Embed Size (px)
Citation preview
ESENTAS
Pediatric Parapharyngeal Tumors
Ossama A.Hamid, MDProfessor Otolaryngology, Head-Neck SurgeryAin Shams UniversityGS: Egyptian Society of Ear, Nose, Throat and Allied Sciences ESENTAS
Alexandria ORL, April 2010Alexandria ORL, April 2010
Parapharyngeal SpaceParapharyngeal SpaceParapharyngeal SpaceParapharyngeal Space
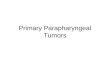
Th l f h d i l f i liTh l f h d i l f i li The layers of the deep cervical fascia split to The layers of the deep cervical fascia split to envelop different structures of H&N, leading to envelop different structures of H&N, leading to the formation of different fascial spacesthe formation of different fascial spaces
The suprahyoid area encompasses the deep The suprahyoid area encompasses the deep hidden spaces between the skull base & hyoid hidden spaces between the skull base & hyoid bonebonebonebone
Parapharyngeal space PPS is the centrally Parapharyngeal space PPS is the centrally located suprahyoid spacelocated suprahyoid space
It is incompletely ensheathed by the deep It is incompletely ensheathed by the deep cervical fasciacervical fascia Can be easily displaced by surrounding lesionsCan be easily displaced by surrounding lesions Can be easily displaced by surrounding lesionsCan be easily displaced by surrounding lesions
It is a fat containing spaceIt is a fat containing space Can be easily identified radiologicallyCan be easily identified radiologically
Parapharyngeal SpaceParapharyngeal SpaceParapharyngeal SpaceParapharyngeal Space
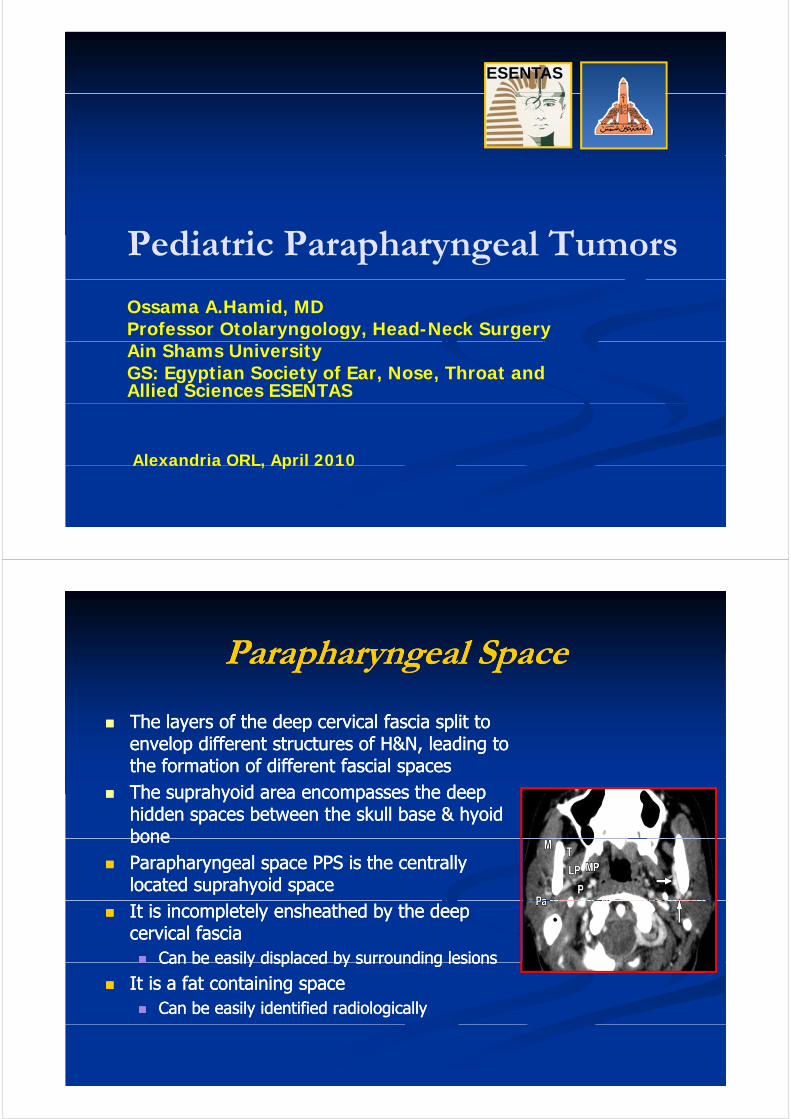
A i ll i i di id d iA i ll i i di id d i Anatomically, it is divided into:Anatomically, it is divided into: Prestyloid part: PPS properPrestyloid part: PPS proper Poststyloid part: Carotid space CSPoststyloid part: Carotid space CSy p py p p
The structures found in each space can give origin to different The structures found in each space can give origin to different pathologies.pathologies.PPS t iPPS t i PPS contains:PPS contains: Minor salivary glandsMinor salivary glands Lymphoid tissue of the Waldeyer’s ringLymphoid tissue of the Waldeyer’s ringy p y gy p y g Mucosal surface related to the nasopharynx & oropharynxMucosal surface related to the nasopharynx & oropharynx
CS: contains:CS: contains:C tid h th ICA IJV C i l 9C tid h th ICA IJV C i l 9 1212 Carotid sheath: ICA. IJV, Cranial nerves 9Carotid sheath: ICA. IJV, Cranial nerves 9--1212
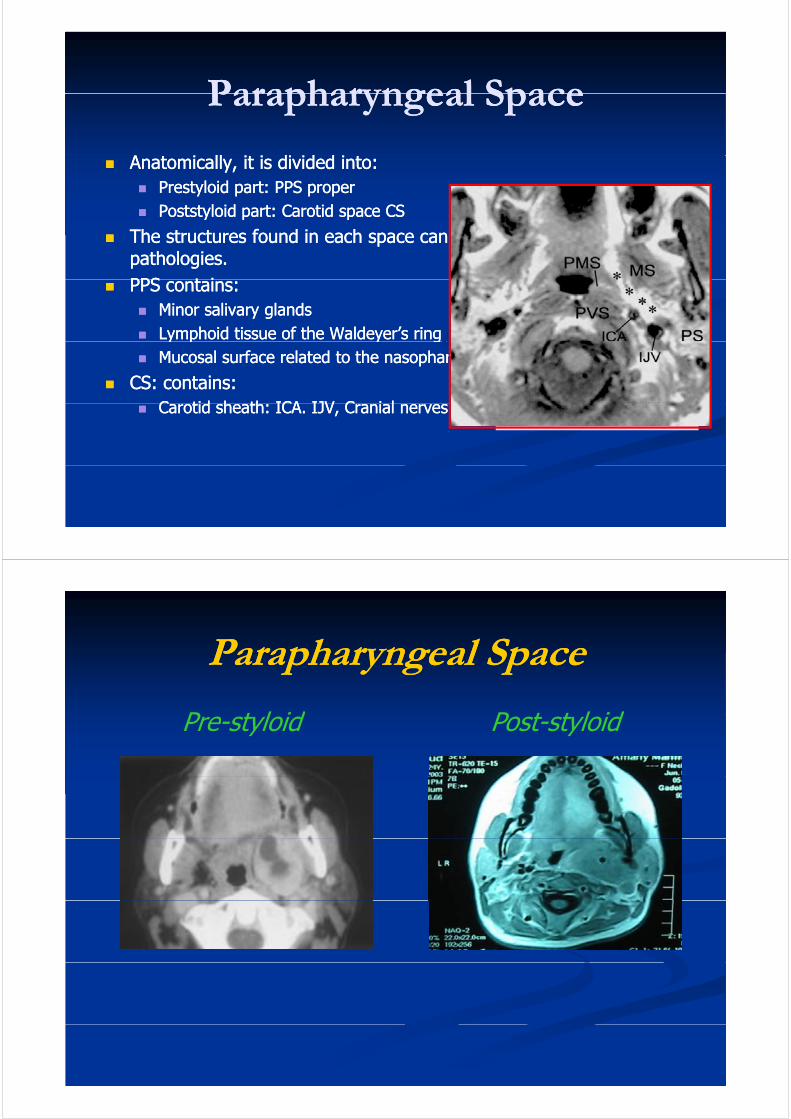
Parapharyngeal SpaceParapharyngeal SpaceParapharyngeal SpaceParapharyngeal Space
P t l id P t t l idPre-styloid Post-styloid
Parapharyngeal SpaceParapharyngeal SpaceParapharyngeal SpaceParapharyngeal Space
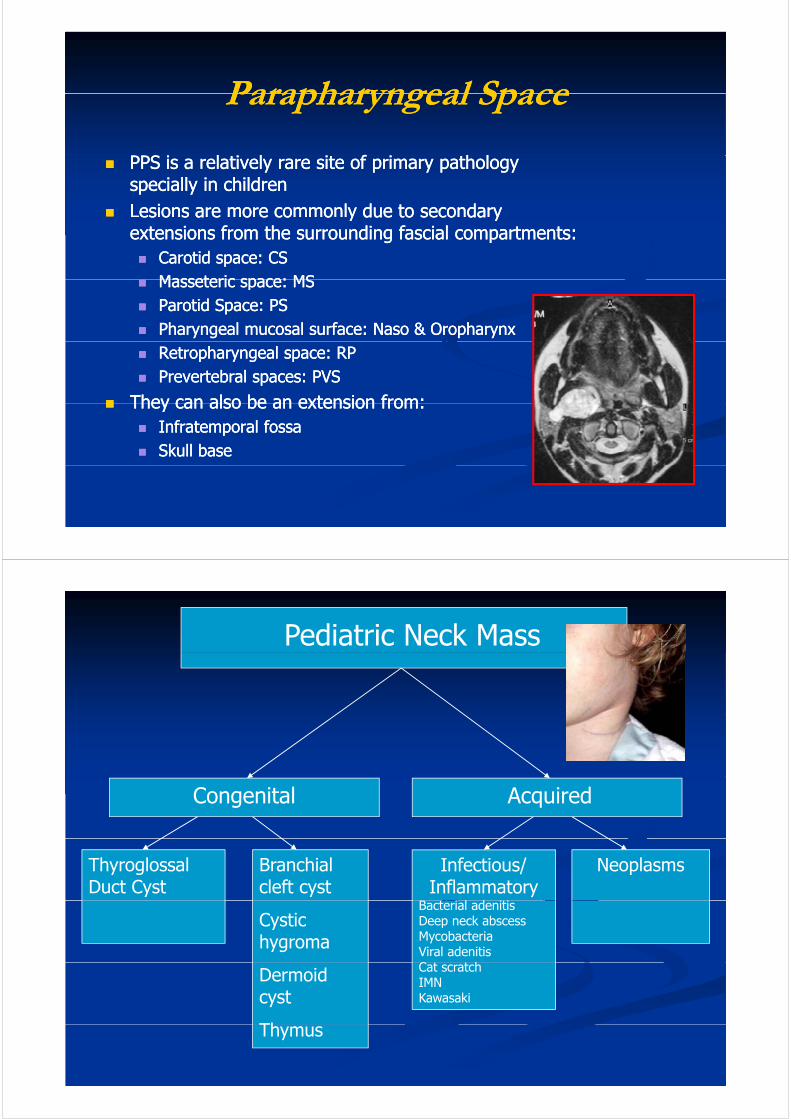
PPS i l i l i f i h lPPS i l i l i f i h l PPS is a relatively rare site of primary pathology PPS is a relatively rare site of primary pathology specially in childrenspecially in children
Lesions are more commonly due to secondary Lesions are more commonly due to secondary es o s a e o e co o y due to seco da yes o s a e o e co o y due to seco da yextensions from the surrounding fascial compartments:extensions from the surrounding fascial compartments: Carotid space: CSCarotid space: CS
Masseteric space: MSMasseteric space: MS Masseteric space: MSMasseteric space: MS Parotid Space: PSParotid Space: PS Pharyngeal mucosal surface: Naso & OropharynxPharyngeal mucosal surface: Naso & Oropharynx Retropharyngeal space: RPRetropharyngeal space: RP Prevertebral spaces: PVSPrevertebral spaces: PVS
They can also be an extension from:They can also be an extension from: They can also be an extension from:They can also be an extension from: Infratemporal fossaInfratemporal fossa Skull baseSkull base
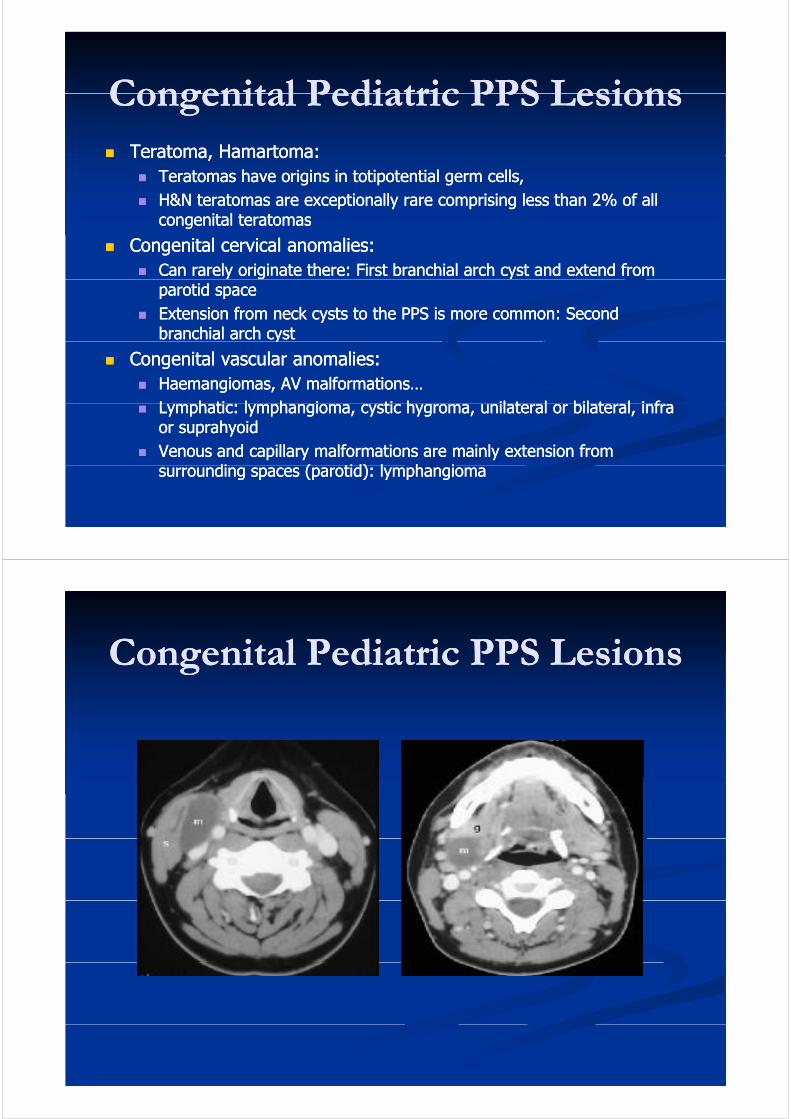
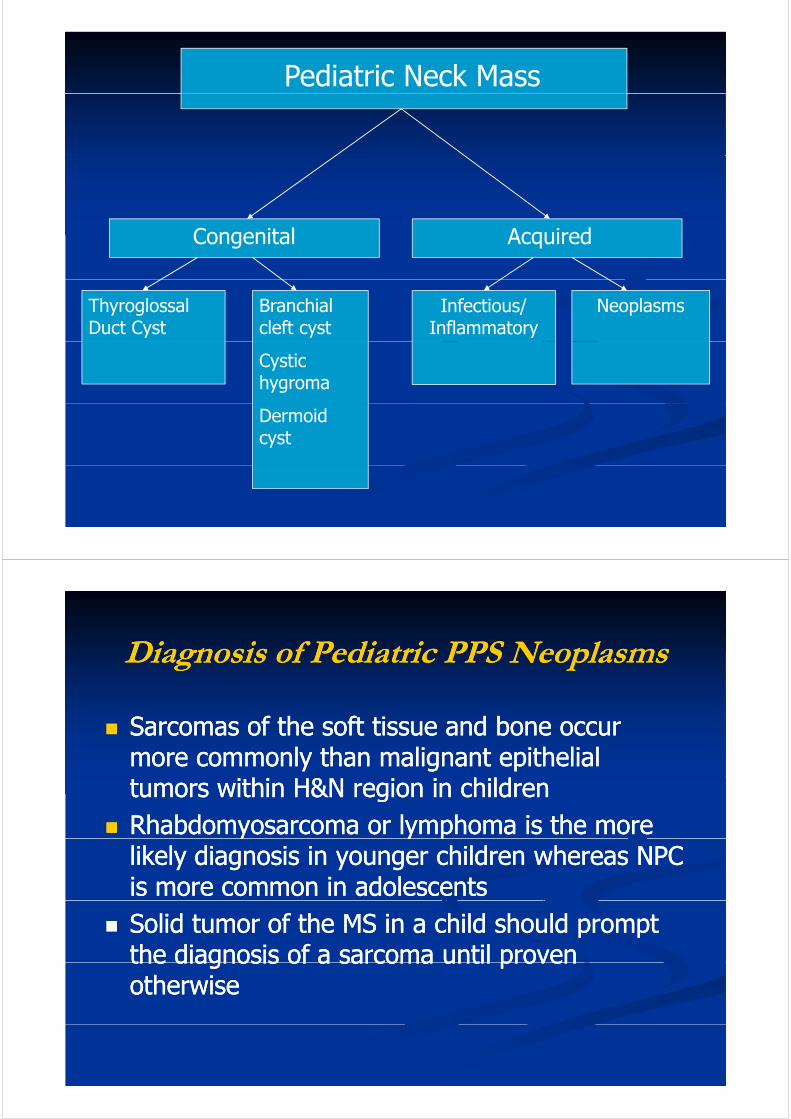
Pediatric Neck Mass
Congenital Acquired
Thyroglossal Duct Cyst
Infectious/Inflammatory
B i l d i i
NeoplasmsBranchial cleft cyst
Bacterial adenitisDeep neck abscessMycobacteriaViral adenitisC h
Cystic hygroma
Cat scratchIMNKawasaki
Dermoid cyst
ThThymus
Congenital Pediatric PPS LesionsCongenital Pediatric PPS LesionsCongenital Pediatric PPS LesionsCongenital Pediatric PPS Lesions TeratomaTeratoma,, HamartomaHamartoma:: TeratomaTeratoma, , HamartomaHamartoma: :
TeratomasTeratomas have origins in have origins in totipotentialtotipotential germ cells, germ cells, H&N H&N teratomasteratomas are exceptionally rare comprising less than are exceptionally rare comprising less than 22% of all % of all
congenitalcongenital teratomasteratomascongenital congenital teratomasteratomas
Congenital cervical anomalies:Congenital cervical anomalies: Can rarely originate there: First Can rarely originate there: First branchialbranchial arch cyst and extend from arch cyst and extend from
parotid spaceparotid space Extension from neck cysts to the PPS is more common: Second Extension from neck cysts to the PPS is more common: Second
branchialbranchial arch cystarch cystyy
Congenital vascular anomalies:Congenital vascular anomalies: HaemangiomasHaemangiomas, AV malformations…, AV malformations…
L h tiL h ti l h il h i titi hh il t l bil t l i fil t l bil t l i f Lymphatic: Lymphatic: lymphangiomalymphangioma, cystic , cystic hygromahygroma, unilateral or bilateral, infra , unilateral or bilateral, infra or or suprahyoidsuprahyoid
Venous and capillary malformations are mainly extension from Venous and capillary malformations are mainly extension from di ( tid)di ( tid) l h il h isurrounding spaces (parotid): surrounding spaces (parotid): lymphangiomalymphangioma
Congenital Pediatric PPS LesionsCongenital Pediatric PPS LesionsCongenital Pediatric PPS LesionsCongenital Pediatric PPS Lesions
Congenital Pediatric PPS LesionsCongenital Pediatric PPS LesionsCongenital Pediatric PPS LesionsCongenital Pediatric PPS Lesions
Inflammatory Pediatric PPS LesionsInflammatory Pediatric PPS LesionsInflammatory Pediatric PPS LesionsInflammatory Pediatric PPS Lesions
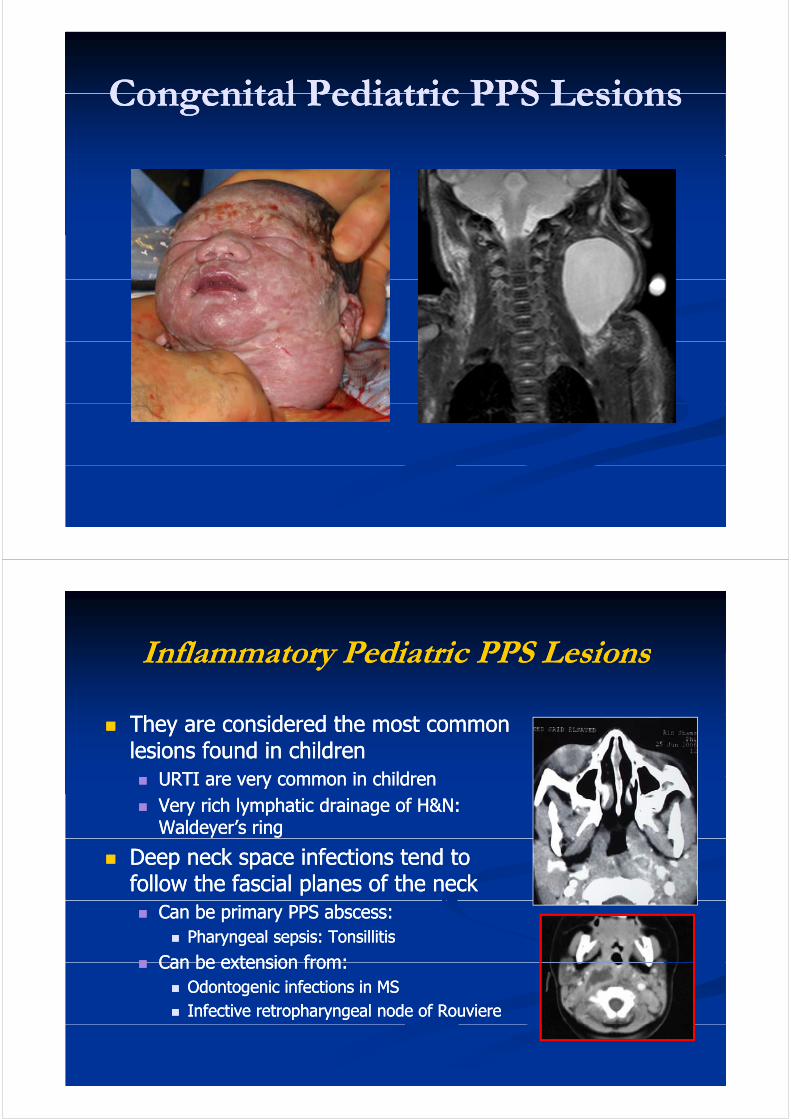
They are considered the most common They are considered the most common lesions found in childrenlesions found in children
URTI are very common in childrenURTI are very common in children URTI are very common in childrenURTI are very common in children Very rich lymphatic drainage of H&N: Very rich lymphatic drainage of H&N:
Waldeyer’sWaldeyer’s ringring
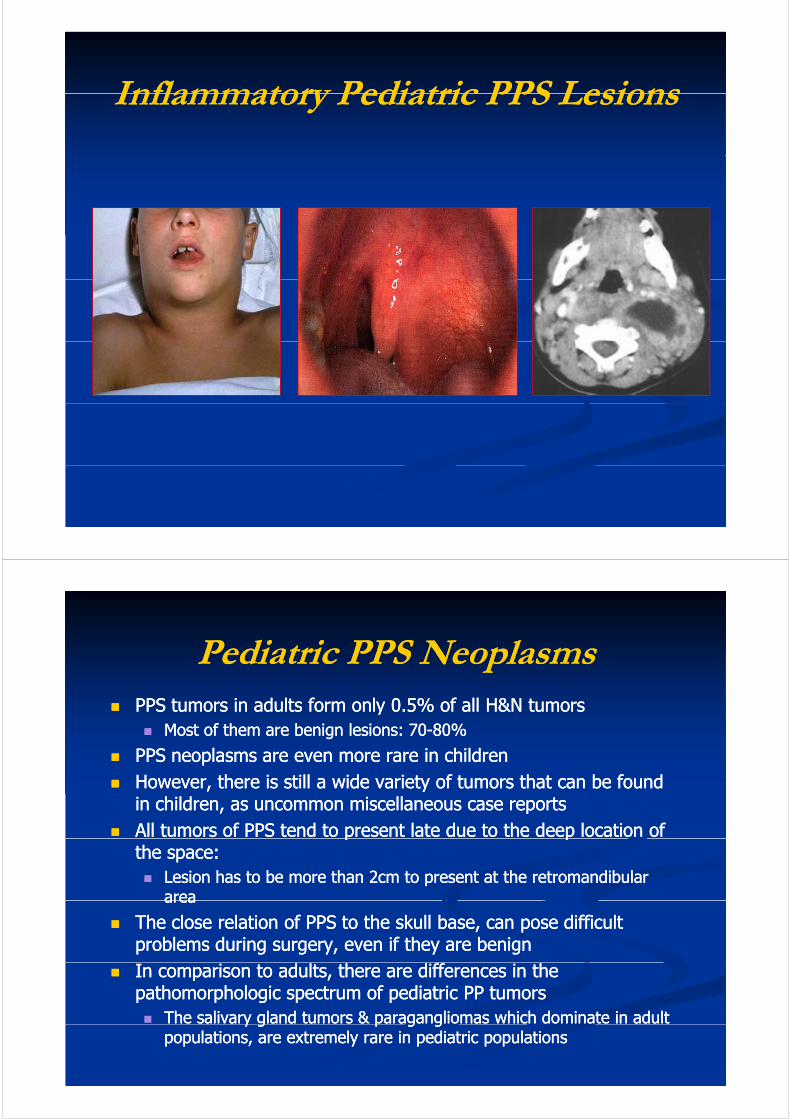
Deep neck space infections tend to Deep neck space infections tend to follow the follow the fascialfascial planes of the neckplanes of the neck Can be primary PPS abscess:Can be primary PPS abscess:
Pharyngeal sepsis: TonsillitisPharyngeal sepsis: Tonsillitis
Can be extension from:Can be extension from: Can be extension from:Can be extension from: OdontogenicOdontogenic infections in MSinfections in MS Infective retropharyngeal node of Infective retropharyngeal node of RouviereRouviere
Inflammatory Pediatric PPS LesionsInflammatory Pediatric PPS LesionsInflammatory Pediatric PPS LesionsInflammatory Pediatric PPS Lesions
Pediatric PPS NeoplasmsPediatric PPS NeoplasmsPediatric PPS NeoplasmsPediatric PPS Neoplasms PPS tumors in adults form only PPS tumors in adults form only 00..55% of all H&N tumors % of all H&N tumors yy
Most of them are benign lesions: Most of them are benign lesions: 7070--8080%%
PPS neoplasms are even more rare in childrenPPS neoplasms are even more rare in childrenH th i till id i t f t th t b f dH th i till id i t f t th t b f d However, there is still a wide variety of tumors that can be found However, there is still a wide variety of tumors that can be found in children, as uncommon miscellaneous case reportsin children, as uncommon miscellaneous case reports
All tumors of PPS tend to present late due to the deep location of All tumors of PPS tend to present late due to the deep location of p pp pthe space: the space: Lesion has to be more than Lesion has to be more than 22cm to present at the retromandibular cm to present at the retromandibular
areaareaareaarea
The close relation of PPS to the skull base, can pose difficult The close relation of PPS to the skull base, can pose difficult problems during surgery, even if they are benignproblems during surgery, even if they are benign
In comparison to adults, there are differences in the In comparison to adults, there are differences in the pathomorphologic spectrum of pediatric PP tumorspathomorphologic spectrum of pediatric PP tumors The salivary gland tumors & paragangliomas which dominate in adult The salivary gland tumors & paragangliomas which dominate in adult y g p g gy g p g g
populations, are extremely rare in pediatric populationspopulations, are extremely rare in pediatric populations
Pediatric PPS NeoplasmsPediatric PPS NeoplasmsPediatric PPS NeoplasmsPediatric PPS Neoplasms
PPS tumors represent a heterogeneous group of PPS tumors represent a heterogeneous group of uncommon neoplasmsuncommon neoplasmsB i t ll A id i t fB i t ll A id i t f Benign tumors are generally very rare. A wide variety of Benign tumors are generally very rare. A wide variety of tissues give rise to a wide variety of uncommon lesions.tissues give rise to a wide variety of uncommon lesions.
Primary malignant tumors of PPS in children are alsoPrimary malignant tumors of PPS in children are also Primary malignant tumors of PPS in children are also Primary malignant tumors of PPS in children are also rarerare
More commonly they are an extension of malignancyMore commonly they are an extension of malignancy More commonly they are an extension of malignancy More commonly they are an extension of malignancy from surrounding spaces from surrounding spaces
Unfortunately, these tumors tend to be locally advancedUnfortunately, these tumors tend to be locally advanced Unfortunately, these tumors tend to be locally advanced Unfortunately, these tumors tend to be locally advanced by the time they are diagnosed mainly because the by the time they are diagnosed mainly because the clinical presentation is nonclinical presentation is non--specificspecific
Pediatric PPS LesionsPediatric PPS LesionsPediatric PPS LesionsPediatric PPS Lesions Benign:Benign: Benign: Benign:
Commonest: neurogenic: neuroblastic tumors, Commonest: neurogenic: neuroblastic tumors, neurofibromaneurofibroma
LipomaLipomaLipomaLipoma Malignant:Malignant:
Lymphoma: Lymphoma: extraextra--nodal NHL, H&N most common site, nodal NHL, H&N most common site, , ,, ,
Waldeyer’s ringWaldeyer’s ring Burkitt’s lymphomaBurkitt’s lymphoma
Soft tissue sarcomas: rhabdo, chondro, fibro, Soft tissue sarcomas: rhabdo, chondro, fibro, hemangio neurohemangio neurohemangio, neurohemangio, neuro
Rhabdomyosarcoma: H&N is the most common Rhabdomyosarcoma: H&N is the most common site of origin: orbit, nasopharynx, PNSsite of origin: orbit, nasopharynx, PNS
NeuroblastomaNeuroblastoma Nasopharyngeal carcinoma: UndifferentiatedNasopharyngeal carcinoma: Undifferentiated
Pediatric PPS NeoplasmsPediatric PPS NeoplasmsPediatric PPS NeoplasmsPediatric PPS Neoplasms
II L hL h II-- Lymphoma: Lymphoma: Lymphomas are the third most frequent type of Lymphomas are the third most frequent type of
childhood cancerchildhood cancerchildhood cancerchildhood cancer Hodgkin lymphomaHodgkin lymphoma ExtraExtra--nodal NHL H&N most common site withnodal NHL H&N most common site with ExtraExtra nodal NHL, H&N most common site, with nodal NHL, H&N most common site, with
involvement of the Waldeyer’s ring.involvement of the Waldeyer’s ring. Fever, night sweats and loss of weoghtFever, night sweats and loss of weoght, g g, g g Burkitt’s lymphomaBurkitt’s lymphoma
Pediatric PPS NeoplasmsPediatric PPS NeoplasmsPediatric PPS NeoplasmsPediatric PPS Neoplasms
IIII-- Sarcomas of the soft tissue and bone:Sarcomas of the soft tissue and bone: Heterogeneous group of malignant diseases Heterogeneous group of malignant diseases HN sarcomas are difficult to treatHN sarcomas are difficult to treat Most common site is masseteric space, from where it Most common site is masseteric space, from where it
directly extends to PPSdirectly extends to PPS Any type of soft tissue sarcomas can be found: Any type of soft tissue sarcomas can be found:
h bd h d fib h i lih bd h d fib h i lirhabdo, chondroma, fibro, hemangio, neuro, lipo…rhabdo, chondroma, fibro, hemangio, neuro, lipo… Rhabdomyosarcoma: common HN sites are: orbit, Rhabdomyosarcoma: common HN sites are: orbit,
h PNSh PNSnasopharynx, PNSnasopharynx, PNS
Pediatric PPS NeoplasmsPediatric PPS NeoplasmsPediatric PPS NeoplasmsPediatric PPS Neoplasms
IIIIII N h l iN h l i IIIIII-- Nasopharyngeal carcinoma:Nasopharyngeal carcinoma: < 1% of all childhood cancers< 1% of all childhood cancers
C 10C 10 1919 Common 10Common 10--19 years 19 years Undifferentiated NPC is commonest: advanced Undifferentiated NPC is commonest: advanced
locoregional spread and distant metastaseslocoregional spread and distant metastaseslocoregional spread and distant metastases locoregional spread and distant metastases PPS involvement may occur through:PPS involvement may occur through:
Extension of the mucosal lesion to PPS occurs when the Extension of the mucosal lesion to PPS occurs when the tumor breaches the pharyngobasilar fascia: T2b according tumor breaches the pharyngobasilar fascia: T2b according to AJCC TNM classification 6th edition (2002): to AJCC TNM classification 6th edition (2002):
Early detection, while the tumor is confined to the soft tissues Early detection, while the tumor is confined to the soft tissues y ,y ,of the nasopharynx is essentialof the nasopharynx is essential
The primary echelon of lymphatic drainage from the The primary echelon of lymphatic drainage from the nasopharynx include the lateral retropharyngeal groupnasopharynx include the lateral retropharyngeal groupnasopharynx include the lateral retropharyngeal groupnasopharynx include the lateral retropharyngeal group
Pediatric PPS NeoplasmsPediatric PPS NeoplasmsPediatric PPS NeoplasmsPediatric PPS Neoplasms
IIIIII N h l iN h l i IIIIII-- Nasopharyngeal carcinoma:Nasopharyngeal carcinoma: Local symptoms are nonspecific and typically are Local symptoms are nonspecific and typically are
caused by ET obstruction and nasal blockage by thecaused by ET obstruction and nasal blockage by thecaused by ET obstruction and nasal blockage by the caused by ET obstruction and nasal blockage by the massmass
As adenoidal hypertrophy is by far the most common As adenoidal hypertrophy is by far the most common cause of a mass in the posterior nasopharynx incause of a mass in the posterior nasopharynx incause of a mass in the posterior nasopharynx in cause of a mass in the posterior nasopharynx in children, pediatric NPC is generally not suspected children, pediatric NPC is generally not suspected clinically until late into the disease process. clinically until late into the disease process. A t i h l thA t i h l th Asymmetric nasopharyngeal mass may arouse the Asymmetric nasopharyngeal mass may arouse the suspicion of NPC in children.suspicion of NPC in children.
Subtle involvement of PPS may be difficult to Subtle involvement of PPS may be difficult to Subtle involvement of PPS may be difficult to Subtle involvement of PPS may be difficult to appreciate:appreciate:
Pediatric PPS NeoplasmsPediatric PPS NeoplasmsPediatric PPS NeoplasmsPediatric PPS Neoplasms
IVIV Sympathetic nervous system tumors: NeuroblasticSympathetic nervous system tumors: Neuroblastic IVIV-- Sympathetic nervous system tumors: Neuroblastic Sympathetic nervous system tumors: Neuroblastic tumors:tumors: Derived from the primordial neural crest cells (sympathogonia) Derived from the primordial neural crest cells (sympathogonia)
th t f th th ti tth t f th th ti tthat form the sympathetic nervous system that form the sympathetic nervous system Neuroblastic tumors are the third most common cause of solid Neuroblastic tumors are the third most common cause of solid
tumors in early childhood tumors in early childhood C i l t t f lC i l t t f l 11 55% f f% f f Cervical tumors account for only Cervical tumors account for only 11--55% of cases of % of cases of neuroblastomasneuroblastomas
Neuroblastic tumors are remarkable for their varied biologic Neuroblastic tumors are remarkable for their varied biologic behaviorbehaviorbehaviorbehavior Differ in their degree of cellular and extracellular maturation:Differ in their degree of cellular and extracellular maturation: Precursor cells may remain undifferentiated = malignant, or they Precursor cells may remain undifferentiated = malignant, or they
may mature = benignmay mature = benignmay mature benignmay mature benign
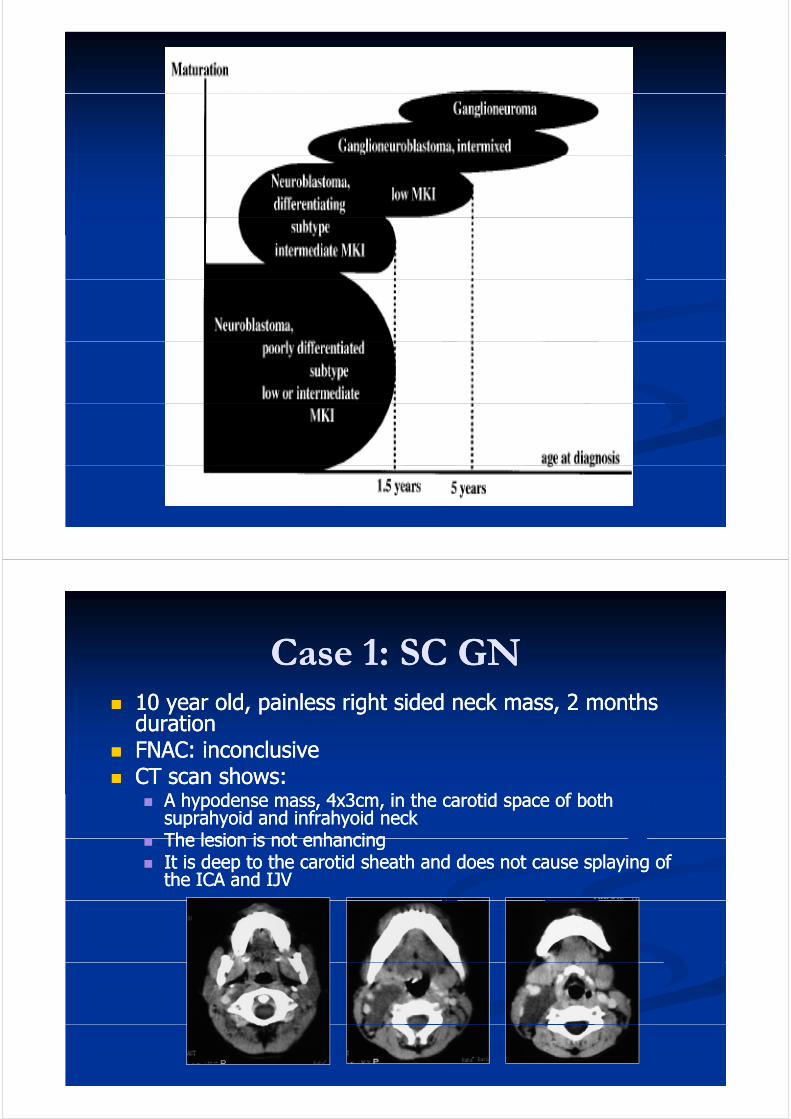
Neuroblastic tumorsNeuroblastic tumorsNeuroblastic tumorsNeuroblastic tumors They define a spectrum of sympatheticThey define a spectrum of sympathetic They define a spectrum of sympathetic They define a spectrum of sympathetic
neuroectodermal tumorsneuroectodermal tumors Ganglioneuroma GN:Ganglioneuroma GN: Ganglioneuroma GN: Ganglioneuroma GN:
Composed of gangliocytes & mature stroma. occur in Composed of gangliocytes & mature stroma. occur in children ≈ 7 years and tend to behave in a benign fashion. children ≈ 7 years and tend to behave in a benign fashion.
Ganglioneuroblastoma GNB: Ganglioneuroblastoma GNB: Composed of both mature gangliocytes and immature Composed of both mature gangliocytes and immature
bl t d h i t di t li t t ti lbl t d h i t di t li t t ti lneuroblasts and has intermediate malignant potentialneuroblasts and has intermediate malignant potential
Neuroblastoma NB: Neuroblastoma NB: Is the most immature undifferentiated & malignant :Is the most immature undifferentiated & malignant : Is the most immature, undifferentiated & malignant : Is the most immature, undifferentiated & malignant :
aggressive and occur in younger patients < 2 years. It is aggressive and occur in younger patients < 2 years. It is considered the third most common pediatric malignancy, considered the third most common pediatric malignancy, ft l k i d t l t tft l k i d t l t tafter leukemia and central nervous system tumors. after leukemia and central nervous system tumors.
Neuroblastic tumorsNeuroblastic tumorsNeuroblastic tumorsNeuroblastic tumors
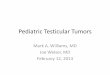
CaseCase 11: SC GN: SC GNCase Case 11: SC GN: SC GN 10 10 year old, painless right sided neck mass, year old, painless right sided neck mass, 2 2 months months
dddurationduration FNAC: inconclusiveFNAC: inconclusive CT scan shows:CT scan shows: CT scan shows:CT scan shows:
A hypodense mass, A hypodense mass, 44xx33cm, in the carotid space of both cm, in the carotid space of both suprahyoid and infrahyoid necksuprahyoid and infrahyoid neck
The lesion is not enhancingThe lesion is not enhancing The lesion is not enhancingThe lesion is not enhancing It is deep to the carotid sheath and does not cause splaying of It is deep to the carotid sheath and does not cause splaying of
the ICA and IJV the ICA and IJV
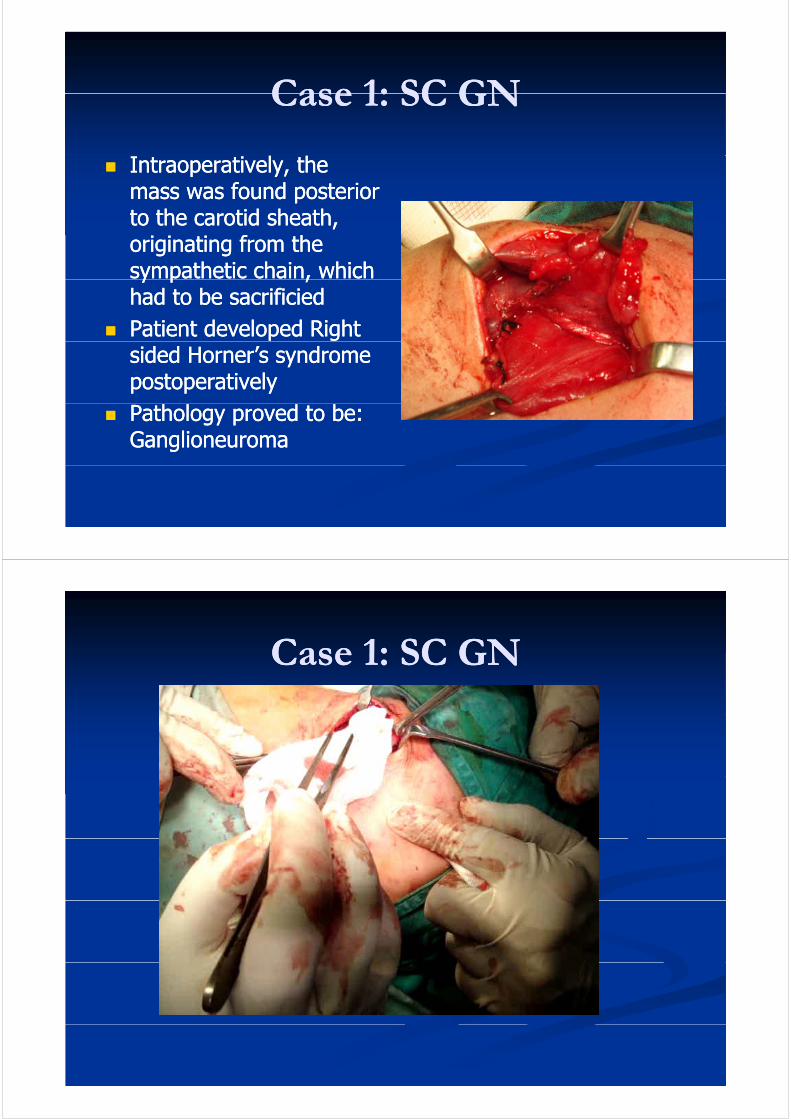
Case 1: SC GNCase 1: SC GNCase 1: SC GNCase 1: SC GN
Intraoperatively, the Intraoperatively, the mass was found posterior mass was found posterior to the carotid sheathto the carotid sheathto the carotid sheath, to the carotid sheath, originating from the originating from the sympathetic chain, which sympathetic chain, which y p ,y p ,had to be sacrificiedhad to be sacrificied
Patient developed Right Patient developed Right sided Horner’s syndrome sided Horner’s syndrome postoperativelypostoperatively
Pathology proved to be: Pathology proved to be: Ganglioneuroma Ganglioneuroma
CaseCase 11: SC GN: SC GNCase Case 11: SC GN: SC GN
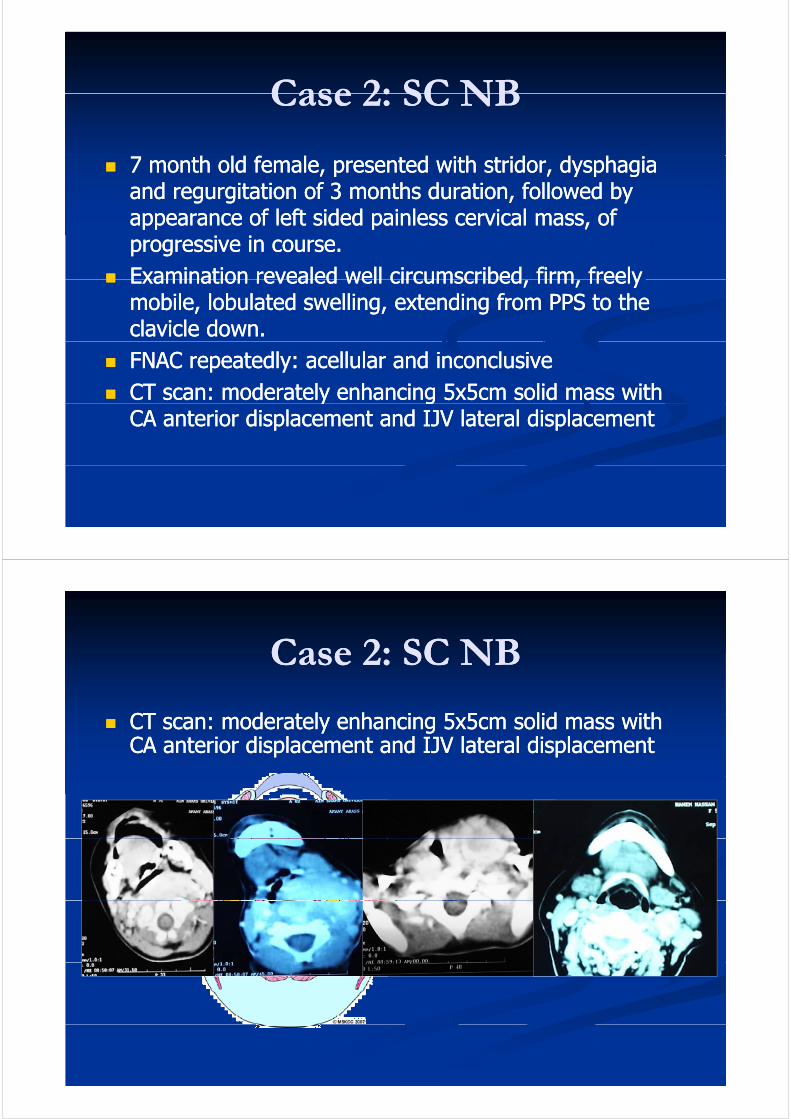
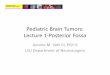
CaseCase 22: SC NB: SC NBCase Case 22: SC NB: SC NB
7 month old female, presented with 7 month old female, presented with stridorstridor, , dysphagiadysphagiaand regurgitation of 3 months duration, followed by and regurgitation of 3 months duration, followed by appearance of left sided painless cervical mass ofappearance of left sided painless cervical mass ofappearance of left sided painless cervical mass, of appearance of left sided painless cervical mass, of progressive in course.progressive in course.
Examination revealed well circumscribed firm freelyExamination revealed well circumscribed firm freely Examination revealed well circumscribed, firm, freely Examination revealed well circumscribed, firm, freely mobile, mobile, lobulatedlobulated swelling, extending from PPS to the swelling, extending from PPS to the clavicle down. clavicle down.
FNAC repeatedly: FNAC repeatedly: acellularacellular and inconclusiveand inconclusive CT scan: moderately enhancing 5x5cm solid mass with CT scan: moderately enhancing 5x5cm solid mass with y gy g
CA anterior displacement and IJV lateral displacement CA anterior displacement and IJV lateral displacement
Case 2: SC NBCase 2: SC NBCase 2: SC NBCase 2: SC NB
CT d t l h iCT d t l h i 55 55 lid ithlid ith CT scan: moderately enhancing CT scan: moderately enhancing 55xx55cm solid mass with cm solid mass with CA anterior displacement and IJV lateral displacement CA anterior displacement and IJV lateral displacement
CaseCase 22: SC NB: SC NBCase Case 22: SC NB: SC NB
I t ti lI t ti l IntraoperativelyIntraoperatively: mass : mass was posterior to the was posterior to the carotid vessels, pushing carotid vessels, pushing ca ot d esse s, pus gca ot d esse s, pus gIJV & X laterallyIJV & X laterally
Complete surgical Complete surgical i i d t thi i d t thexcision was done at the excision was done at the
expense of sacrificing the expense of sacrificing the sympathetic nerve trunksympathetic nerve trunksympathetic nerve trunk sympathetic nerve trunk from which it was from which it was originatingoriginatingP S tP S t Pressure Symptoms were Pressure Symptoms were immediately relieved immediately relieved postoperativelypostoperativelypostoperativelypostoperatively
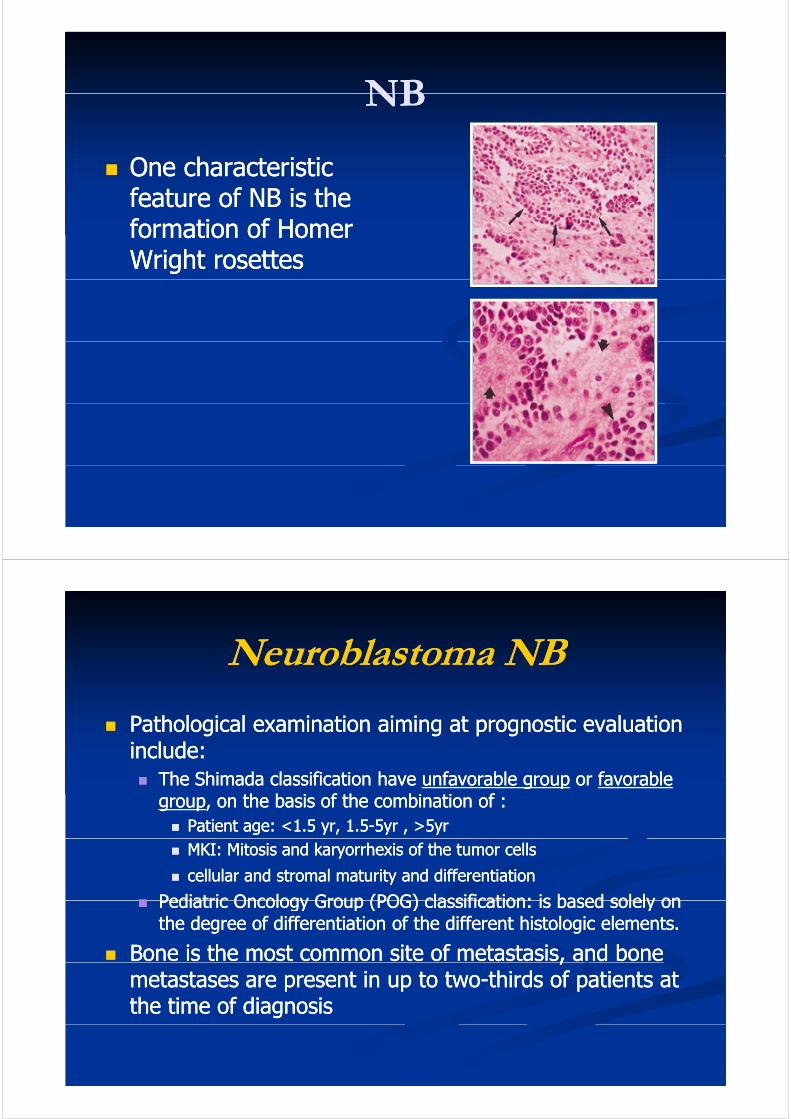
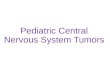
NBNBNBNB
One characteristic One characteristic feature of NB is the feature of NB is the formation of Homer formation of Homer Wright rosettes Wright rosettes
Neuroblastoma NBNeuroblastoma NBNeuroblastoma NBNeuroblastoma NB
Pathological examination aiming at prognostic evaluation Pathological examination aiming at prognostic evaluation include: include:
The Shimada classification haveThe Shimada classification have unfavorable groupunfavorable group oror favorablefavorable The Shimada classification have The Shimada classification have unfavorable groupunfavorable group or or favorable favorable groupgroup, on the basis of the combination of :, on the basis of the combination of : Patient age: <Patient age: <11..5 5 yr, yr, 11..55--55yr , >yr , >55yryr MKI: Mitosis and MKI: Mitosis and karyorrhexiskaryorrhexis of the tumor cells of the tumor cells
cellular and cellular and stromalstromal maturity and differentiationmaturity and differentiation
Pediatric Oncology Group (POG) classification: is based solely onPediatric Oncology Group (POG) classification: is based solely on Pediatric Oncology Group (POG) classification: is based solely on Pediatric Oncology Group (POG) classification: is based solely on the degree of differentiation of the different the degree of differentiation of the different histologichistologic elements.elements.
Bone is the most common site of metastasis, and bone Bone is the most common site of metastasis, and bone ,,metastases are present in up to twometastases are present in up to two--thirds of patients at thirds of patients at the time of diagnosis the time of diagnosis
Neuroblastoma NBNeuroblastoma NBNeuroblastoma NBNeuroblastoma NB
International Neuroblastoma Staging System (INSS): International Neuroblastoma Staging System (INSS): 19861986
Based on clinical radiologic and surgical featuresBased on clinical radiologic and surgical features Based on clinical, radiologic, and surgical featuresBased on clinical, radiologic, and surgical features
30% of all NBs display Myc30% of all NBs display Myc--N amplification, a protoN amplification, a proto--oncogene that indicates rapid tumor progression and aoncogene that indicates rapid tumor progression and aoncogene, that indicates rapid tumor progression and a oncogene, that indicates rapid tumor progression and a poor outcome poor outcome
By combining the Shimada classification, INSS stage,By combining the Shimada classification, INSS stage,By combining the Shimada classification, INSS stage, By combining the Shimada classification, INSS stage, and some genetic features, it is possible to stratify NB and some genetic features, it is possible to stratify NB into:into: LowLow--, intermediate, intermediate--, and high, and high--risk groups. risk groups.
Treatment is based on risk group. Treatment is based on risk group.
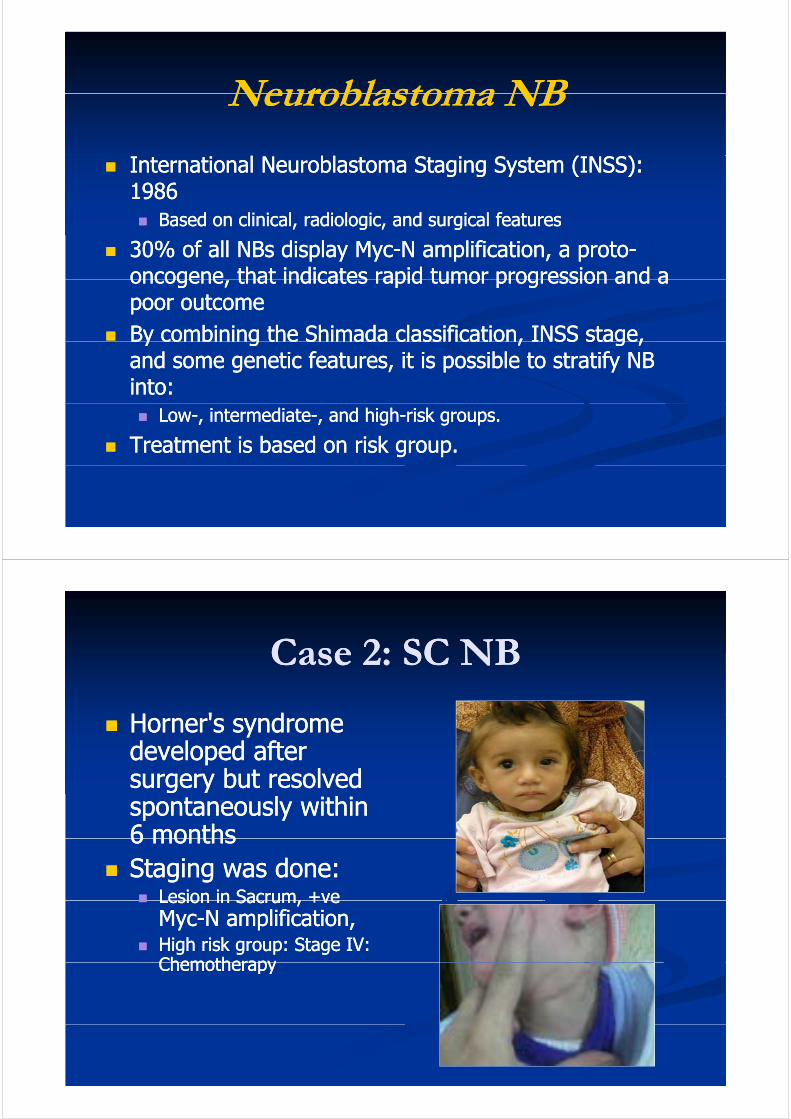
Case 2: SC NBCase 2: SC NBCase 2: SC NBCase 2: SC NB
H ' dH ' d Horner's syndrome Horner's syndrome developed after developed after surgery but resolvedsurgery but resolvedsurgery but resolved surgery but resolved spontaneously within spontaneously within 66 monthsmonths6 6 months months
Staging was done: Staging was done: Lesion in Sacrum, +veLesion in Sacrum, +ve Lesion in Sacrum, +ve Lesion in Sacrum, +ve
MycMyc--N amplification, N amplification, High risk group: Stage IV: High risk group: Stage IV:
ChemotherapyChemotherapyChemotherapyChemotherapy
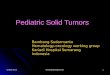
CaseCase 33: Teratoma: TeratomaCase Case 33: Teratoma: Teratoma
A A 15 15 year old male patient, presented with a year old male patient, presented with a left sided squint and diplopia of left sided squint and diplopia of 3 3 months months duration.duration.
On examination he had a left sided lateral On examination he had a left sided lateral rectus paralysis, left sided parapharyngeal rectus paralysis, left sided parapharyngeal swelling pushing the left tonsil medially, with a swelling pushing the left tonsil medially, with a g p g yg p g ymass in the left submandibular area, mass in the left submandibular area, 55xx55cm, cm, firm in consistency, non tender and non firm in consistency, non tender and non pulsatile. pulsatile.
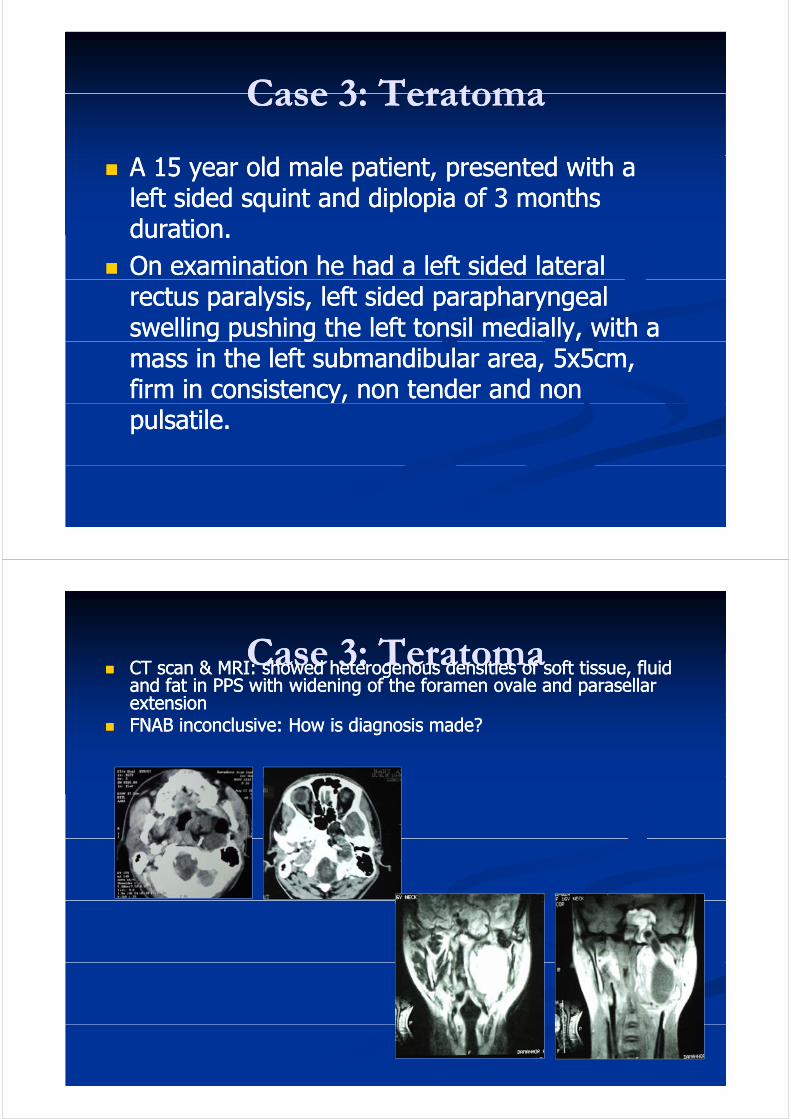
CaseCase 33: Teratoma: TeratomaCase Case 33: Teratoma: Teratoma CT scan & MRI: showed heterogenous densities of soft tissue, fluid CT scan & MRI: showed heterogenous densities of soft tissue, fluid
and fat in PPS with widening of the foramen ovale and parasellar and fat in PPS with widening of the foramen ovale and parasellar extensionextension
FNAB inconclusive: How is diagnosis made?FNAB inconclusive: How is diagnosis made?
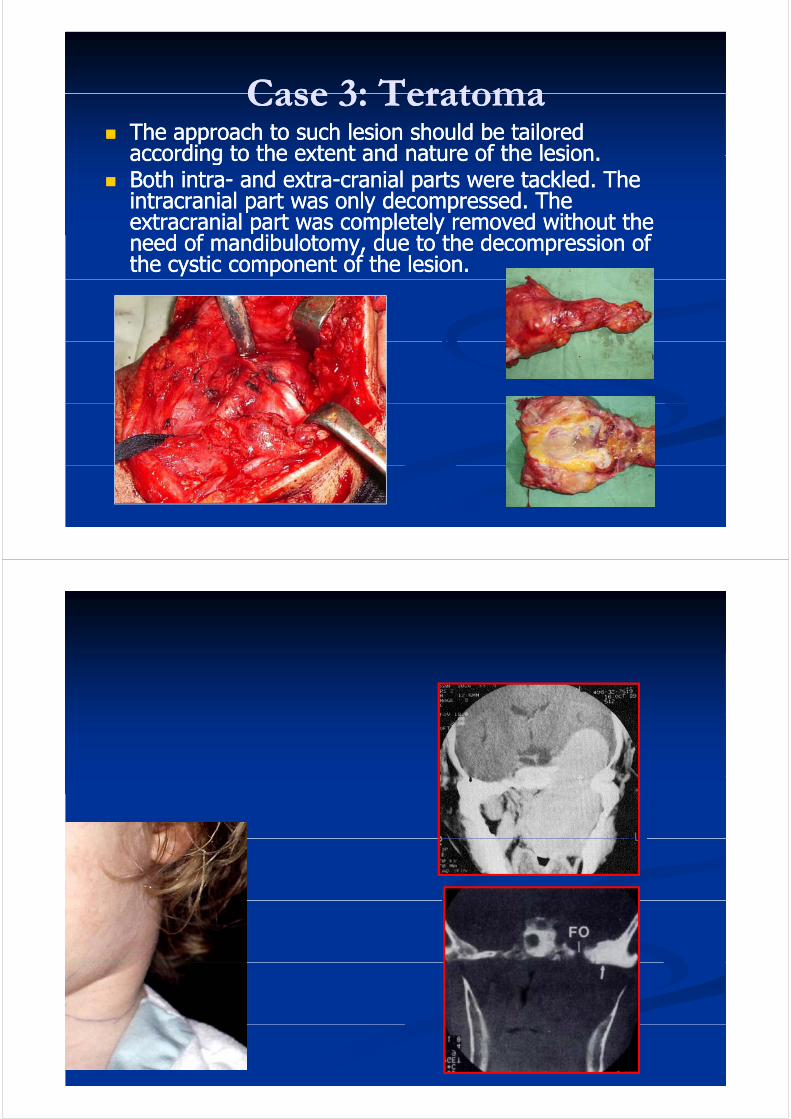
CaseCase 33: Teratoma: TeratomaCase Case 33: Teratoma: Teratoma The approach to such lesion should be tailored The approach to such lesion should be tailored
according to the extent and nature of the lesionaccording to the extent and nature of the lesionaccording to the extent and nature of the lesion. according to the extent and nature of the lesion. Both intraBoth intra-- and extraand extra--cranial parts were tackled. The cranial parts were tackled. The
intracranial part was only decompressed. The intracranial part was only decompressed. The e t ac anial pa t as completel emo ed itho t thee t ac anial pa t as completel emo ed itho t theextracranial part was completely removed without the extracranial part was completely removed without the need of mandibulotomy, due to the decompression of need of mandibulotomy, due to the decompression of the cystic component of the lesion.the cystic component of the lesion.
Pediatric Neck Mass
Congenital Acquired
Thyroglossal Duct Cyst
Infectious/Inflammatory
NeoplasmsBranchial cleft cyst
Cystic hygroma
Dermoid cyst
Diagnosis of Pediatric PPS NeoplasmsDiagnosis of Pediatric PPS NeoplasmsDiagnosis of Pediatric PPS NeoplasmsDiagnosis of Pediatric PPS Neoplasms
Sarcomas of the soft tissue and bone occur Sarcomas of the soft tissue and bone occur more commonly than malignant epithelial more commonly than malignant epithelial tumors within H&N region in childrentumors within H&N region in children
Rhabdomyosarcoma or lymphoma is the more Rhabdomyosarcoma or lymphoma is the more y y py y plikely diagnosis in younger children whereas NPC likely diagnosis in younger children whereas NPC is more common in adolescentsis more common in adolescents
Solid tumor of the MS in a child should prompt Solid tumor of the MS in a child should prompt the diagnosis of a sarcoma until proventhe diagnosis of a sarcoma until proventhe diagnosis of a sarcoma until proven the diagnosis of a sarcoma until proven otherwiseotherwise
Diagnosis of Pediatric PPS NeoplasmsDiagnosis of Pediatric PPS NeoplasmsDiagnosis of Pediatric PPS NeoplasmsDiagnosis of Pediatric PPS Neoplasms
AA-- Clinical Diagnosis:Clinical Diagnosis: Due to the rarity of these tumors, the clinical experience in Due to the rarity of these tumors, the clinical experience in
diagnosis and treatment of this condition is limiteddiagnosis and treatment of this condition is limitedd ag os s a d t eat e t o t s co d t o s tedd ag os s a d t eat e t o t s co d t o s ted The clinical symptoms of PPS tumors are versatile and nonThe clinical symptoms of PPS tumors are versatile and non--
specific, depending on the exact origin, nature and extensionsspecific, depending on the exact origin, nature and extensionsP t ti i ll d l d PPS i d l it t dP t ti i ll d l d PPS i d l it t d Presentation is usually delayed as PPS is deeply situated:Presentation is usually delayed as PPS is deeply situated: Tumors must be at least Tumors must be at least 22cm in size before causing a cm in size before causing a
detectable bulgedetectable bulge Unfortunately, malignant tumors tend to be locally advanced by Unfortunately, malignant tumors tend to be locally advanced by
the time they are diagnosedthe time they are diagnosed The therapeutic implications of a delayed diagnosis of malignantThe therapeutic implications of a delayed diagnosis of malignant The therapeutic implications of a delayed diagnosis of malignant The therapeutic implications of a delayed diagnosis of malignant
lesion in this area can be significantlesion in this area can be significant
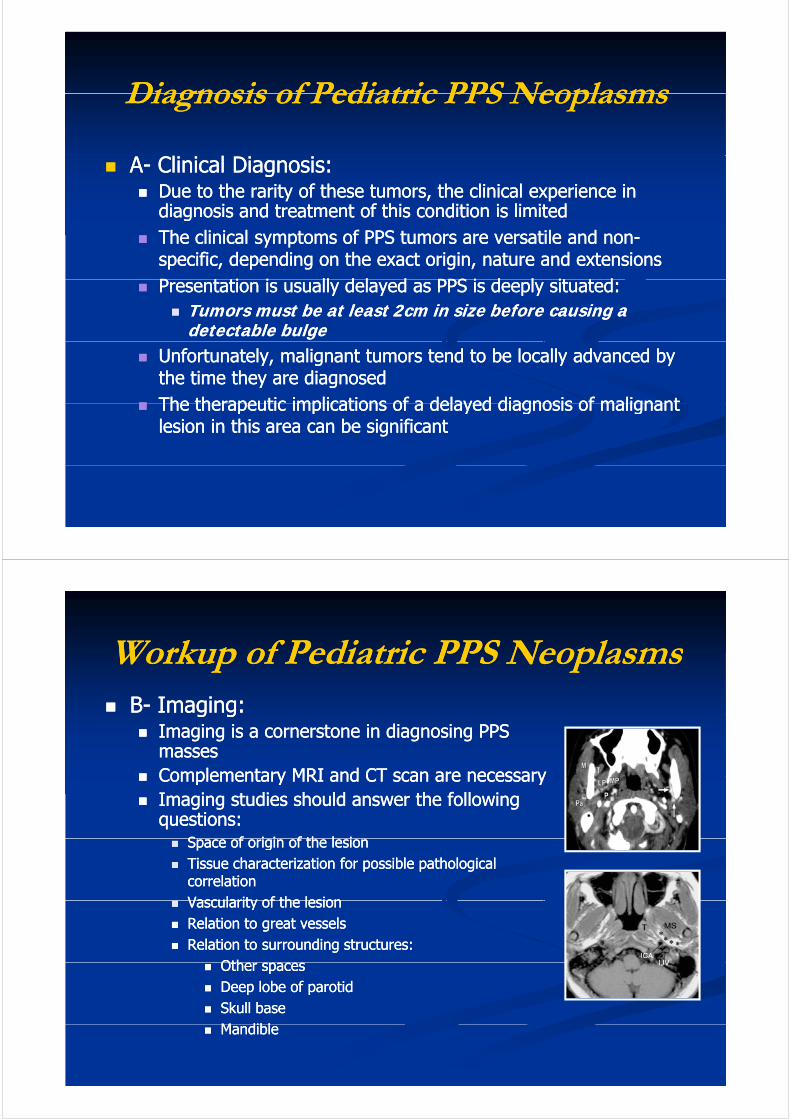
Workup of Pediatric PPS NeoplasmsWorkup of Pediatric PPS NeoplasmsWorkup of Pediatric PPS NeoplasmsWorkup of Pediatric PPS Neoplasms BB-- Imaging:Imaging:g gg g
Imaging is a cornerstone in diagnosing PPS Imaging is a cornerstone in diagnosing PPS massesmasses
Complementary MRI and CT scan are necessaryComplementary MRI and CT scan are necessary Complementary MRI and CT scan are necessary Complementary MRI and CT scan are necessary Imaging studies should answer the following Imaging studies should answer the following
questions:questions:S f i i f th l iS f i i f th l i Space of origin of the lesionSpace of origin of the lesion
Tissue characterization for possible pathological Tissue characterization for possible pathological correlationcorrelationVascularity of the lesionVascularity of the lesion Vascularity of the lesionVascularity of the lesion
Relation to great vesselsRelation to great vessels Relation to surrounding structures:Relation to surrounding structures:
OthOth Other spaces Other spaces Deep lobe of parotidDeep lobe of parotid Skull baseSkull base
M diblM dibl MandibleMandible
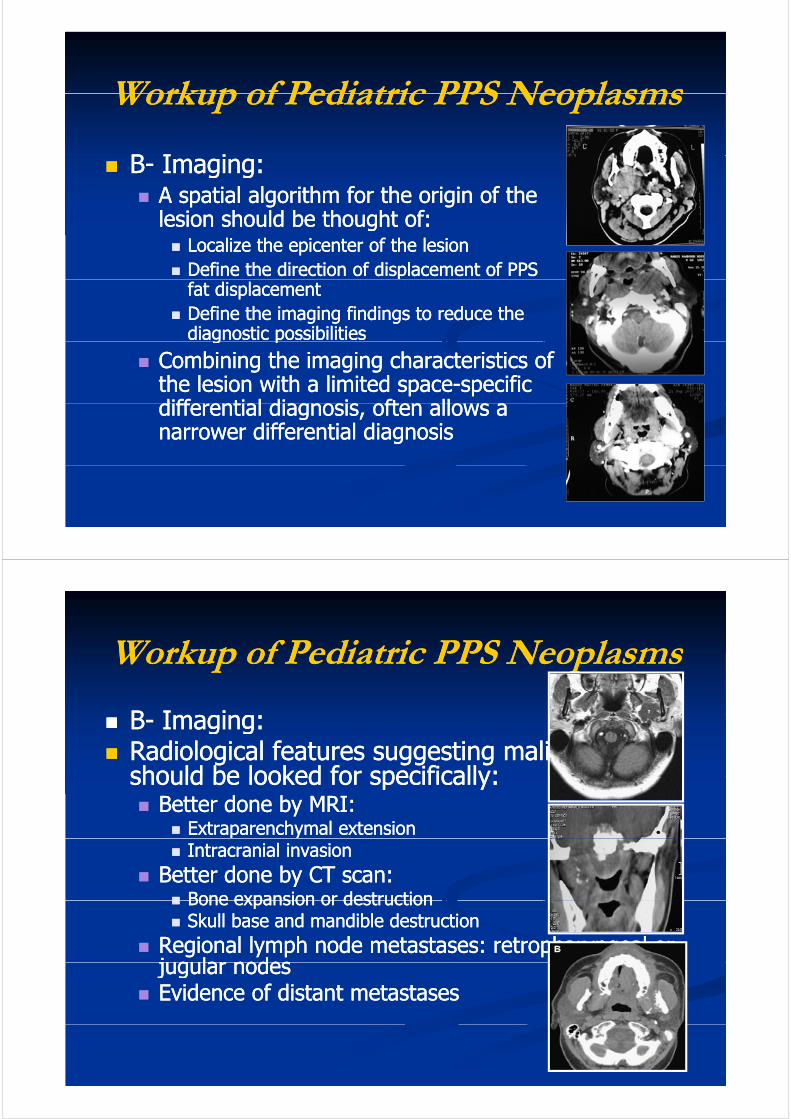
Workup of Pediatric PPS NeoplasmsWorkup of Pediatric PPS NeoplasmsWorkup of Pediatric PPS NeoplasmsWorkup of Pediatric PPS Neoplasms
BB I iI i BB-- Imaging:Imaging: A spatial algorithm for the origin of the A spatial algorithm for the origin of the
lesion should be thought of:lesion should be thought of:lesion should be thought of:lesion should be thought of: Localize the epicenter of the lesionLocalize the epicenter of the lesion Define the direction of displacement of PPS Define the direction of displacement of PPS pp
fat displacementfat displacement Define the imaging findings to reduce the Define the imaging findings to reduce the
diagnostic possibilitiesdiagnostic possibilitiesg pg p
Combining the imaging characteristics of Combining the imaging characteristics of the lesion with a limited spacethe lesion with a limited space--specific specific diffe enti l di gno i often llodiffe enti l di gno i often llodifferential diagnosis, often allows a differential diagnosis, often allows a narrower differential diagnosisnarrower differential diagnosis
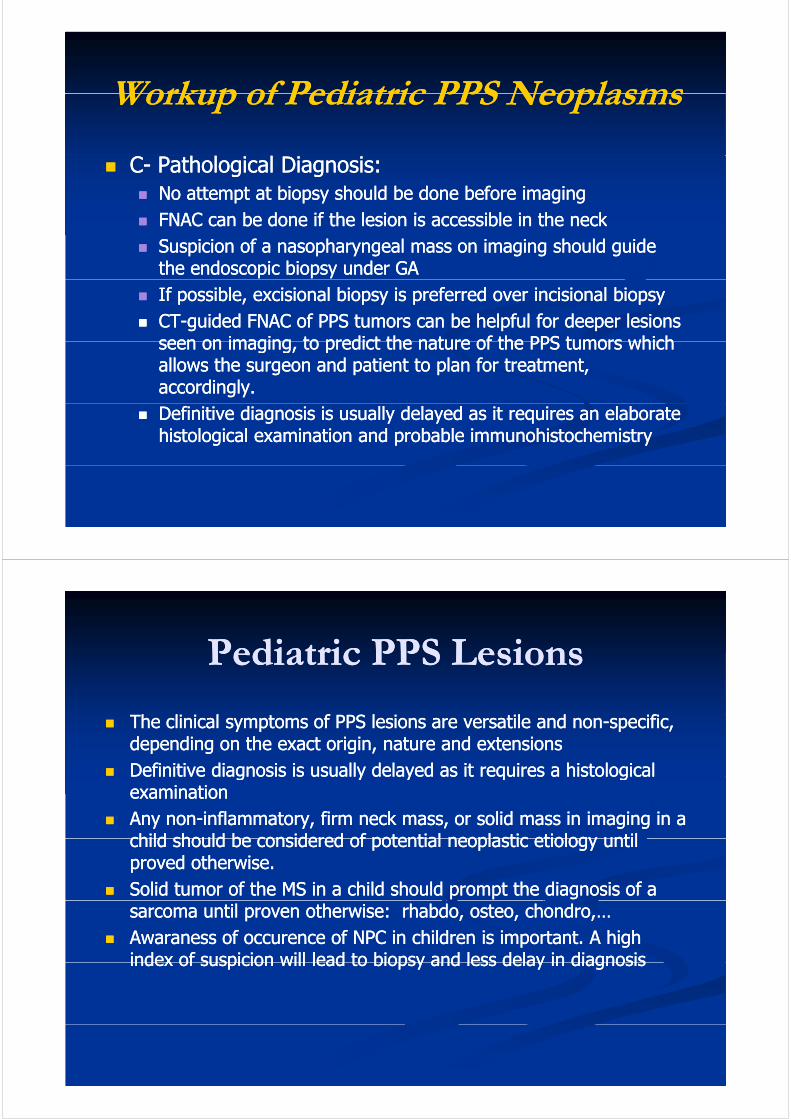
Workup of Pediatric PPS NeoplasmsWorkup of Pediatric PPS NeoplasmsWorkup of Pediatric PPS NeoplasmsWorkup of Pediatric PPS Neoplasms
BB I iI i BB-- Imaging:Imaging: Radiological features suggesting malignancy Radiological features suggesting malignancy
should be looked for specifically:should be looked for specifically:should be looked for specifically:should be looked for specifically: Better done by MRI:Better done by MRI:
Extraparenchymal extensionExtraparenchymal extension Intracranial invasionIntracranial invasion
Better done by CT scan:Better done by CT scan: Bone expansion or destructionBone expansion or destruction Bone expansion or destructionBone expansion or destruction Skull base and mandible destructionSkull base and mandible destruction
Regional lymph node metastases: retropharyngeal or Regional lymph node metastases: retropharyngeal or jugular nodesjugular nodesjugular nodes jugular nodes
Evidence of distant metastasesEvidence of distant metastases
Workup of Pediatric PPS NeoplasmsWorkup of Pediatric PPS NeoplasmsWorkup of Pediatric PPS NeoplasmsWorkup of Pediatric PPS Neoplasms
CC-- Pathological Diagnosis:Pathological Diagnosis: No attempt at biopsy should be done before imagingNo attempt at biopsy should be done before imaging
FNAC can be done if the lesion is accessible in the neckFNAC can be done if the lesion is accessible in the neck FNAC can be done if the lesion is accessible in the neckFNAC can be done if the lesion is accessible in the neck Suspicion of a nasopharyngeal mass on imaging should guide Suspicion of a nasopharyngeal mass on imaging should guide
the endoscopic biopsy under GAthe endoscopic biopsy under GA If possible, If possible, excisionalexcisional biopsy is preferred over biopsy is preferred over incisionalincisional biopsybiopsy CTCT--guided FNAC of PPS tumors can be helpful for deeper lesions guided FNAC of PPS tumors can be helpful for deeper lesions
seen on imaging to predict the nature of the PPS tumors whichseen on imaging to predict the nature of the PPS tumors whichseen on imaging, to predict the nature of the PPS tumors which seen on imaging, to predict the nature of the PPS tumors which allows the surgeon and patient to plan for treatment, allows the surgeon and patient to plan for treatment, accordingly. accordingly.
Definitive diagnosis is usually delayed as it requires an elaborate Definitive diagnosis is usually delayed as it requires an elaborate histological examination and probable histological examination and probable immunohistochemistryimmunohistochemistry
Pediatric PPS LesionsPediatric PPS LesionsPediatric PPS LesionsPediatric PPS Lesions
Th li i l f PPS l i il dTh li i l f PPS l i il d ifiifi The clinical symptoms of PPS lesions are versatile and nonThe clinical symptoms of PPS lesions are versatile and non--specific, specific, depending on the exact origin, nature and extensionsdepending on the exact origin, nature and extensions
Definitive diagnosis is usually delayed as it requires a histological Definitive diagnosis is usually delayed as it requires a histological e t e d ag os s s usua y de ayed as t equ es a sto og cae t e d ag os s s usua y de ayed as t equ es a sto og caexamination examination
Any nonAny non--inflammatory, firm neck mass, or solid mass in imaging in a inflammatory, firm neck mass, or solid mass in imaging in a child should be considered of potentialchild should be considered of potential neoplasticneoplastic etiology untiletiology untilchild should be considered of potential child should be considered of potential neoplasticneoplastic etiology until etiology until proved otherwise.proved otherwise.
Solid tumor of the MS in a child should prompt the diagnosis of a Solid tumor of the MS in a child should prompt the diagnosis of a sarcoma until proven otherwise: sarcoma until proven otherwise: rhabdorhabdo, , osteoosteo, , chondrochondro,…,…
AwaranessAwaraness of of occurenceoccurence of NPC in children is important. A high of NPC in children is important. A high index of suspicion will lead to biopsy and less delay in diagnosisindex of suspicion will lead to biopsy and less delay in diagnosisindex of suspicion will lead to biopsy and less delay in diagnosis index of suspicion will lead to biopsy and less delay in diagnosis
Pediatric PPS NeoplasmsPediatric PPS NeoplasmsPediatric PPS NeoplasmsPediatric PPS Neoplasms
N k i hild h id diff ti lN k i hild h id diff ti lTake Home Message
Neck mass in children have a wide differential, Neck mass in children have a wide differential, age at presentation is importantage at presentation is important
Although rare malignant tumors of PPS doesAlthough rare malignant tumors of PPS does Although rare, malignant tumors of PPS does Although rare, malignant tumors of PPS does occur in childrenoccur in children
Pediatric malignant tumors of the head and neckPediatric malignant tumors of the head and neck Pediatric malignant tumors of the head and neck Pediatric malignant tumors of the head and neck are basically curable, if early discoveredare basically curable, if early discovered
Awareness of occurrence of malignant tumors in Awareness of occurrence of malignant tumors in ggH&N and PPS in children, by the clinician is H&N and PPS in children, by the clinician is crucialcrucialCareful evaluation for radiographic features ofCareful evaluation for radiographic features of Careful evaluation for radiographic features of Careful evaluation for radiographic features of malignancy by the radiologist is essentialmalignancy by the radiologist is essential
Pediatric PPS NeoplasmsPediatric PPS NeoplasmsPediatric PPS NeoplasmsPediatric PPS Neoplasms
AA i fl t fi k lidi fl t fi k lid
Take Home Message
Any nonAny non--inflammatory, firm neck mass, or solid inflammatory, firm neck mass, or solid mass in imaging in a child should be considered mass in imaging in a child should be considered of potential neoplastic etiology until provedof potential neoplastic etiology until provedof potential neoplastic etiology until proved of potential neoplastic etiology until proved otherwiseotherwise
Rare PPS location of uncommon lesions givesRare PPS location of uncommon lesions gives Rare PPS location of uncommon lesions, gives Rare PPS location of uncommon lesions, gives rise to difficulty in diagnosis, and final diagnosis rise to difficulty in diagnosis, and final diagnosis is not made until excised tumor is examinedis not made until excised tumor is examinedis not made until excised tumor is examined is not made until excised tumor is examined pathologicallypathologically
A high index of suspicion will lead to less delayA high index of suspicion will lead to less delay A high index of suspicion will lead to less delay A high index of suspicion will lead to less delay in diagnosis and better prognosisin diagnosis and better prognosis
ESENTASEgyptian Society of Ear, Nose, Throat and Allied Sciences
Welcome membershipWelcome membership Site www.esentas.org
Journal EJENTAS Journal EJENTAS
Alexandria ORL, April 2010
Pediatric Parapharyngeal Tumors
THANK YOU
Ossama A.Hamid, MDOssama A.Hamid, MDProfessor Otolaryngology, Head-Neck SurgeryAin Shams Universitywww.entainshams-egypt.com
ESENTASGS: Egyptian Society of Ear, Nose, Throat and Allied Sciences ESENTASwww.esentas.org
ESENTAS
g