Embed Size (px)
Citation preview

American Journal of Medical Genetics Part C (Seminars in Medical Genetics) 166C:302–314 (2014)
A R T I C L E
Phenotype and Genotype inNicolaides–Baraitser SyndromeSÉRGIO B. SOUSA, RAOUL C. HENNEKAM, AND THE NICOLAIDES–BARAITSER SYNDROMEINTERNATIONAL CONSORTIUM
Grant sponsConflict of iSérgio Sous
interest in dyscharacterizatio
Raoul HennAmsterdam, aLondon. He isdysmorphologmechanisms an
*CorresponPediátrico de CE‐mail: sbsousa
DOI 10.100Article first p
� 2014 Wil
Nicolaides–Baraitser syndrome (NCBRS) is an intellectual disability (ID)/multiple congenital anomalies syndromecaused by non‐truncating mutations in the ATPase region of SMARCA2, which codes for one of the twoalternative catalytic subunits of the BAF chromatin remodeling complex. We analyzed 61 molecularly confirmedcases, including all previously reported patients (n¼47) and 14 additional unpublished individuals. NCBRS isclinically and genetically homogeneous. The cardinal features (ID, short stature, microcephaly, typical face, sparsehair, brachydactyly, prominent interphalangeal joints, behavioral problems and seizures), are almost universallypresent. There is variability however, as ID can range from severe to mild, and sparse hair may be present only incertain age groups. There may be a correlation between the severity of the ID and presence of seizures, absentspeech, short stature and microcephaly. SMARCA2 mutations causing NCBRS are likely to act through adominant‐negative effect. There may be some genotype–phenotype correlations (mutations at domain VI withsevere ID and seizures; mutations affecting residues Pro883, Leu946, and Ala1201 with mild phenotypes) butnumbers are still too small to draw definitive conclusions. © 2014 Wiley Periodicals, Inc.
KEYWORDS: Nicolaides–Baraitser syndrome; natural history; intellectual disability; phenotype; genotype; SMARCA2; BAF (SWI/SNF) complex
How to cite this article: Sousa SB, Hennekam RC, the Nicolaides–Baraitser Syndrome InternationalConsortium. 2014. Phenotype and genotype in Nicolaides–Baraitser syndrome.
Am J Med Genet Part C 166C:302–314.
INTRODUCTION
Nicolaides–Baraitser syndrome(NCBRS, OMIM #601358) is charac-terized by severe intellectual disability(ID), seizures, short stature, sparse hair,typical face, brachydactyly, and promi-nent interphalangeal joints. It was firstdescribed in 1993 by pediatric neurolo-gist Paola Nicolaides and clinical genet-icist Michael Baraitser, when theyreported a 16‐year‐old British girl withthis unusual combination of features
or: Fundação Para a Ciência e Tecnnterest: The authors have no conflica is a clinical geneticist at the Centrmorphology, skeletal dysplasias, mn of rare genetic syndromes.ekam is Professor of Pediatrics andnd Professor of Clinical Genetics aa pediatrician and clinical geneticisty, connective tissue disorders and rad the natural history.dence to: Sérgio B. Sousa, M.D.,oimbra, Av. Afonso Romao, 3000‐@chc.min-saude.pt2/ajmg.c.31409ublished online in Wiley Online Lib
ey Periodicals, Inc.
[Nicolaides and Baraitser, 1993]. In thefirst 15 years thereafter five further caseswere reported [Krajewska‐Walaseket al., 1996; Morin et al., 2003; Wittersand Fryns, 2003; Castori et al., 2008]. In2009, the follow‐up of these patients anddescription of 18 additional patientsallowed the establishment of NCBRSas a discrete syndrome [Sousa et al.,2009]. Follow‐up of the original patientat 32 years of age showed her to have hadseizures refractory to treatment withmultiple drugs, a gradual decline of her
ologia; Grant number: SFRH/BD/46778/2008.t of interest to declare.o Hospitalar e Universitário de Coimbra, withetabolic diseases and clinical and molecular
of Translational Genetics at the University ofnd Dysmorphology at the University Collegewith interest in intellectual disability, autism,
re syndromes, studying phenotypes, molecular
Ph.D., Servico de Genética Médica, Hospital602 Coimbra, Portugal.
rary (wileyonlinelibrary.com): 28 August 2014
motor and mental abilities, and moremarked physical features: of note her hair
In 2009 the follow‐up of thesepatients and description of 18additional patients allowed theestablishment of NCBRS as a
discrete syndrome.
became more sparse, her facial featurescoarsened and the joint anomaliesbecame prominent. She died at 33 yearsof age as a consequence of statusepilepticus and subsequent respiratorycomplications. It became clear by theevolution of this and several otherpatients, that certain features of NCBRScan be progressive. The patients andfamilies that participated in that publi-cation [Sousa et al., 2009] startedan international NCBRS parents sup-port group, which has met yearly since2010.

ARTICLE AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 303
All the known NCBRS affectedindividuals were sporadic and unrelatedcases, from various ancestry groups, withno difference in severity or prevalence
Follow‐up of the originalpatient at 32 years of ageshowed her to have had
seizures refractory to treatmentwith multiple drugs, a gradual
decline of her motor andmental abilities, and moremarked physical features: ofnote her hair became moresparse, her facial featurescoarsened and the joint
anomalies became prominent.
between the sexes. Neither familial recur-rence (except for one pair of monozygotictwins) nor consanguinity has been re-ported. These characteristics, added to thespecificity of the phenotype, led to thehypothesis that NCBRS could be causedby a small microdeletion and/or by de novoheterozygous dominant mutations in asingle gene. We performed classicalcytogenetic studies and array‐based com-parative genomic hybridization in 12NCBRS patients and were unable todetect pathogenic chromosomal abnor-mality. The phenotypic overlap withCoffin–Siris syndrome (CSS, OMIM#135900) was recognized [Coffin andSiris, 1970; Schrier Vergano et al., 2013]and it was suggested that either the entitieswere allelic or caused by geneswith relatedfunctions [Sousa et al., 2009].
Following our above‐mentionedwork, we set out to identify the geneticcause of NCBRS using whole‐exomesequencing and filtering variants accord-ing with the predicted mode of inheri-tance. In a joint project betweenAmsterdam and Leuven, SMARCA2,coding for one of the components ofthe “BRG1/SMARCA4 and hBRM/SMARCA2‐associated factor” (BAF)complex, was identified in 2012 as the
causative gene of NCBRS [Van Houdtet al., 2012]. At the time, 44 patients werestudied, 22 of the 26 previously reportedpatients [Nicolaides and Baraitser, 1993;Krajewska‐Walasek et al., 1996; Morinet al., 2003; Witters and Fryns, 2003;Castori et al., 2008; Sousa et al., 2009;Gana et al., 2011], and 22 additionalcases. We classified these patients in twocategories of 37 and seven patients,respectively, with high (group 1) andlow (group 2) certainty by which thediagnosis could be retained. Heterozy-gous mutations in the ATPase region ofSMARCA2 were identified in 34 out of37 patients of group 1 and on two of theseven individuals of group 2.
In the present reviewwe focused onmutation positive patients only andcollected information on a total of 61cases (Table I), aiming to better charac-terize the NCBRS clinical spectrum andevaluate possible genotype‐phenotypecorrelations.
METHODS
We contacted the physicians of allpatients known to us with NCBRS inwhom a SMARCA2mutation had beenfound, and invited them to collaborateby filling out a detailed questionnaire.The format of this questionnaire wasdeveloped to retrieve data, not only onNCBRS, but also on the related entitiesCSS, DOOR(S) syndrome and Van derAa–Kooy syndrome (caused by ADNPmutations). We supplemented the datawith information previously gathered byus, and available clinical pictures for allaffected individuals. The genotype ofthe study participants was obtainedeither through publications [Van Houdtet al., 2012; Wolff et al., 2012; Koshoet al., 2013; Santen et al., 2013; Wiec-zorek et al., 2013] or collected from themolecular genetics Diagnostic Labora-tories from the Academic MedicalCenter in Amsterdam, the Centre forHuman Genetics in Leuven and theGreat Ormond Street Hospital in Lon-don, using standard Sanger sequencing.
PATIENTS
In total, 61 cases have been analyzed,including all previously reported
SMARCA2 mutation‐positive patients(n¼ 47) [Van Houdt et al., 2012; Wolffet al., 2012; Kosho et al., 2013; Santenet al., 2013; Wieczorek et al., 2013] and14 additional unpublished individuals.Patients originate from the five con-tinents and several ethnic backgrounds,although the majority (2/3) are fromEuropean countries. The male to femaleratio is 35:26. The median age at the lastclinical evaluation is 10 years (range 2–33years). Mean paternal age at birth is 32.9years and mean maternal age is 30.1years. Due to the mixed origin offamilies we are unsure whether this fallswithin normal limits or not.
One hitherto unreported patient isdiscussed separately as the SMARCA2mutation was identified by whole‐exome sequencing in a patient notsuspected to have NCBRS, and islocated outside the ATPase domain(see below).
PHENOTYPE
Growth
One‐third of NCBRS patients (19/57)are small for gestational age. Length atbirth is<�2 SD in 21% (8/38) but>þ2SD in 13% (5/38) of the newborns.Postnatally, short stature is common,present in over half (30/56) of thepatients. Almost all have a height belowthe 50th centile. Adult height in adultmales varies between 1.44 and 1.80m(n¼ 5, mean 1.58m), and in adultfemales between 1.30 and 1.69m(n¼ 6, mean 1.57m). Body proportionsare normal. Microcephaly at birth ispresent in 23% (7/30), and later on in65% (34/52). Mean adult head size is52.8 cm in males (n¼ 4, range 50–56 cm) and 53.2 cm (n¼ 6, range50.5–54 cm) in females. Body weight is<50th centile in three‐quarter (36/46)of patients and <�2 SD in half of them(24/46). No patient is overweight.
Face
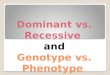
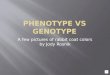
The facial characteristics are typically noteasily recognized in younger patients(Fig. 1a,b). Several patients have initiallybeen suspected to have Williams

TABLE I. Major Signs and Symptoms of 61 Individuals with Nicolaides–Baraitser Syndrome
Age groups (yrs) All patients (n¼ 61)
0–6.9(n¼ 14)
7–11.9(n¼ 23)
12–16.9(n¼ 14)
�17(n¼ 10) %
Growth at birthLength (cm): mean vs. median (range)a 48.7 vs. 49 (42–54)Length at birth <�2 SD 8/38 21.1Length at birth >þ2 SD 5/38 13.2Weight (g): mean vs median (range)a 2732 vs. 2700 (1774–3850)Weight <�2 SD 19/57 33.3Head circumference (cm): mean vs. median (range)a 33.1 vs. 33.0 (30–34.5)Head circumference <�2 SD 7/30 23.3
Growth post‐natalWeight <�2 SD 7/12 5/16 9/11 3/7 24/46 52.2Stature <�2 SD 9/14 9/19 9/14 3/9 30/56 53.6Head circumference <�2 SD 8/12 12/19 9/13 5/8 34/52 65.4
NeurodevelopmentID ‐ Mild vs. Moderate vs. Severeb 2 vs. 6 vs. 6/14 5 vs. 11 vs. 7/23 1 vs. 4 vs. 9/14 3 vs. 1 vs. 6/10 11 vs. 22 vs. 28/61 18.0 vs. 36.1 vs. 45.9Sitting age (months) — mean vs. median (range) 9 vs. 8 (6–20)Walking independently age (months) mean vs. median (range) 21 vs. 18 (10–60)Hypotonia 19/51 37.3Absent speech 19/60 31.7First words age (months) mean vs. median (range) 29.5 vs. 24 (10–96)Speech decline at a later age 9/42 21.4
Seizures 8/14 16/23 10/14 5/10 39/61 63.9Age of first seizure (months) — mean vs. median (range) 23.9 vs. 18 (0–168)
Craniofacial featuresCoarse face 9/11 14/22 13/13 7/10 43/56 76.6Progressive coarse features 6/7 4/10 4/8 4/6 18/31 58.0Low anterior hairline 7/11 15/21 10/14 7/10 39/56 69.6Sparse hair 14/14 22/23 13/14 10/10 59/61 96.7Narrow forehead 1/11 7/21 8/11 2/10 18/53 40.0Prominent eyelashes 12/14 19/23 8/14 5/10 44/61 86.2Ptosis 1/13 5/23 4/12 2/10 12/58 20.7Synophrys 2/11 4/22 4/12 2/10 12/55 21.8Thick eyebrows 10/14 14/23 10/12 6/10 40/59 67.8Increased skin wrinkling 7/14 14/23 8/14 4/10 33/61 54.1Sagging periorbital skin 9/11 16/22 8/14 5/10 38/57 66.7Narrow palpebral fissures 0/11 5/22 2/14 2/10 9/57 15.8Upward vs. Downward slant palpebral fissures 1 vs. 4/11 0 vs. 15/22 1 vs. 10/13 0 vs. 2/10 2 vs. 31/56 3.5 vs. 55.4Wide vs. Narrow nasal bridge 7 vs. 1/11 6 vs. 9/22 1 vs. 10/12 4 vs. 4/10 18 vs. 24/55 32.7 vs. 43.6Upturned nasal tip 11/13 15/23 9/14 5/10 40/60 66.7Short nose 7/11 4/22 4/11 5/8 20/52 38.5Broad nasal tip 9/11 13/22 9/13 5/10 36/56 64.3Thick alae nasi 11/13 17/23 11/13 8/10 47/59 79.7Broad nasal base 8/11 14/22 11/14 8/10 41/57 71.9Choanal stenosis 0/13 0/22 0/14 1/10 1/59 1.7Broad philtrum 11/14 12/22 12/14 9/10 44/60 73.3Long vs. Short philtrum 7 vs. 3/13 17 vs. 0/23 8 vs. 3/13 4 vs. 2/10 36 vs. 8/59 61.0 vs. 13.6Large mouth 11/13 18/23 10/14 8/10 47/60 78.3Thin upper vermillion 11/14 20/22 10/14 6/10 47/60 78.3Thick lower vermillion 12/13 19/23 11/14 8/10 50/60 83.3Drooping lower lip 5/11 11/21 6/13 8/10 30/55 54.5Cleft palate 0/14 0/23 1/14 0/10 1/61 1.6Widely spaced teeth 8/10 11/22 8/14 5/9 32/53 58.2Abnormal enamel 0/8 1/16 1/10 1/8 3/42 7.1Hypo/oligodontia 2/8 2/16 3/11 1/8 8/43 18.6Gum hypertrophy 2/8 0/21 0/10 9/10 2/48 4.0Malformed ears 4/14 9/22 3/13 1/10 17/59 28.8Ear tags 1/14 1/22 0/13 0/9 2/58 3.4
Trunk and limbsBroad neck 3/11 1/21 1/12 5/10 10/54 18.5Scoliosis 0/14 5/22 8/14 4/10 17/60 28.3Widely spaced nipples 1/8 0/18 2/11 1/9 4/45 8.8Pectus excavatum 0/11 0/19 1/8 2/9 3/47 6.4Cryptorchidism 3/8 9/13 6/9 2/4 20/34 58.8Umbilical/inguinal hernia 6/11 11/22 7/14 2/10 26/57 45.6Small 5th finger 3/14 4/21 0/13 0/9 7/57 12.3Prominent interphalangeal joints 10/13 18/22 14/14 8/10 50/59 84.7Prominent distal phalanges 9/14 17/21 9/14 5/10 40/59 67.8Fetal finger pads 2/11 11/20 6/13 3/9 22/53 41.5Dislocated hips 0/10 2/16 1/12 1/7 4/45 8.9Small patellae 0/11 0/15 0/12 1/6 1/44 2.3Joint laxity 5/14 6/12 1/18 4/8 16/52 30.8Sandal gap 5/10 10/19 7/14 4/8 26/51 50.1
304 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) ARTICLE

TABLE I. (Continued)Age groups (yrs) All patients (n¼ 61)
0–6.9(n¼ 14)
7–11.9(n¼ 23)
12–16.9(n¼ 14)
�17(n¼ 10) %
Nail anomaliesSmall nails 5th finger/toe only 0/34 0Small nails thumbs/halluces 2/33 6.1Small nails all fingers/toes 6/34 17.6
RadiologyBone age (Delayed vs. Advanced) 16 vs. 2/39 41.0 vs. 5.1Short Metacarpals vs. Metatarsals 16 vs. 4/41 39.0 vs. 9.8Short phalanges 9/43 20.9Cone shaped epiphyses 9/34 26.5
Other featuresBehavioral problems 19/?Hypertrichosis (not scalp) 22/50 44.0Eczema 22/58 37.9Feeding problems 23/49 46.9Frequent infections 13/48 27.1Cardiac defect (see text) 6/61 9.8Hearing loss 4/59 6.8Myopia 10/?Astigmatism 4/?Hypospadias 1/36 2.8Malignancy 0/61 0
aFor these calculations, only babies born between 38–42 weeks were considered: n¼ 47 for weight; n¼ 30 for length; and n¼ 28 for headcircumference.bþmild (IQ50–69);þþmoderate (IQ35–49);þþþ severe (IQ< 35); IQ levels are estimates as formal testing has often not been performed.
ARTICLE AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 305
syndrome. The face in NCBRS ischaracterized by a triangular shape,dense and prominent eyelashes, broadnasal base, thick nares, upturned nasaltip, rounded premaxilla, broad philtrum,thin upper vermilion, thick and evertedlower vermilion, and wide mouth. Thepalpebral fissures are sometimes narrowand/or downslanting. The broad phil-trum is often associated with a protru-sion of the central region of the upperlip, evoking a cupid bow–shape of theupper vermillion, especially in youngerchildren. With increasing age theamount of subcutaneous fat tissue tendsto decrease, making the skin below theorbits sagging and wrinkled, especially atthe cheeks when smiling. However,some individuals retain full cheeks.Facial characteristics are typically morepronounced with age (Fig. 1b). Thefacial features are coarse in three‐quarter(43/56) and progressive coarsening isnoted in 58% (18/31) of cases. In someadults the lower third of the facebecomes markedly broad, especially atthe angle of the mandible, and mayinvolve the neck. A single patient hadcongenital choanal atresia, and one otherhad a cleft palate.
The face in NCBRS ischaracterized by a triangularshape, dense and prominenteyelashes, broad nasal base,thick nares, upturned nasal
tip, rounded premaxilla, broadphiltrum, thin upper
vermilion, thick and evertedlower vermilion, and wide
mouth.
Hair
Sparse scalp hair is a major sign ofNCBRS that often gradually becomesmore pronounced with age and ispresent in almost all (59/61) individuals(Fig. 1b). At birth, there may be facialhypertrichosis and a low anterior hair-line. The sparseness of scalp hair canbe present in the first months of life, butcan also start to become evident in thesecond half of the first decade and in the
second decade. The growth and textureof hair is usually normal, some patientsbeing noted to have increased thickness.Microscopic evaluation does notshow significant abnormalities. In someNCBRS individuals the sparseness of thescalp hair improves with time. Theeyebrows are normal or even dense atfirst but usually follow the same reduc-tion in density over time. Eyelashesremain prominent. Pubic hair developsnormally but facial hair is very limited inadult males.
Skin and Teeth
The skin is wrinkled in half of the cases(33/61), being more noticeable at thedistal limbs. Subcutaneous veins are veryvisible, likely also due to poor develop-ment of subcutaneous fat tissue. A totalof 44% of the patients have hyper-trichosis mainly on their neck and back.Eczema is present in one third of thepatients, involves mainly the distal limbsand face, is severe in some patients, andalmost invariably decreases in the secondhalf of the first decade. The skin is oftensensitive and somewhat pale. Six patientshave generally small nails. No individual

Figure 1. Clinical pictures of some of the present individuals with Nicolaides–Baraitser syndrome. (A) Faces at various ages: a. male,8 months; b. male, 12 months; c. male, 14 months; d. male, 21 months; e. male, 2 years; f. male, 3 years, g. male, 3 years (same person as inc); h. female, 6 years; i. female, 9 years; j. female, 10 years; k. male, 10 years; l. male, 11 years; m. male, 12 years; n. male, 13 years; o. female,13 years; p. female, 16 years; q. female, 19 years (same person also depicted in B row c); r. male, 26 years. (B) Changes in facial characteristicsin three individuals with Nicolaides–Baraitser syndrome. a: male, left 5 years and 9 years, right 11 years. b: male, left 9 years, right 15 years.c: female, left 2 years, right 14 years (same person also depicted in A, patient q).
306 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) ARTICLE

ARTICLE AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 307
has small nails of only the fifth fingers.Unusual skin manifestations are hypo-hidrosis, spots of hypopigmentation, asingle café‐au‐lait spot, and patchy skinhyperpigmentation, each present in asingle individual. One patient has anextra nipple.
Teeth are widely spaced in 58.2% ofcases, and hypodontia is reported in18.6%. Dental eruption is delayed inone‐third of cases, which may involveprimary dentition, but more frequentlyinvolved secondary dentition. Surgicalinterventions to allow eruption have notbeen uncommon.
Limbs
At birth, hands and feet are usuallyunremarkable. With time, distal phalan-
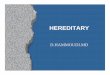
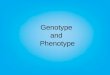
Figure 2. Variability of some of the handphalanges in all directions, prominence of int
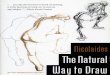
ges broaden in all directions in three‐quarters of the cases. Almost half ofthe patients have increased fetal pads.Prominent inter‐phalangeal joints arethe most characteristic sign, present in84.7% (Fig. 2). At first, mobility isnormal and in several NCBRS childrenfingers are described as hypermobile.But later on mobility often decreases,and some older individuals dislikepassive movements of their fingers.Prominence of the other large jointshas been reported in a few cases. Truearthritis has not been found in anypatient. Sandal gaps are present in 50%of the patients, and although thickeningof the distal toes occurs, it is lesspronounced compared to the fingers(Fig. 3). Cone‐shaped epiphyses, at firstthought to be a major characteristic
s of the present series of Nicolaides–Baraitser syndrome. Noteerphalangeal joints, and short metacarpals.
With time, distal phalangesbroaden in all directions inthree‐quarters of the cases.Almost half of the patientshave increased fetal pads.
Prominent inter‐phalangealjoints are the most
characteristic sign, presentin 84.7%.
[Nicolaides and Baraitser, 1993] is foundin nine individuals. A few patients haveivory epiphyses. Other radiological find-ings of the hands include short meta-carpals and/or short phalanges, which
the thickening of the distal

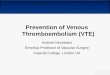
Figure 3. Variability of some of the feet of the present series of Nicolaides–Baraitser syndrome. Note the variable but usually mildshortening of the toes, sandal gaps, and some thickening of the distal phalanx of mainly the hallux.
308 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) ARTICLE
may be present in all fingers butespecially in the 4th and 5th rays. Onlya few patients have small 5th fingers ortoes but no individual has small or absentdistal phalanges and none had absentnails of the fifth fingers or toes. Bone agecan vary remarkably, from normal(53.9%), delayed (41%) or advanced(5.1%). Osteoporosis is not uncommonand indeed several patients developfractures in puberty or thereafter.Congenital hip dislocation is presentoccasionally, a single patient has patelladislocations, and a few patients havegeneralized joint laxity. Scoliosis ispresent in 28.3%.
Other Physical Features
Hearing loss is found in four patients,three with conductive and one withcongenital sensorineural deafness. My-opia was diagnosed in 10 patients andastigmatism in four. Easy chokingoccurs very frequently. Indeed, feedingproblems are common (46.9%) butusually mild and not requiring nasogas-tric tube. Many like their food to becompletely blended, a preferencewhichcontinues into adulthood. Cryptorchi-dism is present in 58.8% of the males.One boy has hypospadias. Inguinaland/or umbilical hernias were presentin 45.6% of patients, and one patient
was born with an omphalocele. Threepatients have a pectus excavatum. Sixpatients had cardiac anomalies (doubleaortic arch; small ostium secundumatrial septal defect and mild stenosis ofthe left pulmonary artery [spontaneousresolution]; mild pulmonary stenosisand mild left ventricular hypertrophy[spontaneous resolution]; small ostiumsecundum atrial septal defect andpersistent ductus arteriosus; mild aorticcoarctation and persistent ductus arte-riosus; truncus brachiocephalica cross-ing the midline and compressing thetrachea). Menarche occurred at a medi-an age of 14.8 years (range: 11–19 years)and menses were normal except for asingle female who had oligomenorrhea.At least half of the adult femaleshave poor mammary development.Recurrent infections do occur, mainlyurinary tract infections, but are notfrequent. Vesico‐ureteral reflux, IgAnephritis, marked constipation, villousatrophy, mild dyslipidemia, abnormalcarnitine profile, spastic paraplegia, areeach present in a single individual. Nopatient is known to have developed amalignancy.
Neurodevelopment and Behavior
Impaired cognition is ubiquitous inNCBRS. For the majority of patients,
no formal assessment was performedbut in most the delay was consideredto be severe (45.9%). The delay can alsobe moderate (36.1.%) or mild (18%).Language is particularly limited, andindeed at least 30% of patients neverdevelop speech. In nine patients, theirinitial words were lost or significantlyreduced later in life. In some patients theloss of speech co‐incided with their firstseizure. Hypotonia is reported in onethird of patients, but major motormilestones such as sitting (mean 9months) and walking independently(mean 21 months) are usually not verydelayed. Brain imaging was performedin at least 42 patients and usually yieldednormal results. Three patients had largeventricles and two had a small corpuscallosum. Typically patients are happyand very friendly, but may have tempertantrums and periods of aggression aswell. Often their behavior also showssymptoms that can be found in autism,although in none of the patients de-scribed was a formal diagnosis of autismmade. Several patients have a shortattention span and high threshold forpain. Many show a remarkable sensitivi-ty for loud noises, which tends todecrease with age. Several parents havenoticed that their children have oralsensitivity. Still they do like salty andspicy food. In older individuals, slowing

ARTICLE AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 309
down of movements has been reportedby parents.
Epilepsy
Epilepsy occurs in two‐third of patients.The type of seizure is variable, evenwithin the same individual. Mean andmedian ages at the first seizure are 23.9and 18 months, respectively. Seizurescan show increased frequency in somepatients despite multiple anti‐epilepticdrugs, and indeed treatment can be verydifficult. Sodium valproate is the medi-cation of first choice for many. Someparents have noticed a co‐occurrence ofdecreasingmental abilities with the onsetof seizures. It seems unlikely that thisis the case: in affected identical twins acognitive decline co‐incided with thestart of seizures in one, while in the otherthe same decline occurred but seizuresonly started two years later [Sousa et al.,2009]. We have suggested that the sameprocess that causes the decrease in
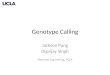
Figure 4. Schematic diagram of SMARC(NM_003070.3). To better interpret the conseendings indicate that exons start or end after a cnext exon, arrows to the left indicate that thepreviously published NCBRS patients are deaccording to UniProt (P51531). The only muglutamine domain; HSA, small helicase/SANhelicase‐related sequencemotifs (I, Ia–VI; yellolight gray boxes with dashed line) as reviewedNCBRS patients included in the present stud
cognitive abilities is also responsible forthe seizures [Sousa et al., 2009]. Theelectroencephalograms do not showspecific abnormalities.
GENOTYPE
SMARCA2
SMARCA2, also known as hBRM, islocated on chromosome 9p24.3. Thelongest transcript (NM_003070) con-tains 34 exons corresponding to an 1,590amino acids protein (NP_003061),which is one of the two alternativehomologues ATPase subunits (the otherbeing SMARCA4) that constitute thecatalytic core of the BAF complexes[Khavari et al., 1993; Muchardt andYanivl, 1993; Wang et al., 1996] (Fig. 4).Both proteins are members of the Swi2/Snf2 family, which share a helicase‐likeATPase domain [Gorbalenya et al.,1988; Flaus et al., 2006], and whichhas a translocation module consisting of
A2 and location of known germline mutations (quences of multi‐exon deletions, the shape of eachomplete codon, arrows to the right indicate that thlast two bases are located in the exon. The two inpicted. (b) Schematic of SMARCA2 protein (NPtation identified outside the ATPase region is depT‐associated domain (c) SMARCA2 ATPase dw boxes) characteristic of SNF2 group of proteins,by Flaus et al. [2006]. (d) Missense mutations (n¼y.
two similar protein domains that resem-ble the fold of the recombination proteinRecA. The common feature of the Snf2family proteins is a region of sequencesimilarity that includes seven canonicalhelicase‐related sequence motifs (labeledsequentially I, Ia ‐ VI), also found inDExx box helicases, which line at theinter‐domain cleft separating the twoRecA‐like domains and are involvedin ATP‐binding/hydrolysis as well asDNA‐binding [Dürr et al., 2006; Fair-man‐Williams et al., 2010]. In thisregion, 14 additional conserved blocks(A‐N) were also described [Flauset al., 2006] (Fig. 4). SMARCA2 andSMARCA4 proteins are highly similarwith a sequence identity of 74% inhumans and they display similar enzy-matic properties [Khavari et al., 1993;Muchardt and Yanivl, 1993; Chibaet al., 1994]. Despite the similaritiesbetween these two proteins and that incertain circumstances they can poten-tially compensate for each other
n¼ 61). (a) SMARCA2 longest transcriptexon indicates the reading frame. Square
e last base of the last codon is located in the‐frame multi‐exon deletions identified in_003061.3), showing the main domains
icted (see text). QLQ, glutamine‐leucine‐omain highlighting the seven canonicaland 14 additional conserved blocks (A‐N,59) identified thus far as causative in the

310 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) ARTICLE
[Strobeck et al., 2000], a growingnumber of studies have shown that thesetwo alternative ATPase subunits havedifferent and even antagonist roles in theregulation of differentiation, transcrip-tional control, and other important cellprocesses [Reyes et al., 1998; Bultmanet al., 2000; Kadam and Emerson, 2003;Flowers et al., 2009].
Mutations in NCBRS
In the present review, we have onlyincorporated patients in whom a muta-tion was found. Indeed, in the last twoyears in all patients in whom the presentauthors (SBS, RCH) were convincedthe diagnosis NCBRS was correct, amutation was present, so we have noknowledge of NCBRS patients withoutSMARCA2 mutation. Still, noSMARCA2 mutation was found in3/37 cases that we had classified asconvincing NCBRS phenotype [VanHoudt et al., 2012], and in two of these(the patient described by Krajewska‐Walasek et al. [1996] and patient 18 fromSousa et al. [2009]) a pathogenicARID1B mutation was identified. Clin-ically the patients were reclassified ashaving Coffin–Siris syndrome [Santenet al., 2013]. There is also a patientdescribed by Wieczorek et al. [2013],classified as NCBRS without mutationidentified in any of the genes from BAFcomplex. The clinical manifestations inthis patient are not completely convinc-ing for NCBRS however.
All presently known germlineSMARCA2 mutations are depicted inFigure 4. All mutations identified inNCBRS are missense (n¼ 59) or in‐frame deletions (n¼ 2) affecting theATPase SMARCA2 domain. All parentswho were available for molecular analy-sis did not have the same mutation astheir child, which is in accordancewith the predicted genetic etiology.The exonic mutations were clusteredin exons 15 (n¼ 5), 18 (n¼ 16), 19(n¼ 4), 23 (n¼ 2), 24 (n¼ 11), and 25(n¼ 21), so in the region encoding theATPase domain (exon 15–25; 490amino acids). Several mutations wererecurrent; we identified in total 48different missense mutations in 59
patients, affecting 34 different ultra‐conserved amino acids. All mutationswere predicted to be damaging byin silico analysis. The ATPase domain is100% conserved in chimpanzee andmouse and 94.7% conserved in zebraand fish compared to the human proteinand was shown to be functionallyconserved [Khavari et al., 1993; Elfringet al., 1994]. Considering that deletionsencompassing the whole humanSMARCA2 gene do not cause NCBRS[Christ et al., 1999], that mice lackingfunctional mSMARCA2 do not presentwithmajor developmental abnormalities[Reyes et al., 1998; Bultman et al., 2000;Koga et al., 2009], that NCBRSmutations cluster at the SMARCA2ATPase region and that none of thesevariants are truncating, we have pre-dicted that the mutations identified inNCBRS do not lead to haploinsuffi-ciency, but rather have a dominant‐negative or gain‐of‐function effect [VanHoudt et al., 2012].
All mutations identified inNCBRS are missense (n¼ 59)or in‐frame deletions (n¼ 2)
affecting the ATPaseSMARCA2 domain.
Mutations of yeast SNF2 affectingthe ATPase domain conserved motifsresulted in dominant‐negative activityin a functional assay [Richmond andPeterson, 1996], and two of thesemutations are identical to SMARCA2mutations in individuals with NCBRS,while at least an additional four map tothe samemotifs [VanHoudt et al., 2012].This clustering of mutations providesgenetic evidence that abolishing theATP hydrolyzing engine, whichprovides energy directed toward therepositioning of histones on DNA,causes functional inactivation [Hall andMatson, 1999; De La Serna et al., 2000].Several human SMARCA2 (andSMARCA4) mutants involving thehelicase domains were produced and
studied [Khavari et al., 1993; Muchardtand Yanivl, 1993; De La Serna et al.,2000; Magnani and Cabot, 2009]. Inparticular, a missense mutation affectingthe highly conserved lysine residue onthe ATP‐binding site GKT (motif I),also studied in yeast [Laurent et al., 1993;Richmond and Peterson, 1996] andaffecting the same residue as p.Lys755-Arg identified in one NCBRS patient,was transfected in C33 [Muchardt andYanivl, 1993] and in NIH 3T3 cells [DeLa Serna et al., 2000]. These studiesshowed that these mutant proteinshad normal nuclear localization, co‐immunoprecipitated with other unitsof the BAF complex, and impaired thecomplex function.
These data support a model forNCBRS cellular/nuclear pathogenesis,in which non functional but structurallyundamaged SMARCA2 generates BAFcomplexes that may be intact withrespect to their composition and properpositions in the chromatin; but, none-theless, are functionally inactive resultingin a dominant‐negative effect. As themutant SMARCA2 are able to recruitthe other “targeting” subunits of thecomplex in the mentioned studies, thesecomplexes are likely to be targeted toappropriate places in the genome, wherethey would fail to function, presumablyin some event involving the remodelingof nucleosome structure [De La Sernaet al., 2000]. As a consequence andthrough competitive inhibition, at eachmoment, wild‐type endogenous BAFcomplexes would not have access to thegenomic positions already taken by themutant complexes. As previously sug-gested [De La Serna et al., 2000], othermechanisms may contribute to thiseffect, mainly the formation of incom-plete BAF complexes around the mutantATPase subunits depleting the wild‐typeendogenous SMARCA2 and SMARCA4proteins of one or more of theirassociated subunits. Another questionthat arises from this proposed mecha-nism is which type of BAF complexesare affected by these mutant proteins,whether it is only the ones that useSMARCA2 or also the ones that useSMARCA4. A combination of theseeffects is likely to occur.

ARTICLE AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 311
As for CSS [Santen et al., 2012],there is no evidence of increased risk ofmalignancy in NCBRS patients: Thismight suggest that the effect of BAFcomplex subunits germline mutationsidentified in neurodevelopmental disor-ders, such as NCBRS and CSS, isdifferent from the effect of somaticmutations involving the same subunitsin cancer (and germline mutationsassociated with tumor predispositionsyndromes). Nevertheless, the presentcohort is in general still young, andoccurrence of tumors at older agescannot yet be excluded.
GENOTYPE‐PHENOTYPECORRELATIONS
As we did not include mutation‐negative patients in our study, wecannot compare the phenotype ofmutation‐positive versus mutation‐neg-ative NCBRS patients. We have evalu-ated potential correlations between thevarious parts of the phenotype. There isno correlation between the facial char-acteristics and the neurodevelopmentallevel. There is a correlation between theseverity of ID and epilepsy, speechimpairment, short stature and micro-cephaly; individuals with severe ID aremore likely to have postnatal shortstature (17/25 vs. 12/22 vs. 1/9 patientswith severe, moderate and mild ID,respectively), microcephaly (20/23, vs.11/20 vs. 3/9 patients with severe,moderate and mild ID, respectively),absent speech (15/27 vs. 4/22 vs. 0/11patients with severe, moderate and mildID, respectively) and seizures (23/28, vs.13/22 vs. 3/11 patients with severe,moderate and mild ID, respectively).
Comparing the groups with (39/59)and without (20/59) seizures, there isa correlation with ID severity (23/39patients with seizures have severe ID vs.13/39 having moderate ID and 3/39having mild ID). Severe ID and seizuresare especially prevalent in mutationslocated in motif VI (and II), and less inmutations affecting alanine 1201, pro-line 883 and leucine 946. Patients withseizures also have higher prevalenceof microcephaly (25/35, vs. 10/35 inpatients without seizures).
As illustrated in Figure 4, themissense mutations identified in thepresent NCBRS cohort locate in heli-case motifs I, Ia, II, III, IV, V, and VI andin the SNF2 conserved blocks B, D, andH. In addition, eight highly conservedamino acid residues affected by muta-tions in 13 NCBRS patients are locatedin areas not previously identified asespecially conserved or associated witha particular role, suggesting that thesemay also constitute functionally impor-tant motifs/residues of the ATPasedomain. This seems particularly inter-esting in the area distal to motif VI andblocksM/N, where mutations are foundin seven patients (especially residues1201–1205).
More than half of NCBRS patients(36/61) have mutations affecting the C‐terminal helicase region (Helicase_C)from the SMARCA2 ATPase domain(Fig. 4). This group tends to have severeID and higher chance of developingseizures. Conserved motif VI (codedby exon 25) constitutes a hotspot with11 patients having mutations located init, six of which affect the arginine inposition 1,159. This highly conservedresidue interacts with the g‐phosphateof the bound ATP, stabilizing thedomain’s close arrangement, and isalso necessary for the ATP hydrolysis[Dürr et al., 2006]. A mutation affectingthis residue in the yeast was shownto have a more effective dominant‐negative effect than mutations affectingthe ATP‐binding site [Richmond andPeterson, 1996]. These studies corrob-orate the phenotype severity of the sixidentified patients with mutationsaffecting this residue: all have severeID, all have epilepsy (first episode at1–2.5 years of life), three patientsnever developed speech and furthertwo lost speech when seizures started,three have short stature and four havemicrocephaly. Four patients with mod-erate‐severe phenotypes have mutationsaffecting the highly conserved argininein position 1,105 located at conservedblock D.
Two patients are described withmulti‐exon deletions affecting the C‐terminal helicase domain (Fig. 4a) andwhich are also reviewed in the present
study. Patient 1 from Wolff et al. [2012](Fig. 1Ab) has a 32 kb de novo in‐framedeletion of exons 20–26 and subject19 from Tsurusaki et al. [2012] (later re‐described as SMARCA2‐1 by Koshoet al. [2013]) has a 55 kb in‐framedeletion of exons 20–27. Both patientshave typical physical features of NCBRSassociated with severe ID, absent speech,and seizures, but the Japanese patienthas additional unusual features such ashypospadias and an episode of grosshaematuria caused by immunoglobulinA nephropathy.
Twenty patients have mutations atthe N‐terminal/ATP‐binding helicaseregion, nine of which located at themotif II (Fig. 4), which is also involved inATP hydrolysis. However, in here wewere not able to identify any consistentcorrelation.
Mutations p.Ala1201Val (n¼ 4),p.Pro883Leu (n¼ 3), and p.Leu946Ser/p.Leu946Phe (n¼ 2) are associated inthe present study with a mild‐moderatedegree of intellectual disability, lessspeech impairment and a reducedchance of developing epilepsy. However,given the small number of patients andthe fact that severely affected patientsharbor mutations located in adjacentresidues, one must be cautious ininterpreting these observations.
All aforementioned patients withSMARCA2 mutations have been iden-tified by targeted screening motivatedby a NCBRS phenotype. We mustassume that the phenotypic spectrumof SMARCA2 mutations can be wider.We reviewed a single patient (Fig. 5)in whom there was no suspicion forNCBRS and in whom exome sequenc-ing identified a de novo SMARCA2heterozygous variant (c.4258G>A, p.Gly1420Arg). This variant is not locatedat the ATPase helicase‐like domain butat the evolutionarily conserved acetyl‐lysine binding bromodomain (Fig. 4).This patient has phenotype distinct fromNCBRS (no sparse hair or typical face,no independent walking and severefeeding problems) but still demonstratesoverlap with NCBRS (severe ID,seizures, absent speech, rounded pre‐maxilla, decreased subcutaneous fat, andslight prominence of interphalangeal

Figure 5. Clinical photographs of the patient with mutation p.Gly1420Arg located at the SMARCA2 bromodomain and identified bywhole exome sequencing (male: left six years, middle seven years and right facial and hand photograph at 17 years). This patient was notincluded in the analyzed cohort (see text). Note the distinct but overlapping phenotype with NCBRS.
312 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) ARTICLE
joints in the second decade of life)(Fig. 5). Although this variant is mostlikely causative for the phenotype in thispatient, we did not include this patient inthe NCBRS group analysis due to thedifferences in phenotype and mutationlocation. In our opinion, the diagnosis ofNCBRS should be kept for patientswith sufficient clinical resemblance tothe typical NCBRS phenotype, whichalmost invariably can be caused by a denovo mutation affecting the SMARCA2ATPase domain. Only by checking largegroups of unselected individuals with IDwill we learn the phenotype(s) thatcan be caused by mutations inSMARCA2. In comparison, mutationsin SMARCA4 in individuals withCoffin–Siris syndrome are typicallymissense or in‐frame deletions, andmost are also located at the ATPasedomain. A few CSS patients have beendescribed with similar mutations outsidethis domain [Kosho et al., 2013; Santenet al., 2013] (but not at the bromodo-main) while inactivating germlineSMARCA4 mutations have been iden-tified as causing specific tumor predis-position syndromes (not associated withID) [Schneppenheim et al., 2010; Jelinicet al., 2014; Ramos et al., 2014; Wit-kowski et al., 2014].
Proposed Diagnostic Approach
In countries where whole exome se-quencing is not available on a diagnosticbasis, the molecular approach will bethrough Sanger sequencing. If a patientpresents with a phenotype suggestive of
NCBRS, a careful clinical evaluation isneeded, especially of the limbs andincluding radiographs of the hands.Small distal phalanges or small nails ofthe 5th finger has never been reported inNCBRS, and such a finding points tothe presence of Coffin–Siris syndrome inthe patient. If the diagnosis NCBRSremains likely, sequencing of the exons15–25 of SMARCA2 should be the firstdiagnostic test (proposed sequence:18þ 24þ 25> 15þ 19þ 23> 16þ 17þ 20þ 21þ 22). If this is negative,heterozygous in‐frame deletions of thisregion of SMARCA2 should be investi-gated by MLPA or by detailed arrayCGH. If no SMARCA2 variants areidentified, screening of the wholecoding region of ARID1B gene and, ifnegative, exclusion of heterozygouswhole gene or partial deletions shouldbe the following step. If no mutation isfound, re‐evaluation of the clinicalmanifestations of the patient is sug-gested. If still compatible with NCBRS,untargeted whole exome sequencingcan be considered on a research basis.Alternatively, if locally available, one canperform whole exome sequencing on adiagnostic basis ab initio, either targetedfor all genes coding for proteins in theBAF complexes subunits [Wieczoreket al., 2013], or targeted for all genesknown to cause intellectual disability.If no mutations are identified in thesegenes, untargeted whole exome se-quencing on a research basis in theaffected patient and both parents search-ing for de novo mutations may beindicated.
In the near future, it is predictablethat whole exome sequencing willbecome part of routine diagnostics inmany centers and the above stepwiseSanger approach will probably becomeless utilized. Only then wewill be able toassess the true phenotypic variability ofthis group of conditions and evaluatehow to improve the clinical classificationdiscussed here. A molecularly basedclassification of patients allows a moredetailed understanding of the disease, itsphenotyping (“next‐generation pheno-typing” [Hennekam and Biesecker,2012]) and its natural history. Thepublication of a significant number ofadditional variants involving the BAFcomplex genes and the phenotypepresent in the corresponding individualswill bring insight into the mechanismsunderlying the pathophysiological pro-cess and facilitate the discriminationbetween non‐pathogenic and pathogen-ic variants. Santen et al. [2013] extractedand analyzed all documented variants inthe BAF subunits from the ExomeVariant Server to verify if these putative-ly non‐pathogenic variants could beclassified rightfully as such or might havebeen classified as pathogenic variants ifthey would have been found in patientswith ID. They concluded that variantscan be reclassified reliably for mostgenes. However, for SMARCA2 (asfor SMARCA4 and SMARCE1), it isdifficult to discriminate between non‐pathogenic and pathogenic variantswithout access to parental DNA [Santenet al., 2013]. Exome data on largercohorts of phenotyped individuals,

ARTICLE AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 313
confirmatory studies in variants presentin databases to exclude false positivesand functional studies will be needed toimprove our ability to accurately classifyvariants in these genes [MacArthuret al., 2014]. It will also allow us toassess the phenotypic effect of second orfurther variants in other BAF complexsubunits or elsewhere in the genome.
CONCLUSION
In conclusion, NCBRS has a specificphenotype that has a much more narrowspectrum than the phenotype in Coffin–Siris syndrome. There is a minority ofpatients in whom differentiation be-tween NCBRS and Coffin–Siris syn-drome is difficult, but with increasingexperience of clinicians this will becomeeasier. NCBRS is not only distinctbut also genetically homogeneous as allgenuine patients have de novomutationsin a single gene, SMARCA2. Indeed, inreverse, SMARCA2 mutations have notbeen detected in individuals with otherID syndromes (except a single casedetected by whole exome sequencing,as described above). Our study on theconsequences of having a SMARCA2mutation is biased, as only patients withsyndromic forms of intellectual disabilityin which NCBRS is considered arescreened for mutations using classicalSanger sequencing approaches.With theincreasing use of whole exome sequenc-ing targeted for genes that cause intel-lectual disability, we will recognizeSMARCA2 mutations in individualswith phenotypes that are less clearlydiagnostic of NCBRS. The consequen-ces of such mutations for patients may,temporarily, remain uncertain, so de-tailed phenotyping will be mandatory toelucidate this. These studies, togetherwith long‐term follow‐up data ofcohorts of NCBRS patients shouldprovide additional information that canbe used to optimize care to patients andsupport to their families.
ACKNOWLEDGMENTS
We thank the NCBRS support groupand all families for their encouragementand assistance over the years. S.B.S. was
supported by the Fundação Para aCiência e Tecnologia (SFRH/BD/46778/2008).
The Nicolaides‐Baraitser Syn-drome International Consortium:Omar Abdul‐Rahman (Jackson), Mar-ielle Alders (Amsterdam), Silvia Azzar-ello‐Burri (Zurich), Armand Bottani(Geneva), Sarah Bowdin (Toronto),Marco Castori (Rome), Valerie Corm-ier‐Daire (Paris), Matthew Deardorff(Philadelphia), Miquel Del CampoCasanelles (Barcelona), Koenraad Dev-riendt (Leuven), Christine Fauth (Inns-bruck), Isabel Filges (Basel), Alan Fryer(Liverpool), Livia Garavelli (ReggioEmilia), Gabriele Gillessen‐Kaesback(Luebeck), Bryan Hall (Lexington),Ohasi Hirofumi (Nagoya), Susan Holder(London), Juliane Hoyer (Erlangen),Lucy Jenkins (London), Jacub Klapeki(Waszawa), Malgorzata Krajewska‐Walasek (Warszawa), Tomoki Kosho(Matsumoto), Alma Kuechler (Essen),KayMacDermot (London), AlexMagee(Belfast), Francesca Mari (Siena),Michele Mathieu‐Dramard (Amiens),Melanie Napier (Toronto), Luis A.Pérez‐Jurado (Barcelona), Fanny Mor-ice Picard (Bordeaux), Gilles Morin(Amiens), Victoria Murday (Glasgow),Jacek Pilch (Katowice), Anne Ronan(Waratah), Elizabeth Rosser (London),Gijs W.E. Santen (Leiden), RichardScott (London), Angelo Selicorni (Mi-lano), Nora Shannon (Nottingham),Fernando Santos‐Simarro (Madrid),Helen Stewart (Oxford), Marie‐Josevan den Boogaard (Utrecht), Catheli-neVilain (Brussels), JorisVermeesch(Leuven), AnnickVogels (Leuven),Emma Wakeling (London), DagmarWieczorek (Essen), Gozde Yesil (Istan-bul), OrsettaZuffardi (Pavia), ChristianeZweier (Erlangen), Sérgio B. Sousa(Coimbra) and Raoul C. Hennekam(Amsterdam).
REFERENCES
Bultman S, Gebuhr T, Yee D, La Mantia C,Nicholson J, GilliamA,Randazzo F,MetzgerD, Chambon P, Crabtree G, Magnuson T.2000. A Brg1 null mutation in the mousereveals functional differences among mam-malian SWI/SNF complexes. Mol Cell6:1287–1295.
Castori M, Covaciu C, Rinaldi R, Grammatico P,Paradisi M. 2008. A rare cause of syndromichypotrichosis: Nicolaides‐Baraitser syn-drome. J Am Acad Dermatol 59:S92–98.
Chiba H, Muramatsu M, Nomoto A, Kato H.1994. Two human homologues of Saccharo-myces cerevisiae SWI2/SNF2 and Drosoph-ila brahma are transcriptional coactivatorscooperating with the estrogen receptor andthe retinoic acid receptor. Nucleic Acids Res22:1815–1820.
Christ LA, Crowe CA, Micale MA, Conroy JM,Schwartz S. 1999. Chromosome breakagehotspots and delineation of the critical regionfor the 9p‐deletion syndrome. Am J HumGenet 65:1387–1395.
Coffin GS, Siris E. 1970. Mental retardation withabsent fifth fingernail and terminal phalanx.Am J Dis Child 119:433–439.
De La Serna IL, Carlson Ka, Hill Da, Guidi CJ,Stephenson RO, Sif S, Kingston RE,Imbalzano aN. 2000. Mammalian SWI‐SNF complexes contribute to activation ofthe hsp70 gene. Mol Cell Biol 20:2839–2851.
Dürr H, Flaus A, Owen‐Hughes T, Hopfner KP.2006. Snf2 family ATPases and DExx boxhelicases: Differences and unifying conceptsfrom high‐resolution crystal structures. Nu-cleic Acids Res 34:4160–4167.
Elfring LK, Deuring R, McCallum CM, PetersonCL, Tamkun JW. 1994. Identification andcharacterization of Drosophila relatives of theyeast transcriptional activator SNF2/SWI2.Mol Cell Biol 14:2225–2234.
Fairman‐Williams ME, Guenther UP, JankowskyE. 2010. SF1 and SF2 helicases: Familymatters. Curr Opin Struct Biol 20:313–324.
Flaus A, Martin DM, Barton GJ, Owen‐Hughes T.2006. Identification of multiple distinct Snf2subfamilies with conserved structural motifs.Nucleic Acids Res 34:2887–2905.
Flowers S, Nagl NG, Beck GR, Moran E. 2009.Antagonistic roles for BRM and BRG1SWI/SNF complexes in differentiation.J Biol Chem 284:10067–10075.
Gana S, Panizzon M, Fongaro D, Selicorni A,Memo L, Scandurra V, Vannucci C, BigozziM, Scordo MR. 2011. Nicolaides‐Baraitsersyndrome: Two new cases with autismspectrum disorder. Clin Dysmorphol 20:38–41.
Gorbalenya AE, Koonin EV, Donchenko AP,Blinov VM. 1988. A novel superfamily ofnucleoside triphosphate‐binding motif con-taining proteins which are probably involvedin duplex unwinding in DNA and RNAreplication and recombination. FEBS Lett235:16–24.
Hall MC, Matson SW. 1999. Helicase motifs: theengine that powers DNA unwinding. MolMicrobiology 34: 867–877.
Hennekam RC, Biesecker LG. 2012. Next‐generation sequencing demands next‐generation phenotyping. Hum Mutat 33:884–886.
Van Houdt JKJ, Nowakowska BA, Sousa SB, vanSchaik BDC, Seuntjens E, Avonce N, SifrimA, Abdul‐Rahman OA, van den BoogaardMJH, Bottani A, Castori M, Cormier‐DaireV, Deardorff MA, Filges I, Fryer A, Fryns JP,Gana S, Garavelli L, Gillessen‐Kaesbach G,Hall BD, Horn D, Huylebroeck D, KlapeckiJ, Krajewska‐Walasek M, Kuechler A, Lines

314 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) ARTICLE
MA, Maas S, Macdermot KD, McKee S,Magee A, de Man SA, Moreau Y, Morice‐Picard F, Obersztyn E, Pilch J, Rosser E,Shannon N, Stolte‐Dijkstra I, Van Dijck P,Vilain C, Vogels A, Wakeling E, WieczorekD,Wilson L, Zuffardi O, van Kampen AHC,Devriendt K, Hennekam R, Vermeesch JR.2012. Heterozygous missense mutations inSMARCA2 cause Nicolaides‐Baraitser syn-drome. Nat Genet 44:445–449S1.
Jelinic P, Mueller JJ, Olvera N, Dao F, Scott SN,Shah R, Gao J, Schultz N, GonenM, SoslowRA, Berger MF, Levine DA. 2014. Recur-rent SMARCA4 mutations in small cellcarcinoma of the ovary. Nat Genet 46:424–426.
Kadam S, Emerson BM. 2003. Transcriptionalspecificity of human SWI/SNF BRG1 andBRM chromatin remodeling complexes.Mol Cell 11:377–389.
Khavari PA, Peterson CL, Tamkun JW, MendelDB, Crabtree GR. 1993. BRG1 contains aconserved domain of the SYI2/SNF2 familynecessary for normal mitotic growth andtranscription. Nature 366:170–174.
KogaM, IshiguroH, Yazaki S, Horiuchi Y, AraiM,Niizato K, Iritani S, Itokawa M, Inada T,Iwata N, Ozaki N, Ujike H, Kunugi H,Sasaki T, Takahashi M, Watanabe Y, SomeyaT, Kakita A, Takahashi H, Nawa H,Muchardt C, Yaniv M, Arinami T. 2009.Involvement of SMARCA2/BRM in theSWI/SNF chromatin‐remodeling complexin schizophrenia. HumMol Genet 18:2483–2494.
Kosho T, Okamoto N, Ohashi H, Tsurusaki Y,Imai Y, Hibi‐Ko Y, Kawame H, Homma T,Tanabe S, Kato M, Hiraki Y, Yamagata T,Yano S, Sakazume S, Ishii T,Nagai T,Ohta T,Niikawa N, Mizuno S, Kaname T, NaritomiK, Narumi Y, Wakui K, Fukushima Y,Miyatake S, Mizuguchi T, Saitsu H, MiyakeN,MatsumotoN. 2013. Clinical correlationsof mutations affecting six components of theSWI/SNF complex: Detailed description of21 patients and a review of the literature. AmJ Med Genet A 161:1221–1237.
Krajewska‐Walasek M, Chrzanowska K, Czer-miska‐Kowalska A. 1996. Another patientwith an unusual syndrome of mentalretardation and sparse hair? ClinDysmorphol5:183–186.
Laurent BC, Treich I, Carlson M. 1993. The yeastSNF2/SWI2 protein has DNA‐stimulatedATPase activity required for transcriptionalactivation. Genes Dev 7:583–591.
MacArthur DG, Manolio TA, Dimmock DP,RehmHL, Shendure J, Abecasis GR, AdamsDR, Altman RB, Antonarakis SE, AshleyEA, Barrett JC, Biesecker LG, ConradDF, Cooper GM, Cox NJ, Daly MJ,Gerstein MB, Goldstein DB, HirschhornJN, Leal SM, Pennacchio LA, Stamatoyan-nopoulos JA, Sunyaev SR, Valle D, VoightBF,WincklerW, Gunter C. 2014. Guidelinesfor investigating causality of sequence var-iants in human disease. Nature 508:469–476.
Magnani L, Cabot RA. 2009. Manipulation ofSMARCA2 and SMARCA4 transcript levelsin porcine embryos differentially altersdevelopment and expression of SMARCA1,SOX2, NANOG, and EIF1. Reproduction137:23–33.
Morin G, Villemain L, Baumann C, Mathieu M,Blanc N, Verloes A. 2003. Nicolaides‐Baraitser syndrome: Confirmatory report ofa syndrome with sparse hair, mental retarda-tion, and short stature and metacarpals. ClinDysmorphol 12:237–240.
Muchardt C, Yanivl M. 1993. A human homo-logue of Saccharomyces cerevisiae SNF2/SWI2 and Drosophila brm genes potentiatestranscriptional activation by the glucocorti-coid receptor. EMBO J 12:4279–4290.
Nicolaides P, Baraitser M. 1993. An unusualsyndrome with mental retardation and sparsehair. Clin Dysmorphol 2:232–236.
Ramos P, Karnezis AN, Craig DW, Sekulic A,Russell ML, Hendricks WPD, CorneveauxJJ, Barrett MT, Shumansky K, Yang Y, ShahSP, Prentice LM, Marra MA, Kiefer J,Zismann VL, McEachron TA, Salhia B,Prat J, D’Angelo E, Clarke BA, Pressey JG,Farley JH, Anthony SP, Roden RBS,Cunliffe HE, Huntsman DG, Trent JM.2014. Small cell carcinoma of the ovary,hypercalcemic type, displays frequent inacti-vating germline and somatic mutations inSMARCA4. Nat Genet 46:427–429.
Reyes JC, Barra J, Muchardt C, Camus A, BabinetC, YanivM. 1998. Altered control of cellularproliferation in the absence of mammalianbrahma (SNF2alpha). EMBO J 17:6979–6991.
Richmond E, Peterson CL. 1996. Functionalanalysis of the DNA‐stimulated ATPasedomain of yeast SWI2/SNF2. Nucleic AcidsRes 24:3685–3692.
Santen G, Kriek M, Van Attikum H. 2012. SWI/SNF complex in disorder, SWItching frommalignancies to intellectual disability. Epi-genetics 1219–1224.
Santen GWE, Aten E, Vulto‐van Silfhout AT,Pottinger C, van Bon BWM, van Mind-erhout IJHM, Snowdowne R, van der LansCaC, Boogaard M, Linssen MML, Vijfhui-zen L, van derWielenMJR, Vollebregt MJE,the Coffin‐Siris consortium, Breuning MH,Kriek M, van Haeringen A, den Dunnen JT,Hoischen A, Clayton‐Smith J, de Vries BBA,Hennekam RCM, van Belzen MJ. 2013.Coffin‐Siris Syndrome and the BAF Com-plex: Genotype‐Phenotype Study in 63Patients. Hum Mutat 34:1519–1528.
Schneppenheim R, Frühwald MC, Gesk S,Hasselblatt M, Jeibmann A, Kordes U, KreuzM, Leuschner I, Martin Subero JI, Obser T,Oyen F, Vater I, Siebert R. 2010. Germlinenonsense mutation and somatic inactivationof SMARCA4/BRG1 in a family withrhabdoid tumor predisposition syndrome.Am J Hum Genet 86:279–284.
Schrier Vergano S, Santen G, Wieczorek D,Wollnik B, Matsumoto N, Deardorff M.2013. Coffin‐Siris Syndrome. RA, PagonMP, AdamTD, Bird, al, Ed GeneReviewsTM
[Internet] Seattle. Univ Washington. Seattle:1993‐2013 Available from http://wwwncbinlmnihgov/books/NBK131811/
Sousa SB, Abdul‐Rahman OA, Bottani A,Cormier‐Daire V, Fryer A, Gillessen‐Kaes-bachG,HornD, JosifovaD, Kuechler A, LeesM,MacDermot K, Magee A,Morice‐PicardF, Rosser E, Sarkar A, Shannon N, Stolte‐Dijkstra I, Verloes A, Wakeling E, Wilson L,Hennekam RC. 2009. Nicolaides‐Baraitsersyndrome: Delineation of the phenotype.Am J Med Genet A 149A:1628–1640.
Strobeck MW, Fribourg AF, Puga A, Knudsen ES.2000. Restoration of retinoblastoma medi-ated signaling to Cdk2 results in cell cyclearrest. Oncogene 19:1857–1867.
Tsurusaki Y, Okamoto N, Ohashi H, Kosho T,Imai Y, Hibi‐Ko Y, Kaname T, Naritomi K,Kawame H, Wakui K, Fukushima Y,Homma T, Kato M, Hiraki Y, Yamagata T,Yano S,Mizuno S, Sakazume S, Ishii T,NagaiT, Shiina M, Ogata K, Ohta T, Niikawa N,Miyatake S, Okada I, Mizuguchi T, Doi H,Saitsu H, Miyake N, Matsumoto N. 2012.Mutations affecting components of the SWI/SNF complex cause Coffin‐Siris syndrome.Nat Genet 44:376–8.
Wang W, Côté J, Xue Y, Zhou S, Khavari PA,Biggar SR, Muchardt C, Kalpana GV, GoffSP, Yaniv M, Workman JL, Crabtree GR.1996. Purification and biochemical hetero-geneity of the mammalian SWI‐SNF com-plex. EMBO J 15:5370–5382.
Wieczorek D, Bögershausen N, Beleggia F,Steiner‐Haldenstätt S, Pohl E, Li Y, Milz E,Martin M, Thiele H, Altmüller J, Alanay Y,Kayserili H, Klein‐Hitpass L, Böhringer S,Wollstein A, Albrecht B, Boduroglu K,Caliebe A, Chrzanowska K, Cogulu O,Cristofoli F, Czeschik JC, Devriendt K,Dotti MT, Elcioglu N, Gener B, GoeckeTO, Krajewska‐Walasek M, Guillén‐Nav-arro E, Hayek J, Houge G, Kilic E, Simsek‐Kiper PÖ, López‐González V, Kuechler A,Lyonnet S, Mari F, Marozza A, MathieuDramard M, Mikat B, Morin G, Morice‐Picard F, Ozkynay F, Rauch A, Renieri A,Tinschert S, Utine GE, Vilain C, Vivarelli R,Zweier C, Nürnberg P, Rahmann S,Vermeesch J, Lüdecke HJ, Zeschnigk M,Wollnik B. 2013. A comprehensivemolecular study on Coffin‐Siris andNicolaides‐Baraitser syndromes identifies abroad molecular and clinical spectrumconverging on altered chromatin remodel-ing. Hum Mol Genet 22(25):5121‐35.22:5121–5135.
Witkowski L, Carrot‐Zhang J, Albrecht S, Fahi-miniya S, Hamel N, Tomiak E, Grynspan D,Saloustros E, Nadaf J, Rivera B, Gilpin C,Castellsagué E, Silva‐Smith R, Plourde F,Wu M, Saskin A, Arseneault M, Karabakht-sian RG, Reilly EA, Ueland FR, MargiolakiA, Pavlakis K, Castellino SM, Lamovec J,Mackay HJ, Roth LM, Ulbright TM,Bender TA, Georgoulias V, Longy M,Berchuck A, Tischkowitz M, Nagel I,Siebert R, Stewart CJ, Arseneau J, McClug-gage WG, Clarke BA, Riazalhosseini Y,Hasselblatt M, Majewski J, Foulkes WD.2014. Germline and somatic SMARCA4mutations characterize small cell carcinomaof the ovary, hypercalcemic type. Nat Genet46:438–443.
Witters I, Fryns JP. 2003.Mental retardation, sparsehair, facial dysmorphism with a prominentlower lip, and lipodystrophy. A variantexample of Nicolaides‐Baraitser syndrome?Genet Couns 14:245–247.
Wolff D, Endele S, Azzarello‐Burri S, Hoyer J,Zweier M, Schanze I, Schmitt B, Rauch A,Reis A, Zweier C. 2012. In‐frame deletionand missense mutations of the C‐Terminalhelicase domain of SMARCA2 in threepatients with Nicolaides‐Baraitser syndrome.Mol Syndromol 237–244.