Embed Size (px)
Citation preview
Physical activity and circulating endothelialprogenitor cells: an intervention studyFrancesca Cesari*, Francesco Sofi*,†,‡, Anna M. Gori*,‡, Ilaria Corsani†, Andrea Capalbo†, Roberto Caporale§,Rosanna Abbate*, Gian F. Gensini*,‡ and Alessandro Casini†
*Department of Medical and Surgical Critical Care, Thrombosis Centre, University of Florence, Florence, Italy,†Agency of Nutrition, Azienda Ospedaliero-Universitaria Careggi, Florence, Italy, ‡Don Carlo Gnocchi Foundation,Florence, Italy, §Central Laboratory, Azienda Ospedaliero-Universitaria Careggi, Florence, Italy
ABSTRACT
Background To assess the effect of a personalized physical activity programme on weight and circulating (CPC)and endothelial progenitor cells (EPC) in overweight and obese subjects.
Materials and methods Anthropometric measurements with body composition, cardiopulmonary test, maxi-mal stress exercise test with maximal oxygen uptake (VO2max) and a series of biochemical analyses were takenbefore (T0) and after 3 months of physical activity (T1) in a total of 80 overweight and obese subjects. CPC andEPC were determined using flow cytometry and were defined as CD34+, CD133+ and CD34+ ⁄ CD133+ for CPCand CD34+KDR+, CD133+KDR+ and CD34+CD133+KDR+ for EPC.
Results At the end of the programme, we divided the population into two groups, compliant individuals (groupA, n = 47) and noncompliant individuals (group B, n = 33). Group A reported significant reductions of weight by3Æ1% (P < 0Æ0001) and fat mass by 4Æ4% (P < 0Æ0001), while group B showed a percentage of increase in fatmass by 1Æ5% at T1. In group A, a trend of increase at T1 for circulating levels of CPC and EPC was observed,reaching the statistical significance for all the three types of EPC. On the contrary, group B showed no significantincrease in CPC and EPC. Furthermore, a significant correlation between decrease in fat mass and increase inCD133+ ⁄ KDR+ EPC was reported in group A (r = 0Æ50; P = 0Æ04).
Conclusion Three months of physical activity significantly improved anthropometric measurements. A benefi-cial effect of increased number of EPC in compliant individuals, in relation to weight loss, was observed.
Keywords Endothelial progenitor cells, obesity, physical activity, weight loss.
Eur J Clin Invest 2012
Introduction
Overweight, through an increased oxidative stress and
inflammation, has been demonstrated to determine a sub-
clinical atherosclerosis, representing a susceptibility factor
for the development of cardiovascular events [1]. To date,
the pathophysiological mechanisms linking obesity and
atherosclerosis are not well defined; recently, a role for
endothelial (EPC) and circulating progenitor cells (CPC)
has been reported. [2,3]. In 2008, Muller-Ehmsen et al. [4]
demonstrated for the first time that CPC are inversely
related to body weight, body mass index (BMI) and waist
circumference in a population of obese subjects, with a
higher prevalence of cardiovascular risk factors, such as
diabetes, hypercholesterolaemia and physical inactivity.
Moreover, it has also been reported that reduction of CPC
and, in particular, of the CD34+ subpopulation can be
reversible along with the reduction of the caloric intake
through a dietary intervention [4].
Recently, a study conducted in a limited sample of obese sub-
jects examined the effect of a dietary intervention on early out-
growth EPC number and functional properties, by
demonstrating that, after a 6 months of intervention, a signifi-
cant weight reduction was able to restore the functional capac-
ity of EPC [5].
Actually, physical exercise is an important part of obesity
treatment concepts, by inducing and supporting fat mobiliza-
tion from adipose tissue [6]. Over the past few years, research
about the effect of physical activity on stem cells’ mobilization
produced some interesting findings. In fact, physical exercise
has been reported to augment the number of both CPC and
EPC in coronary artery disease patients as well as in athletes,
European Journal of Clinical Investigation 1
DOI: 10.1111/j.1365-2362.2012.02670.x
ORIGINAL ARTICLE
showing a positive effect on stem cells’ mobilization [7–10]. To
date, however, the effect of weight loss obtained through a
personalized physical activity programme able to induce
adipose tissue lipolysis, and not limited a restrictive diet, on
CPC and EPC number has not been investigated.
We aimed this study to assess, in a population of overweight
and obese subjects, the effect of a personalized physical activity
programme on CPC and EPC number and on weight reduction.
Materials and methods
Study populationEighty [40 M, 40 F; median age, 44Æ5 years (range, 24–69)] over-
weight and obese subjects referring to the Agency of Nutrition
of the University Hospital of Careggi, Florence for a weight loss
programme were recruited through questionnaires, advertise-
ments in the local newspaper, primary care, and the home ser-
vice administration organized by the local authorities.
Eligibility criteria were BMI > 25 kg ⁄ m2, with the absence of
any other established cardiovascular risk factors (i.e. hyperten-
sion, diabetes, dyslipidaemia, family history of cardiovascular
diseases), 18–70 years of age and stable weight (modification
not > 2 kg during the last 12 months). Exclusion criteria were
presence of diagnosed type I and II diabetes, blood hyperten-
sion, dyslipidaemia, inability to undertake a maximal exercise
test to achieve maximum aerobic capacity, people with medica-
tions known to affect heart rate or body composition, recent
cardiac problems requiring hospital care, recent hip fracture or
surgery during the last 6 months, present cancer treatment,
stroke within the last 2 years, pregnancy or lactation. The local
Ethic Committee approved the study, and all participants gave
written informed consent. The study conforms to the STROBE
statement along with reference to STROBE statement and to the
broader EQUATOR guidelines [11].
Study designAt the beginning and at the end of the study, full medical evalu-
ation consisting of physical examination, blood tests, anthropo-
metric measurements, resting electrocardiogram, resting
energy expenditure, maximal exercise test and maximal oxygen
uptake was obtained from all the participants. BMI was calcu-
lated as weight (kg) ⁄ height (m2). Bioelectrical impedance for
the measurement of body composition was performed with the
use of a soft tissue analysis ⁄ bioelectrical impedance analysis
device (Tanita B420MA; SensorMedics Italia Srl, Milan, Italy).
Cardiorespiratory fitness testAll participants underwent at baseline and at the end of the
intervention a graded bicycle test with spirometry until exhaus-
tion. Subjects started exercising at a load of 25 Watts, with an
incremental load of 5 Watts every 2 min. Twelve-lead ECG and
heart rate were recorded continuously, and automatic cuff
blood pressure was measured every 2 min and at peak exercise.
The exercise test was started when oxygen consumption (VO2)
at rest showed stable levels. The recovery period lasted 4 min
or until the heart rate and blood pressure normalized, which-
ever was longer. Subjects were encouraged to exercise until
exhaustion, and all of them performed a maximal test according
to the identification of individual anaerobic threshold (IAT).
The IAT indicates the exercise intensity corresponding to the
maximal lactate steady state. This corresponds to the individual
level of physical activity for training.
Exercise respiratory variables were continuously recorded
breath-by-breath by portable lightweight equipment, which did
not interfere with movements (K4b; Cosmed, Rome, Italy). Full
calibration of the system was obtained before each test. During
the test, subjects were wearing a neoprene mask holding a sup-
port for the gas sampling line and pneumotachograph. Five
commonly used markers of maximal and threshold cardiorespi-
ratory capacity were provided in the main test: resting heart
rate, maximal oxygen uptake (VO2max), IAT and maximal heart
rate. IAT was estimated by spirometer algorithms.
Physical activity programmeParticipants were instructed to attend a programme of physical
activity, which consisted of 45-min session of aerobic exercise
(walking briskly or moderate running) to be performed three
times per week, with a strict control of the heart rate in order
not to exceed their individual IAT. All subjects were encour-
aged to purchase a heart rate transmitter belt, together with a
receiver watch. A tailored physical activity programme was
determined for each participant, with indications on heart rate
to be followed for the entire session of physical activity.
Furthermore, to avoid confounding factors for weight
modifications, the subjects were recommended not to modify
the quantity and quality of their usual diet. At the end of the
3-month intervention programme with physical activity, the
study population was divided into compliant individuals
(group A) and noncompliant individuals (group B). Compliant
individuals were identified as subjects who either self-reported
an adherence to the whole training programme or showed an
increase in VO2max > 10% (median level of increase among the
subjects who reported to have adhered to the programme) after
3 months of intervention.
Laboratory parametersBlood sample was taken in the morning after an overnight fast-
ing and was collected from the antecubital vein into evacuated
plastic tubes (BD Vacutainer; Becton Dickinson, Plymouth, UK)
containing ethylenediaminotetracetate 0Æ17 M for CPC and EPC
evaluation. Whole venous blood was also collected in tubes
without anticoagulant. Haematological parameters, lipid
2 ª 2012 The Authors. European Journal of Clinical Investigation ª 2012 Stichting European Society for Clinical Investigation Journal Foundation
F. CESARI ET AL. www.ejci-online.com
profile and blood glucose were analysed using conventional
procedures. CPC and EPC number was assessed contemporar-
ily using flow cytometry as previously described [12]. CPC
were defined as cells forming a cluster with low side scatter
and low-to-intermediate CD45 staining and positive for CD34,
CD133 and CD34 ⁄ CD133. EPC were identified through the
expression of CD34, KDR and CD133 and were considered as
CD34+ ⁄ KDR+, CD133+ ⁄ KDR+ and CD34+ ⁄ CD133+ ⁄ KDR+.
Statistical analysisStatistical analysis was performed by the SPSS (Statistical
Package for Social Sciences Inc., Chicago, IL, USA) software for
Windows (Version 14.0). Results are expressed either as
mean ± standard deviation (SD) or as median and range, as
appropriate. Sample size was calculated as a number of subjects
able to detect a difference after the physical activity programme,
in line with the modest effect of physical activity observed in
previous studies (approximately 7% of the initial weight). The
analyses were simplified by calculating the absolute change for
each variable tested (mean value at baseline subtracted from the
mean value after intervention for each subject) with indepen-
dent t sample tests. Data that were not normally distributed
were logarithmically transformed or analysed by the nonpara-
metric Wilcoxon signed-ranked test. Data were analysed using
paired t tests for significant differences between changes
observed during test and control intervention periods. A gen-
eral linear model for repeated measurements (interaction term:
before and after intervention) adjusted for age, gender and
change of VO2max was performed to test whether weight change
followed by physical activity intervention programme was able
to determine significant changes of CPC and EPC. A P-value
< 0Æ05 was considered to indicate statistical significance.
Results
All the enrolled subjects completed the study and entered into
the final analysis. Mean BMI of the study population was
31Æ5 ± 5Æ6 kg ⁄ m2.
Demographic and clinical characteristics of the two groups at
baseline were reported in Table 1. No significant differences
between the group A and group B were detected. In Table 2,
changes after the intervention programme for anthropometric
and biochemical variables in both groups are reported. At the
end of the programme, group A subjects showed a significant
decrease in anthropometric measurements such as BMI
()3Æ1%), total weight ()3Æ1%) and fat mass ()4%), with a signifi-
cant improvement of free-fat mass (+0Æ9%) and cardiopulmo-
nary capacity, as detected by VO2max (+10Æ8%). No significant
changes were reported for biochemical parameters. On the
contrary, group B subjects showed no significant improvement
in anthropometric measurements with an increase in fat mass
(+1Æ5%) and a decrease in cardiopulmonary capacity, as seen by
VO2max ()6Æ3%).
In a subgroup of subjects (n = 40; 22 M, 18 F with a median
age of 48 years), similar for characteristics with the whole study
population, we analysed CPC and EPC at baseline and at the
end of the programme to test the possible influence of such per-
sonalized intervention programme on CPC and EPC. Of these,
21 were ascribed to group A and 19 to group B. At baseline, no
significant differences for all the population of CPC and EPC
between group A and group B were observed (data not
reported). To test the effect of the personalized programme
with physical activity on the number of CPC and EPC, we per-
formed a general linear model for repeated measurements after
adjustment for age, gender and changes of VO2max (Table 3).
Three months of personalized programme with physical activ-
ity were able to determine a significant increase in all the three
groups of EPC (CD34+ ⁄ KDR+: +33Æ3%; CD133 ⁄ KDR+: +35%;
CD34+ ⁄ CD133+ ⁄ KDR+: +35Æ7%) in group A, while no signifi-
cant changes in group B were detected. Moreover, to investi-
gate the possible association between changes of
anthropometric measurements at the end of the programme
and changes of CPC and EPC, we performed correlation analy-
ses, which revealed a significant correlation between decrease
in fat mass and increase in CD133+ ⁄ KDR+ EPC (R = 0Æ50,
P = 0Æ04) in group A, whereas no significant correlations in
group B were reported.
Discussion
In this intervention study, we demonstrated the beneficial
effects of a personalized physical activity programme on EPC
number as well as on weight reduction and body composition
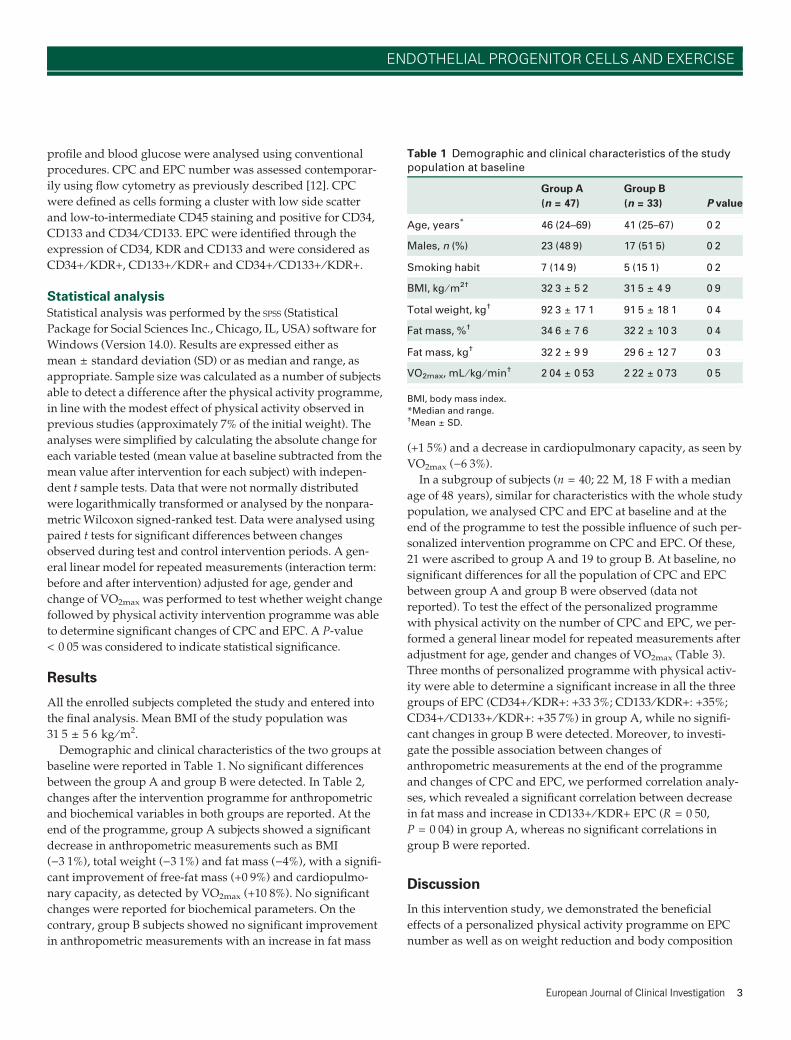
Table 1 Demographic and clinical characteristics of the studypopulation at baseline
Group A
(n = 47)
Group B
(n = 33) P value
Age, years* 46 (24–69) 41 (25–67) 0Æ2
Males, n (%) 23 (48Æ9) 17 (51Æ5) 0Æ2
Smoking habit 7 (14Æ9) 5 (15Æ1) 0Æ2
BMI, kg ⁄ m2† 32Æ3 ± 5Æ2 31Æ5 ± 4Æ9 0Æ9
Total weight, kg† 92Æ3 ± 17Æ1 91Æ5 ± 18Æ1 0Æ4
Fat mass, %† 34Æ6 ± 7Æ6 32Æ2 ± 10Æ3 0Æ4
Fat mass, kg† 32Æ2 ± 9Æ9 29Æ6 ± 12Æ7 0Æ3
VO2max, mL ⁄ kg ⁄ min† 2Æ04 ± 0Æ53 2Æ22 ± 0Æ73 0Æ5
BMI, body mass index.
*Median and range.†Mean ± SD.
European Journal of Clinical Investigation 3
ENDOTHELIAL PROGENITOR CELLS AND EXERCISE
of obese and overweight subjects. Indeed, a 3-month interven-
tion programme with physical activity was able to decrease
total weight and percentage of fat mass, by augmenting the
number of circulating EPC. Moreover, a significant correlation
between the decrease of percentage of fat mass and the increase
of EPC, suggesting a possible link between adipose tissue
reduction and EPC mobilization, has been also reported.
Over the last few years, a beneficial role for bone-marrow-
derived EPC and CPC in the vascular homeostasis has emerged
[13]. EPC have been demonstrated to be key player in restora-
tion of injured endothelium, either by integrating in the endo-
thelial cell layer or by secreting angiogenic growth factors [13].
Currently, several factors have been reported to influence the
number of circulating EPC: decreased levels have been found to
be associated with increasing age, hypertension, smoking habit,
hypercholesterolaemia and BMI, while increased levels have
been reported to be associated with the use of some pharmaco-
logical treatments such as statins, erythropoietin, peroxisome
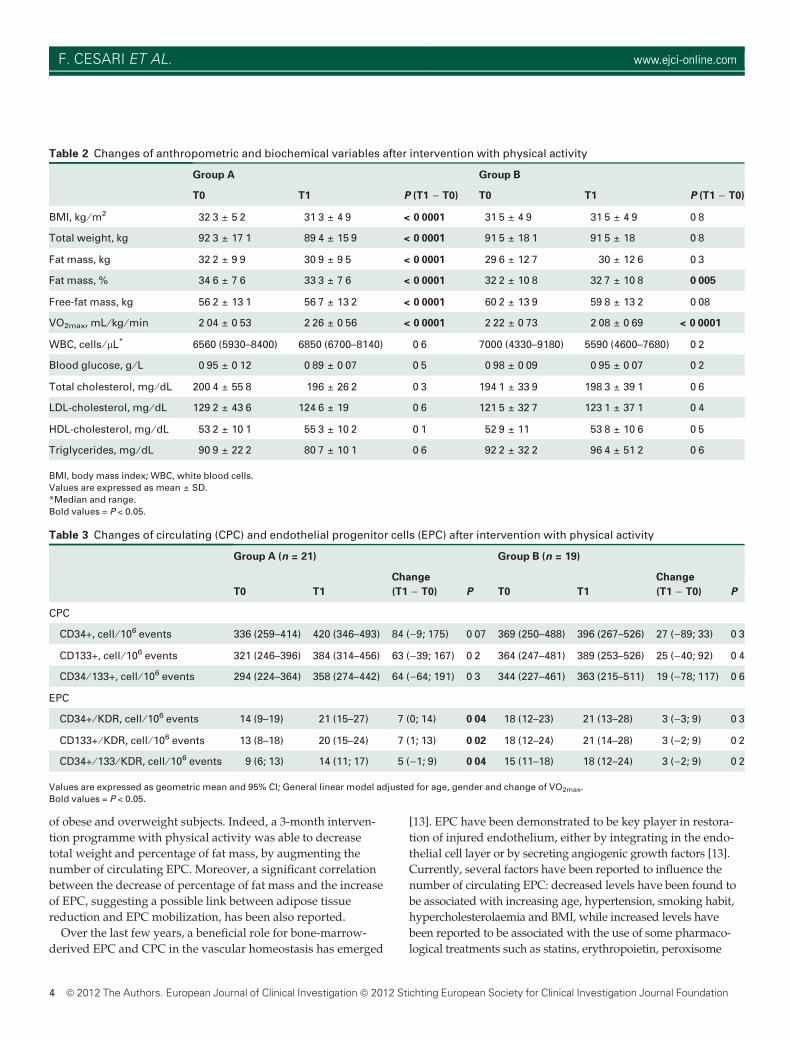
Table 2 Changes of anthropometric and biochemical variables after intervention with physical activity
Group A Group B
T0 T1 P (T1 ) T0) T0 T1 P (T1 ) T0)
BMI, kg ⁄ m2 32Æ3 ± 5Æ2 31Æ3 ± 4Æ9 < 0Æ0001 31Æ5 ± 4Æ9 31Æ5 ± 4Æ9 0Æ8
Total weight, kg 92Æ3 ± 17Æ1 89Æ4 ± 15Æ9 < 0Æ0001 91Æ5 ± 18Æ1 91Æ5 ± 18 0Æ8
Fat mass, kg 32Æ2 ± 9Æ9 30Æ9 ± 9Æ5 < 0Æ0001 29Æ6 ± 12Æ7 30 ± 12Æ6 0Æ3
Fat mass, % 34Æ6 ± 7Æ6 33Æ3 ± 7Æ6 < 0Æ0001 32Æ2 ± 10Æ8 32Æ7 ± 10Æ8 0Æ005
Free-fat mass, kg 56Æ2 ± 13Æ1 56Æ7 ± 13Æ2 < 0Æ0001 60Æ2 ± 13Æ9 59Æ8 ± 13Æ2 0Æ08
VO2max, mL ⁄ kg ⁄ min 2Æ04 ± 0Æ53 2Æ26 ± 0Æ56 < 0Æ0001 2Æ22 ± 0Æ73 2Æ08 ± 0Æ69 < 0Æ0001
WBC, cells ⁄ lL* 6560 (5930–8400) 6850 (6700–8140) 0Æ6 7000 (4330–9180) 5590 (4600–7680) 0Æ2
Blood glucose, g ⁄ L 0Æ95 ± 0Æ12 0Æ89 ± 0Æ07 0Æ5 0Æ98 ± 0Æ09 0Æ95 ± 0Æ07 0Æ2
Total cholesterol, mg ⁄ dL 200Æ4 ± 55Æ8 196 ± 26Æ2 0Æ3 194Æ1 ± 33Æ9 198Æ3 ± 39Æ1 0Æ6
LDL-cholesterol, mg ⁄ dL 129Æ2 ± 43Æ6 124Æ6 ± 19 0Æ6 121Æ5 ± 32Æ7 123Æ1 ± 37Æ1 0Æ4
HDL-cholesterol, mg ⁄ dL 53Æ2 ± 10Æ1 55Æ3 ± 10Æ2 0Æ1 52Æ9 ± 11 53Æ8 ± 10Æ6 0Æ5
Triglycerides, mg ⁄ dL 90Æ9 ± 22Æ2 80Æ7 ± 10Æ1 0Æ6 92Æ2 ± 32Æ2 96Æ4 ± 51Æ2 0Æ6
BMI, body mass index; WBC, white blood cells.
Values are expressed as mean ± SD.
*Median and range.
Bold values = P < 0.05.
Table 3 Changes of circulating (CPC) and endothelial progenitor cells (EPC) after intervention with physical activity
Group A (n = 21) Group B (n = 19)
T0 T1
Change
(T1 ) T0) P T0 T1
Change
(T1 ) T0) P
CPC
CD34+, cell ⁄ 106 events 336 (259–414) 420 (346–493) 84 ()9; 175) 0Æ07 369 (250–488) 396 (267–526) 27 ()89; 33) 0Æ3
CD133+, cell ⁄ 106 events 321 (246–396) 384 (314–456) 63 ()39; 167) 0Æ2 364 (247–481) 389 (253–526) 25 ()40; 92) 0Æ4
CD34 ⁄ 133+, cell ⁄ 106 events 294 (224–364) 358 (274–442) 64 ()64; 191) 0Æ3 344 (227–461) 363 (215–511) 19 ()78; 117) 0Æ6
EPC
CD34+ ⁄ KDR, cell ⁄ 106 events 14 (9–19) 21 (15–27) 7 (0; 14) 0Æ04 18 (12–23) 21 (13–28) 3 ()3; 9) 0Æ3
CD133+ ⁄ KDR, cell ⁄ 106 events 13 (8–18) 20 (15–24) 7 (1; 13) 0Æ02 18 (12–24) 21 (14–28) 3 ()2; 9) 0Æ2
CD34+ ⁄ 133 ⁄ KDR, cell ⁄ 106 events 9 (6; 13) 14 (11; 17) 5 ()1; 9) 0Æ04 15 (11–18) 18 (12–24) 3 ()2; 9) 0Æ2
Values are expressed as geometric mean and 95% CI; General linear model adjusted for age, gender and change of VO2max.
Bold values = P < 0.05.
4 ª 2012 The Authors. European Journal of Clinical Investigation ª 2012 Stichting European Society for Clinical Investigation Journal Foundation
F. CESARI ET AL. www.ejci-online.com

proliferator-activated receptor gamma-agonists and angiotensin
II receptor antagonists [4,14,15].
In our study, we demonstrate, for the first time, that a ‘lipo-
lytic’ physical exercise, that is below the anaerobic individual
threshold, is able to determine not only a significant weight
reduction, but also an increase of EPC as well as a modification
of the composition of the body mass, with a significant decrease
in fat mass and increase in free-fat mass.
Owing to the nature of the study, we are not able to distin-
guish which of the two main components – physical exercise
and weight change – is the main contributor of the increased
levels of EPC. To determine which of the two components,
physical exercise by itself or weight reduction, determined by
physical exercise, is mostly related to the increase of EPC, an ad
hoc study should be performed.
Actually, several studies reported the positive influence of
physical exercise on EPC and CPC levels and function in both
patients with vascular disease and healthy subjects, by sug-
gesting this effect on progenitor cells to be one of the most
important beneficial outcomes of physical exercise, probably
mediated by a shear stress-induced up-regulation of endothe-
lial nitric oxide synthase [7–9,14]. Moreover, two recent stud-
ies conducted among obese subjects reported that a period of
dietary caloric restriction with a subsequent weight loss is able
to increase the number of CPC and determine a beneficial effect
on the functional properties of early outgrowth EPC [4,5].
In our sample of subjects, we showed a significant and
inverse relationship between fat mass’ loss and EPC. The link
between adipose tissue and EPC is, to date, only speculative. In
2007, Matsuo et al. [16] demonstrated in coronary artery disease
patients plasma levels of adiponectin significantly associated
with an increase of EPC number. In addition, the effects of
adiponectin on EPC have been recently investigated in animal
models of hindlimb ischaemia, demonstrating that it regulates
the level of circulating EPC in response to ischaemic injury,
possibly stimulating, in cultured progenitor cell populations,
the expression of endothelial cell marker proteins, the incorpo-
ration in an endothelial network, as well as the promotion of
EPC differentiation and function [17].
However, in the present study, we chose not to use dietary
approaches for weight reduction in overweight and obese sub-
jects, as the primary aim of the study was to investigate the
effects of physical activity ‘per se’ on moderate reduction of
weight and progenitor cells and not to test the effect of a spe-
cific dietary plan.
Therefore, we could hypothesize that the ‘prescription’ of the
physical activity able to achieve a significant weight loss, and in
turn a significant increase of EPC, can vary, so requiring a per-
sonalized approach. In fact, only among subjects who resulted
to follow the personalized prescription, despite starting from
lower EPC levels, the compliance to the programme was able to
exceed the unfavourable effect of older age and greater BMI.
Moreover, in this group of patients, a decrease in fat mass and
an increase in EPC have been evidenced, suggesting perhaps an
effect of a moderate reduction of weight and adipose tissue on
EPC mobilization, rather than of physical exercise.
Some limitations are present in this study. First of all, the lim-
ited number of subjects investigated as well as the limited dura-
tion of follow-up allows us only to hypothesize the possible
relation between physical exercise and increase of CPC and
EPC, and secondly, the use of an arbitrary method to identify
subjects ‘compliant individuals’. The compliance to such inter-
vention studies is not easy to measure and establish. We used
the combination of a self-reported statement of adherence and,
as an indirect method to measure the adherence, the increased
level of VO2max at the end of the training programme. However,
we are fully aware that this is not a specific method to establish
the real compliance of the subjects and that this could have led
to an underestimation or overestimation of number of subjects
in the two groups. Nonetheless, strengths of the present study
are the type of intervention, as well as the subjects studied.
Indeed, the intervention was based only on physical activity,
and not on dietary modification, it was personalized according
to subject’s variables, and the study population represented a
typical ‘primary prevention’ group where no other risk factor
or comorbidity was present.
In conclusion, the present intervention study confirms the
positive effect of physical activity on weight reduction and vas-
cular health, as shown by a significant increase of EPC. Further
studies investigating type, duration and intensity of physical
activity to be conducted for obtaining a persistent increase in
such progenitor cells need to be conducted.
Address
Department of Medical and Surgical Critical Care, Thrombosis
Centre, University of Florence, Largo Brambilla, 350134
Florence, Italy (F. Cesari, F. Sofi, A. M. Gori, R. Abbate,
G. F. Gensini); Agency of Nutrition, Azienda Ospedaliero-
Universitaria Careggi, Largo Brambilla, 350134 Florence, Italy
(F. Sofi, I. Corsani, A. Capalbo, A. Casini); Don Carlo Gnocchi
Foundation, Onlus IRCCS, Impruneta, Largo Brambilla, 350134
Florence, Italy (F. Sofi, A. M. Gori, G. F. Gensini); Central
Laboratory, Azienda Ospedaliero-Universitaria Careggi,
Largo Brambilla, 350134 Florence, Italy (R. Caporale).
Correspondence to: Francesco Sofi, MD, Department of
Medical and Surgical Critical Care, Thrombosis Centre,
Viale Morgagni, 85, 50134 Florence, Italy.
Tel.: +39-055-7949420; fax: +39-055-7949418;
e-mail: [email protected]
Received 2 September 2011; accepted 3 March 2012
European Journal of Clinical Investigation 5
ENDOTHELIAL PROGENITOR CELLS AND EXERCISE

References1 Rossi R, Iaccarino D, Nuzzo A, Chiurlia E, Bacco L, Venturelli A
et al. Influence of body mass index on extent of coronary atheroscle-rosis and cardiac events in a cohort of patients at risk of coronaryartery disease. Nutr Metab Cardiovasc Dis 2011;21:86–93.
2 Tobler K, Freudenthaler A, Baumgartner-Parzer SM, Wolzt M, Lud-vik B, Nansalmaa E et al. Reduction of both number and prolifera-tive activity of human endothelial progenitor cells in obesity. Int JObes 2010;34:687–700.
3 MacEneaney OJ, Kushner EJ, Van Guilder GP, Greiner JJ, StaufferBL, DeSouza CA. Endothelial progenitor cell number and colony-forming capacity in overweight and obese adults. Int J Obes2009;33:219–25.
4 Muller-Ehmsen J, Braun D, Schneider T, Pfister R, Worm N, Wielc-kens K et al. Decreased number of circulating progenitor cells inobesity: beneficial effects of weight reduction. Eur Heart J2008;29:1560–8.
5 Heida NM, Muller JP, Cheng IF, Leifheit-Nestler M, Faustin V, Rigg-ert J et al. Effects of obesity and weight loss on the functional proper-ties of early outgrowth endothelial progenitor cells. J Am Coll Cardiol2010;55:357–67.
6 Byrne NM, Meerkin JD, Laukkanen R, Ross R, Fogelholm M, HillsAP. Weight loss strategies for obese adults: personalized weightmanagement program vs. standard care. Obesity 2006;14:1777–88.
7 Laufs U, Werner N, Link A, Endres M, Wassmann S, Jurgens K et al.Physical training increases endothelial progenitor cells, inhibits neo-intima formation, and enhances angiogenesis. Circulation2004;109:220–6.
8 Steiner S, Niessner A, Ziegler S, Richter B, Seidinger D, Pleiner Jet al. Endurance training increases the number of endothelial pro-genitor cells in patients with cardiovascular risk and coronary arterydisease. Atherosclerosis 2005;181:305–10.
9 Thijssen DHJ, Vos JB, Verseyden C, van Zonneveld AJ, Smits P,Sweep FC et al. Haematopoietic stem cells and endothelial progeni-tor cells in healthy men: effect of aging and training. Aging Cell2006;5:495–503.
10 Adams V, Lenk K, Linke A, Lenz D, Erbs S, Sandri M et al. Increaseof circulating endothelial progenitor cells in patients with coronaryartery disease after exercise-induced ischemia. Arterioscler ThrombVasc Biol 2004;24:684–90.
11 Simera I, Moher D, Hoey J, Schulz KF, Altman DG. A catalogue ofreporting guidelines for health research. Eur J Clin Invest 2010;40:35–53.
12 Cesari F, Nencini P, Nesi M, Caporale R, Giusti B, Abbate R et al.Bone marrow-derived progenitor cells in the early phase of ischemicstroke: relation with stroke severity and discharge outcome. J CerebBlood Flow Metab 2009;29:1983–90.
13 Hill JM, Zalos G, Halcox JP, Schenke WH, Waclawiw MA, QuyyumiAA et al. Circulating endothelial progenitor cells, vascular function,and cardiovascular risk. N Engl J Med 2003;348:593–600.
14 Van Craenenbroeck E, Conraads VM. Endothelial progenitor cells invascular health: focus on lifestyle. Microvascular Res 2010;79:184–92.
15 Xiao Q, Kiechl S, Patel S, Oberhollenzer F, Weger S, Mayr A et al.Endothelial progenitor cells, cardiovascular risk factors, cytokinelevels and atherosclerosis – results from a large population-basedstudy. PLoS ONE 2007;2:e975.
16 Matsuo Y, Imanishi T, Kuroi A, Kitabata H, Kubo T, Hayashi Y et al.Effects of plasma adiponectin levels on the number and function ofendothelial progenitor cells in patients with coronary artery disease.Circ J 2007;71:1376–82.
17 Shibata R, Skurk C, Ouchi N, Galasso G, Kondo K, Ohashi T et al.Adiponectin promotes endothelial progenitor cell number and func-tion. FEBS Lett 2008;582:1607–12.
6 ª 2012 The Authors. European Journal of Clinical Investigation ª 2012 Stichting European Society for Clinical Investigation Journal Foundation
F. CESARI ET AL. www.ejci-online.com






![Effect of vitamin D on endothelial progenitor cells function · vitamin D on EPCs function. Aim ... immune cells and endothelial cells [16]). Additional studies suggest a favorable](https://img.pdfslide.net/doc/110x75/60c10a1fa60e3e04a118fdb0/effect-of-vitamin-d-on-endothelial-progenitor-cells-function-vitamin-d-on-epcs-function.jpg)






















