Embed Size (px)
DESCRIPTION
Citation preview

Pediatric RadiologyPediatric RadiologyPediatric RadiologyPediatric Radiology

Indications for Pediatric Radiographic Examination
• History• Will the imaging give you any added
clinical data?• Benefits vs. risk
– American College of Radiology (ACR) Appropriateness Criteria available at www.acr.org

• All radiological exams carry risk• gonads• breast• thyroid• lung• Bone
The concept of ALARA (as low as reasonably achievable) should be
applied to all patients…

Radiation Exposure - Children
• Considerably more sensitive to radiation than adults
• Also have a longer life expectancy– a larger window of opportunity for
expressing radiation damage
Compared with a 40-year old, the same radiation dose given to a neonate is several times more likely
to produce a cancer over the patient’s lifetime
Retrieved 01-17-05 from http://www.cancer.gov/cancertopics/causes/radiation-risks-pediatric-CT

Never radiograph routinely!
• Will the results change my management?
• Will the study confirm my clinical suspicions?
• Is this the appropriate study for what I’m trying to confirm?

Technical Issues
• Instructional compliance• Motion
– The child should be stabilized by the parent
• Recumbent radiographs a necessity in young children– acute fractures

uprightupright recumbentrecumbent

• Must know the normal radiographic appearance at each age for accurate interpretation– Atlas of normal developmental anatomy– Consult a DACCBR?
• Chiropractic line analysis– Children are not small adults…
Does the technique recognize this?
Radiographic Interpretation

Normal Pediatric Variants
• Pseudosubluxation• Pseudospread of C1 on C2• ADI space• Absence of cervical lordosis• Normal appearance of ossification
centers and epiphyses

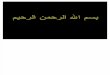
Pseudosubluxation
• Normal variant• Occurs most commonly at C2/C3
– 40% of normal children <7 years of age– 24% of those under 16 years
• Also occurs at C3/C4– 20% of those <7 years; 9% <16 years
http://www.medcyclopaedia.com/library/topics/volume_vii/p/pseudosubluxation.aspx

• A line drawn connecting the anterior cortices of the spinous processes of C1 and C3 should intersect or lie within 1 mm of the anterior cortex of the spinous process of C2
• If C2 is >2mm off of this line = true injury
http://www.uth.tmc.edu/radiology/test/er_primer/spine/images/csp40.html
http://www.medcyclopaedia.com/library/topics/volume_vii/p/pseudosubluxation.aspx
Swischuk's line distinguishes pseudosubluxation from pathological subluxation


Pseudospread of C1 on C2
• Normal variant• Lateral mass displacement relative
to the dens – Up to 6mm is common <4 yoa– Can be seen up to 7 yoa
Lustrin ES, Karakas SP, Ortiz AO et al. Pediatric Cervical Spine: Normal Anatomy, Variants and Trauma. RadioGraphics 2003; 23:539-60.

Pseudospread of C1 on C2
Lustrin ES, Karakas SP, Ortiz AO et al. Pediatric Cervical Spine: Normal Anatomy, Variants and Trauma. RadioGraphics 2003; 23:539-60.

Other Common Variants• ADI space
– Maximum of 4mm (new literature) in children
• Absence of cervical lordosis– Can be seen in children up to 16 yoa
• Oval/wedge shaped vertebrae are normal– Not to be confused with compression fx
• Normal appearance of ossification centers and epiphyses can simulate fractures…
Lustrin ES, Karakas SP, Ortiz AO et al. Pediatric Cervical Spine: Normal Anatomy, Variants and Trauma. RadioGraphics 2003; 23:539-60.

Copyright ©Radiological Society of North America, 2003
Lustrin, E. S. et al. Radiographics 2003;23:539-560
Figure 1b
synchondrosis

Copyright ©Radiological Society of North America, 2003
Lustrin, E. S. et al. Radiographics 2003;23:539-560
Figure 4

• The spaces between the sacral segments are synchondroses composed of fibrocartilage, not discs– Bone starts to be deposited in the
fibrocartilage starting at puberty
*They do not move like vertebrae…
Gray, Henry. Anatomy of the Human Body. Philadelphia: Lea & Febiger, 1918; Bartleby.com, 2000. www.bartleby.com/107/. [January 20, 2006].
http://www.bio.psu.edu/people/faculty/strauss/anatomy/skel/sacrum2.htm

Where is the anomaly?

Os Odontoideum
• Results from injury at the odontoid synchondrosis
• Flexion/extension radiographs• Neurological deficit?• Neurologist/orthopedist consult

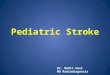
Epiphyseal Plate Injuries
Salter-Harris Classification

http://xray.20m.com/photo4.html

Child Abuse
• Physical, sexual, nutritional abuse or neglect
Must report to appropriate agency!
– Remain professional and objective– Be non-judgemental toward parents

Radiography plays an important part in documenting physical abuse
• Technical considerations– reveal soft tissues well– high detail radiographs – sectionals, not “babygram”

Battered child syndrome
• Metaphyseal “corner” fractures• Multiple fractures at various stages of
healing• Ribs, scapula• Head injuries
– Skull fx, subdural hematoma, shearing injuries*MC cause of death + disability in child abuse
• Soft tissue swelling and injuries – i.e. contusions, burns, etc.

Oblique fractureOblique fracture
Periosteal reactionPeriosteal reaction
Metaphyseal corner fxMetaphyseal corner fx

Linear skull fracturesLinear skull fractures
Multiple metacarpal Multiple metacarpal fracturesfractures

Rib fractures– Especially posterior aspect

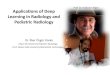
Hx: 2 yo with vomiting and diarrhea
Initial abdomen and chest films normal
Increased WBC
Elevated ESR
Findings:
-decreased disc height
-abnormal signal in two adjacent VB
-paraspinal mass
Dx: discitis
Swischuk LE. Vomiting, diarrhea and--oh! oh! what is that? Pediatr Emerg Care. 2004 Jan;20(1):54-6

Spinal infectionDiscitis• A common problem in infants• MC lumbar region, lower thoracics
• S/S: back pain (often can’t directly communicate) and difficulty walking or limping
Therefore, when one has exhausted all of the more common causes of limping, one should look to the lower thoracic and lumbar spine regions for the presence of discitis.
Swischuk LE. Vomiting, diarrhea and--oh! oh! what is that? Pediatr Emerg Care. 2004 Jan;20(1):54-6