Embed Size (px)
Citation preview
HALT 2016 Ireland National Report 1
Point Prevalence Survey of Healthcare-Associated Infections & Antimicrobial Use in Long-Term Care Facilities (HALT): May 2016
IRELAND: NATIONAL REPORT – MARCH 2017
Report Authors: Sarah Hennessy, Helen Murphy & Karen Burns, HPSC
SUGGESTED CITATION: HEALTH PROTECTION SURVEILLANCE CENTRE, POINT PREVALENCE
SURVEY OF HEALTHCARE-ASSOCIATED INFECTIONS & ANTIMICROBIAL USE IN LONG-TERM
CARE FACILITIES: MAY 2016 – IRELAND NATIONAL REPORT: MARCH 2017
HALT 2016 Ireland National Report 2
Table of Contents Acknowledgements .......................................................................................................... 3
Executive Summary .......................................................................................................... 4
Priorities for Implementation ........................................................................................... 8
Plain Language Summary ............................................................................................. 1-18
1. INTRODUCTION ....................................................................................................... 21
2. METHODS ................................................................................................................ 22
3. HALT 2016 RESULTS ................................................................................................. 25
3.1 NATIONAL OVERVIEW ............................................................................................. 25
Description of Participating LTCF .................................................................................................. 25
Governance Structures ................................................................................................................. 27
3.2 HCAI ................................................................................................................. 40
MICROBIOLOGY RESULTS – PATHOGENS & ANTIMICROBIAL RESISTANCE ............................................ 45
4. PREVIOUS HALT SURVEYS ........................................................................................ 55
LTCF-ACQUIRED INFECTION (LAI): 2010 - 2016 ........................................................................ 55
ANTIMICROBIAL USE: 2010 - 2016 ......................................................................................... 57
5. DISCUSSION ............................................................................................................. 61
6. REFERENCES ............................................................................................................ 75
7. APPENDICES ............................................................................................................ 78
APPENDIX A: LIST OF HALT 2016 PARTICIPATING LTCF ............................................................... 78
HSE-OWNED LTCF, STRATIFIED BY CHO AND BY CARE TYPE ........................................................... 85
APPENDIX B: HALT 2016 NATIONAL STEERING GROUP MEMBERSHIP ............................................. 86
APPENDIX C: ACRONYMS USED IN THIS REPORT ........................................................................... 87
APPENDIX D: HALT RESIDENT QUESTIONNAIRE & HCAI DEFINITIONS .............................................. 90
APPENDIX E: COMMUNITY HEALTHCARE ORGANISATIONS (CHO) MAP OF IRELAND ............................. 94
HALT 2016 Ireland National Report 3
Acknowledgements
All of the HALT 2016 participating facilities are listed in Appendix A
The members of the HALT Steering Group (Appendix B) would like to sincerely acknowledge the
commitment of all healthcare staff who volunteered to participate and those who supported the
2016 HALT survey:
Local HALT coordinators
Local HALT data collectors
Long-term care facility nursing staff who assisted with completion of ward lists and resident
questionnaires
Long-term care facility directors of nursing and management staff
Infection prevention and control nursing staff who assisted with data collection
Clinicians and general practitioners who assisted with data collection
Community and long-term care facility pharmacy staff who assisted with data collection
Staff of the facility who volunteered as the HALT data validation site
Dr Nuala O’Connor, ICGP Lead for HCAI & AMR & member of HALT 2016 Steering Group
Ms Mary Wynne, Interim Nursing & Midwifery Services Director, HSE
Ms Deirdre Mulligan, Interim Area Director, Nursing & Midwifery Planning & Development,
HSE
Dr Darina O’Flanagan, Director HPSC (Retired May 2016)
Dr Kevin Kelleher, Assistant National Director, Health & Wellbeing – Health Protection, HSE
Dr Philip Crowley, HSE National Director, Quality Improvement Division
Ms Katrien Latour, HALT European Coordinating Team, Scientific Institute for Public Health
(WIV-ISP), Brussels, Belgium
Ms Béatrice Jans, HALT European Coordinating Team, Scientific Institute for Public Health
(WIV-ISP), Brussels, Belgium (Retired November 2016)
Dr Carl Suetens, Senior Expert Antimicrobial Resistance & Healthcare-Associated Infections,
European Centre for Disease Prevention & Control, Stockholm, Sweden
HALT 2016 Ireland National Report 4
Executive Summary
In May 2016, 10,044 residents in 224 Irish long-term care facilities (LTCF) were included in a
European point prevalence survey (PPS) of healthcare-associated infections (HCAI) and antimicrobial
use. The survey is also known as the HALT survey. This is the national report for Ireland.
Aims of the HALT survey
1. To calculate the prevalence of HCAI in residents of Irish LTCF
2. To calculate the prevalence of and indications for antimicrobial use in Irish LTCF
3. To provide the Irish Government, Department of Health, Health Service Executive (HSE), the
managers, doctors and nurses caring for residents in all of the participating LTCF with
information for action: to reduce the numbers of residents who develop HCAI and to
influence positive antimicrobial stewardship practices in LTCF
4. To provide residents, their families, friends, carers and members of the public with more
information about HCAI in Ireland and which types of infections are most commonly seen in
Irish LTCF
Participating LTCF
Of the 224 LTCF, the majority were owned by the HSE [n=136; 61%], followed by private
[n=54; 24%] and voluntary services [n=34; 15%]
The median capacity of participating LTCF was 42 beds (range = 5 – 176) and the median
bed occupancy on the HALT survey date was 93%
Overall, single room accommodation accounted for a median of 71% of available beds.
The proportion of single room accommodation in HSE-owned (52%) was lower than that
of private (83%) and voluntary (87%) LTCF
For the purposes of data analysis and reporting, the HALT steering group stratified the
224 LTCF into the following care type categories, based on the characteristics and
estimated length-of-stay (LOS) for the majority of the residents:
i. General nursing homes >12 months (GN>12m): 88 long-stay facilities with 4,722
residents
ii. Mixed care type facilities >12 months (Mixed>12m): 46 long-stay facilities with
2,499 residents
HALT 2016 Ireland National Report 5
iii. LTCF caring for residents with intellectual disabilities (Intellectually disabled): 31
long-stay facilities with 1,251 residents
iv. LTCF (either general nursing homes or mixed care type facilities) <12 months
(LTCF<12m): 14 short-stay facilities with 441 residents
v. LTCF caring for residents with psychiatric conditions (Psychiatric): 23 long-stay
facilities with 505 residents
vi. Other care types: Facilities caring for residents with palliative care needs (seven
long-stay facilities with 134 residents), rehabilitation needs (five long-stay facilities
with 245 residents), physical disabilities (one long-stay facilities with 13 residents)
and ‘other’ care types (nine long-stay facilities with 234 residents)
Nurse and healthcare assistant staffing, medical care and coordination, infection prevention &
control & antimicrobial stewardship
For the first time, HALT 2016 collected information on nurse and healthcare assistant
staffing ratios per 100 LTCF beds, with differences observed based on LTCF ownership and
LTCF care type. The observed staffing ratios do not necessarily reflect the national picture
for multiple reasons and additional information which directly influences staffing levels was
not collected (e.g., resident dependency and comorbidities)
Overall, resident medical care was provided by the resident’s own general practitioner (GP)
in 49.5%, by a directly-employed doctor in 28.5% and by a mix of GP plus directly-employed
doctor care in 22% of LTCF. However, when LTCF were stratified by ownership, GP-led
medical care was 96% in private LTCF versus 33% in HSE LTCF
A designated coordinating physician, with responsibility for coordination and standardisation
of policies/practices for resident medical care within the LTCF was available for 65% of LTCF
overall and for 56% of private LTCF
An active local infection prevention and control committee (IPCC) was reported by 61% of
LTCF
Access to a staff member with infection prevention and control (IPC) training was reported
by 76% of LTCF overall and by 57% of private LTCF. For the vast majority of LTCF with a
trained IPC staff member, that person was an infection prevention and control nurse (IPCN)
(93.5%). However, for the majority of LTCF (58%), the IPCN was not based in the LTCF on a
day-to-day basis
A written local hand hygiene policy was available in 95% of LTCF, with provision of a staff
hand hygiene training session in the past 12 months reported by 83% of LTCF. The available
HALT 2016 Ireland National Report 6
products for hand hygiene were alcohol-based hand rub (ABHR) and liquid soap in 96% and
95% of LTCF, respectively
Compliance with hand hygiene opportunities was not collected in HALT 2016
The provision of seasonal influenza vaccination for residents was not universal, with 9% of
LTCF overall reporting this was not routine local practice
The vast majority (98%) reported having no active local antimicrobial stewardship
committee (ASC), training on antimicrobial prescribing was not provided by 94% and 56% of
LTCF reported having no local antimicrobial prescribing guidelines
Prescriber feedback regarding local antimicrobial consumption was available in just 14% of
LTCF
LTCF with a designated coordinating physician were significantly more likely to demonstrate
positive local antimicrobial stewardship practices such as; an active ASC, training for
prescribers and local prescribing guidelines
Resident demographics, nursing care requirements and HCAI risk factors
Female residents predominated in most care types, other than psychiatric and palliative
LTCF. The proportion of residents aged ≥85 years was highest in GN>12m (49%), Mixed>12m
(47%) and LTCF<12m (41%). In contrast, 1% of intellectually disabled LTCF residents were
aged ≥ 85 years
Selected indicators of resident nursing care requirements (incontinence, disorientation and
impaired mobility) were evident in all care types, but most prevalent in GN>12m,
Mixed>12m and LTCF<12m
HCAI risk factors (presence of urinary or vascular catheter, pressure sores or ‘other’ wounds)
were most prevalent in palliative care LTCF
Almost two percent (n=170) of residents with an infection or taking antimicrobials, had a
history of hospitalisation within three months of the survey
LTCF-acquired infections (LAI)
For infections acquired in long-term care, the national crude prevalence was 4.4% and the
median prevalence was 3.4%. The median prevalence was higher in LTCF<12m (6.6%),
rehabilitation (4.9%) and mixed>12m (4.5%). The highest prevalence was reported in
palliative care LTCF (8.3%), which may reflect underlying illness and the prevalence of HCAI
risk factors encountered in that unique resident cohort
HALT 2016 Ireland National Report 7
The most prevalent LAI types were: respiratory tract infections (RTI), urinary tract infections
(UTI) and skin infections; affecting 1.5%, 1.5% and 1.1% of all residents, respectively
A relevant microbiological specimen had been obtained for 37% of infections, with
microorganisms isolated in 14%. Escherichia coli (35%) and Staphylococcus aureus (29%)
were the most frequently reported microorganisms. Of those with available antimicrobial
susceptibility results, 4% of E. coli were resistant to 3rd generation cephalosporins and 16%
of S. aureus were meticillin/flucloxacillin resistant (i.e., MRSA). There were no LAI associated
with carbapenem resistant Enterobacteriaceae (CRE) reported during the HALT survey
Hospital-acquired infections (HAI)
For the first time, HALT 2016 collected data on hospital-acquired infections (HAI), whereby
the resident was transferred to the LTCF with an active HAI or developed a HAI on day one
or day two following transfer to the LTCF. No HAI were reported by 88% of LTCF. The crude
national prevalence of HAI in Irish LTCF was 0.4%. Therefore, the vast majority of HCAI in
LTCF in Ireland are acquired within the LTCF
Antimicrobial use and antimicrobial resistance
The national crude antimicrobial use prevalence was 9.8%, with a median antimicrobial use
prevalence of 8.3%. The median prevalence was higher in LTCF<12m (12.1%) and
rehabilitation LTCF (10.9%). At 30.8%, the prevalence in palliative care LTCF was more similar
to that reported in acute hospitals
The majority of antimicrobials were prescribed within the LTCF (83%)
Overall, 59% of antimicrobials were prescribed to treat infection. However, antimicrobial
prophylaxis accounted for the majority of prescriptions in intellectually disabled LTCF (54%)
During HALT 2016, 3.4% of Mixed>12m and 3.1% of GN>12m residents were prescribed
antimicrobials for UTI prophylaxis. Prophylaxis against RTI was most prevalent in
intellectually disabled (2.0%) and palliative care (1.5%) LTCF

HALT 2016 Ireland National Report 8
Priorities for Implementation
There have been four HALT surveys conducted in Ireland since 2010. The findings of the most recent
survey in May 2016 demonstrates that HCAI and antimicrobial use remain prevalent issues in Irish
LTCF, regardless of the LTCF care type. The annual increase in LTCF participating in HALT is a positive
finding, with 96 LTCF performing their first HALT survey in 2016 and 39 having participated in all four
HALT surveys to date. There is now evidence that participation in repeated HALT surveys has
impacted positively on the prevalence of infection and antimicrobial use in 2016 for the 39 LTCF that
have completed all four HALT surveys, as shown in Figure 4.1.5. However, many Irish LTCF have yet
to undertake a HALT survey and participation in surveillance alone is not enough to drive sustained
improvement. The findings of the HALT surveys to date and the recommended priorities now need
to be implemented.
The existing gaps in resourcing have become acutely evident, in the context of a rapidly increasing
national incidence of antimicrobial resistant bacteria, such as multi-drug resistant Klebsiella
pneumoniae (MDRKP) and carbapenem resistant Enterobacteriaceae (CRE), with cases and
outbreaks in Irish LTCF reported. For HSE-owned LTCF, the development of an Accountability
Framework for Quality & Safety within the Social Care Division is welcomed and has potential to
drive the implementation of many of the recommendations for HSE Social Care Division within this
HALT report. However, the delivery of residential care in Ireland is not limited to services provided
by the HSE and antimicrobial resistant bacteria will not respect boundaries of services providers.
Therefore, it is vitally important that implementation of the recommended priorities and investment
in resources ensures that residents in all Irish LTCF, regardless of care type and ownership have
equitable access to the specialist input of multi-disciplinary infection prevention and control and
antimicrobial stewardship teams and geriatricians with community input and that regional HCAI &
antimicrobial resistance (AMR) Committees are established in each community healthcare
organisation (CHO), with membership, governance and oversight including all LTCF, regardless of
ownership.
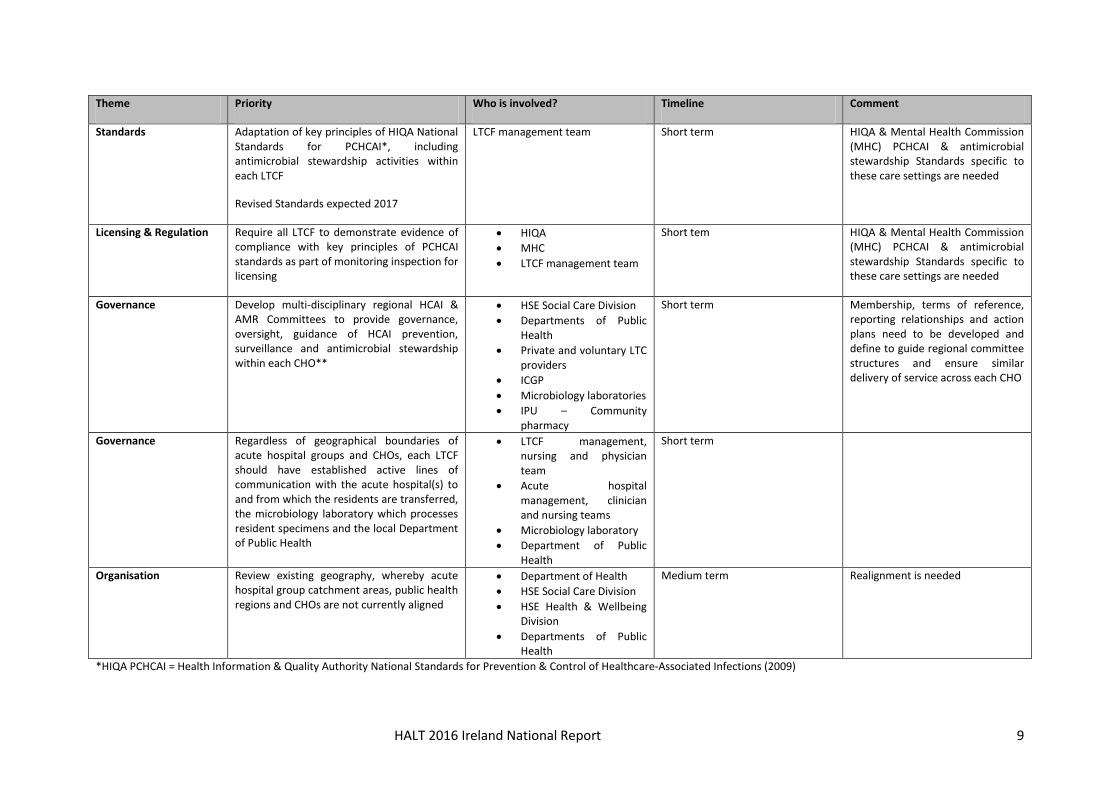
The recommended priorities for implementation arising from the findings of HALT 2016 are outlined
in the following tables. For each theme, the column describing ‘who is involved’ in delivering on
implementation is not intended to restrict participation and will require more in-depth discussion to
attribute ownership on publication of this report. Within the tables, LTCF management team refers
to all LTCF, regardless of care type or ownership.
HALT 2016 Ireland National Report 9
Theme Priority Who is involved? Timeline Comment
Standards Adaptation of key principles of HIQA National Standards for PCHCAI*, including antimicrobial stewardship activities within each LTCF
Revised Standards expected 2017
LTCF management team Short term HIQA & Mental Health Commission (MHC) PCHCAI & antimicrobial stewardship Standards specific to these care settings are needed
Licensing & Regulation Require all LTCF to demonstrate evidence of compliance with key principles of PCHCAI standards as part of monitoring inspection for licensing
HIQA
MHC
LTCF management team
Short tem HIQA & Mental Health Commission (MHC) PCHCAI & antimicrobial stewardship Standards specific to these care settings are needed
Governance Develop multi-disciplinary regional HCAI & AMR Committees to provide governance, oversight, guidance of HCAI prevention, surveillance and antimicrobial stewardship within each CHO**
HSE Social Care Division
Departments of Public Health
Private and voluntary LTC providers
ICGP
Microbiology laboratories
IPU – Community pharmacy
Short term Membership, terms of reference, reporting relationships and action plans need to be developed and define to guide regional committee structures and ensure similar delivery of service across each CHO
Governance Regardless of geographical boundaries of acute hospital groups and CHOs, each LTCF should have established active lines of communication with the acute hospital(s) to and from which the residents are transferred, the microbiology laboratory which processes resident specimens and the local Department of Public Health
LTCF management, nursing and physician team
Acute hospital management, clinician and nursing teams
Microbiology laboratory
Department of Public Health
Short term
Organisation Review existing geography, whereby acute hospital group catchment areas, public health regions and CHOs are not currently aligned
Department of Health
HSE Social Care Division
HSE Health & Wellbeing Division
Departments of Public Health
Medium term Realignment is needed
*HIQA PCHCAI = Health Information & Quality Authority National Standards for Prevention & Control of Healthcare-Associated Infections (2009)
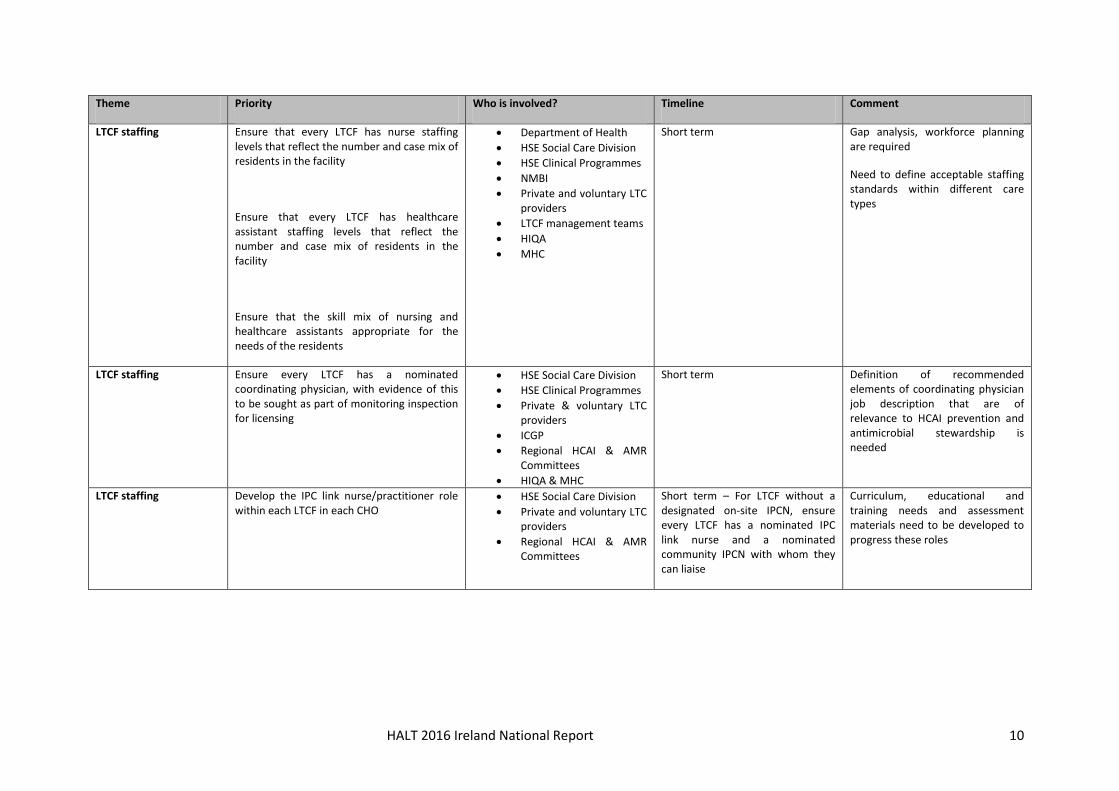
HALT 2016 Ireland National Report 10
Theme Priority Who is involved? Timeline Comment
LTCF staffing Ensure that every LTCF has nurse staffing levels that reflect the number and case mix of residents in the facility
Ensure that every LTCF has healthcare assistant staffing levels that reflect the number and case mix of residents in the facility
Ensure that the skill mix of nursing and healthcare assistants appropriate for the needs of the residents
Department of Health
HSE Social Care Division
HSE Clinical Programmes
NMBI
Private and voluntary LTC providers
LTCF management teams
HIQA
MHC
Short term Gap analysis, workforce planning are required
Need to define acceptable staffing standards within different care types
LTCF staffing Ensure every LTCF has a nominated coordinating physician, with evidence of this to be sought as part of monitoring inspection for licensing
HSE Social Care Division
HSE Clinical Programmes
Private & voluntary LTC providers
ICGP
Regional HCAI & AMR Committees
HIQA & MHC
Short term Definition of recommended elements of coordinating physician job description that are of relevance to HCAI prevention and antimicrobial stewardship is needed
LTCF staffing Develop the IPC link nurse/practitioner role within each LTCF in each CHO
HSE Social Care Division
Private and voluntary LTC providers
Regional HCAI & AMR Committees
Short term – For LTCF without a designated on-site IPCN, ensure every LTCF has a nominated IPC link nurse and a nominated community IPCN with whom they can liaise
Curriculum, educational and training needs and assessment materials need to be developed to progress these roles
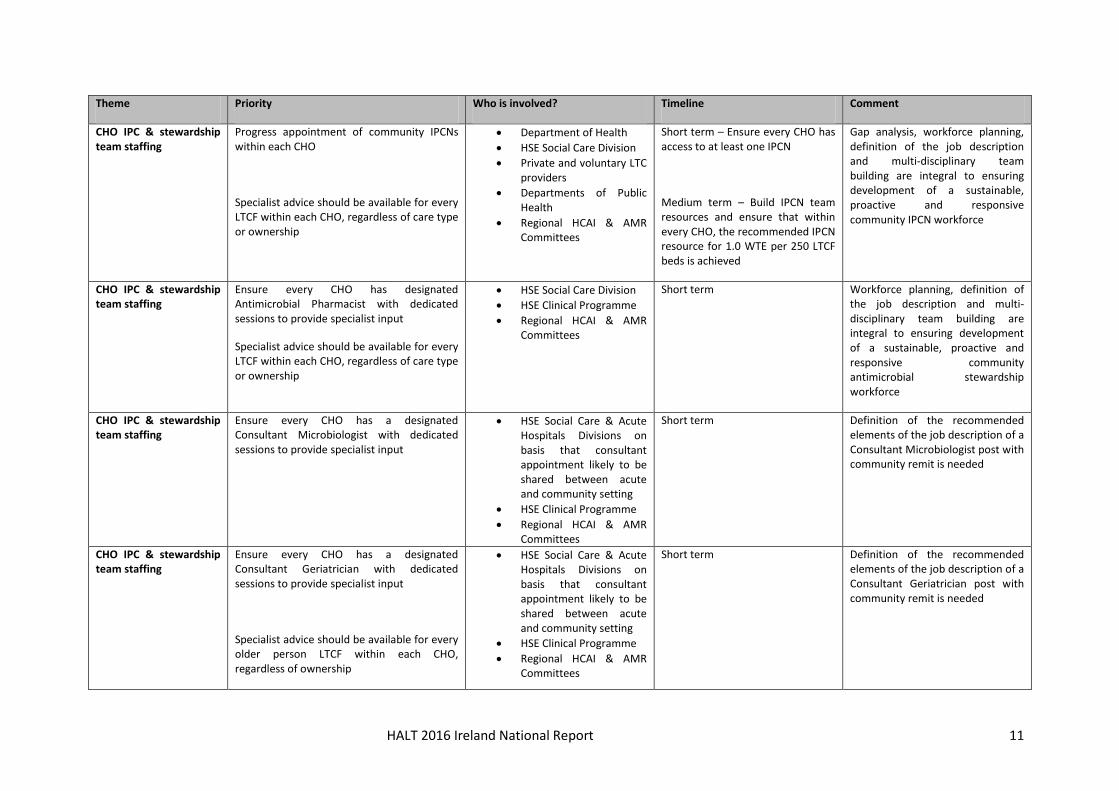
HALT 2016 Ireland National Report 11
Theme Priority Who is involved? Timeline Comment
CHO IPC & stewardship team staffing
Progress appointment of community IPCNs within each CHO
Specialist advice should be available for every LTCF within each CHO, regardless of care type or ownership
Department of Health
HSE Social Care Division
Private and voluntary LTC providers
Departments of Public Health
Regional HCAI & AMR Committees
Short term – Ensure every CHO has access to at least one IPCN
Medium term – Build IPCN team resources and ensure that within every CHO, the recommended IPCN resource for 1.0 WTE per 250 LTCF beds is achieved
Gap analysis, workforce planning, definition of the job description and multi-disciplinary team building are integral to ensuring development of a sustainable, proactive and responsive community IPCN workforce
CHO IPC & stewardship team staffing
Ensure every CHO has designated Antimicrobial Pharmacist with dedicated sessions to provide specialist input
Specialist advice should be available for every LTCF within each CHO, regardless of care type or ownership
HSE Social Care Division
HSE Clinical Programme
Regional HCAI & AMR Committees
Short term Workforce planning, definition of the job description and multi-disciplinary team building are integral to ensuring development of a sustainable, proactive and responsive community antimicrobial stewardship workforce
CHO IPC & stewardship team staffing
Ensure every CHO has a designated Consultant Microbiologist with dedicated sessions to provide specialist input
HSE Social Care & Acute Hospitals Divisions on basis that consultant appointment likely to be shared between acute and community setting
HSE Clinical Programme
Regional HCAI & AMR Committees
Short term Definition of the recommended elements of the job description of a Consultant Microbiologist post with community remit is needed
CHO IPC & stewardship team staffing
Ensure every CHO has a designated Consultant Geriatrician with dedicated sessions to provide specialist input
Specialist advice should be available for every older person LTCF within each CHO, regardless of ownership
HSE Social Care & Acute Hospitals Divisions on basis that consultant appointment likely to be shared between acute and community setting
HSE Clinical Programme
Regional HCAI & AMR Committees
Short term Definition of the recommended elements of the job description of a Consultant Geriatrician post with community remit is needed
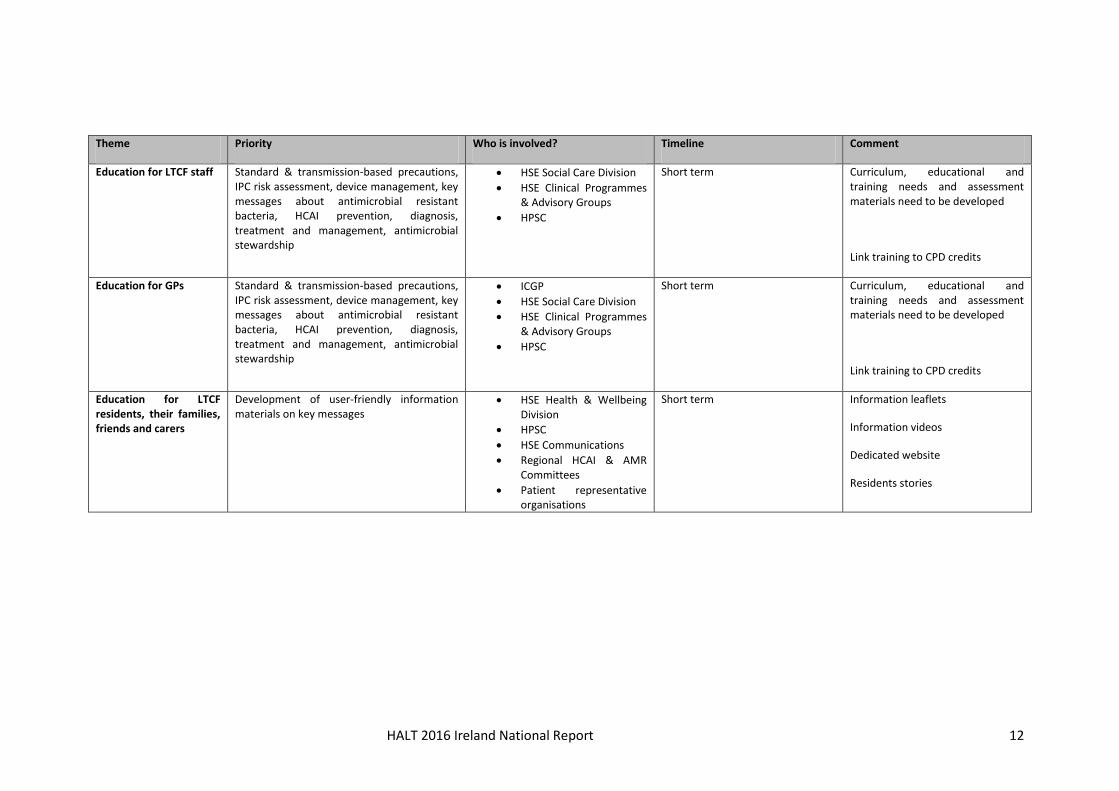
HALT 2016 Ireland National Report 12
Theme Priority Who is involved? Timeline Comment
Education for LTCF staff Standard & transmission-based precautions, IPC risk assessment, device management, key messages about antimicrobial resistant bacteria, HCAI prevention, diagnosis, treatment and management, antimicrobial stewardship
HSE Social Care Division
HSE Clinical Programmes & Advisory Groups
HPSC
Short term Curriculum, educational and training needs and assessment materials need to be developed
Link training to CPD credits
Education for GPs Standard & transmission-based precautions, IPC risk assessment, device management, key messages about antimicrobial resistant bacteria, HCAI prevention, diagnosis, treatment and management, antimicrobial stewardship
ICGP
HSE Social Care Division
HSE Clinical Programmes & Advisory Groups
HPSC
Short term Curriculum, educational and training needs and assessment materials need to be developed
Link training to CPD credits
Education for LTCF residents, their families, friends and carers
Development of user-friendly information materials on key messages
HSE Health & Wellbeing Division
HPSC
HSE Communications
Regional HCAI & AMR Committees
Patient representative organisations
Short term Information leaflets
Information videos
Dedicated website
Residents stories
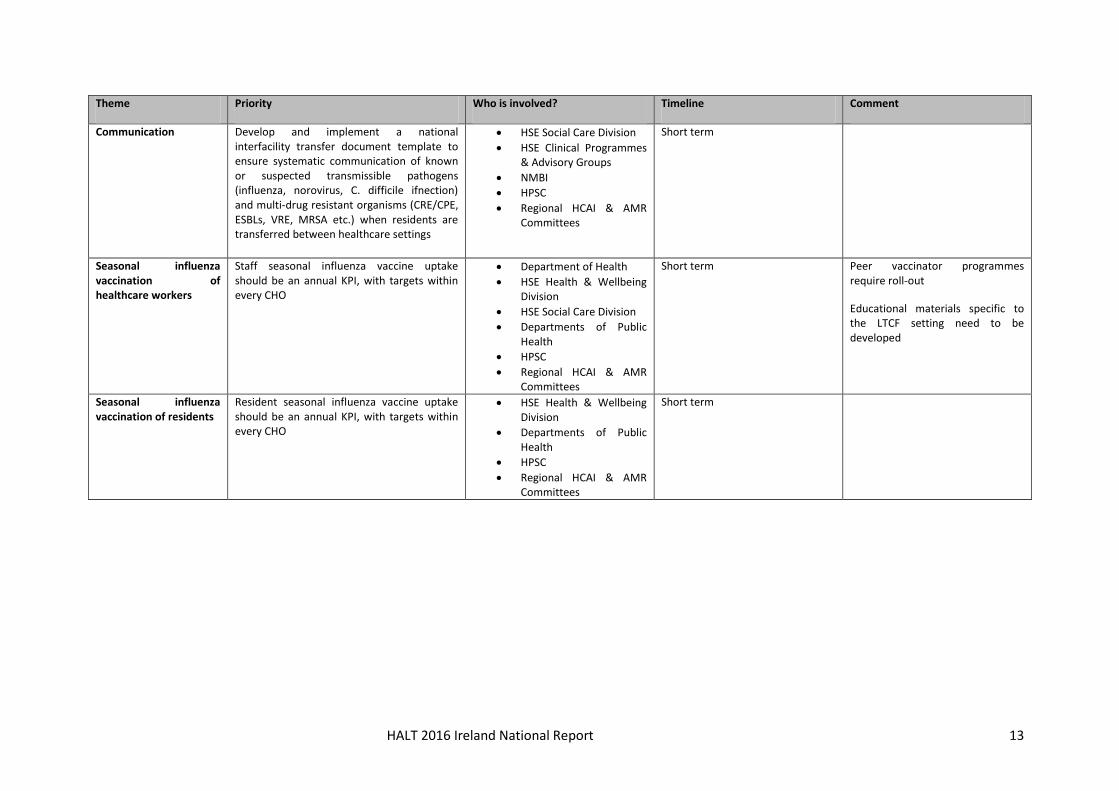
HALT 2016 Ireland National Report 13
Theme Priority Who is involved? Timeline Comment
Communication Develop and implement a national interfacility transfer document template to ensure systematic communication of known or suspected transmissible pathogens (influenza, norovirus, C. difficile ifnection) and multi-drug resistant organisms (CRE/CPE, ESBLs, VRE, MRSA etc.) when residents are transferred between healthcare settings
HSE Social Care Division
HSE Clinical Programmes & Advisory Groups
NMBI
HPSC
Regional HCAI & AMR Committees
Short term
Seasonal influenza vaccination of healthcare workers
Staff seasonal influenza vaccine uptake should be an annual KPI, with targets within every CHO
Department of Health
HSE Health & Wellbeing Division
HSE Social Care Division
Departments of Public Health
HPSC
Regional HCAI & AMR Committees
Short term Peer vaccinator programmes require roll-out
Educational materials specific to the LTCF setting need to be developed
Seasonal influenza vaccination of residents
Resident seasonal influenza vaccine uptake should be an annual KPI, with targets within every CHO
HSE Health & Wellbeing Division
Departments of Public Health
HPSC
Regional HCAI & AMR Committees
Short term
HALT 2016 Ireland National Report 14
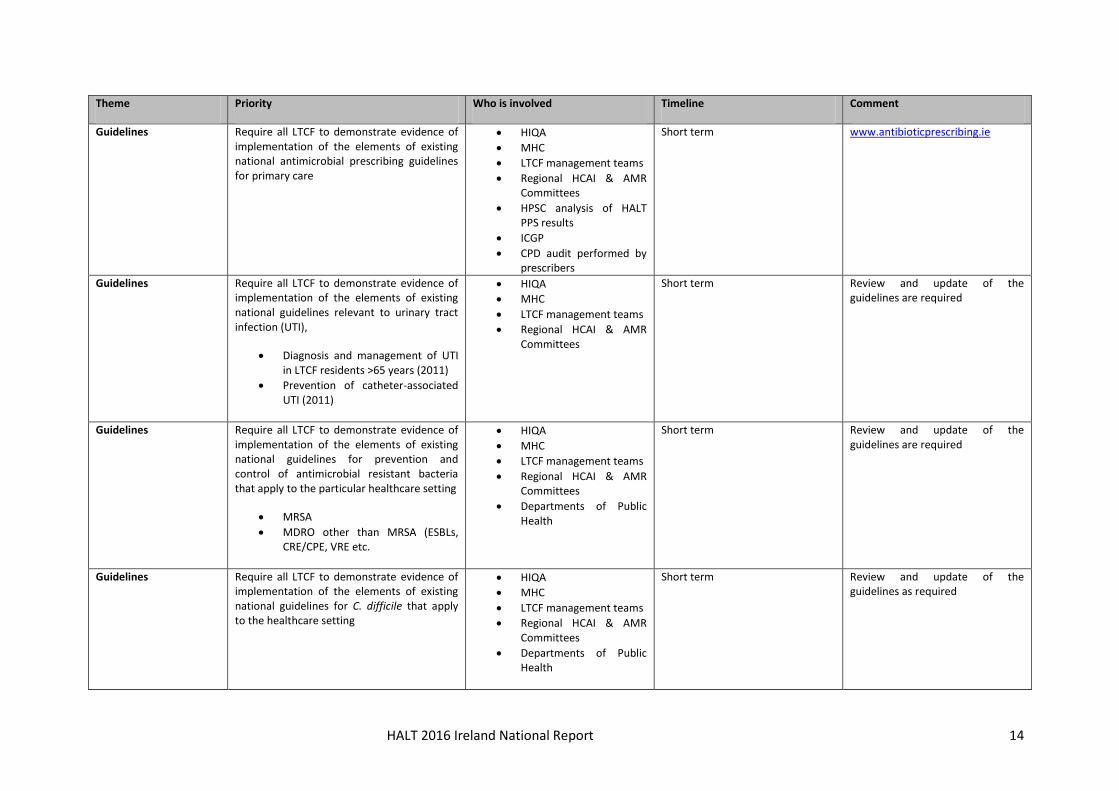
Theme Priority Who is involved Timeline Comment
Guidelines Require all LTCF to demonstrate evidence of implementation of the elements of existing national antimicrobial prescribing guidelines for primary care
HIQA
MHC
LTCF management teams
Regional HCAI & AMR Committees
HPSC analysis of HALT PPS results
ICGP
CPD audit performed by prescribers
Short term www.antibioticprescribing.ie
Guidelines Require all LTCF to demonstrate evidence of implementation of the elements of existing national guidelines relevant to urinary tract infection (UTI),
Diagnosis and management of UTI in LTCF residents >65 years (2011)
Prevention of catheter-associated UTI (2011)
HIQA
MHC
LTCF management teams
Regional HCAI & AMR Committees
Short term Review and update of the guidelines are required
Guidelines Require all LTCF to demonstrate evidence of implementation of the elements of existing national guidelines for prevention and control of antimicrobial resistant bacteria that apply to the particular healthcare setting
MRSA
MDRO other than MRSA (ESBLs, CRE/CPE, VRE etc.
HIQA
MHC
LTCF management teams
Regional HCAI & AMR Committees
Departments of Public Health
Short term Review and update of the guidelines are required
Guidelines Require all LTCF to demonstrate evidence of implementation of the elements of existing national guidelines for C. difficile that apply to the healthcare setting
HIQA
MHC
LTCF management teams
Regional HCAI & AMR Committees
Departments of Public Health
Short term Review and update of the guidelines as required
HALT 2016 Ireland National Report 15
Theme Priority Who is involved Timeline Comment
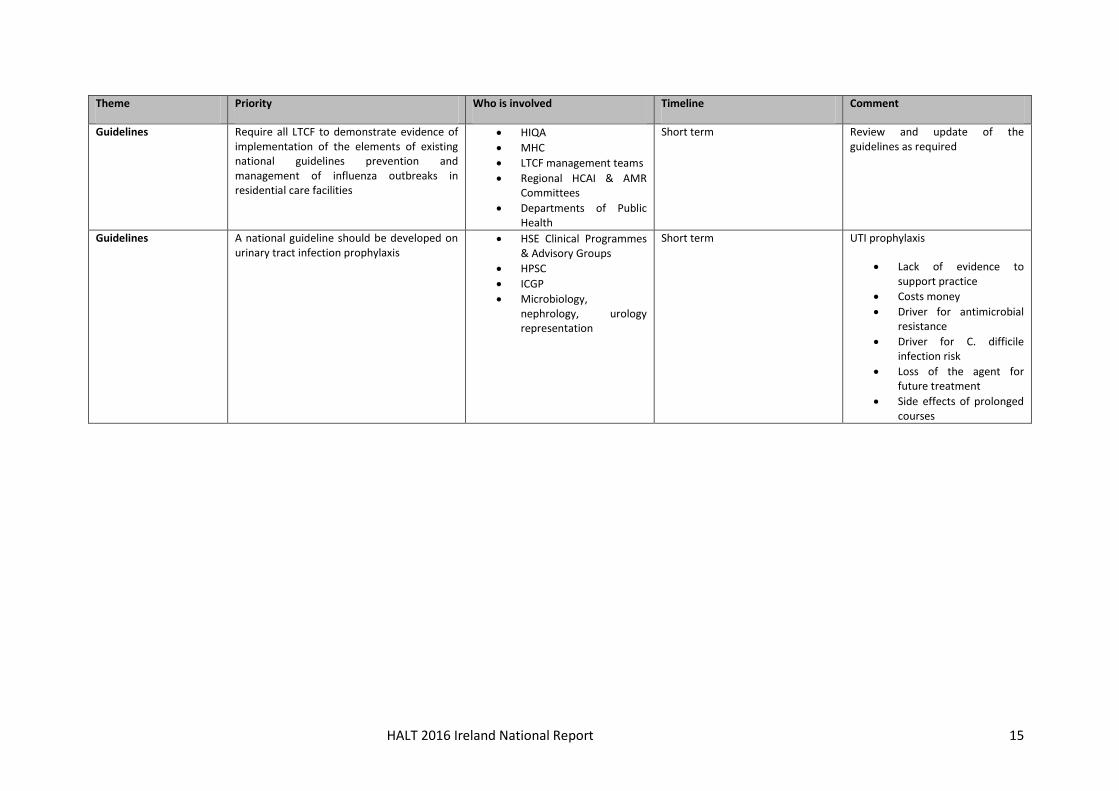
Guidelines Require all LTCF to demonstrate evidence of implementation of the elements of existing national guidelines prevention and management of influenza outbreaks in residential care facilities
HIQA
MHC
LTCF management teams
Regional HCAI & AMR Committees
Departments of Public Health
Short term Review and update of the guidelines as required
Guidelines A national guideline should be developed on urinary tract infection prophylaxis
HSE Clinical Programmes & Advisory Groups
HPSC
ICGP
Microbiology, nephrology, urology representation
Short term UTI prophylaxis
Lack of evidence to support practice
Costs money
Driver for antimicrobial resistance
Driver for C. difficile infection risk
Loss of the agent for future treatment
Side effects of prolonged courses
HALT 2016 Ireland National Report 16
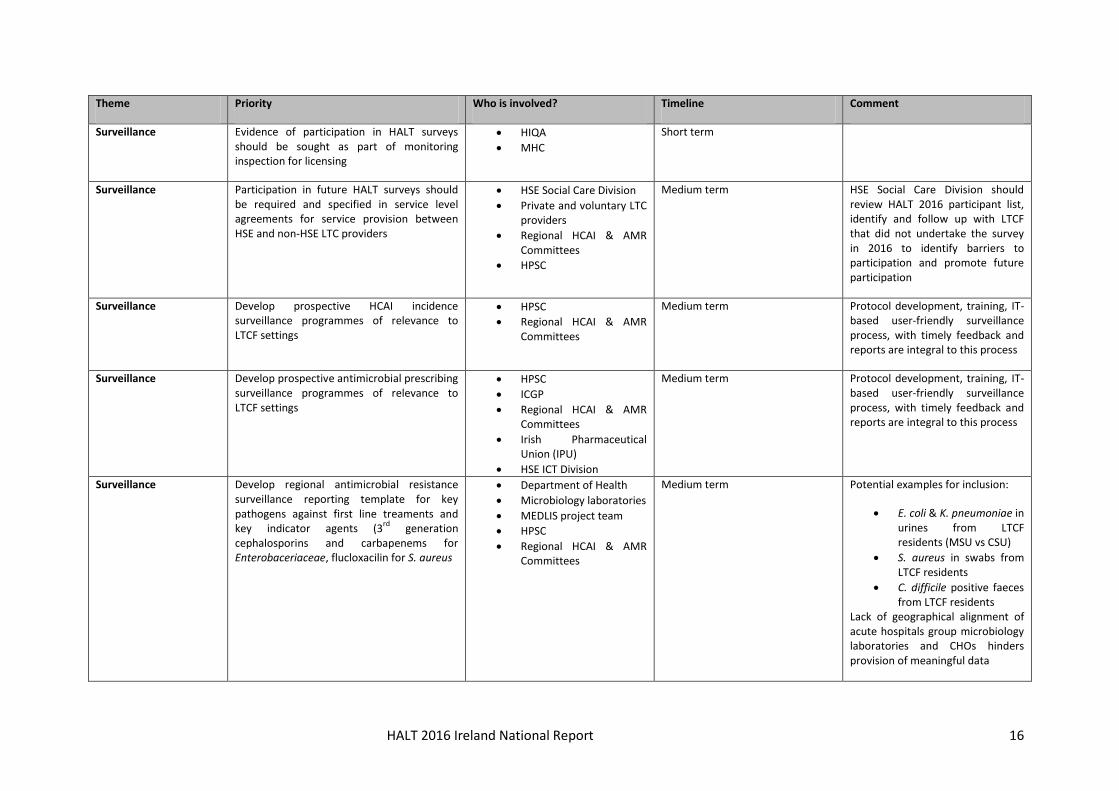
Theme Priority Who is involved? Timeline Comment
Surveillance Evidence of participation in HALT surveys should be sought as part of monitoring inspection for licensing
HIQA
MHC
Short term
Surveillance Participation in future HALT surveys should be required and specified in service level agreements for service provision between HSE and non-HSE LTC providers
HSE Social Care Division
Private and voluntary LTC providers
Regional HCAI & AMR Committees
HPSC
Medium term HSE Social Care Division should review HALT 2016 participant list, identify and follow up with LTCF that did not undertake the survey in 2016 to identify barriers to participation and promote future participation
Surveillance Develop prospective HCAI incidence surveillance programmes of relevance to LTCF settings
HPSC
Regional HCAI & AMR Committees
Medium term Protocol development, training, IT-based user-friendly surveillance process, with timely feedback and reports are integral to this process
Surveillance Develop prospective antimicrobial prescribing surveillance programmes of relevance to LTCF settings
HPSC
ICGP
Regional HCAI & AMR Committees
Irish Pharmaceutical Union (IPU)
HSE ICT Division
Medium term Protocol development, training, IT-based user-friendly surveillance process, with timely feedback and reports are integral to this process
Surveillance
Develop regional antimicrobial resistance surveillance reporting template for key pathogens against first line treaments and key indicator agents (3
rd generation
cephalosporins and carbapenems for Enterobaceriaceae, flucloxacilin for S. aureus
Department of Health
Microbiology laboratories
MEDLIS project team
HPSC
Regional HCAI & AMR Committees
Medium term Potential examples for inclusion:
E. coli & K. pneumoniae in urines from LTCF residents (MSU vs CSU)
S. aureus in swabs from LTCF residents
C. difficile positive faeces from LTCF residents
Lack of geographical alignment of acute hospitals group microbiology laboratories and CHOs hinders provision of meaningful data
HALT 2016 Ireland National Report 17
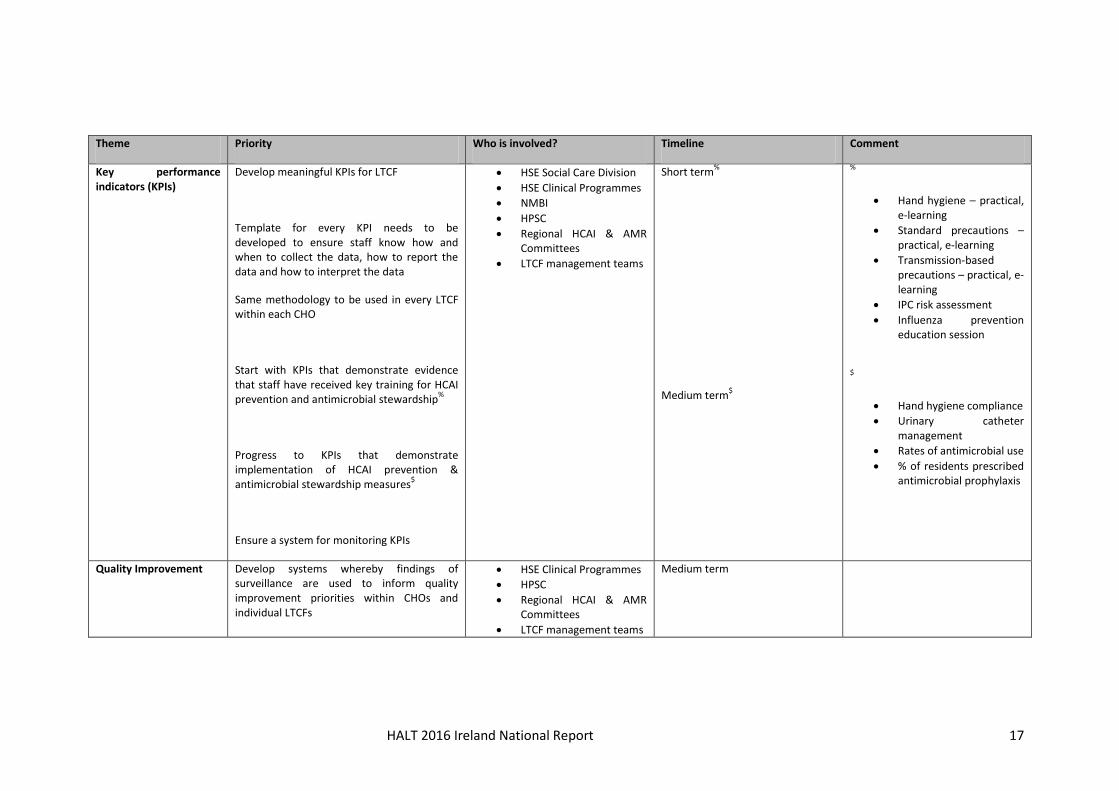
Theme Priority Who is involved? Timeline Comment
Key performance indicators (KPIs)
Develop meaningful KPIs for LTCF
Template for every KPI needs to be developed to ensure staff know how and when to collect the data, how to report the data and how to interpret the data
Same methodology to be used in every LTCF within each CHO
Start with KPIs that demonstrate evidence that staff have received key training for HCAI prevention and antimicrobial stewardship
%
Progress to KPIs that demonstrate implementation of HCAI prevention & antimicrobial stewardship measures
$
Ensure a system for monitoring KPIs
HSE Social Care Division
HSE Clinical Programmes
NMBI
HPSC
Regional HCAI & AMR Committees
LTCF management teams
Short term%
Medium term$
%
Hand hygiene – practical, e-learning
Standard precautions – practical, e-learning
Transmission-based precautions – practical, e-learning
IPC risk assessment
Influenza prevention education session
$
Hand hygiene compliance
Urinary catheter management
Rates of antimicrobial use
% of residents prescribed antimicrobial prophylaxis
Quality Improvement Develop systems whereby findings of surveillance are used to inform quality improvement priorities within CHOs and individual LTCFs
HSE Clinical Programmes
HPSC
Regional HCAI & AMR Committees
LTCF management teams
Medium term
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Plain Language Summary 18
Plain Language Summary
Background
During May 2016, 224 Irish long-term care facilities (LTCF) took part in a European survey known as
the HALT survey. It was coordinated in Ireland by the Health Protection Surveillance Centre (HPSC).
The HPSC is the national centre for the surveillance of infections in Ireland. An invitation to
participate in the HALT survey has been extended to all European Union countries.
During April 2016, staff members from the LTCF went to a training day, where they were taught how
to perform the survey. The survey was then carried out in each LTCF, using the same set of
instructions. Once the survey was completed, the results from each LTCF were collected and
checked at the HPSC. The results have been put together to produce this national report for Ireland.
The results for every LTCF that took part have also been returned to each individual LTCF, so they
can be used to help the staff to make future plans to further improve resident care.
The HALT survey was done for the following reasons:
1. To count the number of residents with an infection, which may have occurred as a result of
healthcare: so-called ‘healthcare associated infection’ or HCAI for short
2. To count the number of residents who were prescribed antibiotics
3. To provide the Irish Government, Department of Health, Health Service Executive, the
managers, doctors and nurses in all of the LTCF that took part, with information about HCAI
and antibiotic prescribing in Irish LTCF in 2016 and to compare progress since the HALT
survey was last undertaken in Ireland in 2013. This information is important to plan future
ways to reduce the numbers of residents who get HCAI and to reduce the chance that
antibiotics may be prescribed unnecessarily
4. To provide residents, their families, friends, carers and members of the public with more
information about HCAI in Ireland and which types of infections are most commonly seen in
Irish LTCF
The count of the residents with a HCAI and the residents prescribed antibiotics is called ‘prevalence’.
These results provide us with a picture or a snapshot of the number of residents with a HCAI and the
number of residents prescribed antimicrobials in the Irish LTCF that took part in the HALT survey in
May 2016.
In this report, each of the participating LTCF has been categorised into commonly encountered care
types, based on the typical characteristics and length-of-stay for the majority of residents in the
LTCF: The most common LTCF care types in Ireland are: general nursing homes (long-stay), mixed
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Plain Language Summary 19
care type LTCF (long-stay), LTCF where the majority of residents stay for less than 12 months (short-
stay), intellectually disabled LTCF, psychiatric LTCF, rehabilitation LTCF and palliative care LTCF.
Long-term care facility-acquired infections
These are infections that developed more than two days after a resident was admitted to the LTCF.
Such infections are important because they can cause harm to residents. Not every infection can be
prevented from happening, but every opportunity should be taken to prevent infection, whenever
possible.
In Ireland, there were 10,044 residents counted in 224 LTCF. Of those, 441 had a LTCF-acquired
infection at the time of the survey. This means that 4.4% or just under one-in-twenty residents
present in Irish LTCF in May 2016 had a LTCF-acquired infection. However, because different LTCF
may care for different types of residents, it is not possible to directly compare the results of one
LTCF with those of another LTCF.
The most common types of infections reported in the survey were as follows:
1. Respiratory tract infections, which may include chest infections and pneumonia
2. Urinary tract infections, which may include infections of the bladder or kidneys
3. Skin or wound infections
In this survey, it was found that residents who had an infection were more likely to have some of the
common ‘risk factors’. Well-known risk factors for developing infection can include: having had a
recent operation, having a drip or a bladder catheter and being older. Three LTCF residents were
reported to have acquired Clostridium difficile infection during the HALT survey.
Antibiotic use
Antibiotics are extremely important to treat infection caused by bacteria. There is concern around
the world that bacteria are becoming more and more resistant to antibiotics, so they no longer work
to treat common infections. This problem is made worse by the fact that there have been very few
new types of antibiotics developed to overcome this problem of resistance. It is very important that
antibiotics are only used when they are absolutely necessary and that they are not used in the
incorrect circumstances, such as to try and treat infections caused by viruses. It is also very
important that antibiotics are not used for too long and that the course of treatment is kept as short
as possible.
This survey found that of the 10,044 residents who were counted, 981 were prescribed antibiotics.
This means that 9.8% or about one-in-ten residents present in Irish LTCF in May 2016 were taking an

PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Plain Language Summary 20
antibiotic. However, because different LTCF may care for different types of residents, it is not
possible to directly compare the results of one LTCF with those of another LTCF.
This survey shows that antibiotic prescribing is common in Irish LTCF. Most residents were
prescribed antibiotics to treat infection. However, a proportion of residents were prescribed
antibiotics to prevent infection, which is also known as prophylaxis. Most antibiotic prophylaxis was
prescribed to prevent urinary tract infection. The results of the survey show that it is very important
to make sure that antibiotic prescribing in LTCF is done properly and that antibiotics are prescribed
appropriately. This in turn, will reduce the chances of antibiotic resistant bacteria becoming
commonplace in Irish LTCF, reduce the risk of residents picking up Clostridium difficile infection and
preserve the use of antibiotics for treatment of infection in residents in the future.

PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Introduction 21
1. Introduction
This report outlines the findings of the fourth national survey conducted in May 2016 to assess the
prevalence of HCAI and antimicrobial prescribing practices in Irish LTCF. Irish LTCF first participated
in a European-wide PPS of HCAI in long-term care facilites (HALT) in 2010. (1-3) In 2011, Ireland
repeated a national HALT survey. (4) The third HALT survey in Ireland and the second European HALT
survey took place during May 2013. (5-6)
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Methods 22
2. Methods
The HALT survey in Europe is coordinated by the European Centre for Disease Prevention & Control
(ECDC) and the Scientific Institute of Public Health (WIV-ISP), Brussels, Belgium. The HALT survey in
Ireland is coordinated by the Health Protection Surveillance Centre (HPSC) and was overseen by a
multi-disciplinary steering group convened in January 2016, under the auspices of the Royal College
of Physicians of Ireland (RCPI) Clinical Advisory Group on HCAI & AMR (Appendix B). The steering
group met on four occasions between January and October 2016 to plan for the HALT survey and the
report of its findings.
In January 2016, an invitation to participate in HALT was extended to LTCF by HPSC. Participation
was voluntary. However, at least one person from each participating LTCF was required to attend a
training day. During April 2016, 214 healthcare workers attended one of six regional training days to
learn about the survey protocol and methodology. The schedule of presentations for each training
day included; an introduction to HALT survey methodology, presentations and practical case studies
to enable trainees to practice completion of the HALT data collection forms (Appendix D). All
training materials were posted on the HALT section of the HPSC website. A dedicated HALT e-mail
address was established to address any queries from participants. A frequently-asked questions
section was also maintained on the HPSC website. Information leaflets were prepared for residents
and their families, friends or carers, for LTCF staff and General Practitioners (GPs).
The survey was conducted using a standard protocol devised by the European HALT Coordinating
Team. The European HALT protocol was adapted for use in Ireland. All study documentation related
to HALT 2016, including protocol and data collection forms were posted on a dedicated HALT section
of the HPSC website:
http://www.hpsc.ie/hpsc/A-
Z/MicrobiologyAntimicrobialResistance/InfectionControlandHAI/Surveillance/HCAIinlongtermcarefa
cilities/
During the HALT survey, all eligible residents in each LTCF were surveyed by a local HALT team for
anonymous demographic details, risk factors, antimicrobial use and the presence of an active HCAI.
HCAI were defined using standardised infection definitions. The McGeer criteria for defining HCAI in
LTCF were published in 1991. (7) They have not been formally validated. In 2009, the Society for
Healthcare Epidemiology of America (SHEA) and the US Centers for Disease Control & Prevention
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Methods 23
(CDC) convened a multi-disciplinary group to update the McGeer criteria by systematic review of
literature. (8) Most studies evaluated were small observational or uncontrolled case series and
evidence was generally judged to be of low quality. Therefore, grading of evidence was not done and
the updated criteria require validation in different types of LTCF. The revised criteria incorporate
changes to surveillance definitions of UTI and RTI and added new categories for norovirus
gastroenteritis and Clostridium difficile infection (CDI). (8)
Similar to previous HALT surveys performed in 2010, 2011 and 2013, participants in HALT 2016 were
required to record all relevant signs and symptoms on a resident questionnaire. For HALT 2010 and
2011, the McGeer criteria were adapted to include the criterion ‘physician diagnosis’. In earlier HALT
surveys, the HALT software analysed recorded signs and symptoms and reported the presence or
absence of a HCAI according to the McGeer criteria. However, in 2013 and 2016, participants were
required to follow algorithms on the resident questionnaire and decide for themselves whether a
HCAI was present or absent using the revised CDC/SHEA definitions. (Appendix D – Resident
Questionnaire).
For the first time in 2016, the HALT survey also collected information on hospital-acquired infections
(HAI), whereby a resident returned from the hospital to complete their HAI treatment course in the
LTCF or developed signs and symptoms meeting surveillance criteria for infection on day one or day
two following transfer to the LTCF. As a HAI, surgical site infection (SSI) was added as a separate
infection type to the HALT 2016 protocol. Specific definitions for timing of infection acquisition were
also utilised for CDI and SSI.
For the purposes of this report, healthcare-associated infections (HCAI) are subdivided into two
separate categories:
1. Long-term care facility (LTCF)-acquired infections (LAI) – Collected in all HALT surveys to date
2. Hospital-acquired infections (HAI) – Collected in HALT 2016 only
In prior HALT surveys, whenever an antimicrobial was prescribed, information was sought regarding
whether or not a relevant microbiological sample had been taken from the resident prior to starting
the antimicrobial. In HALT 2016, the protocol changed, whereby information on microbiology
samples was sought only on residents who fulfilled a HCAI surveillance definition. Therefore, the
microbiology findings from 2016 are not comparable with those of previous HALT surveys.
A local HALT report was issued by HPSC to each of the 224 participating LTCF by November 2016.

PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Methods 24
Data Management & Analysis
Data were collected on paper forms (Appendix D) and subsequently entered electronically to a
downloadable software application. The completed data file was returned electronically from each
participating LTCF to HPSC.
The complete dataset from Ireland was also returned to the HALT European Coordinating Team for
inclusion in the European HALT analysis and report, which is expected to be published in 2018.
Data was analysed using Microsoft Access and Excel. Statistical analysis were carried out using
STATA/SE v11.2 and OpenEpi v3.01. ArcView GIS v3.2 was used for data mapping.
Data Validation
Ireland also contributed HALT data to a European validation study. This was designed to validate the
HALT data collection across Europe. During May 2016, two members of the HALT national
coordinating team visited one LTCF and conducted a parallel HALT survey. The anonymous data
collected simultaneously by the local HALT team and the validation team were returned for inclusion
in the European HALT validation analysis and report.
Of 224 LTCF, 35 (16%) reported that a local physician had been involved in validating the data
collected on residents who were prescribed antimicrobials and/or who had signs or symptoms
suggestive of an active HCAI.
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 25
3. HALT 2016 Results
3.1 National Overview
Description of Participating LTCF
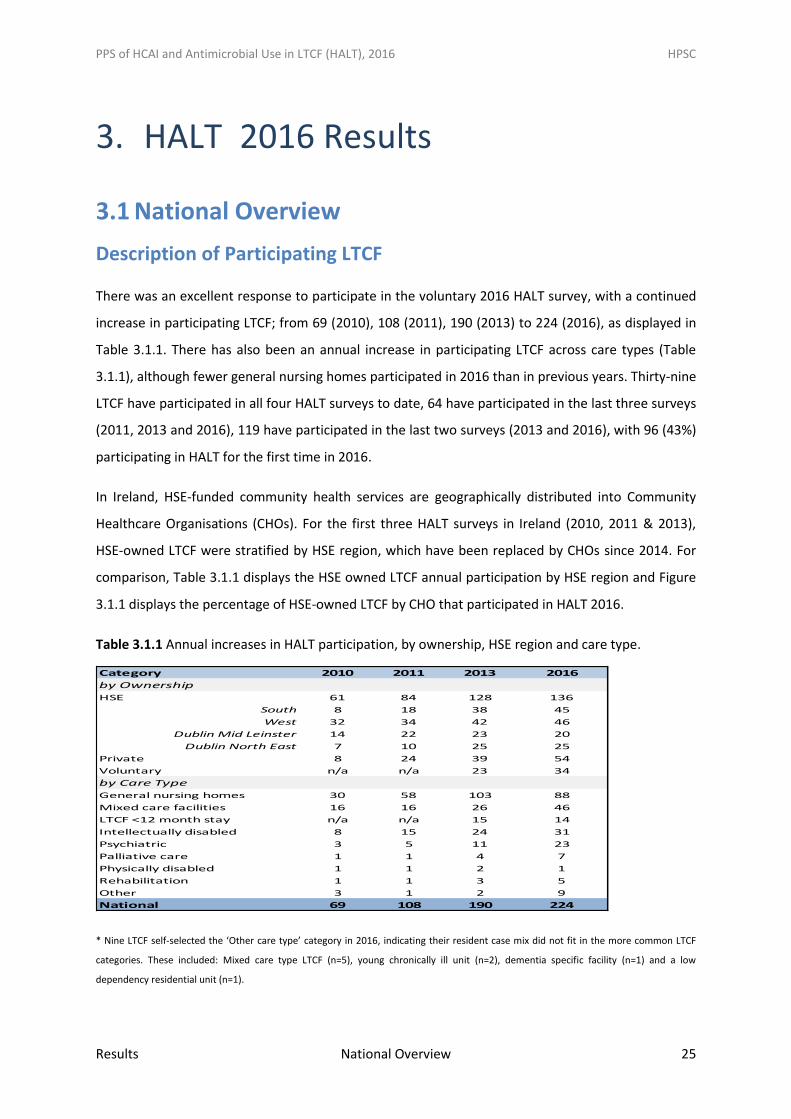
There was an excellent response to participate in the voluntary 2016 HALT survey, with a continued
increase in participating LTCF; from 69 (2010), 108 (2011), 190 (2013) to 224 (2016), as displayed in
Table 3.1.1. There has also been an annual increase in participating LTCF across care types (Table
3.1.1), although fewer general nursing homes participated in 2016 than in previous years. Thirty-nine
LTCF have participated in all four HALT surveys to date, 64 have participated in the last three surveys
(2011, 2013 and 2016), 119 have participated in the last two surveys (2013 and 2016), with 96 (43%)
participating in HALT for the first time in 2016.
In Ireland, HSE-funded community health services are geographically distributed into Community
Healthcare Organisations (CHOs). For the first three HALT surveys in Ireland (2010, 2011 & 2013),
HSE-owned LTCF were stratified by HSE region, which have been replaced by CHOs since 2014. For
comparison, Table 3.1.1 displays the HSE owned LTCF annual participation by HSE region and Figure
3.1.1 displays the percentage of HSE-owned LTCF by CHO that participated in HALT 2016.
Table 3.1.1 Annual increases in HALT participation, by ownership, HSE region and care type.
* Nine LTCF self-selected the ‘Other care type’ category in 2016, indicating their resident case mix did not fit in the more common LTCF
categories. These included: Mixed care type LTCF (n=5), young chronically ill unit (n=2), dementia specific facility (n=1) and a low
dependency residential unit (n=1).
Category 2010 2011 2013 2016
by Ownership
HSE 61 84 128 136
South 8 18 38 45
West 32 34 42 46
Dublin Mid Leinster 14 22 23 20
Dublin North East 7 10 25 25
Private 8 24 39 54
Voluntary n/a n/a 23 34
by Care Type
General nursing homes 30 58 103 88
Mixed care facilities 16 16 26 46
LTCF <12 month stay n/a n/a 15 14
Intellectually disabled 8 15 24 31
Psychiatric 3 5 11 23
Palliative care 1 1 4 7
Physically disabled 1 1 2 1
Rehabilitation 1 1 3 5
Other 3 1 2 9
National 69 108 190 224
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 26
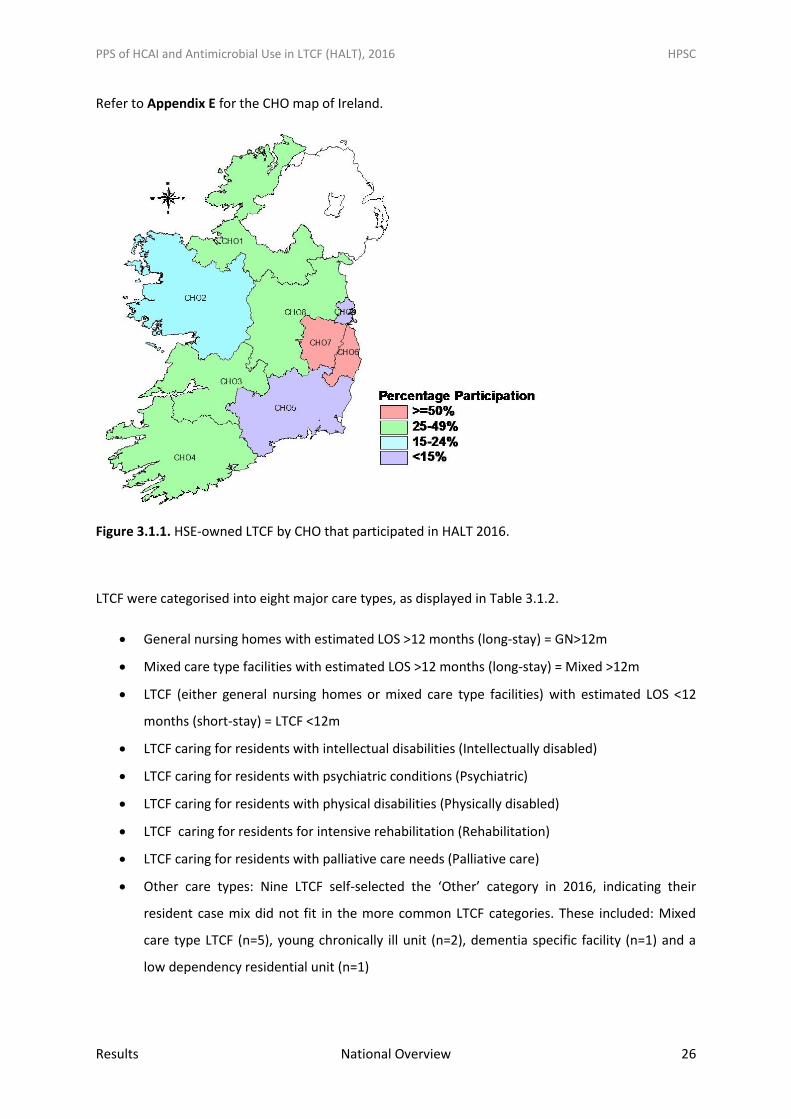
Refer to Appendix E for the CHO map of Ireland.
Figure 3.1.1. HSE-owned LTCF by CHO that participated in HALT 2016.
LTCF were categorised into eight major care types, as displayed in Table 3.1.2.
General nursing homes with estimated LOS >12 months (long-stay) = GN>12m
Mixed care type facilities with estimated LOS >12 months (long-stay) = Mixed >12m
LTCF (either general nursing homes or mixed care type facilities) with estimated LOS <12
months (short-stay) = LTCF <12m
LTCF caring for residents with intellectual disabilities (Intellectually disabled)
LTCF caring for residents with psychiatric conditions (Psychiatric)
LTCF caring for residents with physical disabilities (Physically disabled)
LTCF caring for residents for intensive rehabilitation (Rehabilitation)
LTCF caring for residents with palliative care needs (Palliative care)
Other care types: Nine LTCF self-selected the ‘Other’ category in 2016, indicating their
resident case mix did not fit in the more common LTCF categories. These included: Mixed
care type LTCF (n=5), young chronically ill unit (n=2), dementia specific facility (n=1) and a
low dependency residential unit (n=1)
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 27
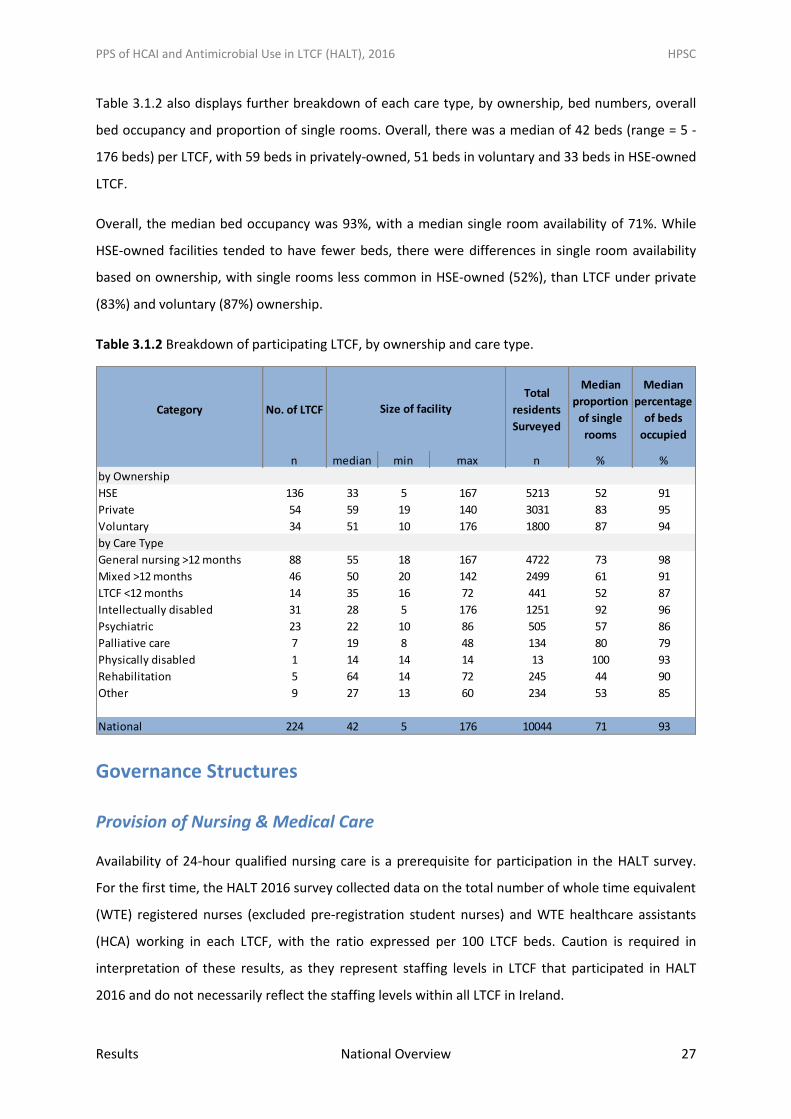
Table 3.1.2 also displays further breakdown of each care type, by ownership, bed numbers, overall
bed occupancy and proportion of single rooms. Overall, there was a median of 42 beds (range = 5 -
176 beds) per LTCF, with 59 beds in privately-owned, 51 beds in voluntary and 33 beds in HSE-owned
LTCF.
Overall, the median bed occupancy was 93%, with a median single room availability of 71%. While
HSE-owned facilities tended to have fewer beds, there were differences in single room availability
based on ownership, with single rooms less common in HSE-owned (52%), than LTCF under private
(83%) and voluntary (87%) ownership.
Table 3.1.2 Breakdown of participating LTCF, by ownership and care type.
Governance Structures
Provision of Nursing & Medical Care
Availability of 24-hour qualified nursing care is a prerequisite for participation in the HALT survey.
For the first time, the HALT 2016 survey collected data on the total number of whole time equivalent
(WTE) registered nurses (excluded pre-registration student nurses) and WTE healthcare assistants
(HCA) working in each LTCF, with the ratio expressed per 100 LTCF beds. Caution is required in
interpretation of these results, as they represent staffing levels in LTCF that participated in HALT
2016 and do not necessarily reflect the staffing levels within all LTCF in Ireland.
Category No. of LTCF
Total
residents
Surveyed
Median
proportion
of single
rooms
Median
percentage
of beds
occupied
n median min max n % %
by Ownership
HSE 136 33 5 167 5213 52 91
Private 54 59 19 140 3031 83 95
Voluntary 34 51 10 176 1800 87 94
by Care Type
General nursing >12 months 88 55 18 167 4722 73 98
Mixed >12 months 46 50 20 142 2499 61 91
LTCF <12 months 14 35 16 72 441 52 87
Intellectually disabled 31 28 5 176 1251 92 96
Psychiatric 23 22 10 86 505 57 86
Palliative care 7 19 8 48 134 80 79
Physically disabled 1 14 14 14 13 100 93
Rehabilitation 5 64 14 72 245 44 90
Other 9 27 13 60 234 53 85
National 224 42 5 176 10044 71 93
Size of facility
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 28
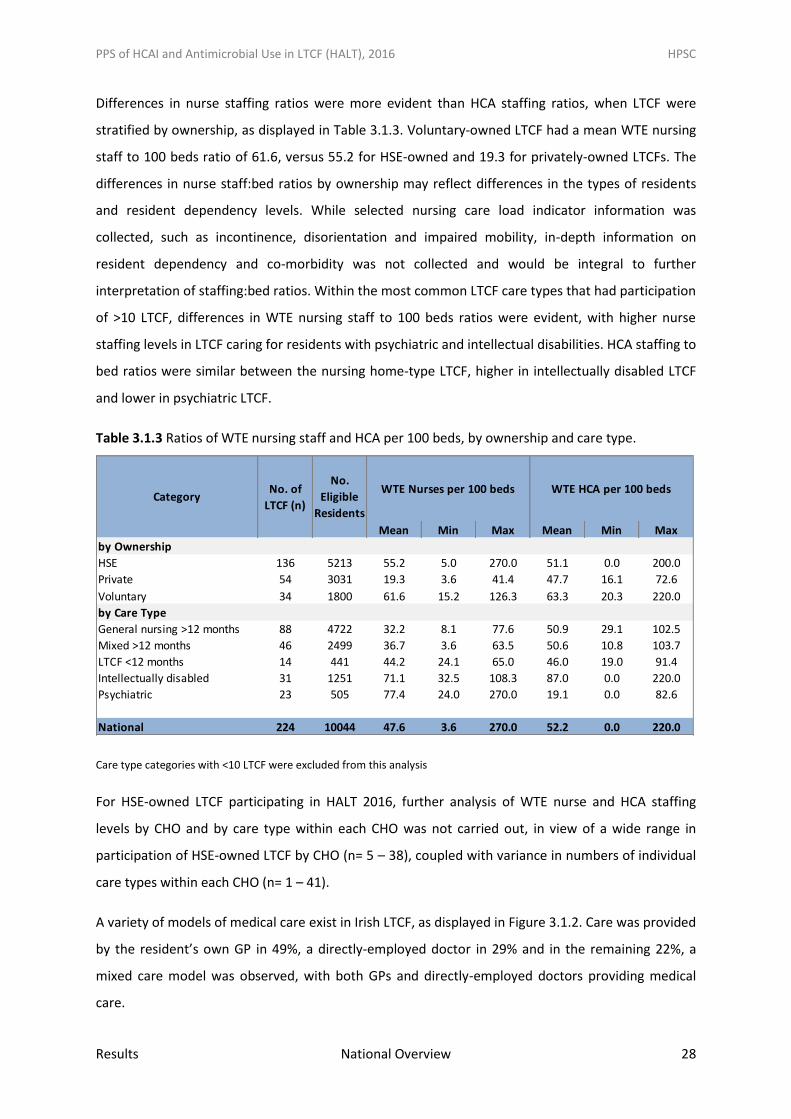
Differences in nurse staffing ratios were more evident than HCA staffing ratios, when LTCF were
stratified by ownership, as displayed in Table 3.1.3. Voluntary-owned LTCF had a mean WTE nursing
staff to 100 beds ratio of 61.6, versus 55.2 for HSE-owned and 19.3 for privately-owned LTCFs. The
differences in nurse staff:bed ratios by ownership may reflect differences in the types of residents
and resident dependency levels. While selected nursing care load indicator information was
collected, such as incontinence, disorientation and impaired mobility, in-depth information on
resident dependency and co-morbidity was not collected and would be integral to further
interpretation of staffing:bed ratios. Within the most common LTCF care types that had participation
of >10 LTCF, differences in WTE nursing staff to 100 beds ratios were evident, with higher nurse
staffing levels in LTCF caring for residents with psychiatric and intellectual disabilities. HCA staffing to
bed ratios were similar between the nursing home-type LTCF, higher in intellectually disabled LTCF
and lower in psychiatric LTCF.
Table 3.1.3 Ratios of WTE nursing staff and HCA per 100 beds, by ownership and care type.
Care type categories with <10 LTCF were excluded from this analysis
For HSE-owned LTCF participating in HALT 2016, further analysis of WTE nurse and HCA staffing
levels by CHO and by care type within each CHO was not carried out, in view of a wide range in
participation of HSE-owned LTCF by CHO (n= 5 – 38), coupled with variance in numbers of individual
care types within each CHO (n= 1 – 41).
A variety of models of medical care exist in Irish LTCF, as displayed in Figure 3.1.2. Care was provided
by the resident’s own GP in 49%, a directly-employed doctor in 29% and in the remaining 22%, a
mixed care model was observed, with both GPs and directly-employed doctors providing medical
care.
Mean Min Max Mean Min Max
by Ownership
HSE 136 5213 55.2 5.0 270.0 51.1 0.0 200.0
Private 54 3031 19.3 3.6 41.4 47.7 16.1 72.6
Voluntary 34 1800 61.6 15.2 126.3 63.3 20.3 220.0
by Care Type
General nursing >12 months 88 4722 32.2 8.1 77.6 50.9 29.1 102.5
Mixed >12 months 46 2499 36.7 3.6 63.5 50.6 10.8 103.7
LTCF <12 months 14 441 44.2 24.1 65.0 46.0 19.0 91.4
Intellectually disabled 31 1251 71.1 32.5 108.3 87.0 0.0 220.0
Psychiatric 23 505 77.4 24.0 270.0 19.1 0.0 82.6
National 224 10044 47.6 3.6 270.0 52.2 0.0 220.0
WTE Nurses per 100 beds WTE HCA per 100 bedsCategory
No. of
LTCF (n)
No.
Eligible
Residents
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 29
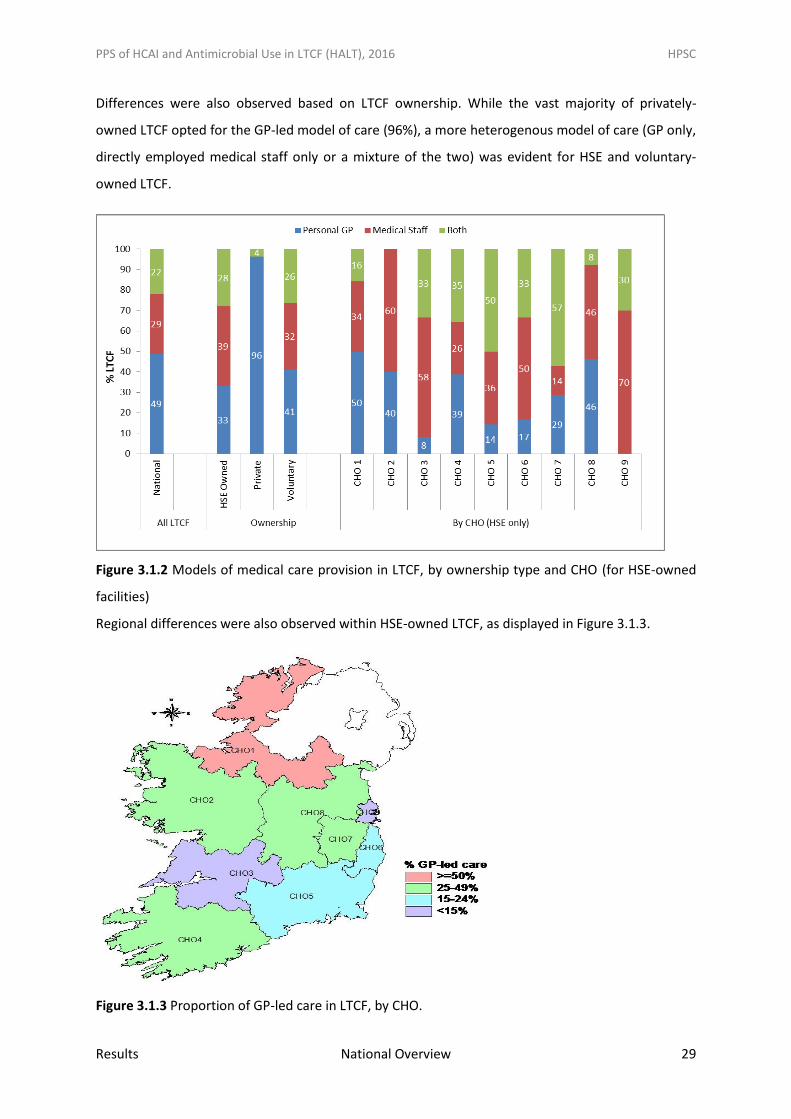
Differences were also observed based on LTCF ownership. While the vast majority of privately-
owned LTCF opted for the GP-led model of care (96%), a more heterogenous model of care (GP only,
directly employed medical staff only or a mixture of the two) was evident for HSE and voluntary-
owned LTCF.
Figure 3.1.2 Models of medical care provision in LTCF, by ownership type and CHO (for HSE-owned
facilities)
Regional differences were also observed within HSE-owned LTCF, as displayed in Figure 3.1.3.
Figure 3.1.3 Proportion of GP-led care in LTCF, by CHO.
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 30
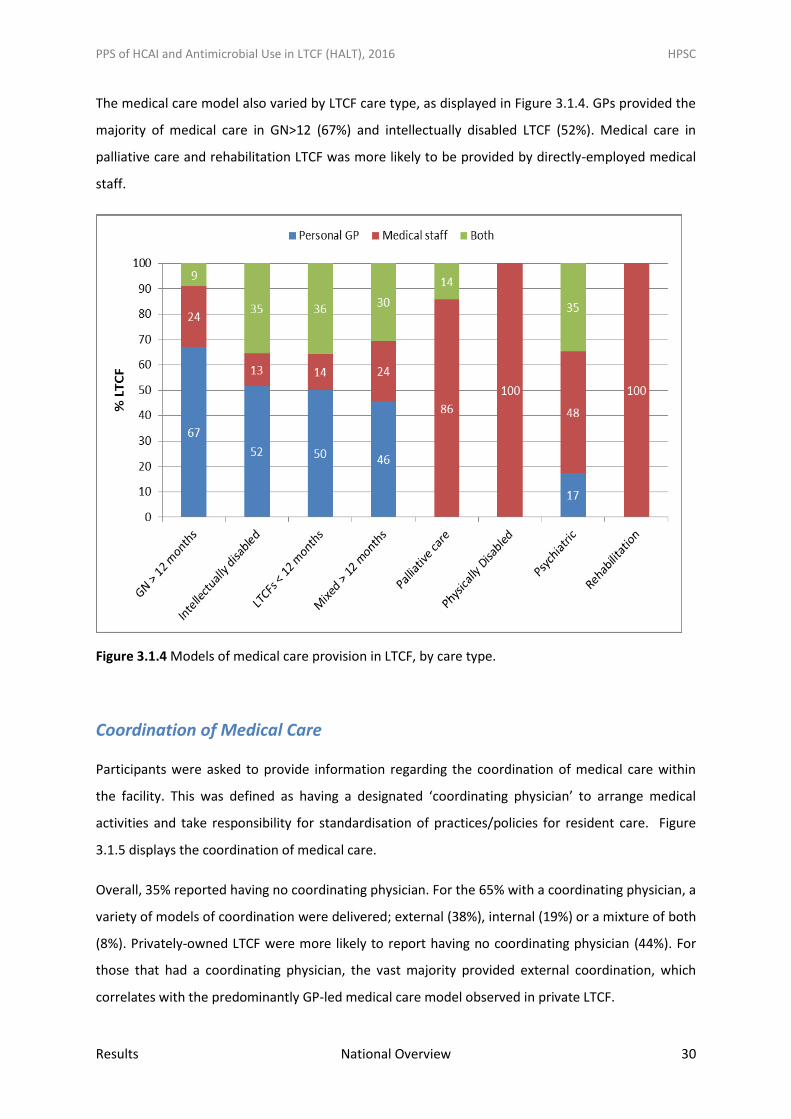
The medical care model also varied by LTCF care type, as displayed in Figure 3.1.4. GPs provided the
majority of medical care in GN>12 (67%) and intellectually disabled LTCF (52%). Medical care in
palliative care and rehabilitation LTCF was more likely to be provided by directly-employed medical
staff.
Figure 3.1.4 Models of medical care provision in LTCF, by care type.
Coordination of Medical Care
Participants were asked to provide information regarding the coordination of medical care within
the facility. This was defined as having a designated ‘coordinating physician’ to arrange medical
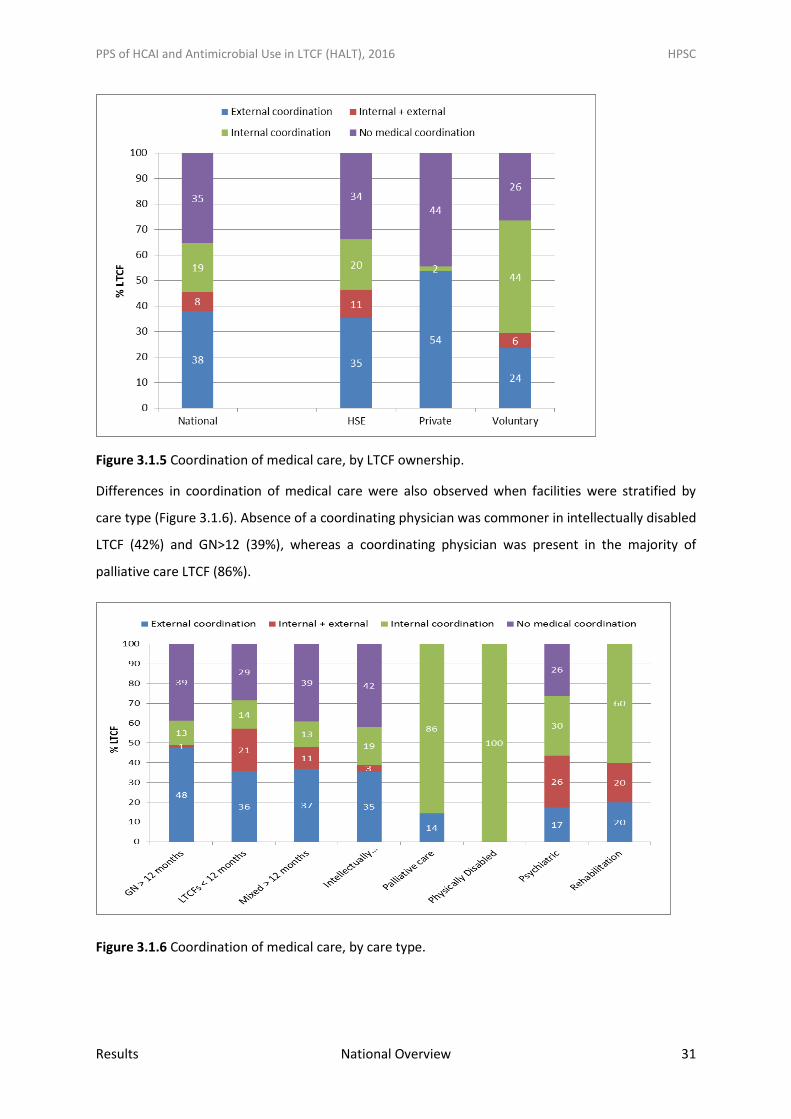
activities and take responsibility for standardisation of practices/policies for resident care. Figure
3.1.5 displays the coordination of medical care.
Overall, 35% reported having no coordinating physician. For the 65% with a coordinating physician, a
variety of models of coordination were delivered; external (38%), internal (19%) or a mixture of both
(8%). Privately-owned LTCF were more likely to report having no coordinating physician (44%). For
those that had a coordinating physician, the vast majority provided external coordination, which
correlates with the predominantly GP-led medical care model observed in private LTCF.
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 31
Figure 3.1.5 Coordination of medical care, by LTCF ownership.
Differences in coordination of medical care were also observed when facilities were stratified by
care type (Figure 3.1.6). Absence of a coordinating physician was commoner in intellectually disabled
LTCF (42%) and GN>12 (39%), whereas a coordinating physician was present in the majority of
palliative care LTCF (86%).
Figure 3.1.6 Coordination of medical care, by care type.
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 32
Infection Prevention & Control (IPC) Practices
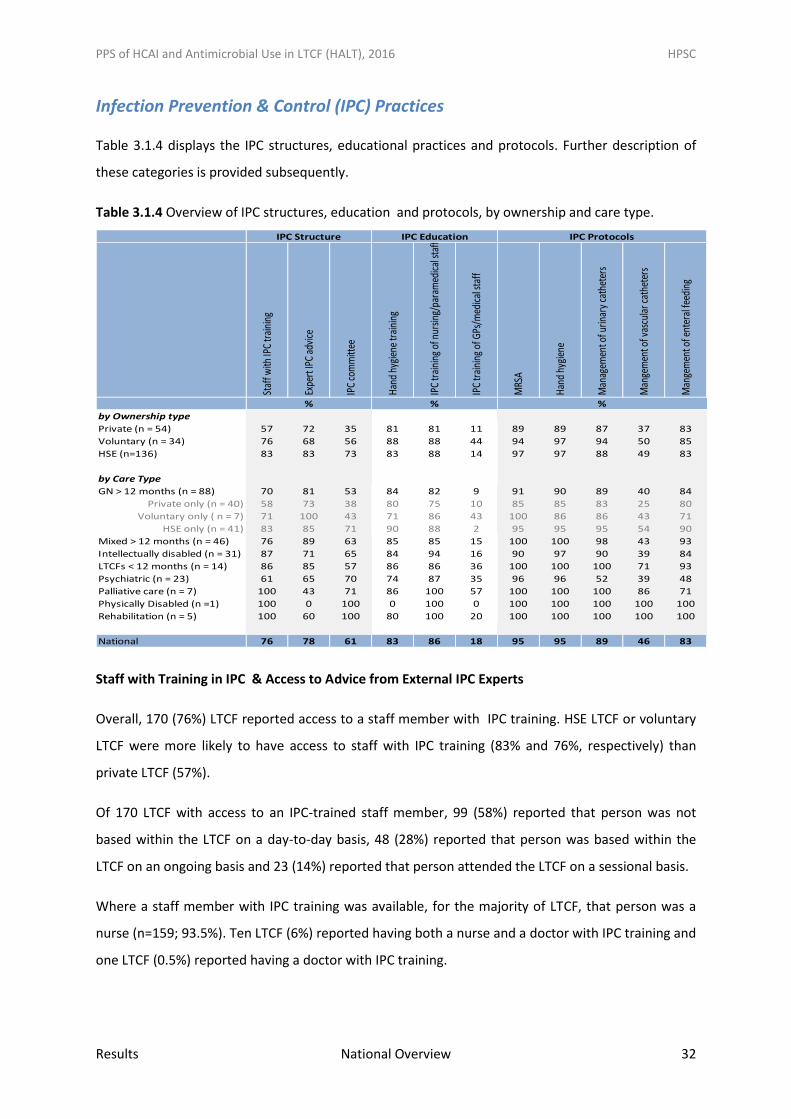
Table 3.1.4 displays the IPC structures, educational practices and protocols. Further description of
these categories is provided subsequently.
Table 3.1.4 Overview of IPC structures, education and protocols, by ownership and care type.
Staff with Training in IPC & Access to Advice from External IPC Experts
Overall, 170 (76%) LTCF reported access to a staff member with IPC training. HSE LTCF or voluntary
LTCF were more likely to have access to staff with IPC training (83% and 76%, respectively) than
private LTCF (57%).
Of 170 LTCF with access to an IPC-trained staff member, 99 (58%) reported that person was not
based within the LTCF on a day-to-day basis, 48 (28%) reported that person was based within the
LTCF on an ongoing basis and 23 (14%) reported that person attended the LTCF on a sessional basis.
Where a staff member with IPC training was available, for the majority of LTCF, that person was a
nurse (n=159; 93.5%). Ten LTCF (6%) reported having both a nurse and a doctor with IPC training and
one LTCF (0.5%) reported having a doctor with IPC training.
Staf
f with
IPC
trai
ning
Expe
rt IP
C ad
vice
IPC
com
mitt
ee
Han
d hy
gien
e tr
aini
ng
IPC
trai
ning
of n
ursin
g/pa
ram
edic
al st
aff
IPC
trai
ning
of G
Ps/m
edic
al st
aff
MRS
A
Han
d hy
gien
e
Man
agem
ent o
f urin
ary
cath
eter
s
Man
gem
ent o
f vas
cula
r cat
hete
rs
Man
gem
ent o
f ent
eral
feed
ing
by Ownership type
Private (n = 54) 57 72 35 81 81 11 89 89 87 37 83
Voluntary (n = 34) 76 68 56 88 88 44 94 97 94 50 85
HSE (n=136) 83 83 73 83 88 14 97 97 88 49 83
by Care Type
GN > 12 months (n = 88) 70 81 53 84 82 9 91 90 89 40 84
Private only (n = 40) 58 73 38 80 75 10 85 85 83 25 80
Voluntary only ( n = 7) 71 100 43 71 86 43 100 86 86 43 71
HSE only (n = 41) 83 85 71 90 88 2 95 95 95 54 90
Mixed > 12 months (n = 46) 76 89 63 85 85 15 100 100 98 43 93
Intellectually disabled (n = 31) 87 71 65 84 94 16 90 97 90 39 84
LTCFs < 12 months (n = 14) 86 85 57 86 86 36 100 100 100 71 93
Psychiatric (n = 23) 61 65 70 74 87 35 96 96 52 39 48
Palliative care (n = 7) 100 43 71 86 100 57 100 100 100 86 71
Physically Disabled (n =1) 100 0 100 0 100 0 100 100 100 100 100
Rehabilitation (n = 5) 100 60 100 80 100 20 100 100 100 100 100
National 76 78 61 83 86 18 95 95 89 46 83
IPC Protocols
% % %
IPC EducationIPC Structure
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 33
In addition to having access to staff with IPC training, information was sought on access to external
expert IPC advice (e.g., from the local hospital or Department of Public Health). Overall, 175 LTCF
(78%) reported having access to such advice, with no access reported by 49 LTCF (22%). Access to
expert IPC advice was less common in psychiatric LTCF (65%), rehabilitation LTCF (60%) and palliative
care LTCF (43%).
Infection Prevention and Control Committee (IPCC)
An active local IPCC was reported by 137 (61%) LTCF, with a median of three meetings per year
(range = 0 - 12). Private GN >12 (38%), voluntary GN >12 (43%) and LTCF <12 months (57%) were less
likely to have an IPCC.
Staff Training
Overall, provision of IPC training was available in the majority of LTCF (86%) for nursing and
paramedical staff, but in the minority of LTCF (18%) for medical staff. Private LTCF offered less access
to staff IPC training for nursing, paramedical and medical staff. Medical staff were more likely to
receive IPC training if they worked in a voluntary-owned LTCF (44%) or a palliative care LTCF (57%).
Hand Hygiene Training
Overall, 83% reported that a staff hand hygiene training session had been organised during the
previous year (2015). This figure was higher in voluntary LTCF (88%) and HSE GN>12 (90%). Hand
hygiene training was lower in psychiatric LTCF (74%) and voluntary GN>12 (71%).
Seventy-three percent of LTCFs reported completing hand hygiene training in 2014 and 66%
reported hand hygiene training in both 2014 and 2015.
Access to Hand Hygiene Products
The HALT protocol did not specify whether data on hand hygiene product availability applied to staff
use only or whether resident hand hygiene products could be included.The vast majority of LTCF
reported having alcohol-based hand rub (ABHR) (96%) and liquid soap (95%) as available hand
hygiene products (Table 3.1.5). Alcohol-based wipes were reported to be available in 41% of LTCF,
ABHR was reported as the preferred hand hygiene method in 68%. Data on the estimated volume of
ABHR consumed during the previous year (2015) was provided by 78% of LTCF, reporting an average
consumption of 145 litres. Hand washing with a non-antiseptic soap was the preferred method in
20% and hand washing with antiseptic soap in 8% of LTCF.
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 34
Observation of Hand Hygiene Opportunities
For the first time, HALT 2016 collected data on observation of hand hygiene opportunities within
individual LTCF during the previous year (2015). Data on compliance with hand hygiene
opportunities was not collected. However, 51% of LTCF reported that formal audit of staff hand
hygiene compliance was carried out in the previous year (2015).
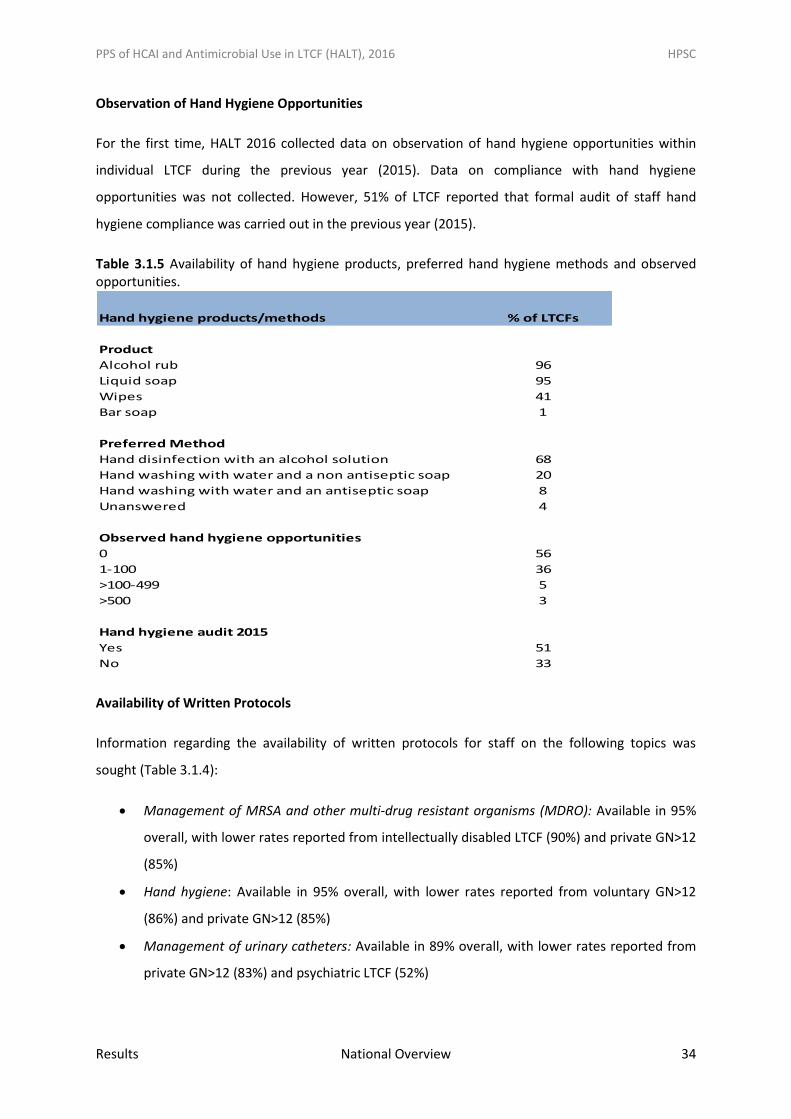
Table 3.1.5 Availability of hand hygiene products, preferred hand hygiene methods and observed opportunities.
Availability of Written Protocols
Information regarding the availability of written protocols for staff on the following topics was
sought (Table 3.1.4):
Management of MRSA and other multi-drug resistant organisms (MDRO): Available in 95%
overall, with lower rates reported from intellectually disabled LTCF (90%) and private GN>12
(85%)
Hand hygiene: Available in 95% overall, with lower rates reported from voluntary GN>12
(86%) and private GN>12 (85%)
Management of urinary catheters: Available in 89% overall, with lower rates reported from
private GN>12 (83%) and psychiatric LTCF (52%)
Hand hygiene products/methods
Product
Alcohol rub
Liquid soap
Wipes
Bar soap
Preferred Method
Hand disinfection with an alcohol solution
Hand washing with water and a non antiseptic soap
Hand washing with water and an antiseptic soap
Unanswered
Observed hand hygiene opportunities
0
1-100
>100-499
>500
Hand hygiene audit 2015
Yes
No
% of LTCFs
96
95
41
8
4
56
1
68
20
36
5
3
51
33
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 35
Management of vascular catheters: Available in 46% overall, with lower rates reported from
intellectually disabled and psychiatric LTCF (both 39%) and private GN>12 (25%)
Management of enteral feeding: Available in 83% overall, with lower rates reported from
voluntary GN>12 and palliative care LTCF (both 71%) and psychiatric LTCF (48%)
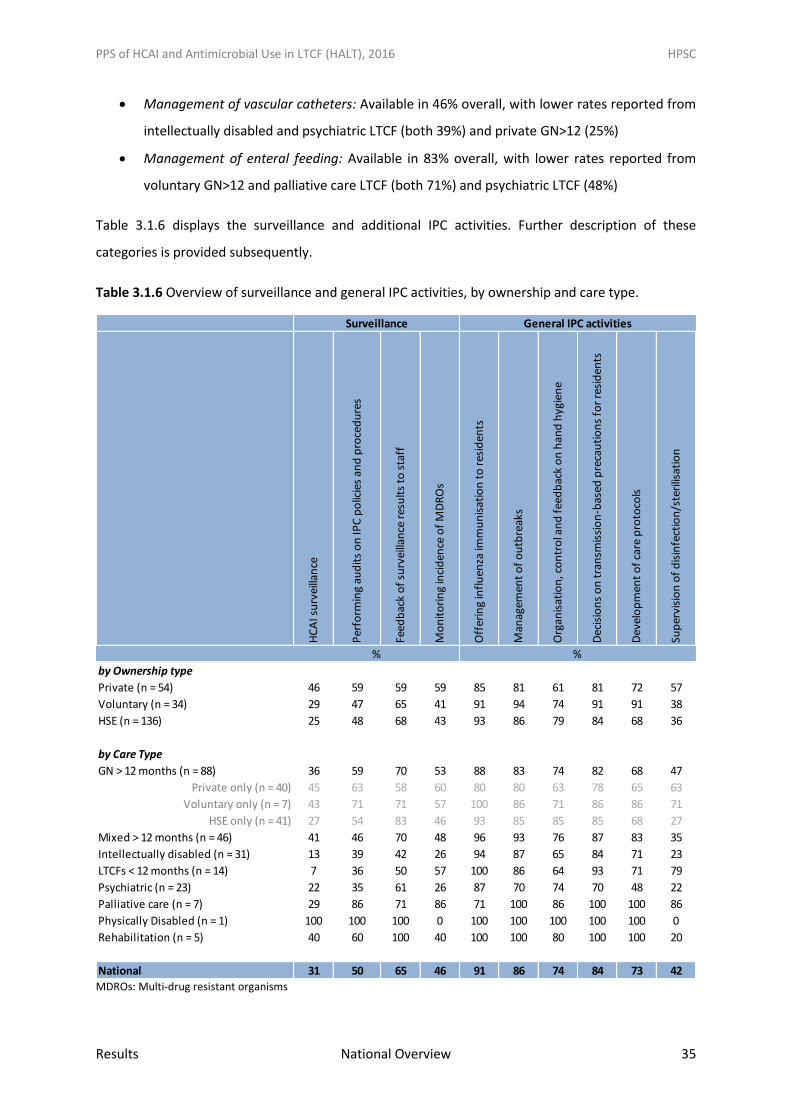
Table 3.1.6 displays the surveillance and additional IPC activities. Further description of these
categories is provided subsequently.
Table 3.1.6 Overview of surveillance and general IPC activities, by ownership and care type.
MDROs: Multi-drug resistant organisms
HC
AI s
urv
eilla
nce
Per
form
ing
aud
its
on
IPC
po
licie
s an
d p
roce
du
res
Feed
bac
k o
f su
rvei
llan
ce r
esu
lts
to s
taff
Mo
nit
ori
ng
inci
den
ce o
f M
DR
Os
Off
erin
g in
flu
enza
imm
un
isat
ion
to
res
iden
ts
Man
agem
ent
of
ou
tbre
aks
Org
anis
atio
n, c
on
tro
l an
d f
eed
bac
k o
n h
and
hyg
ien
e
Dec
isio
ns
on
tra
nsm
issi
on
-bas
ed p
reca
uti
on
s fo
r re
sid
ents
Dev
elo
pm
ent
of
care
pro
toco
ls
Sup
ervi
sio
n o
f d
isin
fect
ion
/ste
rilis
atio
nby Ownership type
Private (n = 54) 46 59 59 59 85 81 61 81 72 57
Voluntary (n = 34) 29 47 65 41 91 94 74 91 91 38
HSE (n = 136) 25 48 68 43 93 86 79 84 68 36
by Care Type
GN > 12 months (n = 88) 36 59 70 53 88 83 74 82 68 47
Private only (n = 40) 45 63 58 60 80 80 63 78 65 63
Voluntary only (n = 7) 43 71 71 57 100 86 71 86 86 71
HSE only (n = 41) 27 54 83 46 93 85 85 85 68 27
Mixed > 12 months (n = 46) 41 46 70 48 96 93 76 87 83 35
Intellectually disabled (n = 31) 13 39 42 26 94 87 65 84 71 23
LTCFs < 12 months (n = 14) 7 36 50 57 100 86 64 93 71 79
Psychiatric (n = 23) 22 35 61 26 87 70 74 70 48 22
Palliative care (n = 7) 29 86 71 86 71 100 86 100 100 86
Physically Disabled (n = 1) 100 100 100 0 100 100 100 100 100 0
Rehabilitation (n = 5) 40 60 100 40 100 100 80 100 100 20
National 31 50 65 46 91 86 74 84 73 42
% %
Surveillance General IPC activities
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 36
HCAI Surveillance Programme
Some form of a HCAI surveillance programme was reported by 31% (n=69) of LTCF (Table
3.1.6). Ongoing participation in repeated HALT surveys could be regarded as a HCAI
surveillance programme. Some care types were more likely to report having HCAI
surveillance activities; private GN>12 (45%), voluntary GN>12 (43%) and mixed >12 (41%).
HCAI surveillance was less common in psychiatric (22%), intellectually disabled LTCF (13%)
and LTCF <12 months (7%)
Audits of IPC policies and procedures were reported by 50%, feedback of surveillance results
to staff by 65% and monitoring of incidence of MDRO by 46%
Notably, facilities with an active IPCC were more likely to report having MDRO surveillance
programmes than those without
A designated staff member for reporting and management of infection outbreaks was
available in 86% overall, with lower levels reported from private LTCFs (81%)
A system in place for the organisation, control and feedback on hand hygiene was reported
as available in 74% overall, with lower levels reported from intellectually disabled LTCF
(65%), LTCF <12 months (64%) and private GN<12 (63%)
A system for management of patients with MDRO (e.g., patient isolation, additional IPC
precautions) was available in 84% overall, with less availability in psychiatric LTCF (70%) and
private GN>12 (78%)
Overall, a system for development of resident care protocols available in 73%, with lower
availability in HSE GN>12 (68%) and psychiatric LTCF (48%)
Overall, 91% reported that seasonal influenza vaccine is offered to residents. However,
lower figures were reported from psychiatric LTCF (87%) and private GN>12 (80%)
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 37
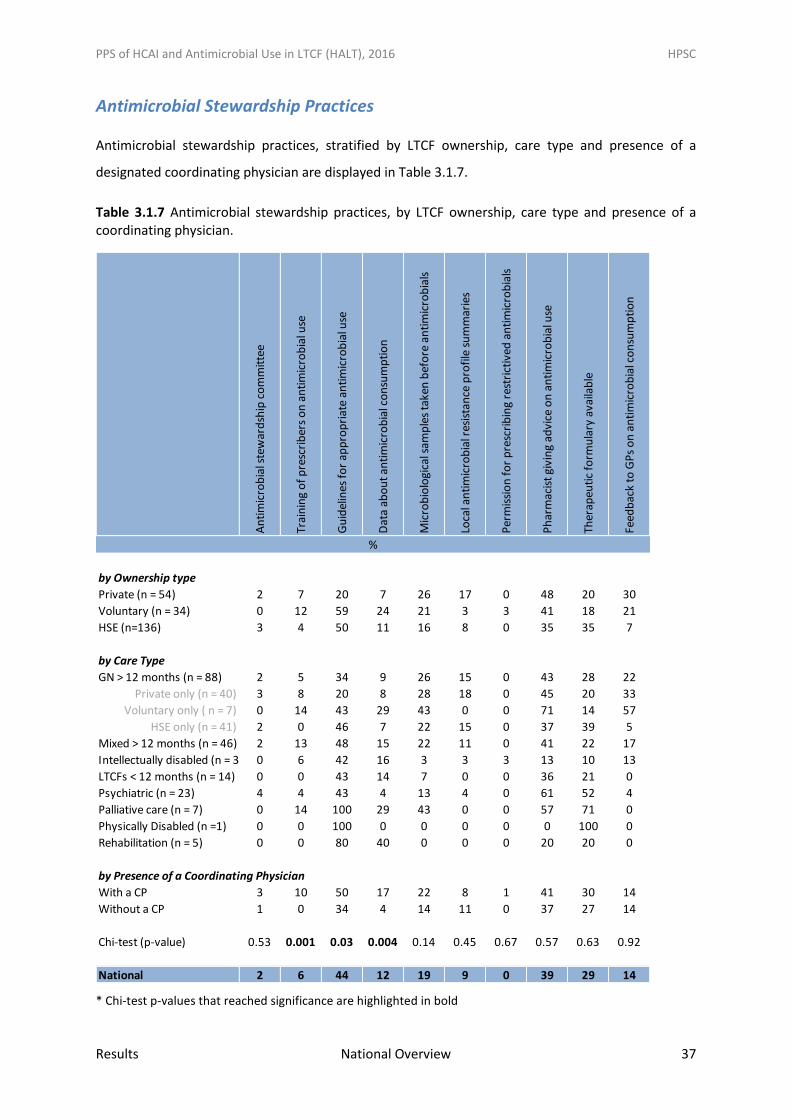
Antimicrobial Stewardship Practices
Antimicrobial stewardship practices, stratified by LTCF ownership, care type and presence of a
designated coordinating physician are displayed in Table 3.1.7.
Table 3.1.7 Antimicrobial stewardship practices, by LTCF ownership, care type and presence of a coordinating physician.
* Chi-test p-values that reached significance are highlighted in bold
An
tim
icro
bia
l ste
war
dsh
ip c
om
mit
tee
Trai
nin
g o
f p
resc
rib
ers
on
an
tim
icro
bia
l use
Gu
idel
ines
fo
r ap
pro
pri
ate
anti
mic
rob
ial u
se
Dat
a ab
ou
t an
tim
icro
bia
l co
nsu
mp
tio
n
Mic
rob
iolo
gica
l sam
ple
s ta
ken
bef
ore
an
tim
icro
bia
ls
Loca
l an
tim
icro
bia
l res
ista
nce
pro
file
su
mm
arie
s
Per
mis
sio
n f
or
pre
scri
bin
g re
stri
ctiv
ed a
nti
mic
rob
ials
Ph
arm
acis
t gi
vin
g ad
vice
on
an
tim
icro
bia
l use
Ther
apeu
tic
form
ula
ry a
vaila
ble
Feed
bac
k to
GP
s o
n a
nti
mic
rob
ial c
on
sum
pti
on
by Ownership type
Private (n = 54) 2 7 20 7 26 17 0 48 20 30
Voluntary (n = 34) 0 12 59 24 21 3 3 41 18 21
HSE (n=136) 3 4 50 11 16 8 0 35 35 7
by Care Type
GN > 12 months (n = 88) 2 5 34 9 26 15 0 43 28 22
Private only (n = 40) 3 8 20 8 28 18 0 45 20 33
Voluntary only ( n = 7) 0 14 43 29 43 0 0 71 14 57
HSE only (n = 41) 2 0 46 7 22 15 0 37 39 5
Mixed > 12 months (n = 46) 2 13 48 15 22 11 0 41 22 17
Intellectually disabled (n = 31) 0 6 42 16 3 3 3 13 10 13
LTCFs < 12 months (n = 14) 0 0 43 14 7 0 0 36 21 0
Psychiatric (n = 23) 4 4 43 4 13 4 0 61 52 4
Palliative care (n = 7) 0 14 100 29 43 0 0 57 71 0
Physically Disabled (n =1) 0 0 100 0 0 0 0 0 100 0
Rehabilitation (n = 5) 0 0 80 40 0 0 0 20 20 0
by Presence of a Coordinating Physician
With a CP 3 10 50 17 22 8 1 41 30 14
Without a CP 1 0 34 4 14 11 0 37 27 14
Chi-test (p-value) 0.53 0.001 0.03 0.004 0.14 0.45 0.67 0.57 0.63 0.92
National 2 6 44 12 19 9 0 39 29 14
%
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 38
Overview of Antimicrobial Stewardship Practices & Guidelines
The vast majority of LTCF (n=219; 98%) reported having no antimicrobial stewardship
committee (ASC). Of the five LTCF with an ASC (2%), one was privately-owned
Additionally, the vast majority (94%) reported that annual training on antimicrobial
prescribing was not provided
A local antimicrobial prescribing guideline was available in 99 LTCF (44%) overall. Private
GN>12 were less likely (20%) than palliative care (100%) and rehabilitation LTCF (80%) to
have guidelines
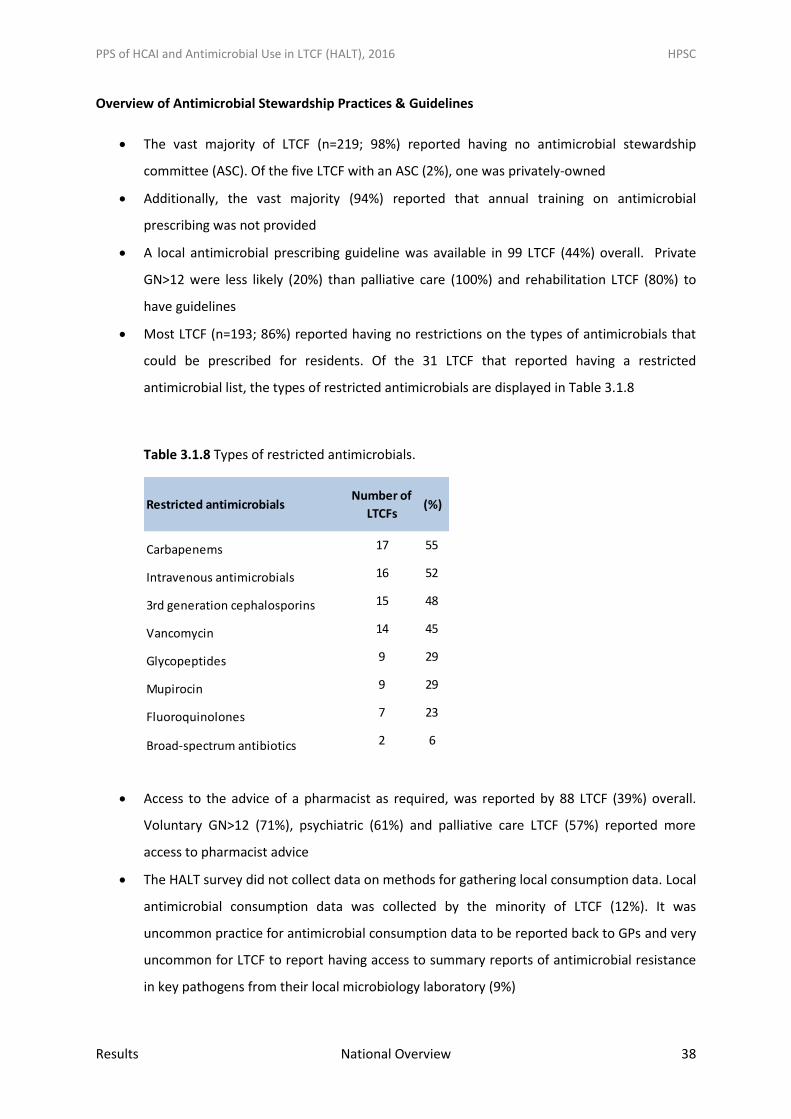
Most LTCF (n=193; 86%) reported having no restrictions on the types of antimicrobials that
could be prescribed for residents. Of the 31 LTCF that reported having a restricted
antimicrobial list, the types of restricted antimicrobials are displayed in Table 3.1.8
Table 3.1.8 Types of restricted antimicrobials.
Access to the advice of a pharmacist as required, was reported by 88 LTCF (39%) overall.
Voluntary GN>12 (71%), psychiatric (61%) and palliative care LTCF (57%) reported more
access to pharmacist advice
The HALT survey did not collect data on methods for gathering local consumption data. Local
antimicrobial consumption data was collected by the minority of LTCF (12%). It was
uncommon practice for antimicrobial consumption data to be reported back to GPs and very
uncommon for LTCF to report having access to summary reports of antimicrobial resistance
in key pathogens from their local microbiology laboratory (9%)
Restricted antimicrobialsNumber of
LTCFs (%)
Carbapenems 17 55
Intravenous antimicrobials 16 52
3rd generation cephalosporins 15 48
Vancomycin 14 45
Glycopeptides 9 29
Mupirocin 9 29
Fluoroquinolones 7 23
Broad-spectrum antibiotics 2 6
Total 31 100
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 39
A minority (19%) reported having a system in place to remind staff of the importance of
obtaining relevant clinical specimens from the resident prior to commencing antimicrobial
therapy for infection (e.g., the importance of taking a urine specimen before starting
treatment for a suspected UTI)
Information was sought regarding the frequency with which a urine dipstick test was used
for UTI diagnosis. Of the 219 (98%) who answered, urine dipstick was performed routinely in
133 (61%) and sometimes in 86 (39%)
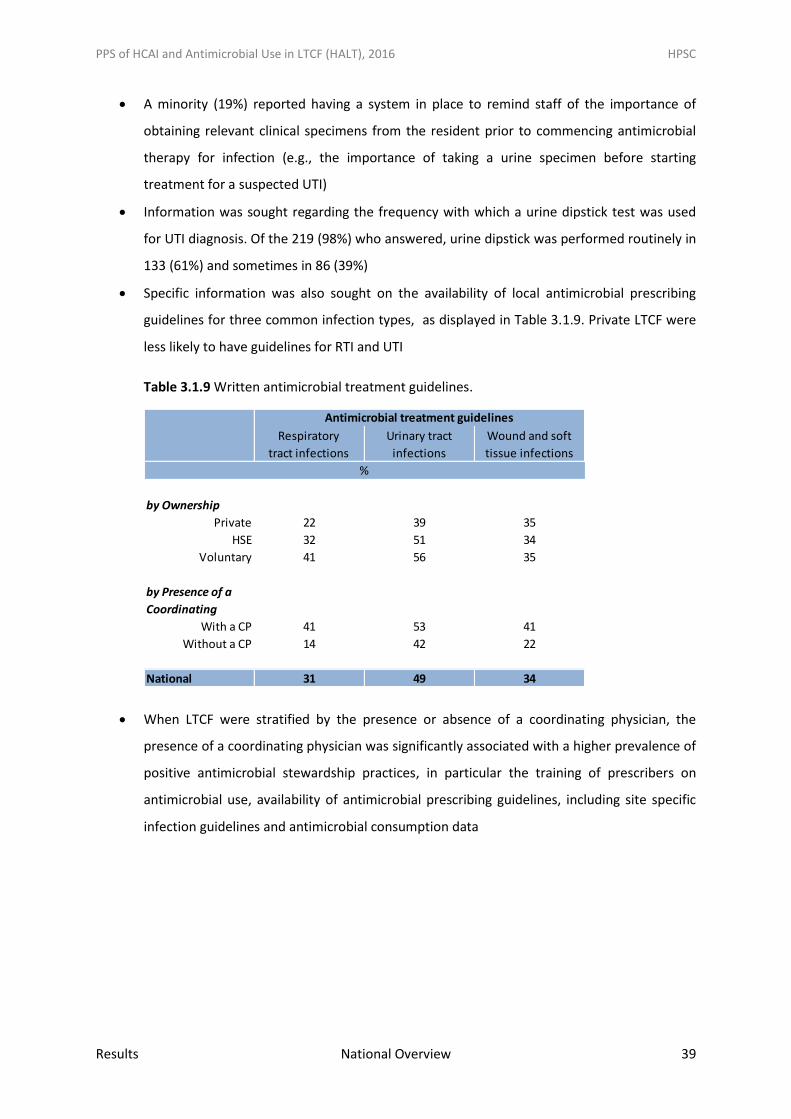
Specific information was also sought on the availability of local antimicrobial prescribing
guidelines for three common infection types, as displayed in Table 3.1.9. Private LTCF were
less likely to have guidelines for RTI and UTI
Table 3.1.9 Written antimicrobial treatment guidelines.
When LTCF were stratified by the presence or absence of a coordinating physician, the
presence of a coordinating physician was significantly associated with a higher prevalence of
positive antimicrobial stewardship practices, in particular the training of prescribers on
antimicrobial use, availability of antimicrobial prescribing guidelines, including site specific
infection guidelines and antimicrobial consumption data
Respiratory
tract infections
Urinary tract
infections
Wound and soft
tissue infections
by Ownership
Private 22 39 35
HSE 32 51 34
Voluntary 41 56 35
With a CP 41 53 41
Without a CP 14 42 22
National 31 49 34
Antimicrobial treatment guidelines
by Presence of a
Coordinating
%
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 40
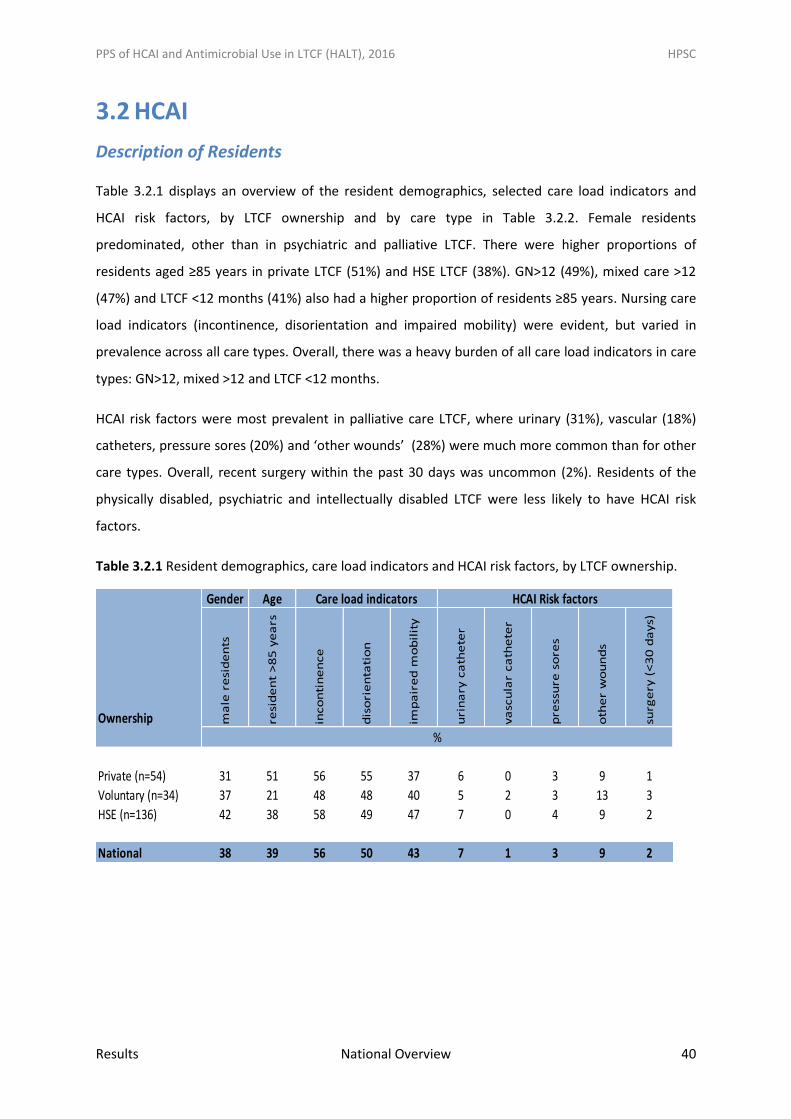
3.2 HCAI
Description of Residents
Table 3.2.1 displays an overview of the resident demographics, selected care load indicators and
HCAI risk factors, by LTCF ownership and by care type in Table 3.2.2. Female residents
predominated, other than in psychiatric and palliative LTCF. There were higher proportions of
residents aged ≥85 years in private LTCF (51%) and HSE LTCF (38%). GN>12 (49%), mixed care >12
(47%) and LTCF <12 months (41%) also had a higher proportion of residents ≥85 years. Nursing care
load indicators (incontinence, disorientation and impaired mobility) were evident, but varied in
prevalence across all care types. Overall, there was a heavy burden of all care load indicators in care
types: GN>12, mixed >12 and LTCF <12 months.
HCAI risk factors were most prevalent in palliative care LTCF, where urinary (31%), vascular (18%)
catheters, pressure sores (20%) and ‘other wounds’ (28%) were much more common than for other
care types. Overall, recent surgery within the past 30 days was uncommon (2%). Residents of the
physically disabled, psychiatric and intellectually disabled LTCF were less likely to have HCAI risk
factors.
Table 3.2.1 Resident demographics, care load indicators and HCAI risk factors, by LTCF ownership.
Gender Age
Ownership ma
le r
esi
de
nts
resi
de
nt
>8
5 y
ea
rs
inco
nti
ne
nce
dis
ori
en
tati
on
imp
air
ed
mo
bil
ity
uri
na
ry c
ath
ete
r
va
scu
lar
ca
the
ter
pre
ssu
re s
ore
s
oth
er
wo
un
ds
surg
ery
(<
30
da
ys)
Private (n=54) 31 51 56 55 37 6 0 3 9 1
Voluntary (n=34) 37 21 48 48 40 5 2 3 13 3
HSE (n=136) 42 38 58 49 47 7 0 4 9 2
National 38 39 56 50 43 7 1 3 9 2
%
Care load indicators HCAI Risk factors
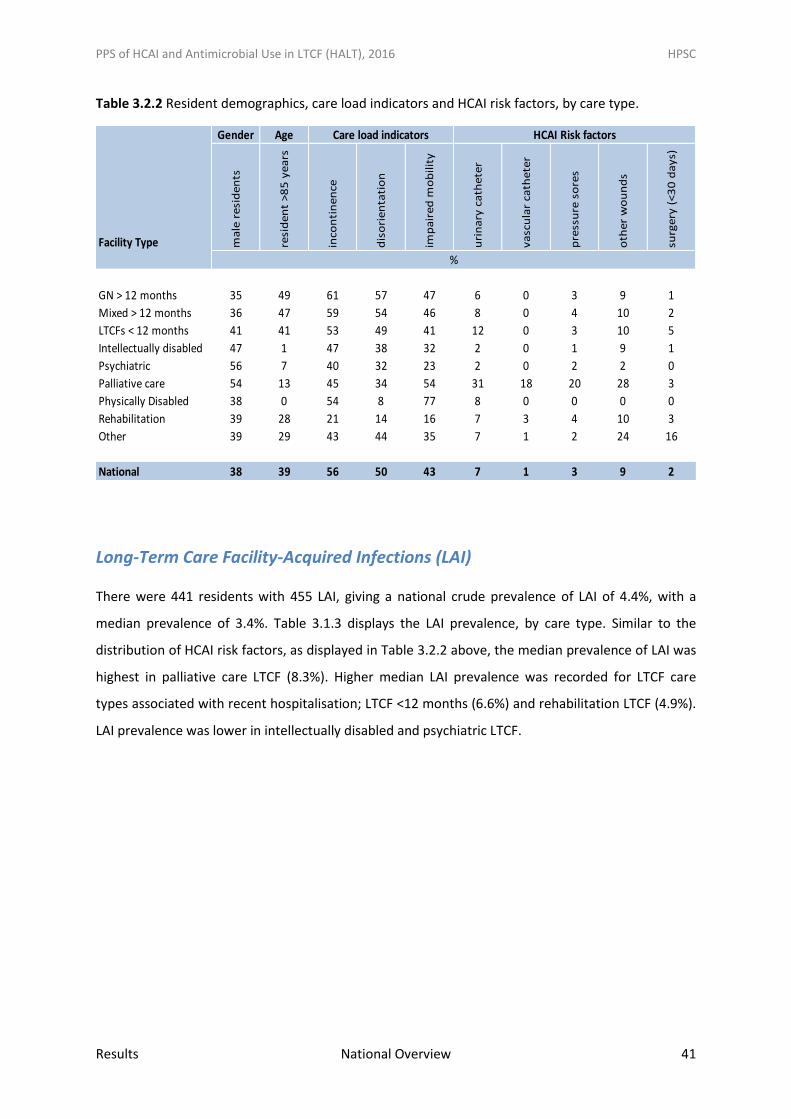
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 41
Table 3.2.2 Resident demographics, care load indicators and HCAI risk factors, by care type.
Long-Term Care Facility-Acquired Infections (LAI)
There were 441 residents with 455 LAI, giving a national crude prevalence of LAI of 4.4%, with a
median prevalence of 3.4%. Table 3.1.3 displays the LAI prevalence, by care type. Similar to the
distribution of HCAI risk factors, as displayed in Table 3.2.2 above, the median prevalence of LAI was
highest in palliative care LTCF (8.3%). Higher median LAI prevalence was recorded for LTCF care
types associated with recent hospitalisation; LTCF <12 months (6.6%) and rehabilitation LTCF (4.9%).
LAI prevalence was lower in intellectually disabled and psychiatric LTCF.
Gender Age
Facility Type ma
le r
esi
de
nts
resi
de
nt
>8
5 y
ea
rs
inco
nti
ne
nce
dis
ori
en
tati
on
imp
air
ed
mo
bil
ity
uri
na
ry c
ath
ete
r
va
scu
lar
cath
ete
r
pre
ssu
re s
ore
s
oth
er
wo
un
ds
surg
ery
(<
30
da
ys)
GN > 12 months 35 49 61 57 47 6 0 3 9 1
Mixed > 12 months 36 47 59 54 46 8 0 4 10 2
LTCFs < 12 months 41 41 53 49 41 12 0 3 10 5
Intellectually disabled 47 1 47 38 32 2 0 1 9 1
Psychiatric 56 7 40 32 23 2 0 2 2 0
Palliative care 54 13 45 34 54 31 18 20 28 3
Physically Disabled 38 0 54 8 77 8 0 0 0 0
Rehabilitation 39 28 21 14 16 7 3 4 10 3
Other 39 29 43 44 35 7 1 2 24 16
National 38 39 56 50 43 7 1 3 9 2
Care load indicators HCAI Risk factors
%
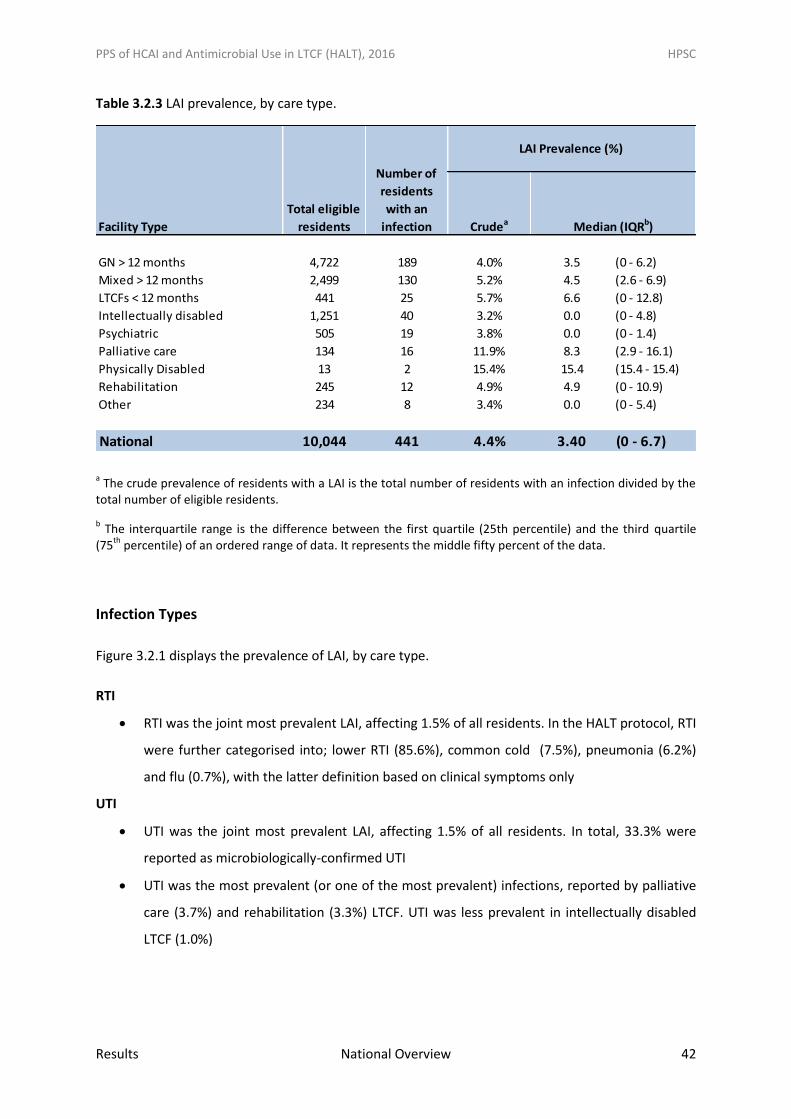
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 42
Table 3.2.3 LAI prevalence, by care type.
a The crude prevalence of residents with a LAI is the total number of residents with an infection divided by the
total number of eligible residents.
b The interquartile range is the difference between the first quartile (25th percentile) and the third quartile
(75th
percentile) of an ordered range of data. It represents the middle fifty percent of the data.
Infection Types
Figure 3.2.1 displays the prevalence of LAI, by care type.
RTI
RTI was the joint most prevalent LAI, affecting 1.5% of all residents. In the HALT protocol, RTI
were further categorised into; lower RTI (85.6%), common cold (7.5%), pneumonia (6.2%)
and flu (0.7%), with the latter definition based on clinical symptoms only
UTI
UTI was the joint most prevalent LAI, affecting 1.5% of all residents. In total, 33.3% were
reported as microbiologically-confirmed UTI
UTI was the most prevalent (or one of the most prevalent) infections, reported by palliative
care (3.7%) and rehabilitation (3.3%) LTCF. UTI was less prevalent in intellectually disabled
LTCF (1.0%)
Crudea
GN > 12 months 4,722 189 4.0% 3.5 (0 - 6.2)
Mixed > 12 months 2,499 130 5.2% 4.5 (2.6 - 6.9)
LTCFs < 12 months 441 25 5.7% 6.6 (0 - 12.8)
Intellectually disabled 1,251 40 3.2% 0.0 (0 - 4.8)
Psychiatric 505 19 3.8% 0.0 (0 - 1.4)
Palliative care 134 16 11.9% 8.3 (2.9 - 16.1)
Physically Disabled 13 2 15.4% 15.4 (15.4 - 15.4)
Rehabilitation 245 12 4.9% 4.9 (0 - 10.9)
Other 234 8 3.4% 0.0 (0 - 5.4)
National 10,044 441 4.4% 3.40 (0 - 6.7)
Facility Type
Total eligible
residents
Number of
residents
with an
infection
LAI Prevalence (%)
Median (IQRb)
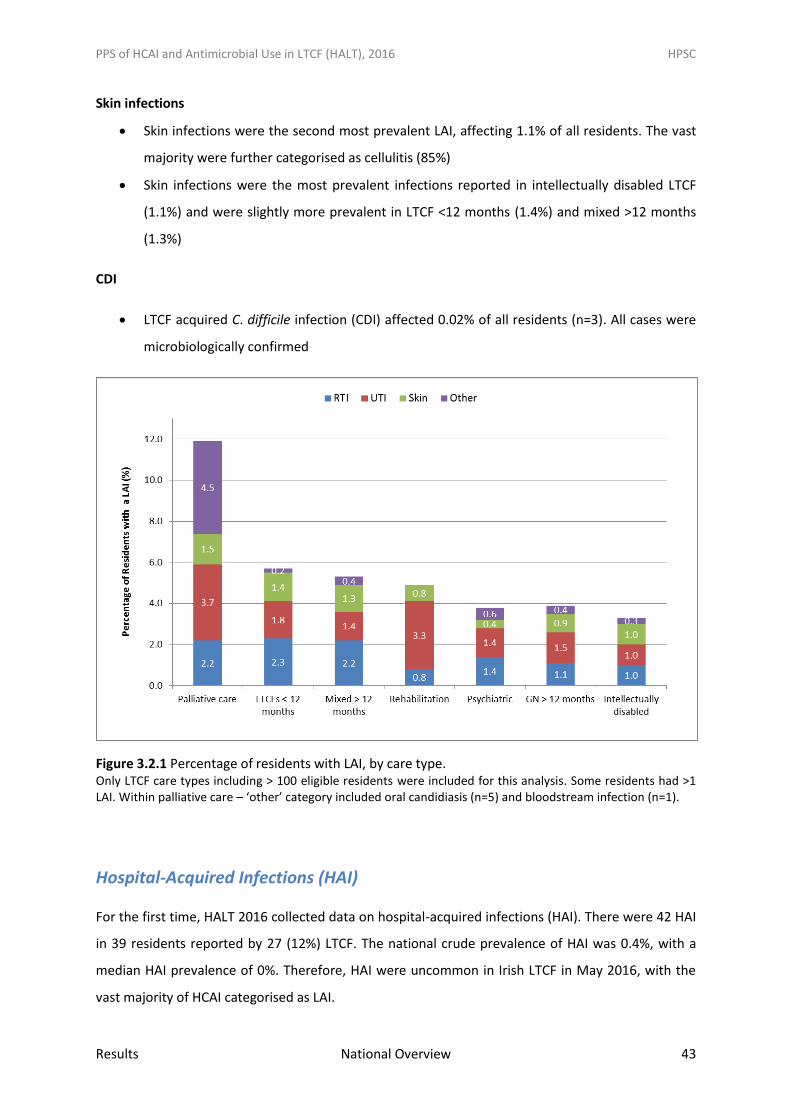
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 43
Skin infections
Skin infections were the second most prevalent LAI, affecting 1.1% of all residents. The vast
majority were further categorised as cellulitis (85%)
Skin infections were the most prevalent infections reported in intellectually disabled LTCF
(1.1%) and were slightly more prevalent in LTCF <12 months (1.4%) and mixed >12 months
(1.3%)
CDI
LTCF acquired C. difficile infection (CDI) affected 0.02% of all residents (n=3). All cases were
microbiologically confirmed
Figure 3.2.1 Percentage of residents with LAI, by care type. Only LTCF care types including > 100 eligible residents were included for this analysis. Some residents had >1 LAI. Within palliative care – ‘other’ category included oral candidiasis (n=5) and bloodstream infection (n=1).
Hospital-Acquired Infections (HAI)
For the first time, HALT 2016 collected data on hospital-acquired infections (HAI). There were 42 HAI
in 39 residents reported by 27 (12%) LTCF. The national crude prevalence of HAI was 0.4%, with a
median HAI prevalence of 0%. Therefore, HAI were uncommon in Irish LTCF in May 2016, with the
vast majority of HCAI categorised as LAI.
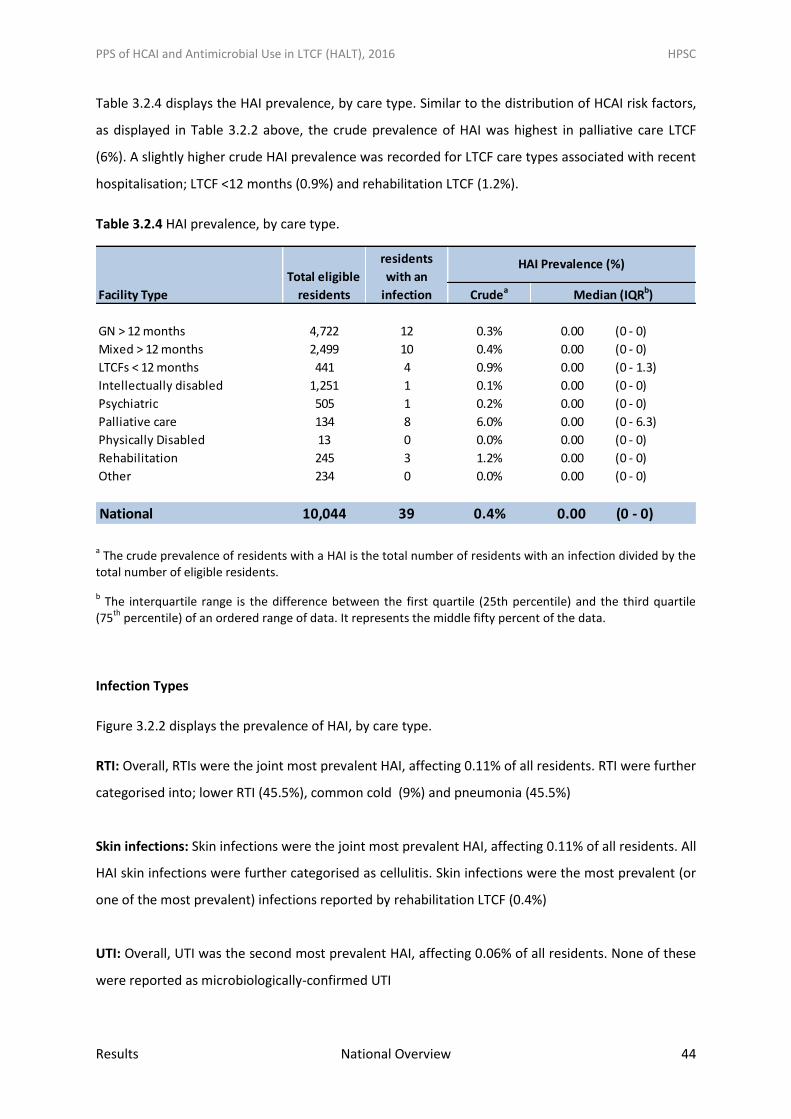
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 44
Table 3.2.4 displays the HAI prevalence, by care type. Similar to the distribution of HCAI risk factors,
as displayed in Table 3.2.2 above, the crude prevalence of HAI was highest in palliative care LTCF
(6%). A slightly higher crude HAI prevalence was recorded for LTCF care types associated with recent
hospitalisation; LTCF <12 months (0.9%) and rehabilitation LTCF (1.2%).
Table 3.2.4 HAI prevalence, by care type.
a The crude prevalence of residents with a HAI is the total number of residents with an infection divided by the
total number of eligible residents.
b The interquartile range is the difference between the first quartile (25th percentile) and the third quartile
(75th
percentile) of an ordered range of data. It represents the middle fifty percent of the data.
Infection Types
Figure 3.2.2 displays the prevalence of HAI, by care type.
RTI: Overall, RTIs were the joint most prevalent HAI, affecting 0.11% of all residents. RTI were further
categorised into; lower RTI (45.5%), common cold (9%) and pneumonia (45.5%)
Skin infections: Skin infections were the joint most prevalent HAI, affecting 0.11% of all residents. All
HAI skin infections were further categorised as cellulitis. Skin infections were the most prevalent (or
one of the most prevalent) infections reported by rehabilitation LTCF (0.4%)
UTI: Overall, UTI was the second most prevalent HAI, affecting 0.06% of all residents. None of these
were reported as microbiologically-confirmed UTI
Crudea
GN > 12 months 4,722 12 0.3% 0.00 (0 - 0)
Mixed > 12 months 2,499 10 0.4% 0.00 (0 - 0)
LTCFs < 12 months 441 4 0.9% 0.00 (0 - 1.3)
Intellectually disabled 1,251 1 0.1% 0.00 (0 - 0)
Psychiatric 505 1 0.2% 0.00 (0 - 0)
Palliative care 134 8 6.0% 0.00 (0 - 6.3)
Physically Disabled 13 0 0.0% 0.00 (0 - 0)
Rehabilitation 245 3 1.2% 0.00 (0 - 0)
Other 234 0 0.0% 0.00 (0 - 0)
National 10,044 39 0.4% 0.00 (0 - 0)
Facility Type
Total eligible
residents
Number of
residents
with an
infection
HAI Prevalence (%)
Median (IQRb)
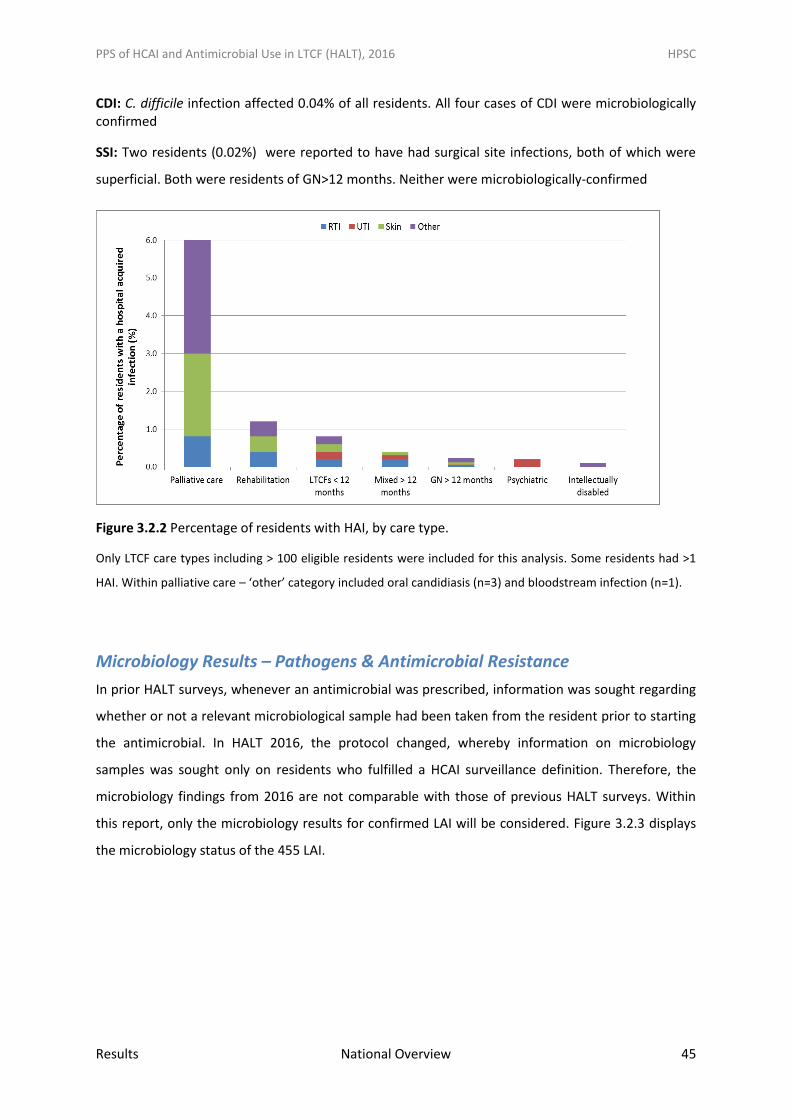
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 45
CDI: C. difficile infection affected 0.04% of all residents. All four cases of CDI were microbiologically confirmed
SSI: Two residents (0.02%) were reported to have had surgical site infections, both of which were
superficial. Both were residents of GN>12 months. Neither were microbiologically-confirmed
Figure 3.2.2 Percentage of residents with HAI, by care type.
Only LTCF care types including > 100 eligible residents were included for this analysis. Some residents had >1
HAI. Within palliative care – ‘other’ category included oral candidiasis (n=3) and bloodstream infection (n=1).
Microbiology Results – Pathogens & Antimicrobial Resistance
In prior HALT surveys, whenever an antimicrobial was prescribed, information was sought regarding
whether or not a relevant microbiological sample had been taken from the resident prior to starting
the antimicrobial. In HALT 2016, the protocol changed, whereby information on microbiology
samples was sought only on residents who fulfilled a HCAI surveillance definition. Therefore, the
microbiology findings from 2016 are not comparable with those of previous HALT surveys. Within
this report, only the microbiology results for confirmed LAI will be considered. Figure 3.2.3 displays
the microbiology status of the 455 LAI.
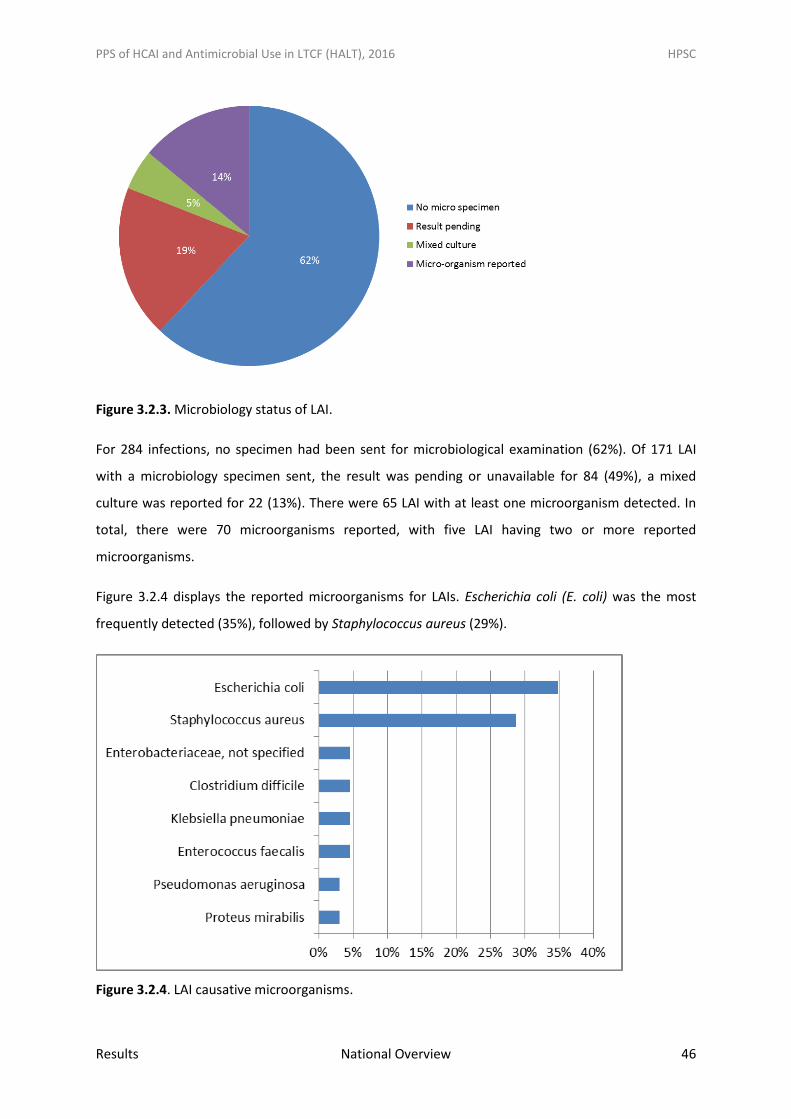
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 46
Figure 3.2.3. Microbiology status of LAI.
For 284 infections, no specimen had been sent for microbiological examination (62%). Of 171 LAI
with a microbiology specimen sent, the result was pending or unavailable for 84 (49%), a mixed
culture was reported for 22 (13%). There were 65 LAI with at least one microorganism detected. In
total, there were 70 microorganisms reported, with five LAI having two or more reported
microorganisms.
Figure 3.2.4 displays the reported microorganisms for LAIs. Escherichia coli (E. coli) was the most
frequently detected (35%), followed by Staphylococcus aureus (29%).
Figure 3.2.4. LAI causative microorganisms.

PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 47
Figures 3.2.5 and 3.2.6 display the proportion of pathogens reported from relevant positive
microbiological specimens taken from urinary tract and skin/wound LAIs. E. coli was the most
frequently isolated organism of 36 UTI with positive microbiology (62%, n=22), with S. aureus the
most frequently isolated organism from 17 skin/wound infections with positive microbiology (82%,
n=14). Just two RTIs had positive microbiology; Serratia marcescens (n=1) and unspecified Candida
species (n=1),with the latter likely colonising flora in the setting of RTI.
Figure 3.2.5 Causative pathogens of LTCF-acquired UTIs
Figure 3.2.6 Causative pathogens of LTCF-acquired skin/wound infections
Of 23 E. coli isolates, 3rd generation cephalosporin (3GC) susceptibility results were unknown for
52%, 44% were susceptible to 3GC, 4% were resistant to 3GC. There were no LAI with a positive
microbiology result for carbapenem resistant Enterobacteriaceae (CRE) reported (Figure 3.2.7).

PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 48
Figure 3.2.7 E. coli antimicrobial susceptibility results.
Of 19 Staphylococcus aureus isolates, 74% were susceptible (MSSA) and 16% were resistant to
meticillin/flucloxacillin (MRSA). For 10%, antimicrobial susceptibility results were unknown. (Figure
3.2.8)
Figure 3.2.8 Staphylococcus aureus antimicrobial susceptibility results.
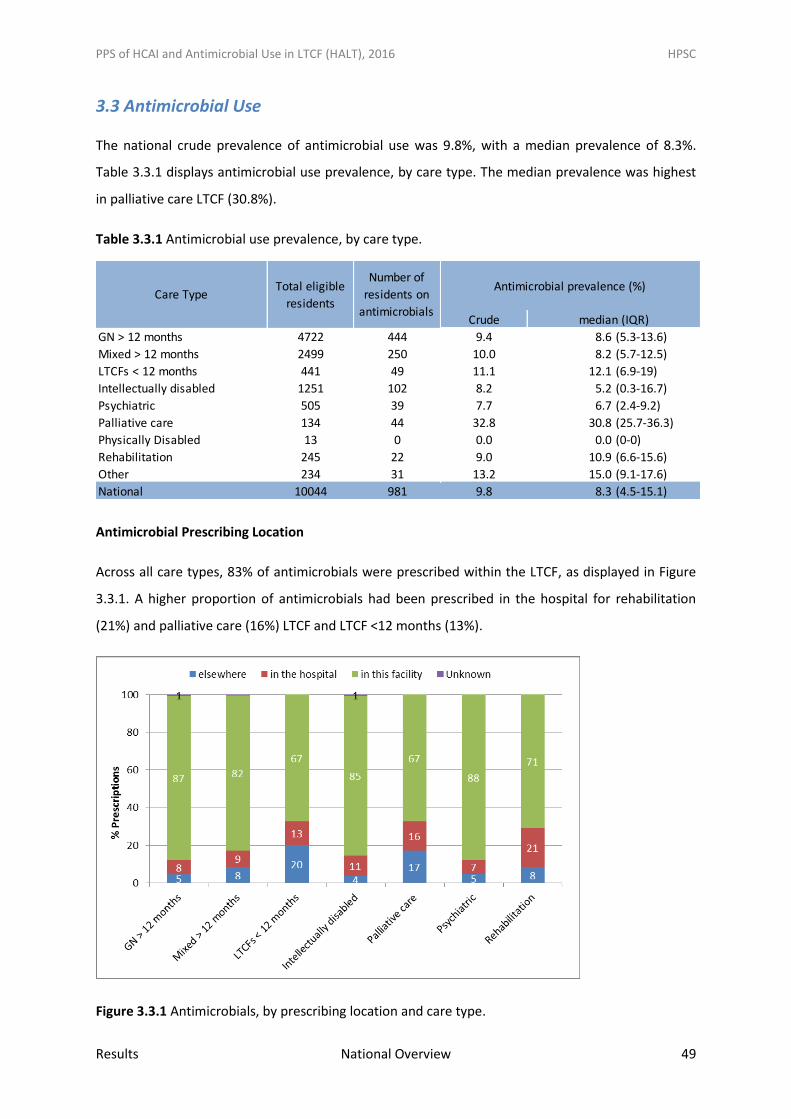
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 49
3.3 Antimicrobial Use
The national crude prevalence of antimicrobial use was 9.8%, with a median prevalence of 8.3%.
Table 3.3.1 displays antimicrobial use prevalence, by care type. The median prevalence was highest
in palliative care LTCF (30.8%).
Table 3.3.1 Antimicrobial use prevalence, by care type.
Antimicrobial Prescribing Location
Across all care types, 83% of antimicrobials were prescribed within the LTCF, as displayed in Figure
3.3.1. A higher proportion of antimicrobials had been prescribed in the hospital for rehabilitation
(21%) and palliative care (16%) LTCF and LTCF <12 months (13%).
Figure 3.3.1 Antimicrobials, by prescribing location and care type.
Crude
GN > 12 months 4722 444 9.4 8.6 (5.3-13.6)
Mixed > 12 months 2499 250 10.0 8.2 (5.7-12.5)
LTCFs < 12 months 441 49 11.1 12.1 (6.9-19)
Intellectually disabled 1251 102 8.2 5.2 (0.3-16.7)
Psychiatric 505 39 7.7 6.7 (2.4-9.2)
Palliative care 134 44 32.8 30.8 (25.7-36.3)
Physically Disabled 13 0 0.0 0.0 (0-0)
Rehabilitation 245 22 9.0 10.9 (6.6-15.6)
Other 234 31 13.2 15.0 (9.1-17.6)
National 10044 981 9.8 8.3 (4.5-15.1)
Care TypeTotal eligible
residents
Number of
residents on
antimicrobials
Antimicrobial prevalence (%)
median (IQR)
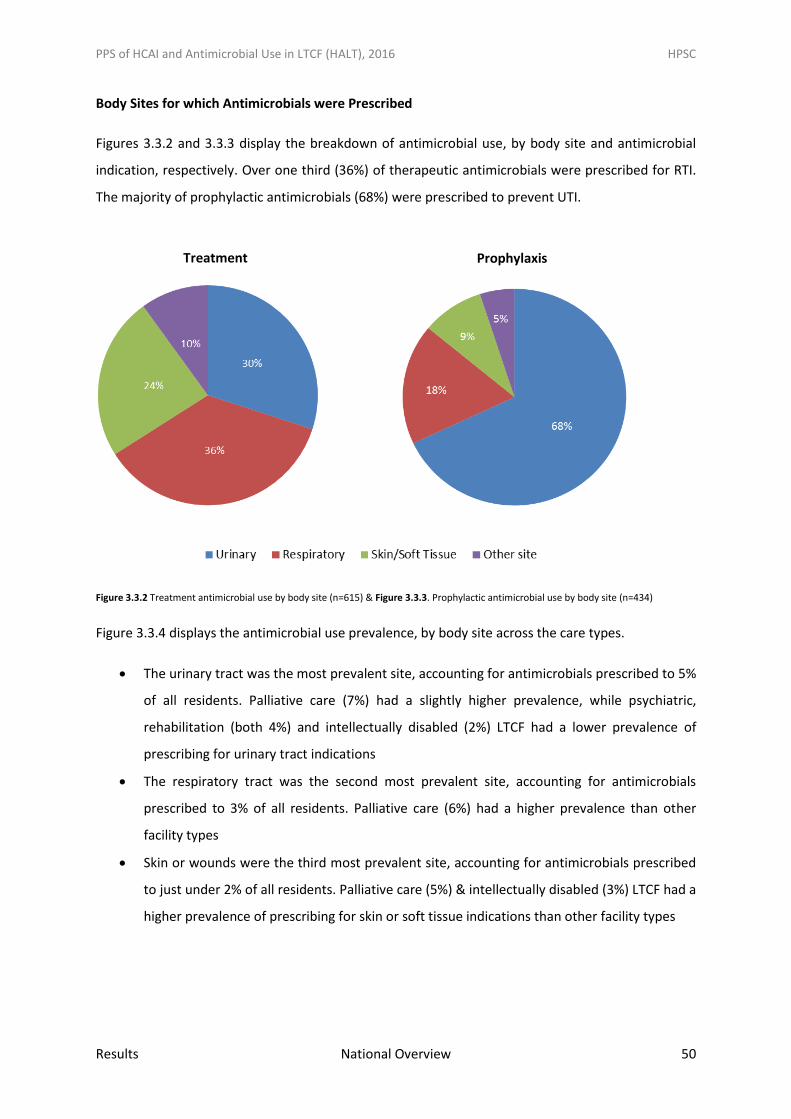
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 50
Body Sites for which Antimicrobials were Prescribed
Figures 3.3.2 and 3.3.3 display the breakdown of antimicrobial use, by body site and antimicrobial
indication, respectively. Over one third (36%) of therapeutic antimicrobials were prescribed for RTI.
The majority of prophylactic antimicrobials (68%) were prescribed to prevent UTI.
Figure 3.3.2 Treatment antimicrobial use by body site (n=615) & Figure 3.3.3. Prophylactic antimicrobial use by body site (n=434)
Figure 3.3.4 displays the antimicrobial use prevalence, by body site across the care types.
The urinary tract was the most prevalent site, accounting for antimicrobials prescribed to 5%
of all residents. Palliative care (7%) had a slightly higher prevalence, while psychiatric,
rehabilitation (both 4%) and intellectually disabled (2%) LTCF had a lower prevalence of
prescribing for urinary tract indications
The respiratory tract was the second most prevalent site, accounting for antimicrobials
prescribed to 3% of all residents. Palliative care (6%) had a higher prevalence than other
facility types
Skin or wounds were the third most prevalent site, accounting for antimicrobials prescribed
to just under 2% of all residents. Palliative care (5%) & intellectually disabled (3%) LTCF had a
higher prevalence of prescribing for skin or soft tissue indications than other facility types
Treatment Prophylaxis
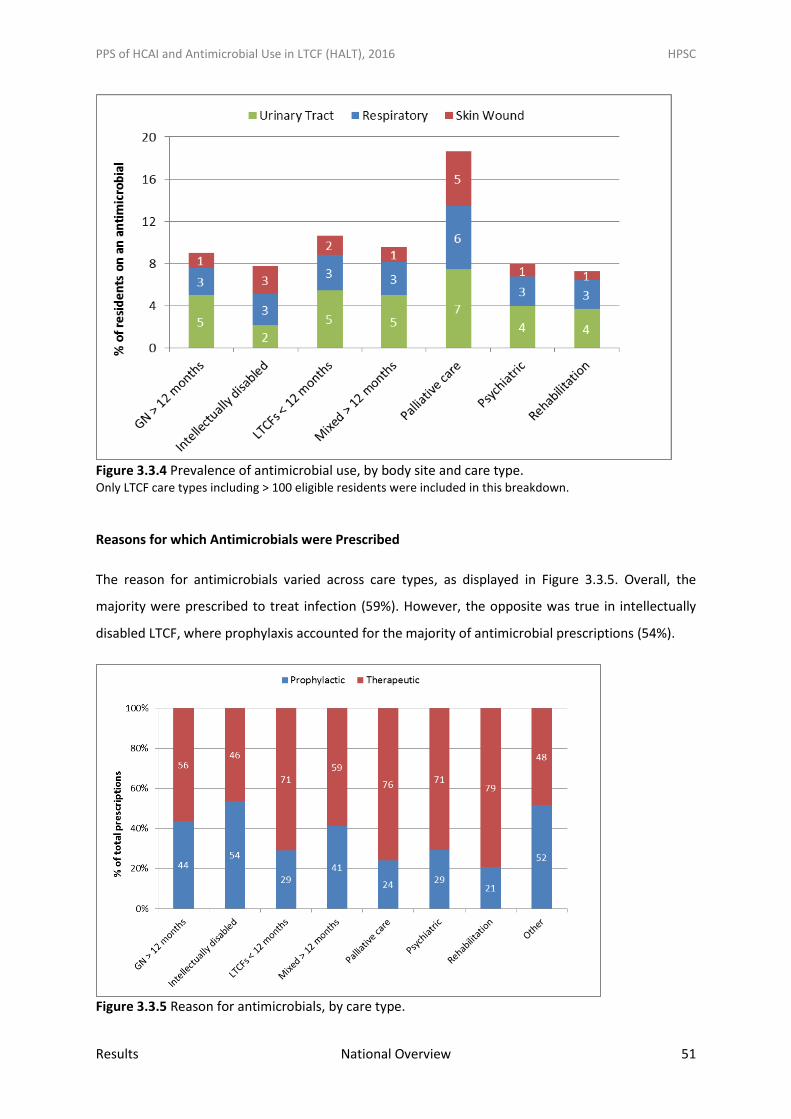
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 51
Figure 3.3.4 Prevalence of antimicrobial use, by body site and care type. Only LTCF care types including > 100 eligible residents were included in this breakdown.
Reasons for which Antimicrobials were Prescribed
The reason for antimicrobials varied across care types, as displayed in Figure 3.3.5. Overall, the
majority were prescribed to treat infection (59%). However, the opposite was true in intellectually
disabled LTCF, where prophylaxis accounted for the majority of antimicrobial prescriptions (54%).
Figure 3.3.5 Reason for antimicrobials, by care type.
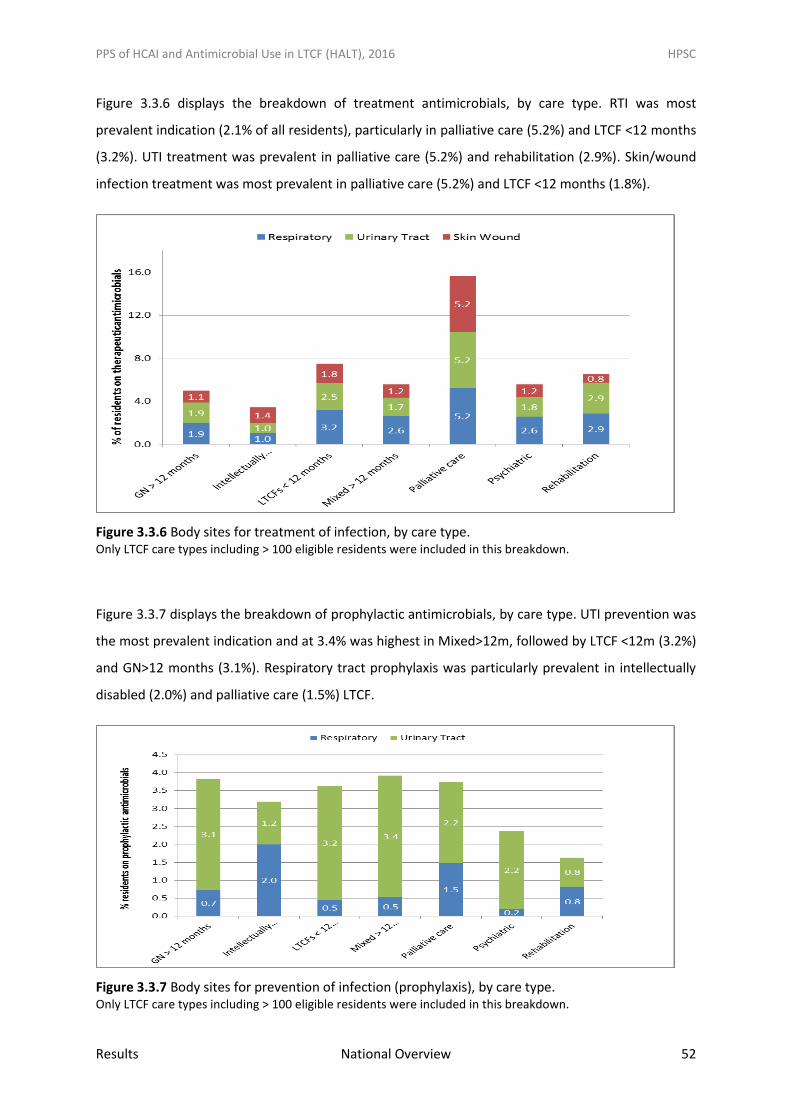
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 52
Figure 3.3.6 displays the breakdown of treatment antimicrobials, by care type. RTI was most
prevalent indication (2.1% of all residents), particularly in palliative care (5.2%) and LTCF <12 months
(3.2%). UTI treatment was prevalent in palliative care (5.2%) and rehabilitation (2.9%). Skin/wound
infection treatment was most prevalent in palliative care (5.2%) and LTCF <12 months (1.8%).
Figure 3.3.6 Body sites for treatment of infection, by care type. Only LTCF care types including > 100 eligible residents were included in this breakdown.
Figure 3.3.7 displays the breakdown of prophylactic antimicrobials, by care type. UTI prevention was
the most prevalent indication and at 3.4% was highest in Mixed>12m, followed by LTCF <12m (3.2%)
and GN>12 months (3.1%). Respiratory tract prophylaxis was particularly prevalent in intellectually
disabled (2.0%) and palliative care (1.5%) LTCF.
Figure 3.3.7 Body sites for prevention of infection (prophylaxis), by care type. Only LTCF care types including > 100 eligible residents were included in this breakdown.
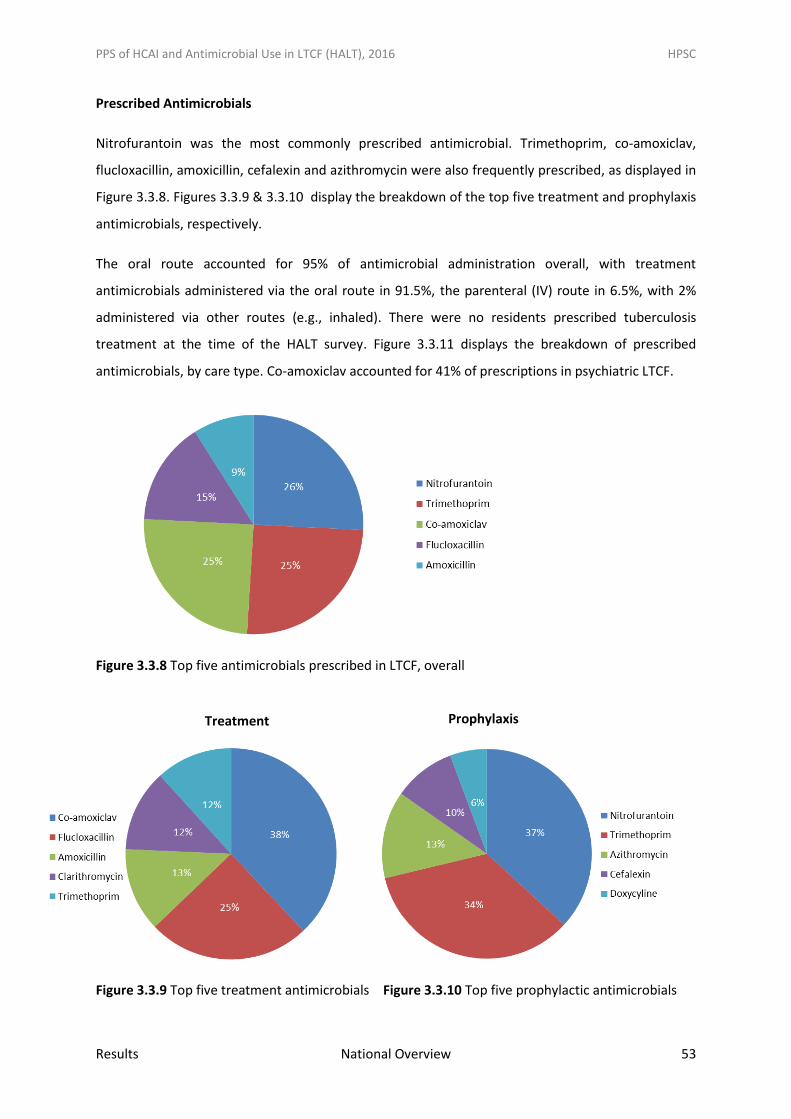
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 53
Prescribed Antimicrobials
Nitrofurantoin was the most commonly prescribed antimicrobial. Trimethoprim, co-amoxiclav,
flucloxacillin, amoxicillin, cefalexin and azithromycin were also frequently prescribed, as displayed in
Figure 3.3.8. Figures 3.3.9 & 3.3.10 display the breakdown of the top five treatment and prophylaxis
antimicrobials, respectively.
The oral route accounted for 95% of antimicrobial administration overall, with treatment
antimicrobials administered via the oral route in 91.5%, the parenteral (IV) route in 6.5%, with 2%
administered via other routes (e.g., inhaled). There were no residents prescribed tuberculosis
treatment at the time of the HALT survey. Figure 3.3.11 displays the breakdown of prescribed
antimicrobials, by care type. Co-amoxiclav accounted for 41% of prescriptions in psychiatric LTCF.
Figure 3.3.8 Top five antimicrobials prescribed in LTCF, overall
Figure 3.3.9 Top five treatment antimicrobials Figure 3.3.10 Top five prophylactic antimicrobials
Treatment Prophylaxis
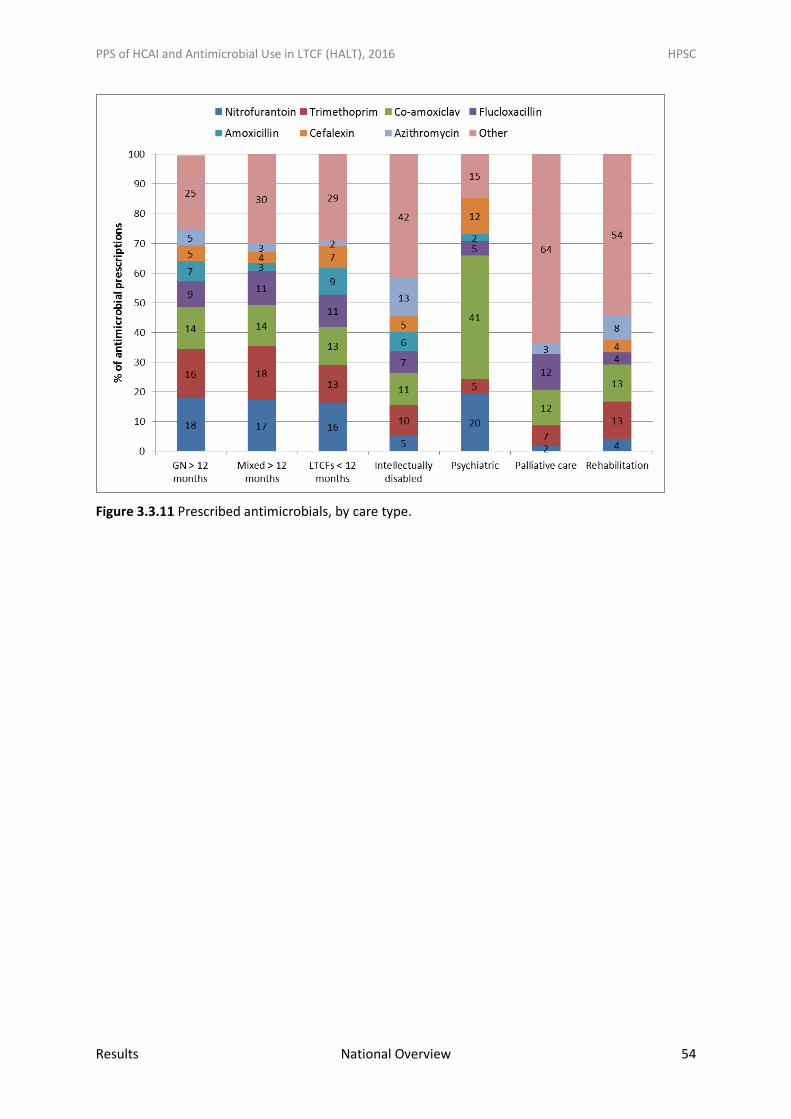
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 54
Figure 3.3.11 Prescribed antimicrobials, by care type.
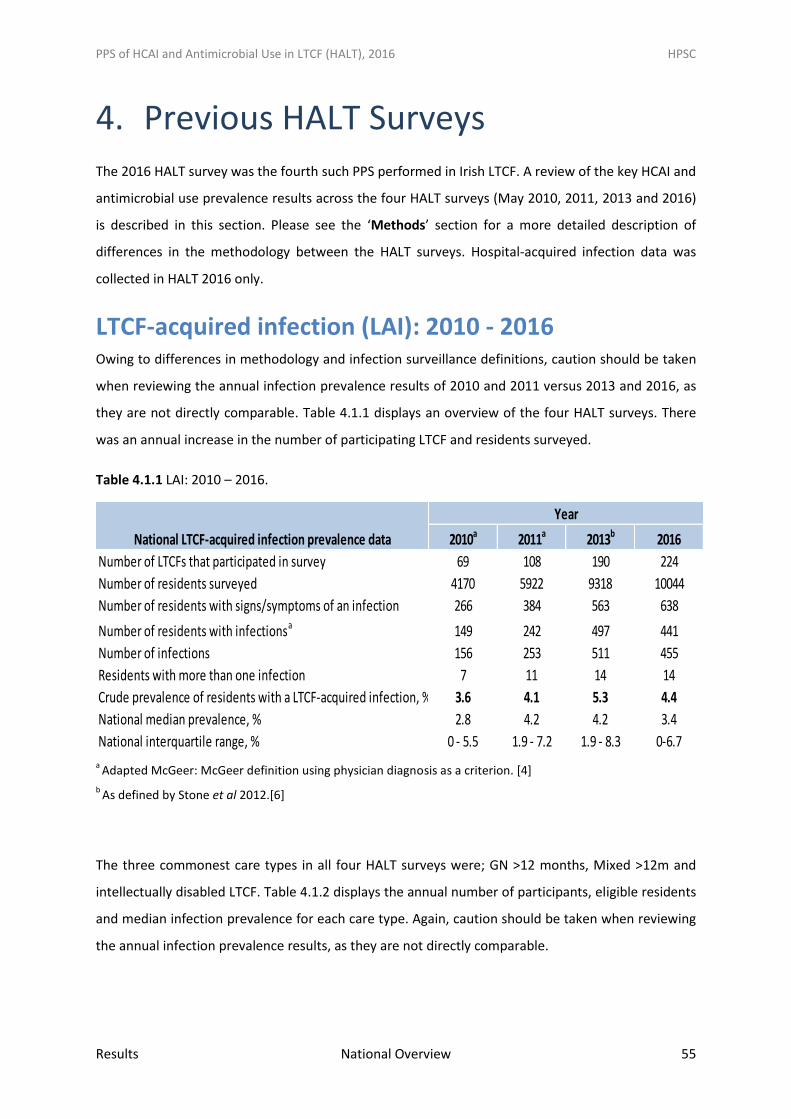
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 55
4. Previous HALT Surveys
The 2016 HALT survey was the fourth such PPS performed in Irish LTCF. A review of the key HCAI and
antimicrobial use prevalence results across the four HALT surveys (May 2010, 2011, 2013 and 2016)
is described in this section. Please see the ‘Methods’ section for a more detailed description of
differences in the methodology between the HALT surveys. Hospital-acquired infection data was
collected in HALT 2016 only.
LTCF-acquired infection (LAI): 2010 - 2016 Owing to differences in methodology and infection surveillance definitions, caution should be taken
when reviewing the annual infection prevalence results of 2010 and 2011 versus 2013 and 2016, as
they are not directly comparable. Table 4.1.1 displays an overview of the four HALT surveys. There
was an annual increase in the number of participating LTCF and residents surveyed.
Table 4.1.1 LAI: 2010 – 2016.
a
Adapted McGeer: McGeer definition using physician diagnosis as a criterion. [4]
b As defined by Stone et al 2012.[6]
The three commonest care types in all four HALT surveys were; GN >12 months, Mixed >12m and
intellectually disabled LTCF. Table 4.1.2 displays the annual number of participants, eligible residents
and median infection prevalence for each care type. Again, caution should be taken when reviewing
the annual infection prevalence results, as they are not directly comparable.
2010a 2011a 2013b 2016
Number of LTCFs that participated in survey 69 108 190 224
Number of residents surveyed 4170 5922 9318 10044
Number of residents with signs/symptoms of an infection 266 384 563 638
Number of residents with infectionsa 149 242 497 441
Number of infections 156 253 511 455
Residents with more than one infection 7 11 14 14
Crude prevalence of residents with a LTCF-acquired infection, % 3.6 4.1 5.3 4.4
National median prevalence, % 2.8 4.2 4.2 3.4
National interquartile range, % 0 - 5.5 1.9 - 7.2 1.9 - 8.3 0-6.7
Year
National LTCF-acquired infection prevalence data
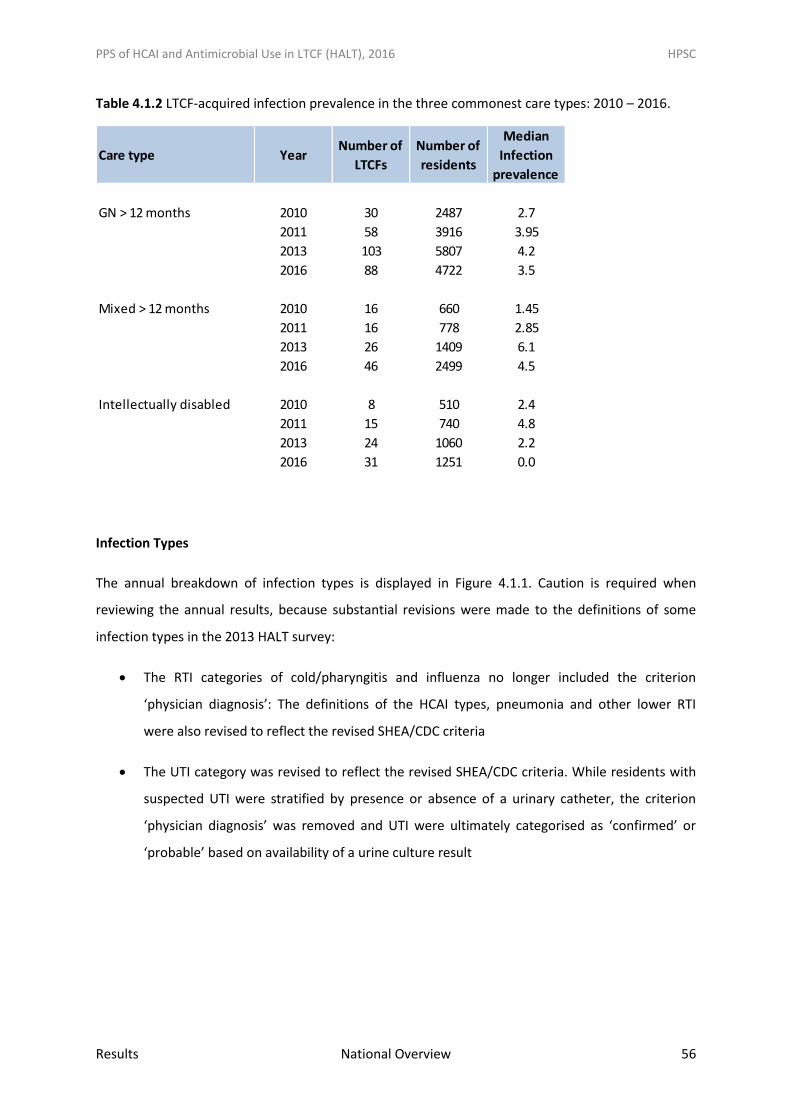
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 56
Table 4.1.2 LTCF-acquired infection prevalence in the three commonest care types: 2010 – 2016.
Infection Types
The annual breakdown of infection types is displayed in Figure 4.1.1. Caution is required when
reviewing the annual results, because substantial revisions were made to the definitions of some
infection types in the 2013 HALT survey:
The RTI categories of cold/pharyngitis and influenza no longer included the criterion
‘physician diagnosis’: The definitions of the HCAI types, pneumonia and other lower RTI
were also revised to reflect the revised SHEA/CDC criteria
The UTI category was revised to reflect the revised SHEA/CDC criteria. While residents with
suspected UTI were stratified by presence or absence of a urinary catheter, the criterion
‘physician diagnosis’ was removed and UTI were ultimately categorised as ‘confirmed’ or
‘probable’ based on availability of a urine culture result
Care type YearNumber of
LTCFs
Number of
residents
Median
Infection
prevalence
GN > 12 months 2010 30 2487 2.7
2011 58 3916 3.95
2013 103 5807 4.2
2016 88 4722 3.5
Mixed > 12 months 2010 16 660 1.45
2011 16 778 2.85
2013 26 1409 6.1
2016 46 2499 4.5
Intellectually disabled 2010 8 510 2.4
2011 15 740 4.8
2013 24 1060 2.2
2016 31 1251 0.0
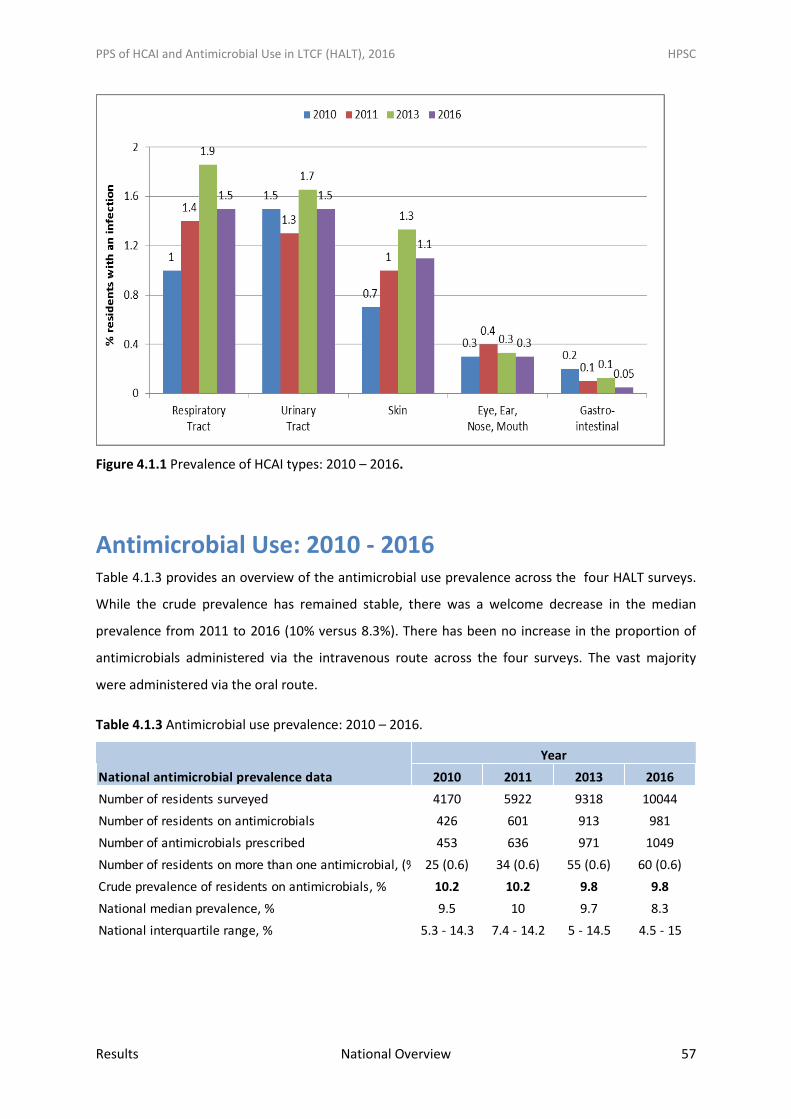
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 57
Figure 4.1.1 Prevalence of HCAI types: 2010 – 2016.
Antimicrobial Use: 2010 - 2016 Table 4.1.3 provides an overview of the antimicrobial use prevalence across the four HALT surveys.
While the crude prevalence has remained stable, there was a welcome decrease in the median
prevalence from 2011 to 2016 (10% versus 8.3%). There has been no increase in the proportion of
antimicrobials administered via the intravenous route across the four surveys. The vast majority
were administered via the oral route.
Table 4.1.3 Antimicrobial use prevalence: 2010 – 2016.
National antimicrobial prevalence data 2010 2011 2013 2016
Number of residents surveyed 4170 5922 9318 10044
Number of residents on antimicrobials 426 601 913 981
Number of antimicrobials prescribed 453 636 971 1049
Number of residents on more than one antimicrobial, (%) 25 (0.6) 34 (0.6) 55 (0.6) 60 (0.6)
Crude prevalence of residents on antimicrobials, % 10.2 10.2 9.8 9.8
National median prevalence, % 9.5 10 9.7 8.3
National interquartile range, % 5.3 - 14.3 7.4 - 14.2 5 - 14.5 4.5 - 15
Year
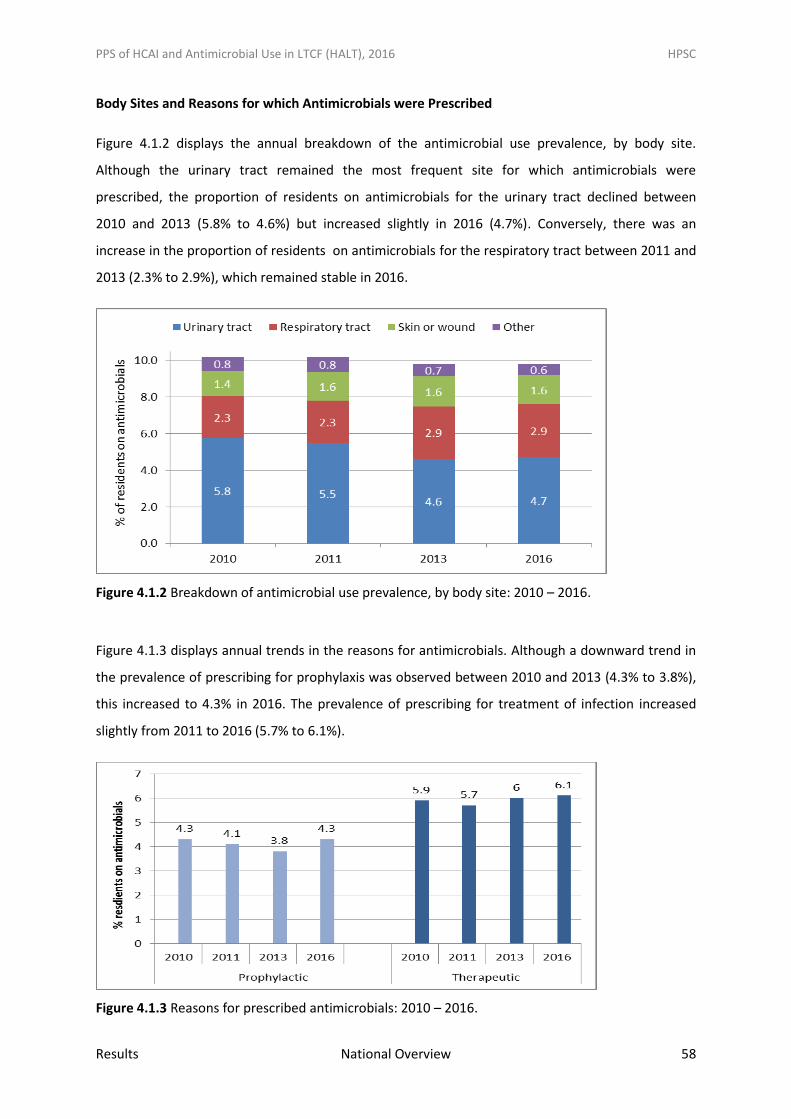
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 58
Body Sites and Reasons for which Antimicrobials were Prescribed
Figure 4.1.2 displays the annual breakdown of the antimicrobial use prevalence, by body site.
Although the urinary tract remained the most frequent site for which antimicrobials were
prescribed, the proportion of residents on antimicrobials for the urinary tract declined between
2010 and 2013 (5.8% to 4.6%) but increased slightly in 2016 (4.7%). Conversely, there was an
increase in the proportion of residents on antimicrobials for the respiratory tract between 2011 and
2013 (2.3% to 2.9%), which remained stable in 2016.
Figure 4.1.2 Breakdown of antimicrobial use prevalence, by body site: 2010 – 2016.
Figure 4.1.3 displays annual trends in the reasons for antimicrobials. Although a downward trend in
the prevalence of prescribing for prophylaxis was observed between 2010 and 2013 (4.3% to 3.8%),
this increased to 4.3% in 2016. The prevalence of prescribing for treatment of infection increased
slightly from 2011 to 2016 (5.7% to 6.1%).
Figure 4.1.3 Reasons for prescribed antimicrobials: 2010 – 2016.
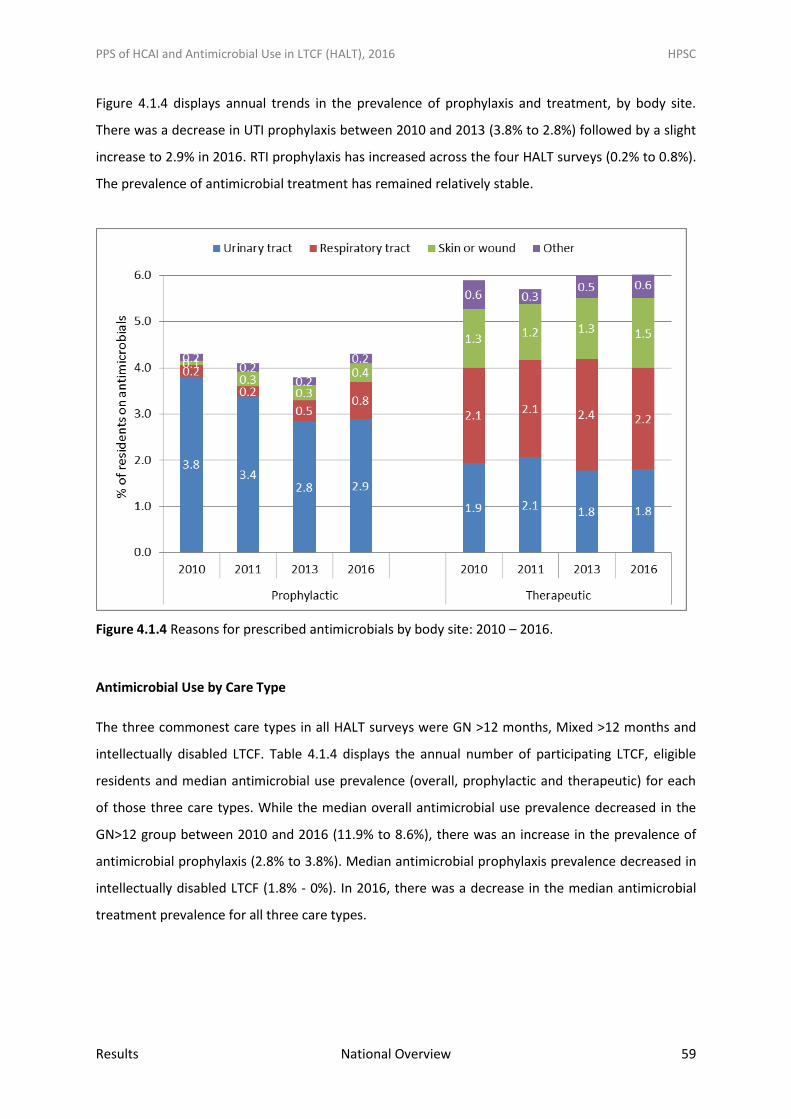
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 59
Figure 4.1.4 displays annual trends in the prevalence of prophylaxis and treatment, by body site.
There was a decrease in UTI prophylaxis between 2010 and 2013 (3.8% to 2.8%) followed by a slight
increase to 2.9% in 2016. RTI prophylaxis has increased across the four HALT surveys (0.2% to 0.8%).
The prevalence of antimicrobial treatment has remained relatively stable.
Figure 4.1.4 Reasons for prescribed antimicrobials by body site: 2010 – 2016.
Antimicrobial Use by Care Type
The three commonest care types in all HALT surveys were GN >12 months, Mixed >12 months and
intellectually disabled LTCF. Table 4.1.4 displays the annual number of participating LTCF, eligible
residents and median antimicrobial use prevalence (overall, prophylactic and therapeutic) for each
of those three care types. While the median overall antimicrobial use prevalence decreased in the
GN>12 group between 2010 and 2016 (11.9% to 8.6%), there was an increase in the prevalence of
antimicrobial prophylaxis (2.8% to 3.8%). Median antimicrobial prophylaxis prevalence decreased in
intellectually disabled LTCF (1.8% - 0%). In 2016, there was a decrease in the median antimicrobial
treatment prevalence for all three care types.
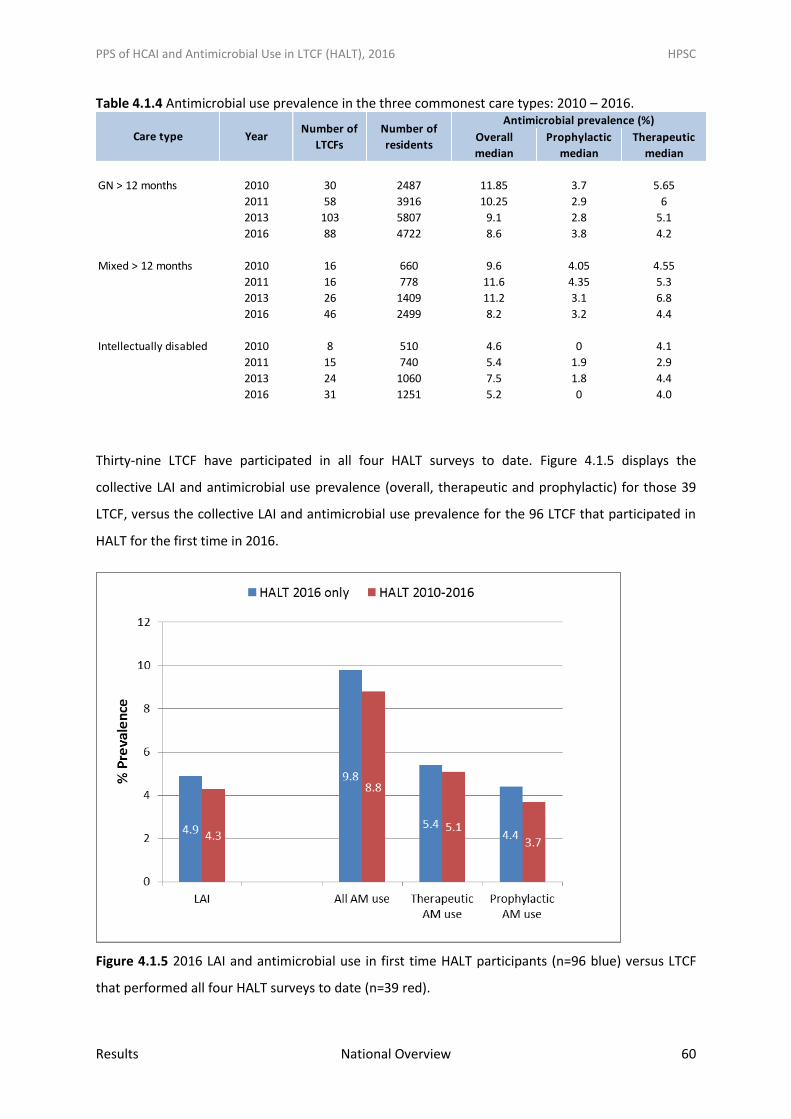
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Results National Overview 60
Table 4.1.4 Antimicrobial use prevalence in the three commonest care types: 2010 – 2016.
Thirty-nine LTCF have participated in all four HALT surveys to date. Figure 4.1.5 displays the
collective LAI and antimicrobial use prevalence (overall, therapeutic and prophylactic) for those 39
LTCF, versus the collective LAI and antimicrobial use prevalence for the 96 LTCF that participated in
HALT for the first time in 2016.
Figure 4.1.5 2016 LAI and antimicrobial use in first time HALT participants (n=96 blue) versus LTCF
that performed all four HALT surveys to date (n=39 red).
Overall Prophylactic Therapeutic
median median median
GN > 12 months 2010 30 2487 11.85 3.7 5.65
2011 58 3916 10.25 2.9 6
2013 103 5807 9.1 2.8 5.1
2016 88 4722 8.6 3.8 4.2
Mixed > 12 months 2010 16 660 9.6 4.05 4.55
2011 16 778 11.6 4.35 5.3
2013 26 1409 11.2 3.1 6.8
2016 46 2499 8.2 3.2 4.4
Intellectually disabled 2010 8 510 4.6 0 4.1
2011 15 740 5.4 1.9 2.9
2013 24 1060 7.5 1.8 4.4
2016 31 1251 5.2 0 4.0
Care type
Antimicrobial prevalence (%)
YearNumber of
LTCFs
Number of
residents
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Discussion 61
5. Discussion Ireland contributed approximately 10% of the total resident population in the 2010 and 2013
European HALT surveys, with 2016 data expected from ECDC in 2018. Four HALT surveys have been
undertaken in Ireland (May 2010, 2011, 2013 and 2016) and there has been a welcomed annual
increase in the numbers of participants, including HSE, voluntary and private LTCF. In 2016, 96 LTCF
performed their first HALT survey (43%). This highlights the ongoing dedication of healthcare
professionals in Irish LTCF to improving the quality and safety of resident care. However, the
majority of residential care facilities registered with HIQA did not participate in HALT 2016. It is
recommended that evidence of each LTCF’s participation in HALT surveys be actively sought during
future monitoring inspections conducted by Health Information & Quality Authority (HIQA) and the
Mental Health Commission (MHC) and that all LTCF are encouraged to and facilitated in participating
in future HALT surveys.
The voluntary HALT survey provides participants with valuable information regarding infrastructure,
staffing, models of medical care, IPC and antimicrobial stewardship practices, resident dependency
levels, HCAI risk factors, HCAI and antimicrobial prescribing in Irish LTCF. The HALT survey clearly
demonstrates the diversity within the Irish long-term care population. In an attempt to reflect this
and provide a more meaningful interpretation of the data collected, LTCF were subdivided into eight
separate care types, which best reflected the typical characteristics and length-of-stay for the
majority of residents. The top three care types combined, which were predominantly long-stay
facilities (GN>12m, Mixed>12m and intellectually disabled LTCF), accounted for 84% of residents
surveyed. The results demonstrate differences between Irish LTCF care types, with regard to
resident demographics, nursing care load indicators, HCAI risk factors, LAI & HAI prevalence,
infection types, antimicrobial use prevalence and antimicrobial prescribing practices. The female
gender predominated across LTCF care types, other than psychiatric and palliative care LTCF.
Residents of intellectually disabled, psychiatric and palliative care LTCF tended to have a younger age
profile than residents of other care types. In November 2016, participating LTCF were provided with
a HALT report displaying the local results and enabling comparison with the collective results for
LTCF of the same care type. For prior HALT participants, review of the LTCF’s performance over time
was also provided.
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Discussion 62
Standards
In Ireland, facilities providing residential care to older people are legally required to register with
HIQA. In 2009, HIQA published National Quality Standards for Residential Care Settings for Older
People in Ireland and updated Standards were published in 2016, with facilities inspected by HIQA
according to these standards. (10,11) There were 580 older persons LTCF listed as registered on
HIQA’s website in February 2017.
Inpatient facilities providing care and treatment to people with a mental illness must be listed on the
register of approved centres, maintained by the MHC, the responsible body for regulating and
monitoring mental health services in Ireland. In 2007, MHC published a Quality Framework for
Mental Health Services in Ireland, which comprises 24 standards and mental health services are
monitored according to these standards. (14) According to the MHC Annual Report for 2015, there
were 61 approved centres with 2,767 beds in December 2015. (41) The addition of a requirement for
psychiatric LTCF to undertake HCAI prevention and antimicrobial stewardship to the MHC’s
standards should be progressed as a matter of priority, particularly as the crude infection prevalence
in psychiatric LTCF was very similar to that in GN>12m (3.8% and 4.0%, respectively).
Effective November 1st 2013, HIQA became the responsible body for regulation of residential
services for children and adults with disabilities. This followed publication of the National Standards
for Residential Services for Children and Adults with Disabilities in January 2013. (15) According to
the National Intellectual Disability Database (NIID), in December 2015, there were 7,724 people in
residential care settings in Ireland. (45)
Staffing
The requirement for each LTCF to have sufficient staff with necessary skills to deliver safe resident
care is enshrined in HIQA Standards for residential care of older people and people with disabilities
and in the MHC standards for psychiatric facilities. (11, 14, 15)
The 2016 HALT survey sought information on nurse and healthcare assistant staffing levels within
participating LTCF for the first time. The analysis for the European HALT survey reports published to
date have focused on nursing homes and mixed care type LTCF only. Upon publication of the
European HALT report by ECDC, which is expected during 2018, it will be possible to compare both
nurse and HCA staffing levels in the general nursing homes and mixed care type LTCF in all EU
Member States.
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Discussion 63
The nurse and HCA staffing data collected in HALT 2016 are not representative of the national
picture and should not be used to interpret nurse and HCA staffing levels for Irish LTCF in general, for
many reasons including; heterogeneity in care types, different categories of LTCF ownership, the
voluntary nature of the HALT survey, with incomplete participation in 2016. The wide range in
numbers of participating HSE-owned LTCF precluded analysis by CHO. Additionally, selected resident
care load indicators were collected in HALT, with no information on resident dependency or
comorbidities collected, which directly influence staffing levels within LTCF.
The HALT survey results have consistently demonstrated differences in the models of resident
medical care delivery, by ownership and geographical location. GP-led medical care is the preferred
model in privately-owned LTCF and when stratified by CHO, much commoner in CHOs 1, 2, 4, and 8
(Figure 3.1.2 and Appendix E). Regardless of the preferred medical care model, in accordance with
HIQA and MHC standards, each facility should have a clearly defined management structure, to
incorporate a defined system of clinical governance. The designation of a coordinating physician
role, with oversight of all elements of resident medical care is a valuable addition to LTCF
governance structures, especially as the median capacity of LTCF participating in HALT 2016 was 42
beds. In HALT 2016, the coordinating physician role was established in 62% of Irish LTCF overall (up
from 45% in 2013) and 56% of privately-owned LTCF (up from 26% in 2013).
The model of primary care delivery in Ireland is unique, with medical care delivered both by group
GP practices and individual GPs, with patients having the right to select their own GP. For example, if
a resident’s medical care in the community has been delivered by his or her local GP, the resident
may prefer to remain under their own GP’s care after moving into a LTCF. It is important that every
effort is made to accommodate a resident’s own preference for his/her medical care. Where a LTCF
already has or plans to develop a designated coordinating physician post, it is particularly important
that the GP-led and coordinating physician-led models of medical care do not become mutually
exclusive and that residents benefit from the input of both types of healthcare professional.
There are many potential duties for a coordinating physician, depending upon the needs of each
LTCF’s resident population. The HALT survey results demonstrate how the presence of a
coordinating physician was consistently associated with a higher prevalence of positive antimicrobial
stewardship practices. Access to a coordinating physician would undoubtedly have other potential
benefits for resident medical care, beyond antimicrobial stewardship practices.
A recommended intervention is the resourcing of external healthcare professionals to provide
specialist advice to all of the LTCF within a CHO, regardless of ownership. For example, the

PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Discussion 64
resourcing of specialist input from a geriatrician with a community remit to review residents and
their prescribed medicines, to identify opportunities to refine chronic medications and minimise
polypharmacy issues and the input of a clinical microbiologist with a community remit, to provide
advice and oversee the development of antimicrobial stewardship, infection prevention and control
education, guidelines and surveillance programmes, as part of a wider multi-disciplinary community
IPC and antimicrobial stewardship team.
There is undoubtedly a severe shortage of specialist IPC resources for Irish LTCF. Almost one quarter
of all LTCF participating in HALT 2016 (24%) reported having no access to a staff member with
specialist IPC training, which reflects an improvement from 38% without access in HALT 2013. The
deficit was even more marked in privately-owned LTCF (43%), but improved from 90% in HALT 2013.
Additional analysis performed after HALT 2013, reported an overall estimated WTE IPCN:LTCF bed
ratio for Ireland of 1:496 which was much higher than the 1:250, previously recommended by a
Canadian expert group. (16) It should be noted that the Canadian recommendation was based on an
evaluation of IPCNs working specifically within LTCF and did not take into account the much broader
remit of the community-based IPCN role in Ireland. Typically, community IPCNs are involved in
provision of IPC advice, education and training, development of policies, procedures and guidelines,
audit and surveillance activity across the breadth of community health services, incorporating
primary care, dentistry and long-term care. Therefore, it could be anticipated that the adequate
community IPCN resource required in Ireland could be even higher than 1:250 LTCF beds. During
2015, the HSE HCAI & AMR Clinical Programme commenced a project to identify current IPCN
resources for non-acute healthcare settings in Ireland. Key findings included; variance in the IPC
service provided across LTCF, with many areas reporting limited or no access to an IPCN, a lack of
clarity regarding the job specification for community IPCNs, with many working in isolation without
the support of a multi-disciplinary team, covering large geographical areas, without administrative
support and a lack of clarity surrounding governance and reporting relationships within CHOs, which
were established in 2014. There is a need for each CHO to undertake a gap analysis of existing
community IPCN resources and to develop a workforce plan to recruit sufficient numbers of
community IPCNs, who will have a remit over all LTCF within the CHO, regardless of care type or
ownership. Building multi-disciplinary IPC and antimicrobial stewardship teams within each CHOs is a
critical intervention to address the priorities identified from HALT surveys performed to date.
It is also important to make the distinction between the knowledge and skills of a healthcare
professional with specialist IPC training (IPCN) and a healthcare professional (e.g., staff nurse) who
has received some introductory IPC training and has an interest in supporting the practice of the
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Discussion 65
IPCN specialist, the so-called IPC link nurse or link practitioner. (17) In addition to enhancing the
skills and practice of the IPC link practitioner, such roles support and facilitate the specialist role of
the IPCN. In recent years, courses providing an introduction to HCAI and IPC for healthcare workers,
including LTCF staff have been faciliated by the HPSC, the Royal College of Surgeons in Ireland,
University College Cork and the University of Limerick. While the development of an IPC link nurse
role within each LTCF should be facilitated and encouraged, it cannot replace the urgent need to
improve the overall specialist community IPCN staffing levels in Ireland.
Links between the acute hospital and LTCF
Infection acquired within LTCF is a common issue, with a crude prevalence of 4.4% in all LTCF
residents in May 2016. This figure is similar to the crude prevalence of hospital-acquired infection
(HAI) reported from the May 2012 hospital PPS during which 9,030 inpatients in 50 acute hospitals
were surveyed and 5.2% were reported to have a HAI. (18) The hospital PPS will be repeated across
Ireland in May 2017.
For the first time, HALT 2016, collected data on HAI, in addition to long-term care acquired infections
(LAI), which has been collected as part of all HALT surveys to date. The addition of a HAI category
added complexity to the HALT protocol and data collector training. A data field ‘infection imported’
was added to the resident questionnaire to capture HAI. This was straightforward if a resident
developed signs and symptoms matching the surveillance case definition and required timeline for
HAI (e.g., symptom onset on day one or day two after discharge from hospital to the LTCF or specific
timelines for CDI and SSI). However, if a resident was transferred from hospital to the LTCF already
on treatment for a HAI which had begun while in the hospital, the protocol allowed the resident to
be categorised as having a HAI, despite data collectors not having access to documented evidence of
signs or symptoms for the infection which started in the hospital. This questions the validity of the
categorisation of such HAI, in the absence of access to documentation that the surveillance
definition for the infection was actually met. In 2016, just 12% of LTCF reported a total of 42 HAI,
with the vast majority of all HCAI (455; 92%) acquired within the LTCF (LAI). These findings and the
practical difficulties encountered during training and data collection support a recommendation that
HAI data is excluded from future European HALT surveys.
During HALT 2013, 2% of LTCF residents were absent from the facility owing to hospitalisation. This
data was not captured in HALT 2016. The 2013 results highlighted the frequent exchange of
patients/residents between acute hospitals and LTCF. LAI may result in residents requiring
hospitalisation for further management. Additionally, in the period following an acute illness for
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Discussion 66
which hospitalisation is required, a LTCF resident may be more vulnerable to acquiring infection. It is
critically important to ensure excellent communication between the acute hospital and the LTCF,
especially when residents are being transferred between the two settings. For example, where
hospital referral becomes indicated for a resident with a transmissible infection such as influenza-
like illness or diarrhoea of potentially infectious aetiology or a resident has a positive result for an
antimicrobial resistant organism (e.g., MRSA, ESBLs, CRE/CPE, VRE etc.) or a resident is being
transferred from a LTCF with an ongoing outbreak, this information must be conveyed to the
receiving healthcare facility to ensure safe placement and management of the resident. Likewise,
where the resident is transferred back to the LTCF, all relevant information (e.g., colonisation or
infection with antimicrobial resistant organisms, presence of indwelling devices, ongoing
antimicrobial therapy and infection issues) must be provided by the hospital to the LTCF prior to the
arrival of the resident, again to faciliate safe placement and management. With this in mind, it is
recommended that the development of a generic inter-facility transfer template to capture critical
information should be progressed at a national level and disseminated for local implementation by
all acute hospitals and LTCF.
Antimicrobial stewardship & surveillance
After four HALT surveys, while the crude prevalence of antimicrobial use in Irish LTCF has remained
unchanged, with around 1 in 10 residents prescribed antimicrobials, the median prevalence has
decreased, from 10% (2011) to 8.3% (2016). The 2013 European HALT report found that residents of
Irish LTCF were more than twice as likely to be on an antimicrobial than their European
counterparts, where the crude prevalence of antimicrobial use was just 4.4%. Ireland ranked sixth
highest of 19 EU Member States participating in HALT 2013 for the proportion of prophylactic
antimicrobials. (6) It is a positive finding that for the 39 Irish LTCF that have participated in all HALT
surveys to date, overall antimicrobial prevalence (8.8%), therapeutic prevalence (5.1%) and
prophylactic prevalence (3.7%) was lower than for the 96 LTCF participating in their first HALT in
2016 (9.8%, 5.4%, 4.4%, respectively).
Guidelines for antimicrobial prescribing in primary care in Ireland were issued in 2010 and are
periodically updated by the Primary Care Antimicrobial Guidelines Editorial Group. The guidelines
are available as a web version, suitable for use on mobile devices. The guidelines are endorsed by
the RCPI & HSE Clinical Advisory Group for HCAI and AMR and by the Irish College of General
Practitioners (ICGP) and it is recommended that these guidelines are used to guide prescribing in
LTCF. Co-amoxiclav is rarely recommended for treatment of infection in the community. In the Irish
guidelines, co-amoxiclav is a first line antimicrobial for quite limited infection indications (e.g.,
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Discussion 67
pyelonephritis, bite wounds) and a second line antimicrobial for sinusitis and infective exacerbations
of COPD unresponsive to first line treatments. Despite the recommendations of national guidelines,
in HALT 2016, co-amoxiclav accounted for 41% of all antimicrobials in psychiatric LTCF, versus 11 –
14% for all other care types. Of therapeutic prescriptions, co-amoxiclav was the most commonly
prescribed antimicrobial accounting for 38% of all prescriptions. Formal implementation of the
primary care prescribing guidelines within all Irish LTCF, regardless of care type is recommended and
has potential to positively impact on unnecessary use of broad spectrum antimicrobials, such as co-
amoxiclav. The guidelines may be viewed at www.antibioticprescribing.ie
Periodic PPS is useful to monitor trends over time, but can’t provide the same level of comparative
data as undertaking prospective incidence surveillance. It is recommended that HALT participants
build on HCAI and antimicrobial stewardship surveillance skills, developed from participation in HALT
surveys. Potential areas for local prospective surveillance by LTCF could include:
1. Daily monitoring of residents for new-onset of ‘alert’ symptoms and signs (fever, influenza-
like-illness, diarrhoea, vomiting, conjunctivitis, rash etc.). Such a programme would greatly
facilitate the early identification of potentially transmissible infections and mitigate the
development of outbreaks
2. Surveillance of UTI
3. Surveillance of C. difficile infection
4. Periodic surveillance of antimicrobial use, which might be incorporated into the requirement
for quarterly medicines reconciliation. This could be used to identify residents prescribed
prophylaxis, to review and discontinue such antimicrobials, where appropriate and to audit
compliance with local prescribing guidelines
It is recommended that surveillance protocols, training and user-friendly data collection methods for
incidence surveillance be developed specifically nationally, for use by LTCF within each CHO.
In HALT 2016, microbiology data was gathered for residents who met the case definition for
infection. This differs from previous HALT surveys when microbiology data was gathered for
residents prescribed antimicrobials, regardless of infection. Therefore, the microbiology data from
2016 is not comparable with prior HALT surveys. For the purposes of this report, analysis of
microbiology relates to LAI only, as microbiology results may not have been available to data
collectors for HAI, whereby specimens were submitted while the resident remained in hospital.
For the majority of LAI, no microbiology specimen was submitted to the laboratory (62%), with
microorganisms reported in just 14% of specimens taken from residents with LAI. The presence of a
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Discussion 68
microorganism in a clinical specimen does not necessarily confirm it was the causative pathogen of
the LAI (e.g., detection of candida from sputum reflects colonisers, rather than pathogens).
Although the issue of AMR has been long-recognised, it has received increasing attention in recent
years. Of particular concern is the successful dissemination of resistant Enterobacteriaceae (e.g., E.
coli and K. pneumoniae) both in acute hospitals and LTCF. Infections caused by these bacteria are
associated with increased morbidity and mortality. (19) Resistance genes encoding production of
extended spectrum β lactamases (ESBLs), carbapenemases and conferring resistance to additional
antimicrobial classes (e.g., fluoroquinolones and aminoglycosides), whereby bacteria are termed
multi-drug resistant (MDR) transmit readily. Outbreaks and increasing prevalence of antimicrobial
resistant Enterobacteriaceae are well-described in Irish LTCF. (20 – 22) Indeed, Enterobacteriaceae
(E. coli, K. pneumoniae, Proteus mirabilis and other Enterobacteriaceae) were the commonest
microorganisms reported from residents with LAI in HALT 2016.
The prevalence of MDR-Enterobacteriaceae (i.e., ESBL positive and resistant to both fluorquinolones
and aminoglycosides or carbapenemase-producers) has exhibited large increases in Ireland since
2010, with cases reported from both acute hospitals and LTCF (Source: HPSC). Increasing incidence
of MDR-K. pneumoniae (MDRKP) resulted in the establishment of a national enhanced surveillance
system in 2014. To the end of Q3 2016, it had become evident that MDRKP are widely disseminated
across the Irish healthcare system, with 15% of isolates reported from LTCF residents (Source: HPSC).
Of even greater concern, 16% of those were also carbapenem resistant (CRE).
Resistance to 3rd generation cephalosporins (3GC) is a potential marker for ESBL production.
Unfortunately, 3GC susceptibility results were unavailable for 52% of E. coli isolates in HALT 2016,
with 4% confirmed 3GC resistant. Fortunately, there were no cases of CRE reported during HALT
2016.
Improvements have been demonstrated in Ireland and abroad with regard to the proportions of
invasive infections caused by MRSA. In HALT 2016, Staphylococcus aureus accounted for 29% of
reported microorganisms, with 16% of S. aureus reported as MRSA.
From the HALT survey, it is evident that Irish LTCF rarely receive information regarding the
antimicrobial resistance profiles of common pathogens from their local microbiology laboratories.
Such information is important for the development of local prescribing guidelines and to inform
antimicrobial stewardship within LTCF.
Strict attention to standard and transmission-based precautions by all healthcare workers, careful
antimicrobial stewardship, excellent communication between the acute hospital and LTCF, coupled

PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Discussion 69
with ongoing healthcare worker education and surveillance are critical to halting the progressive
dissemination of antimicrobial resistant bacteria.
It is recommended that regional HCAI and AMR Committees are established within each CHO, with
governance over all LTCF within the CHO, regardless of care type or ownership and multi-disciplinary
membership, including representation from LTCF, local acute hospitals and their microbiology
laboratories, community pharmacies, Departments of Public Health and the multi-disciplinary
community IPC & antimicrobial stewardship teams. Such Commitees should be resourced to provide
support to all LTCF within the CHO, with regard to education and training, surveillance activities,
data analysis, monitoring of agreed key performance indicators (KPIs) and feedback of comparative
HCAI surveillance and AMR data.
Prevention & Education
Seasonal influenza is an annual event. A safe vaccine is available, with an interim overall vaccine
efficacy (VE) estimate of 46% for those aged >65 years in the US 2016/17 season. VE depends on
match between vaccine and circulating influenza virus, with age and immune status also contributing
factors. (23, 24) Because of antigenic variance exhibited by the influenza virus, the vaccine must be
administered on an annual basis to optimise the match between vaccine and circulating influenza
types. The ideal time for vaccination is the autumn, prior to the anticipated onset of the annual
influenza season, to facilitate the recipient in mounting an optimal immune response prior to
potential exposure to the influenza virus. However, the vaccine may be administered at any time
during the influenza season and should be considered for any person in a category for which annual
seasonal influenza vaccine is recommended. National guidelines are available on the prevention and
management of influenza outbreaks in residential care facilities, with vaccination of residents and
healthcare workers key guideline recommendations. (25) Of the 224 LTCF participating in HALT 2016,
91% overall reported that annual seasonal influenza vaccine is offered to residents, a decline from
94% in 2013. However, an increase in participation by palliative care LTCF in 2016 may have
contributed to this. A survey of influenza vaccine uptake in residents of HSE-owned LTCF during the
2015-2016 influenza season reported that 87% of residents had been immunised against influenza
since the start of the season, an increase from 73% on the previous influenza season. (26)
Death is reported in 0.5 – 1.0 per 1000 cases of influenza. Research undertaken by the HPSC
estimates between 200 and 500 people in Ireland die each year from influenza-related illness. There
is a wealth of evidence that the elderly are at increased risk of both hospitalisation and death from
influenza infection. (27 – 29) During the 2015-16 influenza season in Ireland, 36 influenza outbreaks
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Discussion 70
were notified, 21 of which were in LTCF. Of 84 deaths reported during the 2015-16 influenza season,
the median patient age was 65 years and four deaths were associated with influenza outbreaks. (30)
LTCF residents are likely to come into contact with influenza virus via infected healthcare workers
and visitors. The protective effect of the seasonal influenza vaccine is diminished in elderly or
immunocompromised patients. It is for these reasons that vaccination of healthcare workers is
recommended in Irish immunisation guidelines. (31) However, a survey of influenza vaccine uptake
in healthcare workers in 101 Irish LTCF during the 2015-16 influenza season, reported that just 26%
had availed of the opportunity to be vaccinated, an increase from 15% during the 2012-13 season.
(26) A systematic review of the effect of influenza vaccination of healthcare personnel on morbidity
and mortality among patients concluded that this intervention can enhance patient safety, as there
is evidence that it reduces the rate of hospitalisation and death due to influenza. (32) A Cochrane
review on influenza vaccination for healthcare staff caring for LTCF residents aged >60 years found
just five studies for inclusion and reported serious risks of methodological bias and very low quality
evidence arising from the included studies. The review highlighted the need for high quality
randomised control trials in this area. (44) Seasonal influenza vaccination should be offered to all
residents and staff of Irish LTCF, regardless of ownership, throughout the season, with up-to-date
records maintained of resident and staff immunisation status. It is imperative that staff have easy
access to vaccination in the workplace, through peer vaccinator programmes and that clear and
accurate information is provided to inform their decisions on vaccination. The percentage of
residents and staff immunised against influenza annually should be a KPI subject to regular review by
the senior management team of every LTCF and via the governance structures of regional HCAI &
AMR Committees.
In addition to annual seasonal influenza vaccination, LTCF residents should be assessed for
immunisation against Streptococcus pneumoniae and hepatitis B virus, where recommended by the
Immunisation Guidelines for Ireland. Up-to-date and accessible vaccination records should be
maintained for every resident.
Hand hygiene is an evidence-based intervention to prevent transmission of pathogenic
microorganisms and to prevent HCAI. The World Health Organisation (WHO) has published
Guidelines for Hand Hygiene in Healthcare and the WHO five moments for hand hygiene are the
basis for hand hygiene education programmes and audit of compliance. (46) ABHR is the preferred
method recommended by WHO for hand hygiene when hands are not visibly soiled. In 2016, 68% of
LTCF reported that ABHR was the preferred hand hygiene method, an improvement from 53% in
2013.

PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Discussion 71
Hand hygiene education and compliance audit are well-established in acute hospitals in Ireland, with
biannual acute hospital compliance audit results published on the HPSC website since 2011 and
training for lead hand hygiene auditors in acute hospitals coordinated by the HPSC. (47) While hand
hygiene training was reported to have been provided in the past year by 83% of LTCF in HALT 2016,
this was a reduction from 88% in 2013. Compliance audit of hand hygiene was reported to have
been carried out in the past year by 51% of LTCF. Further data on the protocol, methodology and
audit results was not captured by HALT 2016. It must be noted that hand hygiene compliance audit
protocols for acute hospitals are not automatically transferrable to LTCF settings and development
of national hand hygiene compliance audit protocols and tools specific to LTCF are required, with roll
out of lead hand hygiene auditor training and a train-the-trainer approach for hand hygiene audit, to
ensure that meaningful hand hygiene audits are conducted, using the same methodology and that
audit results are comparable across different CHOs.
The use of antimicrobials to prevent infection (prophylaxis) is not uncommon. However, the
evidence for this practice is limited, especially for the indications where it appears to be most
frequently used in LTCF. In 2016, UTI prevention accounted for 68% of prophylactic prescribing and
was particularly prevalent in Mixed>12m (3.4%), LTCF<12m (3.2%) and GN>12m (3.1%). However,
the prevalence of prophylaxis against RTI has increased from 2.3% (2010) to 2.9% (2016) and in 2016
was particularly prevalent in intellectually disabled (2%) and palliative care (1.5%) LTCF. It is
recommended that the indications for and duration of prophylaxis in these resident populations
should be further evaluated, in conjunction with any available evidence for such practices.
In 2011, national guidelines for the prevention of catheter-associated UTI were published by the
HPSC and after the publication of the 2011 HALT national report, the HALT steering group and
community antimicrobial stewardship committee developed a guideline for diagnosis and
management of UTI in long-term care residents >65 years, which states that antimicrobial
prophylaxis is not recommended for the prevention of symptomatic UTI in catheterised patients.
(33, 34) It is therefore of concern that 17% of residents prescribed UTI prophylaxis in 2016 were
reportedly catheterised (n=50 of 294).
The 2011 guideline also states that antimicrobial prophylaxis may be considered in patients for
whom the number of urinary infections are of such frequency or severity that they chronically
impinge on function and well‐being. (34) Guidance is also provided on signs and symptoms of UTI,
the indications for sending a urine specimen to the microbiology laboratory and on the
interpretation of culture results. Where residents are incontinent and disoriented, typical signs and
symptoms of recurrent UTI may be more difficult to elicit. Therefore, one might expect that it would
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Discussion 72
be more difficult to justify the use of prophylaxis in such patients, particularly where diagnostic
uncertainty is commonplace (34)
LTCF staff education regarding the differences between asymptomatic bacteriuria and symptomatic
UTI is required. The presence of a positive urinary culture in the absence of urinary tract-specific
signs and symptoms may not equate to a UTI. It is possible that residents may have been mistakenly
labelled as suffering from recurrent UTIs, solely on the basis of repeated positive urine culture
results.
The HALT survey did not capture data regarding the duration of antimicrobial prescriptions.
However, it is recommended that a trial of urinary tract prophylaxis should not exceed six months.
The decision to prescribe prophylaxis should not be taken lightly and the resident must be fully
informed of the potential risks associated with antimicrobial exposure, particularly their increased
susceptibility to Clostridium difficile infection.
It is also important that any resident for whom nitrofurantoin is being prescribed for a prolonged
period is counselled about the potential serious complications of hepatic and pulmonary toxicity.
(37) In France, following a national drug monitoring alert issued in 2011, based on a frequency of
one case of severe hepatic or pulmonary toxicity per 7,666 nitrofurantoin prescriptions >1 month
duration, the French Agency for the Safety of Medicine and Health Products published guidelines
which recommended that nitrofurantoin must not be used for UTI prophylaxis. (38)
Those who prescribe and dispense antimicrobials must understand that when an antimicrobial is
prescribed for long-term prophylaxis, that agent may be lost as a future potential therapeutic agent,
owing to the development of AMR. The emergence and dissemination of ESBL-producing
Enterobacteriaceae in LTCF is a cause for concern. Nitrofurantoin is one of the very limited oral
antimicrobial options for treating uncomplicated UTI due to ESBL-producing E. coli and the loss of
this agent via uncontrolled prophylaxis further diminishes therapeutic options. Finally, indiscriminate
and prolonged courses of antimicrobial prophylaxis are costly both in economic terms and in
valuable nursing time, with regard to daily dispensing and administration.
There is evidence that the repeated HALT surveys and publication of the UTI guideline for LTCF have
had a positive impact on reducing prophylactic prescribing in Ireland. The overall prevalence
decreased from 4.3% to 3.8% between 2010 and 2013, but increased back to 4.3% in 2016. The UTI
prophylaxis prevalence decreased from 3.8% to 2.8% between 2010 and 2013, remaining stable at
2.9% in 2016. The fact that 43% of LTCF were first-time participants in HALT may have contributed to
the 2016 findings.
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Discussion 73
Older age, immunocompromise and antimicrobial exposure are major risk factors for CDI. In HALT
2016, seven residents with CDI were reported, of whom four were deemed to have hospital-
acquired CDI. National guidelines for the surveillance, diagnosis and management of CDI were
updated in 2014 and it is recommended that they are also implemented by all Irish LTCF. (39)
Prospective surveillance and feedback of antimicrobial consumption is a key component of any
antimicrobial stewardship programme and it is recommended that this is advanced in each LTCF.
(40) Consumption surveillance could be reported for the overall LTCF, broken down further for
individual units/wards within the LTCF or for individual prescribers. Where the LTCF receives the
supply of prescription medication from an acute hospital pharmacy or a community pharmacy, a
summary report of antimicrobial consumption and expenditure by that LTCF should be requested on
a periodic basis (i.e., quarterly or biannually) by mutual agreement between the LTCF and pharmacy
management. The findings of each report should be formally discussed locally, fed back to medical
and nursing staff and trends monitored over time. With new developments in information
technology being utilised in general practice, GPs may also be able to obtain electronic summary
reports of their individual antimicrobial prescribing practices. The ability to further stratify
prescribing by patient/resident location and by indication should be sought. It is recommended that
the future provision of prescriber-level feedback to GPs on antimicrobial use be explored via existing
mechanisms, such as the Irish Primary Care Research Network.
As most GPs are self-employed and based within the community, it is important that they have easy
access to ongoing educational activities on HCAI prevention and management, AMR and
antimicrobial stewardship and that such educational activities are linked to continuing professional
development (CPD) credits, as part of the annual requirements of clinical professional competence
schemes. Educational materials should be available via a variety of routes, including e-learning,
publications and face-to-face educational workshops. The development of specific educational
‘toolkits’ for HCAI prevention and antimicrobial prescribing for use by trainee GPs and GPs should be
progressed, in conjunction with the ICGP.
LTCF residents and their families, friends and carers have an important role to play in the prevention
of HCAI and AMR in LTCF. Residents and their visitors should receive practical education on the
importance of social hand hygiene and be provided with easy access to hand hygiene products. It is
also recommended that educational materials, including information leaflets and access to on-line
resources be developed specifically for use by LTCF residents and their families, friends and carers,
with input from patient representative organisations. Information leaflets on hand hygiene,
influenza vaccination, prudent use of antibiotics and antibiotic resistant bacteria, such as MRSA,

PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Discussion 74
ESBLs, CRE and VRE should be developed for LTCF and displayed prominently within each LTCF. The
local HALT survey results and quality improvement plans within each LTCF should also be shared
with residents and their families.
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
References 75
6. References
1. Cotter M, Donlon S, Roche F, Byrne H, Fitzpatrick F. Healthcare-associated infection in Irish long-term care facilities: results f rom the First National Prevalence Study. J Hosp Infect 2012 Mar; 80(3):212-6.
2. Health Protection Surveillance Centre. European point prevalence survey on healthcare-associated infections and antibiotic use in long-term care facilities (HALT) National Report 2010 - Republic of Ireland. 2010 Nov 1. http://www.hpsc.ie/A-Z/MicrobiologyAntimicrobialResistance/InfectionControlandHAI/Surveillance/HCAIinlongtermcarefacilities/HALTReports/2010Report/
3. Suetens C. Healthcare-associated infections in European long-term care facilities: how big is the challenge? Euro Surveill 2012; 17(35).
4. Health Protection Surveillance Centre. Second national prevalence survey on healthcare-associated infections and antibiotic use in long-term care facilities (HALT) national report 2011 - Republic of Ireland. 2011 Aug 1. http://www.hpsc.ie/A-Z/MicrobiologyAntimicrobialResistance/InfectionControlandHAI/Surveillance/HCAIinlongtermcarefacilities/HALTReports/2011Report/
5. Health Protection Surveillance Centre. Point prevalence survey of healthcare associated infections and antimicrobial use in long-term care facilities (HALT): May 2013 – Republic of Ireland National Report: March 2014. http://www.hpsc.ie/A-Z/MicrobiologyAntimicrobialResistance/InfectionControlandHAI/Surveillance/HCAIinlongtermcarefacilities/HALTReports/2013Report/
6. European Centre for Disease Prevention & Control (ECDC). Point Prevalence Survey of Healthcare Associated Infections and Antimicrobial Use in European Long-term Care Facilities April – May 2013. http://ecdc.europa.eu/en/publications/publications/healthcare-associated-infections-point-prevalence-survey-long-term-care-facilities-2013.pdf
7. McGeer A, Campbell B, Emori TG, et al. Definitions of infection for surveillance in long-term care facilities. Am J Infect Control 1991 Feb; 19(1):1-7.
8. Stone ND, Ashraf MS, Calder J, et al. Surveillance definitions of infections in long-term care facilities: revisiting the McGeer criteria. Infect Control Hosp Epidemiol 2012 Oct; 33(10):965-77.
9. Health Protection Surveillance Centre. Influenza surveillance in Ireland - Weekly Report. 2016 May 2nd – May 15th (Weeks 18 & 19). http://www.hpsc.ie/A-Z/Respiratory/Influenza/SeasonalInfluenza/Surveillance/InfluenzaSurveillanceReports/PreviousInfluenzaSeasonsSurveillanceReports/20152016Season/File,15680,en.pdf
10. Health Information and Quality Authority. National Quality Standards for Residential Care Settings for Older People in Ireland (2009). https://www.hiqa.ie/reports-and-publications/standards/previous-national-quality-standards-residential-care-settings
11. Health Information and Quality Authority. National Quality Standards for Residential Care Settings for Older People in Ireland (2016). https://www.hiqa.ie/reports-and-publications/standards/current-national-standards-residential-care-settings-older
12. Health Information and Quality Authority. National Standards for the Prevention and Control of Healthcare Associated Infections (2009). https://www.hiqa.ie/reports-and-publications/standards/national-standards-prevention-and-control-healthcare-associated
13. Minster for Health I. Health Act 2007 (Care and welfare of residents in designated centres for older people) regulations S.I. No. 415 of 2013. 2013.
14. Mental Health Commission. Quality Framework Mental Health Services in Ireland (2007). http://www.mhcirl.ie/File/qframemhc.pdf
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
References 76
15. Health Information and Quality Authority. National Standards for Residential Services for Children and Adults with Disabilities (2013). https://www.hiqa.ie/reports-and-publications/standards/national-standards-residential-services-children-and-adults
16. Health Canada NaOIS. Development of a resource model for infection prevention and control programs in acute, long term, and home care settings: Conference proceedings of the Infection Prevention and Control Alliance. Am J Infect Control 2004 Feb 1; 32(2):2-6.
17. Royal College of Nursing. The role of the link nurse in infection prevention and control: developing a link nurse framework. 2012 Oct 18.
18. Health Protection Surveillance Centre. Point Prevalence Survey of Hospital Acquired Infections & Antimicrobial Use in European Acute Care Hospitals: May 2012 - Republic of Ireland National Report. http://www.hpsc.ie/A-Z/MicrobiologyAntimicrobialResistance/InfectionControlandHAI/Surveillance/HospitalPointPrevalenceSurveys/2012/PPS2012ReportsforIreland/
19. Patel G, Huprikar S, Factor SH, Jenkins SG, Calfee DP. Outcomes of carbapenem-resistant Klebsiella pneumoniae infection and the impact of antimicrobial and adjunctive therapies. Infect Control Hosp Epidemiol 2008 Dec; 29(12):1099-106.
20. Dhanji H, Doumith M, Rooney PJ, et al. Molecular epidemiology of fluoroquinolone-resistant ST131 Escherichia coli producing CTX-M extended-spectrum beta-lactamases in nursing homes in Belfast, UK. J Antimicrob Chemother 2011 Feb; 66(2):297-303.
21. Fennell J, Vellinga A, Hanahoe B, et al. Increasing prevalence of ESBL production among Irish clinical Enterobacteriaceae from 2004 to 2008: an observational study. BMC Infect Dis 2012; 12:116.
22. Pelly H, Morris D, O'Connell E, et al. Outbreak of extended spectrum beta-lactamase producing E. coli in a nursing home in Ireland, May 2006. Euro Surveill 2006; 11(8):E060831.
23. Flannery B, Chung JR, Thaker SN et al. Interim estimates of 2016-17 seasonal influenza vaccine effectiveness - United States, February 2017. Morb Mortal Wkly Rep 2017;66(6):167-171
24. Griffin MR. Influenza vaccination of healthcare workers: making the grade for action. Clin Infect Dis 2014 Jan; 58(1):58-60.
25. Public Health Medicine Communicable Disease Group. Public Health Guidelines on the Prevention and Management of Influenza Outbreaks in Residential Care Facilities in Ireland: 2016/2017. http://www.hpsc.ie/A-Z/Respiratory/Influenza/SeasonalInfluenza/Guidance/ResidentialCareFacilitiesGuidance/File,13195,en.pdf
26. Health Protection Surveillance Centre. Uptake of the Seasonal Influenza Vaccine in Acute Hospitals and Long-term Care Facilities in Ireland in 2015-2016 http://www.hpsc.ie/A-Z/Respiratory/Influenza/SeasonalInfluenza/InfluenzaandHealthcareWorkers/HCWInfluenzaVaccineUptakeReports/File,15542,en.pdf
27. Mazick A, Gergonne B, Nielsen J, et al. Excess mortality among the elderly in 12 European countries, February and March 2012. Euro Surveill 2012; 17(14).
28. Mertz D, Kim TH, Johnstone J, et al. Populations at risk for severe or complicated influenza illness: systematic review and meta-analysis. BMJ 2013; 347:f5061.
29. Nielsen J, Mazick A, Andrews N, et al. Pooling European all-cause mortality: methodology and findings for the seasons 2008/2009 to 2010/2011. Epidemiol Infect 2013 Sep; 141(9):1996-2010.
30. Health Protection Surveillance Centre. Annual Report of the Health Protection Surveillance Centre 2015. http://www.hpsc.ie/AboutHPSC/AnnualReports/
31. National Immunisation Advisory Committee. Immunisation Guidelines for Ireland - Chapter 11 - Influenza. (Updated September 2016) http://www.hse.ie/eng/health/immunisation/hcpinfo/guidelines/chapter11.pdf
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
References 77
32. Ahmed F, Lindley MC, Allred N, Weinbaum CM, Grohskopf L. Effect of influenza vaccination of healthcare personnel on morbidity and mortality among patients: systematic review and grading of evidence. Clin Infect Dis 2014 Jan; 58(1):50-7.
33. Health Protection Surveillance Centre. Guidelines for the Prevention of Catheter-Associated Urinary Tract Infection (2011). http://www.hpsc.ie/A-Z/MicrobiologyAntimicrobialResistance/InfectionControlandHAI/UrinaryCatheters/Publications/
34. Strategy for the Control of Antimicrobial Resistance in Ireland Working Group. Diagnosis and management of urinary tract infection in long-term care residents aged over 65 years (2011). http://www.hpsc.ie/A-Z/MicrobiologyAntimicrobialResistance/InfectionControlandHAI/Guidelines/File,12929,en.pdf
35. Mody L, Juthani-Mehta M. Urinary Tract Infections in Older Women. Journal of the American Medical Association 2014 Feb 26; 311(8):844-54.
36. Enzler MJ, Berbari E, Osmon DR. Antimicrobial prophylaxis in adults. Mayo Clin Proc 2011 Jul; 86(7):686-701.
37. Marshall AD, Dempsey OJ. Is "nitrofurantoin lung"on the increase? BMJ 2013; 346:f3897. 38. Slekovec C, Leroy J, Huttner A, et al. When the precautionary principle disrupts 3 years of
antibiotic stewardship: nitrofurantoin in the treatment of urinary tract infections. J Antimicrob Chemother 2014 Jan; 69(1):282-4.
39. National Clinical Effectiveness Committee. Surveillance, diagnosis and management of C. difficile infection in Ireland (2014) http://www.hpsc.ie/A-Z/MicrobiologyAntimicrobialResistance/InfectionControlandHAI/Guidelines/File,13950,en.pdf
40. Strategy for the Control of Antimicrobial Resistance in Ireland Working Group. Guidelines for Antimicrobial Stewardship in Hospitals in Ireland (2009) http://www.hpsc.ie/A-Z/MicrobiologyAntimicrobialResistance/InfectionControlandHAI/Guidelines/File,4116,en.pdf
41. Mental Health Commission Annual Report (2015) http://www.mhcirl.ie/Publications/Annual_Reports/
42. RCPI & HSE Clinical Advisory Group on HCAI & AMR. Guidelines for prevention and control of multi-drug resistant organisms, excluding MRSA in the healthcare setting (2013). http://www.hpsc.ie/A-Z/MicrobiologyAntimicrobialResistance/InfectionControlandHAI/Guidelines/File,12922,en.pdf
43. National Clinical Effectiveness Committee. Prevention and Control Methicillin Resistant Staphylococcus aureus (MRSA) (2013). http://www.hpsc.ie/A-Z/MicrobiologyAntimicrobialResistance/InfectionControlandHAI/Guidelines/File,14478,en.pdf
44. Thomas RE, Jefferson T, Lasserson TJ. Influenza vaccine for healthcare workers who care for people aged 60 or older living in long-term care institutions. Cochrane Database of Systematic Reviews 2016, Issue 6. Art. No. CD005187.
45. Health Research Board; Doyle A, Carew AM. Annual Report of the National Intellectual Disability Database Committee 2015 www.hrb.ie/publications
46. World Health Organisation (WHO) Guidelines on Hand Hygiene in Healthcare http://www.who.int/gpsc/5may/tools/9789241597906/en/
47. HPSC. National Hand Hygiene Compliance Results. See weblink below for latest available data: http://www.hpsc.ie/A-Z/MicrobiologyAntimicrobialResistance/EuropeanSurveillanceofAntimicrobialConsumptionESAC/PublicMicroB/HHA/Report1.html
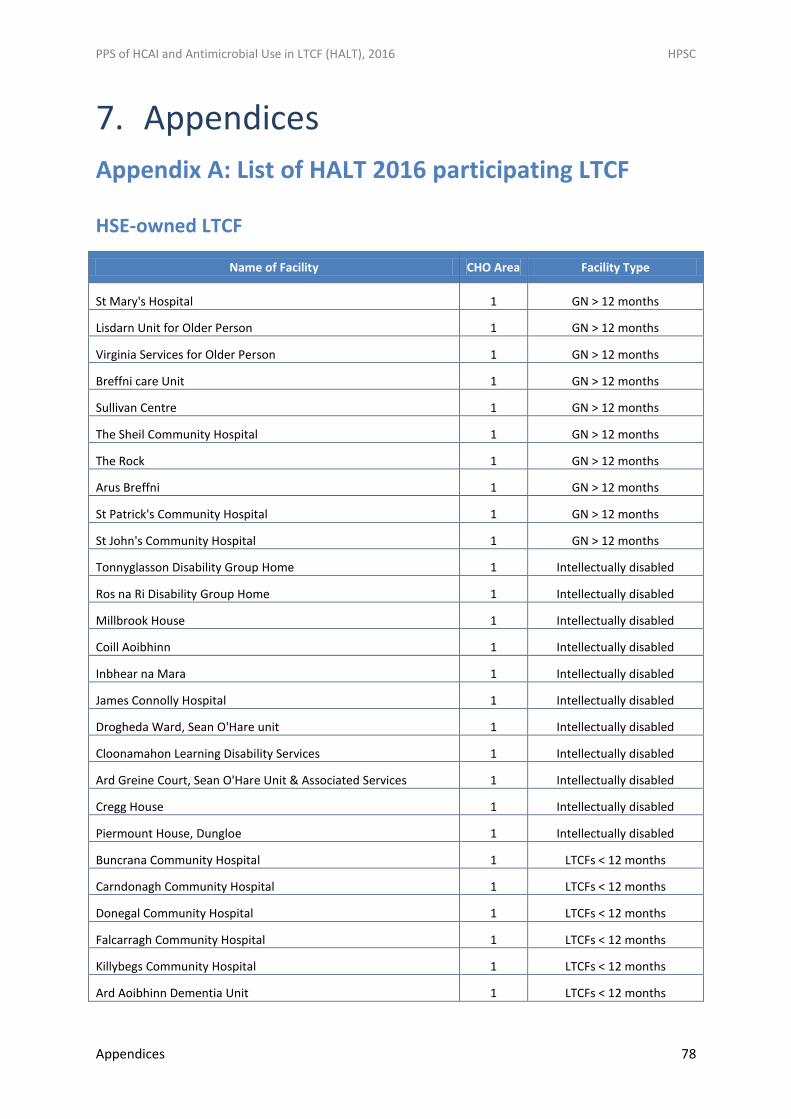
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Appendices 78
7. Appendices
Appendix A: List of HALT 2016 participating LTCF
HSE-owned LTCF
Name of Facility CHO Area Facility Type
St Mary's Hospital 1 GN > 12 months
Lisdarn Unit for Older Person 1 GN > 12 months
Virginia Services for Older Person 1 GN > 12 months
Breffni care Unit 1 GN > 12 months
Sullivan Centre 1 GN > 12 months
The Sheil Community Hospital 1 GN > 12 months
The Rock 1 GN > 12 months
Arus Breffni 1 GN > 12 months
St Patrick's Community Hospital 1 GN > 12 months
St John's Community Hospital 1 GN > 12 months
Tonnyglasson Disability Group Home 1 Intellectually disabled
Ros na Ri Disability Group Home 1 Intellectually disabled
Millbrook House 1 Intellectually disabled
Coill Aoibhinn 1 Intellectually disabled
Inbhear na Mara 1 Intellectually disabled
James Connolly Hospital 1 Intellectually disabled
Drogheda Ward, Sean O'Hare unit 1 Intellectually disabled
Cloonamahon Learning Disability Services 1 Intellectually disabled
Ard Greine Court, Sean O'Hare Unit & Associated Services 1 Intellectually disabled
Cregg House 1 Intellectually disabled
Piermount House, Dungloe 1 Intellectually disabled
Buncrana Community Hospital 1 LTCFs < 12 months
Carndonagh Community Hospital 1 LTCFs < 12 months
Donegal Community Hospital 1 LTCFs < 12 months
Falcarragh Community Hospital 1 LTCFs < 12 months
Killybegs Community Hospital 1 LTCFs < 12 months
Ard Aoibhinn Dementia Unit 1 LTCFs < 12 months
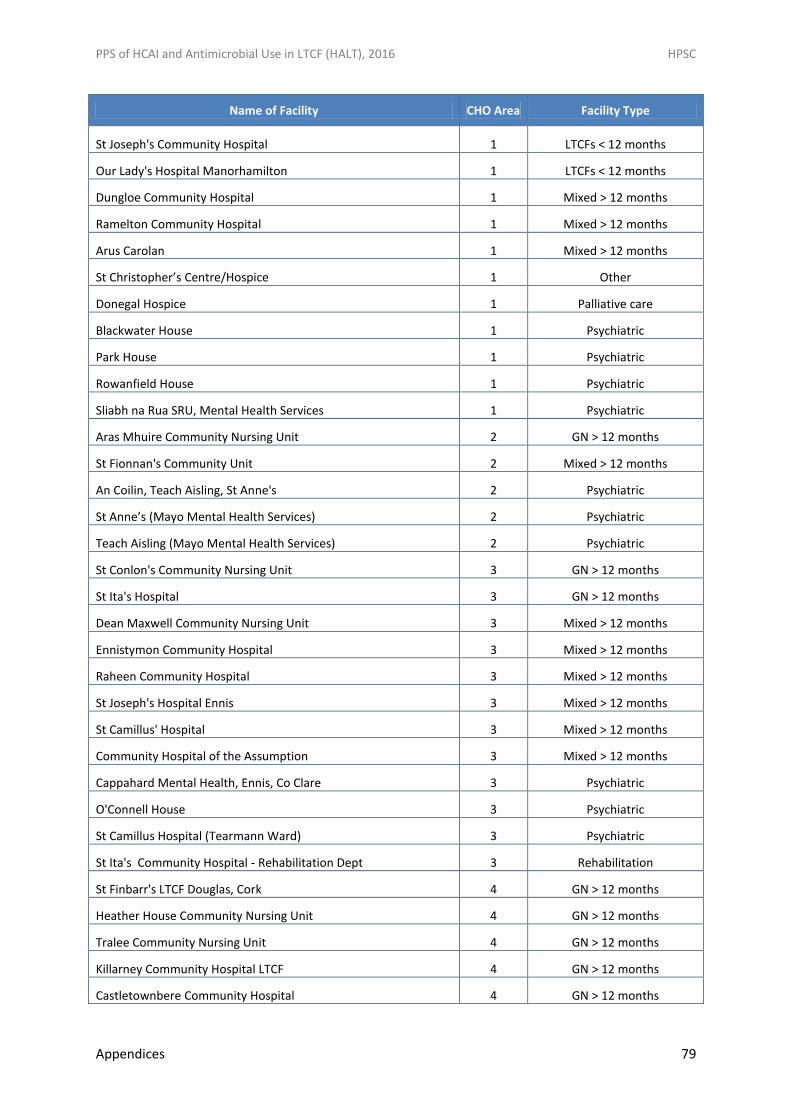
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Appendices 79
Name of Facility CHO Area Facility Type
St Joseph's Community Hospital 1 LTCFs < 12 months
Our Lady's Hospital Manorhamilton 1 LTCFs < 12 months
Dungloe Community Hospital 1 Mixed > 12 months
Ramelton Community Hospital 1 Mixed > 12 months
Arus Carolan 1 Mixed > 12 months
St Christopher’s Centre/Hospice 1 Other
Donegal Hospice 1 Palliative care
Blackwater House 1 Psychiatric
Park House 1 Psychiatric
Rowanfield House 1 Psychiatric
Sliabh na Rua SRU, Mental Health Services 1 Psychiatric
Aras Mhuire Community Nursing Unit 2 GN > 12 months
St Fionnan's Community Unit 2 Mixed > 12 months
An Coilin, Teach Aisling, St Anne's 2 Psychiatric
St Anne’s (Mayo Mental Health Services) 2 Psychiatric
Teach Aisling (Mayo Mental Health Services) 2 Psychiatric
St Conlon's Community Nursing Unit 3 GN > 12 months
St Ita's Hospital 3 GN > 12 months
Dean Maxwell Community Nursing Unit 3 Mixed > 12 months
Ennistymon Community Hospital 3 Mixed > 12 months
Raheen Community Hospital 3 Mixed > 12 months
St Joseph's Hospital Ennis 3 Mixed > 12 months
St Camillus' Hospital 3 Mixed > 12 months
Community Hospital of the Assumption 3 Mixed > 12 months
Cappahard Mental Health, Ennis, Co Clare 3 Psychiatric
O'Connell House 3 Psychiatric
St Camillus Hospital (Tearmann Ward) 3 Psychiatric
St Ita's Community Hospital - Rehabilitation Dept 3 Rehabilitation
St Finbarr's LTCF Douglas, Cork 4 GN > 12 months
Heather House Community Nursing Unit 4 GN > 12 months
Tralee Community Nursing Unit 4 GN > 12 months
Killarney Community Hospital LTCF 4 GN > 12 months
Castletownbere Community Hospital 4 GN > 12 months
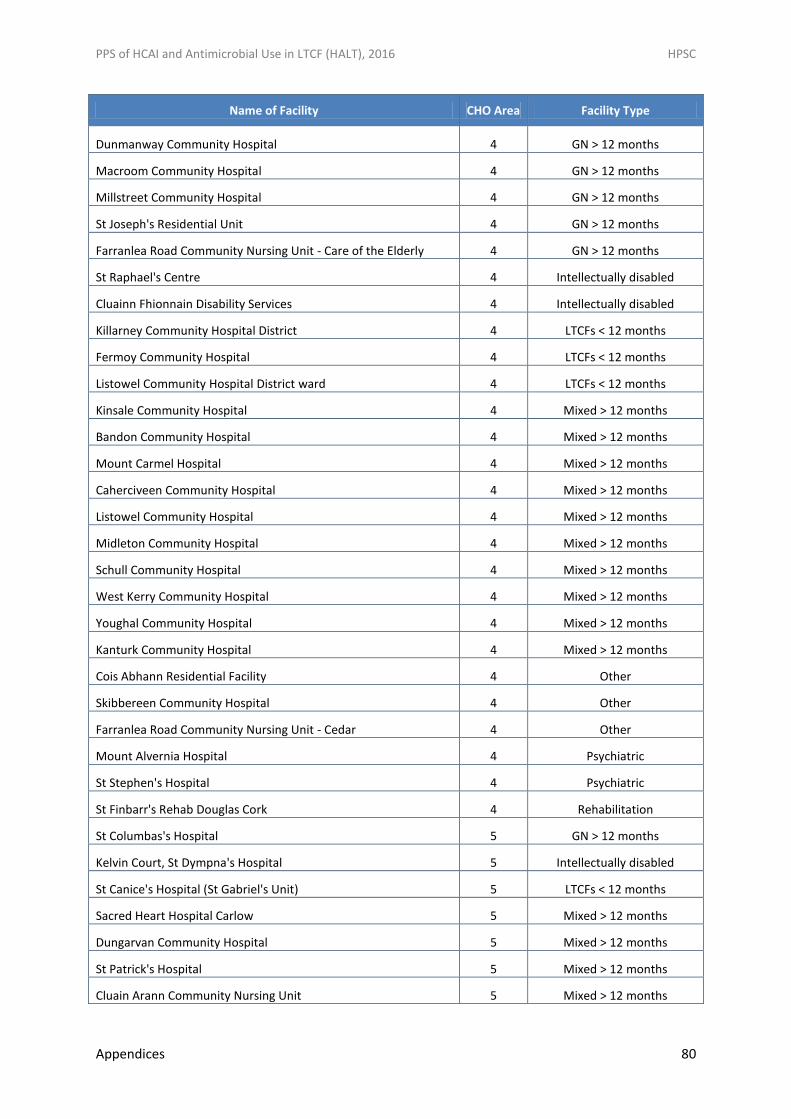
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Appendices 80
Name of Facility CHO Area Facility Type
Dunmanway Community Hospital 4 GN > 12 months
Macroom Community Hospital 4 GN > 12 months
Millstreet Community Hospital 4 GN > 12 months
St Joseph's Residential Unit 4 GN > 12 months
Farranlea Road Community Nursing Unit - Care of the Elderly 4 GN > 12 months
St Raphael's Centre 4 Intellectually disabled
Cluainn Fhionnain Disability Services 4 Intellectually disabled
Killarney Community Hospital District 4 LTCFs < 12 months
Fermoy Community Hospital 4 LTCFs < 12 months
Listowel Community Hospital District ward 4 LTCFs < 12 months
Kinsale Community Hospital 4 Mixed > 12 months
Bandon Community Hospital 4 Mixed > 12 months
Mount Carmel Hospital 4 Mixed > 12 months
Caherciveen Community Hospital 4 Mixed > 12 months
Listowel Community Hospital 4 Mixed > 12 months
Midleton Community Hospital 4 Mixed > 12 months
Schull Community Hospital 4 Mixed > 12 months
West Kerry Community Hospital 4 Mixed > 12 months
Youghal Community Hospital 4 Mixed > 12 months
Kanturk Community Hospital 4 Mixed > 12 months
Cois Abhann Residential Facility 4 Other
Skibbereen Community Hospital 4 Other
Farranlea Road Community Nursing Unit - Cedar 4 Other
Mount Alvernia Hospital 4 Psychiatric
St Stephen's Hospital 4 Psychiatric
St Finbarr's Rehab Douglas Cork 4 Rehabilitation
St Columbas's Hospital 5 GN > 12 months
Kelvin Court, St Dympna's Hospital 5 Intellectually disabled
St Canice's Hospital (St Gabriel's Unit) 5 LTCFs < 12 months
Sacred Heart Hospital Carlow 5 Mixed > 12 months
Dungarvan Community Hospital 5 Mixed > 12 months
St Patrick's Hospital 5 Mixed > 12 months
Cluain Arann Community Nursing Unit 5 Mixed > 12 months
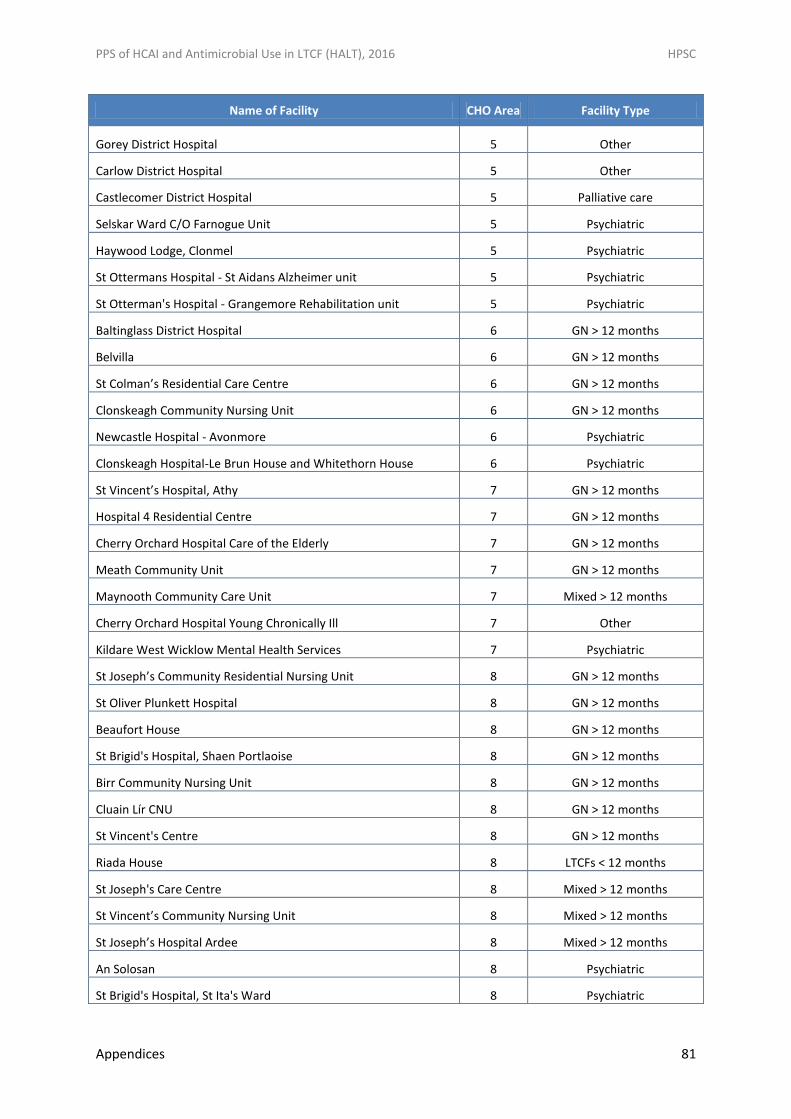
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Appendices 81
Name of Facility CHO Area Facility Type
Gorey District Hospital 5 Other
Carlow District Hospital 5 Other
Castlecomer District Hospital 5 Palliative care
Selskar Ward C/O Farnogue Unit 5 Psychiatric
Haywood Lodge, Clonmel 5 Psychiatric
St Ottermans Hospital - St Aidans Alzheimer unit 5 Psychiatric
St Otterman's Hospital - Grangemore Rehabilitation unit 5 Psychiatric
Baltinglass District Hospital 6 GN > 12 months
Belvilla 6 GN > 12 months
St Colman’s Residential Care Centre 6 GN > 12 months
Clonskeagh Community Nursing Unit 6 GN > 12 months
Newcastle Hospital - Avonmore 6 Psychiatric
Clonskeagh Hospital-Le Brun House and Whitethorn House 6 Psychiatric
St Vincent’s Hospital, Athy 7 GN > 12 months
Hospital 4 Residential Centre 7 GN > 12 months
Cherry Orchard Hospital Care of the Elderly 7 GN > 12 months
Meath Community Unit 7 GN > 12 months
Maynooth Community Care Unit 7 Mixed > 12 months
Cherry Orchard Hospital Young Chronically Ill 7 Other
Kildare West Wicklow Mental Health Services 7 Psychiatric
St Joseph’s Community Residential Nursing Unit 8 GN > 12 months
St Oliver Plunkett Hospital 8 GN > 12 months
Beaufort House 8 GN > 12 months
St Brigid's Hospital, Shaen Portlaoise 8 GN > 12 months
Birr Community Nursing Unit 8 GN > 12 months
Cluain Lír CNU 8 GN > 12 months
St Vincent's Centre 8 GN > 12 months
Riada House 8 LTCFs < 12 months
St Joseph's Care Centre 8 Mixed > 12 months
St Vincent’s Community Nursing Unit 8 Mixed > 12 months
St Joseph’s Hospital Ardee 8 Mixed > 12 months
An Solosan 8 Psychiatric
St Brigid's Hospital, St Ita's Ward 8 Psychiatric
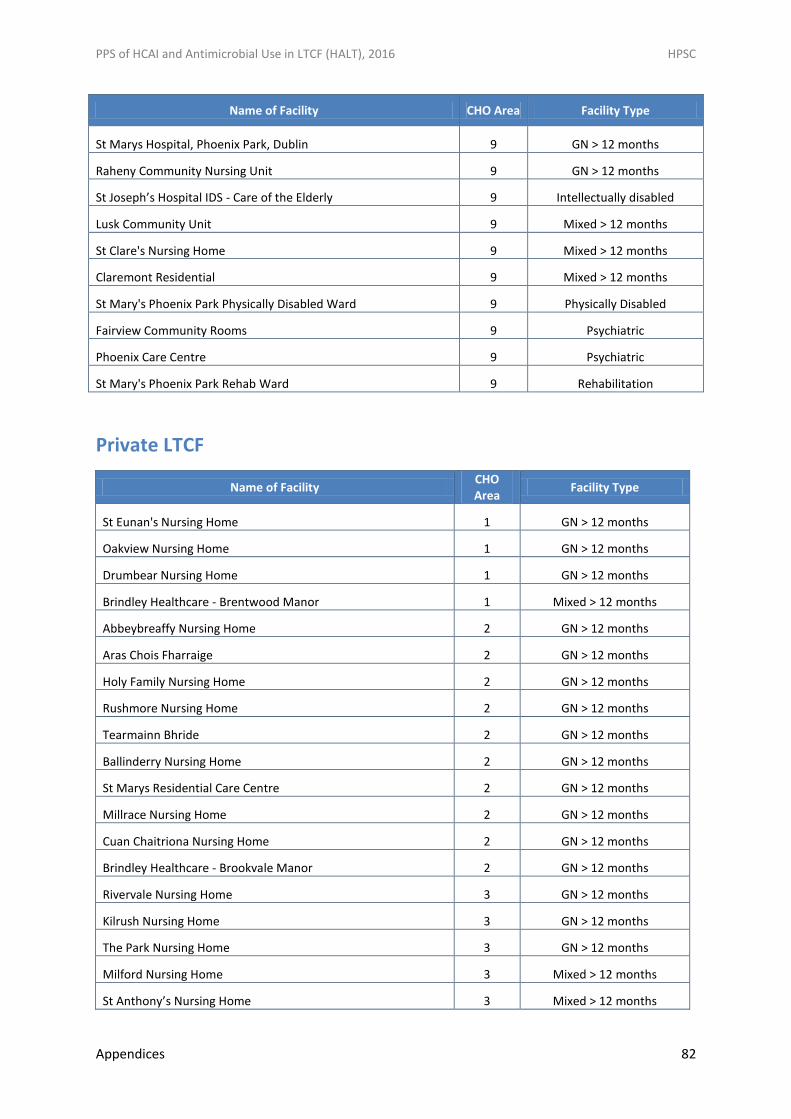
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Appendices 82
Name of Facility CHO Area Facility Type
St Marys Hospital, Phoenix Park, Dublin 9 GN > 12 months
Raheny Community Nursing Unit 9 GN > 12 months
St Joseph’s Hospital IDS - Care of the Elderly 9 Intellectually disabled
Lusk Community Unit 9 Mixed > 12 months
St Clare's Nursing Home 9 Mixed > 12 months
Claremont Residential 9 Mixed > 12 months
St Mary's Phoenix Park Physically Disabled Ward 9 Physically Disabled
Fairview Community Rooms 9 Psychiatric
Phoenix Care Centre 9 Psychiatric
St Mary's Phoenix Park Rehab Ward 9 Rehabilitation
Private LTCF
Name of Facility CHO Area
Facility Type
St Eunan's Nursing Home 1 GN > 12 months
Oakview Nursing Home 1 GN > 12 months
Drumbear Nursing Home 1 GN > 12 months
Brindley Healthcare - Brentwood Manor 1 Mixed > 12 months
Abbeybreaffy Nursing Home 2 GN > 12 months
Aras Chois Fharraige 2 GN > 12 months
Holy Family Nursing Home 2 GN > 12 months
Rushmore Nursing Home 2 GN > 12 months
Tearmainn Bhride 2 GN > 12 months
Ballinderry Nursing Home 2 GN > 12 months
St Marys Residential Care Centre 2 GN > 12 months
Millrace Nursing Home 2 GN > 12 months
Cuan Chaitriona Nursing Home 2 GN > 12 months
Brindley Healthcare - Brookvale Manor 2 GN > 12 months
Rivervale Nursing Home 3 GN > 12 months
Kilrush Nursing Home 3 GN > 12 months
The Park Nursing Home 3 GN > 12 months
Milford Nursing Home 3 Mixed > 12 months
St Anthony’s Nursing Home 3 Mixed > 12 months
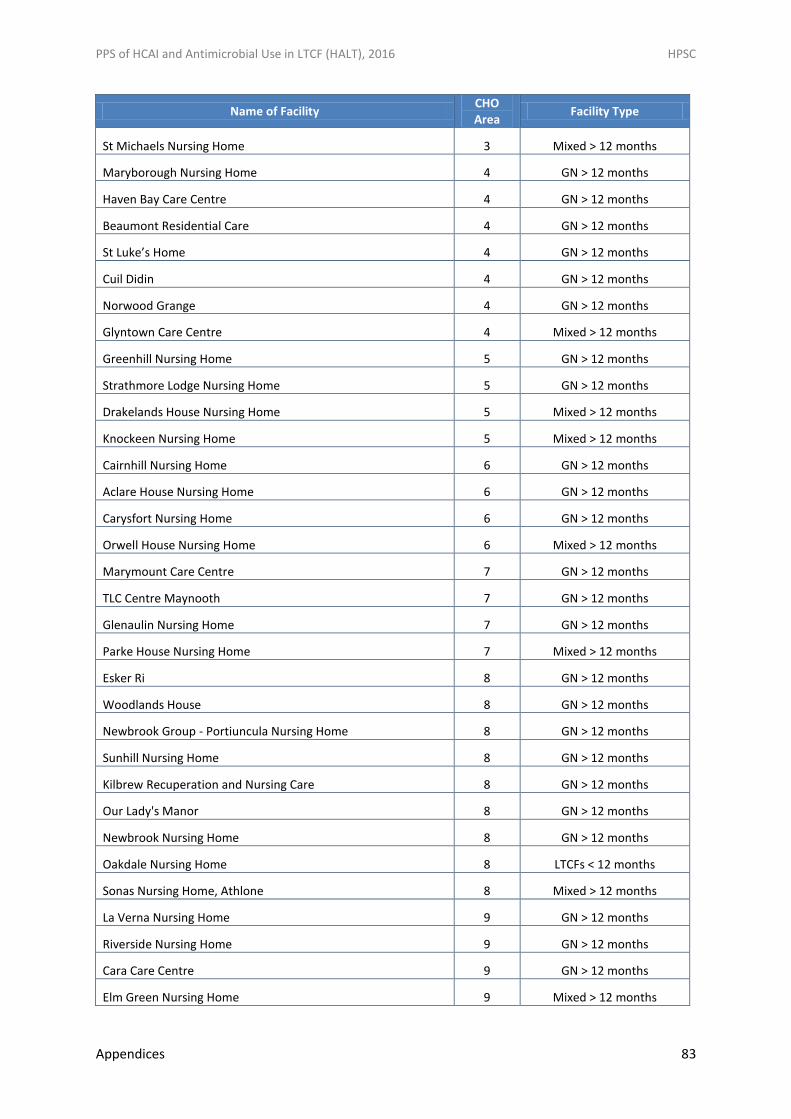
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Appendices 83
Name of Facility CHO Area
Facility Type
St Michaels Nursing Home 3 Mixed > 12 months
Maryborough Nursing Home 4 GN > 12 months
Haven Bay Care Centre 4 GN > 12 months
Beaumont Residential Care 4 GN > 12 months
St Luke’s Home 4 GN > 12 months
Cuil Didin 4 GN > 12 months
Norwood Grange 4 GN > 12 months
Glyntown Care Centre 4 Mixed > 12 months
Greenhill Nursing Home 5 GN > 12 months
Strathmore Lodge Nursing Home 5 GN > 12 months
Drakelands House Nursing Home 5 Mixed > 12 months
Knockeen Nursing Home 5 Mixed > 12 months
Cairnhill Nursing Home 6 GN > 12 months
Aclare House Nursing Home 6 GN > 12 months
Carysfort Nursing Home 6 GN > 12 months
Orwell House Nursing Home 6 Mixed > 12 months
Marymount Care Centre 7 GN > 12 months
TLC Centre Maynooth 7 GN > 12 months
Glenaulin Nursing Home 7 GN > 12 months
Parke House Nursing Home 7 Mixed > 12 months
Esker Ri 8 GN > 12 months
Woodlands House 8 GN > 12 months
Newbrook Group - Portiuncula Nursing Home 8 GN > 12 months
Sunhill Nursing Home 8 GN > 12 months
Kilbrew Recuperation and Nursing Care 8 GN > 12 months
Our Lady's Manor 8 GN > 12 months
Newbrook Nursing Home 8 GN > 12 months
Oakdale Nursing Home 8 LTCFs < 12 months
Sonas Nursing Home, Athlone 8 Mixed > 12 months
La Verna Nursing Home 9 GN > 12 months
Riverside Nursing Home 9 GN > 12 months
Cara Care Centre 9 GN > 12 months
Elm Green Nursing Home 9 Mixed > 12 months
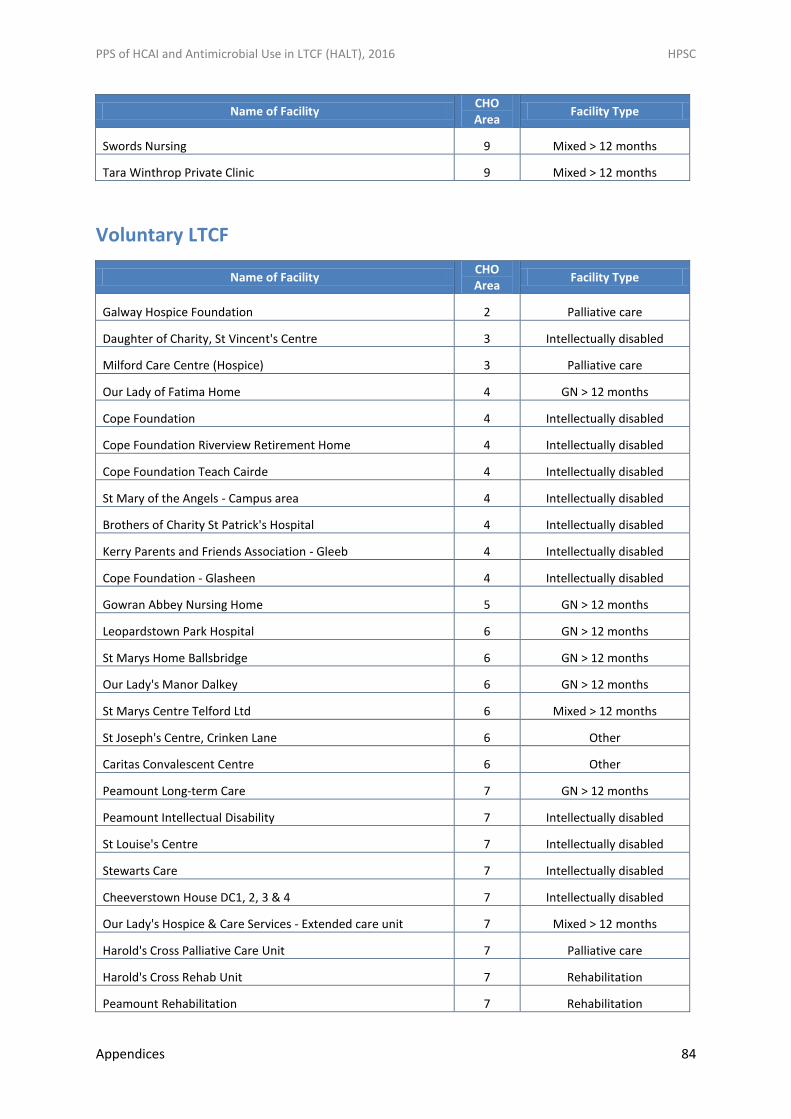
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Appendices 84
Name of Facility CHO Area
Facility Type
Swords Nursing 9 Mixed > 12 months
Tara Winthrop Private Clinic 9 Mixed > 12 months
Voluntary LTCF
Name of Facility CHO Area
Facility Type
Galway Hospice Foundation 2 Palliative care
Daughter of Charity, St Vincent's Centre 3 Intellectually disabled
Milford Care Centre (Hospice) 3 Palliative care
Our Lady of Fatima Home 4 GN > 12 months
Cope Foundation 4 Intellectually disabled
Cope Foundation Riverview Retirement Home 4 Intellectually disabled
Cope Foundation Teach Cairde 4 Intellectually disabled
St Mary of the Angels - Campus area 4 Intellectually disabled
Brothers of Charity St Patrick's Hospital 4 Intellectually disabled
Kerry Parents and Friends Association - Gleeb 4 Intellectually disabled
Cope Foundation - Glasheen 4 Intellectually disabled
Gowran Abbey Nursing Home 5 GN > 12 months
Leopardstown Park Hospital 6 GN > 12 months
St Marys Home Ballsbridge 6 GN > 12 months
Our Lady's Manor Dalkey 6 GN > 12 months
St Marys Centre Telford Ltd 6 Mixed > 12 months
St Joseph's Centre, Crinken Lane 6 Other
Caritas Convalescent Centre 6 Other
Peamount Long-term Care 7 GN > 12 months
Peamount Intellectual Disability 7 Intellectually disabled
St Louise's Centre 7 Intellectually disabled
Stewarts Care 7 Intellectually disabled
Cheeverstown House DC1, 2, 3 & 4 7 Intellectually disabled
Our Lady's Hospice & Care Services - Extended care unit 7 Mixed > 12 months
Harold's Cross Palliative Care Unit 7 Palliative care
Harold's Cross Rehab Unit 7 Rehabilitation
Peamount Rehabilitation 7 Rehabilitation
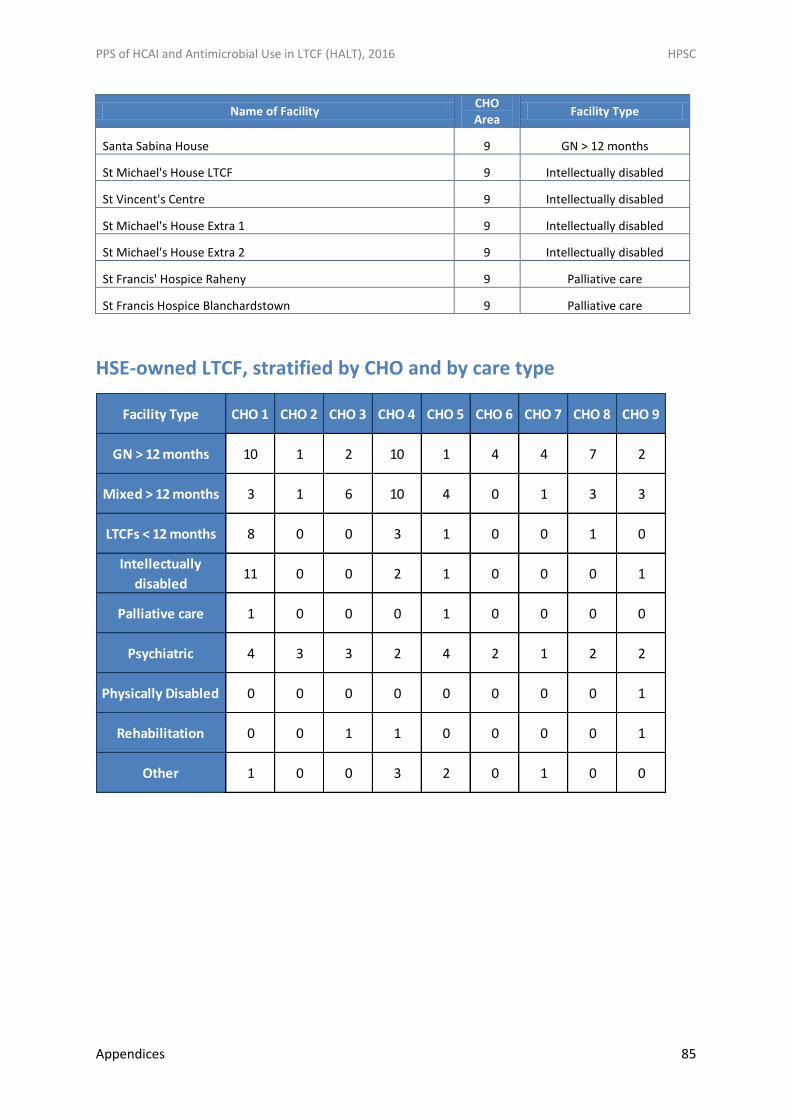
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Appendices 85
Name of Facility CHO Area
Facility Type
Santa Sabina House 9 GN > 12 months
St Michael's House LTCF 9 Intellectually disabled
St Vincent's Centre 9 Intellectually disabled
St Michael's House Extra 1 9 Intellectually disabled
St Michael's House Extra 2 9 Intellectually disabled
St Francis' Hospice Raheny 9 Palliative care
St Francis Hospice Blanchardstown 9 Palliative care
HSE-owned LTCF, stratified by CHO and by care type
Facility Type CHO 1 CHO 2 CHO 3 CHO 4 CHO 5 CHO 6 CHO 7 CHO 8 CHO 9
GN > 12 months 10 1 2 10 1 4 4 7 2
Mixed > 12 months 3 1 6 10 4 0 1 3 3
LTCFs < 12 months 8 0 0 3 1 0 0 1 0
Intellectually
disabled11 0 0 2 1 0 0 0 1
Palliative care 1 0 0 0 1 0 0 0 0
Psychiatric 4 3 3 2 4 2 1 2 2
Physically Disabled 0 0 0 0 0 0 0 0 1
Rehabilitation 0 0 1 1 0 0 0 0 1
Other 1 0 0 3 2 0 1 0 0
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Appendices 86
Appendix B: HALT 2016 National Steering Group Membership
Dr Karen Burns, Consultant Microbiologist, HSE-HPSC & Beaumont Hospital (Chair)
Ms Helen Murphy, Infection Prevention & Control Nurse Manager, HSE-HPSC
Ms Margaret Nadin, Project Manager, HSE NMPDU, Dublin-North East
Ms Mary McKenna, Lead Infection Prevention & Control ADON, HSE HCAI & AMR Clinical
Programme, Quality Improvement Division
Ms Grainne Parker, Communicable Disease Control Nurse, Public Health Department, HSE
South (South East)
Ms Mags Moran, Community Infection Control Nurse Manager, Donegal Community
Services, HSE West
Dr Nuala O’Connor, General Practitioner & ICGP Lead HSE HCAI & AMR Clinical Programme,
Quality Improvement Division
Dr Diarmuid O’Shea, Consultant Geriatrician, St Vincent’s University Hospital & HSE Clinical
Programme for Older People, Clinical Lead
Dr Mimi Fan, Consultant Geriatrician, Mater Hospital, Irish Society for Physicians in Geriatric
Medicine
Ms Fiona McMahon, Project Manager, HSE NMPDU Mid-West/ONMSD
Mr Gerry Clerkin, Head of Quality & Safety, HSE Social Care Division
Ms Linda Moore, Quality, Standards & Compliance Officer, HSE National Mental Health
Division
Ms Lisa Malone, Practice Development Facilitator, Nursing Homes Ireland
Dr Fidelma Fitzpatrick, Consultant Microbiologist, Beaumont Hospital & Senior Lecturer in
Microbiology, RCSI
Dr Fiona Roche, Trinity College Dublin, Bioinformatics Support Research Fellow
Dr Ian Callanan, Group Clinical Audit Facilitator, St Vincent’s Healthcare Group
Dr Akke Vellinga, Senior Lecturer & Epidemiologist, School of Medicine, NUI Galway
Ms Sheila Donlon, ADON Infection Prevention & Control Department, Beaumont Hospital
Mr Sean Egan, Regulatory Lead for Antimicrobial Stewardship, Health Information & Quality
Authority
Ms Meera Tandan, PhD student, NUI Galway
Ms Rita Torrans, Community Pharmacist, Abbey Healthcare, Irish Pharmaceutical Union
Ms Josephine Galway, Director of Nursing, St Columba’s Hospital & Castlecomer District
Hospital, Irish Association of Directors of Nursing & Midwifery
The HALT 2016 Steering Group has been convened under the auspices of the Royal College of
Physicians of Ireland & Health Service Executive Clinical Advisory Group on Healthcare-Associated
Infections & Antimicrobial Resistance
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Appendices 87
Appendix C: Acronyms used in this Report
ABHR Alcohol-Based Hand Rub
AMR Antimicrobial Resistance
ASC Antimicrobial Stewardship Committee
CDC US Centers for Disease Control & Prevention
CDI Clostridium difficile infection
CHO Community Healthcare Organisation
CPD Continuing Professional Development
CRE Carbapenem resistant Enterobacteriaceae
ECDC European Centre for Disease Prevention and Control
ESBL Extended Spectrum Beta Lactamase
FAQ Frequently-Asked Questions
GN>12m General nursing homes with LOS > 12 months
GP General Practitioner
HAI Hospital-acquired Infection
HALT Healthcare-Associated Infections in Long-Term Care Facilities
HCA Healthcare Assistant
HCAI Healthcare-Associated Infection
HIQA Health Information & Quality Authority
HPSC Health Protection Surveillance Centre
HSE Health Service Executive
ICGP Irish College of General Practitioners
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Appendices 88
IPC Infection Prevention & Control
IPCC Infection Prevention & Control Committee
IPCN Infection Prevention & Control Nurse
KPI Key Performance Indicator
LAI Long-Term Care Facility-Acquired Infection
LOS Length-of-Stay
LTCF Long-Term Care Facility/Facilities
LTCF<12m LTCF (either general nursing home or mixed care type) with LOS < 12 months
MDR Multi-drug resistant
MDRKP MDR Klebsiella pneumoniae
MHC Mental Health Commission
Mixed>12m Mixed care facilities with LOS > 12 months
MRSA Meticillin Resistant Staphylococcus aureus
MSSA Meticillin Susceptible Staphylococcus aureus
MDRO Multi-Drug Resistant Organisms
PPE Personal Protective Equipment
PPS Point Prevalence Survey
RCPI Royal College of Physicians of Ireland
RTI Respiratory Tract Infection
SHEA Society for Healthcare Epidemiology of America
SSI Surgical Site Infection
UTI Urinary Tract Infection
VE Vaccine Efficacy
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Appendices 89
VRE Vancomycin Resistant Enterococci
WHO World Health Organisation
WIV-ISP Scientific Institute for Public Health, Brussels, Belgium
WTE Whole Time Equivalent
3GC 3rd Generation Cephalosporins
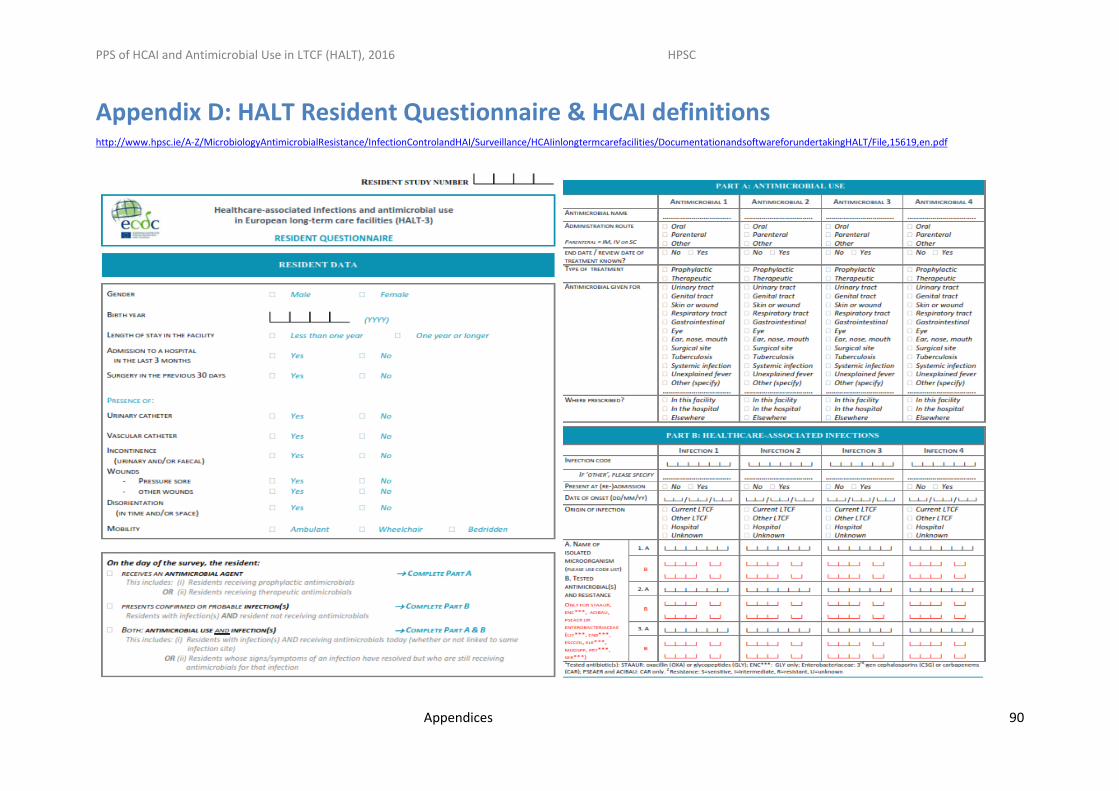
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Appendices 90
Appendix D: HALT Resident Questionnaire & HCAI definitions http://www.hpsc.ie/A-Z/MicrobiologyAntimicrobialResistance/InfectionControlandHAI/Surveillance/HCAIinlongtermcarefacilities/DocumentationandsoftwareforundertakingHALT/File,15619,en.pdf
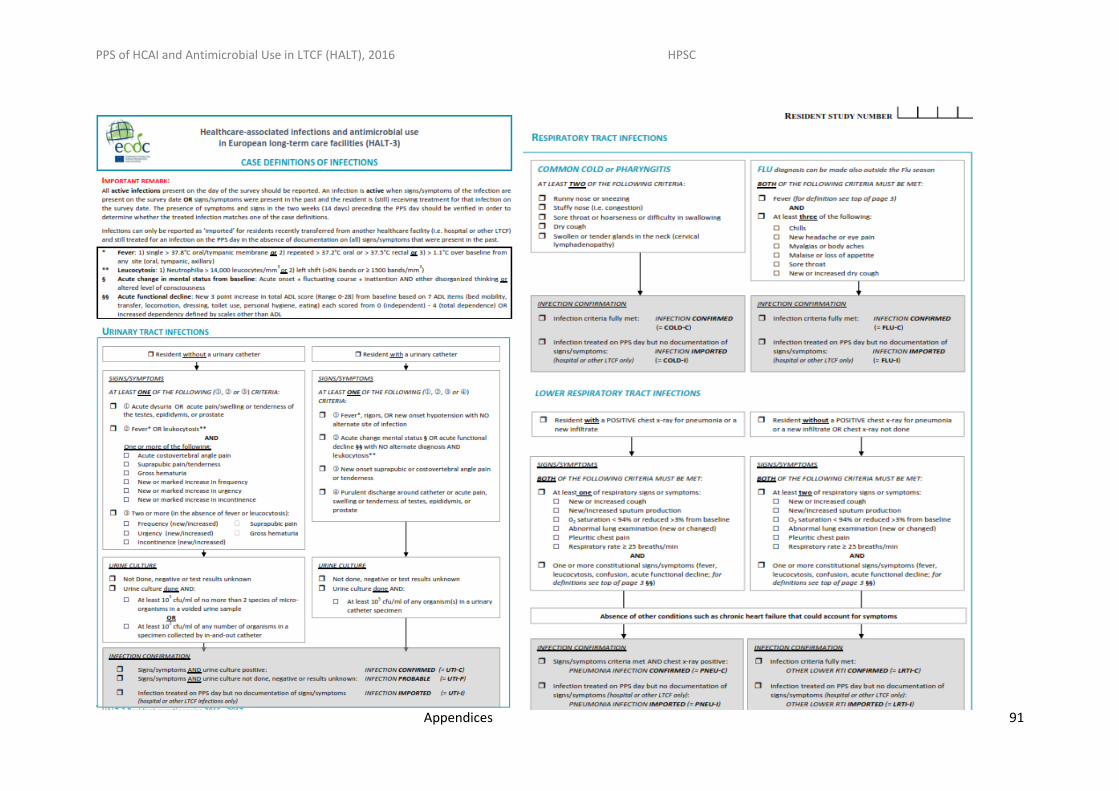
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Appendices 91
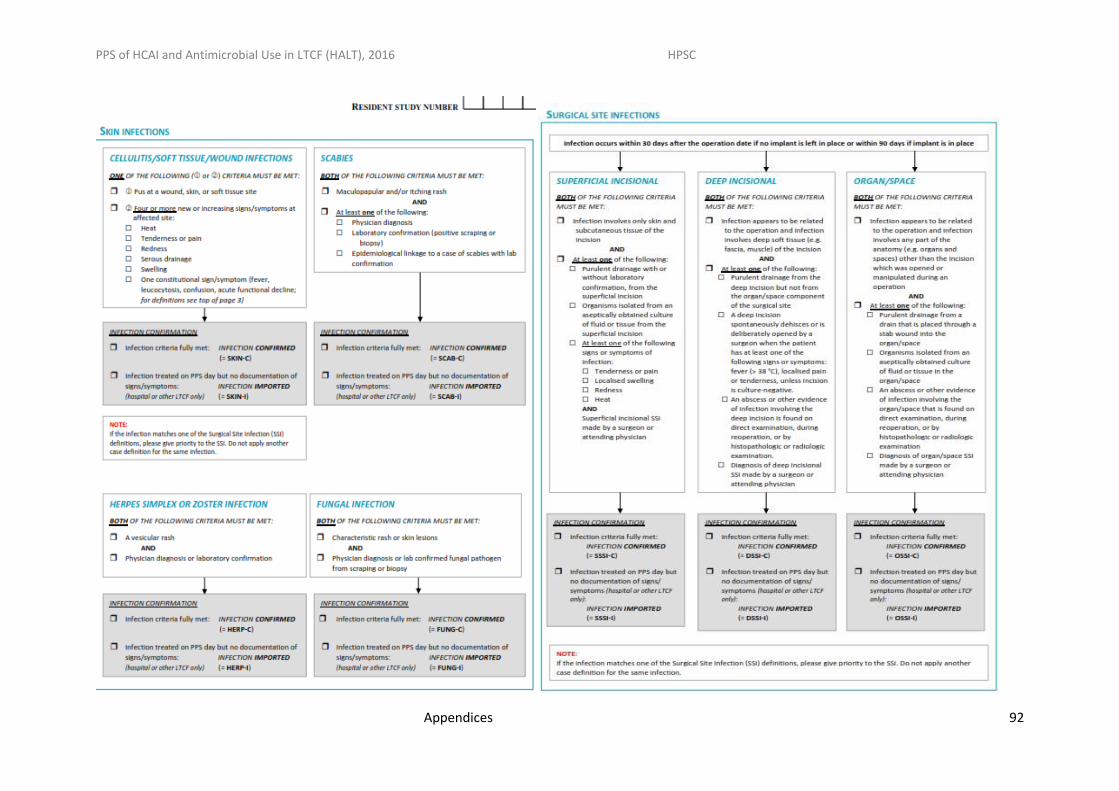
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Appendices 92
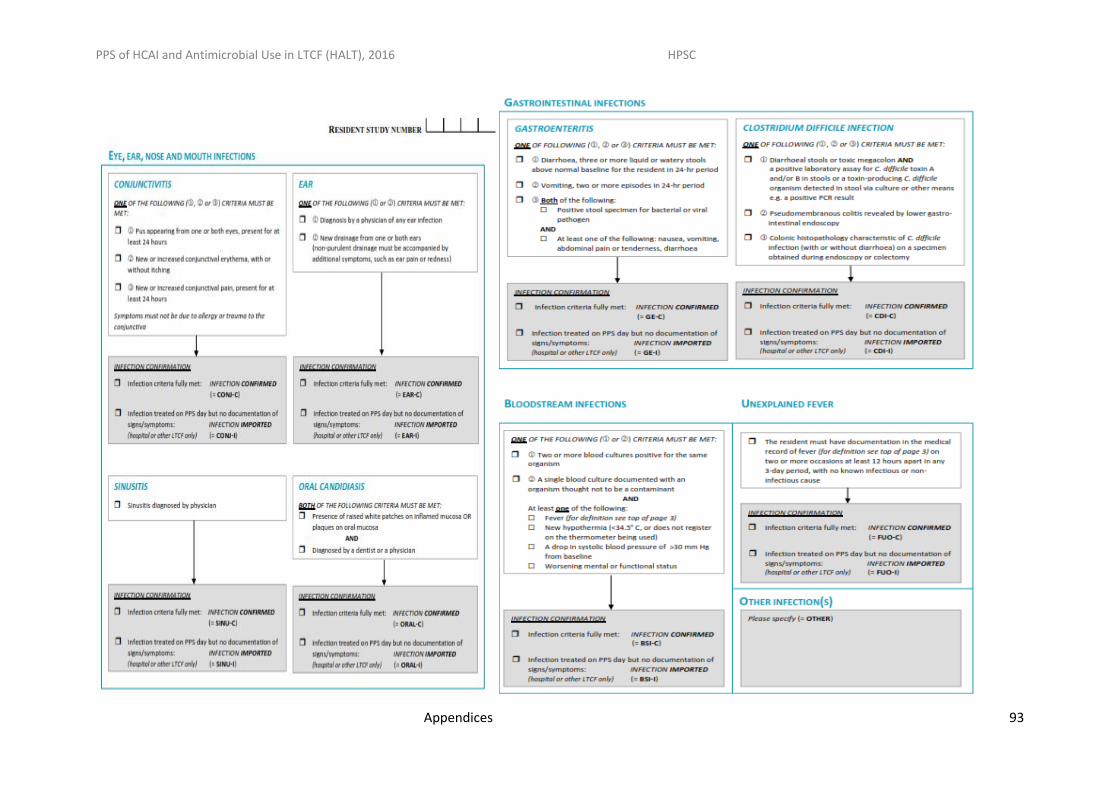
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Appendices 93
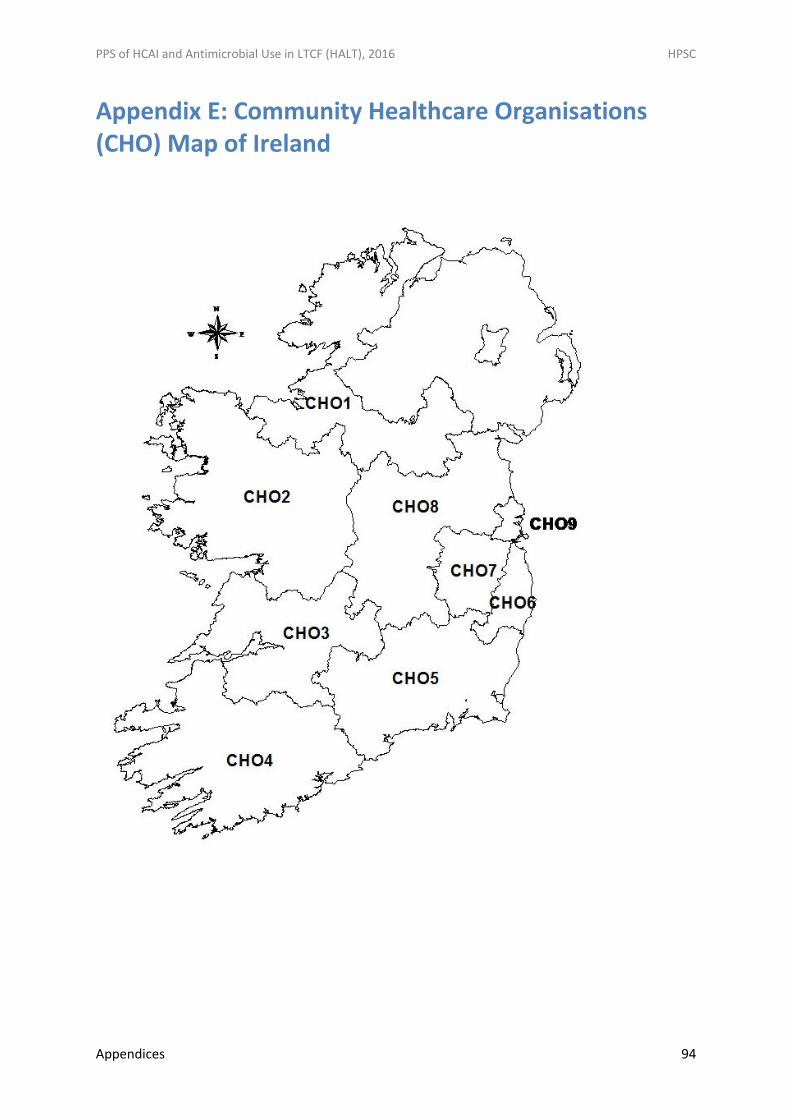
PPS of HCAI and Antimicrobial Use in LTCF (HALT), 2016 HPSC
Appendices 94
Appendix E: Community Healthcare Organisations (CHO) Map of Ireland





























