Embed Size (px)
Citation preview
Pneumonia
Barriers to infection:• Epiglottis: protects airway from aspiration.• Cough reflex*.• Mucociliary escalator.• Alveolar macrophage & antimicrobial.
compounds: lysozyme, lactoferrin, complement and IgA.
Pneumonia:Inflammation of the lung parenchyma: Inflammation of alveoli, alveolar ducts, bronchioles, and interstitial tissue of lung, induced by microbial invasion of natural barriers.
Classification of pneumonia: Clinical Classification: • Acute: less than three weeks duration • Chronic pneumonias. Acute pneumonia is further classified
according to place where it was acquired, source of transmission, and etiology.
Classification of Acute Pneumonia: Community acquired:o Person to person Bacterial:Classical bacterial pneumoniaAtypical bacterial pneumonia
Viral pneumoniao Animal, or Environmental Exposure.
Nosocomial acquired.
Community-acquired acute pneumonia: Person-to-Person: A- Classic bacterial pneumonia: • Streptococcus pneumoniae.• Haemophilus influenzae.• Klebsiella pneumoniae.• Moraxella catarrhalis.• Aspiration pneumonia* (mixture of bacteria
including gram negatives, anaerobes and Staphylococcus aureus).
N
Person to Person: B- Atypical bacterial pneumonia:• Chlamydophila pneumoniae• Mycoplasma pneumoniae.
C- Viral pneumonia:• Influenza virus type A, B, and C• Coronaviruses.• Others: RSV, measles, adenoviruses,
CMV…..
Environmental or Animal Exposure:o Legionellosis.o Tularemia. o Plague. o Q fever. o Anthrax.
Streptococcus pneumoniae : Reservoir: nasopharynx of children and adults.
(patients or asymptomatic carriers). Transmission: droplets inhalation.Pathogenesis and microbial virulence:o Colonization of the nasopharynx then spread to the
bronchi and alveoli.o Polysaccharide capsule resist phagocytosis.o Production of pneumolysin: cholesterol-binding
toxin; epithelial cell-damage.o Production of hydrogen peroxide; cell damage, and
inhibition of other bacteria.o Inflammation: production of cytokines; TNFα,IL-1,
IL-8 by alveolar macrophage
(stages of pneumonia): Filling of alveoli by fluids*: many bacteria, and
few inflammatory cells. Early consolidation* stage; infiltration of alveoli
by neutrophils, activation of complement and CRP which interact with bacterial teichoic acid. (battle b/w the bacteria and the immune system).
Late Consolidation stage: heavy infiltration by neutrophils which kill the microbe helped by the specific Ab and complement, (Hepatization).
Infection eradication (resolution): Replacement of neutrophils by alveolar macrophages.
Clinical presentation: Acute lobar pneumonia.
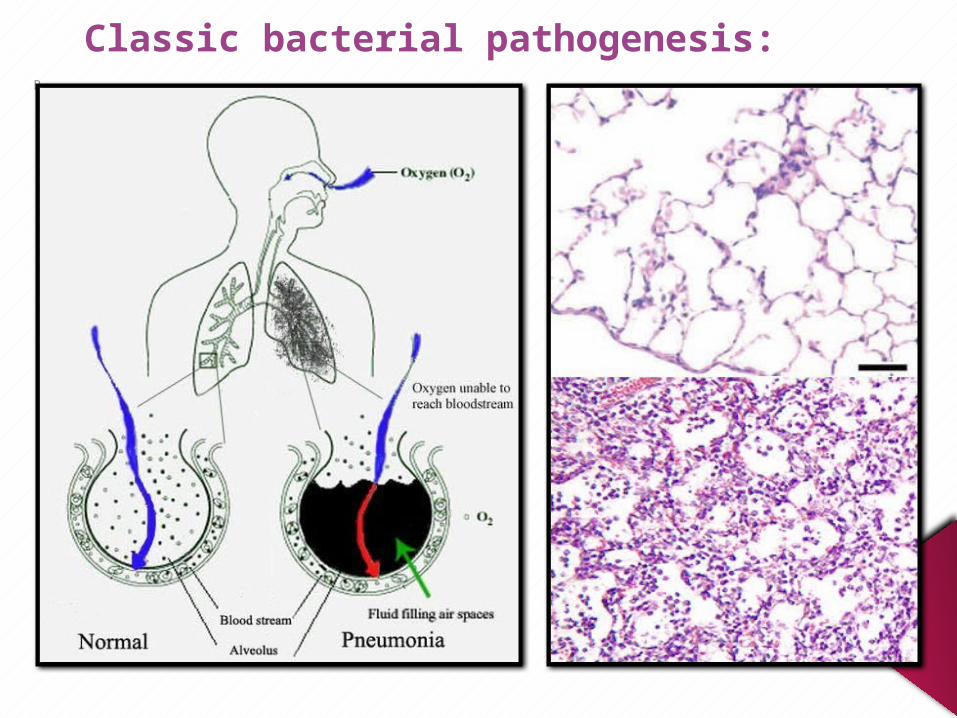
Classic bacterial pathogenesis: R
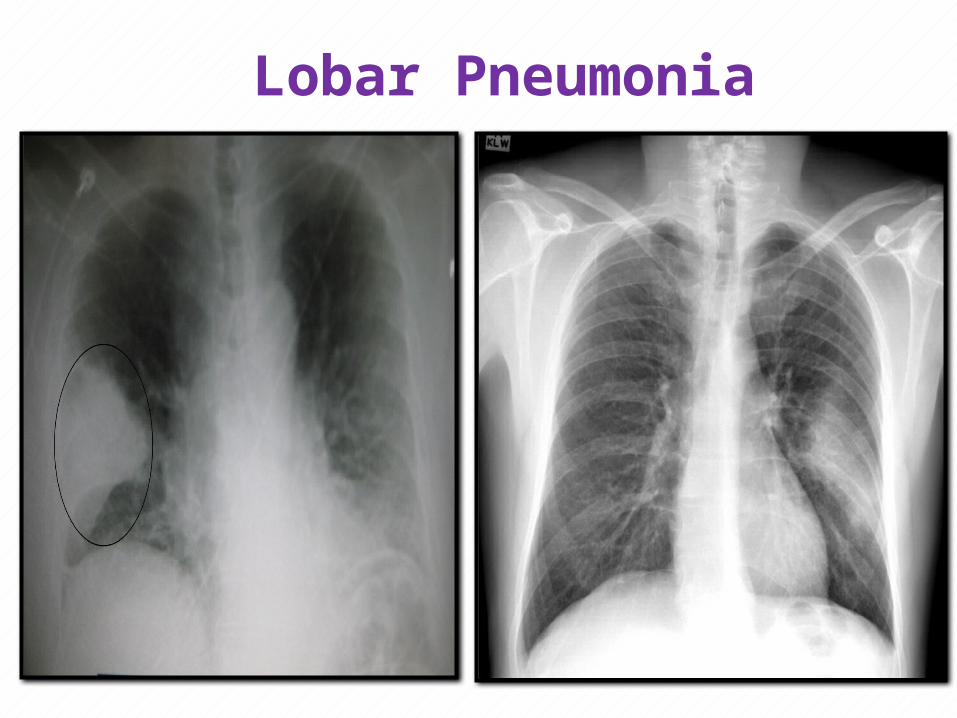
Lobar Pneumonia
N
Complications of Streptococcus pneumonia: Local complications: Pleural effusion; Outpouring of fluid into pleural
space in 25% of cases. Empyema (pus in the pleura): in 1% of cases,
require drainage of fluid. Systemic complications: • Bacteremia (pneumococcemia): through
lymphatic vessels of the lung to thoracic duct.• Positive blood culture in only 25% of cases
(transient bacteremia).
• Defense: humoral factors and lymphatic system to remove the bacteria from the blood.
• Meningitis esp. in splenectomy, sickle cell anaemia
Diagnosis of S. pneumoniae:
• Clinical specimens: Sputum, transtracheal aspirate, broncheoalveolar lavage or lung biopsy.• Direct Microscopy:Streptococcus pneumoniae are Gram positive lanceolate (lancet shaped) diplococci arranged in pairs or chains, and capsulated.• Cultural characteristics:Facultative anaerobic bacteria, alpha hemolytic on blood agar, optochin sensitive.
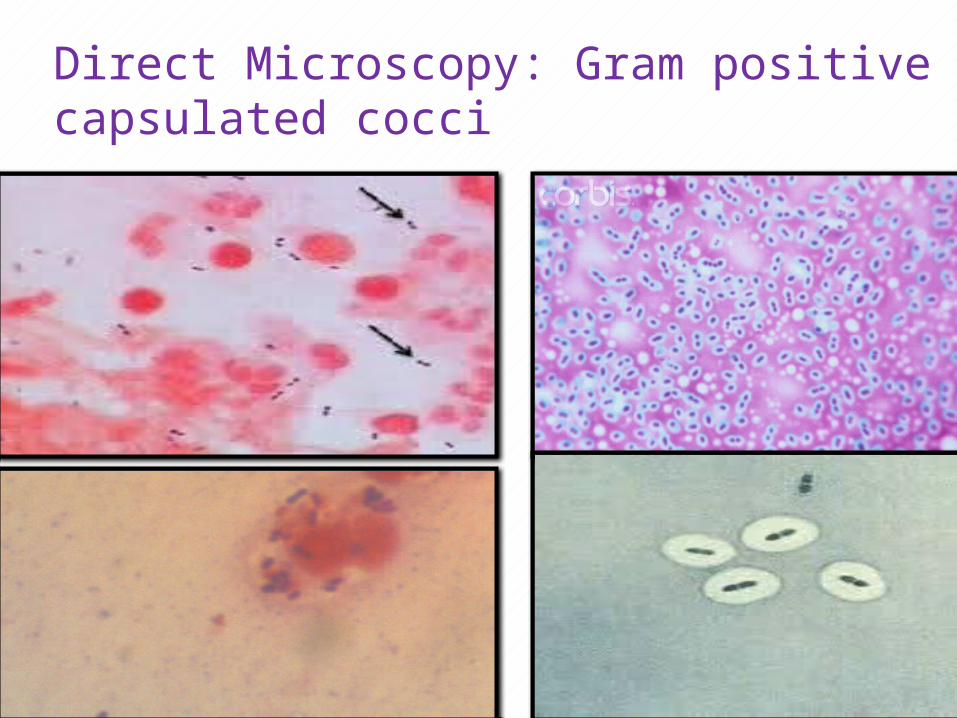
Direct Microscopy: Gram positive capsulated cocci
N
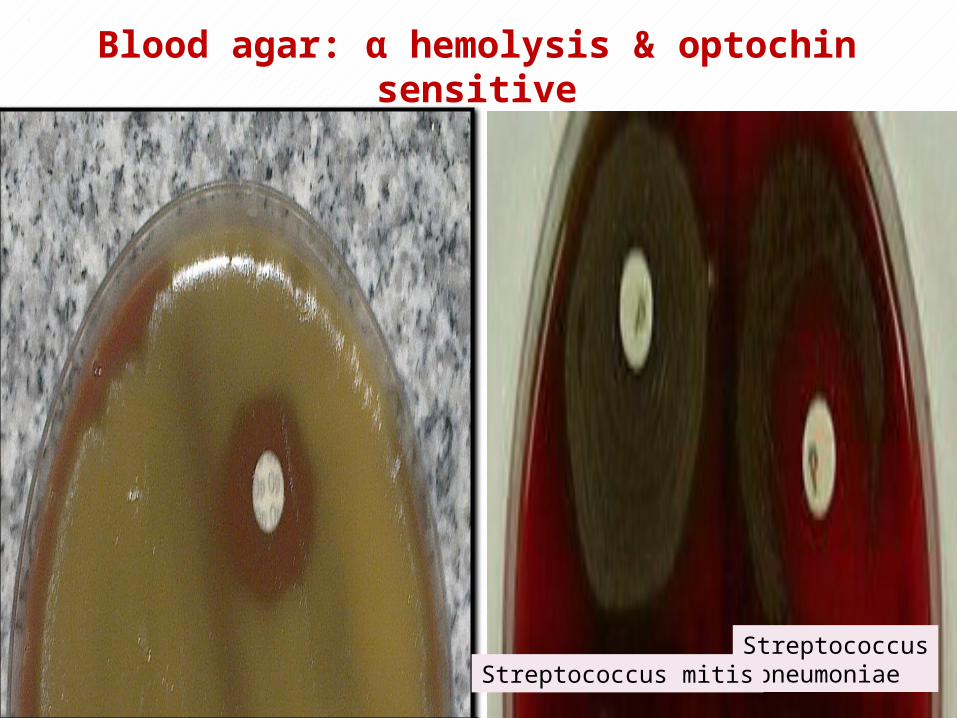
Blood agar: α hemolysis & optochin sensitive
Streptococcus pneumoniaeStreptococcus mitis
N
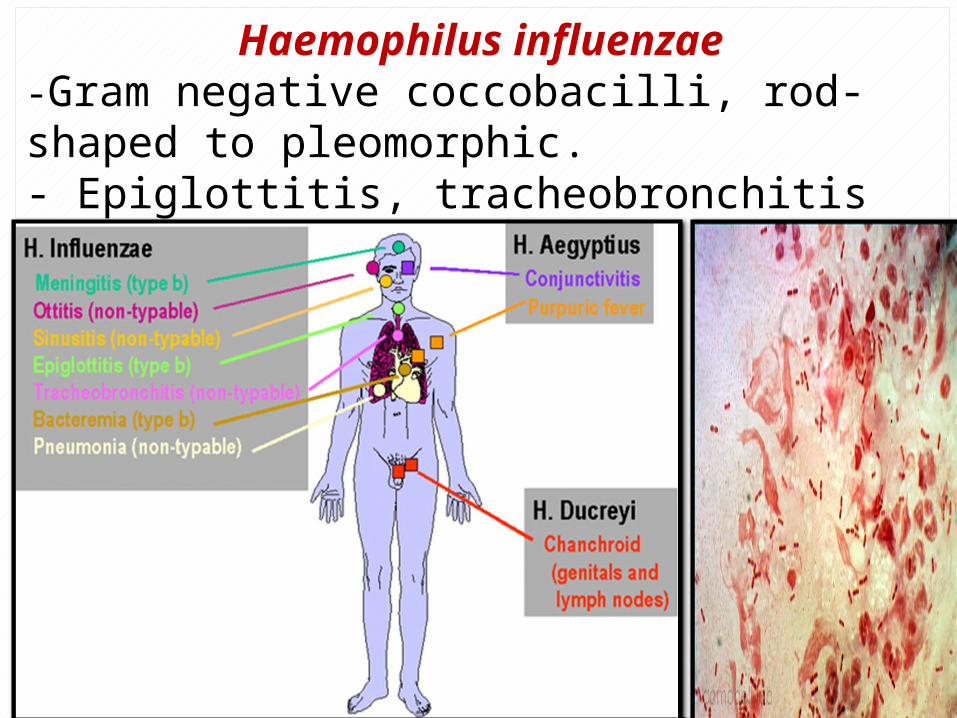
Haemophilus influenzae-Gram negative coccobacilli, rod-shaped to pleomorphic.- Epiglottitis, tracheobronchitis and pneumonia.
N
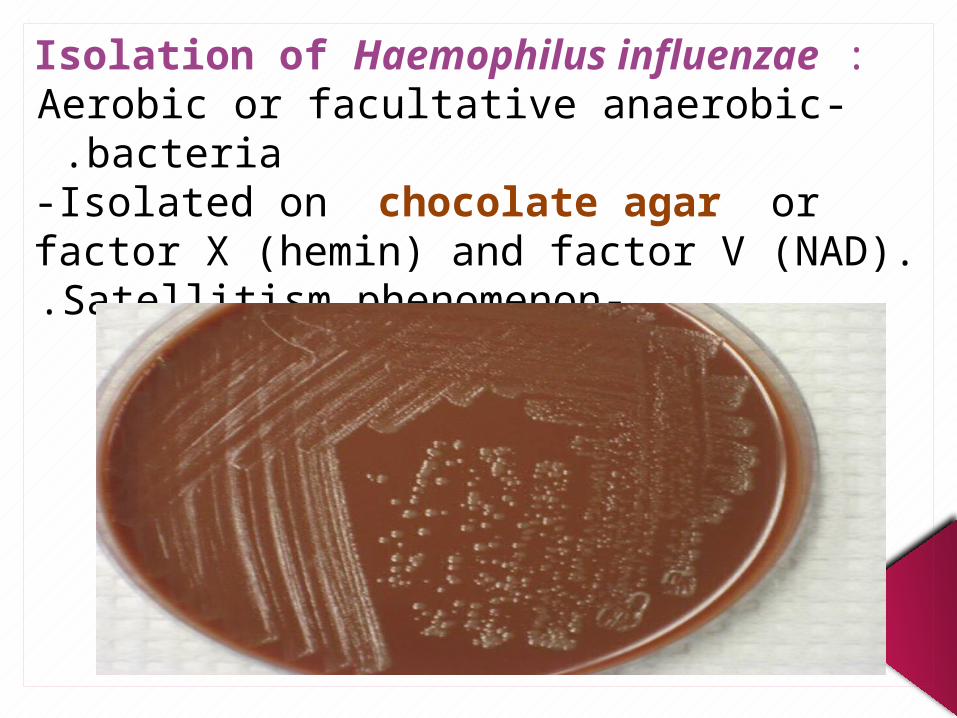
Isolation of Haemophilus influenzae :-Aerobic or facultative anaerobic bacteria .
-Isolated on chocolate agar or factor X (hemin) and factor V (NAD).
-Satellitism phenomenon.

Satellitism around S.aureus.
N
Treatment of S. pneumoniae and H. influenzae:• Beta-lactam antibiotic.• If the patient is allergic to penicillin or the
bacteria is not sensitive: macrolide or fluoroquinolones.
• Penicillin-resistant streptococcus due to mutation in penicillin-binding protein by transformation.
Vaccine: -Conjugated capsular antigen vaccines for S. pneumoniae and H. influenzae type b.
Atypical bacterial pneumonia:
Chlamydophila pneumoniae: • Infective stage: Elementary bodies.-Target cells: columnar epithelial cells, endothelial cells of the vessels and macrophages.- Receptor-mediated endocytosis (intracellular infection).- Lymphocytic infiltration; IF-γ creates persistence infection by slowing the growth of the RB. • Diagnostic stage: Reticulate bodies.
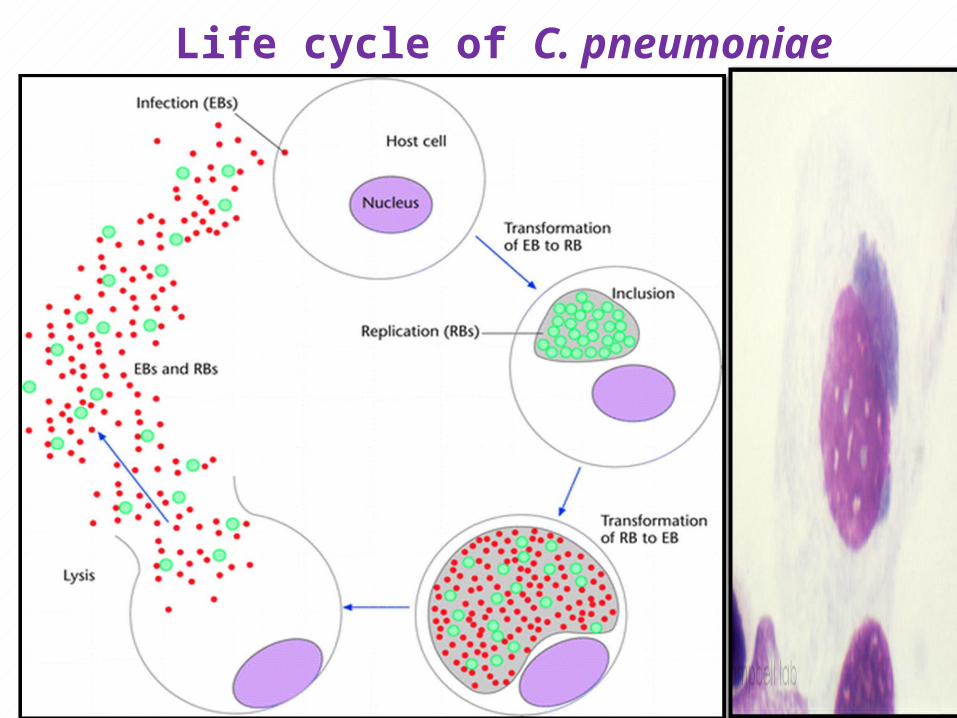
Life cycle of C. pneumoniae
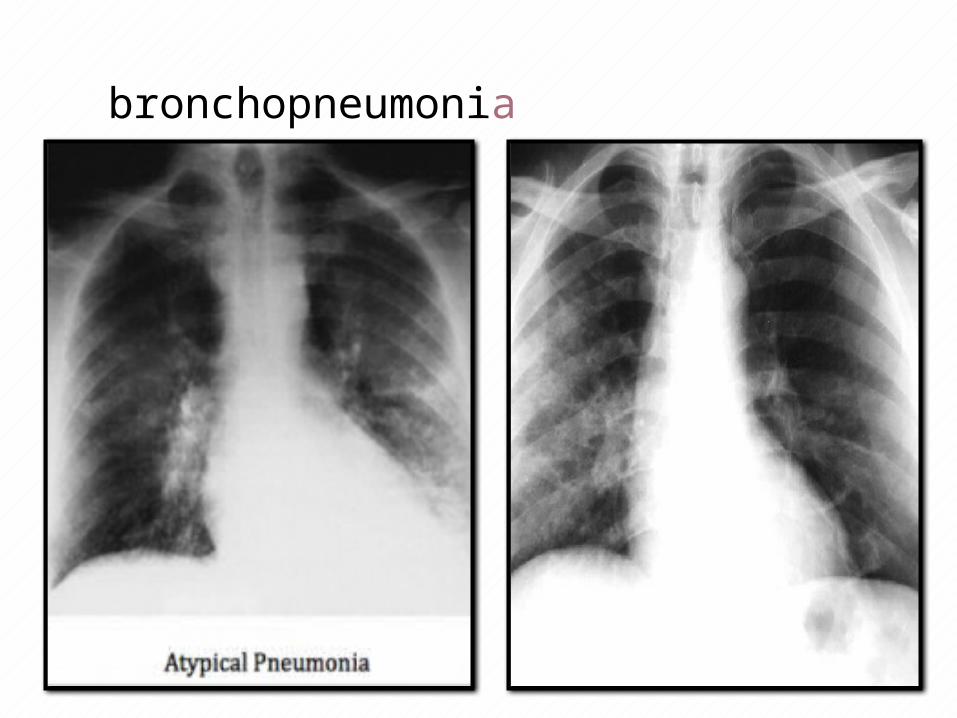
Clinical presentation: Acute tracheobronchitis. Bronchopneumonia (patchy infiltrates on
radiography). C. pneumoniae is associated with Coronary
artery disease (CAD):o Adults with CAD have a high antibodies titer
against this bacterium.o The microbe can be isolated from
atherosclerotic lesions.o The microbe established CAD in animal
model studies.
bronchopneumonia
N
Diagnosis: • Immunofluorescent microscopy for antigen and
antibodies detection.• PCR. Treatment:- Macrolide: Long-term Cmax (maximum serum concentration) of azithromycin. - Or doxycycline for 7 days.- Pregnant women: erythromycin or azithromycin.
N
Mycoplasma pneumoniae:• Smallest prokaryotes that lack cell-wall.• Infect mainly individuals aged 5-20 years old.• Pathogenesis:
Tip structure mediated attachment to carbohydrate containing receptor on columnar epithelial cells.
The infection is not highly destructive but the ciliary function is impaired. Exotoxins:• ADP-ribosyltransferase: inhibition of neutrophils
chemotaxis and phagocytosis.• Vacuolating toxin: apoptosis of ciliated cells. • Monocytic infiltration. (few neutrophils)
N
Clinical presentation: • Tracheobronchitis (persistent dry cough). • Bronchopneumonia; (infiltration of
monocytes with few neutrophils); patchy infiltrate on radiography.
• In 50% of severe mycoplasma infections; mild-autoimmune hemolytic anemia* due to cold hemagglutinin formation.
Complications:• Encephalitis, renal disease and arthritis
(antibody complex), autoimmune thrombocytopenic purpura** (erythema multiforme).

N
Diagnosis:-Direct: PCR or Immunofluorescent microscopy.-Indirect: serology: Complement fixation or cold agglutinin test. Treatment:-Macrolide.-Resistance strains; Tetracycline or Fluoroquinolones.










![Comparative Regional Analysis of Bacterial Pneumonia ...Failure (CHF) and Bacterial Pneumonia [1] have recorded high re-admission rates reflecting discrepancies in medical procedures](https://img.pdfslide.net/doc/110x75/5ebb9879318fa16d813750c8/comparative-regional-analysis-of-bacterial-pneumonia-failure-chf-and-bacterial.jpg)