nephrotic syndrome occurring in the first
3 months of life. Multi-system congenital
disorders and congenital infections, such as those from syphilis
and cytomegalovirus, can also present as
CNS.
-
7/23/2019 Pediatric Nephrotic Nephritic Syndromes
5/18
5
From 3 months to 1 year old, 40% are due to genetic causes.
Beyond 1 year, INS predominates,
wherein MNCS comprise 80% of the cases. For children more than
10 years old, the proportion of
secondary nephrotic cases
increases.
Pathogenesis
The central abnormality in all cases of nephrotic syndrome is
the development of massive
proteinuria. Evidences from literature show that nephrotic
syndrome may be a consequence of a primary
glomerular defect, circulating factors, or an immunological
abnormality.
Primary glomerular defects have been observed in histologic
samples in nephrotic syndrome and
these include: is loss of negative charge of the GBM; swelling,
retraction, and effacement (spreading) of
the podocyte distal foot processes; vacuole formation,
occurrence of occluding junctions, displacement
of slit diaphragms; and detachment of podocytes from the
GBM.
Circulating factors or soluble mediators that may alter the
capillary wall permeability have been
implicated in the development of nephrotic syndrome as evidenced
by (1) development of nephrotic
syndrome in newborn babies born to mothers with nephrotic
syndrome (2) Marked reduction of
proteinuria following treatment with protein A immunoadsorption
(3) recurrence of FSGS in transplanted
kidneys in patients with primary FSGS and (4) induction of
enhanced glomerular permeability inexperimental animals injected
with serum from patients with FSGS.
Immunological abnormality leading to dysregulation of T cell
function is evidenced by (1)
responsiveness of most forms of primary nephrotic syndrome to
corticosteroids, alkylating agents,
calcineurin inhibitors (2) Induction of remission of nephrotic
syndrome following infections with measles
and malaria (3) identification of MCNS as a paraneoplastic
manifestation of Hodgkins disease and other
lymphoreticular malignancies
-
7/23/2019 Pediatric Nephrotic Nephritic Syndromes
6/18
6
Pathophysiology
In nephrotic syndrome, urinary excretion of albumin produces a
hypoalbuminemic state which
causes sodium and fluid retention. The bodys compensatory
response of fluid and sodium accumulation
in the extracellular space or interstitial space leads to facial
or generalized edema. The movement of fluidcan be explained by the
Starling equation which shows that a decrease in oncotic pressure
would result
to unopposed capillary hydrostatic pressure favoring fluid
extravasation and edema.
The decrease in pressure distention will be detected by
mechanoreceptors in the carotid sinus,
aortic arch, left ventricle, and afferent arterioles in the
glomeruli. This produces (1) increased sympathetic
nervous system (SNS) outflow from the central nervous system,
(2) activation of the Renin-Angiotensin-
Aldosterone System (RAAS), and (3) nonosmotic release of
Arginine Vasopressin (AVP) from the
hypothalamus. These 3 changes result in peripheral
vasoconstriction (increased SNS and angiotensin II),
sodium retention (increased SNS, angiotensin II, and
aldosterone), and water retention.
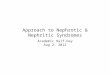
The above mentioned process is called the underfill hypothesis.
Even though the above
mentioned process is the more famous one, the overfill
hypothesis also gains support from chronically
nephrotic patients and some animal models. The overfill
hypothesis states that there is hypervolemia
intravascularly in contrast with hypovolemia in the underfill
hypothesis.
Underfill hypothesis Overfill hypothesis
-
7/23/2019 Pediatric Nephrotic Nephritic Syndromes
7/18
7
Clinical Features
Nephrotic syndrome is usually diagnosed by nephrotic range
proteinuria with a triad of clinical
findings associated with large urinary losses of protein.
Nephrotic proteinuria refers to urinary protein
excretion greater than 40mg/m2/hr or urinary protein-creatinine
ration (UPr/Cr) greater than 2. The triad
of clinical findings include (1) hypoalbuminemia (serum albumin
250mg/dL), and (3) edema.
A child with nephrotic syndrome will typically present with
periorbital or generalized edema.
Edema is clinically detectable when the fluid retention exceeds
3-5% of the body weight. It is starts in the
periorbital region then to the dependent portions of the body.
It is usually pitting, soft, and found on the
dependent portions of the body. Some children may have abdominal
distention secondary to ascites or
anterior wall edema. Severe distention may also cause discomfort
or pain; wherein bacterial peritonitis
should be ruled out. Gut edema and gut ischemia due to
intravascular volume depletion can also cause
abdominal discomfort. Diarrhea due to intestinal edema may also
occur. Coughing, tachypnea, and
breathing difficulties may indicate pleural effusion.
Pericardial effusions and anasarca may also develop.
Hypertension may be found in 25% of the children. Painful
extremities can possibly be encountered as a
manifestation of venous thrombosis, one of complications of
nephrotic syndrome.
Systemic symptoms including fevers, weight loss, night sweats,
polyuria, polydipsia, hair loss, oral
ulcers, rashes, abdominal pain, and joint pain or swelling
should also be elicited, because they may be
manifestations of systemic diseases such as systemic lupus
erythematosus, Henoch-Schnlein purpura, or
diabetes mellitus, which can all cause nephrotic syndrome.
History of intake of drugs such as NSAIDS, gold,
and penicillamine may also be elicited in some patients. A
careful family history may also reveal hereditary
forms of nephrotic syndrome.
Laboratory Findings
Urinalysis is essential in evaluating nephrotic syndrome.
Diagnosis of nephrotic syndrome is
confirmed by the triad of generalized edema, proteinuria,
albuminuria (>2+ on dipstick or urineprotein/creatinine ratio
>2 mg/mg), and hypoalbuminemia (serum albumin
-
7/23/2019 Pediatric Nephrotic Nephritic Syndromes
8/18
8
For patients at an older age at presentation or with atypical
presentation, additional serum
studies to exclude secondary causes of nephrotic syndrome should
include C3 and C4 complement levels;
antinuclear antibody (ANA) and possibly anti-double-stranded
DNA; HIV antibody; hepatitis A, B, and C
serologies; and consideration of other viral serologies such as
HIV antibodies.
Renal biopsy is indicated only in the setting of atypical
features such as (1) age at onset (10 years), (2) steroid dependent
or steroid resistance, (3) gross or persistent microscopic
hematuria
or presence of red cell casts, (4) abnormal serologies, or (5)
significant persistent renal failure. It is also
indicated before initiation and every 2 years of use of of
second-line or third-line immunosuppressive
agents, such as cyclosporine and tacrolimus due to the known
nephrotoxicity (interstitial fibrosis) of
calcineurin inhibitors.
Differential Diagnoses
Transient proteinuria which occurs after vigorous exercise,
fever, significant dehydration,
seizures, and adrenergic agonist therapy. In contrast to
nephrotic syndrome, the proteinuria usually is
mild (UPr/Cr < 1), and always resolves within a few days.
Postural (orthostatic) proteinuria is a benign condition defined
by normal protein excretion while
recumbent, but significant proteinuria when upright. It is more
common in adolescents and tall, thin
individuals and not associated with progressive renal disease.
Many children with orthostatic proteinuria
continue this process into adulthood.
Tubular proteinuria is the preponderance of low-molecular-weight
proteins in the urine which is
suspected in conditions associated with acute tubular necrosis
(ATN), pyelonephritis, structural renal
disorders, polycystic kidney disease, and tubular toxins such as
antibiotics or chemotherapeutic agents.
Forms of Nephrotic Syndrome
The various histologic glomerular lesions presenting as
nephrotic syndrome are confirmed
through renal biopsy, but their different clinic-demographic
profiles can be used as clues distinguishamong them.
Minimal change nephrotic syndrome (MCNS) accounts for about 85%
of total cases of nephrotic
syndrome in children. The glomeruli appear normal or show a
minimal increase in mesangial cells and
matrix. Findings on immunofluorescence microscopy are typically
negative, and electron microscopy
simply reveals effacement of the epithelial cell foot processes.
More than 95% of children with minimal
change disease respond to corticosteroid therapy.
Mesangial proliferation is characterized by a diffuse increase
in mesangial cells and matrix on light
microscopy. Immunofluorescence microscopy is usually negative
but may reveal trace to 1+ mesangial
IgM and/or IgA staining. Electron microscopy reveals increased
numbers of mesangial cells and matrix as
well as effacement of the epithelial cell foot processes.
Approximately 50% of patients with this histologic
lesion respond to corticosteroid therapy.
Focal segmental glomerulosclerosis (FSGS), glomeruli show
lesions that are both focal (present
only in a proportion of glomeruli) and segmental (localized to 1
intraglomerulartufts). The lesions consist
of mesangial cell proliferation segmental scarring on light
microscopy. Immunofluorescence microscopy
is positive for IgM and C3 staining in the areas of segmental
sclerosis. Electron microscopy demonstrates
segmental scarring of the glomerular tuft with obliteration of
the glomerular capillary lumen. Only 20% of
-
7/23/2019 Pediatric Nephrotic Nephritic Syndromes
9/18
9
patients with FSGS respond to prednisone. The disease is often
progressive, ultimately involving all
glomeruli, and ultimately leads to end-stage renal disease in
most patients.
Summary of the differences between MCNS and FSGS
MCNS FSGSAge 2-6, some adults 2-10, some adults
Sex 2:1 male 1.3:1 male
Manifest as nephrotic syndrome 100% 90%
Asymptomatic proteinuria 0 10%
Hematuria 10-20% 60-80%
Hypertension 10% 20% early
Rate of progression to renal
failure
Does not progress 10yr
Light microscopy Normal Focal sclerotic lesions
Immunofluorescence Negative IgM, C3 in all lesions
Response to steroids 90% 15-20%
Treatment
Nephrotic syndrome is often classified with its response to
treatment.
The initial treatment for new-onset nephrotic syndrome generally
includes Prednisone
60mg/m2/day (maximum 80 mg/d) for 4 to 8 weeks followed by 40
mg/m2every other day for 4 to 8
weeks, and then a gradual taper until it is discontinued.
Approximately 75% of the children enter remission
within 2 weeks of treatment and 90-95% enter remission in the
initial 4 weeks of treatment.
Edema can be managed by salt restriction, moderate fluid
restriction, and judicious use of
diuretics. Albumin can be initiated with 25% albumin at 1-2
g/kg/d either as a continuous infusion or
-
7/23/2019 Pediatric Nephrotic Nephritic Syndromes
10/18
1
divided q 6-8 hours. Albumin treatment should continue for 4 to
6 hours before initial administration of
diuretics to minimize the risk of worsening any intravascular
volume depletion that may be present. In
general, slowly increasing the serum albumin level to ~2.8 g/dl
adequately restores the intravascular
oncotic pressure and volume, but there appears to be little
additional clinical benefit to increasing the
albumin level to normal values. Diuretic, usually furosemide, is
incorporated to lessen the extracellular
fluid. Furosemide incorporation with albumin transfusion or post
transfusion also prevents dissipation offurosemide into the
interstitial space. Protein intake is also suggested to be
approximately 130% to 140%
of the RDA for age.
Hyperlipidemia is usually transient and require no therapeutic
interventions to dietary restrictions
of lipids. In a few chronic cases, hydroxymethylglutaryl CoA
(HMG CoA) reductase inhibitors (statins) can
be used.
Angiotensin converting enzyme inhibitors (ACEIs)
are increasingly being used in the management of
persistent proteinuria and control of hypertension in
children with Steroid-Resistant Nephrotic syndrome
(SRNS) or Steroid-Dependent Nephrotic syndrome (SDNS).
Its antiproteinuric effects include reduction of glomerular
capillary plasma flow rate, decrease in transcapillary
hydraulic pressure, and alteration of the permeability of
the glomerular filtration barrier.
For SRNS, Calcineurin inhibitors such as
Cyclosporine, alkylating agents, and other
immunosuppressives.
Complications
Patients with nephrotic syndrome are prone to infections due to
the excretion of IgG, abnormal
T lymphocyte function, and decreased levels of factors (factor B
and D) for the alternate complement
pathway. Serious infections developed in as many as 75% of
children with nephrotic syndrome, and the
mortality rate was almost 60%. In the past 3 decades, an
estimated 70% of deaths in children with
nephrotic syndrome occur due to infection, 50% of which are due
to peritonitis. Other than peritonitis,
cellulitis, and sepsis are also common. Streptococcus
pneumoniais the most common offending agent,
although infections by Gram-negative organisms such as
Escherichia coli and Haemophilus influenzae, are
also commonly seen. The use of steroids and other
immunosuppressive agents is also a risk factor for
infections.
Infections, hypovolemia, hypercoagulable state, and
immobilizations are predisposing factors for
thrombosis. A study found out that furosemide was found to be
the major risk factor for thrombosis,
having been used in 78% of cases of thrombosis (7 of 9
children). Decreased coagulation inhibitors such
asantithrombin III are also usually seen, due to urinary losses,
and appear to correlate with the degree of
hypoalbuminemia. The incidence of thromboembolism in children
has been reported to range from 1.8 -
5%. The majority of episodes of thrombosis in children are
venous in origin, although arterial thrombosis
has been reported in 1945% of cases. The most common sites for
thrombosis are the deep leg veins,
-
7/23/2019 Pediatric Nephrotic Nephritic Syndromes
11/18
1
inferior vena cava, and ileofemoral veins although other blood
vessels may also be affected. Pain and
swelling of an extremity is suggestive of a deep venous
thrombosis.
Children with nephrotic syndrome may have restricted growth.
Urinary loss of protein hormones
could lead to stunting and hypothyroidism. Corticosteroid
therapy can also cause decreased bone
formation and increased bone resorption.
Acute Renal Failure (ARF) in nephrotic syndrome is usually
transient but rare cases may require
temporary dialysis. ARF in the setting of nephrotic syndrome may
be due to: renal vein thrombosis,
reduced renal perfusion, acute tubular necrosis, interstitial
edema within the renal parenchymal bed, and
alterations in glomerular permeability.
Prognosis
The single most important prognostic factor for maintenance of
long-term normal renal function
in nephrotic syndrome is the patients initial response to
corticosteroids. Steroid responsiveness varies by
renal histologic type. Steroid responsiveness was 93% for MCNS,
30% for FSGS, 56% for mesangial
proliferative glomerulonephritis, 7% for MPGN, and 0% for
membranous nephropathy.
Relapses of nephrotic syndrome occur commonly in SSNS. Only 30%
patients with SSNS will never
experience a relapse, although the overall tendency to relapse
decreases with time. The risk factors for
frequent relapses or a steroid-dependent course include, age of
less than 5 years at onset and prolonged
time to initial remission.
NEPHRITIC SYNDROMESNephritic syndrome is due to glomerular
injury with glomerular inflammation. Clinical
presentations of nephritic syndrome include acute nephritic
syndrome, syndrome of rapidly progressive
-
7/23/2019 Pediatric Nephrotic Nephritic Syndromes
12/18
1
glomerulonephritis, syndrome of recurrent macroscopic hematuria,
and syndrome of chronic
glomerulonephritis.
Glomerulonephritis is characterized by glomerular hematuria and
other cardinal features of
glomerular injury such as proteinuria, hypertension, edema,
oliguria, and renal insufficiency. There are
many types of glomerulonephritis; the classification of which
are usually based on histologic examination.
Acute nephritis is defined as acute glomerular injury with:
Acute kidney injury (AKI) (oliguria,
uremia, and elevated creatinine), hypertension (salt and water
retention), hematuria (microscopic or
macroscopic with red cell casts on microscopy),
peripheral and/or pulmonary edema, and
proteinuria (which can reach nephrotic range in
nephritic-nephrotic syndrome).
Acute nephritis can be caused by post
infectious nephritis, HenochSchnlein purpura
(HSP), IgA nephropathy (IgAN), Systemic lupus
erythematous (SLE), Membranoproliferativeglomerulonephritis
(MPGN, anti-GBM disease, or
pauci-immune glomerulonephritis. The main
cause of acute nephritic syndrome is acute post
infectious glomerulonephritis, which usually
follows a streptococcal infection.
ACUTE POSTINFECTIOUS GLOMERULONEPHRITISAcute postinfectious
glomerulonephritis (APIG) is characterized by the sudden onset of
gross
hematuria, edema, hypertension, renal insufficiency and/or
evidence of antecedent streptococcal
infection and interstitium concentrations. Approximately 80% is
caused by Streptococcal infections,wherein it is more appropriately
termed Acute Post Streptococcal Glomerulonephritis (APSGN)11.
The
following discussions will use APSGN since it is a prototype for
other APIG.
Epidemiology
APIG is the most common renal pathology in underdeveloped
countries. In hot climates with high
humidity, it can be a complication of pyoderma. In countries
with moderate and cold climates, it is a
complication of upper respiratory tract infections (pharyngitis)
during the winter months. Populations at
risk were children and soldiers due to intimate contact,
overcrowded living conditions, and poor hygiene
and sanitation systems. sThe male: female ratio is up to 2:1 and
it is most common in children aged 3 to12
years.
Etiology
APIG can be due to various pathogenic organisms ranging from
bacteria to parasites.
1Some sources simply use post-streptococcal glomerulonephritis
or PSGN instead of APSGN. Denis F. Geary, Franz
Schaefer. 2008. Comprehensive pediatric nephrology. Mosbly
Elsevier. Philadelphia.
-
7/23/2019 Pediatric Nephrotic Nephritic Syndromes
13/18
1
Group A -hemolytic Streptococcusis the most common etiologic
agent. The capsular M-protein
defines whether the bacterial strain is nephritogenic.
Nephritogenic strains are divided into pharyngitis-
associated serotypes (1, 3, 4, 12 and 49) and skin
infection-associated serotypes (2,49, 55, 57, and 60).
Pathogenesis
APSGN is an immune complex disease although the nature of the
nephritogenic antigen is still
unknown. The proposed mechanisms involve: (1) deposition of
circulating immune complexes containing
nephritogenic antigen in glomeruli, (2) implantation of the
nephritogenic antigen into glomerular
structures and in situ formation of immune complexes, (3)
molecular mimicry between streptococcal
antigens and normal glomerular antigens that react with
antibodies against streptococcal antigens, and
(4) direct activation of the complement system by implanted
streptococcal antigens.
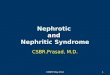
Pathology
The most typical feature observed via light microscopy is
diffuse enlargement of all glomeruli due to hypercellularity.
Swelling
of the endothelial cells leads to the obliteration of the
capillary loops.
There is increased number of mesangial cells. There is
recruitment of
numerous inflammatory cells in the glomeruli, mainly
polymorphonuclear leukocytes and monocytes; thus this
pathological picture is termed exudative proliferative
glomerulonephritis.
Immunofluorescent study shows irregular granular deposits
of complement and immunoglobulins. The most common finding
is
the presence of C3 and IgG, but C4, C1q, IgM, fibrinogen, and
factor
B may be also found.
-
7/23/2019 Pediatric Nephrotic Nephritic Syndromes
14/18
1
Starry sky is the fine granular deposition of C3 and IgG along
the capillary walls in the 1st week of
the disease. Mesangial pattern is found between the 4th and 6th
week after disease onset (C3, which is
found in mesangial location). Garland type is characterized
by
dense, confluent deposits along the capillary loops, while
mesangial and endocapillary locations are preserved.
Clinical Features
Approximately 90% of APSGN cases occur in young
children after streptococcal pharyngeal or skin infections.
The
latency period from infection to presentation is 714 days
for
pharyngeal and 1421 days for post-impetigo disease.
One-third
of APSGN patients develop discrete microscopic hematuria
and/or proteinuria in the latent period.
Usually the disease has sudden onset with development
of nephritic syndrome (edema, oliguria, azotemia, hematuria,
and hypertension). At the onset of the disease, initial
nonspecificsymptoms may be present, such as pallor, malaise,
low-grade
fever, lethargy, anorexia, and headache. Dull abdominal or
flank
pain may be present.
Gross hematuria with brownish (coke-or-tea-colored)
discoloration of urine is present in 30% to 70% of patients
while
microscopic hematuria is present in all patients.
There is edema from retention of salt and water. Most children
have mild morning periorbital
edema. Also edema may be located in the pretibial area and may
be generalized (anasarca) with presence
of pleural effusion and ascites. Mild edema may not often be
recognized by parents, but it becomes
obvious when a child had significant weight loss in the diuretic
phase.
Hypertension is the 3rd cardinal sign in APSGN. It is found in
up to 70% of hospitalized children. It
Retention of water and salt leads to expansion of the
extracellular fluid volume with consequent
suppression of the renin-angiotensin-aldosterone axis.
Normalization of the blood pressure correlates
with increased diuresis and recovery of renal function. If
elevated blood pressure persists 4 weeks after
disease onset, rapidly progressive disease or chronic
glomerulonephritis should be suspected.
Laboratory Findings
Urinalysis with microscopic studies would show red cell casts
are present in association with
dysmorphic of red cells, frequently presenting doughnut shape
with one or more blebs. Macroscopic
hematuria usually disappears after a few days but microscopic
hematuria may persist for a year andoccasionally exacerbates during
febrile episodes and more rarely after strenuous exercise.
Massive proteinuria with or without other features of the
nephrotic syndrome are found in
about 24% of the cases and its persistence is a risk factor for
progression to chronic renal disease.
A mild dilutional anemia may be seen at the onset of the
disease, and is due to expansion of the
extracellular fluid volume. Serologic testing would, in 90% of
the cases, show a reduction in serum
complement levels. Typically, complement levels normalize in 6 -
8 weeks. If hypocomplementemia
-
7/23/2019 Pediatric Nephrotic Nephritic Syndromes
15/18
1
persists more than 3 months, an alternative diagnosis, such as
membranoproliferative
glomerulonephritis, should be strongly considered. IgG and IgM
serum levels are elevated 8090% of the
patients with APSGN.
Rising antistreptococcal antibody titers are the usual clinical
indication of a preceding
streptococcal infection since positive cultures are obtained in
only 2025% of the cases. Antistreptolysin
O titers and anti-DNAse B titers are the most frequently
elevated antibody titers after streptococcal throat
infections and after streptococcal impetigo, respectively.
Renal Biopsy is the confirmatory test in difficult cases.
Differential Diagnoses
Urinary tract infection (UTI) is the most common identifiable
cause of hematuria in children;
hence other symptoms, of edema and hypertension, as well as the
progression of the disease should not
be missed out in the examination of the patient. Hematuria may
also occurs in sickle cell trait or disease,
after strenuous exercise, and after renal trauma.
Benign familial hematuria is a relatively common,
nonprogressive, usually autosomal dominantdisorder, characterized
by thinning of the glomerular basement membrane (GBM).
Treatment
Antibiotic therapy is indicated if there are still signs of
streptococcal infection (pharyngitis,
pyoderma) or patients have a positive throat or skin culture.
Antibiotic treatment does not alter the
course of the disease, but it is very important in preventing
the spread of nephritogenic strains of GABHS.
A 10-day course of systemic antibiotic therapy recommended to
limit the spread of nephritogenic
strain. Penicillin is the drug of choice. Oral penicillin V (or
erythromycin for allergic patients) is preferred
over parenteral penicillin. Amoxicillin or Co-amoxiclav can also
be given as alternatives.
In those with over 30% crescents seen in histologic examination,
they may be treated with pulse
methylprednisolone 0.5-1.0 g/1.73 m2for 3 - 5 days. Salt intake
should be limited to less than 1.0 g/day.
Protein intake should be limited to 1.0 g/kg/day. Loop diuretics
(furosemide 1-2 mg/kg/day) are indicated
if there is moderate circulatory congestion. Higher doses up to
5 mg/kg per intravenous (IV) dose are
indicated if there is pulmonary edema.
-
7/23/2019 Pediatric Nephrotic Nephritic Syndromes
16/18
1
Prognosis
Complete recovery occurs in 95% of children with post-strep GN.
Mortality avoided by
appropriate management of acute renal failure, cardiac failure
and hypertension. Infrequently acute
phase maybe severe and lead to glomerular hyalinization and
chronic kidney disease. Recurrences is
extremely rare.
Rapidly Progressive GlomerulonephritisRapidly Progressive
Glomerulonephritis or RPGN is a clinical syndrome characterized by
an acute
nephritic illness accompanied by a rapid loss of renal function
(>50% decrease in GFR) over days to weeks.
The terms RPGN and crescentic GN are used interchangeably. There
is a large presence of epithelial
crescents in the Bowmans space involving 50% or more
glomeruli.
Etiology
RPGN is believed to be the result of severe non-specific
glomerular injury, with numerous underlying
causes.
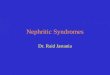
Pathogenesis
There is a physical gap in the glomerular capillary
wall and glomerular basement membrane (GBM). Breaks
in the integrity of the capillary wall lead to passage of
plasma proteins and inflammatory mediators into the
Bowmans space with fibrin formation, influx of
macrophages and T cells, and release of proinflammatory
cytokines.The presence of coagulation factors and various
proliferating cells, chiefly macrophages, parietal
glomerular epithelial cells, and interstitial fibroblasts
initiates the development of crescents.
Clinical Manifestations
The spectrum of presenting features is variable,
and includes macroscopic hematuria (in 6090% patients), oliguria
(60100%), hypertension (6080%)
and edema (6090%) (10, 13, 18). The illness may be complicated
by the occurrence of hypertensive
emergencies, pulmonary edema and cardiac failure. Occasionally,
RPGN has an insidious onset with the
initial symptoms being fatigue or edema. Nephrotic syndrome is
rare and seen in patients with less severe
renal insufficiency.
Diagnosis
There is hematuria in all patients with dysmorphic red cells and
red cell casts seen microscopically.
Most also have gross hematuria. A variable degree of
nonselective proteinuria (2+ to 4+) is present in
more than 65% of patients. Urinalysis also shows leukocyte,
granular, and tubular epithelial cell casts.
-
7/23/2019 Pediatric Nephrotic Nephritic Syndromes
17/18
1
Renal insufficiency is present at diagnosis in almost all cases,
with the plasma creatinine
concentration often exceeding 3 mg/dl (264 mol/L).
Treatment
The specific treatment of RPGN broadly comprises two phases: (1)
induction of remission and its
(2) maintenance. Combination therapy with high-dose
corticosteroids and cyclophosphamide is the
current standard for induction treatment, with additional
therapy for those with life- or organ threatening
disease. The treatment includes Cyclophosphamide oral dose of 2
mg/kg/day, or IV starting at 500 mg/m2
and increased monthly by 125 mg/m2to a maximum of 750 mg/m2,IV
pulses of methylprednisolone (15-20 mg/kg, maximum 1 g/day) for 3
to 6 days,
followed by high-dose oral prednisone (1.5-2
mg/kg daily) for 4 weeks, tapering to 0.5
mg/kg daily by 3months and alternate-day
prednisone for 6 to 12 months.
The requirement for maintenance
therapy in RPGN depends on the underlying
disease.
MEMBRANOPROLIFERATIVE GLOMERULONEPHRITISAlso referred to as
mesangiocapillary glomerulonephritis, Membranoproliferative
glomerulonephritis is a collection of morphologically related
but pathogenetically distinct disorders. They
are characterized by glomerular hypercellularity, increased
mesangial matrix, and thickening of the
peripheral capillary walls.
-
7/23/2019 Pediatric Nephrotic Nephritic Syndromes
18/18
1
The morphologic pattern upon light microscopy shows a pattern of
injury characterized by
mesangial proliferation and thickening of the peripheral GBM.
The thickening is due to mesangial cell
interposition with double contours of the GBM and
cloverleaf-like accentuation of the glomerular tuft
IGA NEPHROPATHYIgA nephropathy is a glomerular disease
characterized by the presence of IgA deposits prevalent
over other classes of immunoglobulins. It can be observed in
association with features of systemic
vasculitis in Henoch- Schnlein purpura or can be renal limited,
as described by Berger (primary IgAN).
It presents as recurrent episodes of gross hematuria concomitant
with upper respiratory tract
infections or other mucosal inflammatory processes. The 1st
episode of macroscopic hematuria generally
occurs between 15 and 30 years of age. Affected children do not
present symptoms or urinary signs before
the age of 3 thereafter the frequency increases with age. Gross
hematuria affects 30% to 40% of children
with IgAN.
The treatment is based on the clinical features. Medical
interventions range from no specific
treatment to ACEI or Angtiotensin Receptor Blockers (ARBs) to
Prednisone or Prednisolone.