Embed Size (px)
Citation preview

Pneumatic Retinopexy for GiantRetinal Tears
Alexander R. Irvine, MD, ]. Michael Lahey, MD
Background: New techniques adapted for vitrectomy surgery, including the useof silicone oil and perfluorocarbon liquids, have been applied very successfully to giantretinal tears. Most surgeons thus turn immediately to vitrectomy for all giant tears. Theauthors have found that patients with giant tears usually have such rapid flow of fluidfrom the vitreous to the aqueous that repeated paracenteses can be performed withoutshallowing the anterior chamber, thus allowing injection of sufficient gas into the vitreouscavity to unroll and tamponade the giant tear without the need for vitrectomy. Thismakes pneumatic retinopexy a feasible alternative for those selected fresh giant tearsthat have mobile flaps and extend less than 180 0
•
Methods: Five consecutive patients with giant retinal tears were treated with pneumatic retinopexy using paracentesis and two or more gas injections. They were followedat least 2 years.
Results: Four of the five tears were successfully reattached, although a new teardeveloped in one , and scleral buckling surgery was performed 11 months after thepneumatic retinopexy.
Conclusion: The authors conclude that pneumatic retinopexy is a reasonable alternative for selected patients with giant retinal tears.Ophthalmology 1994; 10 1:524-528
Because of the success of more recent vitrectomy techniques using silicone oil or perfluocarbon liquids to treatgiant retinal tears.l' many vitreoretinal surgeons haveforgotten that Nortorr':" described the use of intravitrealgas to unroll the flaps of giant tears and allow their treatment without buckling or vitrectomy before the onset ofmodern vitrectomy. Norton's technique required use ofan operating room and drainage of subretinal fluid. Thisproved quite successful for tears not more than 1800 thathad mobile flaps. When Hilton and colleaguesv' introduced pneumatic retinopexy for treatment of retinal detachment without the need for drainage or an operatingroom, they limited its use to tears not greater than I clockhour. That technique subsequentl y has been extended ina few cases to include tears up to 2.5 clock hours/ butthat has been the limit. Many surgeons have believed that
Originally received: May 13, 1993.Revision accepted: September I, 1993,
From the Departm ent of Ophthalmology, University of California, SanFrancisco.
Reprint requests to Alexander R. Irvine, MD, Department ofOphthalmology, K30 I, Box 0730, University of California, San Francisco, SanFrancisco, CA 94143.
524
one could not inject a bubble large enough to cover a teargreater than that size without draining subretinal fluid.Kre issig and associates" reported treating giant tears without drainage by injecting more expan sive perfluorocarbongases, after compressing the vitreous with either massageor an external balloon. Their technique was more complexand differed from that of Hilton and Grizzard, in thatthey injected gas through the tear behind the ora serrata,directing the needle into the retrohyaloid space under direct visualization. They monitored the central retinal artery and released fluid from the balloon as needed tomaintain patency of the arte ry.
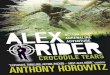
We have found that the majority of patients withfresh giant tears ha ve either high myopia or have traumatic avulsion of th e vitreous base. In either of thesesituation s, there is usually sufficient flow of fluid fromthe vitreous to the anterior chamber so an adequatevolume can be removed by paracentesis to avoid th eneed for drainage and thus combine the techniques described by Norton with those of Hilton and Grizzard"to treat giant tears by pneumatic retinopexy (Fig I) .Five consecutive pat ients with mobile giant tears notmore than 180 0 were treated in th is manner and followed a minimum of 2 years.

Irvine and Lahey . Pneumatic Retinopexy for Giant Retinal Tears
Figure 1. Fluid flow from the posterior to the anterior segment at the time of paracentesis in patients with giant retinal tears. A, in patients withhigh myopia or in patients with pseudophakia after posterior capsulotomy, there seems to be enough vitreous liquefaction for fluid to flow rapidlyfrom the vitreous cavity. B, with traumatic avulsion of the vitreous base, there seems to be direct communication between the subretinal space andthe aqueous.
Methods
All patients were admitted to the hospital. At bedside,after retrobulbar anesthetic injection, the eye was massaged a full 5 minutes. The patient then was positionedwith the tear dependent. A lid speculum was inserted, andthe conjunctiva was prepared with povidone-iodine (Betadine) solution and 0.4 to 0.6 ml of either sulfur hexafluoride or perfluoropropane gas was injected through thepars plana on the side opposite the tear. A paracentesisthen was performed with controlled aspiration using a 30gauge needle and a tuberculin syringe. The patient thenwas repositioned and a second similar injection was made,placing the needle into the first gas bubble. Elevated pressure usually required a second paracentesis. The patientthen was rolled so that the gas bubble passed posteriorlyover the macula and unrolled the flap, as described byothers.Y? For a temporal tear, this meant rolling the patient toward that temporal side and then around for 270°until the patient came to rest with the nasal side down.For a superior tear, the patient's legs were raised and anassisted reverse somersault was performed, bringing thepatient to a sitting position. A total of approximately 1.0ml of gas usually provided an adequate bubble to initiallyunroll and position the tear. After the tear had been unfolded, the patient was maintained in that position overnight-the patient's position was checked hourly. Pillowswere used to prevent turning while asleep. If the patientgot up, each time he laid down again, he turned in thesame manner, so that the bubble passed across the maculaand then pushed to unroll the flap. The following day,
the bubble had usually expanded adequately to cover thetear completely and flatten the detachment. If not, anadditional injection of gas was given. Laser then was performed to produce a triple row of confluent burns all alongthe posterior portion of the tear. This treatment was extended to the ora serrata at either end of the tear usingeither cryopexy or the indirect ophthalmoscope-mountedlaser.
Case Reports
Case 1. A 55-year-old man had a subluxated cataractouslens secondary to old blunt trauma in his left eye (Fig 2A). Tendays after intracapsular cataract extraction, anterior vitrectomy,and placement of an anterior chamber intraocular lens, he hada 2-day history of progressive field loss with loss of central vision.He had a tear extending from the 8:30 to the 11:30 position,with a torn "bucket-handle" avulsion of the vitreous base. Theedge of the tear was rolled tightly, but the rest of the flap wasfreely mobile. It appeared that a longstanding traumatic dialysishad been present, but had progressed to a large tear and symptomatic detachment only after the cataract extraction.
The patient responded well to pneumatic retinopexy, and 6years later his postoperative visual acuity remains 20/40.
Case 2. A 48-year-old man with myopia (-10 diopters)had a tear extending from the 10:30 to the 3:30 position in hisright eye (Fig 2B). The tear folded over the disc and maculawhen he was in an upright position, but it unfolded to show anattached macula when he was in the prone position.
The patient responded well to pneumatic retinopexy, and hisvisual acuity remained 20/25 after 3 years. However, at 3.5 years,
525
Ophthalmology Volume 101, Number 3, March 1994
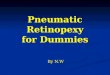
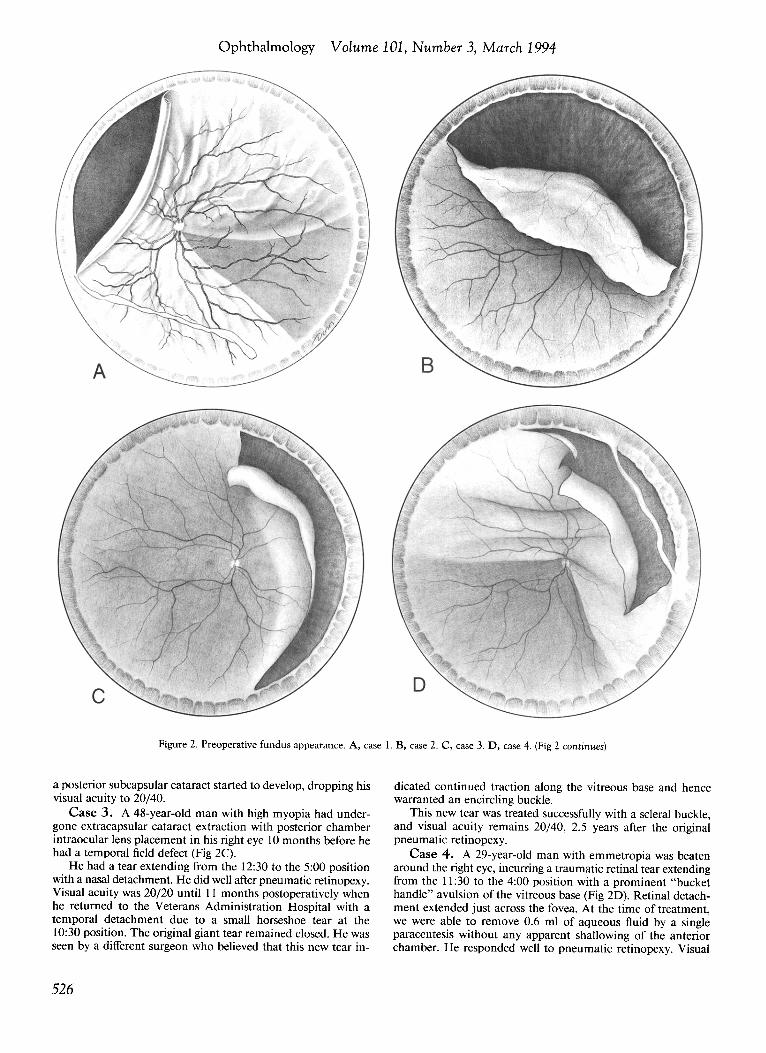
Figure 2. Preoperative fundus appearance. A, case 1. B, case 2. C, case 3. D, case 4. (Fig 2 continues)
a posterior subcapsular cataract started to develop , dropping hisvisual acuity to 20/40.
Case 3. A 48-year-old man with high myopia had undergone extracapsular cataract extraction with posterior chamberintraocular lens placement in his right eye 10 months before hehad a temporal field defect (Fig 2C).
He had a tear extending from the 12:30 to the 5:00 positionwith a nasal detachment. He did well after pneumatic retinopexy.Visual acuity was 20/20 until II months postoperatively whenhe returned to the Veterans Administration Hospital with atemporal detachment due to a small horseshoe tear at the10:30 position. The original giant tear remained closed. He wasseen by a different surgeon who believed that this new tear in-
526
dicated continued traction along the vitreous base and hencewarranted an encircling buckle.
This new tear was treated successfully with a scleral buckle,and visual acuity remains 20/40, 2.5 years after the originalpneumatic retinopexy.
Case 4. A 29-year-old man with emmetropia was beatenaround the right eye, incurring a traumatic retinal tear extendingfrom the II :30 to the 4:00 position with a prominent "buckethandle" avulsion of the vitreous base (Fig 20). Retinal detachment extended just across the fovea. At the time of treatment,we were able to remove 0.6 ml of aqueous fluid by a singleparacentesis without any apparent shallowing of the anteriorchamber. He responded well to pneumatic retinopexy. Visual
Irvine and Lahey· Pneumatic Retinopexy for Giant Retinal Tears
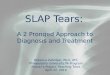
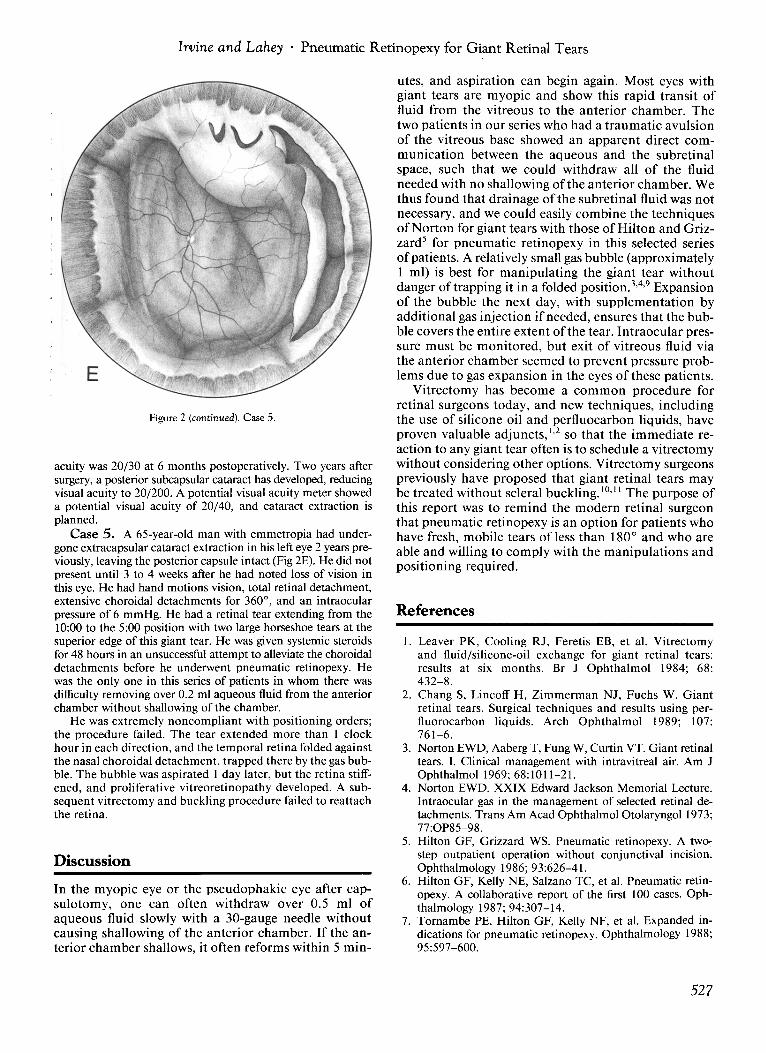
Figure 2 (continued). Case 5.
acuity was 20/30 at 6 months postoperatively. Two years aftersurgery, a posterior subcapsular cataract has developed, reducingvisual acuity to 20/200. A potential visual acuity meter showeda potential visual acuity of 20/40, and cataract extraction isplanned.
Case 5. A 65-year-old man with emmetropia had undergone extracapsular cataract extraction in his left eye 2 years previously, leaving the posterior capsule intact (Fig 2E). He did notpresent until 3 to 4 weeks after he had noted loss of vision inthis eye. He had hand motions vision, total retinal detachment,extensive choroidal detachments for 360 0
, and an intraocularpressure of 6 mmHg. He had a retinal tear extending from the10:00 to the 5:00 position with two large horseshoe tears at thesuperior edge of this giant tear. He was given systemic steroidsfor 48 hours in an unsuccessful attempt to alleviate the choroidaldetachments before he underwent pneumatic retinopexy. Hewas the only one in this series of patients in whom there wasdifficulty removing over 0.2 ml aqueous fluid from the anteriorchamber without shallowing of the chamber.
He was extremely noncompliant with positioning orders;the procedure failed. The tear extended more than I clockhour in each direction, and the temporal retina folded againstthe nasal choroidal detachment, trapped there by the gas bubble. The bubble was aspirated 1 day later, but the retina stiffened, and proliferative vitreoretinopathy developed. A subsequent vitrectomy and buckling procedure failed to reattachthe retina.
Discussion
In the myopic eye or the pseudophakic eye after capsulotomy, one can often withdraw over 0.5 ml ofaqueous fluid slowly with a 30-gauge needle withoutcausing shallowing of the anterior chamber. If the anterior chamber shallows, it often reforms within 5 min-
utes, and aspiration can begin again. Most eyes withgiant tears are myopic and show this rapid transit offluid from the vitreous to the anterior chamber. Thetwo patients in our series who had a traumatic avulsionof the vitreous base showed an apparent direct communication between the aqueous and the subretinalspace, such that we could withdraw all of the fluidneeded with no shallowing of the anterior chamber. Wethus found that drainage of the subretinal fluid was notnecessary, and we could easily combine the techniquesof Norton for giant tears with those of Hilton and Grizzard' for pneumatic retinopexy in this selected seriesof patients. A relatively small gas bubble (approximately1 ml) is best for manipulating the giant tear withoutdanger of trapping it in a folded position.Y? Expansionof the bubble the next day, with supplementation byadditional gas injection if needed, ensures that the bubble covers the entire extent of the tear. Intraocular pressure must be monitored, but exit of vitreous fluid viathe anterior chamber seemed to prevent pressure problems due to gas expansion in the eyes of these patients.
Vitrectomy has become a common procedure forretinal surgeons today, and new techniques, includingthe use of silicone oil and perfluocarbon liquids, haveproven valuable adjuncts.l' so that the immediate reaction to any giant tear often is to schedule a vitrectomywithout considering other options. Vitrectomy surgeonspreviously have proposed that giant retinal tears maybe treated without scleral buckling. 10,11 The purpose ofthis report was to remind the modern retinal surgeonthat pneumatic retinopexy is an option for patients whohave fresh, mobile tears of less than 1800 and who areable and willing to comply with the manipulations andpositioning required.
References
1. Leaver PK, Cooling RJ, Feretis EB, et al. Vitrectomyand fluid/silicone-oil exchange for giant retinal tears:results at six months. Br J Ophthalmol 1984; 68:432-8.
2. Chang S, Lincoff H, Zimmerman NJ, Fuchs W. Giantretinal tears. Surgical techniques and results using perfluorocarbon liquids. Arch Ophthalmol 1989; 107:761-6.
3. Norton EWD, Aaberg T, Fung W, Curtin VT. Giant retinaltears. 1. Clinical management with intravitreal air. Am JOphthalmol 1969; 68: 1011-21.
4. Norton EWD. XXIX Edward Jackson Memorial Lecture.Intraocular gas in the management of selected retinal detachments. Trans Am Acad Ophthalmol Otolaryngol 1973;77:0P85-98.
5. Hilton GF, Grizzard WS. Pneumatic retinopexy. A twostep outpatient operation without conjunctival incision.Ophthalmology 1986; 93:626-41.
6. Hilton GF, Kelly NE, Salzano TC, et al. Pneumatic retinopexy. A collaborative report of the first 100 cases. Ophthalmology 1987; 94:307-14.
7. Tornambe PE, Hilton GF, Kelly NF, et al. Expanded indications for pneumatic retinopexy. Ophthalmology 1988;95:597-600.
527

Ophthalmology Volume 101, Number 3, March 1994
8. Kreissig I, Lincoff H, Stanowsky A. The treatment of gianttear detachments using retrohyaloidal perfluorocarbon gaseswithout drainage or vitrectomy. Graefes Arch Clin ExpOphthalmol 1987; 225:94-8.
9. LincoffH. A small bubble technique for manipulating giantretinal tears. Ann Ophthalmol 1981; 13:241-3.
528
10. Hoffman ME, Sorr EM. Management of giant retinal tearswithout scleral buckling. Retina 1986; 6:197-204.
11. Kreiger AE, Lewis H. Management of giant retinal tearswithout scleral buckling. Use of radical dissection of thevitreous base and perfluoro-octane and intraocular tamponade. Ophthalmology 1992; 99:491-7.