Embed Size (px)
Citation preview
AJR:198, June 2012 W555
susceptible patients include those with hema-tologic malignancies, those undergoing che-motherapy for malignancy, and those under-going long-term corticosteroid therapy for inflammatory and connective tissue diseases such as Wegener granulomatosis and systemic lupus erythematosus [1].
Chest radiography is usually the initial imaging examination performed for patients with suspected pneumonia. However, the ra-diographic findings of PJP are nonspecific, and as many as one third of infected patients may have normal radiographic findings [3, 4]. Volumetric high-resolution (HRCT) may be indicated in the evaluation of immuno-compromised patients with normal or near-normal chest radiographic findings, and the results can be suggestive of PJP in the correct clinical situation. This pictorial essay de-scribes the clinical circumstances in which PJP should be considered and illustrates the spectrum of HRCT manifestations of PJP.
Clinical PresentationPJP usually develops in HIV-infected pa-
tients when the CD4+ cell count decreases to fewer than 200 cells/mm3 and particularly to fewer than 100 cells/mm3. Nevertheless, HIV-infected patients with CD4+ counts greater than 200 cells/mm3 account for 10–15% of cases of PJP [5]. The presentation of PJP in a patient with HIV infection typically is subacute, characterized by a gradual on-
Pneumocystis jiroveci Pneumonia: High-Resolution CT Findings in Patients With and Without HIV Infection
Jeffrey P. Kanne1 Donald R. Yandow
Cristopher A. Meyer
Kanne JP, Yandow DR, Meyer CA
1Department of Radiology, University of Wisconsin School of Medicine and Public Health, 600 Highland Ave, MC 3252, Madison WI 53792-3252. Address correspond-ence to J. P. Kanne ([email protected]).
Cardiopulmonar y Imaging • Pictor ia l Essay
CMEThis article is available for CME credit.
WEB This is a Web exclusive article.
AJR 2012; 198:W555–W561
0361–803X/12/1986–W555
© American Roentgen Ray Society
Pneumocystis jiroveci is an atypi-cal fungus that causes pneumo-nia in immunocompromised hu-man hosts, particularly those
with deficiency in cell-mediated immunity. P. jiroveci lives almost exclusively in the pul-monary alveoli, adhering to the alveolar epi-thelium. Intraalveolar macrophages serve as the primary host defense against P. jiroveci, and macrophage deficiency or dysfunction can lead to infection [1]. CD4+ T lympho-cytes, the count of which decreases in HIV infection, are essential to eradicating P. jir-oveci infection and contribute to inflamma-tory lung damage [2].
Bacterial pneumonia is the most common pulmonary infection among persons with AIDS, but despite widespread use of highly active antiretroviral therapy (HAART) and chemoprophylaxis, P. jiroveci pneumonia (PJP) is the most common opportunistic in-fection among persons with AIDS in the Unit-ed States. PJP occurs primarily among per-sons unaware that they have HIV infection [1] and is an AIDS-defining illness. In industri-alized countries, the incidence of PJP among persons without HIV infection exceeds that associated with HIV infection [1]. Neverthe-less, the incidence of PJP in solid organ and blood stem cell transplant recipients remains low because of widespread chemoprophylax-is. Most transplant-related PJP infections oc-cur in the early posttransplant period. Other
Keywords: high-resolution CT, HIV, immunocompromise, pneumonia, transplant
DOI:10.2214/AJR.11.7329
Received June 7, 2011; accepted after revision July 26, 2011.
J.P. Kanne is a paid consultant for Perceptive Informatics and PTC Therapeutics.
OBJECTIVE. The purpose of this essay is to review the spectrum of high-resolution CT findings of Pneumocystis jiroveci pneumonia in immunocompromised patients with and without HIV infection.
CONCLUSION. Pneumocystis jiroveci pneumonia is a common opportunistic infection affecting immunosuppressed patients. High-resolution CT may be indicated for evaluation of immunosuppressed patients with suspected pneumonia and normal chest radiographic find-ings. The most common high-resolution CT finding of Pneumocystis jiroveci pneumonia is diffuse ground-glass opacity. Consolidation, nodules, cysts, and spontaneous pneumothorax also can develop.
Kanne et al.CT of Pneumocystis jiroveci Pneumonia
Cardiopulmonary ImagingPictorial Essay

W556 AJR:198, June 2012
Kanne et al.
set of dry cough and dyspnea; in many cas-es, the onset period lasts as long as 1 month. Pulmonary auscultation is often unrevealing, but patients have signs of respiratory com-promise, including tachypnea, tachycardia, and cyanosis. Elevated serum lactate dehy-drogenase levels are highly sensitive but not specific for PJP. Because of the accompany-ing severe inflammatory response, PJP in pa-tients without HIV infection presents as an acute illness associated with severe hypoxia and results in rapid respiratory deterioration and respiratory failure requiring mechanical ventilation [6, 7].
High-Resolution CT FindingsAt HRCT, extensive ground-glass opacity
is the principal finding in PJP, reflecting ac-cumulation of intraalveolar fibrin, debris, and organisms (Figs. 1–4). A study involving 32 patients with AIDS-related PJP showed a cen-tral distribution of ground-glass opacity with relative peripheral sparing in 41% of patients, a mosaic pattern in 29%, and a diffuse distri-bution in 24% [8]. A predilection for the up-per lobes has also been described [3, 9]. In patients without HIV infection, the extent of ground-glass opacity is often greater [6].
With more advanced disease, septal lines (Fig. 5) with or without intralobular lines su-perimposed on ground-glass opacity (crazy paving) [8] (Fig. 6) and consolidation (Figs. 7 and 8) may develop [9, 10]. Lung consoli-dation is more common in patients without HIV infection and tends to develop more rapidly, reflecting pulmonary damage from the host immune response [11].
With widespread use of chemoprophylax-is, other HRCT manifestations of AIDS-re-lated PJP are more commonly reported. Pul-monary cysts (Figs. 9–12) of varying shape, size, and wall thickness occur in as many as one third of patients with PJP [3, 8, 9]. Cysts are associated with an increased fre-quency of spontaneous pneumothorax (Fig. 13), although spontaneous pneumothorax can occur in the absence of definable lung cysts [12]. Cysts may resolve after treatment and clearing of infection [9]. The incidence of pulmonary cysts has been reported to be lower in patients without HIV infection than in HIV-infected patients [6, 13].
Granulomatous inflammation occurs in approximately 5% of patients, usually ear-ly in the course of HIV infection while im-munodeficiency is more limited, and can be-come evident at HRCT as a solitary nodule or mass mimicking lung carcinoma or as mul-
tiple nodules ranging from a few millime-ters to more than 1 cm [10] (Fig. 14). How-ever, small nodules and tree-in-bud opacities are uncommon in patients with AIDS and PJP and usually indicate the presence of in-fectious bronchiolitis from other organisms [14]. Patients recovering from PJP may have residual interstitial fibrosis [4, 9, 10, 15]. In addition, although rare, interstitial fibrosis can occur in AIDS patients with low-grade chronic PJP, a condition termed chronic Pneumocystis pneumonia [16].
DiagnosisCulturing P. jiroveci is extremely difficult.
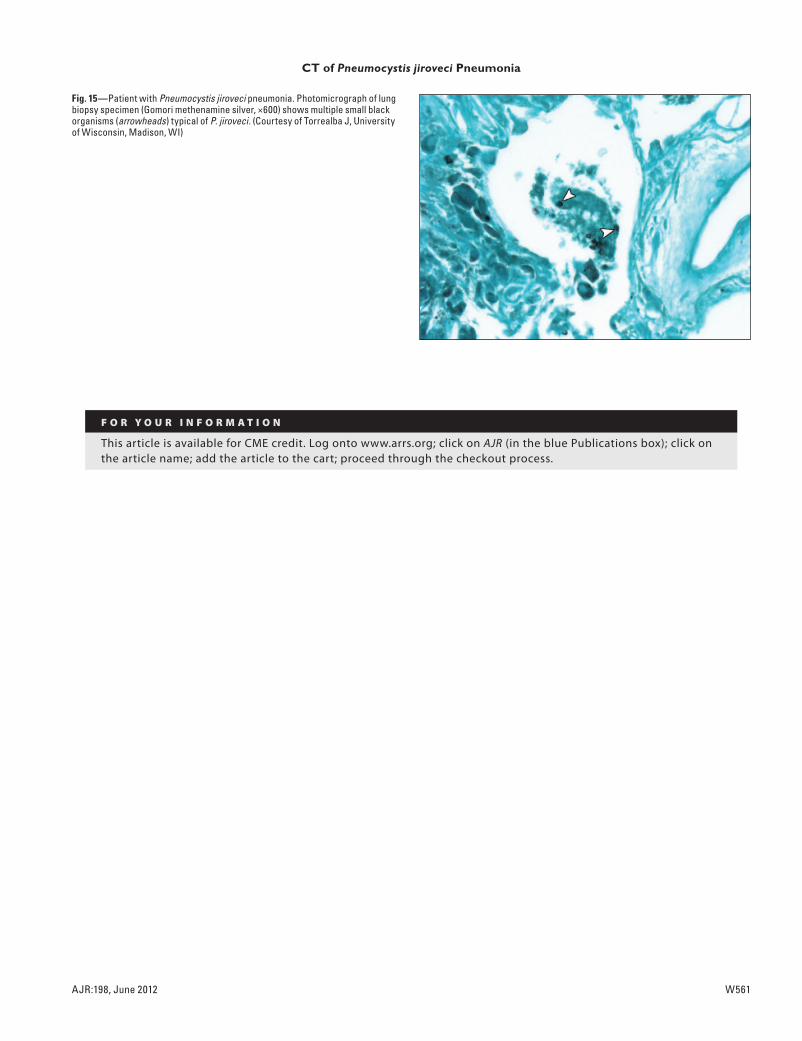
Confirmation of the diagnosis requires iden-tification of organisms in sputum or bron-choalveolar lavage fluid (Fig. 15). Monoclo-nal antibodies for detecting P. jiroveci are available and have a sensitivity greater than 90% for detecting P. jiroveci in induced spu-tum from HIV-infected patients. Confirma-tion of PJP can be difficult in patients with-out HIV infection because of the much lower burden of organisms [1]. Several polymerase chain reaction methods have been devel-oped. PCR has low sensitivity for confirming PJP but has a high negative predictive value. Currently, PCR is an investigative tool [1].
Treatment and PrognosisOral trimethoprim-sulfamethoxazole
(TMP-SMX) is first-line treatment of pa-tients with PJP. Second-line therapy for mild to moderate infection in patients who cannot tolerate TMP-SMX includes dapsone and trimethoprim, atovaquone, and clindamycin and primaquine. IV pentamidine can be used to treat patients with moderate to severe PJP who cannot tolerate TMP-SMX. By reduc-ing inflammatory lung injury, corticosteroids have been found to improve survival among HIV-infected patients when administered in the first 72 hours of treatment. The role of corticosteroids in the care of patients without HIV infection remains unclear. Despite ther-apy, the mortality of PJP remains high, espe-cially among patients without HIV infection. Patients with HIV infection have higher sur-vival rates, ranging from 86% to 92%; pa-tients without HIV infection have survival rates ranging from 51% to 80% [1].
ConclusionDespite widespread use of HAART and che-
moprophylaxis in industrialized countries, P. jiroveci remains a potentially life-threatening cause of pneumonia among immunocompro-
mised persons because of prolonged surviv-al of patients with hematologic malignancies, solid organ and blood stem cell transplant re-cipients, and patients undergoing chemothera-py and prolonged corticosteroid therapy. Fur-thermore, PJP can be the initial manifestation of AIDS in patients who do not have access to HAART or patients in whom HAART fails. HRCT plays a central role in evaluating im-munocompromised patients with new-onset lung disease. PJP should be strongly suspect-ed when any immunocompromised patient has respiratory tract signs and systems and exten-sive, patchy, upper-lobe-predominant ground-glass opacity on HRCT images.
References 1. Catherinot E, Lanternier F, Bougnoux ME, Lecuit
M, Couderc LJ, Lortholary O. Pneumocystis jir-
ovecii pneumonia. Infect Dis Clin North Am 2010;
24:107–138
2. Huang L, Morris A, Limper AH, Beck JM. An
official ATS workshop summary: recent advances
and future directions in Pneumocystis pneumonia
(PCP). Proc Am Thorac Soc 2006; 3:655–664
3. Kuhlman JE, Kavuru M, Fishman EK, Siegelman
SS. Pneumocystis carinii pneumonia: spectrum
of parenchymal CT findings. Radiology 1990;
175:711–714
4. Kuhlman JE. Imaging pulmonary disease in AIDS:
state of the art. Eur Radiol 1999; 9:395–408
5. Kovacs JA, Masur H. Evolving health effects of
Pneumocystis: one hundred years of progress in di-
agnosis and treatment. JAMA 2009; 301:2578–2585
6. Hardak E, Brook O, Yigla M. Radiological fea-
tures of Pneumocystis jirovecii pneumonia in im-
munocompromised patients with and without
AIDS. Lung 2010; 188:159–163
7. Mansharamani NG, Garland R, Delaney D,
Koziel H. Management and outcome patterns for
adult Pneumocystis carinii pneumonia, 1985 to
1995: comparison of HIV-associated cases to
other immunocompromised states. Chest 2000;
118:704–711
8. Fujii T, Nakamura T, Iwamoto A. Pneumocystis
pneumonia in patients with HIV infection: clini-
cal manifestations, laboratory findings, and radio-
logical features. J Infect Chemother 2007; 13:1–7
9. Boiselle PM, Crans CA Jr, Kaplan MA. The
changing face of Pneumocystis carinii pneumo-
nia in AIDS patients. AJR 1999; 172:1301–1309
10. Marchiori E, Muller NL, Soares Souza A Jr, Es-
cuissato DL, Gasparetto EL, Franquet T. Pulmo-
nary disease in patients with AIDS: high-resolu-
tion CT and pathologic findings. AJR 2005;
184:757–764
11. Tasaka S, Tokuda H, Sakai F, et al. Comparison of
clinical and radiological features of Pneumocystis
AJR:198, June 2012 W557
CT of Pneumocystis jiroveci Pneumonia
pneumonia between malignancy cases and ac-
quired immunodeficiency syndrome cases: a mul-
ticenter study. Intern Med 2010; 49:273–281
12. Chow C, Templeton PA, White CS. Lung cysts as-
sociated with Pneumocystis carinii pneumonia:
radiographic characteristics, natural history, and
complications. AJR 1993; 161:527–531
13. Kovacs JA, Hiemenz JW, Macher AM, et al.
Pneumocystis carinii pneumonia: a comparison
between patients with the acquired immunodefi-
ciency syndrome and patients with other immuno-
deficiencies. Ann Intern Med 1984; 100:663–671
14. Mayaud C, Parrot A, Cadranel J. Pyogenic bacte-
rial lower respiratory tract infection in human im-
munodeficiency virus–infected patients. Eur
Respir J Suppl 2002; 36:28s–39s
15. Gruden JF, Huang L, Turner J, et al. High-resolu-
tion CT in the evaluation of clinically suspected
Pneumocystis carinii pneumonia in AIDS pa-
tients with normal, equivocal, or nonspecific ra-
diographic findings. AJR 1997; 169:967–975
16. Wassermann K, Pothoff G, Kirn E, Fatkenheuer
G, Krueger GR. Chronic Pneumocystis carinii
pneumonia in AIDS. Chest 1993; 104:667–672
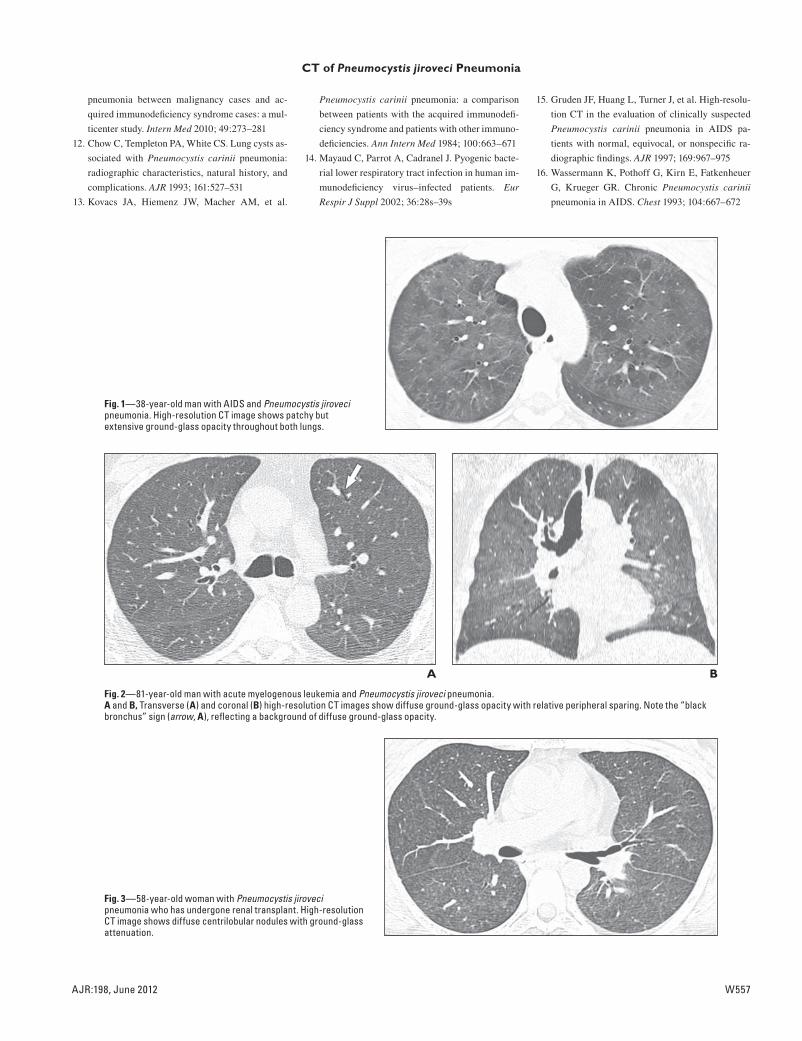
Fig. 1—38-year-old man with AIDS and Pneumocystis jiroveci pneumonia. High-resolution CT image shows patchy but extensive ground-glass opacity throughout both lungs.
A
Fig. 2—81-year-old man with acute myelogenous leukemia and Pneumocystis jiroveci pneumonia.A and B, Transverse (A) and coronal (B) high-resolution CT images show diffuse ground-glass opacity with relative peripheral sparing. Note the “black bronchus” sign (arrow, A), reflecting a background of diffuse ground-glass opacity.
B
Fig. 3—58-year-old woman with Pneumocystis jiroveci pneumonia who has undergone renal transplant. High-resolution CT image shows diffuse centrilobular nodules with ground-glass attenuation.
W558 AJR:198, June 2012
Kanne et al.
A
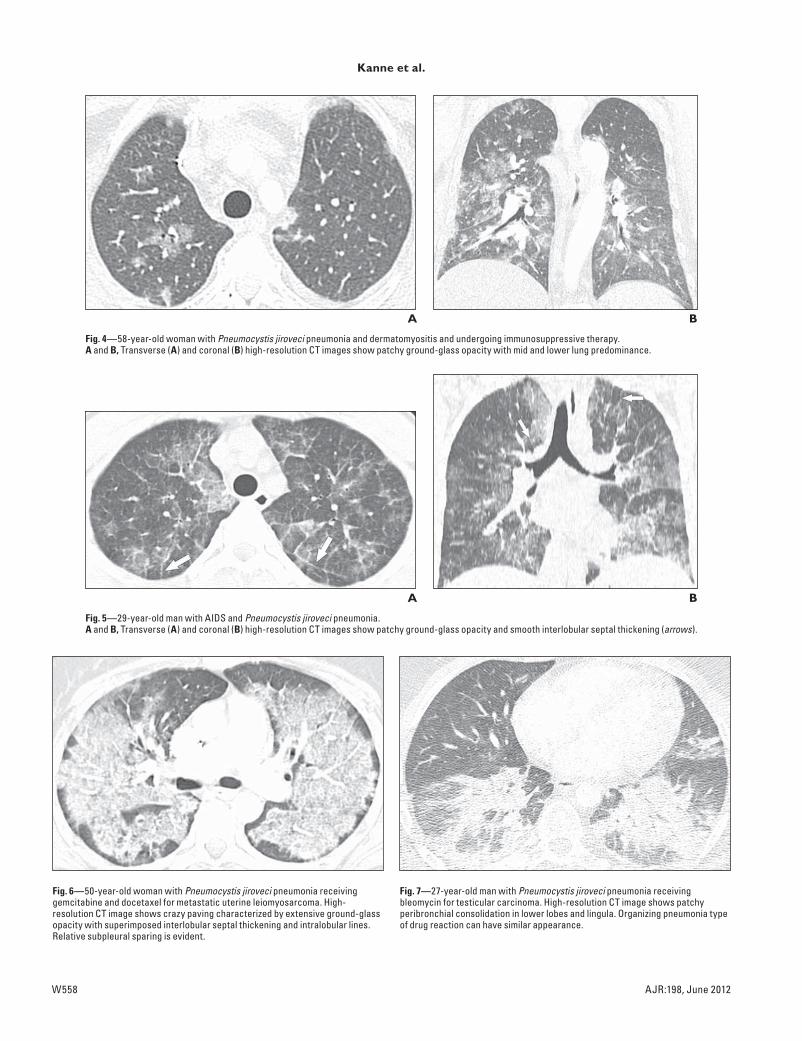
Fig. 4—58-year-old woman with Pneumocystis jiroveci pneumonia and dermatomyositis and undergoing immunosuppressive therapy.A and B, Transverse (A) and coronal (B) high-resolution CT images show patchy ground-glass opacity with mid and lower lung predominance.
B
A
Fig. 5—29-year-old man with AIDS and Pneumocystis jiroveci pneumonia.A and B, Transverse (A) and coronal (B) high-resolution CT images show patchy ground-glass opacity and smooth interlobular septal thickening (arrows).
B
Fig. 6—50-year-old woman with Pneumocystis jiroveci pneumonia receiving gemcitabine and docetaxel for metastatic uterine leiomyosarcoma. High-resolution CT image shows crazy paving characterized by extensive ground-glass opacity with superimposed interlobular septal thickening and intralobular lines. Relative subpleural sparing is evident.
Fig. 7—27-year-old man with Pneumocystis jiroveci pneumonia receiving bleomycin for testicular carcinoma. High-resolution CT image shows patchy peribronchial consolidation in lower lobes and lingula. Organizing pneumonia type of drug reaction can have similar appearance.

AJR:198, June 2012 W559
CT of Pneumocystis jiroveci Pneumonia
A
Fig. 8—67-year-old man with AIDS and Pneumocystis jiroveci pneumonia (PJP).A, High-resolution CT image shows patchy ground-glass opacity, greater in left lung.B, High-resolution CT image 17 days after A shows development of superimposed reticulation and formation of dense consolidation (arrow). Small pleural effusions (arrowheads) are not common finding in PJP and may be related to fluid resuscitation.
B
Fig. 9—41-year-old man with AIDS and Pneumocystis jiroveci pneumonia. High-resolution CT image shows scattered small foci of ground-glass opacity and consolidation with scattered small cysts (arrows).
Fig. 10—37-year-old man with AIDS and Pneumocystis jiroveci pneumonia. High-resolution CT image shows numerous thin-walled cysts (arrows) on background of patchy ground-glass opacity. Mild focal consolidation (arrowhead) is present in left lower lobe. (Courtesy of Sirajuddin A, Northwestern Memorial Hospital, Chicago, IL)
Fig. 11—54-year-old man with AIDS and Pneumocystis jiroveci pneumonia. High-resolution CT image shows extensive bilateral ground-glass opacity and single thin-walled cyst (arrow) in right upper lobe.
W560 AJR:198, June 2012
Kanne et al.
A
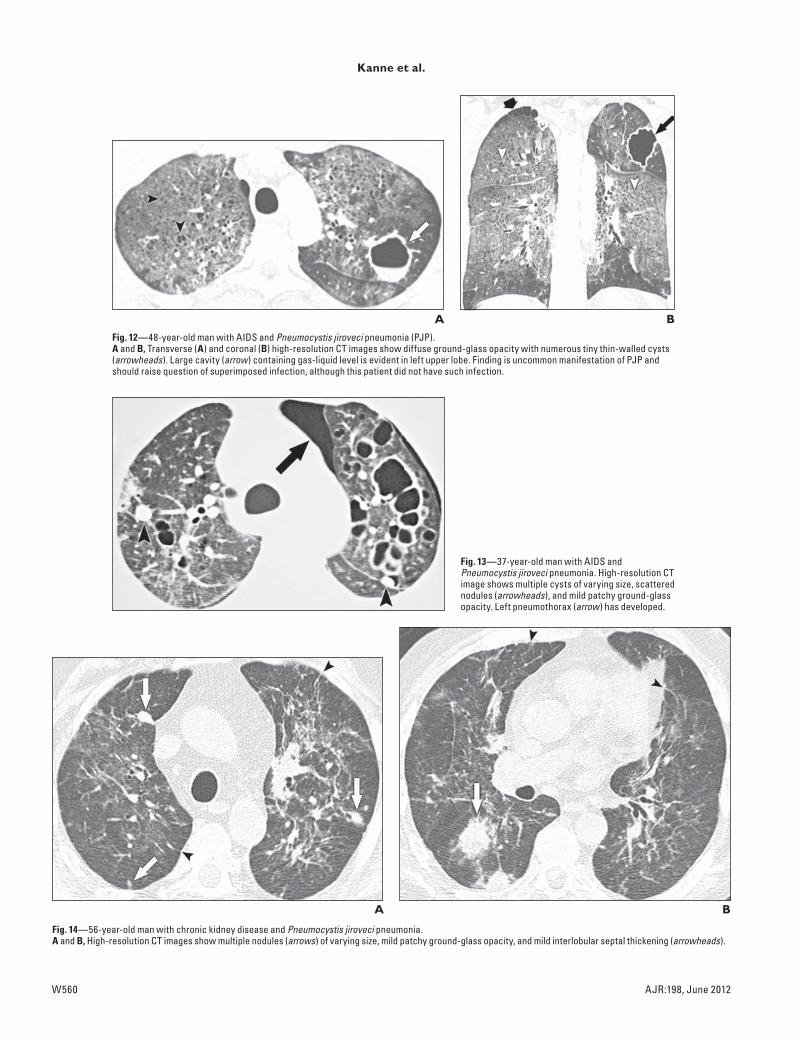
Fig. 12—48-year-old man with AIDS and Pneumocystis jiroveci pneumonia (PJP).A and B, Transverse (A) and coronal (B) high-resolution CT images show diffuse ground-glass opacity with numerous tiny thin-walled cysts (arrowheads). Large cavity (arrow) containing gas-liquid level is evident in left upper lobe. Finding is uncommon manifestation of PJP and should raise question of superimposed infection, although this patient did not have such infection.
B
Fig. 13—37-year-old man with AIDS and Pneumocystis jiroveci pneumonia. High-resolution CT image shows multiple cysts of varying size, scattered nodules (arrowheads), and mild patchy ground-glass opacity. Left pneumothorax (arrow) has developed.
A
Fig. 14—56-year-old man with chronic kidney disease and Pneumocystis jiroveci pneumonia.A and B, High-resolution CT images show multiple nodules (arrows) of varying size, mild patchy ground-glass opacity, and mild interlobular septal thickening (arrowheads).
B
AJR:198, June 2012 W561
CT of Pneumocystis jiroveci Pneumonia
Fig. 15—Patient with Pneumocystis jiroveci pneumonia. Photomicrograph of lung biopsy specimen (Gomori methenamine silver, ×600) shows multiple small black organisms (arrowheads) typical of P. jiroveci. (Courtesy of Torrealba J, University of Wisconsin, Madison, WI)
F O R Y O U R I N F O R M A T I O N
This article is available for CME credit. Log onto www.arrs.org; click on AJR (in the blue Publications box); click on the article name; add the article to the cart; proceed through the checkout process.





























