Embed Size (px)
Citation preview
http://cat.sagepub.com/Clinical and Applied Thrombosis/Hemostasis
http://cat.sagepub.com/content/20/4/355The online version of this article can be found at:
DOI: 10.1177/1076029613516188
2014 20: 355 originally published online 11 December 2013CLIN APPL THROMB HEMOSTJoost DeJongh, Johan Frieling, Simon Lowry and Henk-Jan Drenth
Hereditary Antithrombin DeficiencyPharmacokinetics of Recombinant Human Antithrombin in Delivery and Surgery Patients With
Published by:
http://www.sagepublications.com
can be found at:Clinical and Applied Thrombosis/HemostasisAdditional services and information for
Immediate free access via SAGE ChoiceOpen Access:
http://cat.sagepub.com/cgi/alertsEmail Alerts:
http://cat.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://cat.sagepub.com/content/20/4/355.refs.htmlCitations:
What is This?
- Dec 11, 2013OnlineFirst Version of Record
- Mar 4, 2014OnlineFirst Version of Record
- Apr 2, 2014Version of Record >>
at UCSF LIBRARY & CKM on August 21, 2014cat.sagepub.comDownloaded from at UCSF LIBRARY & CKM on August 21, 2014cat.sagepub.comDownloaded from
Original Article
Pharmacokinetics of RecombinantHuman Antithrombin in Deliveryand Surgery Patients With HereditaryAntithrombin Deficiency
Joost DeJongh, PhD1, Johan Frieling, MD, PhD2,Simon Lowry, MD2, and Henk-Jan Drenth, PhD1
AbstractPopulation pharmacokinetic (PK) analyses were conducted to refine dosing recommendations for recombinant humananti-thrombin therapy in surgery and delivery patients with hereditary antithrombin deficiency (HD). Single-dose PK data frompatients with HD and nonlinear mixed-effects modeling were used to devise a dosing regimen to target antithrombin (AT) activitylevels between 80% and 120% of normal. External validation with data from a phase 3 trial confirmed the correctness of acovariate-free model for surgery patients, but dosing adjustment was necessary for delivery patients. After different covariateswere tested, the model was updated to incorporate the influential covariate, delivery. Simulations were used to develop a ther-apeutic drug-monitoring scenario that results in steady state AT activity levels within the target range as quickly as practicallyfeasible. Data from a second clinical trial provided additional external validation and confirmed the accuracy of the dosing modelfor both groups of patients.
Keywordsrecombinant antithrombin, dosing, model validation, population pharmacokinetics
Introduction
Venous thromboembolism (VTE), which consists of deep vein
thrombosis and pulmonary embolism, is a major health problem
in the United States and worldwide, especially among subgroups
such as pregnant women and patients who are undergoing
surgical procedures.1,2 Risk factors for VTE are generally cumu-
lative2 and include deficiencies of natural coagulation inhibitors
(eg, antithrombin [AT]) and thrombophilias.3
Hereditary AT deficiency (HD), a well-characterized,
almost always heterozygous, autosomal dominant disorder that
is caused by either a reduction in AT production (type I HD) or
the presence of a dysfunctional form of AT (type II HD), is
associated with a high risk of VTE.4 Although HD is rare, with
an overall prevalence between 1:2000 and 1:5000 in the gen-
eral population,5 affected individuals have a �50% lifetime
risk of developing VTE, which is the highest risk among all
inherited thrombophilias.6 As in healthy individuals, the
probability of VTE may be further elevated in patients with
HD during high-risk situations such as surgery and delivery.
Approximately half of the VTEs in patients with hypercoagula-
tion disorders such as HD are thought to be provoked in these
high-risk situations.7,8 Primary, long-term anticoagulant pro-
phylaxis is recommended only for symptomatic individuals
with AT deficiency.9 However, short-term AT replacement
therapy is recommended to prevent VTE in patients with HD
during high-risk situations. The goal of such therapy is to
reduce the risk of VTE by maintaining AT activity levels
between 80% and 120% of normal.6
Several pooled human plasma-derived AT concentrates and
1 recombinant human AT concentrate (ATryn;10 rEVO Biolo-
gics, Framingham, Massachusetts) are available for the preven-
tion of VTE in connection with surgical or obstetric procedures
in patients with HD. Dosing of pooled human plasma-derived
AT consists of individualized bolus loading and bolus mainte-
nance doses at least once a day. The loading dose is based on
the patient’s pretreatment AT activity level, with the goal of
maintaining trough plasma AT activity levels above 80% of
normal. Subsequent doses are based on the individual trough
levels measured during treatment. Results from a pharmacoki-
netic (PK) study in healthy volunteers11 clearly suggested that
1 LAP&P Consultants BV, Leiden, the Netherlands2 rEVO Biologics, Framingham, MA, USA
Corresponding Author:
Johan Frieling, Clinical Development, rEVO Biologics, Inc. 175 Crossing Blvd,
Framingham, MA 01702, USA.
Email: [email protected]
Clinical and AppliedThrombosis/Hemostasis2014, Vol. 20(4) 355-364ª The Author(s) 2013Reprints and permission:sagepub.com/journalsPermissions.navDOI: 10.1177/1076029613516188cat.sagepub.com
at UCSF LIBRARY & CKM on August 21, 2014cat.sagepub.comDownloaded from

the PK characteristics of recombinant human AT are different
from those reported for pooled human plasma-derived concen-
trates,12 necessitating a different approach to dosing.
The objective of the present report is to describe the devel-
opment of the current dosing recommendations for recombi-
nant human AT in surgery and delivery patients. Single-dose
PK data from patients with HD were used for nonlinear
mixed-effects modeling to establish an initial dosing regimen.
After the predictive strength of the model was tested in a
second study of surgery and delivery patients, delivery was
observed to be a significant covariate for PK, and the model
was updated. A final external validation was performed on both
surgery and delivery patients from a third study.
Methods
Studies and Patients
A total of 47 patients with HD who received recombinant
human AT treatment during 3 trials formed the study popula-
tion for this PK analysis. An open-label, single-dose PK study
(AT III 009-00) included nonpregnant HD patients not in high-
risk situations who were sufficiently healthy to undergo the
necessary tests and procedures. The female–male ratio was
13:2, and the mean baseline AT activity was approximately
51%. The 2 clinical trials, AT III 01002 (clinicaltrials.gov
NCT00056550)13 and AT HD 012-04 (clinicaltrials.gov
NCT00110513; M. J. Paidas, MD, accepted for publication)
were similar in design and included a total of 32 patients with
HD in high-risk situations (21 delivery and 11 surgery).
Patients were treated with recombinant human AT during the
perioperative or peripartum period to prevent occurrence of
VTE. Treatment was started the day before the procedure (or
as soon as possible after confirmation of active labor in
delivery patients) and continued for at least 3 days. Approvals
for all studies were obtained from the applicable authorities and
institutional review boards/ethics committees. All patients pro-
vided informed consent before any study-related procedure was
performed.
Study Drug Administration
Patients in the initial PK study received a single-recombinant
human AT intravenous bolus dose of either 50 IU/kg (n ¼ 9)
or 100 IU/kg (n¼ 6). In study AT III 01002, loading and main-
tenance doses were determined by formulas that accounted for
both individual baseline AT activity and body weight. In AT
study HD 012-04, dosing calculation formulas also accounted
for the type of high-risk situation (i.e., surgery or delivery).
Loading doses were administered as 15-minute bolus infusions
and were followed immediately by maintenance dosing via
continuous infusion (CI).
Blood Sampling
In the PK study, blood samples were collected at the screening
visit and at 1 hour before and 15 minutes before recombinant
human AT dosing. Postdose samples were collected at the fol-
lowing times after infusion cessation: 0, 5, 10, 15, 30, 45, and
60 minutes and 2, 4, 6, 8, 24 (+2), 48 (+2), and 72 (+2)
hours. In the clinical trials, predose blood samples were
collected at screening and baseline. In study AT III 01002,
samples were collected for AT activity measurements 0.5 hour
after the start of the maintenance infusion. If AT activity was
outside the target range, the dose was adjusted, and another
sample was drawn for AT activity measurement 0.5 hour later.
If no dose adjustment was needed, AT activity was measured 4
hours later and at least every 24 hours for the duration of the
infusion. In the AT HD 012-04 study, samples were collected,
and AT activity was measured 2 hours after the start of the infu-
sion and again 2 hours later (if the dose was adjusted) or 4 hours
later (if the dose was not adjusted). Subsequently, samples were
collected 1 or 2 times daily during the infusion, with dosing
adjustment as needed to maintain AT activity in the target
range.
Population PK Analysis
A population PK model was developed on the basis of PK study
data from 15 patients with HD. This model was used to create a
dosing algorithm to achieve plasma AT activity levels between
80% and 120% of normal. On the basis of results from a
previous study of recombinant human AT PK in healthy volun-
teers,11 a 2-compartment model with linear elimination from
the central compartment was chosen as a starting point.
Pretreatment AT activity was considered as a separate, inde-
pendent model parameter at baseline, and any increased AT
activity due to recombinant human AT infusion was modeled
additive to this baseline. The population PK analysis and exter-
nal validation were performed using nonlinear mixed-effects
modeling in NONMEM (versions V.2 and 7.2; Icon PLC,
Dublin, Ireland), which describes the population PK, simulta-
neously accounting for interindividual and intraindividual
variabilities in 1 joint model optimization run. First-order condi-
tional estimation with interaction (METHOD ¼ 1 INTER) was
used as a minimization method for all model runs. Subsequent
postprocessing of NONMEM results was performed using the
statistical software package S-Plus for Windows (versions 6.1
and 8; TIBCO, Somerville, Massachusetts). The model was
sequentially optimized for interindividual variability (IIV) of
each PK parameter until no further improvement in goodness
of fit of the model to the data was observed, and all relevant
random effects for IIV had been assigned. Description of the
residual variability between model predictions and observations
was optimized on the basis of a proportional error model.
Because of the small population, a formal, model-based analysis
of demographic covariates was not performed.
For model development, the simplest possible model that
adequately described the data was accepted as final, using the
forward addition/backward deletion principle. The effects of
adding structural or stochastic parameters to the model on
model fit were assessed by inspection of both the diagnostic
plots of observations versus individual/population predictions
356 Clinical and Applied Thrombosis/Hemostasis 20(4)
at UCSF LIBRARY & CKM on August 21, 2014cat.sagepub.comDownloaded from
and the weighted residuals versus time/population predictions,
as well as statistical considerations. Internal model validation
using visual predictive check (VPC) and bootstrapping con-
firmed that model accuracy and precision were adequate for
simulation of expected AT activity during prolonged clinical
treatment with recombinant human AT.
Data from both clinical studies were used for external vali-
dation of the initial model. For each study, baseline AT activ-
ities were described by optimization of 1 fixed and 1 random
effect (i.e., mean baseline and IIV) to the validation data. All
other population PK model parameters were fixed to their pre-
viously derived values. Residual variability (ie, the difference
between individually observed and predicted AT activity val-
ues) was also optimized to the data. Predicted versus actual
observed AT activity values were visually inspected for ran-
dom distribution around the identity line. Patient plasma AT
activity levels were modeled on the basis of patient infusion
rate records. The final population PK model was used to infer
the most likely value of baseline AT activity while allowing for
specification of IIV in the baseline values. The results were
used to describe the observed AT activity in the population for
study AT III 01002. Predicted AT activity values were com-
pared with observed values, and the corresponding residuals for
predicted/observed activities were determined. The influence
of relevant covariates on the residuals was analyzed in an
exploratory way by plotting the residuals against each of the
covariates (ie, age, gender, body weight, study center, high-
risk situation, and concomitant medications). Potentially
distinct covariates were incorporated into the model to test
diminished bias in the predictions. Categorical covariates were
included in the model by assuming different typical values
(population means) of the structural model parameters (ys) for
different categories.
Simulations to Optimize Therapeutic Drug Monitoring
Two dosing models were used for simulations (in 10 000
patients) to determine the optimal number of dose adjustments
needed for loading and infusion of recombinant human AT to
attain AT activity in the target range within the shortest time.
One set of model parameters was derived for surgical patients
and validated by a dataset from AT III 01002, and the other was
derived for delivery patients. A typical body weight of 76 kg,
and normal distribution were assumed, with a variance of
204 kg.2 The influence of the following factors was investi-
gated: initial and second sampling times, cutoff values, and dif-
ferent dosing algorithms or dose adjustments factors.
Results
Study Descriptions and PK of Recombinant Human AT
Of the 47 patients included in the development and external
validation of the population PK model in patients with HD,
15 were not in high-risk situations. The remaining 32 patients
treated with recombinant human AT in the 2 clinical trials were
exposed to high-risk situations (either surgery or delivery).
Table 1 shows the total and maintenance recombinant human
AT doses and the treatment durations for patients in the 2 clin-
ical studies.
Determination of the Population PK Model (AT III 009-00 Study)
Descriptive PK parameters from the AT III 009-00 study are
shown in Table 2. Initially, a 2-compartment model with 5
structural PK model parameters (ie, plasma clearance [CL],
steady state volume of distribution [Vss], central volume of dis-
tribution [Vcentral], intercompartmental clearance [Q], and AT
activity level at baseline [ATBL]) was optimized to the data.
Next, random effects of IIV were sequentially added to each
of the structural PK model parameters. Overall, the best model
fit was obtained when IIV coefficients were assigned to Vss,
CL, ATBL, and Q. To account for possible correlation between
IIV coefficients, a full 4 � 4 covariance matrix was implemen-
ted for the IIV coefficients for these parameters, which resulted
in a small, but significant, improvement in the goodness-of-fit
model. To optimize the description of the IIV coefficients and
their interdependence, Q was expressed as a multiple of CL.
This led to a model structure with IIV coefficients for CL and
Vss, linked by a 2 � 2 covariance matrix, and a single indepen-
dent IIV coefficient for ATBL. Goodness of fit was only
marginally decreased when compared with the previous model
the previous model, but numerical stability was acceptable. The
original description of residual variability was also challenged,
but the optimal description was always proportional to the mod-
eled AT value.
The accuracy of the model was internally evaluated by com-
paring the actual AT activity values (AT III 009-00 study data-
set) with the 10th and 90th percentiles of the simulated data and
using a VPC (excluding the baseline values; Figure 1). In the
50- and 100-IU/kg recombinant human AT dose groups, 84%
Table 1. AT III 01002 and AT HD 012-04 Study Dosing.
AT III 01002 AT HD 012-04
Number of patients, no. 14 18Surgery group 5 6Delivery group 9 12
Screening AT activity, mean (range), %Surgery group 50 (37-62) 54 (45-65)Delivery group 46 (33-58) 49 (29-65.7)
Total dose, median (range), IU/kgSurgery group 1194 (1041-3346) 523 (377-1913)Delivery group 973 (518-3018) 770 (208-3372)
Total maintenance dose, median (range), IU/kgSurgery group 1147 (1003-3311) 509 (359-1885)Delivery group 954 (493-2970) 726 (174-3359)
Treatment duration; median (range), dSurgery group 11.5 (8-19) 3.0 (3-14)Delivery group 3.1 (3-10) 3.6 (1-14)
Abbreviations: AT, antithrombin; HD, hereditary AT deficiency.
DeJongh et al 357
at UCSF LIBRARY & CKM on August 21, 2014cat.sagepub.comDownloaded from
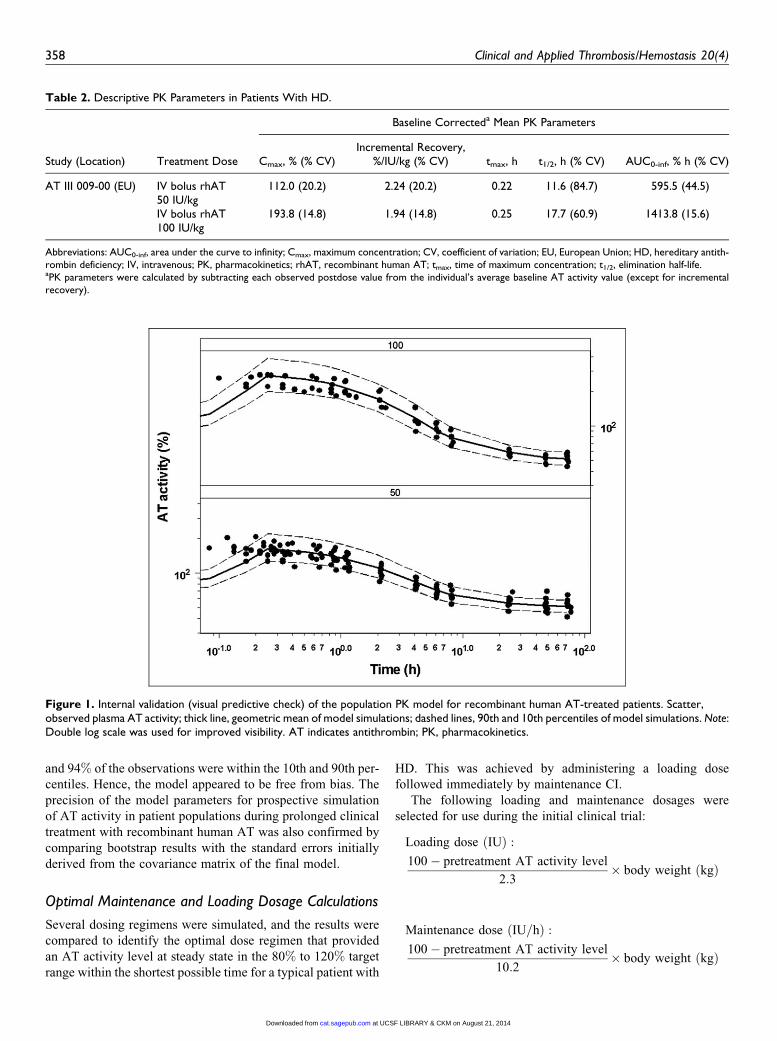
and 94% of the observations were within the 10th and 90th per-
centiles. Hence, the model appeared to be free from bias. The
precision of the model parameters for prospective simulation
of AT activity in patient populations during prolonged clinical
treatment with recombinant human AT was also confirmed by
comparing bootstrap results with the standard errors initially
derived from the covariance matrix of the final model.
Optimal Maintenance and Loading Dosage Calculations
Several dosing regimens were simulated, and the results were
compared to identify the optimal dose regimen that provided
an AT activity level at steady state in the 80% to 120% target
range within the shortest possible time for a typical patient with
HD. This was achieved by administering a loading dose
followed immediately by maintenance CI.
The following loading and maintenance dosages were
selected for use during the initial clinical trial:
Loading dose IUð Þ :
100� pretreatment AT activity level
2:3� body weight kgð Þ
Maintenance dose IU=hð Þ :
100� pretreatment AT activity level
10:2� body weight kgð Þ
Figure 1. Internal validation (visual predictive check) of the population PK model for recombinant human AT-treated patients. Scatter,observed plasma AT activity; thick line, geometric mean of model simulations; dashed lines, 90th and 10th percentiles of model simulations. Note:Double log scale was used for improved visibility. AT indicates antithrombin; PK, pharmacokinetics.
Table 2. Descriptive PK Parameters in Patients With HD.
Study (Location) Treatment Dose
Baseline Correcteda Mean PK Parameters
Cmax, % (% CV)Incremental Recovery,
%/IU/kg (% CV) tmax, h t1/2, h (% CV) AUC0-inf, % h (% CV)
AT III 009-00 (EU) IV bolus rhAT50 IU/kg
112.0 (20.2) 2.24 (20.2) 0.22 11.6 (84.7) 595.5 (44.5)
IV bolus rhAT100 IU/kg
193.8 (14.8) 1.94 (14.8) 0.25 17.7 (60.9) 1413.8 (15.6)
Abbreviations: AUC0-inf, area under the curve to infinity; Cmax, maximum concentration; CV, coefficient of variation; EU, European Union; HD, hereditary antith-rombin deficiency; IV, intravenous; PK, pharmacokinetics; rhAT, recombinant human AT; tmax, time of maximum concentration; t1/2, elimination half-life.aPK parameters were calculated by subtracting each observed postdose value from the individual’s average baseline AT activity value (except for incrementalrecovery).
358 Clinical and Applied Thrombosis/Hemostasis 20(4)
at UCSF LIBRARY & CKM on August 21, 2014cat.sagepub.comDownloaded from
Results of Monte Carlo simulations of AT activity versus
time suggest that in 79.5% of patients, the infusion regimen
results in AT activity levels 80% to 120% of normal without the
need for further adjustment of the infusion rate. For patients
who are estimated to have AT activity levels that are either too
high (14.5% of patients) or too low (6.4% of patients), thera-
peutic drug monitoring (TDM; adjustment of infusion rate
according to actual plasma AT activity levels) will be needed
to drive these values into the target range.
Pharmacokinetic Model Validation
Dosing information from patients with HD in high-risk situa-
tions (surgery and delivery, from study AT III 01002) was
applied to the model described previously to predict AT activ-
ity. These AT activity values were compared with the actual
observed AT activity data from the study, which revealed that
the initial population PK model tended to overpredict the AT
activity in this cohort.
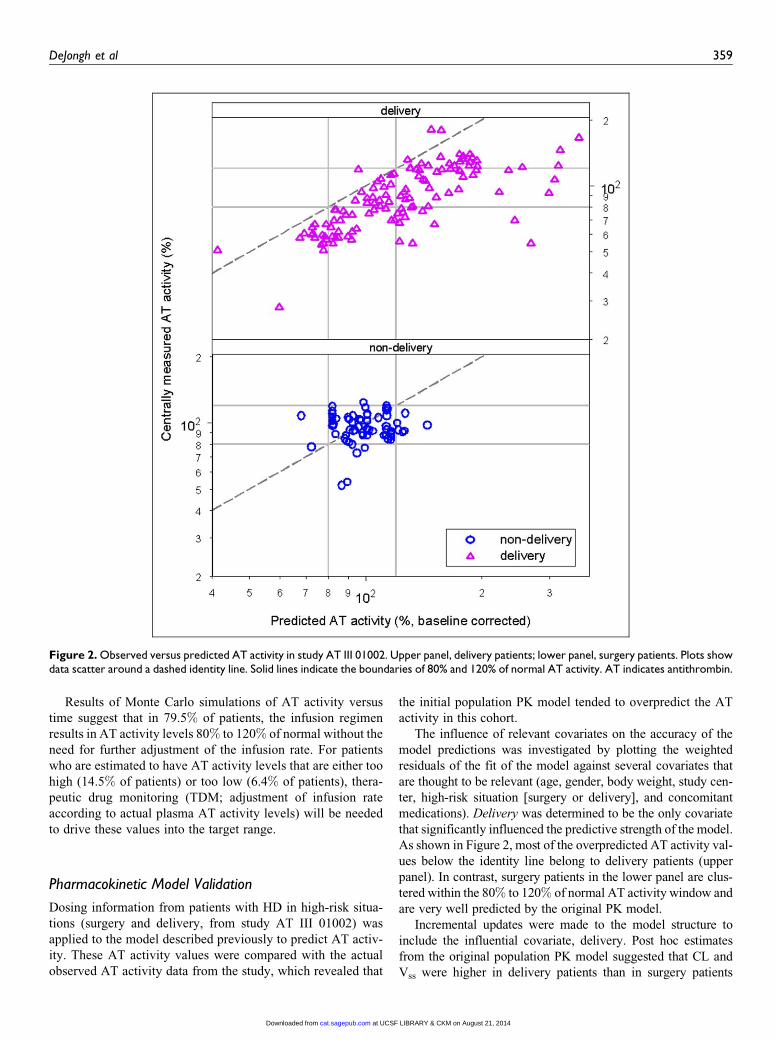
The influence of relevant covariates on the accuracy of the
model predictions was investigated by plotting the weighted
residuals of the fit of the model against several covariates that
are thought to be relevant (age, gender, body weight, study cen-
ter, high-risk situation [surgery or delivery], and concomitant
medications). Delivery was determined to be the only covariate
that significantly influenced the predictive strength of the model.
As shown in Figure 2, most of the overpredicted AT activity val-
ues below the identity line belong to delivery patients (upper
panel). In contrast, surgery patients in the lower panel are clus-
tered within the 80% to 120% of normal AT activity window and
are very well predicted by the original PK model.
Incremental updates were made to the model structure to
include the influential covariate, delivery. Post hoc estimates
from the original population PK model suggested that CL and
Vss were higher in delivery patients than in surgery patients
Figure 2. Observed versus predicted AT activity in study AT III 01002. Upper panel, delivery patients; lower panel, surgery patients. Plots showdata scatter around a dashed identity line. Solid lines indicate the boundaries of 80% and 120% of normal AT activity. AT indicates antithrombin.
DeJongh et al 359
at UCSF LIBRARY & CKM on August 21, 2014cat.sagepub.comDownloaded from
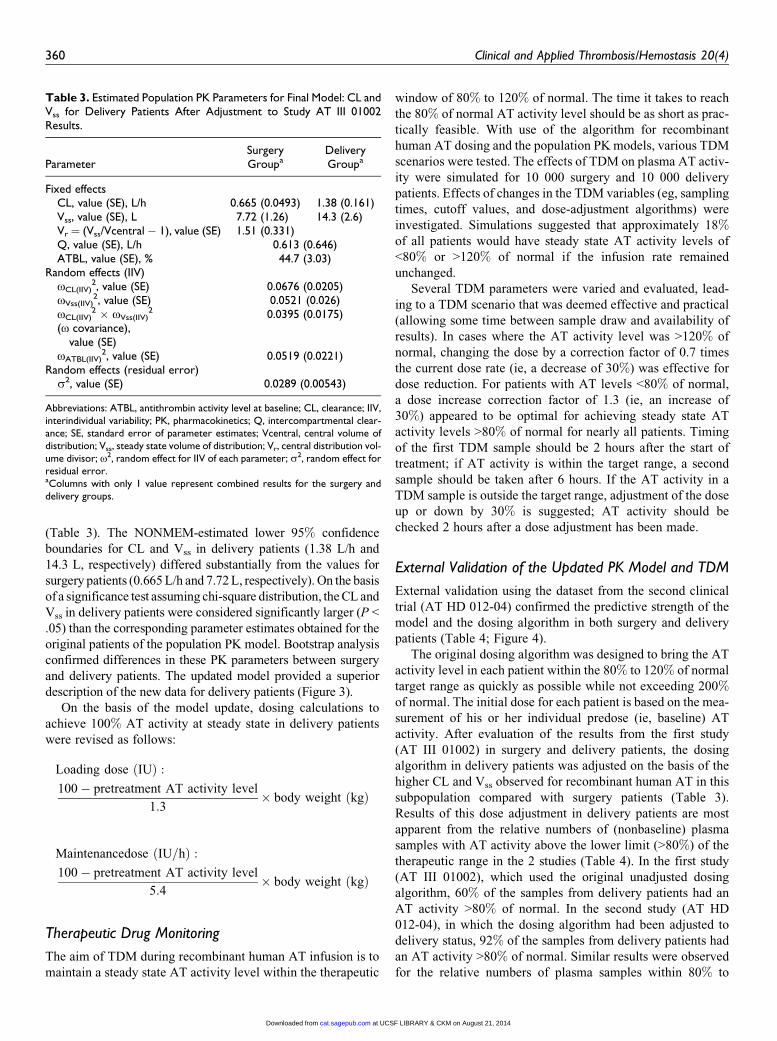
(Table 3). The NONMEM-estimated lower 95% confidence
boundaries for CL and Vss in delivery patients (1.38 L/h and
14.3 L, respectively) differed substantially from the values for
surgery patients (0.665 L/h and 7.72 L, respectively). On the basis
of a significance test assuming chi-square distribution, the CL and
Vss in delivery patients were considered significantly larger (P <
.05) than the corresponding parameter estimates obtained for the
original patients of the population PK model. Bootstrap analysis
confirmed differences in these PK parameters between surgery
and delivery patients. The updated model provided a superior
description of the new data for delivery patients (Figure 3).
On the basis of the model update, dosing calculations to
achieve 100% AT activity at steady state in delivery patients
were revised as follows:
Loading dose IUð Þ :
100� pretreatment AT activity level
1:3� body weight kgð Þ
Maintenancedose IU=hð Þ :
100� pretreatment AT activity level
5:4� body weight kgð Þ
Therapeutic Drug Monitoring
The aim of TDM during recombinant human AT infusion is to
maintain a steady state AT activity level within the therapeutic
window of 80% to 120% of normal. The time it takes to reach
the 80% of normal AT activity level should be as short as prac-
tically feasible. With use of the algorithm for recombinant
human AT dosing and the population PK models, various TDM
scenarios were tested. The effects of TDM on plasma AT activ-
ity were simulated for 10 000 surgery and 10 000 delivery
patients. Effects of changes in the TDM variables (eg, sampling
times, cutoff values, and dose-adjustment algorithms) were
investigated. Simulations suggested that approximately 18%of all patients would have steady state AT activity levels of
<80% or >120% of normal if the infusion rate remained
unchanged.
Several TDM parameters were varied and evaluated, lead-
ing to a TDM scenario that was deemed effective and practical
(allowing some time between sample draw and availability of
results). In cases where the AT activity level was >120% of
normal, changing the dose by a correction factor of 0.7 times
the current dose rate (ie, a decrease of 30%) was effective for
dose reduction. For patients with AT levels <80% of normal,
a dose increase correction factor of 1.3 (ie, an increase of
30%) appeared to be optimal for achieving steady state AT
activity levels >80% of normal for nearly all patients. Timing
of the first TDM sample should be 2 hours after the start of
treatment; if AT activity is within the target range, a second
sample should be taken after 6 hours. If the AT activity in a
TDM sample is outside the target range, adjustment of the dose
up or down by 30% is suggested; AT activity should be
checked 2 hours after a dose adjustment has been made.
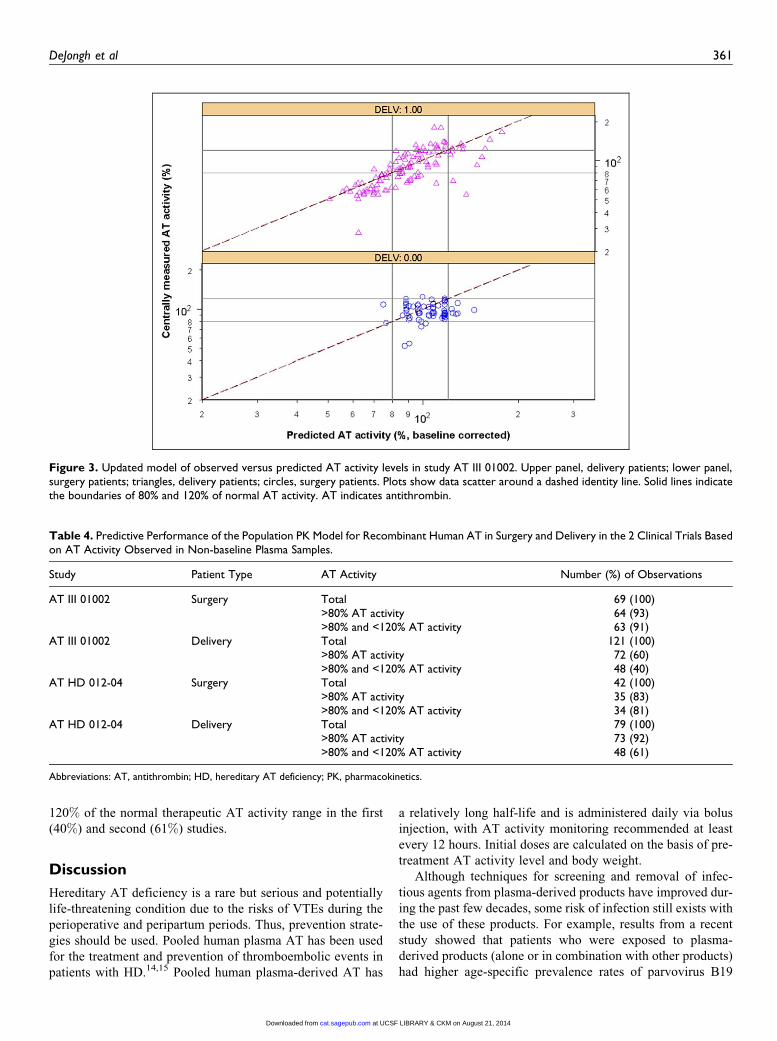
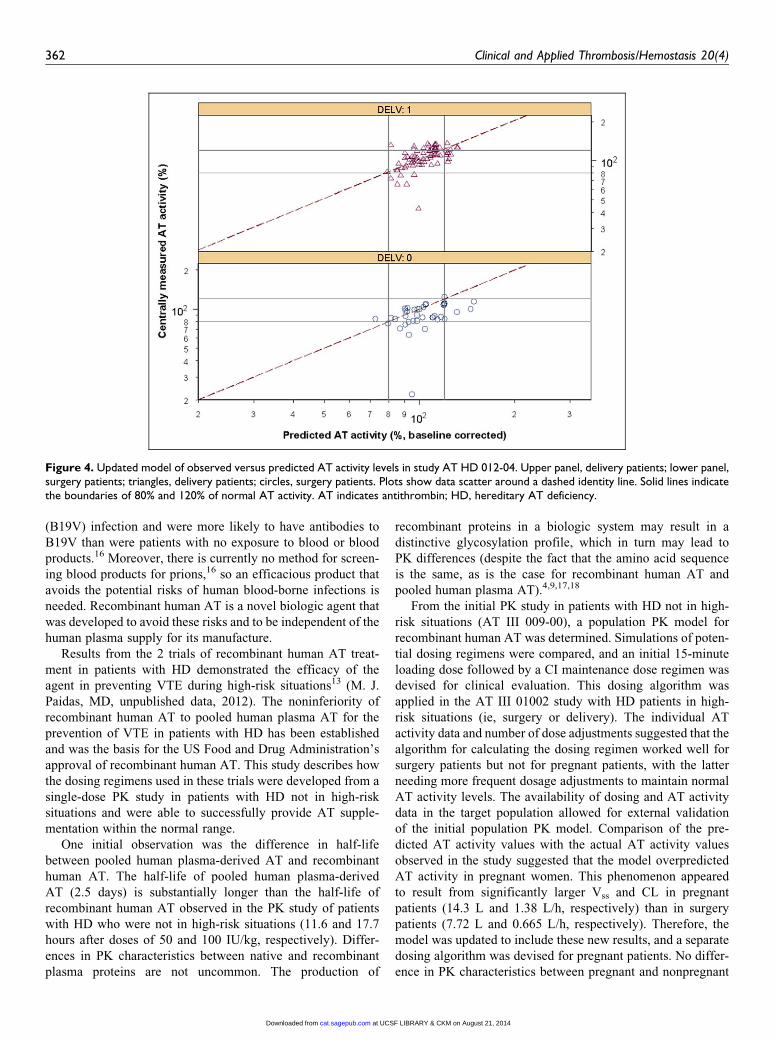
External Validation of the Updated PK Model and TDM
External validation using the dataset from the second clinical
trial (AT HD 012-04) confirmed the predictive strength of the
model and the dosing algorithm in both surgery and delivery
patients (Table 4; Figure 4).
The original dosing algorithm was designed to bring the AT
activity level in each patient within the 80% to 120% of normal
target range as quickly as possible while not exceeding 200%of normal. The initial dose for each patient is based on the mea-
surement of his or her individual predose (ie, baseline) AT
activity. After evaluation of the results from the first study
(AT III 01002) in surgery and delivery patients, the dosing
algorithm in delivery patients was adjusted on the basis of the
higher CL and Vss observed for recombinant human AT in this
subpopulation compared with surgery patients (Table 3).
Results of this dose adjustment in delivery patients are most
apparent from the relative numbers of (nonbaseline) plasma
samples with AT activity above the lower limit (>80%) of the
therapeutic range in the 2 studies (Table 4). In the first study
(AT III 01002), which used the original unadjusted dosing
algorithm, 60% of the samples from delivery patients had an
AT activity >80% of normal. In the second study (AT HD
012-04), in which the dosing algorithm had been adjusted to
delivery status, 92% of the samples from delivery patients had
an AT activity >80% of normal. Similar results were observed
for the relative numbers of plasma samples within 80% to
Table 3. Estimated Population PK Parameters for Final Model: CL andVss for Delivery Patients After Adjustment to Study AT III 01002Results.
ParameterSurgeryGroupa
DeliveryGroupa
Fixed effectsCL, value (SE), L/h 0.665 (0.0493) 1.38 (0.161)Vss, value (SE), L 7.72 (1.26) 14.3 (2.6)Vr ¼ (Vss/Vcentral � 1), value (SE) 1.51 (0.331)Q, value (SE), L/h 0.613 (0.646)ATBL, value (SE), % 44.7 (3.03)
Random effects (IIV)oCL(IIV)
2, value (SE) 0.0676 (0.0205)oVss(IIV)
2, value (SE) 0.0521 (0.026)oCL(IIV)
2 � oVss(IIV)2
(o covariance),value (SE)
0.0395 (0.0175)
oATBL(IIV)2, value (SE) 0.0519 (0.0221)
Random effects (residual error)s2, value (SE) 0.0289 (0.00543)
Abbreviations: ATBL, antithrombin activity level at baseline; CL, clearance; IIV,interindividual variability; PK, pharmacokinetics; Q, intercompartmental clear-ance; SE, standard error of parameter estimates; Vcentral, central volume ofdistribution; Vss, steady state volume of distribution; Vr, central distribution vol-ume divisor; o2, random effect for IIV of each parameter; s2, random effect forresidual error.aColumns with only 1 value represent combined results for the surgery anddelivery groups.
360 Clinical and Applied Thrombosis/Hemostasis 20(4)
at UCSF LIBRARY & CKM on August 21, 2014cat.sagepub.comDownloaded from
120% of the normal therapeutic AT activity range in the first
(40%) and second (61%) studies.
Discussion
Hereditary AT deficiency is a rare but serious and potentially
life-threatening condition due to the risks of VTEs during the
perioperative and peripartum periods. Thus, prevention strate-
gies should be used. Pooled human plasma AT has been used
for the treatment and prevention of thromboembolic events in
patients with HD.14,15 Pooled human plasma-derived AT has
a relatively long half-life and is administered daily via bolus
injection, with AT activity monitoring recommended at least
every 12 hours. Initial doses are calculated on the basis of pre-
treatment AT activity level and body weight.
Although techniques for screening and removal of infec-
tious agents from plasma-derived products have improved dur-
ing the past few decades, some risk of infection still exists with
the use of these products. For example, results from a recent
study showed that patients who were exposed to plasma-
derived products (alone or in combination with other products)
had higher age-specific prevalence rates of parvovirus B19
Figure 3. Updated model of observed versus predicted AT activity levels in study AT III 01002. Upper panel, delivery patients; lower panel,surgery patients; triangles, delivery patients; circles, surgery patients. Plots show data scatter around a dashed identity line. Solid lines indicatethe boundaries of 80% and 120% of normal AT activity. AT indicates antithrombin.
Table 4. Predictive Performance of the Population PK Model for Recombinant Human AT in Surgery and Delivery in the 2 Clinical Trials Basedon AT Activity Observed in Non-baseline Plasma Samples.
Study Patient Type AT Activity Number (%) of Observations
AT III 01002 Surgery Total 69 (100)>80% AT activity 64 (93)>80% and <120% AT activity 63 (91)
AT III 01002 Delivery Total 121 (100)>80% AT activity 72 (60)>80% and <120% AT activity 48 (40)
AT HD 012-04 Surgery Total 42 (100)>80% AT activity 35 (83)>80% and <120% AT activity 34 (81)
AT HD 012-04 Delivery Total 79 (100)>80% AT activity 73 (92)>80% and <120% AT activity 48 (61)
Abbreviations: AT, antithrombin; HD, hereditary AT deficiency; PK, pharmacokinetics.
DeJongh et al 361
at UCSF LIBRARY & CKM on August 21, 2014cat.sagepub.comDownloaded from
(B19V) infection and were more likely to have antibodies to
B19V than were patients with no exposure to blood or blood
products.16 Moreover, there is currently no method for screen-
ing blood products for prions,16 so an efficacious product that
avoids the potential risks of human blood-borne infections is
needed. Recombinant human AT is a novel biologic agent that
was developed to avoid these risks and to be independent of the
human plasma supply for its manufacture.
Results from the 2 trials of recombinant human AT treat-
ment in patients with HD demonstrated the efficacy of the
agent in preventing VTE during high-risk situations13 (M. J.
Paidas, MD, unpublished data, 2012). The noninferiority of
recombinant human AT to pooled human plasma AT for the
prevention of VTE in patients with HD has been established
and was the basis for the US Food and Drug Administration’s
approval of recombinant human AT. This study describes how
the dosing regimens used in these trials were developed from a
single-dose PK study in patients with HD not in high-risk
situations and were able to successfully provide AT supple-
mentation within the normal range.
One initial observation was the difference in half-life
between pooled human plasma-derived AT and recombinant
human AT. The half-life of pooled human plasma-derived
AT (2.5 days) is substantially longer than the half-life of
recombinant human AT observed in the PK study of patients
with HD who were not in high-risk situations (11.6 and 17.7
hours after doses of 50 and 100 IU/kg, respectively). Differ-
ences in PK characteristics between native and recombinant
plasma proteins are not uncommon. The production of
recombinant proteins in a biologic system may result in a
distinctive glycosylation profile, which in turn may lead to
PK differences (despite the fact that the amino acid sequence
is the same, as is the case for recombinant human AT and
pooled human plasma AT).4,9,17,18
From the initial PK study in patients with HD not in high-
risk situations (AT III 009-00), a population PK model for
recombinant human AT was determined. Simulations of poten-
tial dosing regimens were compared, and an initial 15-minute
loading dose followed by a CI maintenance dose regimen was
devised for clinical evaluation. This dosing algorithm was
applied in the AT III 01002 study with HD patients in high-
risk situations (ie, surgery or delivery). The individual AT
activity data and number of dose adjustments suggested that the
algorithm for calculating the dosing regimen worked well for
surgery patients but not for pregnant patients, with the latter
needing more frequent dosage adjustments to maintain normal
AT activity levels. The availability of dosing and AT activity
data in the target population allowed for external validation
of the initial population PK model. Comparison of the pre-
dicted AT activity values with the actual AT activity values
observed in the study suggested that the model overpredicted
AT activity in pregnant women. This phenomenon appeared
to result from significantly larger Vss and CL in pregnant
patients (14.3 L and 1.38 L/h, respectively) than in surgery
patients (7.72 L and 0.665 L/h, respectively). Therefore, the
model was updated to include these new results, and a separate
dosing algorithm was devised for pregnant patients. No differ-
ence in PK characteristics between pregnant and nonpregnant
Figure 4. Updated model of observed versus predicted AT activity levels in study AT HD 012-04. Upper panel, delivery patients; lower panel,surgery patients; triangles, delivery patients; circles, surgery patients. Plots show data scatter around a dashed identity line. Solid lines indicatethe boundaries of 80% and 120% of normal AT activity. AT indicates antithrombin; HD, hereditary AT deficiency.
362 Clinical and Applied Thrombosis/Hemostasis 20(4)
at UCSF LIBRARY & CKM on August 21, 2014cat.sagepub.comDownloaded from

patients with HD has been described for human pooled plasma
AT, although Weiner et al19 described a shorter half-life for AT
III concentrate in pregnant women without HD than in healthy
nonpregnant patients. Recent analyses of dosing and AT
activity from a retrospectively derived dataset of patients
treated with pooled human plasma-derived AT also suggest
substantial differences in PK parameters between pregnant and
nonpregnant patients with HD (J. Frieling, MD, PhD, unpub-
lished data, 2012). The exact reason for this difference between
pregnant and nonpregnant patients is not clear and probably
multifactorial. However, it is well known that significant
changes in intra- and extravascular volume occur during
pregnancy, also potentially leading to the increased Vss for antith-
rombin. In addition, hepatic clearance is known to have been
changed during pregnancy.20
Other potentially relevant covariates (age, gender, body
weight, study center, and concomitant medications) did not
have a significant influence on the accuracy of the model pre-
dictions. Therefore, the loading and maintenance infusion
doses were increased in the algorithm for pregnant patients to
ensure that target AT levels are more easily achieved, thus
managing the risk of VTE around the time of delivery.
In addition to the update of the dosing algorithm, simulations
were performed to design a practical TDM scenario. The model
allows for simulation of data from large numbers of patients (in
this case, AT activity data for 10 000 surgery and 10 000 deliv-
ery patients) and use of this information to choose the TDM
scenario that maximizes the percentage of patients who achieve
the target range of AT activity and minimizes the amount of time
spent outside of that range. However, the TDM scenario should
be practical for implementation in current medical practice,
accounting for factors such as turnaround time for AT activity
analysis. The simulations showed that if a sample is taken too
soon (e.g., after 1 hour), the result is not sufficiently predictive
of the patient’s steady state AT activity level to allow appropri-
ate changes in the infusion rate. Therefore, the first TDM sample
should be taken 2 hours after the start of the infusion. The simu-
lations also indicated that for patients with AT activity levels
outside the target range at the time of the first TDM sample,
increasing or decreasing the dose by 30% will bring the level
within the target range in almost all cases. With the recom-
mended TDM, maintenance of AT activity levels within the lim-
its of the therapeutic window (80%-120%) is clinically feasible.
Subsequent use of the updated dosing algorithm and TDM
scenario in the second clinical trial (AT HD 012-04) confirmed
that tight control of AT activity levels was possible in both
pregnant and nonpregnant patients with HD. Very few dose
adjustments were needed to achieve and maintain target AT
activity levels. External validation showed that the final model
had great predictive strength for both surgery and delivery
patients and confirmed the proposed TDM scenario.
Conclusions
Population PK analysis is a strong tool for developing a recom-
binant human AT dosing regimen for patients in high-risk
situations. Using single-dose PK data, an algorithm for recom-
binant human AT dosing over several days in patients with HD
in high-risk situations was established. External validation con-
firmed the model’s correctness for surgery patients and
revealed important PK differences with use of recombinant
human AT in pregnant patients. Adjustment of the dosing regi-
men for delivery patients led to successful use in a second
study. The devised dosing regimen achieves AT activity in the
therapeutic range in most patients with HD within a short time
frame.
Author’s Note
Data described herein were submitted in abstract form for presentation
at the 2013 Annual Meeting of the Society for Gynecologic Investiga-
tion. Manuscript preparation, including medical writing and editorial
assistance, was provided by MedLogix Communications and was sup-
ported by rEVO Biologics. This article reflects the concepts of the
authors and is their sole responsibility. The authors reviewed and edi-
ted this article to ensure accuracy.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest
with respect to the research, authorship, and/or publication of this arti-
cle: Henk-Jan Drenth and Joost DeJongh are employees of LAP&P
Consultants and were hired by rEVO Biologics to perform the popu-
lation PK model analysis and simulations described in this work.
Johan Frieling and Simon Lowry are employees of rEVO Biologics.
Funding
The author(s) disclosed receipt of the following financial support for
the research, authorship and/or publication of this article: The research
was funded by rEVO Biologics.
References
1. Heit JA. The epidemiology of venous thromboembolism in the
community. Arterioscler Thromb Vasc Biol. 2008;28(3):370-372.
2. Ageno W, Spyropoulos AC, Turpie AG. Role of new anticoagu-
lants for the prevention of venous thromboembolism after major
orthopaedic surgery and in hospitalised acutely ill medical
patients. Thromb Haemost. 2012;107(6):1027-1034.
3. Makris M. Thrombophilia: grading the risk. Blood. 2009;113(21):
5038-5039.
4. Patnaik MM, Moll S. Inherited antithrombin deficiency: a review.
Haemophilia. 2008;14(6):1229-1239.
5. Rajan A, Grethlein SJ, McKenna R. Antithrombin Deficiency.
Medscape Web Site. http://emedicine.medscape.com/article/
198573-overview. Accessed May 23, 2012.
6. Rodgers GM.Role of antithrombin concentrate in treatment of
hereditary antithrombin deficiency. An update. Thromb Haemost.
2009;101(5):806-812.
7. Kearon C, Crowther M, Hirsh J. Management of patients with her-
editary hypercoagulable disorders. Annu Rev Med. 2000;51:
169-185.
8. Seligohn U, Lubetsky A. Genetic susceptibility to venous throm-
bosis. N Engl J Med. 2001;344(16):1222-1231.
DeJongh et al 363
at UCSF LIBRARY & CKM on August 21, 2014cat.sagepub.comDownloaded from
9. Maclean PS, Tait RC. Hereditary and acquired antithrombin
deficiency: epidemiology, pathogenesis and treatment options.
Drugs. 2007;67(10):1429-1440.
10. ATryn [package insert]. Framingham, MA: GTC Biotherapeutics,
Inc; 2009.
11. Lu W, Mant T, Levy JH, Bailey JM. Pharmacokinetics of recom-
binant transgenic antithrombin in volunteers. Anesth Analg. 2000;
90(3):531-534.
12. Thrombate III [package insert]. Research Triangle Park, NC:
Talecris Biotherapetuics, Inc; 2012.
13. Tiede A, Tait RC, Shaffer DW, et al. Antithrombin alfa in
hereditary antithrombin deficient patients: a phase 3 study of pro-
phylactic intravenous administration in high risk situations.
Thromb Haemost. 2008;99(3):616-622.
14. Schwartz RS, Bauer KA, Rosenberg RD, Kavanaugh EJ, Davies
DC, Bogdanoff DA. Clinical experience with antithrombin III
concentrate in treatment of congenital and acquired deficiency
of antithrombin. The antithrombin III study group. Am J Med.
1989;87(3B):53S-60S.
15. Menache D, O’Malley JP, Schorr JB, et al. Evaluation of the
safety, recovery, half-life, and clinical efficacy of antithrombin III
(human) in patients with hereditary antithrombin III deficiency.
Cooperative study group. Blood. 1990;75(1):33-39.
16. Soucie JM, De Staercke C, Monahan PE, et al. Evidence for the
transmission of parvovirus B19 in patients with bleeding disorders
treated with plasma-derived factor concentrates in the era of
nucleic acid test screening. Transfusion. 2013;53(6):1217-1225.
doi:10.1111/j.1537-2995.2012.03907.x.
17. Edmunds T, Van Patten SM, Pollock J, et al. Transgenically
produced human antithrombin: structural and functional compar-
ison to human plasma-derived antithrombin. Blood. 1998;91(12):
4561-4571.
18. Pal N, Kertai MD, Lakshminarasimhachar A, Avidan MS.
Pharmacology and clinical applications of human recombinant
antithrombin. Expert Opin Biol Ther. 2010;10(7):1155-1168.
19. Weiner CP, Herrig JE, Pelzer GD, Heilskov J. Elimination of
antithrombin III concentrate in healthy pregnant and preeclamptic
women with acquired antithrombin III deficiency. Thromb Res.
1990;58(4):395-401.
20. Dawes M, Chowienczyk PJ. Drugs in pregnancy. Pharmacoki-
netics in pregnancy. Best Pract Res Clin Obstet Gynaecol.
2001;15(6):819-826.
364 Clinical and Applied Thrombosis/Hemostasis 20(4)
at UCSF LIBRARY & CKM on August 21, 2014cat.sagepub.comDownloaded from