Embed Size (px)
Citation preview

Vol. 107 No. 1 January 2009
CLINICOPATHOLOGIC CONFERENCE Editor: Paul C. Edwards
Pigmentation of the hard palateMark A. Lerman, DMD,a,b Nadeem Karimbux, DMD, MMSc,c Kevin A. Guze, DMD,d andSook-Bin Woo, DMD, MMSc,b,e Boston, MassachusettsHARVARD SCHOOL OF DENTAL MEDICINE AND BRIGHAM AND WOMEN’S HOSPITAL
(Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;107:8-12)CASE REPORTA 57-year-old African-American female presented
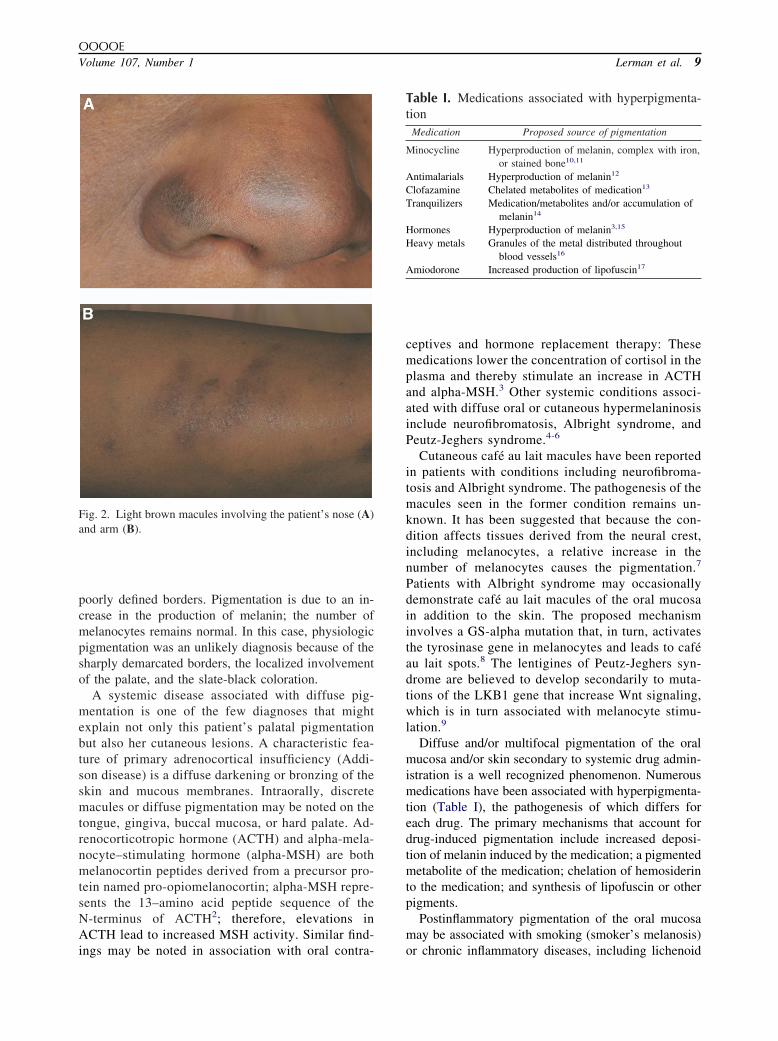
for implant evaluation with slate-black pigmentation ofthe hard palate (Fig. 1). She was unaware of this con-dition, and therefore the duration of the condition couldnot be ascertained. Extraoral examination revealedbrown macular lesions on her nose, extensor surfaces ofarms, and dorsa of hands (Fig. 2). She reported thatthese cutaneous lesions had been present for approxi-mately 12 years.
Her medical history was significant only for discoidlupus erythematosus (DLE). She was prescribed quin-acrine for DLE, and she did not report the use of otherprescription or over-the-counter medications. She re-ported an allergy to penicillin and denied a history ofsmoking or of alcohol use.
DIFFERENTIAL DIAGNOSISThe differential diagnosis for a large flat pigmented
area of the palate included the following: physiologicpigmentation, pigmentation associated with systemicdisease, medication-related pigmentation, postinflam-
aInstructor, Department of Oral Medicine, Infection, and Immunity,Harvard School of Dental Medicine.bDivision of Oral Medicine and Dentistry, Brigham and Women’sHospital.cAssociate Professor, Department of Oral Medicine, Infection, andImmunity, Harvard School of Dental Medicine.dResident, Department of Oral Medicine, Infection, and Immunity,Harvard School of Dental Medicine.eAssociate Professor, Department of Oral Medicine, Infection, andImmunity, Harvard School of Dental Medicine.Received for publication May 29, 2008; returned for revision Jul 16,2008; accepted for publication Jul 17, 2008.1079-2104/$ - see front matter© 2009 Mosby, Inc. All rights reserved.
doi:10.1016/j.tripleo.2008.07.0228
matory pigmentation, oral melanoacanthosis (melano-acanthoma), blue nevus, and malignant mucosal mela-noma. Small localized pigmented lesions including oralmelanotic macules, melanocytic nevi, amalgam tattoos,and vascular lesions were not seriously considered. Adiagnosis of Kaposi sarcoma (KS) was briefly enter-tained; however, the brown and black coloration of thepatient’s skin and oral lesions, her lack of known riskfactors that would predispose her to KS, and the factthat this condition uncommonly presents in women allhelped rule out this diagnosis.
Physiologic (racial) pigmentation is the most com-mon form of intraoral multifocal diffuse pigmentation.1
It is seen most commonly in individuals with darkcomplexions and it may involve any mucosal site. Thepigmentation is asymptomatic and patients are oftenunaware of its presence. Classically, the gingiva,tongue, hard palate, buccal mucosa, and/or lips present
Fig. 1. Black macular pigmentation of the palatal mucosa.
with light to dark brown macules with irregular and
OOOOEVolume 107, Number 1 Lerman et al. 9
poorly defined borders. Pigmentation is due to an in-crease in the production of melanin; the number ofmelanocytes remains normal. In this case, physiologicpigmentation was an unlikely diagnosis because of thesharply demarcated borders, the localized involvementof the palate, and the slate-black coloration.
A systemic disease associated with diffuse pig-mentation is one of the few diagnoses that mightexplain not only this patient’s palatal pigmentationbut also her cutaneous lesions. A characteristic fea-ture of primary adrenocortical insufficiency (Addi-son disease) is a diffuse darkening or bronzing of theskin and mucous membranes. Intraorally, discretemacules or diffuse pigmentation may be noted on thetongue, gingiva, buccal mucosa, or hard palate. Ad-renocorticotropic hormone (ACTH) and alpha-mela-nocyte–stimulating hormone (alpha-MSH) are bothmelanocortin peptides derived from a precursor pro-tein named pro-opiomelanocortin; alpha-MSH repre-sents the 13–amino acid peptide sequence of theN-terminus of ACTH2; therefore, elevations inACTH lead to increased MSH activity. Similar find-
Fig. 2. Light brown macules involving the patient’s nose (A)and arm (B).
ings may be noted in association with oral contra-
ceptives and hormone replacement therapy: Thesemedications lower the concentration of cortisol in theplasma and thereby stimulate an increase in ACTHand alpha-MSH.3 Other systemic conditions associ-ated with diffuse oral or cutaneous hypermelaninosisinclude neurofibromatosis, Albright syndrome, andPeutz-Jeghers syndrome.4-6
Cutaneous café au lait macules have been reportedin patients with conditions including neurofibroma-tosis and Albright syndrome. The pathogenesis of themacules seen in the former condition remains un-known. It has been suggested that because the con-dition affects tissues derived from the neural crest,including melanocytes, a relative increase in thenumber of melanocytes causes the pigmentation.7
Patients with Albright syndrome may occasionallydemonstrate café au lait macules of the oral mucosain addition to the skin. The proposed mechanisminvolves a GS-alpha mutation that, in turn, activatesthe tyrosinase gene in melanocytes and leads to caféau lait spots.8 The lentigines of Peutz-Jeghers syn-drome are believed to develop secondarily to muta-tions of the LKB1 gene that increase Wnt signaling,which is in turn associated with melanocyte stimu-lation.9
Diffuse and/or multifocal pigmentation of the oralmucosa and/or skin secondary to systemic drug admin-istration is a well recognized phenomenon. Numerousmedications have been associated with hyperpigmenta-tion (Table I), the pathogenesis of which differs foreach drug. The primary mechanisms that account fordrug-induced pigmentation include increased deposi-tion of melanin induced by the medication; a pigmentedmetabolite of the medication; chelation of hemosiderinto the medication; and synthesis of lipofuscin or otherpigments.
Postinflammatory pigmentation of the oral mucosamay be associated with smoking (smoker’s melanosis)
Table I. Medications associated with hyperpigmenta-tion
Medication Proposed source of pigmentation
Minocycline Hyperproduction of melanin, complex with iron,or stained bone10,11
Antimalarials Hyperproduction of melanin12
Clofazamine Chelated metabolites of medication13
Tranquilizers Medication/metabolites and/or accumulation ofmelanin14
Hormones Hyperproduction of melanin3,15
Heavy metals Granules of the metal distributed throughoutblood vessels16
Amiodorone Increased production of lipofuscin17
or chronic inflammatory diseases, including lichenoid
OOOOE10 Lerman et al. January 2009
processes. Brown or black macules and patches appearon the affected tissues and are seen more often indark-skinned individuals. Hyperpigmentation may re-sult from stimulation of melanocytes by inflammatorycytokines or reactive oxygen species.18 These pig-mented areas are asymptomatic. Pigmentation second-ary to smoker’s melanosis is usually limited to thegingiva. Involvement of the palate is rare. Although thispatient had a history of DLE, she did not demonstratethe white reticulated and erythematous inflammatorylesions often seen in this condition. It was thereforedeemed unlikely that her extensive area of pigmenta-tion was postinflammatory secondary to lesions ofDLE.
Oral melanoacanthosis is a benign asymptomatic le-sion of the oral mucosa believed to be reactive inorigin.19 The lesions are dark brown-black in color andmay reach up to several centimeters in size. Althoughthis condition shows a predilection for African-Amer-ican women, it is rarely reported covering the entire thehard palate. The most common location is the buccalmucosa.20
A blue nevus is an uncommon acquired melano-cytic macule of the skin or oral mucosa. It appearsblue or blue-black in color and is typically smallerthan 6 mm in size.21 Although blue nevi have apredilection for the palate, this diagnosis was ruledout based on the absence of blue coloration and thelesion’s large size.
Malignant mucosal melanoma must be included inany discussion of pigmented lesions of the oral mu-cosa, owing to the dismal prognosis associated withthis entity. It presents most commonly on the palateor maxillary gingiva,22 generally as an asymptomaticill defined brown or black macule, papule, or nodule,generally with uneven pigmentation. Although thecondition is rare, it is associated with a worse prog-nosis than cutaneous melanoma. The symmetry, welldefined borders, and even pigmentation of thepresent patient’s palatal pigmentation made this di-agnosis less likely.
DIAGNOSISAn incisional punch biopsy was performed under
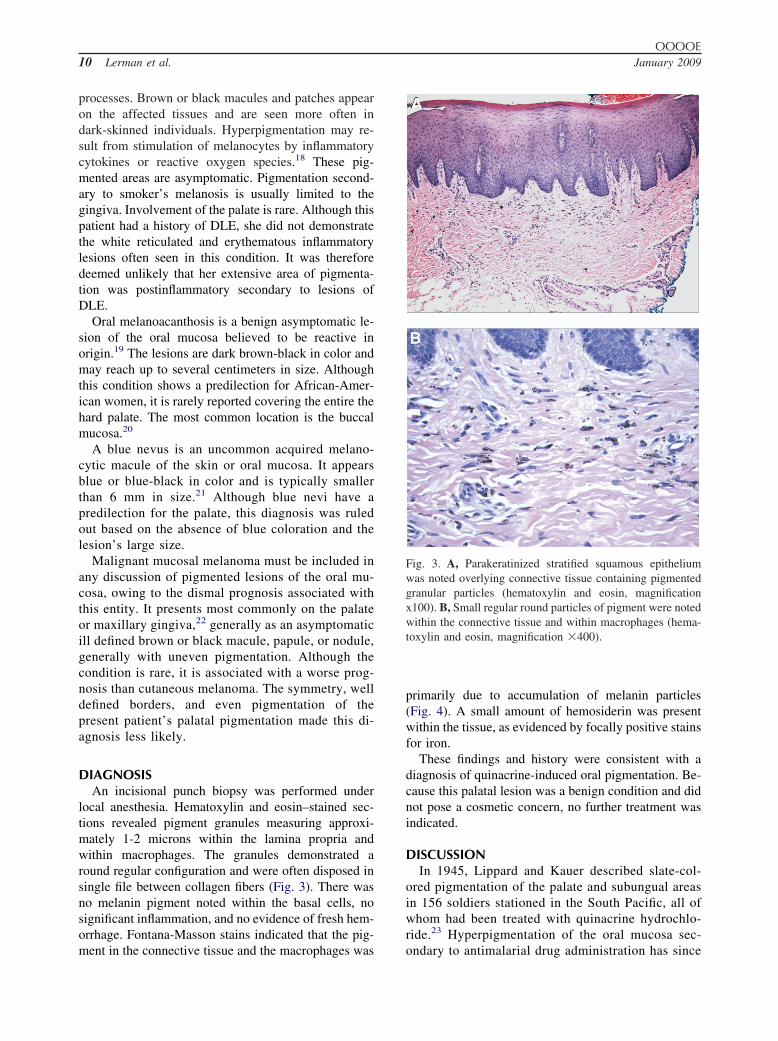
local anesthesia. Hematoxylin and eosin–stained sec-tions revealed pigment granules measuring approxi-mately 1-2 microns within the lamina propria andwithin macrophages. The granules demonstrated around regular configuration and were often disposed insingle file between collagen fibers (Fig. 3). There wasno melanin pigment noted within the basal cells, nosignificant inflammation, and no evidence of fresh hem-orrhage. Fontana-Masson stains indicated that the pig-
ment in the connective tissue and the macrophages wasprimarily due to accumulation of melanin particles(Fig. 4). A small amount of hemosiderin was presentwithin the tissue, as evidenced by focally positive stainsfor iron.
These findings and history were consistent with adiagnosis of quinacrine-induced oral pigmentation. Be-cause this palatal lesion was a benign condition and didnot pose a cosmetic concern, no further treatment wasindicated.
DISCUSSIONIn 1945, Lippard and Kauer described slate-col-
ored pigmentation of the palate and subungual areasin 156 soldiers stationed in the South Pacific, all ofwhom had been treated with quinacrine hydrochlo-ride.23 Hyperpigmentation of the oral mucosa sec-
Fig. 3. A, Parakeratinized stratified squamous epitheliumwas noted overlying connective tissue containing pigmentedgranular particles (hematoxylin and eosin, magnificationx100). B, Small regular round particles of pigment were notedwithin the connective tissue and within macrophages (hema-toxylin and eosin, magnification �400).
ondary to antimalarial drug administration has since

OOOOEVolume 107, Number 1 Lerman et al. 11
been reported by many others, typically restricted tothe hard palate.24 Classic presentation includes asharp line of demarcation between the hard and softpalates, as was seen in the present case.25 Quinacrinehas also been associated with discoloration of theskin; of note, our patient reported that the onset ofher cutaneous lesions was subsequent to initiation ofquinacrine therapy.
Among the numerous antimalarial medications im-plicated in discoloration of the oral tissues are chloro-quine, hydroxychloroquine, quinacrine, and amodia-quine.24 These agents all demonstrate antiinflammatoryproperties in addition to their antimalarial effects. Assuch, they are commonly used to treat not only malariabut also immune-mediated conditions, including rheu-matoid arthritis, lupus erythematosus, and other colla-gen vascular disorders.
Although early studies suggested that antimalarial-associated pigmentation was related to deposition ofhemosiderin,23 increased production of melanin iscurrently believed to be the responsible mecha-nism.12 Positive staining of the granules with theFontana Masson stain is consistent with this expla-nation. Antimalarial drugs have been found to stim-ulate melanocytes either directly and/or by elevatinglevels of androgens, which in turn stimulate melano-cytes. It is unclear why the pigmentation preferen-tially involves the palatal mucosa. Because thesemedications often are used to treat inflammatoryconditions, hemorrhage from inflammation may haveled previous investigators to believe hemosiderin tobe the source of the pigmentation.
Oral mucosal pigmentation secondary to quinacrine
Fig. 4. Histochemical stains confirmed the presence of mel-anin within the connective tissue (Fontana Masson stain,magnification �200).
administration is a benign condition; no intervention is
required once this diagnosis is rendered. The pigmen-tation can be expected to resolve within months ofdiscontinuation of the drug, although the discolorationin this particular case was not in an esthetic area andwas of little concern to the patient.
In summary, we present an example of quinacrine-induced oral pigmentation. The characteristic findingof slate-black pigmentation of the hard palate ex-tending to, but without involving, the soft palateshould immediately alert the clinician to the possi-bility of a medication-related condition. A thoroughmedical history is essential in arriving at the correctdiagnosis.
REFERENCES1. Dummett CO. Normal and locally induced oral pigmentations.
Int Dent J 1976;26:152-6.2. Maaser C, Kannengiesser K, Kucharzik T. Role of the melano-
cortin system in inflammation. Ann N Y Acad Sci 2006;1072:123-34.
3. Perusse R, MR. Oral pigmentation induced by Premarin. Cutis1991;48:61-4.
4. Lucky AW. Pigmentary abnormalities in genetic disorders. Der-matol Clin 1988;6:193-203.
5. Kitigawa. Peutz-Jeghers syndrome. Dermatol Clin 1995;13:127-33.
6. Gavren BA, LH, Cardo VA, Schmidt BL. Multiple pigmentedlesions of the lower lip. J Oral Maxillofac Surg 2002;60:438-45.
7. De Schepper S, Boucneau J, Lambert J, Messiaen L, NaeyaertJM. Pigment cell–related manifestations in neurofibromatosistype 1: an overview. Pigment Cell Res 2005;18:13-24.
8. Kim IS, Kim ER, Nam HJ, et al. Activating mutation of GS alphain McCune-Albright syndrome causes skin pigmentation by ty-rosinase gene activation on affected melanocytes. Horm Res1999;52:235-40.
9. Lin-Marq N, Borel C, Antonarakis SE. Peutz-Jeghers LKB1mutants fail to activate GSK-3beta, preventing it from inhibitingWnt signaling. Mol Genet Genomics 2005;273:184-96.
10. Ridgway HA, Sonnex TS, Kennedy CT, Millard PR, HendersonWJ, Gold SC. Hyperpigmentation associated with oral minocy-cline. Br J Dermatol 1982;107:95-102.
11. Cale AE, Freedman PD, Lumerman H. Pigmentation of thejawbones and teeth secondary to minocycline hydrochloride ther-apy. J Periodontol 1988;59:112-4.
12. Savage NW, BM, Adkins KF. Pigmentary changes in rat oralmucosa following antimalarial therapy. J Oral Pathol 1986;15:468-71.
13. Sakurai I, Skinsnes OK. Histochemistry of B663 pigmentation:ceroid-like pigmentation in macrophages. Int J Lepr Other My-cobact Dis 1977;45:343-54.
14. Carter RJ, Shuster S. Melanocyte-stimulating hormone—mi-metic action of the phenothiazines. J Pharm Pharmacol 1978;30:233-5.
15. Solomon S. POMC-derived peptides and their biological action.Ann N Y Acad Sci 1999;885:22-40.
16. Culora GA, Barnett N, Theaker JM. Artefacts in electron mi-croscopy: ultrastructural features of chrysiasis. J Pathol 1995;176:421-5.
17. Delage C, Lagace R, Huard J. Pseudocyanotic pigmentation ofthe skin induced by amiodarone: a light and electron microscopicstudy. Can Med Assoc J 1975;112:1205-8.
18. Sriwiriyanont P, Ohuchi A, Hachiya A, Visscher MO, Boissy
OOOOE12 Lerman et al. January 2009
RE. Interaction between stem cell factor and endothelin-1:effects on melanogenesis in human skin xenografts. Lab Invest2006;86:1115-25.
19. Goode RK, Crawford BE, Callihan MD, Neville BW. Oral mela-noacanthoma. Review of the literature and report of ten cases. OralSurg Oral Med Oral Pathol Oral Radiol Endod 1983;56:622-8.
20. Fornatora ML, Reich RF, Haber S, Solomon F, Freedman PD.Oral melanoacanthoma: a report of 10 cases, review of theliterature, and immunohistochemical analysis for HMB-45 reac-tivity. Am J Dermatopathol 2003;25:12-5.
21. Papanicolaou SJ, Pierrakou ED, Patsakas AJ. Intraoral blue ne-vus. Review of the literature and a case report. J Oral Med1985;40:32-5.
22. Prasad ML, Busam KJ, Patel SG, Hoshaw-Woodard S, Shah JP, HuvosAG. Clinicopathologic differences in malignant melanoma arising inoral squamous and sinonasal respiratory mucosa of the upper aerodi-
gestive tract. Arch Pathol Lab Med 2003;127:997-1002.23. Lippard VW, Kauer G. Pigmentation of the palate and subungualtissues associated with suppressive quinacrine hydrochloridetherapy. Am J Tropic Med 1945;25:469-471.
24. Kleinegger CL, HH, Finkelstein MW. Oral mucosal hyperpig-mentation secondary to antimalarial drug therapy. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2000;90:189-94.
25. Giansanti JS, TD, Olansky S. Oral mucosal pigmentation result-ing from antimalarial therapy. Oral Surg Oral Med Oral PatholOral Radiol Endod 1971;31:66-9.
Reprint reqeusts:
Dr. Mark A LermanOral Medicine, Infection, and ImmunityHarvard School of Dental Medicine188 Longwood AvenueBoston, MA 02115
[email protected]