Embed Size (px)
Citation preview
1
PNEUMONIA
DR Badri Paudel
Department of Internal Medicine CHRC/GMC
n Infection of the alveoli, distal airways, and interstitium.
PNEUMONIA
4/22/12 2 Badri@GMC
Epidemiology
n Unclear! Few population-based statistics on the condition alone
n influenza for morbidity & mortality data ¨ influenza = 7th leading causes of death in the US
(2001) ¨ Age-adjusted death rate = 21.8 per 100,000 ¨ Mortality rate: 1-5% out-Pt, 12% In-Pt, 40% ICU ¨ Death rates increase with comorbidity and age ¨ Affects race and sex equally
4/22/12 3 Badri@GMC
n Microbial pathogens may enter the lungs by: - Direct extension from the mediastinum or subphrenic space
- Hematogenous seeding from an extrapulmonary focus
- Inhalation of microorganisms into the lower airways
- Aspiration of oropharyngeal contents
PATHOGENESIS
4/22/12 4 Badri@GMC
n Mechanical and structural - nose - cough/gag reflex - Airway branching - Mucociliary clearance - Normal oropharyngeal flora
n Cellular - Macrophages - Epithelial cells - Neutrophils
Humoral / Molecular / Inflammatory - IgG, IgA - Cytokines - Colony stimulating factors
HOST DEFENSES
4/22/12 5 Badri@GMC 4/22/12 6 Badri@GMC
2
4/22/12 7 Badri@GMC 4/22/12 8 Badri@GMC
4/22/12 9 Badri@GMC 4/22/12 10 Badri@GMC
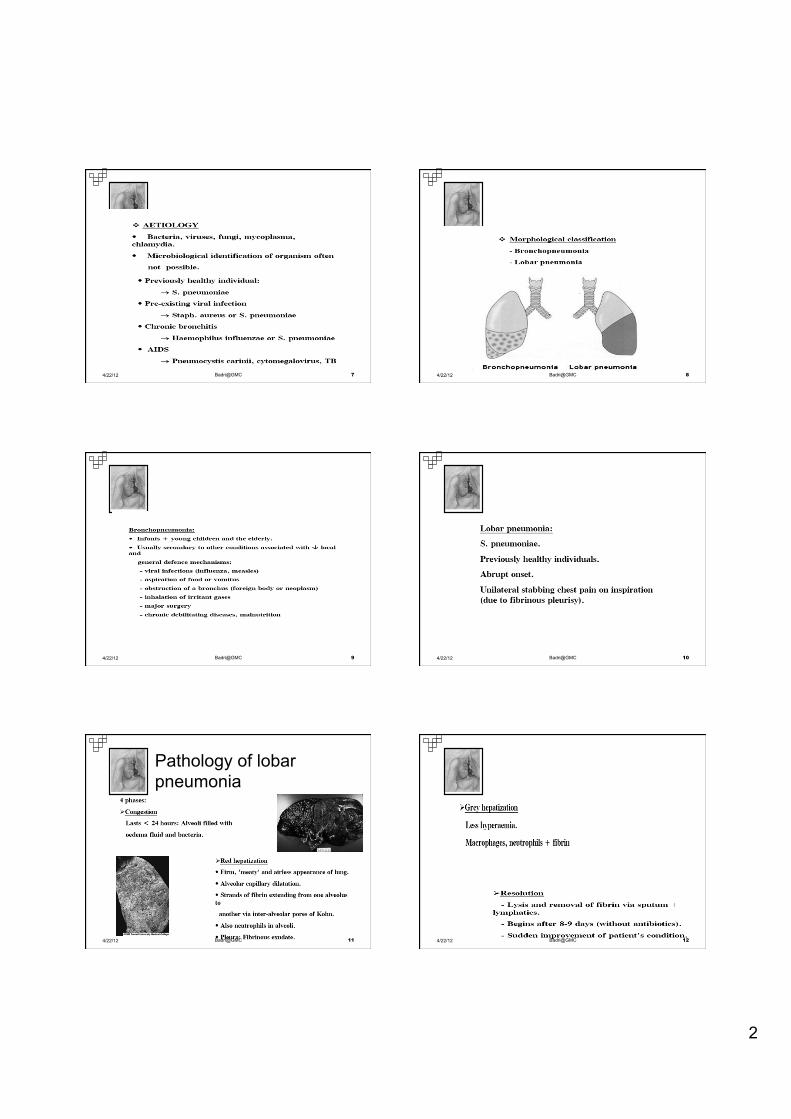
Pathology of lobar pneumonia
4/22/12 11 Badri@GMC 4/22/12 12 Badri@GMC
3
PATHOLOGY
BRONCHOPNEUMONIA
n Patchy consolidation in 1 or more lobes
4/22/12 13 Badri@GMC
PATHOLOGY
INTERSTITIAL PNEUMONIA
n Inflammatory process involving the interstitium, alveolar walls and connective tissues
4/22/12 14 Badri@GMC
PATHOLOGY
MILIARY PNEUMONIA
n Numerous discrete lesions of hematogenous spread
4/22/12 15 Badri@GMC
n Community acquired pneumonia (CAP)
n Nosocomial Pneumonia - Health Care-Associated Pneumonia (HCAP) /“
- Hospital-Acquired Pneumonia (HAP) - Ventilator-Associated pneumonia (VAP)
CLASSIFICATION
4/22/12 16 Badri@GMC
n Widespread use of potent antibiotics n Early transfer to home/low-acuity care n Increased use of outpatient IV antibiotic therapy n General aging of the population n More extensive immunomodulatory therapies
RISK FACTORS FOR MDR PATHOGENS
4/22/12 17 Badri@GMC
CAP
n Infection of the lung parenchyma in a person who is not hospitalized or living in a long-term care facility for ≥ 2 weeks
n 5.6 million cases annually in the U.S. n Estimated total annual cost of health care
= $8.4 billion n Most common pathogen = S. pneumo
(60-70% of CAP cases)
4/22/12 18 Badri@GMC
4
“Nosocomial” Pneumonia
n Healthcare-associated pneumonia (HCAP) ¨ Patients who were hospitalized in an acute care
hospital for two or more days within 90 days of the infection; resided in a nursing home or LTC facility; received recent IV abx, chemotherapy, or wound care within the past 30 days of the current infection; or attended a hospital or hemodialysis clinic
4/22/12 19 Badri@GMC
“Nosocomial” Pneumonia
n Hospital-acquired pneumonia (HAP) ¨ Occurs 48 hours or more after admission,
which was not incubating at the time of admission
n Ventilator-associated pneumonia (VAP) ¨ Arises more than 48-72 hours after
endotracheal intubation
4/22/12 20 Badri@GMC
COMMUNITY-ACQUIRED PNEUMONIA
MICTROBIAL CAUSES OF COMMUNITY-ACQUIRED PNEUMONIA, BY SITE OF CARE
Hospitalization Patients
Outpatients Non-ICU ICU Streptococcus pneumoniae S. pneumoniae S. pneumoniae Mycoplasma pneumoniae M. pneumoniae Staphylococcus aereus Haemophilus influenzae Chlamydophila Legionella spp. C. Pneumoniae pneumoniae Gram-negative bacilli Respiratory viruses H. influenzae H. influenzae Legionella spp. Respiratory viruses
4/22/12 22 Badri@GMC
• Streptococcus pneumoniae 20- 60 %
• Haemophilus influenza 3- 10
• Chlamydea pneumoniae 5- 17
• Vírus 2- 15
• anaeróbes 6- 10
• gram - 3- 10
• S. Aureus 3- 5
• L. Pneumophila 2- 8
• M. Catarrhalis 1- 3
4/22/12 23 Badri@GMC
EPIDEMIOLOGIC FACTORS SUGGESTING POSSIBLE CAUSES OF COMMUNITY-ACQUIRED PNEUMONIA
Factor Possible Pathogen(s) Alcoholism Streptococcus pneumoniae, oral anaerobes, Klebsiella pneumoniae, Acinetobacter spp., Mycobacterium tuberculosis COPD and/or smoking Haemophilus influenzae, Pseudomonas aeruginosa, Legionella spp., S pneumoniae Moraxella catarrhalis, Chlamydophila pneumoniae Structural lung disease P. aeruginosa, Burkholderia cepacia, Staphy- lococcus aureus Dementia stroke, decreased Oral anaerobes, gram-negative enteric bacteria level of conciousness Lung abscess CA_MRSA, oral anaerobes, endemic fungi, M. tuberculosis, atypical mycobacteria
4/22/12 24 Badri@GMC
5
Stay in hotel or on cruise Legionella spp, ship in previous 2 weeks Local influenza activity Influenza virus, 5. pneumoniae, S. aureus Exposure to bats or birds H. capsulatum Exposure to birds Chlamydophila psittaci Exposure to rabbits Francisella tularensis Exposure to sheep, goats, Coxiella burnetii parturient cats
4/22/12 25 Badri@GMC
TEN LEADING CAUSES OF MORBIDITY Rate/100,000 Population PHILIPPINES, 1999
TEN LEADING CAUSES OF MORBIDITY Rate/100,000 Population PHILIPPINES, 1999
Cause Number Rate 1. Diarrheas 908,454 1189.9 2. Bronchitis/Bronchiolitis 717,214 939.4
3. Pneumonia 693,334 908.1 4. Influenza 514,198 673.5 5. Hypertension 208,248 272.8 6. T.B. Respiratory 144,932 189.8 7. Malaria 68,155 89.3 8. Diseases of the Heart 63,167 82.7 9. Chickenpox 35,699 46.8
10. Typhoid Fever 17,675 23.1
Source: FHSIS Annual Report 1999 4/22/12 26 Badri@GMC
TEN LEADING CAUSES OF MORTALITY Number and Rate/100,000 Population PHILIPPINES, 1997
CAUSES NUMBER RATE* 1. Diseases of the Heart 49,962 69.8 2. Diseases of the Vascular System 38,693 54.1 3. Pneumonia 30,811 43.1 4. Accidents 28,563 39.9 5. Malignant Neoplasm 26,842 37.5 6. Tuberculosis, All Forms 23,056 32.2 7. Chronic Obstructive Pulmonary Diseases and Allied Condition 11,807 16.5 8. Other Diseases of the Respiratory System 6,961 9.7 9. Diabetes Mellitus 6,749 9.4 10. Nephritis, Nephrotic Syndrome and Nephrosis 6,704 9.4 Source: Philippine Health Statistics 1997
4/22/12 27 Badri@GMC
n Alcoholism n Asthma n Immunosuppression n Institutionalization n Age > 70 years n Dementia n Seizure disorders n Tobacco smoking n Chronic obstructive pulmonary disease (COPD)
RISK FACTORS FOR CAP
4/22/12 28 Badri@GMC
Penicillin-resistant and drug-resistant pneumococci Age > 65 yr B-Lactam therapy within the past 3 mo Alcoholism Immune-suppressive illness Multiple medical comorbidities Exposure to a child in a day care center Enteric gram-negatives Residence in a nursing home Underlying cardiopulmonary disease Multiple medical comorbidities Recent antibiotic therapy Pseudomonas aeruginosa Structural lung disease (bronchiectasis) Corticosteroid therapy (> 10 mg of prednisone per day) Broad-spectrum antibiotic therapy for > 7 d in the past month Malnutrition
Factores que aumentam o risco de infecção por agentes específicos
In AJCCRM- ATS Guidelines 4/22/12 29 Badri@GMC
n May vary from indolent to fulminant; from mild to fatal n Fever n Tachycardia n Chills and/or sweats n Productive or non-productive cough n Dyspnea (occasionally) n Pleuritic chest pain (if pleura is involved)
n Fatigue, headache, myalgias
CLINICAL MANIFESTATIONS
4/22/12 30 Badri@GMC
6
n Increased RR n Use of accessory muscles of respiration n Increased tactile fremitus, dull percussion note for
consolidation n Decreased tactile fremitus, flat percussion note for
effusion n Crackles, bronchial breath sounds on auscultation
PHYSICAL FINDINGS
4/22/12 31 Badri@GMC
Non infectious causes of fever and pulmonary infiltrates that may mimic
CAP
n Pulmonary edema n Pulmonary infarction n Acute respiratory distress syndrome (ARDS) n Pulmonary hemorrhage n Lung cancer/metastatic cancer n Atelectasis n Radiation pneumonitis n Drug reactions involving the lung n Extrinsic allergic alveolitis n Pulmonary vasculitis n Pulmonary eosinophilia n Bronchiolitis obliterans and organizing pneumonia 4/22/12 32 Badri@GMC
n No particular clinical symptom/physical finding is sufficiently sensitive or specific to confirm/exclude CAP
n Sensitivity of history and PE- 58% n Specificity of history and PE- 67% n Chest radiography is necessary to help
differentiate CAP from other conditions
DIAGNOSIS
4/22/12 33 Badri@GMC
ETIOLOGY
TYPICAL n S. pneumoniae n H. Influenzae n S. aureus n K. pneumoniae n P. aeruginosa
ATYPICAL n M. pneumoniae n C. pneumoniae n Legionella spp. n Respiratory viruses
4/22/12 34 Badri@GMC
Diagnosis, Empiric Management and Prevention of COMMUNITY-ACQUIRED PNEUMONIA In Immunocompetent Adult
n Cough
n Tachycardia CR > 100
n Tachypnea RR > 20
n Fever T >37.8C
n At least one abnormal chest findings - diminished breath sounds, rhonchi, crackles or wheeze
n New x-ray infiltrate with no clear alternative such as lung cancer or pulmonary edema
CRITERIA FOR PNEUMONIA
4/22/12 36 Badri@GMC
7
Clinical Diagnosis: CXR n Demonstrable infiltrate by CXR or other imaging
technique ¨ Establish Dx and presence of complications (pleural
effusion, multilobar disease) ¨ CXR: classically thought of as the gold standard
n May not be possible in some outpatient settings. n Assess severity of disease and presence of
complication n Suggest possible etiology
4/22/12 37 Badri@GMC 4/22/12 38 Badri@GMC
Consolidation Rt lower lobe
4/22/12 39 Badri@GMC 4/22/12 40 Badri@GMC
Atypical Pneumonia
4/22/12 41 Badri@GMC 4/22/12 42 Badri@GMC
8
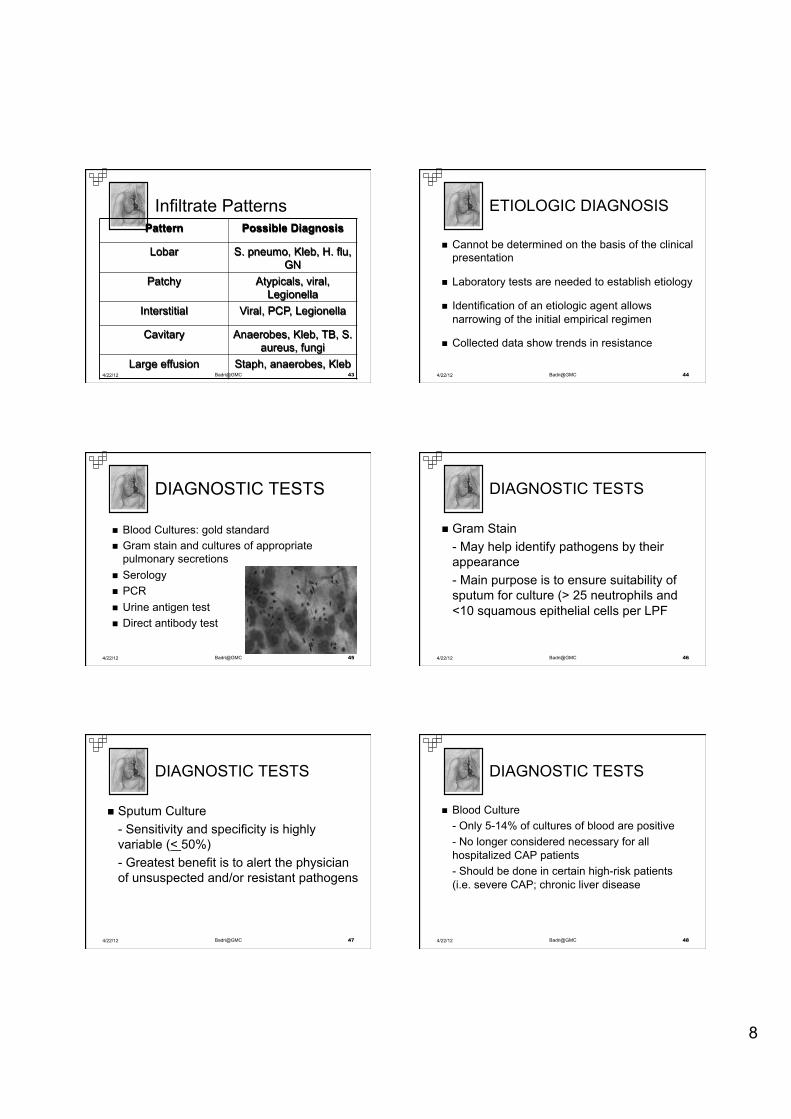
Infiltrate Patterns Pattern Possible Diagnosis
Lobar S. pneumo, Kleb, H. flu, GN
Patchy Atypicals, viral, Legionella
Interstitial Viral, PCP, Legionella
Cavitary Anaerobes, Kleb, TB, S. aureus, fungi
Large effusion Staph, anaerobes, Kleb 4/22/12 43 Badri@GMC
n Cannot be determined on the basis of the clinical presentation
n Laboratory tests are needed to establish etiology
n Identification of an etiologic agent allows narrowing of the initial empirical regimen
n Collected data show trends in resistance
ETIOLOGIC DIAGNOSIS
4/22/12 44 Badri@GMC
DIAGNOSTIC TESTS
n Blood Cultures: gold standard n Gram stain and cultures of appropriate
pulmonary secretions n Serology n PCR n Urine antigen test n Direct antibody test
4/22/12 45 Badri@GMC
n Gram Stain - May help identify pathogens by their appearance - Main purpose is to ensure suitability of sputum for culture (> 25 neutrophils and <10 squamous epithelial cells per LPF
DIAGNOSTIC TESTS
4/22/12 46 Badri@GMC
n Sputum Culture - Sensitivity and specificity is highly variable (< 50%) - Greatest benefit is to alert the physician of unsuspected and/or resistant pathogens
DIAGNOSTIC TESTS
4/22/12 47 Badri@GMC
n Blood Culture - Only 5-14% of cultures of blood are positive - No longer considered necessary for all hospitalized CAP patients - Should be done in certain high-risk patients (i.e. severe CAP; chronic liver disease
DIAGNOSTIC TESTS
4/22/12 48 Badri@GMC
9
n Antigen tests - Two commercially available tests detect pneumococcal and Legionella antigens in urine - Sensitivity and specificity are high for both tests - Can detect antigen even after the initiation of appropriate antibiotic therapy - Limited availability
DIAGNOSTIC TESTS
4/22/12 49 Badri@GMC
n Must take into consideration diminishing health care resources and rising costs of treatment
n Decision to where a patient should be managed is sometimes difficult
n Use of objective tools that assess risk of adverse outcomes and severity of the disease (i.e. PSI; CURB-65)
SITE OF CARE DECISION
4/22/12 50 Badri@GMC
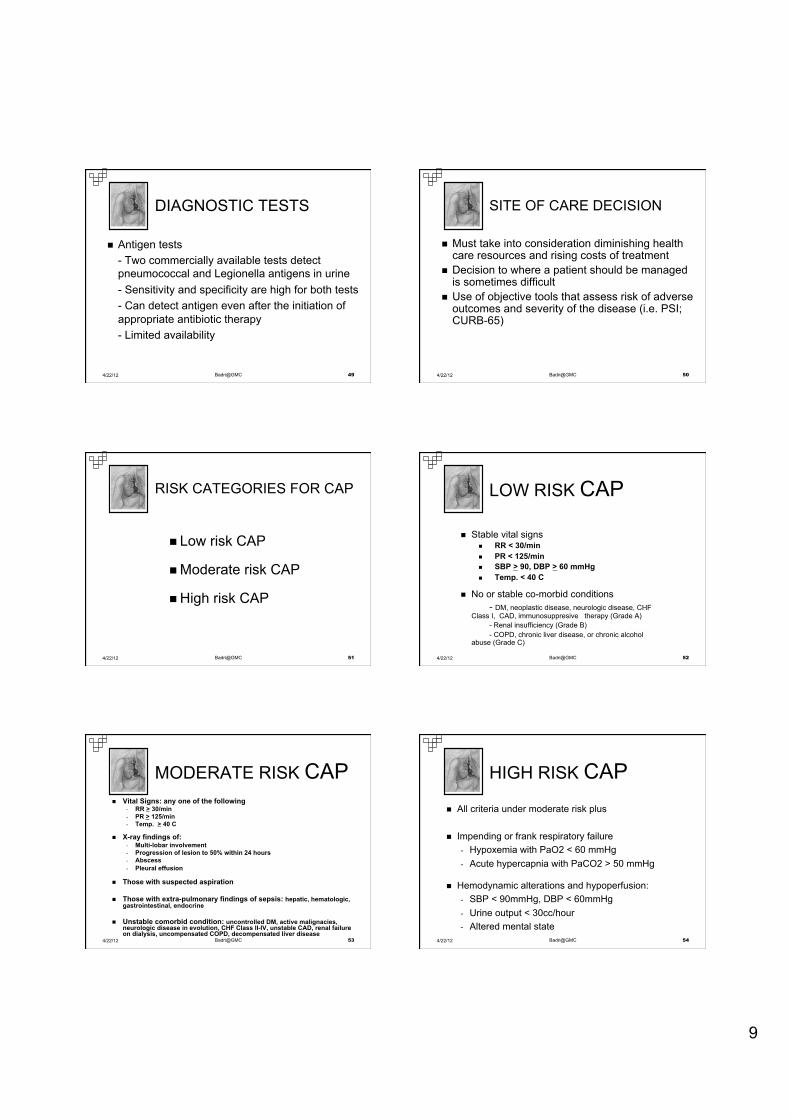
n Low risk CAP
n Moderate risk CAP
n High risk CAP
RISK CATEGORIES FOR CAP
4/22/12 51 Badri@GMC
n Stable vital signs n RR < 30/min n PR < 125/min n SBP > 90, DBP > 60 mmHg n Temp. < 40 C
n No or stable co-morbid conditions - DM, neoplastic disease, neurologic disease, CHF Class I, CAD, immunosuppresive therapy (Grade A) - Renal insufficiency (Grade B) - COPD, chronic liver disease, or chronic alcohol abuse (Grade C)
LOW RISK CAP
4/22/12 52 Badri@GMC
n Vital Signs: any one of the following - RR > 30/min - PR > 125/min - Temp. > 40 C
n X-ray findings of: - Multi-lobar involvement - Progression of lesion to 50% within 24 hours - Abscess - Pleural effusion
n Those with suspected aspiration
n Those with extra-pulmonary findings of sepsis: hepatic, hematologic, gastrointestinal, endocrine
n Unstable comorbid condition: uncontrolled DM, active malignacies, neurologic disease in evolution, CHF Class II-IV, unstable CAD, renal failure on dialysis, uncompensated COPD, decompensated liver disease
MODERATE RISK CAP
4/22/12 53 Badri@GMC
n All criteria under moderate risk plus
n Impending or frank respiratory failure - Hypoxemia with PaO2 < 60 mmHg - Acute hypercapnia with PaCO2 > 50 mmHg
n Hemodynamic alterations and hypoperfusion: - SBP < 90mmHg, DBP < 60mmHg - Urine output < 30cc/hour - Altered mental state
HIGH RISK CAP
4/22/12 54 Badri@GMC
10
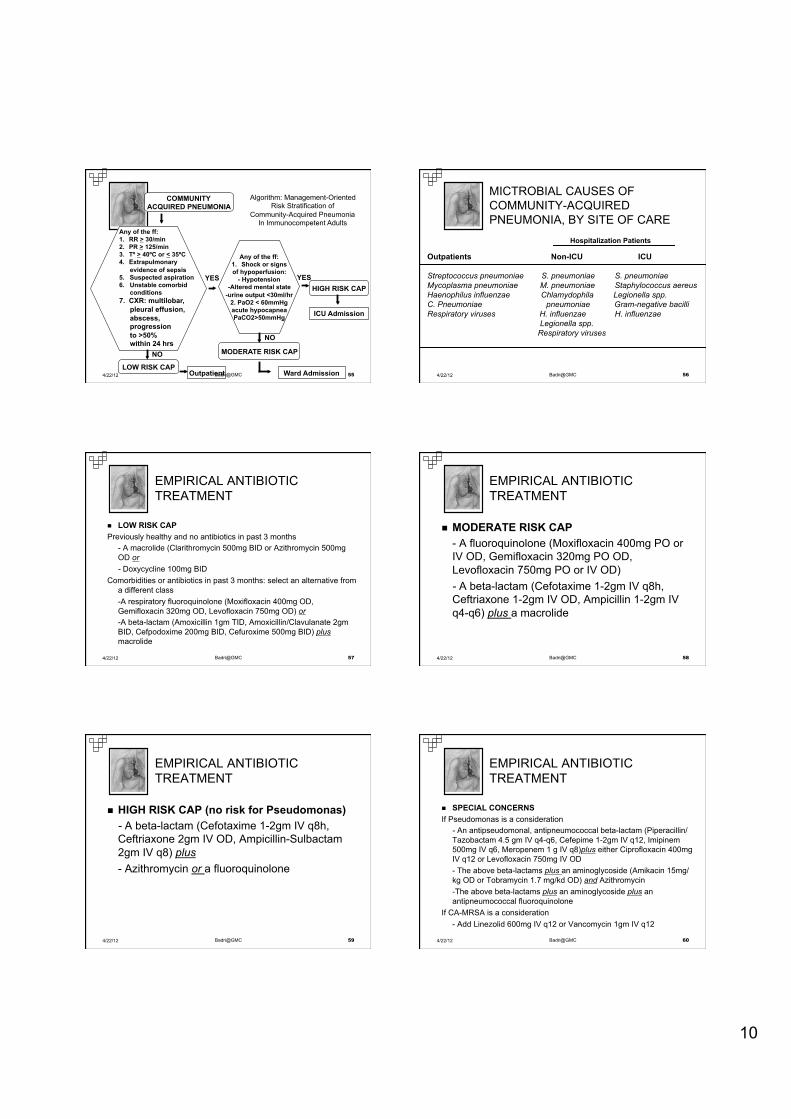
Any of the ff: 1. RR > 30/min 2. PR > 125/min 3. Tº > 40ºC or < 35ºC 4. Extrapulmonary
evidence of sepsis 5. Suspected aspiration 6. Unstable comorbid
conditions 7. CXR: multilobar,
pleural effusion, abscess, progression to >50% within 24 hrs
Any of the ff: 1. Shock or signs of hypoperfusion:
- Hypotension -Altered mental state
-urine output <30ml/hr 2. PaO2 < 60mmHg acute hypocapnea PaCO2>50mmHg
COMMUNITY ACQUIRED PNEUMONIA
LOW RISK CAP
MODERATE RISK CAP
HIGH RISK CAP
Outpatient Ward Admission
ICU Admission
YES YES
NO
NO
Algorithm: Management-Oriented Risk Stratification of
Community-Acquired Pneumonia In Immunocompetent Adults
4/22/12 55 Badri@GMC
MICTROBIAL CAUSES OF COMMUNITY-ACQUIRED PNEUMONIA, BY SITE OF CARE
Hospitalization Patients
Outpatients Non-ICU ICU Streptococcus pneumoniae S. pneumoniae S. pneumoniae Mycoplasma pneumoniae M. pneumoniae Staphylococcus aereus Haenophilus influenzae Chlamydophila Legionella spp. C. Pneumoniae pneumoniae Gram-negative bacilli Respiratory viruses H. influenzae H. influenzae Legionella spp. Respiratory viruses
4/22/12 56 Badri@GMC
n LOW RISK CAP Previously healthy and no antibiotics in past 3 months
- A macrolide (Clarithromycin 500mg BID or Azithromycin 500mg OD or - Doxycycline 100mg BID
Comorbidities or antibiotics in past 3 months: select an alternative from a different class -A respiratory fluoroquinolone (Moxifloxacin 400mg OD, Gemifloxacin 320mg OD, Levofloxacin 750mg OD) or -A beta-lactam (Amoxicillin 1gm TID, Amoxicillin/Clavulanate 2gm BID, Cefpodoxime 200mg BID, Cefuroxime 500mg BID) plus macrolide
EMPIRICAL ANTIBIOTIC TREATMENT
4/22/12 57 Badri@GMC
n MODERATE RISK CAP - A fluoroquinolone (Moxifloxacin 400mg PO or IV OD, Gemifloxacin 320mg PO OD, Levofloxacin 750mg PO or IV OD) - A beta-lactam (Cefotaxime 1-2gm IV q8h, Ceftriaxone 1-2gm IV OD, Ampicillin 1-2gm IV q4-q6) plus a macrolide
EMPIRICAL ANTIBIOTIC TREATMENT
4/22/12 58 Badri@GMC
n HIGH RISK CAP (no risk for Pseudomonas) - A beta-lactam (Cefotaxime 1-2gm IV q8h, Ceftriaxone 2gm IV OD, Ampicillin-Sulbactam 2gm IV q8) plus - Azithromycin or a fluoroquinolone
EMPIRICAL ANTIBIOTIC TREATMENT
4/22/12 59 Badri@GMC
n SPECIAL CONCERNS If Pseudomonas is a consideration
- An antipseudomonal, antipneumococcal beta-lactam (Piperacillin/Tazobactam 4.5 gm IV q4-q6, Cefepime 1-2gm IV q12, Imipinem 500mg IV q6, Meropenem 1 g IV q8)plus either Ciprofloxacin 400mg IV q12 or Levofloxacin 750mg IV OD - The above beta-lactams plus an aminoglycoside (Amikacin 15mg/kg OD or Tobramycin 1.7 mg/kd OD) and Azithromycin -The above beta-lactams plus an aminoglycoside plus an antipneumococcal fluoroquinolone
If CA-MRSA is a consideration - Add Linezolid 600mg IV q12 or Vancomycin 1gm IV q12
EMPIRICAL ANTIBIOTIC TREATMENT
4/22/12 60 Badri@GMC
11
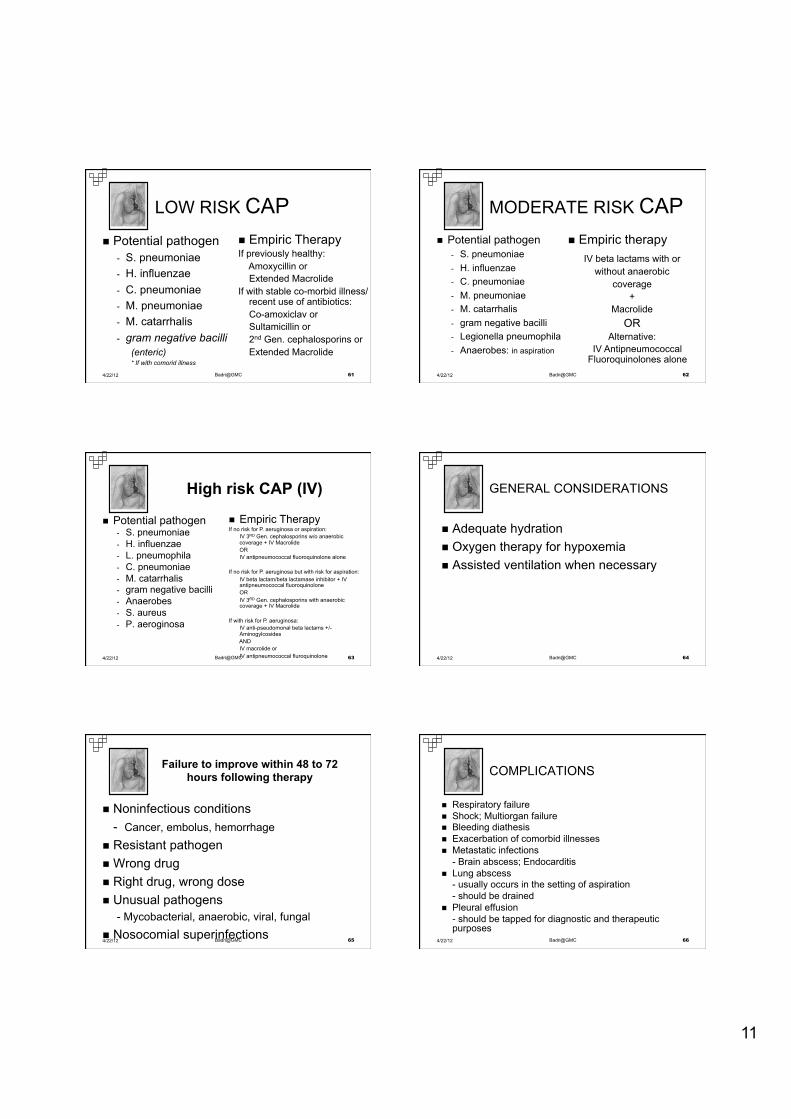
n Potential pathogen - S. pneumoniae - H. influenzae - C. pneumoniae - M. pneumoniae - M. catarrhalis - gram negative bacilli
(enteric) * If with comorid illness
n Empiric Therapy If previously healthy:
Amoxycillin or Extended Macrolide
If with stable co-morbid illness/ recent use of antibiotics: Co-amoxiclav or Sultamicillin or 2nd Gen. cephalosporins or Extended Macrolide
LOW RISK CAP
4/22/12 61 Badri@GMC
n Potential pathogen - S. pneumoniae - H. influenzae - C. pneumoniae - M. pneumoniae - M. catarrhalis - gram negative bacilli - Legionella pneumophila - Anaerobes: in aspiration
n Empiric therapy
IV beta lactams with or without anaerobic
coverage +
Macrolide OR
Alternative: IV Antipneumococcal
Fluoroquinolones alone
MODERATE RISK CAP
4/22/12 62 Badri@GMC
High risk CAP (IV)
n Potential pathogen - S. pneumoniae - H. influenzae - L. pneumophila - C. pneumoniae - M. catarrhalis - gram negative bacilli - Anaerobes - S. aureus - P. aeroginosa
n Empiric Therapy If no risk for P. aeruginosa or aspiration:
IV 3RD Gen. cephalosporins w/o anaerobic coverage + IV Macrolide OR IV antipneumococcal fluoroquinolone alone
If no risk for P. aeruginosa but with risk for aspiration:
IV beta lactam/beta lactamase inhibitor + IV antipneumococcal fluoroquinolone OR IV 3RD Gen. cephalosporins with anaerobic coverage + IV Macrolide
If with risk for P. aeruginosa:
IV anti-pseudomonal beta lactams +/- Aminogylcosides AND IV macrolide or IV antipneumococcal fluroquinolone
4/22/12 63 Badri@GMC
n Adequate hydration n Oxygen therapy for hypoxemia n Assisted ventilation when necessary
GENERAL CONSIDERATIONS
4/22/12 64 Badri@GMC
Failure to improve within 48 to 72 hours following therapy
n Noninfectious conditions - Cancer, embolus, hemorrhage
n Resistant pathogen n Wrong drug n Right drug, wrong dose n Unusual pathogens
- Mycobacterial, anaerobic, viral, fungal n Nosocomial superinfections 4/22/12 65 Badri@GMC
n Respiratory failure n Shock; Multiorgan failure n Bleeding diathesis n Exacerbation of comorbid illnesses n Metastatic infections
- Brain abscess; Endocarditis n Lung abscess
- usually occurs in the setting of aspiration - should be drained
n Pleural effusion - should be tapped for diagnostic and therapeutic purposes
COMPLICATIONS
4/22/12 66 Badri@GMC
12
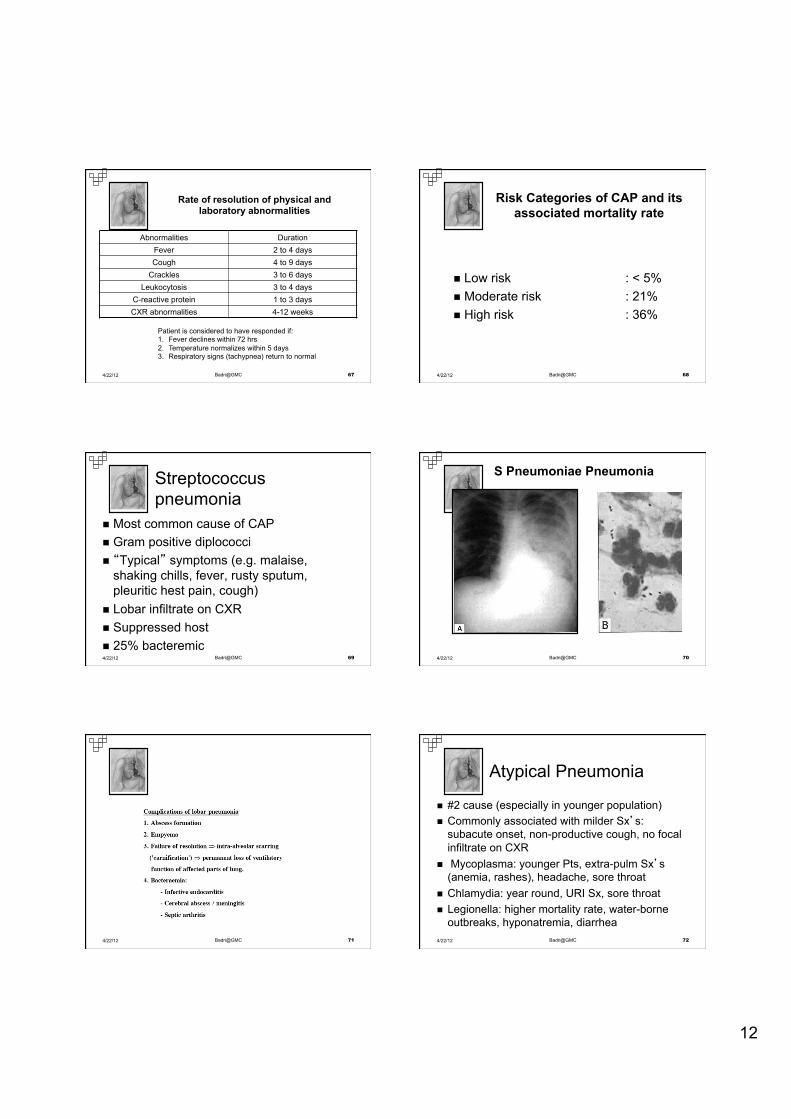
Rate of resolution of physical and laboratory abnormalities
Abnormalities Duration Fever 2 to 4 days Cough 4 to 9 days
Crackles 3 to 6 days Leukocytosis 3 to 4 days
C-reactive protein 1 to 3 days CXR abnormalities 4-12 weeks
Patient is considered to have responded if: 1. Fever declines within 72 hrs 2. Temperature normalizes within 5 days 3. Respiratory signs (tachypnea) return to normal
4/22/12 67 Badri@GMC
Risk Categories of CAP and its associated mortality rate
n Low risk : < 5% n Moderate risk : 21% n High risk : 36%
4/22/12 68 Badri@GMC
Streptococcus pneumonia
n Most common cause of CAP n Gram positive diplococci n “Typical” symptoms (e.g. malaise,
shaking chills, fever, rusty sputum, pleuritic hest pain, cough)
n Lobar infiltrate on CXR n Suppressed host n 25% bacteremic 4/22/12 69 Badri@GMC
S Pneumoniae Pneumonia
4/22/12 70 Badri@GMC
4/22/12 71 Badri@GMC
Atypical Pneumonia
n #2 cause (especially in younger population) n Commonly associated with milder Sx’s:
subacute onset, non-productive cough, no focal infiltrate on CXR
n Mycoplasma: younger Pts, extra-pulm Sx’s (anemia, rashes), headache, sore throat
n Chlamydia: year round, URI Sx, sore throat n Legionella: higher mortality rate, water-borne
outbreaks, hyponatremia, diarrhea
Pneumonia
4/22/12 72 Badri@GMC
13
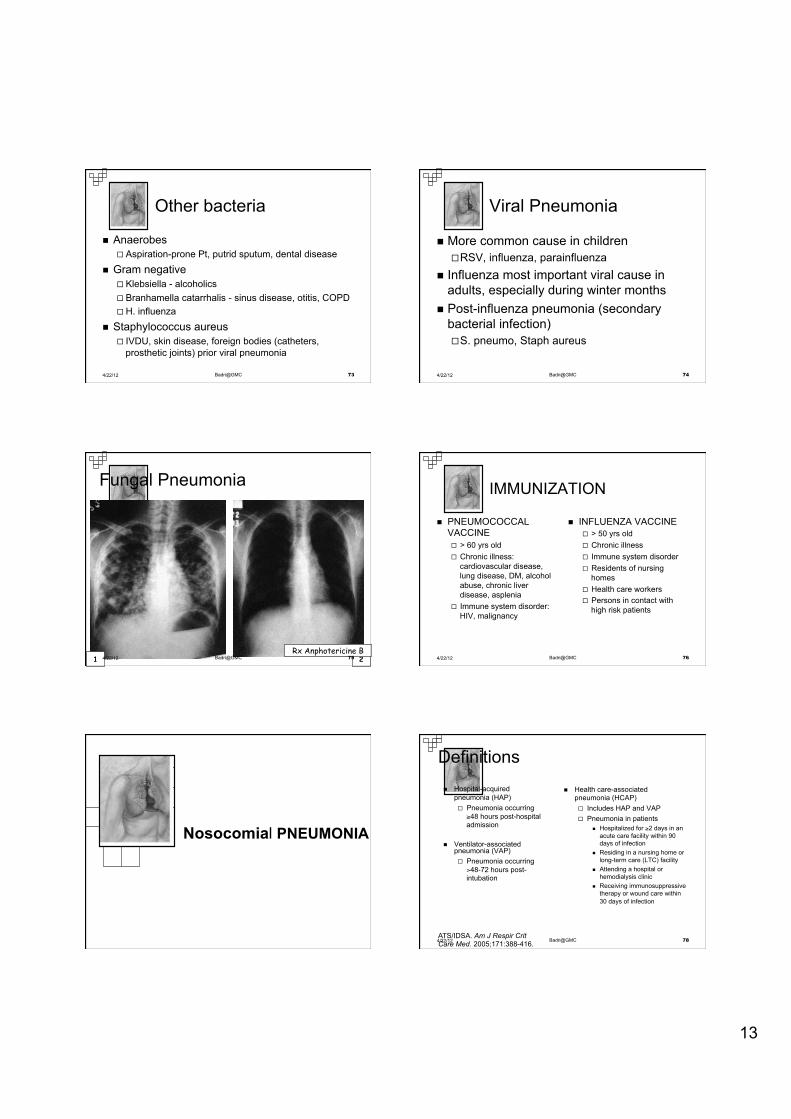
Other bacteria
n Anaerobes ¨ Aspiration-prone Pt, putrid sputum, dental disease
n Gram negative ¨ Klebsiella - alcoholics ¨ Branhamella catarrhalis - sinus disease, otitis, COPD ¨ H. influenza
n Staphylococcus aureus ¨ IVDU, skin disease, foreign bodies (catheters,
prosthetic joints) prior viral pneumonia
4/22/12 73 Badri@GMC
Viral Pneumonia
n More common cause in children ¨ RSV, influenza, parainfluenza
n Influenza most important viral cause in adults, especially during winter months
n Post-influenza pneumonia (secondary bacterial infection) ¨ S. pneumo, Staph aureus
4/22/12 74 Badri@GMC
Fungal Pneumonia
2 Rx Anphotericine B
1 4/22/12 75 Badri@GMC
IMMUNIZATION
n PNEUMOCOCCAL VACCINE ¨ > 60 yrs old ¨ Chronic illness:
cardiovascular disease, lung disease, DM, alcohol abuse, chronic liver disease, asplenia
¨ Immune system disorder: HIV, malignancy
n INFLUENZA VACCINE ¨ > 50 yrs old ¨ Chronic illness ¨ Immune system disorder ¨ Residents of nursing
homes ¨ Health care workers ¨ Persons in contact with
high risk patients
4/22/12 76 Badri@GMC
Nosocomial PNEUMONIA
Definitions
ATS/IDSA. Am J Respir Crit Care Med. 2005;171:388-416.
n Health care-associated pneumonia (HCAP) ¨ Includes HAP and VAP ¨ Pneumonia in patients
n Hospitalized for ≥2 days in an acute care facility within 90 days of infection
n Residing in a nursing home or long-term care (LTC) facility
n Attending a hospital or hemodialysis clinic
n Receiving immunosuppressive therapy or wound care within 30 days of infection
n Hospital-acquired pneumonia (HAP) ¨ Pneumonia occurring
≥48 hours post-hospital admission
n Ventilator-associated pneumonia (VAP) ¨ Pneumonia occurring
>48-72 hours post-intubation
4/22/12 78 Badri@GMC
14
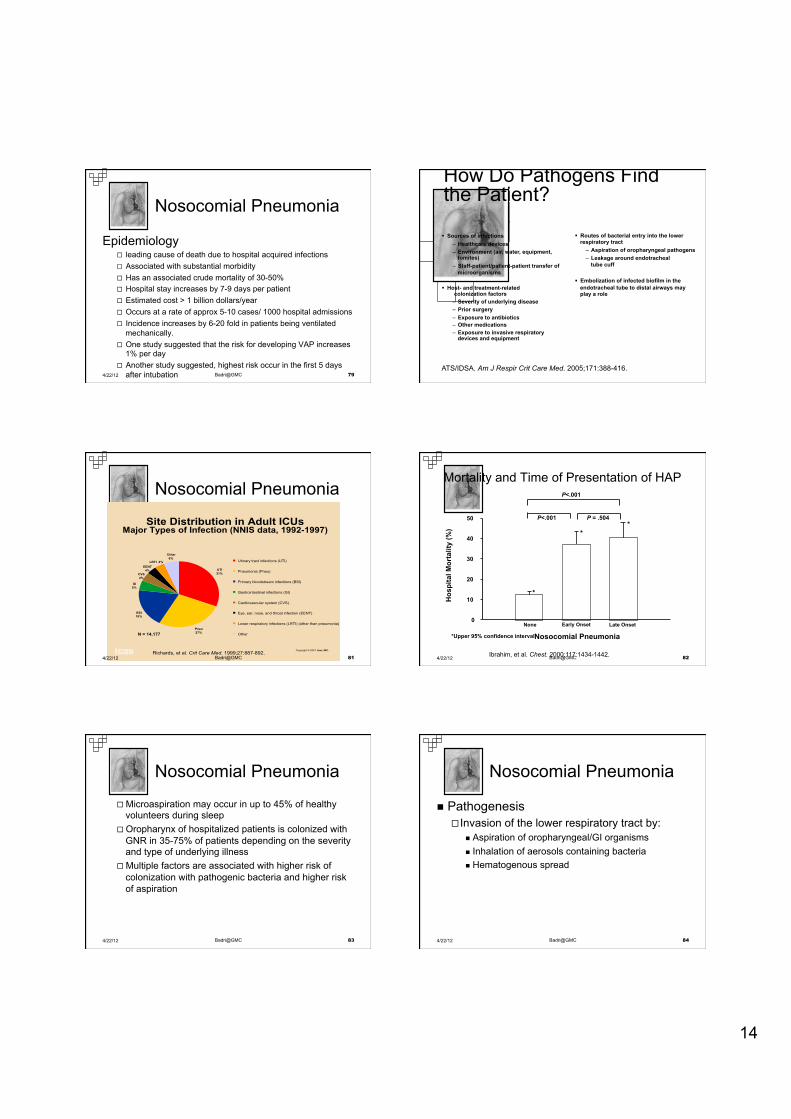
Nosocomial Pneumonia
Epidemiology ¨ leading cause of death due to hospital acquired infections ¨ Associated with substantial morbidity ¨ Has an associated crude mortality of 30-50% ¨ Hospital stay increases by 7-9 days per patient ¨ Estimated cost > 1 billion dollars/year ¨ Occurs at a rate of approx 5-10 cases/ 1000 hospital admissions ¨ Incidence increases by 6-20 fold in patients being ventilated
mechanically. ¨ One study suggested that the risk for developing VAP increases
1% per day ¨ Another study suggested, highest risk occur in the first 5 days
after intubation 4/22/12 79 Badri@GMC
How Do Pathogens Find the Patient?
ATS/IDSA. Am J Respir Crit Care Med. 2005;171:388-416.
§ Sources of infections – Healthcare devices – Environment (air, water, equipment,
fomites) – Staff-patient/patient-patient transfer of
microorganisms
§ Host- and treatment-related colonization factors
– Severity of underlying disease – Prior surgery – Exposure to antibiotics – Other medications – Exposure to invasive respiratory
devices and equipment
§ Routes of bacterial entry into the lower respiratory tract
– Aspiration of oropharyngeal pathogens – Leakage around endotracheal
tube cuff
§ Embolization of infected biofilm in the endotracheal tube to distal airways may play a role
Nosocomial Pneumonia
Copyright © 2001 ican, INC.Richards, et al. Crit Care Med. 1999;27:887-892.
Site Distribution in Adult ICUsMajor Types of Infection (NNIS data, 1992-1997)
27%
GI
CVS
Other
Pneu
31%4%
4%
EENT
BSI19%
5%
6%LRTI 4%
UTI
Urinary tract infections (UTI)
Pneumonia (Pneu)
Primary bloodstream infections (BSI)
Gastrointestinal infections (GI)
Cardiovascular system (CVS)
Eye, ear, nose, and throat infection (EENT)
Lower respiratory infections (LRTI) (other than pneumonia)
OtherN = 14,177
4/22/12 81 Badri@GMC
Hos
pita
l Mor
talit
y (%
)
0 10 20 30 40 50
None Early Onset Late Onset Nosocomial Pneumonia
P = .504 P<.001 P<.001
Mortality and Time of Presentation of HAP
Ibrahim, et al. Chest. 2000;117:1434-1442.
*Upper 95% confidence interval
*
* *
4/22/12 82 Badri@GMC
Nosocomial Pneumonia
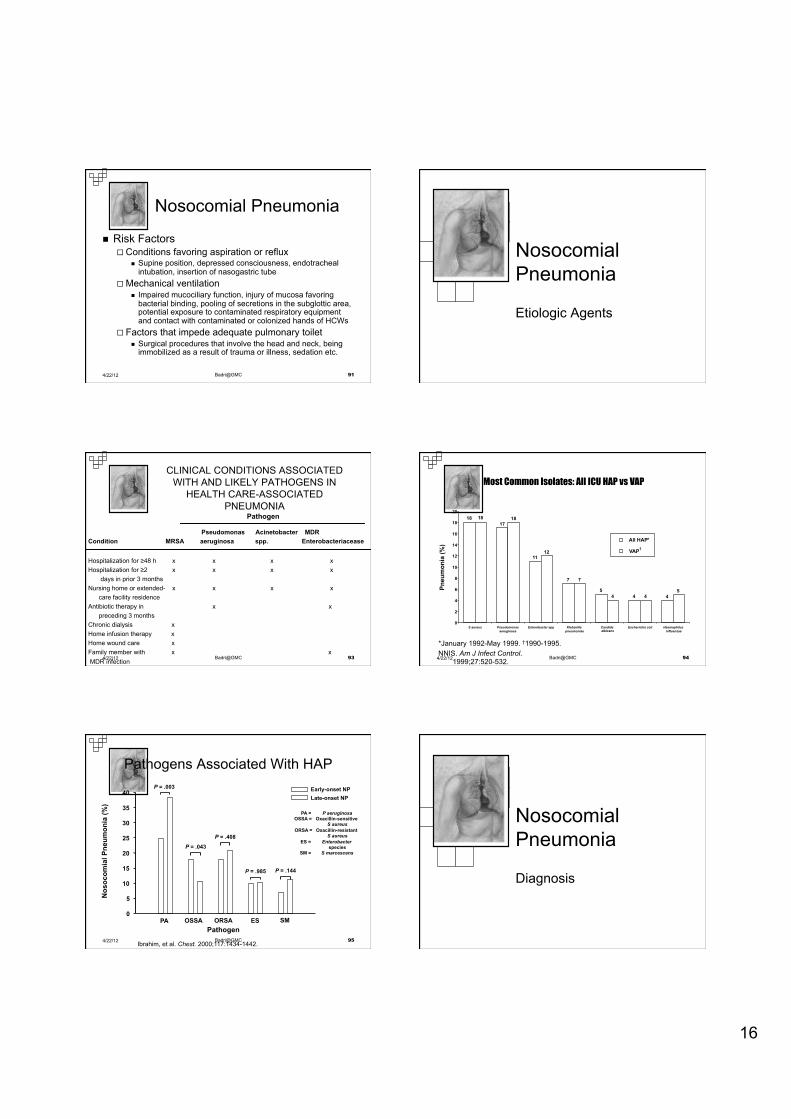
¨ Microaspiration may occur in up to 45% of healthy volunteers during sleep
¨ Oropharynx of hospitalized patients is colonized with GNR in 35-75% of patients depending on the severity and type of underlying illness
¨ Multiple factors are associated with higher risk of colonization with pathogenic bacteria and higher risk of aspiration
4/22/12 83 Badri@GMC
Nosocomial Pneumonia
n Pathogenesis ¨ Invasion of the lower respiratory tract by:
n Aspiration of oropharyngeal/GI organisms n Inhalation of aerosols containing bacteria n Hematogenous spread
4/22/12 84 Badri@GMC
15
4/22/12 85 Badri@GMC
Nosocomial Pneumonia
n Diagnosis ¨ Not necessarily easy to accurately diagnose HAP ¨ Criteria frequently include:
n Clinical ¨ fever ; cough with purulent sputum,
n Radiographic ¨ new or progressive infiltrates on CXR,
n Laboratorial ¨ leukocytosis or leukopenia
n Microbiologic ¨ Suggestive gram stain and positive cultures of sputum,
tracheal aspirate, BAL, bronchial brushing, pleural fluid or blood
¨ Quantitative cultures 4/22/12 86 Badri@GMC
Colonization Aspiration
HAP
MRSA*
4/22/12 87 Badri@GMC
Nosocomial Pneumonia
Risk Factors
Risk Factors for Multidrug-Resistant (MDR) Pathogens Causing HAP, HCAP, and VAP
ATS/IDSA. Am J Respir Crit Care Med. 2005;171:388-416.
§ Antimicrobial therapy in preceding 90 days § Current hospitalization of ≥5 days § High frequency of community or hospital-unit antibiotic resistance § Presence of risk factors for HCAP
– Hospitalization for ≥2 days in preceding 90 days – Residence in a nursing home or LTC facility – Home infusion therapy (including antibiotics) – Chronic dialysis within 30 days – Home wound care – Family member with MDR pathogen
§ Immunosuppressive disease and/or therapy
4/22/12 89 Badri@GMC
Nosocomial Pneumonia
n Risk Factors ¨ Host Factors
n Extremes of age, severe acute or chronic illnesses, immunosupression, coma, alcoholism, malnutrition, COPD, DM
¨ Factors that enhance colonization of the oropharynx and stomach by pathogenic microorganisms
n admission to an ICU, administration of antibiotics, chronic lung disease, endotracheal intubation, etc.
4/22/12 90 Badri@GMC
16
Nosocomial Pneumonia
n Risk Factors ¨ Conditions favoring aspiration or reflux
n Supine position, depressed consciousness, endotracheal intubation, insertion of nasogastric tube
¨ Mechanical ventilation n Impaired mucociliary function, injury of mucosa favoring
bacterial binding, pooling of secretions in the subglottic area, potential exposure to contaminated respiratory equipment and contact with contaminated or colonized hands of HCWs
¨ Factors that impede adequate pulmonary toilet n Surgical procedures that involve the head and neck, being
immobilized as a result of trauma or illness, sedation etc.
4/22/12 91 Badri@GMC
Nosocomial Pneumonia
Etiologic Agents
CLINICAL CONDITIONS ASSOCIATED WITH AND LIKELY PATHOGENS IN
HEALTH CARE-ASSOCIATED PNEUMONIA
Pseudomonas Acinetobacter MDR Condition MRSA aeruginosa spp. Enterobacteriacease Hospitalization for ≥48 h x x x x Hospitalization for ≥2 x x x x days in prior 3 months Nursing home or extended- x x x x care facility residence Antibiotic therapy in x x preceding 3 months Chronic dialysis x Home infusion therapy x Home wound care x Family member with x x MDR infection
Pathogen
4/22/12 93 Badri@GMC NNIS. Am J Infect Control.
1999;27:520-532. Fridkin SK et al. Infect Dis Clin
North Am. 1997;11:479-496.
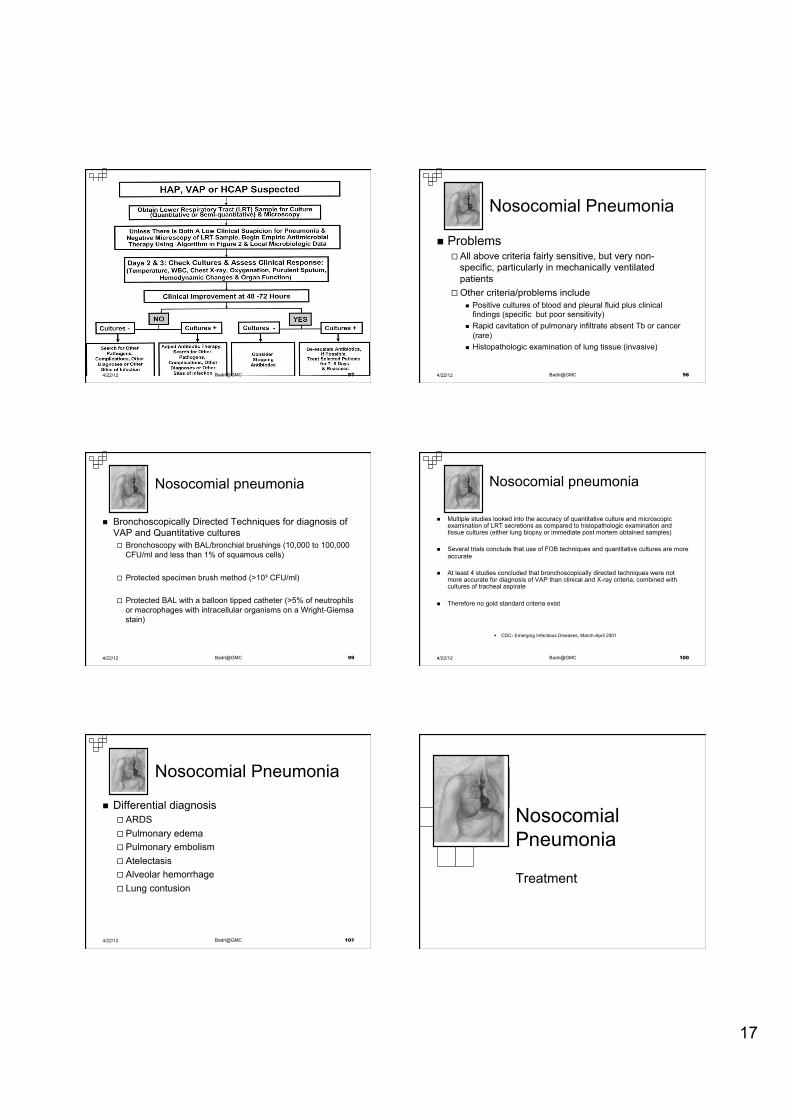
Pneu
mon
ia (%
)
17 18
11
7 5
4 4
18 18
7
12
4 4 5
0 2 4 6 8
10 12 14 16 18 20
S aureus Pseudomonas aeruginosa Enterobacter spp Klebsiella
pneumoniae Candida albicans Escherichia coli Haemophilus
influenzae
All HAP * VAP †
*January 1992-May 1999. †1990-1995.
Most Common Isolates: All ICU HAP vs VAP
4/22/12 94 Badri@GMC
Nos
ocom
ial P
neum
onia
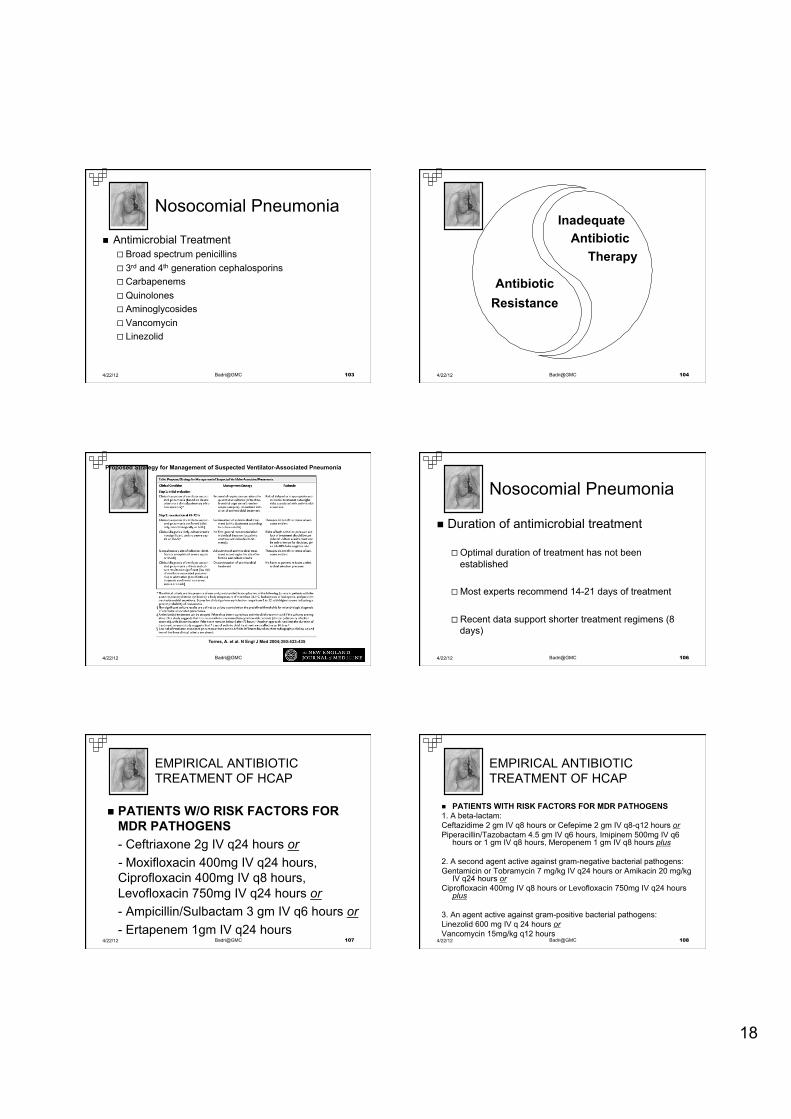
(%)
0 5
10 15 20 25 30 35 40
PA OSSA ORSA ES SM
P = .003
P = .043 P = .408
P = .985 P = .144
Pathogen
Early-onset NP Late-onset NP
PA = P aeruginosa OSSA = Oxacillin-sensitive
S aureus ORSA = Oxacillin-resistant
S aureus ES = Enterobacter
species SM = S marcescens
Pathogens Associated With HAP
Ibrahim, et al. Chest. 2000;117:1434-1442. 4/22/12 95 Badri@GMC
Nosocomial Pneumonia
Diagnosis
17
4/22/12 97 Badri@GMC
Nosocomial Pneumonia
n Problems ¨ All above criteria fairly sensitive, but very non-
specific, particularly in mechanically ventilated patients
¨ Other criteria/problems include n Positive cultures of blood and pleural fluid plus clinical
findings (specific but poor sensitivity) n Rapid cavitation of pulmonary infiltrate absent Tb or cancer
(rare) n Histopathologic examination of lung tissue (invasive)
4/22/12 98 Badri@GMC
Nosocomial pneumonia
n Bronchoscopically Directed Techniques for diagnosis of VAP and Quantitative cultures ¨ Bronchoscopy with BAL/bronchial brushings (10,000 to 100,000
CFU/ml and less than 1% of squamous cells)
¨ Protected specimen brush method (>10³ CFU/ml)
¨ Protected BAL with a balloon tipped catheter (>5% of neutrophils or macrophages with intracellular organisms on a Wright-Giemsa stain)
4/22/12 99 Badri@GMC
Nosocomial pneumonia
n Multiple studies looked into the accuracy of quantitative culture and microscopic examination of LRT secretions as compared to histopathologic examination and tissue cultures (either lung biopsy or immediate post mortem obtained samples)
n Several trials conclude that use of FOB techniques and quantitative cultures are more accurate
n At least 4 studies concluded that bronchoscopically directed techniques were not more accurate for diagnosis of VAP than clinical and X-ray criteria, combined with cultures of tracheal aspirate
n Therefore no gold standard criteria exist
§ CDC- Emerging Infectious Diseases, March-April 2001
4/22/12 100 Badri@GMC
Nosocomial Pneumonia
n Differential diagnosis ¨ ARDS ¨ Pulmonary edema ¨ Pulmonary embolism ¨ Atelectasis ¨ Alveolar hemorrhage ¨ Lung contusion
4/22/12 101 Badri@GMC
Nosocomial Pneumonia
Treatment
18
Nosocomial Pneumonia
n Antimicrobial Treatment ¨ Broad spectrum penicillins ¨ 3rd and 4th generation cephalosporins ¨ Carbapenems ¨ Quinolones ¨ Aminoglycosides ¨ Vancomycin ¨ Linezolid
4/22/12 103 Badri@GMC
Inadequate Antibiotic
Therapy
Antibiotic Resistance
4/22/12 104 Badri@GMC
Torres, A. et al. N Engl J Med 2004;350:433-435
Proposed Strategy for Management of Suspected Ventilator-Associated Pneumonia
4/22/12 105 Badri@GMC
Nosocomial Pneumonia
n Duration of antimicrobial treatment
¨ Optimal duration of treatment has not been established
¨ Most experts recommend 14-21 days of treatment
¨ Recent data support shorter treatment regimens (8 days)
4/22/12 106 Badri@GMC
n PATIENTS W/O RISK FACTORS FOR MDR PATHOGENS - Ceftriaxone 2g IV q24 hours or - Moxifloxacin 400mg IV q24 hours, Ciprofloxacin 400mg IV q8 hours, Levofloxacin 750mg IV q24 hours or - Ampicillin/Sulbactam 3 gm IV q6 hours or - Ertapenem 1gm IV q24 hours
EMPIRICAL ANTIBIOTIC TREATMENT OF HCAP
4/22/12 107 Badri@GMC
n PATIENTS WITH RISK FACTORS FOR MDR PATHOGENS 1. A beta-lactam: Ceftazidime 2 gm IV q8 hours or Cefepime 2 gm IV q8-q12 hours or Piperacillin/Tazobactam 4.5 gm IV q6 hours, Imipinem 500mg IV q6
hours or 1 gm IV q8 hours, Meropenem 1 gm IV q8 hours plus 2. A second agent active against gram-negative bacterial pathogens: Gentamicin or Tobramycin 7 mg/kg IV q24 hours or Amikacin 20 mg/kg
IV q24 hours or Ciprofloxacin 400mg IV q8 hours or Levofloxacin 750mg IV q24 hours
plus 3. An agent active against gram-positive bacterial pathogens: Linezolid 600 mg IV q 24 hours or Vancomycin 15mg/kg q12 hours
EMPIRICAL ANTIBIOTIC TREATMENT OF HCAP
4/22/12 108 Badri@GMC
19
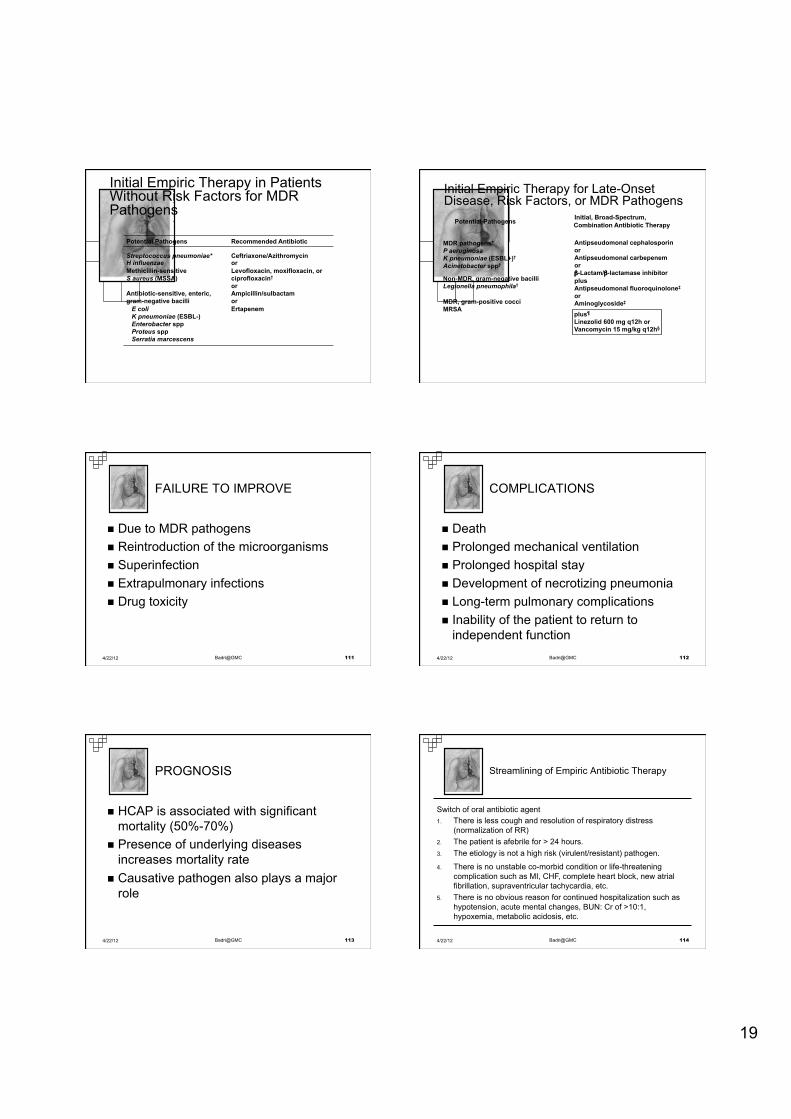
Initial Empiric Therapy in Patients Without Risk Factors for MDR Pathogens
Potential Pathogens Recommended Antibiotic
Streptococcus pneumoniae*
H influenzae Methicillin-sensitive S aureus (MSSA) Antibiotic-sensitive, enteric, gram-negative bacilli E coli K pneumoniae (ESBL-) Enterobacter spp Proteus spp Serratia marcescens
Ceftriaxone/Azithromycin or Levofloxacin, moxifloxacin, or ciprofloxacin† or Ampicillin/sulbactam or Ertapenem
Initial Empiric Therapy for Late-Onset Disease, Risk Factors, or MDR Pathogens
Initial, Broad-Spectrum,
plus¶
Linezolid 600 mg q12h or Vancomycin 15 mg/kg q12h§
Antipseudomonal cephalosporin or Antipseudomonal carbepenem or β-Lactam/β-lactamase inhibitor plus Antipseudomonal fluoroquinolone‡
or Aminoglycoside‡
MDR pathogens* P aeruginosa K pneumoniae (ESBL+)†
Acinetobacter spp†
Non-MDR, gram-negative bacilli Legionella pneumophila† MDR, gram-positive cocci MRSA
Combination Antibiotic Therapy Potential Pathogens
n Due to MDR pathogens n Reintroduction of the microorganisms n Superinfection n Extrapulmonary infections n Drug toxicity
FAILURE TO IMPROVE
4/22/12 111 Badri@GMC
n Death n Prolonged mechanical ventilation n Prolonged hospital stay n Development of necrotizing pneumonia n Long-term pulmonary complications n Inability of the patient to return to
independent function
COMPLICATIONS
4/22/12 112 Badri@GMC
n HCAP is associated with significant mortality (50%-70%)
n Presence of underlying diseases increases mortality rate
n Causative pathogen also plays a major role
PROGNOSIS
4/22/12 113 Badri@GMC
Switch of oral antibiotic agent 1. There is less cough and resolution of respiratory distress
(normalization of RR) 2. The patient is afebrile for > 24 hours. 3. The etiology is not a high risk (virulent/resistant) pathogen.
4. There is no unstable co-morbid condition or life-threatening complication such as MI, CHF, complete heart block, new atrial fibrillation, supraventricular tachycardia, etc.
5. There is no obvious reason for continued hospitalization such as hypotension, acute mental changes, BUN: Cr of >10:1, hypoxemia, metabolic acidosis, etc.
Streamlining of Empiric Antibiotic Therapy
4/22/12 114 Badri@GMC
20
Nosocomial Pneumonia
Prevention
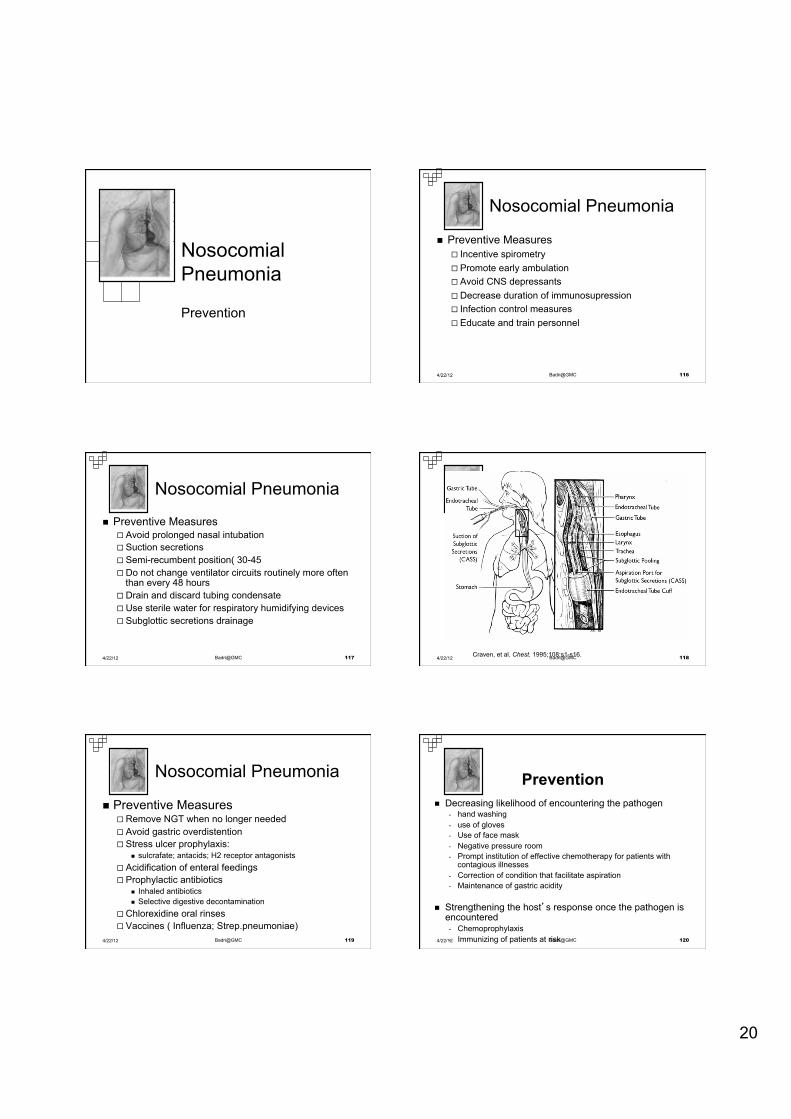
Nosocomial Pneumonia
n Preventive Measures ¨ Incentive spirometry ¨ Promote early ambulation ¨ Avoid CNS depressants ¨ Decrease duration of immunosupression ¨ Infection control measures ¨ Educate and train personnel
4/22/12 116 Badri@GMC
Nosocomial Pneumonia
n Preventive Measures ¨ Avoid prolonged nasal intubation ¨ Suction secretions ¨ Semi-recumbent position( 30-45°head elevation) ¨ Do not change ventilator circuits routinely more often
than every 48 hours ¨ Drain and discard tubing condensate ¨ Use sterile water for respiratory humidifying devices ¨ Subglottic secretions drainage
4/22/12 117 Badri@GMC Craven, et al. Chest. 1995;108:s1-s16. 4/22/12 118 Badri@GMC
Nosocomial Pneumonia
n Preventive Measures ¨ Remove NGT when no longer needed ¨ Avoid gastric overdistention ¨ Stress ulcer prophylaxis:
n sulcrafate; antacids; H2 receptor antagonists ¨ Acidification of enteral feedings ¨ Prophylactic antibiotics
n Inhaled antibiotics n Selective digestive decontamination
¨ Chlorexidine oral rinses ¨ Vaccines ( Influenza; Strep.pneumoniae)
4/22/12 119 Badri@GMC
Prevention n Decreasing likelihood of encountering the pathogen
- hand washing - use of gloves - Use of face mask - Negative pressure room - Prompt institution of effective chemotherapy for patients with
contagious illnesses - Correction of condition that facilitate aspiration - Maintenance of gastric acidity
n Strengthening the host’s response once the pathogen is encountered
- Chemoprophylaxis - Immunizing of patients at risk 4/22/12 120 Badri@GMC
21
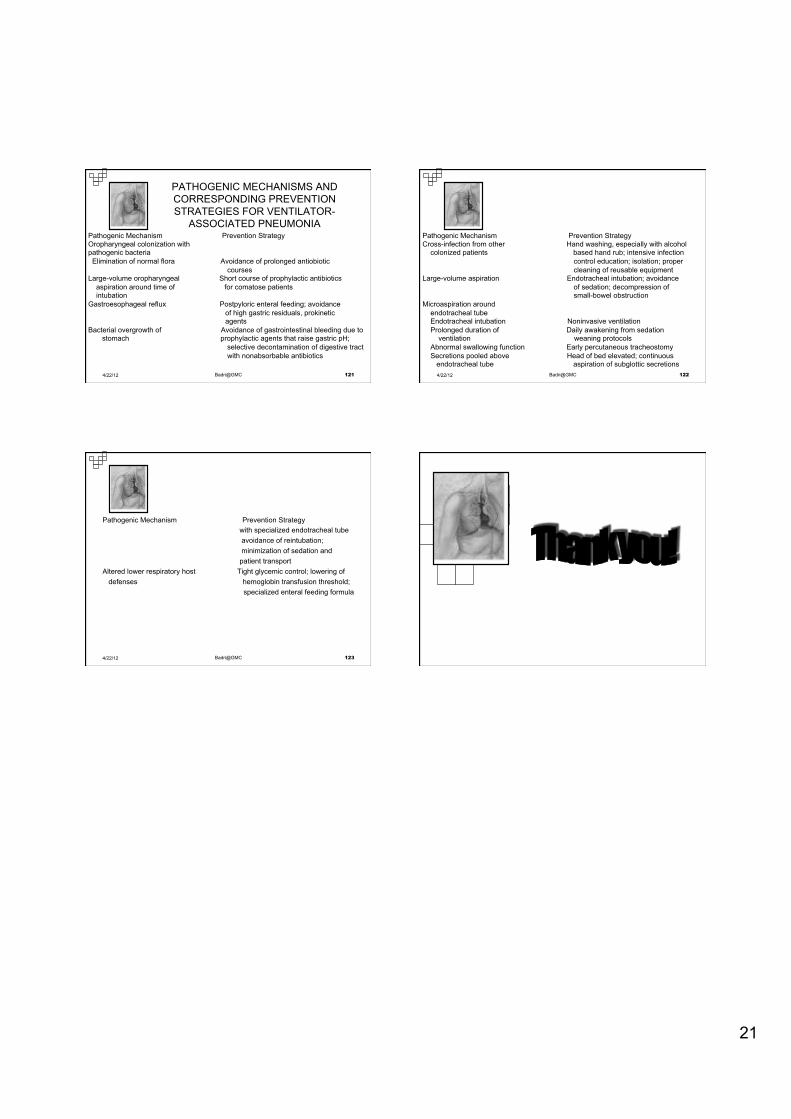
PATHOGENIC MECHANISMS AND CORRESPONDING PREVENTION STRATEGIES FOR VENTILATOR-
ASSOCIATED PNEUMONIA Pathogenic Mechanism Prevention Strategy Oropharyngeal colonization with pathogenic bacteria Elimination of normal flora Avoidance of prolonged antiobiotic courses Large-volume oropharyngeal Short course of prophylactic antibiotics aspiration around time of for comatose patients intubation Gastroesophageal reflux Postpyloric enteral feeding; avoidance of high gastric residuals, prokinetic agents Bacterial overgrowth of Avoidance of gastrointestinal bleeding due to stomach prophylactic agents that raise gastric pH; selective decontamination of digestive tract with nonabsorbable antibiotics 4/22/12 121 Badri@GMC
Pathogenic Mechanism Prevention Strategy Cross-infection from other Hand washing, especially with alcohol colonized patients based hand rub; intensive infection control education; isolation; proper cleaning of reusable equipment Large-volume aspiration Endotracheal intubation; avoidance of sedation; decompression of small-bowel obstruction Microaspiration around endotracheal tube Endotracheal intubation Noninvasive ventilation Prolonged duration of Daily awakening from sedation ventilation weaning protocols Abnormal swallowing function Early percutaneous tracheostomy Secretions pooled above Head of bed elevated; continuous endotracheal tube aspiration of subglottic secretions
4/22/12 122 Badri@GMC
Pathogenic Mechanism Prevention Strategy with specialized endotracheal tube avoidance of reintubation; minimization of sedation and patient transport Altered lower respiratory host Tight glycemic control; lowering of defenses hemoglobin transfusion threshold; specialized enteral feeding formula
4/22/12 123 Badri@GMC