Embed Size (px)
Citation preview

Om
So
Rs(rocs
Carw
Dswectgds
tps(gcsi
th
DM
3
Physical and Mental Health in Mothers of Children with Down Syndrome
JENNY BOURKE, MPH, BERNADETTE RICCIARDO, MBBS, AMI BEBBINGTON, BSC (HONS), KARINA AIBERTI, MPH, PETER JACOBY, MSC,PAULA DYKE, MPH, MICHAEL MSALL, MD, CAROL BOWER, PHD, AND HELEN LEONARD, MBCHB
bjective To identify the relationship between characteristics of the child with Down syndrome and the health of theirother.
tudy design Families with a child/young adult with Down syndrome (<25 years) provided information related to the healthf the child, functioning and behavior, and the health and well-being of the mother (n � 250).
esults The mean physical health score of mothers was 50.2 (SD � 9.6). Factors associated with lower mean physical healthcores were as follows: child having a current heart problem (P � .036), a higher body mass index (P � .006), and higherpoorer) scores on the Developmental Behavior Checklist. Better physical health scores were seen in mothers whose childrenequired no help/supervision in learning new skills (P � .008) and domestic tasks (P � .014). The mean mental health scoref mothers was 45.2 (SD � 10.6), significantly lower than the norm of 50 (P < .0001). Associated child factors includedurrent ear problems (P � .079), muscle/bone problems (P � .004), >4 episodes of illness in past year (P � .016), and highercores on the DBC (P < .0001).
onclusions The most important predictors of maternal health were children’s behavioral difficulties, everyday functioningnd current health status. Mothers of children with Down syndrome appear to experience poorer mental health and mayequire greater support and services to improve behavior management skills for their child and their own psychologicalell-being. (J Pediatr 2008;153:320-6)
own syndrome is the most common genetic cause of intellectual disability, occurring in �1/1000 live births in WesternAustralia.1 Therefore mothers of children with Down syndrome represent asubstantial proportion of mothers of children with intellectual disability. In one
tudy this group of mothers was reported as experiencing better psychological well-beinghen compared with mothers of children with autism or fragile X syndrome.2 Although
xperience of stress for mothers of children with Down syndrome may be lower in earlyhildhood when compared with mothers of children with other intellectual disabilities,heir stress levels have been shown to increase at a significantly higher rate as the childrows up.3 It is possible that as the child enters late childhood and middle adolescence,ifficulty in obtaining services and uncertainty about the child’s future may promotetress.3
Stress can be defined as the balance between external environmental demands andhe perceived internal ability to respond and may occur when the demands prevent theursuit of other life objectives.4 It is important to discern factors that modify caregivertress. Several authors have proposed potential buffers, including: child characteristicse.g., age, sex, behavior) 3-7; disability characteristics (e.g., burden of disease)4,7-9; care-iver characteristics (eg age, marital status and satisfaction, coping style)8,10,11; familyharacteristics (eg functioning, resources)4,5,9,11-13; sociological characteristics (eg socialupport, employment, socio-economic status)8,11,14; and system characteristics (eg, fam-ly-centered care).6
The present population-based study examines multidimensional characteristics ofhe child with Down syndrome and how these characteristics are associated with maternalealth and psychological well-being, as measured by the SF12.15 Specifically, we wanted
BC Developmental Behavior Checklist PCS Physical Component Score
See editorial, p 304
From the Telethon Institute for ChildHealth Research, Centre for Child HealthResearch, University of Western Australia(J.B., A.B., K.A., P.J., P.D., C.B., H.L.), and thePrincess Margaret Hospital for Children(B.R.), Perth, Western Australia, the Pritz-ker School of Medicine, Kennedy MentalRetardation Center, University of Chicago(M.M.) and the Department of Develop-mental and Behavioural Pediatrics, ComerChildren’s and La Rabida Children’s Hospi-tals (M.M.), Chicago, IL.
Supported by the National Institutes ofHealth (5 R01 HD43100-04) and NHMRCprogram grant 353514, and CB byNHMRC Fellowship 353628.
Submitted for publication Sep 4, 2007; lastrevision received Jan 15, 2008; acceptedFeb 22, 2008.
Reprint requests: Helen Leonard, MBChB,Telethon Institute for Child Health Re-search, PO Box 855, West Perth 6872,Western Australia.
0022-3476/$ - see front matter
Copyright © 2008 Mosby Inc. All rightsreserved.
CS Mental Component Score
20
10.1016/j.jpeds.2008.02.047
tlt
twpstS
WlgsaSqihtmaspwd
ttpTSctmwp
CadUsbpp
sttmge
bsCtiibcqthit
tomogieta.fiaw1
mtmmcat(it�f
1fsss
pcera
P
o examine how health status, communication, behavior, andevel of functioning of the child with Down syndrome relateo maternal health.
METHODSIn 2004 all individuals with Down syndrome aged be-
ween 0 and 25 years currently living in Western Australiaere identified from the IDEA (Intellectual Disability Ex-loring Answers) database. The IDEA database uses multipleources.16 Ethical approval for the study has been provided byhe Ethics Committee of the Women’s and Children’s Healthervices in Western Australia.
With the approval of the Ethics Committee of theomen’s and Children’s Health Services in Western Austra-
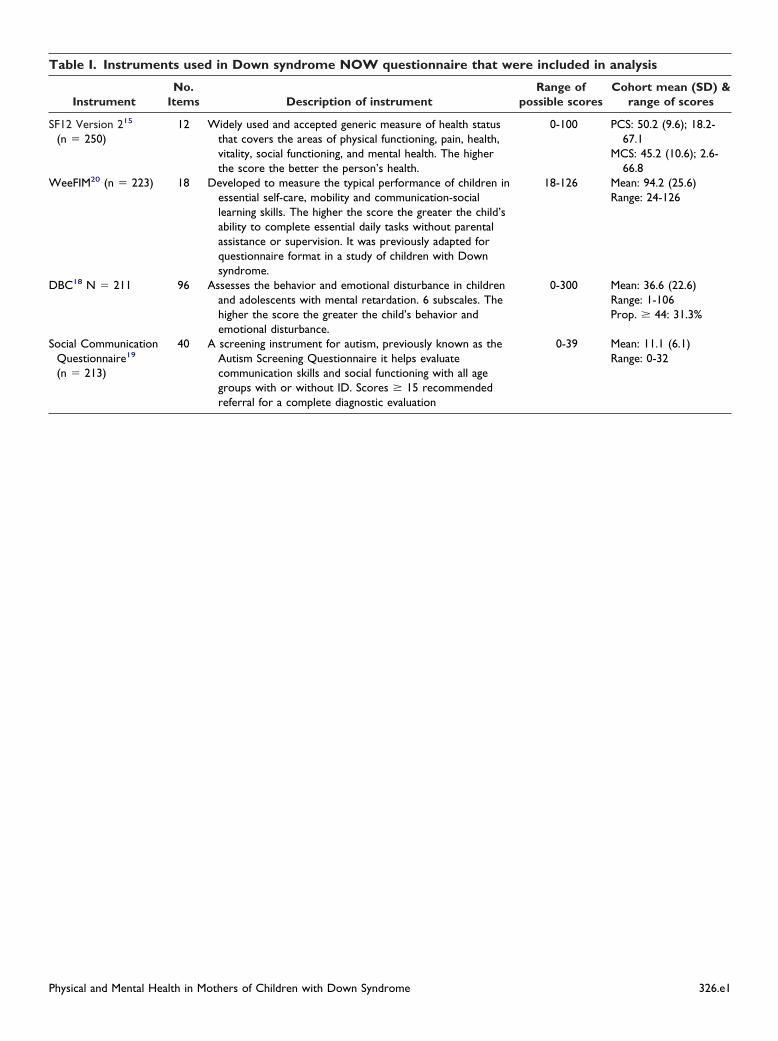
ia and the backing of the Down syndrome parent supportroup, families of 500 children/young adults with Downyndrome registered with Disability Services Commission andble to be contacted were invited to participate in the Downyndrome NOW (Needs, Opinions, Wishes) study. Theuestionnaire consisted of 2 parts. Part 1 pertained to thendividual with Down syndrome and included information onealth, functioning and service needs, whereas Part 2 per-ained to the health and well-being of their family. Theeasures used in this analysis are described in Table I (avail-
ble at www.jpeds.com). Pilot testing with 13 families en-ured that the questionnaire was relevant and captured im-ortant resource, health, functional and family characteristicshile being sensitive to the complexity of ongoing care-givingemands.
Data collection was completed during 2005, with aotal response fraction of 73% (n � 363/500). Three quar-ers of families chose to complete the questionnaire onaper, 12.6% online, and 12.4% by telephone interview.here were 18 questionnaires with missing data from theF-12 measure, 25 questionnaires were completed by thehild’s father, and 70 questionnaires (short version) con-ained responses only to Part 1. To provide a more ho-ogenous cohort for analysis, these 113 questionnairesere excluded, leaving a total of 250 questionnaires com-leted by the child’s mother.
The Physical Component Score (PCS) and Mentalomponent Score (MCS) measures were calculated using the
lgorithm provided in the scoring manual.15 The scores areerived through norm-based scoring methods using the 2002S population so that the general population has a mean
core of 50 and SD of 10 for both scales. All scores above orelow 50 can be interpreted as above or below the generalopulation norm. The SF12 has been validated as an appro-riate measure in the Australian population.17
Univariate linear regression analyses were conductedeparately with the SF-12 version-2 PCS and the MCS ashe outcome variables of interest. We specifically selectedhe variables from the child’s health status, behavior, com-unication and function that we thought would have the
reatest effect on maternal health. These included the
xistence of specific health conditions (such as heart or ihysical and Mental Health in Mothers of Children with Down Syndrom
owel), the number of health conditions, number of epi-odes of illness over the last year, Developmental Behaviorhecklist (DBC)18 scores, Social Communication Ques-
ionnaire19 score, level of communication and understand-ng, level of independence in day to day activities as scoredn the WeeFIM (modified for questionnaire use)20 and theody mass index. We considered the following as possibleonfounders: child’s age and mother’s age at the time ofuestionnaire completion, number of siblings, metropoli-an/rural living, sex of the child and family income. Theseave been taken into account in each of the final multivar-
ate models. The statistical package STATA 9 was used forhis analysis.21
RESULTSComparison of those included and not included in
his analysis showed no significant difference in age groupf the child, sex, child’s place of birth, number of siblings,aternal education, mother’s work status, family income,
r having a partner. There were differences between theroups in use of private health insurance (62% of thosencluded had health insurance compared with 50% of thosexcluded, P � .03), experiencing financial stress (46% ofhose included indicated “they could save a bit every nownd then” compared with only 36% of those excluded, P �07), birth order of child (30% of children included wererst-born compared with 45% of those excluded, P � .02)nd metropolitan or rural residence (29% of those includedere from rural Western Australia compared with only5% of those excluded, P � .04).
Most (70.8%) of the participating families lived in theetropolitan area. Of the 250 mothers completing the ques-
ionnaire, 237 were biological mothers, 11 were adoptiveothers, 1 was a foster mother, and 1 was a stepmother. Theean age of the mothers at the time the questionnaire was
ompleted was 44.4 years, and most (88%) were married or inde facto relationship. Just more than one third (38.6%) of
he mothers had obtained university qualifications, and half50.2%) were in full- or part-time work. The combined grossncome of families in 2004 was reported as �$26,000 (Aus-ralian dollars) by 26.2%, $26,000 to $51,999 by 30%, and
$51,999 by 43.8%. However, nearly half (46.5%) of theamilies described a high level of financial stress.
The mean age of the child with Down syndrome was1.9 years, and there were slightly more males (54.4%) thanemales (45.6%). Only 7.2% of the children with Downyndrome had no siblings, with most (58.4%) having 2 or 3iblings. In those families with siblings the child with Downyndrome was the eldest in 22.4%.
Most (60.9%) of the children had 1 or 2 current healthroblems, with 8.9% having 4 or more and 16.6% having nourrent health problems. The most commonly reported wereye, ear, and muscle/bone problems, in 52%, 32%, and 22%,espectively (co-occurring in a number of these). Althoughlmost all (89.6%) mothers reported at least 1 episode of
llness for their child during 2004, the vast majority of chil-e 321

dontT(wadap
sffpc(sbos(iadcccwst
wAmogtttwo
wcbieshsbmdm
scqstsodisr
soacdcmal
pnsnssmeca
mbish
pD(t(hfDctm
O
3
ren (84%) did not require hospital admission. Using a cut-ff of 44 (sensitivity/specificity of �83%) we found thatearly a third (66/211, 31.3%) of children had scores abovehe clinical threshold for abnormal developmental behavior.22
here were almost equal proportions of males and femalesP � .99). There were slightly higher proportions of childrenith abnormal scores in the 5-to-9-year age group (39.6%)
nd 10 to 13 years (37.8%), but no statistically significantifferences between age groups. For children aged 12 yearsnd older, most needed help with money management, shop-ing, using public transport, and meal preparation.
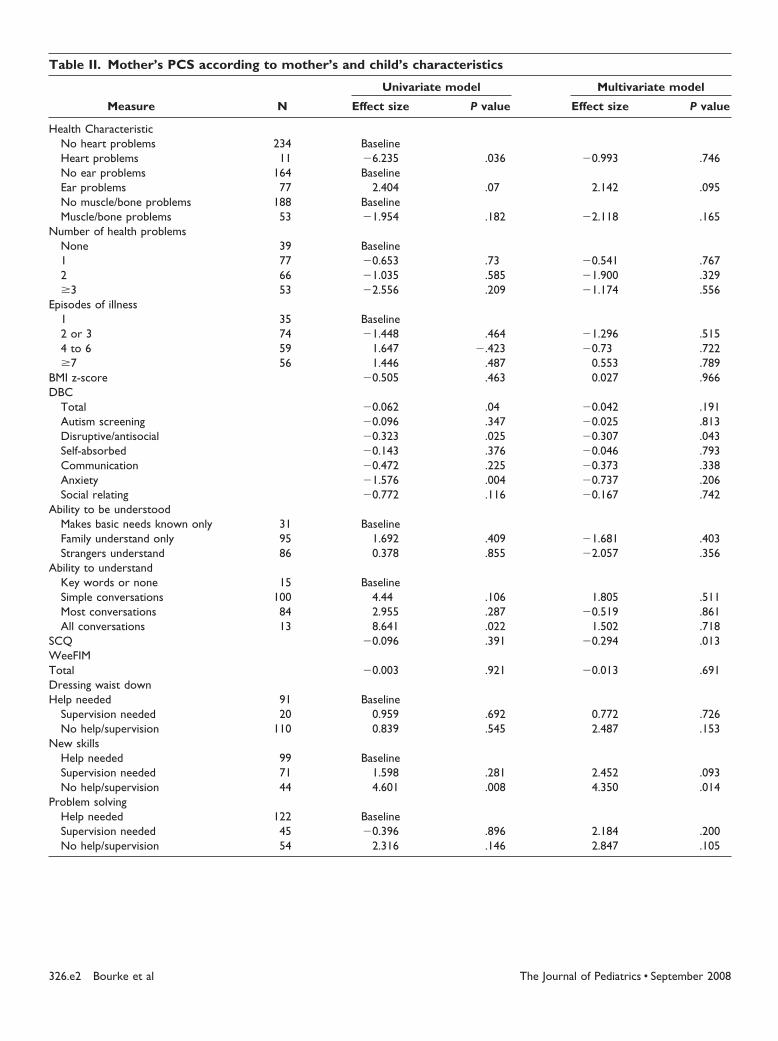
The average maternal PCS score was 50.2 (SD: 9.6),ignificantly higher than but within 1 SD of the Australianemale norm of 48.423 (P � .015). The univariate analysesound that lower mean physical health scores (ie, worsehysical health) were observed in mothers of children withurrent heart problems (mean: 44.2; SD: 12.5) (P � .036)Table II; available at www.jpeds.com). There was noignificant difference in maternal physical health on theasis of the number of current health problems in the childr episodes of illness. Lower physical health scores wereeen in mothers of children who had higher DBC scoresie, more dysfunctional personalities, emotions and behav-or), with significant differences seen in the disruptive/ntisocial and anxiety subscales. There was no significantifference in maternal physical health on the basis of thehild’s ability to be understood, but mothers had signifi-antly better physical health if their child understood allonversations. Significantly better physical health scoresere seen in mothers of children who required no help/
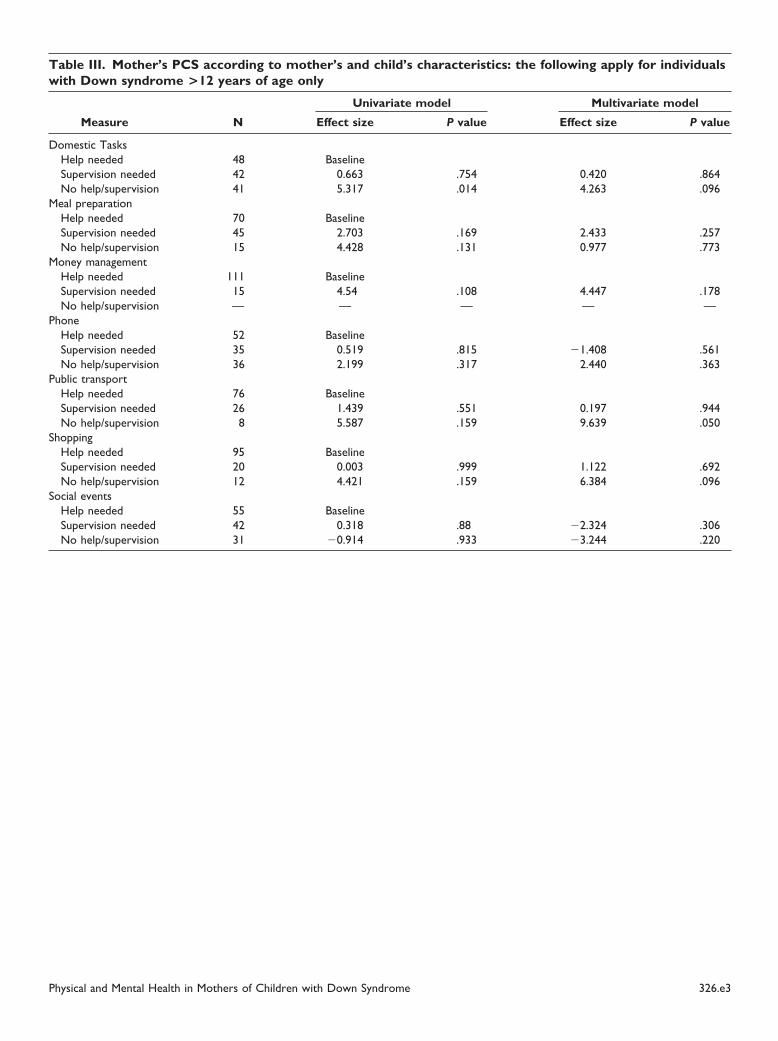
upervision in learning new skills (Table II) and domesticasks (Table III; available at www.jpeds.com).
The average maternal MCS score was 45.2 (SD: 10.6),hich is significantly lower than but within 1 SD of theustralian female norm of 51.4 (P � .0001).23 Mother’sental health improved with maternal age overall (by a factor
f 0.16 per year of age, P � .05). In relation to child’s ageroup the effect was not linear with the scores being lowest inhose aged 10 to 13 years, significantly higher (P � .02) inhose aged 14 to 17 years, and intermediate in those youngerhan 9 years. Once the effect of mother’s age on mental healthas adjusted for, the co-occurring effect of child’s age groupn mother’s mental health was no longer significant.
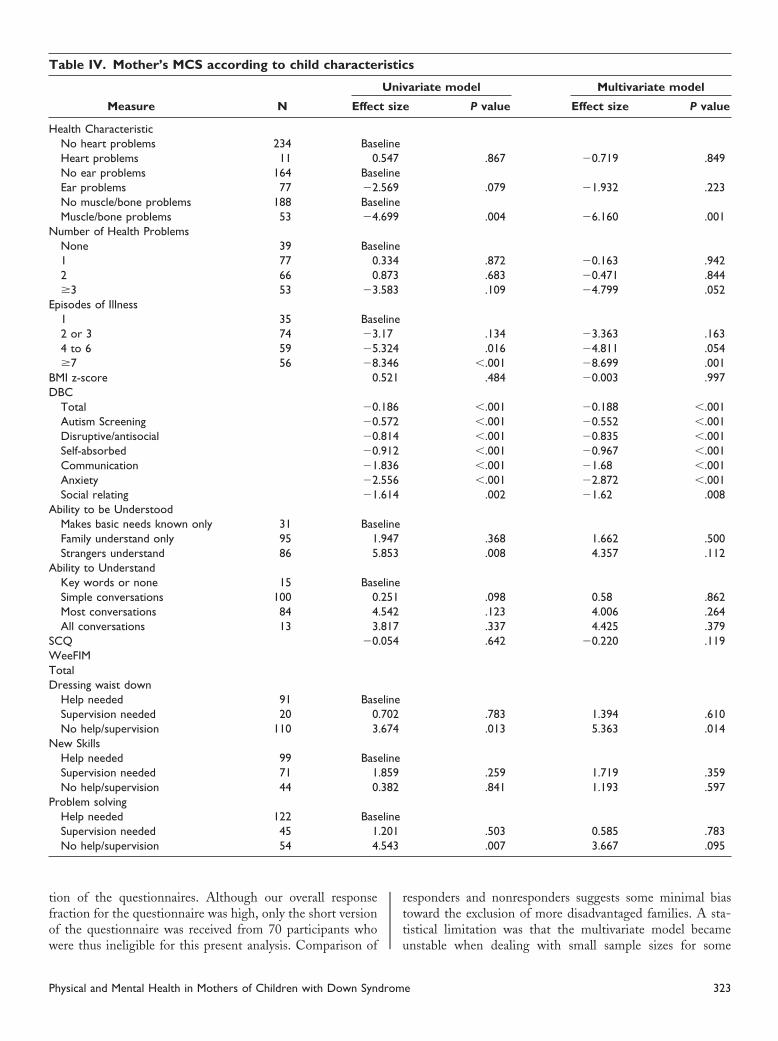
In the univariate analyses, worse maternal mental healthas associated with the child with Down syndrome having
urrent ear problems and current muscle/bone problems (Ta-le IV). Compared with mothers of children with 1 episode ofllness in 2004, those whose children had 4 to 6 or �7pisodes also had poorer mental health. Across all subscales,ignificantly lower mental health scores (ie, worse mentalealth) were seen in mothers of children with higher DBCcores (ie, more dysfunctional personalities, emotions andehavior) (P � .001). Better mental health was observed inothers of children who were able to make themselves un-
erstood to strangers in comparison to those only able to
ake their basic needs known. i22 Bourke et al
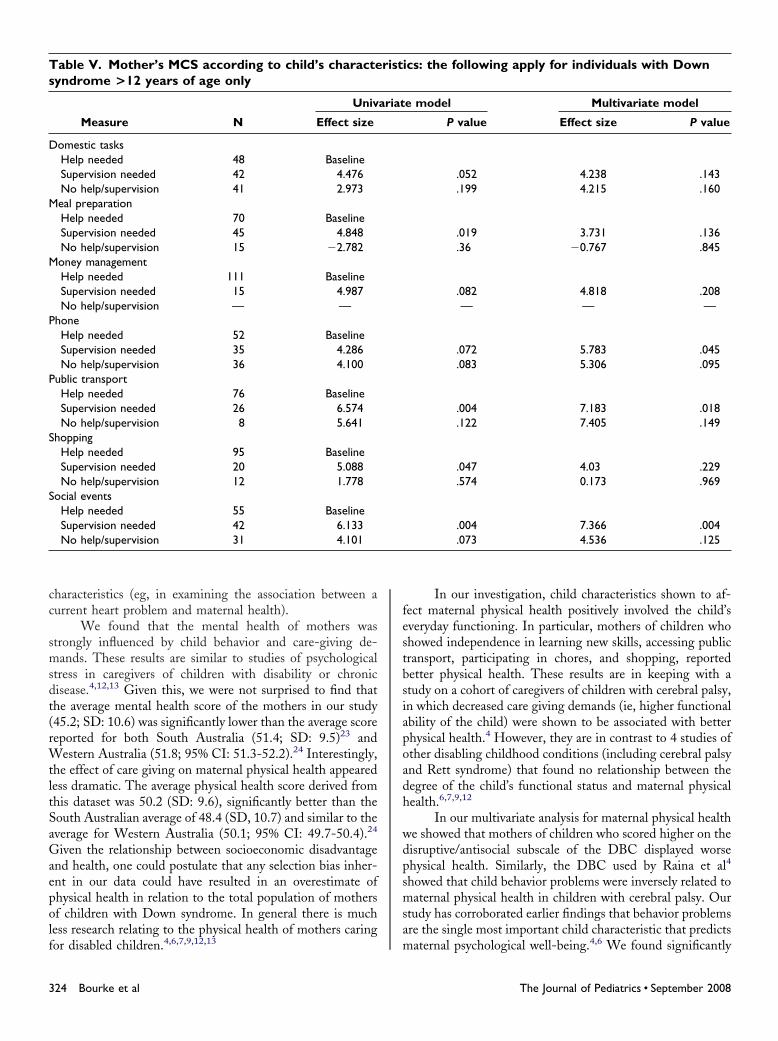
With respect to functional ability, higher mental healthcores (ie, better mental health) were seen in mothers ofhildren who, compared with those who needed help, re-uired no help/supervision in dressing waist down, problemolving (Table IV) and, in children above 12 years, using theelephone (P � .083) and at social events (Table V). Also,ignificantly better mental health was also seen in mothers oflder children when only supervision was required for theaily activities of meal preparation, money management, us-ng the telephone, using public transport, shopping, and atocial events, compared with those mothers whose childrenequired help for these tasks (Table V).
In the final multivariate model the only child variableshown to affect maternal physical health positively were thosebserved on basic functional activities using the WeeFIM and indvanced functional activities in the community. Mothers ofhildren who required no help/supervision in learning new skills,omestic tasks, public transport, and shopping, showed signifi-antly higher mean physical health scores. On the other hand,others of children who scored higher on the DBC disruptive/
ntisocial scale (ie, more disruptive/antisocial behavior) displayedower mean physical health scores (P � .043) (Table II).
The final multivariate model showed the child variablesositively associated with better maternal mental health wereo help/supervision needed for dressing waist down, problemolving (Table IV) and using the telephone, and supervisioneeded using the telephone, using public transport, and atocial events (Table V). Significantly lower mental healthcores were seen in mothers of children who had currentuscle/bone problems, �3 current health problems, 4 to 6
pisodes of illness in 2004, �7 episodes of illness in 2004, andhildren who had more dysfunctional personality, emotionsnd behavior (Table IV).
DISCUSSIONThis study found that the most important predictors of
aternal health, particularly mental health, were the child’sehavioral difficulties, the child’s level of everyday function-ng, the child’s progress in community participation involvinghopping and travel, and to a lesser degree, the child’s currentealth status.
The major strength of our study is that we have aopulation-based cohort of families each with a child withown syndrome with measures of both maternal health
physical and mental) and a wide range of child characteris-ics. In addition, we had a high response to questionnaires73%). To our knowledge, there have been no studies thatave investigated the impact on mother’s health of specificunctional deficits or medical problems in the child withown syndrome. Other strengths of our study are that the
ohort covers a wide range of ages (0-25 years), and we haveaken into account potentially confounding factors in theultivariate analysis.
We acknowledge that the study has some limitations.ur follow-up of nonrespondents was compromised because
t was a requirement to outsource the distribution and collec-
The Journal of Pediatrics • September 2008
tfow
rtt
T
H
N
E
BD
A
A
SWTD
N
P
.543
P
ion of the questionnaires. Although our overall responseraction for the questionnaire was high, only the short versionf the questionnaire was received from 70 participants who
able IV. Mother’s MCS according to child character
Measure N Effec
ealth CharacteristicNo heart problems 234 BaseHeart problems 11 0No ear problems 164 BaseEar problems 77 �2No muscle/bone problems 188 BaseMuscle/bone problems 53 �4umber of Health ProblemsNone 39 Base1 77 02 66 0�3 53 �3
pisodes of Illness1 35 Base2 or 3 74 �34 to 6 59 �5�7 56 �8
MI z-score 0BCTotal �0Autism Screening �0Disruptive/antisocial �0Self-absorbed �0Communication �1Anxiety �2Social relating �1
bility to be UnderstoodMakes basic needs known only 31 BaseFamily understand only 95 1Strangers understand 86 5
bility to UnderstandKey words or none 15 BaseSimple conversations 100 0Most conversations 84 4All conversations 13 3
CQ �0eeFIM
otalressing waist downHelp needed 91 BaseSupervision needed 20 0No help/supervision 110 3ew SkillsHelp needed 99 BaseSupervision needed 71 1No help/supervision 44 0
roblem solvingHelp needed 122 BaseSupervision needed 45 1No help/supervision 54 4
ere thus ineligible for this present analysis. Comparison of u
hysical and Mental Health in Mothers of Children with Down Syndrom
esponders and nonresponders suggests some minimal biasoward the exclusion of more disadvantaged families. A sta-istical limitation was that the multivariate model became
s
ariate model Multivariate model
P value Effect size P value
.867 �0.719 .849
.079 �1.932 .223
.004 �6.160 .001
.872 �0.163 .942
.683 �0.471 .844
.109 �4.799 .052
.134 �3.363 .163
.016 �4.811 .054�.001 �8.699 .001
.484 �0.003 .997
�.001 �0.188 �.001�.001 �0.552 �.001�.001 �0.835 �.001�.001 �0.967 �.001�.001 �1.68 �.001�.001 �2.872 �.001
.002 �1.62 .008
.368 1.662 .500
.008 4.357 .112
.098 0.58 .862
.123 4.006 .264
.337 4.425 .379
.642 �0.220 .119
.783 1.394 .610
.013 5.363 .014
.259 1.719 .359
.841 1.193 .597
.503 0.585 .783
.007 3.667 .095
istic
Univ
t size
line.547line
.569line
.699
line.334.873.583
line.17.324.346.521
.186
.572
.814
.912
.836
.556
.614
line.947.853
line.251.542.817.054
line.702.674
line.859.382
line.201
nstable when dealing with small sample sizes for some
e 323
cc
smsdt(rWtltSaGaepolf
festbsiapoadh
wdpsmsa
Ts
D
M
M
P
P
S
S
3
haracteristics (eg, in examining the association between aurrent heart problem and maternal health).
We found that the mental health of mothers wastrongly influenced by child behavior and care-giving de-ands. These results are similar to studies of psychological
tress in caregivers of children with disability or chronicisease.4,12,13 Given this, we were not surprised to find thathe average mental health score of the mothers in our study45.2; SD: 10.6) was significantly lower than the average scoreeported for both South Australia (51.4; SD: 9.5)23 and
estern Australia (51.8; 95% CI: 51.3-52.2).24 Interestingly,he effect of care giving on maternal physical health appearedess dramatic. The average physical health score derived fromhis dataset was 50.2 (SD: 9.6), significantly better than theouth Australian average of 48.4 (SD, 10.7) and similar to theverage for Western Australia (50.1; 95% CI: 49.7-50.4).24
iven the relationship between socioeconomic disadvantagend health, one could postulate that any selection bias inher-nt in our data could have resulted in an overestimate ofhysical health in relation to the total population of mothersf children with Down syndrome. In general there is muchess research relating to the physical health of mothers caring
able V. Mother’s MCS according to child’s characteyndrome >12 years of age only
Measure N
Univ
Effect size
omestic tasksHelp needed 48 BaselineSupervision needed 42 4.476No help/supervision 41 2.973eal preparationHelp needed 70 BaselineSupervision needed 45 4.848No help/supervision 15 �2.782oney managementHelp needed 111 BaselineSupervision needed 15 4.987No help/supervision — —
honeHelp needed 52 BaselineSupervision needed 35 4.286No help/supervision 36 4.100
ublic transportHelp needed 76 BaselineSupervision needed 26 6.574No help/supervision 8 5.641
hoppingHelp needed 95 BaselineSupervision needed 20 5.088No help/supervision 12 1.778
ocial eventsHelp needed 55 BaselineSupervision needed 42 6.133No help/supervision 31 4.101
or disabled children.4,6,7,9,12,13 m
24 Bourke et al
In our investigation, child characteristics shown to af-ect maternal physical health positively involved the child’sveryday functioning. In particular, mothers of children whohowed independence in learning new skills, accessing publicransport, participating in chores, and shopping, reportedetter physical health. These results are in keeping with atudy on a cohort of caregivers of children with cerebral palsy,n which decreased care giving demands (ie, higher functionalbility of the child) were shown to be associated with betterhysical health.4 However, they are in contrast to 4 studies ofther disabling childhood conditions (including cerebral palsynd Rett syndrome) that found no relationship between theegree of the child’s functional status and maternal physicalealth.6,7,9,12
In our multivariate analysis for maternal physical healthe showed that mothers of children who scored higher on theisruptive/antisocial subscale of the DBC displayed worsehysical health. Similarly, the DBC used by Raina et al4
howed that child behavior problems were inversely related toaternal physical health in children with cerebral palsy. Our
tudy has corroborated earlier findings that behavior problemsre the single most important child characteristic that predicts
cs: the following apply for individuals with Down
e model Multivariate model
P value Effect size P value
.052 4.238 .143
.199 4.215 .160
.019 3.731 .136
.36 �0.767 .845
.082 4.818 .208— — —
.072 5.783 .045
.083 5.306 .095
.004 7.183 .018
.122 7.405 .149
.047 4.03 .229
.574 0.173 .969
.004 7.366 .004
.073 4.536 .125
risti
ariat
aternal psychological well-being.4,6 We found significantly
The Journal of Pediatrics • September 2008

wisw
twddabcebt
fmqam1pecsgra
mlihaifi
dbDAptsdupc
ipbap
awiacowch
n(tanca0ha
WioSqCT
1E2Po3Cb4h25gc6wd7mM8c9a21ps1e1a21
P
orse mental health in mothers of children who scored highern the DBC across all 6 subscales. A number of previoustudies report higher levels of stress in mothers of childrenith more maladaptive behaviours.25-28
Intellectual disability appears to predispose individualso emotional or behavioral problems. This “dual diagnosis” isell-documented in adulthood where adults with intellectualisability have been found to be at an increased risk of mentalisorders,29 and the evidence has now extended to adolescentsnd children as well.30,31 Eisenhower et al26 showed at age 3,ehavioral problems in children with Down syndrome areomparable to those of typically developing children. How-ver, over the next 2 years there was a relative increase inehavior problems in their Down syndrome cohort and, inurn, maternal stress.
In our study, mothers of children with higher everydayunctioning experienced better mental health. In particular,others reported better mental health if their children re-
uired no help or supervision in dressing, problem solvingnd, for children over 12 years, using the telephone. Similarly,others reported better mental health if their child aged over
2 years required supervision but no help in using the tele-hone, using public transportation, and attending socialvents. Three other studies of children with disabilities (in-luding cystic fibrosis, cerebral palsy, and myelodysplasia) hadimilar findings, in that the more dependent the child thereater the mother’s distress.4,8 However, 4 studies found noelationship between the degree of child’s functional statusnd maternal mental health.6,7,9,12
Significantly lower mental health scores were seen inothers of children who had current musculoskeletal prob-
ems, 3 or more current health problems, and �4 episodes ofllness in 2004. Ours is the first study to investigate specificealth characteristics in the child with Down syndrome andssess their impact on mothers’ mental well-being. However,n comparison to functional and behavioral attributes, weound that the health of the child had perhaps less of anmpact than we had anticipated.
In contrast to other studies that have not consistentlyemonstrated an association with poorer psychological well-eing,2,32 our results suggest that mothers of children withown syndrome do often experience poorer mental health.s a result they may require greater support and servicerovision to enhance both behavior management skills andheir own subsequent psychological well-being. Douma et al33
howed that most (88.2%) parents of youths with intellectualisabilities had various support needs that were frequentlynmet. In addition, the study found that the “parents whoerceived both emotional and behavioral problems in theirhild needed support the most.”
As we have seen in our study, maladaptive child behav-or is the single most important child characteristic thatredicts maternal stress. King et al6 showed services are mosteneficial when delivered in a family-centered manner andddressing parent-identified issues such as child behavior
roblems. Service providers need to address both the child’sy1
hysical and Mental Health in Mothers of Children with Down Syndrom
nd parents’ problems, as well as the family’s ability to dealith these problems. As Raina et al4 stated, “Clearly, it is
mportant for health care providers to assess how caregiversre affected by behavioral as well as ‘functional’ aspects of thehild’s disability in the provision of comprehensive family-riented services. In terms of prevention, providing parentsith cognitive and behavioral strategies to manage their
hild’s behaviors may have the potential to change caregiverealth outcomes.”
As endorsed by the biopsychosocial model of the Inter-ational Classification of Functioning, Disability and HealthICF)34, it is the collective responsibility of society to enablehe full participation of people with Down syndrome into allreas of society and community life. In future research, weeed to look at the types and mix of support mothers ofhildren with Down syndrome need and whether their needsre being met. Individuals in this investigation were betweenand 25 years, but as they age families face new challenges,
ence further research should explore the health of mothers ofdults with Down syndrome.
e gratefully acknowledge all the families who have participatedn the Down Syndrome NOW Study and thank them for theirngoing commitment. The authors thank Carol Philippe, Jackieoftly and Michele Le Miere for their assistance with follow-up ofuestionnaires. We also thank the staff at the Disability Servicesommission for their assistance, as well as colleagues at theelethon Institute for Child Health Research.
REFERENCES. Bittles AH, Bower C, Hussain R, Glasson EJ. The four ages of Down syndrome.ur J Public Health 2007;17:221-5.. Abbeduto L, Seltzer MM, Shattuck P, Krauss MW, Orsmond G, Murphy MM.sychological well-being and coping in mothers of youths with autism, Down syndrome,r fragile X syndrome. Am J Ment Retard 2004;109:237-54.. Hauser-Cram P, Warfield ME, Shonkoff JP, Krauss MW, Sayer A, Upshur CC.hildren with disabilities: a longitudinal study of child development and parent well-eing. Monogr Soc Res Child Dev 2001;66:i-viii, 1-114; discussion 5-26.. Raina P, O’Donnell M, Rosenbaum P, Brehaut J, Walter SD, Russell D, et al. Theealth and well-being of caregivers of children with cerebral palsy. Pediatrics005;115:e626-36.. Boyce GC, Behl D, Mortensen L, Akers J. Child characteristics, family demo-raphics and family processes: their effects on the stress experienced by families ofhildren with disabilities. Counseling Psyc Q 1991;4:273-88.. King G, King S, Rosenbaum P, Goffin R. Family-centered care giving andell-being of parents of children with disabilities: linking process with outcome. J Pe-iatr Psychol 1999;24:41-53.. Waddington SR, Busch-Rossnagel NA. The influence of a child’s disability onother’s role functioning and psychological well-being. Genet Soc Gen Psycholonogr 1992;118:293-311.
. Sloper P, Turner S. Risk and resistance factors in the adaptation of parents ofhildren with severe physical disability. J Child Psychol Psychiatr 1993;34:167-88.. Manuel J, Naughton MJ, Balkrishnan R, Paterson Smith B, Koman LA. Stressnd adaptation in mothers of children with cerebral palsy. J Pediatr Psychol003;28:197-201.0. Wallander JL, Pitt LC, Mellins CA. Child functional independence and maternalsychosocial stress as risk factors threatening adaptation in mothers of physically orensorially handicapped children. J Consult Clin Psychol 1990;58:818-24.1. Montes G, Halterman JS. Psychological Functioning and Coping Among Moth-rs of Children With Autism: A Population-Based Study. Pediatrics 2007;119:e1040-6.2. Laurvick CL, Msall ME, Silburn S, Bower C, de Klerk N, Leonard H. Physicalnd mental health of mothers caring for a child with Rett syndrome. Pediatrics006;118:e1152-64.3. Mackey S, Goddard LD. The experience of health and wellness in mothers of
oung children with intellectual disabilities. J Intellect Disabil 2006;10:305-15.4. Emerson E, Hatton C, Llewellyn G, Blacher J, Graham H. Socio-economice 325

pm21tQ1(d1t1ac1C2s2C2bc2bR22h
T[02mR2iR2ia2y2rP3aR3i3r3l3
3
osition, household composition, health status and indicators of the well-being ofothers of children with and without intellectual disabilities. J Intellect Disabil Res
006;50:862-73.5. Ware J.E. Jr, Kosinski M, Turner-Bowker D.M., B. G. How to ScoreVersion 2 ofhe SF-12 Health Survey (With a Supplement Documenting Version 1). Lincoln, RI:ualityMetric Incorporated; 2002.
6. Petterson B, Leonard H, Bourke J, Sanders R, Chalmers R, Jacoby P, et al. IDEAIntellectual Disability Exploring Answers): a population-based database for intellectualisability in Western Australia. Ann Hum Biol 2005;32:237-43.7. Sanderson K, Andrews G. The SF-12 in the Australian population: cross-valida-ion of item selection. Aust N Z J Public Health 2002;26:343-5.8. Einfeld SL, Tonge BT. The developmental behavior checklist: The developmentnd validation of an instrument to assess behavioral and emotional disturbance inhildren and adolescents with mental retardation. J Autism Dev Disord 1995;25:81-104.9. Rutter M, Bailey A, Lord C. Social Communication Questionnaire. Los Angeles,A: Western Psychological Services; 2003.
0. Leonard S, Msall M, Bower C, Tremont M, Leonard H. Functional status ofchool-aged children with Down syndrome. J Paediatr Child Health 2002;38:160-5.1. StataCorp. Stata Statistical Software. Release 80. College Station, Texas: Stataorporation; 2003.
2. Einfeld SL, Tonge BJ. Manual for the Developmental Behavior Checklist. Mel-ourne, Australia: Monash University Centre for Developmental Psychiatry and Psy-hology; 2002.3. Avery J, Dal Grande E, Taylor A. Quality of Life in South Australia as measuredy the SF12 Health Status Questionnaire: Population norms for 2003: Populationesearch and Outcome Studies Unit, Department of Human Services, South Australia;004.
4. Taylor A, Daly A, d’Espaignet E, Wilson D, Eshpeter J, Measey M. Collaborativeealth and wellbeing CATI survey of adults living in Western Australia, Northernd2
26 Bourke et al
erritory and South Australia: Report I - Summary of results by State/Territory. 2002cited 20 July, 2007]; Available from: https://www.library.health.sa.gov.au/Portals//collaborative-health-and-wellbeing-cati-report1.pdf5. Baker BL, Blacher J, Olsson MB. Preschool children with and without develop-ental delay: behavior problems, parents’ optimism and well-being. J Intellect Disabiles 2005;49:575-90.6. Eisenhower AS, Baker BL, Blacher J. Preschool children with intellectual disabil-ty: syndrome specificity, behavior problems, and maternal well-being. J Intellect Disabiles 2005;49:657-71.7. Hassall R, Rose J, McDonald J. Parenting stress in mothers of children with anntellectual disability: the effects of parental cognitions in relation to child characteristicsnd family support. J Intellect Disabil Res 2005;49:405-18.8. Most DE, Fidler DJ, Laforce-Booth C, Kelly J. Stress trajectories in mothers ofoung children with Down syndrome. J Intellect Disabil Res 2006;50:501-14.9. Nezu CM, Nezu AM, Gill-Weiss MJ. Psychopathology in persons with mentaletardation: Clinical guidelines for assessment and treatment Champaign, IL: Researchress; 1992.0. Einfeld SL, Tonge BJ. Population prevalence of psychopathology in children anddolescents with intellectual disability: II. Epidemiological findings. J Intellect Disabiles 1996;40:99-109.1. Gray K, Mohr C. Mental health problems in children and adolescents withntellectual disability. Curr Op Psych 2004;17:365-70.2. Glidden LM, Schoolcraft SA. Depression: its trajectory and correlates in mothersearing children with intellectual disability. J Intellect Disabil Res 2003;47:250-63.3. Douma JCH, Dekker MC, Koot HM. Supporting parents of youths with intel-ectual disabilities and psychopathology. J Intellect Disabil Res 2006;50:570-81.4. World Health Organization. ICF: International classification of functioning,
isability and health/World Health Organization. Geneva: World Health Organization;001.The Journal of Pediatrics • September 2008
T
S
W
D
S
c evaluation
P
able I. Instruments used in Down syndrome NOW
InstrumentNo.
Items Description of in
F12 Version 215
(n � 250)12 Widely used and accepted generic
that covers the areas of physicalvitality, social functioning, and methe score the better the person’
eeFIM20 (n � 223) 18 Developed to measure the typicalessential self-care, mobility and clearning skills. The higher the scoability to complete essential dailyassistance or supervision. It wasquestionnaire format in a study osyndrome.
BC18 N � 211 96 Assesses the behavior and emotionand adolescents with mental retahigher the score the greater theemotional disturbance.
ocial CommunicationQuestionnaire19
(n � 213)
40 A screening instrument for autism,Autism Screening Questionnairecommunication skills and social fgroups with or without ID. Scorreferral for a complete diagnosti
questionnaire that were included in analysis
strumentRange of
possible scoresCohort mean (SD) &
range of scores
measure of health statusfunctioning, pain, health,ntal health. The higher
s health.
0-100 PCS: 50.2 (9.6); 18.2-67.1
MCS: 45.2 (10.6); 2.6-66.8
performance of children inommunication-socialre the greater the child’stasks without parental
previously adapted forf children with Down
18-126 Mean: 94.2 (25.6)Range: 24-126
al disturbance in childrenrdation. 6 subscales. Thechild’s behavior and
0-300 Mean: 36.6 (22.6)Range: 1-106Prop. � 44: 31.3%
previously known as theit helps evaluateunctioning with all agees � 15 recommended
0-39 Mean: 11.1 (6.1)Range: 0-32
hysical and Mental Health in Mothers of Children with Down Syndrome 326.e1
T
H
N
E
BD
A
A
SWTDH
N
P
3
able II. Mother’s PCS according to mother’s and child’s characteristics
Measure N
Univariate model Multivariate model
Effect size P value Effect size P value
ealth CharacteristicNo heart problems 234 BaselineHeart problems 11 �6.235 .036 �0.993 .746No ear problems 164 BaselineEar problems 77 2.404 .07 2.142 .095No muscle/bone problems 188 BaselineMuscle/bone problems 53 �1.954 .182 �2.118 .165umber of health problemsNone 39 Baseline1 77 �0.653 .73 �0.541 .7672 66 �1.035 .585 �1.900 .329�3 53 �2.556 .209 �1.174 .556
pisodes of illness1 35 Baseline2 or 3 74 �1.448 .464 �1.296 .5154 to 6 59 1.647 �.423 �0.73 .722�7 56 1.446 .487 0.553 .789
MI z-score �0.505 .463 0.027 .966BCTotal �0.062 .04 �0.042 .191Autism screening �0.096 .347 �0.025 .813Disruptive/antisocial �0.323 .025 �0.307 .043Self-absorbed �0.143 .376 �0.046 .793Communication �0.472 .225 �0.373 .338Anxiety �1.576 .004 �0.737 .206Social relating �0.772 .116 �0.167 .742
bility to be understoodMakes basic needs known only 31 BaselineFamily understand only 95 1.692 .409 �1.681 .403Strangers understand 86 0.378 .855 �2.057 .356
bility to understandKey words or none 15 BaselineSimple conversations 100 4.44 .106 1.805 .511Most conversations 84 2.955 .287 �0.519 .861All conversations 13 8.641 .022 1.502 .718
CQ �0.096 .391 �0.294 .013eeFIM
otal �0.003 .921 �0.013 .691ressing waist downelp needed 91 BaselineSupervision needed 20 0.959 .692 0.772 .726No help/supervision 110 0.839 .545 2.487 .153ew skillsHelp needed 99 BaselineSupervision needed 71 1.598 .281 2.452 .093No help/supervision 44 4.601 .008 4.350 .014
roblem solvingHelp needed 122 BaselineSupervision needed 45 �0.396 .896 2.184 .200
No help/supervision 54 2.316 .146 2.847 .10526.e2 Bourke et al The Journal of Pediatrics • September 2008
Tw
D
M
M
P
P
S
S
P
able III. Mother’s PCS according to mother’s and child’s characteristics: the following apply for individualsith Down syndrome >12 years of age only
Measure N
Univariate model Multivariate model
Effect size P value Effect size P value
omestic TasksHelp needed 48 BaselineSupervision needed 42 0.663 .754 0.420 .864No help/supervision 41 5.317 .014 4.263 .096eal preparationHelp needed 70 BaselineSupervision needed 45 2.703 .169 2.433 .257No help/supervision 15 4.428 .131 0.977 .773oney managementHelp needed 111 BaselineSupervision needed 15 4.54 .108 4.447 .178No help/supervision — — — — —
honeHelp needed 52 BaselineSupervision needed 35 0.519 .815 �1.408 .561No help/supervision 36 2.199 .317 2.440 .363
ublic transportHelp needed 76 BaselineSupervision needed 26 1.439 .551 0.197 .944No help/supervision 8 5.587 .159 9.639 .050
hoppingHelp needed 95 BaselineSupervision needed 20 0.003 .999 1.122 .692No help/supervision 12 4.421 .159 6.384 .096
ocial eventsHelp needed 55 BaselineSupervision needed 42 0.318 .88 �2.324 .306
No help/supervision 31 �0.914 .933 �3.244 .220hysical and Mental Health in Mothers of Children with Down Syndrome 326.e3