Embed Size (px)
Citation preview
Percutaneous Endoscopic Gastrostomy Tube Placement in a Surgical Training Program James B. Lowe, MD, Carey P. Page, MD, Wayne H. Schwesinger, MD, Harold V. Gaskill, MD,
Jay S. Stauffer, MD, San Antonio, Texas
BACKGROUND: This study examines the patterns of use of percutaneous endoscopic gastrostomy (PEG) and primary open gastrostomy (Gtube) per- formed in a residency training program in sur- gery.
METHODS: A retrospective cohort study that as- sesses the indications and outcomes of 317 PEGS and 75 isolated Gtubes used for gastric access between1987and1997.
RESULTS: The demographics and risk factors of the patients receiving Gtube and PEG were com- parable. The mean number of PEGS performed per resident is currently 13 per year (mean 5 over 10 years) with a 97% PEG success rate; an 88% success rate is demonstrated for placement of jejunal extensions.
CONCLUSIONS: PEGS are generally preferable to Gtubes as primary procedures. Surgical residents should become competent in PEG placement by performing adequate numbers of procedures with fully trained staff. Am J Surg. 1997;174:624-628. 0 1997 by Excerpta Medica, Inc.
P
ercutaneous endoscopic gastrostomy (PEG), first de- scribed by Ponsky and Gauderer’ in 1980, has largely supplanted open gastrostomy (Gtube) in many clini-
cal situations.2-4 The relative ease of the technique, its low complication rate, and the trend toward minimally invasive operations that avoid general anesthesia are all factors in its wider application. 4-8 While nationwide the majority of PEGS are performed by gastroenterologists,9.10 in our surgi- cal training program, residents are instructed in both the PEG and Gtube technique. The PEG technique is taught during an endoscopy rotation proctored by surgical endos- copists in the PG III or PG IV year, and open gastrostomies are taught as a component of regular rotations on general surgery services.
This communication describes our use of the two tech- niques during the last 10 years, examines their relative mer- its, and highlights the legitimate role of the PEG technique in surgical training programs. We emphasize that both tech- niques are often used in high-risk patients who are prone to both complications and death, but that neither tech-
From the Department of Surgery, University of Texas Health Sci- From the Department of Surgery, University of Texas Health Sci- ence Center at San Antonio, Texas. ence Center at San Antonio, Texas.
Requests for reprints should be addressed to Carey P. Page, Requests for reprints should be addressed to Carey P. Page, MD, UTHSCSA-Surgery, 7703 Floyd Curl Drive, San Antonio, MD, UTHSCSA-Surgery, 7703 Floyd Curl Drive, San Antonio, Texas 78284. Texas 78284.
Presented at the 49th Annual Meeting of the Southwestern Sur- Presented at the 49th Annual Meeting of the Southwestern Sur- gical Congress, Ranch0 Mirage, California, April 13-l 6, 1997. gical Congress, Ranch0 Mirage, California, April 13-l 6, 1997.
I
nique is usually responsible for these adverse outcomes. Based on our experience, we believe that primary Gtube placement should become a surgical rarity, relegated to in- stances in which a PEG cannot be placed or is contrain- dicated.
MATERIALS AND METHODS Our surgical database concurrently captures our operative
experience, affiliated complications, and associated treat- ment outcomes. It also reports a variety of patient-related demographics, laboratory and risk data, antibiotic prophy- laxis, case distribution, technical aspects, and associated procedures. It is based on a preliminary operation report form and a series of standardized, weekly reports of patient outcomes by each of our operating services. This database, detailed weekly morbidity and mortality conference minutes (M&M), and selective review of charts and oper- ative notes form the basis for this report. The data cover the interval from January 1987, the date of our first surgical PEG, through December 1996.
We included PEGS or primary Gtubes performed by resi- dents with direct faculty supervision on adolescent or adult patients at our two primary teaching hospitals. The PEGS were placed using commercially available kits via a previ- ously described technique.6.‘1’” The Gtubes were placed us- ing a standard “Stamm” technique.“,‘4 For each of these groups, we categorized both the indication for the procedure (feeding or decompression) and the affiliated condition for which it was placed (eg, cancer or neurological compro- mise). We categorized complications relating to the gas- trostomy tube (surgical site infection, leakage, tube dis- lodgment, access failure, pneumonia, and death).“,” Preexisting complications that prompted the tube place- ment were not included and minor complications (ie, ate- lectasis, transient fever, and urinary tract infection) were not collated. However, failure to establish access by PEG or failure to provide a jejunal extension were noted as com- plications. Both morbidity and mortality were classified as gastrostomy related or non-gastrostomy related. The Amer- ican Society of Anesthesiology (ASA) score and serum al- bumin at the time of the procedure were recorded as a sur- rogates for overall risk.
Data were analyzed by the chi-square test for nominal ob- servations and by Student’s t test for parametric data among unequal groups. Significance was defined as P value < 0.05.
RESULTS Between 1987 and 1997, 372 patients underwent a total
of 3 17 PEG and 75 Gtube procedures. Many were high-risk patients with complex hospital courses (Table I). Of the 162 patients admitted for trauma, head injury was the dom-
624 0 1997 by Excerpta Medica, Inc. 0002-961 O/97/$17.00
All rights reserved. PII SOOO2-9610(97)00177-3
PEG TUBE PLACEMENT IN SURGICAL TRAINING/LOWE ET AL
inant feature in 148 (91.4%). There were also 145 patients with advanced malignancies; those with head and neck cancers represented the largest single group. Overall, the 372 patients underwent a total of 474 operations in addition to gastrostomy during their index hospital admission. Major complications were recorded in 105 (28%) of the patients, and 22 of them (7%) died. Twenty of the deaths were at- tributable to the patient’s underlying condition, 5 died from cancer, 7 from sepsis, 6 from pulmonary failure, and 2 from cardiac events.
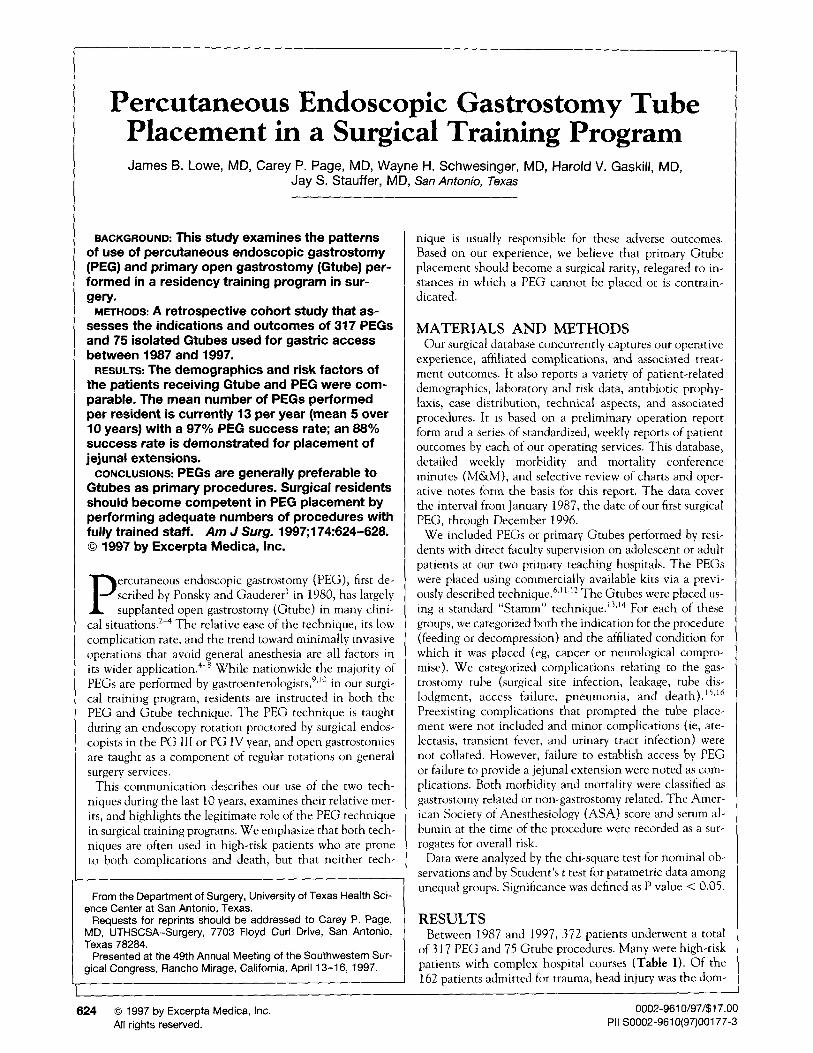
Primary gastrostomy was used for both feeding and for decompression. Our use of primary Gtube and PEG and our historical baseline use for Gtube are depicted in Figure 1. Patient characteristics, selected risk factors, and selected details of the operations are presented in Table I. The ages of the patients, the indications for the primary gastrostomy and the ASA risk classifications were similar between the two groups. Gtube procedures were more likely to involve junior house officers, require general anesthesia, and be as- sociated with perioperative antibiotics. They also averaged longer operative times. Eighty-five PEG procedures were also performed under general anesthesia, mostly in victims of trauma who had head injuries and required concomitant tracheostomy.
Table II presents the complications attributable to the Gtube and PEG. The PEG placement initially failed in 11 patients (3.5%). In 3, a second attempt was successful; a Gtube was inserted in 2 others. The single dislodged Gtube was replaced through a mature stoma site. Of the 7 PEGS that were inadvertently or prematurely withdrawn, 4 were replaced with a second PEG and 3 were converted to a Gtube. In 2 of these latter cases, the PEGS had been elec- tively removed. Gtube subsequently became necessary be- cause treatment of their head and neck cancer failed, and
Year
Figure 1. Gtube and PEG over time. Our historical use of primary gastrostomy. Over time, PEG has come to dominate and expand our use of primary gastrostomy.
we were unable to pass an endoscope into the stomach. Placement of a jejunal extension was attempted in 116 pa- tients and was initially successful in 97 (84%). Repeat en- doscopy was successful in another 5 patients (88% ultimate success rate). Placement of a jejunal extension was not achieved in 11 patients in whom it was considered desir- able.
Aspiration pneumonia was documented in 4 patients (1 Gtube and 3 PEG), and surgical site infection (SSI) was noted in 3 Gtube patients and 9 PEG patients. Site infec- tion was controlled in each case by local drainage. Three of the PEG patients and all of the Gtube patients had re- ceived perioperative antibiotics. Though antibiotics were more commonly used in the Gtube patients than PEG pa- tients (87% versus 48%, P = < O.OOl), the risk of SSI was essentially the same (4% versus 3%).
Gastrostomy leaks were identified in 2 patients in each of the Gtube and PEG groups. In 1 Gtube patient, the leakage
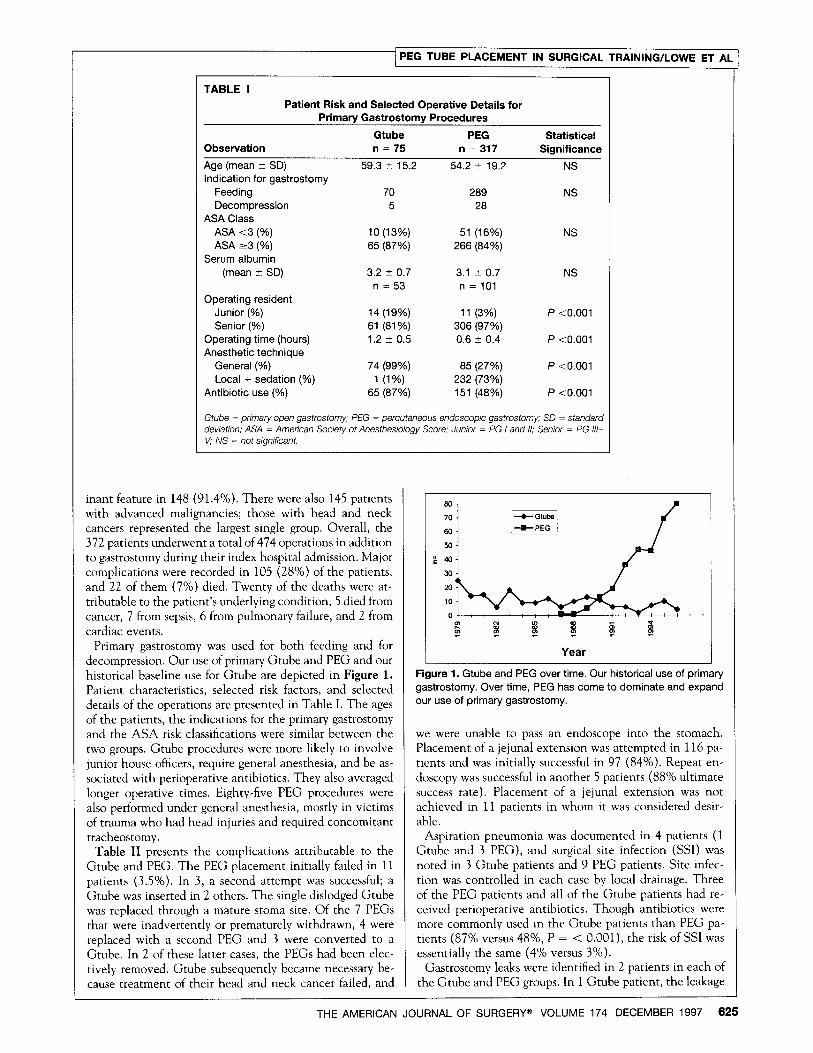
TABLE I
Patient Risk and Selected Operative Details for Primary Gastrostomy Procedures
Observation
Age (mean t SD) Indication for gastrostomy
Feeding Decompression
ASA Class ASA <3 (%) ASA 23 (%)
Serum albumin (mean t SD)
Operating resident Junior (%) Senior (%)
Operating time (hours) Anesthetic technique
General (%) Local + sedation (%)
Antibiotic use (%)
Gtube PEG n = 75 n = 317
59.3 5 15.2 54.2 2 19.2
70 289 5 28
10 (13%) 51 (16%) 65 (87%) 266 (84%)
3.2 T 0.7 3.1 + 0.7 n = 53 n = 101
14 (19%) 11 (3%) 61 (81%) 306 (97%) 1.2 2 0.5 0.6 i- 0.4
74 (99%) 85 (27%) 1 (1%) 232 (73%)
65 (87%) 151 (48%)
Statistical Significance
NS
NS
NS
NS
P <O.OOl
P <O.OOl
P <O.OOl
P <O.OOl
Gtube = prtmary open gastrostomy; PEG = percutaneous endoscopic gastrostomy; SD = standard deviation: ASA = American Society of Anesthesiology Score; Junior = PG I and 0; Senior = PG l/l- V; MS = not significant.
THE AMERICAN JOURNAL OF SURGERY@ VOLUME 174 DECEMBER 1997 625
PEG TUBE PLACEMENT IN Sm
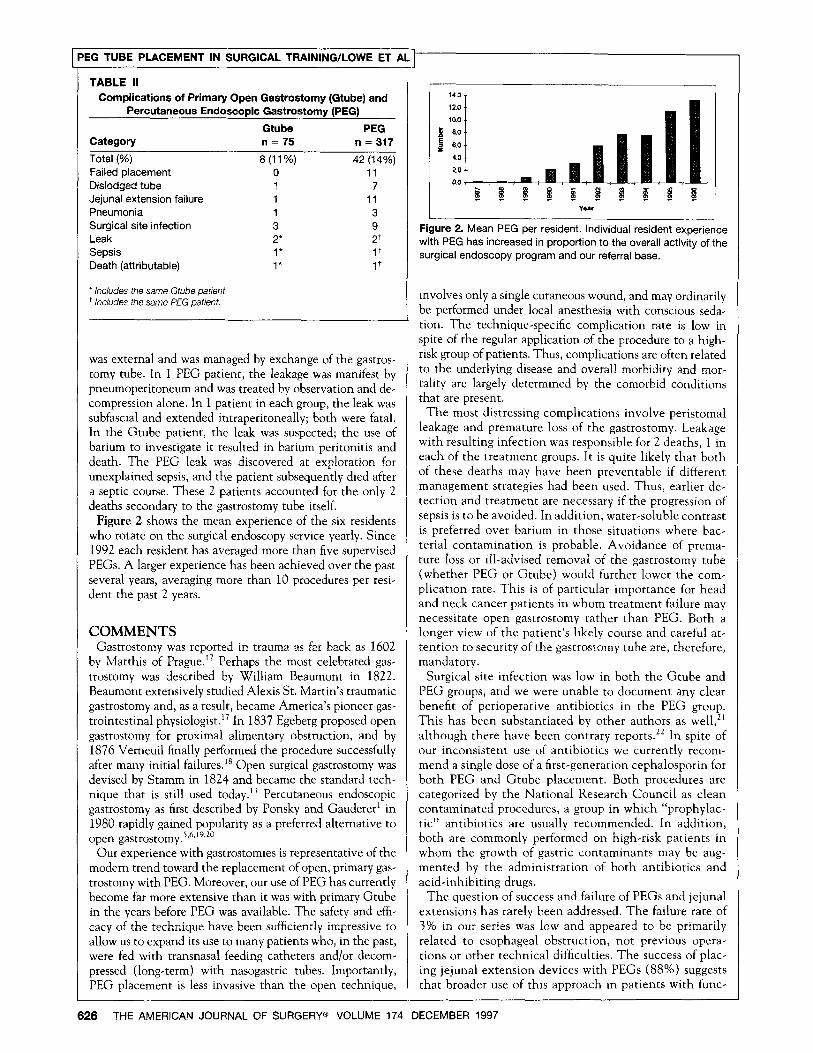
TABLE II Complications of Primary Open Gastrostomy (G&be) and
Percutaneous Endoscopic Gastrostomy (PEG)
Gtube PEG Category n = 75 n = 317
Total (%) 8 (11%) 42 (14%) Failed placement 0 11 Didodged tube 1 7 Jejunal extension failure 1 11 Pneumonia 1 3 Surgical site infection 3 9 Leak 2’ 2+ Sepsis 1* 1+ Death (attributable) 1’ 1+
’ includes the same Gtube patient. + includes the same PEG patient.
was external and was managed by exchange of the gastros- tomy tube. In I PEG patient, the leakage was manifest by pneumoperitoneum and was treated by observation and de- compression alone. In 1 patient in each group, the leak was subfascial and extended intraperitoneally; both were fatal. In the Gtube patient, the leak was suspected; the use of barium to investigate it resulted in barium peritonitis and death. The PEG leak was discovered at exploration for unexplained sepsis, and the patient subsequently died after a septic course. These 2 patients accounted for the only 2 deaths secondary to the gastrostomy tube itself.
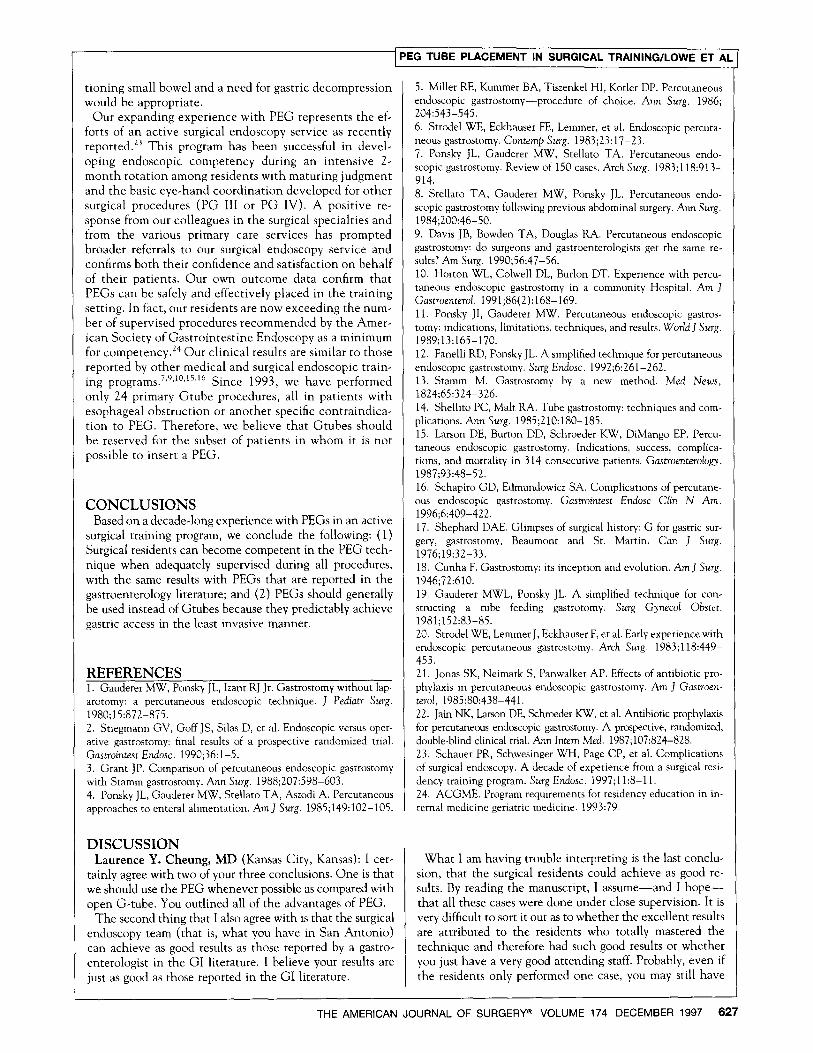
Figure 2 shows the mean experience of the six residents who rotate on the surgical endoscopy service yearly. Since 1992 each resident has averaged more than five supervised PEGS. A larger experience has been achieved over the past several years, averaging more than 10 procedures per resi- dent the past 2 years.
COMMENTS Gastrostomy was reported in trauma as far back as 1602
by Matthis of Prague.i’ Perhaps the most celebrated gas- trostomy was described by William Beaumont in 1822. Beaumont extensively studied Alexis St. Martin’s traumatic gastrostomy and, as a result, became America’s pioneer gas- trointestinal physiologist.i7 In 1837 Egeberg proposed open gastrostomy for proximal alimentary obstruction, and by 1876 Vemeuil finally performed the procedure successfully after many initial failuresI Open surgical gastrostomy was devised by Stamm in 1824 and became the standard tech- nique that is still used today.13 Percutaneous endoscopic gastrostomy as first described by Ponsky and Gaudereri in 1980 rapidly gained popularity as a preferred alternative to open gastrostomy.5,6X*9*2C
Our experience with gastrostomies is representative of the modern trend toward the replacement of open, primary gas- trostomy with PEG. Moreover, our use of PEG has currently become far more extensive than it was with primary Gtube in the years before PEG was available. The safety and effi- cacy of the technique have been sufficiently impressive to allow us to expand its use to many patients who, in the past, were fed with transnasal feeding catheters and/or decom- pressed (long-term) with nasogastric tubes. Importantly, PEG placement is less invasive than the open technique,
Figure 2. Mean PEG per resident. Individual resident experience with PEG has increased in proportion to the overall activity of the surgical endoscopy program and our referral base.
involves only a single cutaneous wound, and may ordinarily be performed under local anesthesia with conscious seda- tion. The technique-specific complication rate is low in spite of the regular application of the procedure to a high- risk group of patients. Thus, complications are often related to the underlying disease and overall morbidity and mor- tality are largely determined by the comorbid conditions that are present.
The most distressing complications involve peristomal leakage and premature loss of the gastrostomy. Leakage with resulting infection was responsible for 2 deaths, 1 in each of the treatment groups. It is quite likely that both of these deaths may have been preventable if different management strategies had been used. Thus, earlier de- tection and treatment are necessary if the progression of sepsis is to be avoided. In addition, water-soluble contrast is preferred over barium in those situations where bac- terial contamination is probable. Avoidance of prema- ture loss or ill-advised removal of the gastrostomy tube (whether PEG or Gtube) would further lower the com- plication rate. This is of particular importance for head and neck cancer patients in whom treatment failure may necessitate open gastrostomy rather than PEG. Both a longer view of the patient’s likely course and careful at- tention to security of the gastrostomy tube are, therefore, mandatory.
Surgical site infection was low in both the Gtube and PEG groups, and we were unable to document any clear benefit of perioperative antibiotics in the PEG group. This has been substantiated by other authors as well,” although there have been contrary reports.‘* In spite of our inconsistent use of antibiotics we currently recom- mend a single dose of a first-generation cephalosporin for both PEG and Gtube placement. Both procedures are categorized by the National Research Council as clean contaminated procedures, a group in which “prophylac- tic” antibiotics are usually recommended. In addition, both are commonly performed on high-risk patients in whom the growth of gastric contaminants may be aug- mented by the administration of both antibiotics and acid-inhibiting drugs.
The question of success and failure of PEGS and jejunal extensions has rarely been addressed. The failure rate of 3% in our series was low and appeared to be primarily related to esophageal obstruction, not previous opera- tions or other technical difficulties. The success of plac- ing jejunal extension devices with PEGS (88%) suggests that broader use of this approach in patients with func-
626 THE AMERICAN JOURNAL OF SURGERYa VOLUME 174 DECEMBER 1997
[PEG TUBE PLACEMENT IN SURGICAL TRAINING/LOWE ET AL
tioning small bowel and a need for gastric decompression would be appropriate.
Our expanding experience with PEG represents the ef- forts of an active surgical endoscopy service as recently reported.23 This program has been successful in devel- oping endoscopic competency during an intensive Z- month rotation among residents with maturing judgment and the basic eye-hand coordination developed for other surgical procedures (PG III or PG IV). A positive re- sponse from our colleagues in the surgical specialties and from the various primary care services has prompted broader referrals to our surgical endoscopy service and confirms both their confidence and satisfaction on behalf of their patients. Our own outcome data confirm that PEGS can be safely and effectively placed in the training setting. In fact, our residents are now exceeding the num- ber of supervised procedures recommended by the Amer- ican Society of Gastrointestine Endoscopy as a minimum for competency. 24 Our clinical results are similar to those reported by other medical and surgical endoscopic train- ing programs.‘~9~‘“~15~‘6 Since 1993, we have performed only 24 primary Gtube procedures, all in patients with esophageal obstruction or another specific contraindica- tion to PEG. Therefore, we believe that Gtubes should be reserved for the subset of patients in whom it is not possible to insert a PEG.
CONCLUSIONS Based on a decade-long experience with PEGS in an active
surgical training program, we conclude the following: (1) Surgical residents can become competent in the PEG tech- nique when adequately supervised during all procedures, with the same results with PEGS that are reported in the gastroenterology literature; and (2) PEGS should generally be used instead of Gtubes because they predictably achieve gastric access in the least invasive manner.
REFERENCES 1. Gauderer MW, Ponsky JL, lzant RJ Jr. Gastrostomy without lap- arotomy: a percutaneous endoscopic technique. J Pediatr Surg. 1980;15:872-875. 2. Stiegmann GV, Goff JS, Silas D, et al. Endoscopic versus oper- ative gastrostomy: fmal results of a prospective randomized trial. Gastrointest Endosc. 1990;36:1-5. 3. Grant JP. Comparison of percutaneous endoscopic gastrostomy with Stamm gastrostomy. Ann Surg. 1988;207:598-603. 4. Ponsky JL, Gauderer MW, Stellaco TA, Aszodi A. Percutaneous approaches to enteral alimentation. Am J Surg. 1985;149:102-105.
DISCUSSION Laurence Y. Cheung, MD (Kansas City, Kansas): I cer-
tainly agree with two of your three conclusions. One is that we should use the PEG whenever possible as compared with open G-tube. You outlined all of the advantages of PEG.
The second thing that I also agree with is that the surgical endoscopy team (that is, what you have in San Antonio) can achieve as good results as those reported by a gastro- enterologist in the GI literature. I believe your results are just as good as those reported in the GI literature.
5. Miller RE, Kummer BA, Tiszenkel HI, Kotler DP. Percutaneous endoscopic gastrostomy-procedure of choice. Ann Surg. 1986; 204:543-545. 6. Strode1 WE, Eckhauser FE, Lemmer, et al. Endoscopic percuta- neous gastrostomy. Contemp Surg. 1983;23:17-23. 7. Ponsky JL, Gauderer MW, Stellato TA. Percutaneous endo- scopic gastrostomy. Review of 150 cases. Arch Surg. 1983;118:913- 914. 8. Stellato TA, Gauderer MW, Ponsky JL. Percutaneous endo- scopic gastrostomy following previous abdominal surgery. Ann Surg. 1984;200:46-50. 9. Davis JB, Bowden TA, Douglas RA. Percutaneous endoscopic gastrostomy: do surgeons and gastroenterologists get the same re- sults? Am Surg. 1990;56:47-56. 10. Horton WL, Colwell DL, Burlon DT. Experience with percu- taneous endoscopic gastrostomy in a community Hospital. Am J Gastroenterol. 1991;86(2):168-169. 11. Ponsky JI, Gauderer MW. Percutaneous endoscopic gastros- tomy: indications, limitations, techniques, and results. World J Surg. 1989;13:165-170. 12. Fanelli RD, Ponsky JL. A simplified technique for percutaneous endoscopic gastrostomy. Surg Endosc. 1992;6:261-262. 13. Stamm M. Gastrostomy by a new method. Med News, 1824;65:324-326. 14. Shellito PC, Malt RA. Tube gastrostomy: techniques and com- plications. Ann Surg. 1985;210:180-185. 15. Larson DE, Burton DD, Schroeder KW, DiMango EP. Percu- taneous endoscopic gastrostomy. Indications, success, complica- tions, and mortality in 314 consecutive patients. Gastroenterology. 1987;93:48-52. 16. Schapiro GD, Edmundowicz SA. Complications of percutane- ous endoscopic gastrostomy. Gastroinrest Endosc Chin N Am. 1996;6:409-422. 17. Shephard DAE. Glimpses of surgical history: G for gastric sur- gery, gastrostomy, Beaumont and St. Martin. Can J Surg. 1976;19:32-33. 18. Cunha F. Gastrostomy: its inception and evolution. Am J Surg. 1946;72:610. 19. Gauderer MWL, Ponsky JL. A simplified technique for con- structing a tube feeding gastrotomy. Surg Gynecol Obstet. 1981;152:83-85. 20. Strode1 WE, Lemmer J, Eckhauser F, er al. Early experience with endoscopic percutaneous gastrostomy. Arch Surg. 1983;118:449- 453. 21. Jonas SK, Neimark S, Panwalker AP. Effects of antibiotic pro- phylaxis in percutaneous endoscopic gastrostomy. Am J Gastroen- rerol, 1985;80:438-441. 22. Jain NK, Larson DE, Schroeder KW, et al. Antibiotic prophylaxis for percutaneous endoscopic gastrostomy. A prospective, randomized, double-blind clinical trial. Ann Intern Med. 1987;107:824-828. 23. Schauer PR, Schwesinger WH, Page CP, et al. Complications of surgical endoscopy. A decade of experience from a surgical resi- dency training program. Surg Endosc. 1997;11:8-11. 24. ACGME. Program requirements for residency education in in- ternal medicine geriatric medicine. 1993:79.
What I am having trouble interpreting is the last conclu- sion, that the surgical residents could achieve as good re- sults. By reading the manuscript, I assume-and I hope- that all these cases were done under close supervision. It is very difficult to sort it out as to whether the excellent results are attributed to the residents who totally mastered the technique and therefore had such good results or whether you just have a very good attending staff. Probably, even if the residents only performed one case, you may still have
THE AMERICAN JOURNAL OF SURGERY@ VOLUME 174 DECEMBER 1997 627
IG TUBE PLACEMENT1
the same excellent results because of the close supervision by attending surgeons.
I think that the only way you could really conclude that the residents could do it well after this low number of cases is if you follow the residents longitudinally after they com- plete their training. I think that before you do that it would be very difficult to give all the credit to the residents instead of to your attending surgeons.
Nicholas Lang, MD (Little Rock, Arkansas): We have been interested in mortality after gastrostomy. In our ex- perience, we find a very high death rate, apparently attrib- utable to the underlying diseases of the patients in whom we are putting these tubes.
I was wondering if your institution had a similar experi- ence, or have you looked at that longer mortality rate to see how long these patients actually use the tube?
CLOSING James B. Lowe, MD: We have looked more long term.
Across the board, there was approximately a 7% mortality rate for the patients overall, a majority of them not related to the PEG and Gtube placement. It is true that this is a high risk group and they are definitely more prone to prob- lems long term.
626 THE AMERICAN JOURNAL OF SURGERY@ VOLUME 174 DECEMBER 1997