Embed Size (px)
Citation preview
Andrew Wang, HMS IIIGillian Lieberman, MD
Positron Emission Tomography Positron Emission Tomography in Lung Cancerin Lung Cancer
Andrew Wang, HMS IIIGillian Lieberman, MD
May 19, 2003
2
Andrew Wang, HMS IIIGillian Lieberman, MD
Patient DDPatient DD
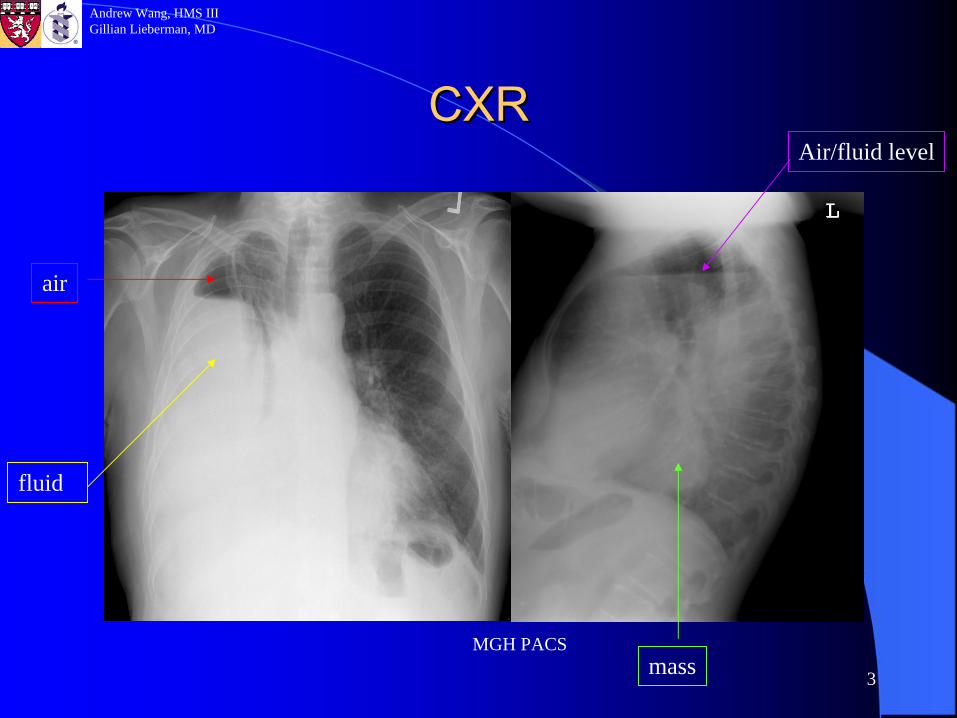
53 y/o gentleman presented with worsening dyspneaon exertion for the past two months30 pack-year smoking Hx and no significant past medical HxInitially had flu like symptoms but never fully resolved+ cough, fever, fatigue (2 months) and night sweats (1 year)- hemoptysis, chest pain, weight changesPA and Left lateral CXRs were obtained
3
Andrew Wang, HMS IIIGillian Lieberman, MD
CXRCXR
MGH PACSmass
air
fluid
Air/fluid level
4
Andrew Wang, HMS IIIGillian Lieberman, MD
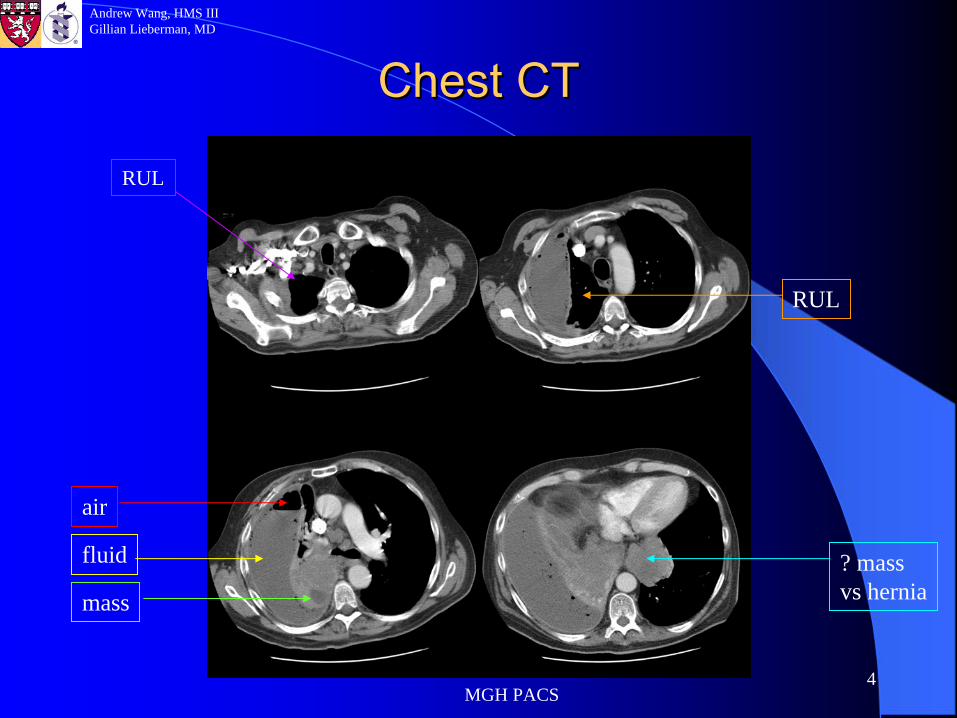
Chest CTChest CT
MGH PACS
air
fluid
mass
? mass vs hernia
RUL
RUL
5
Andrew Wang, HMS IIIGillian Lieberman, MD
Clinical CourseClinical Course
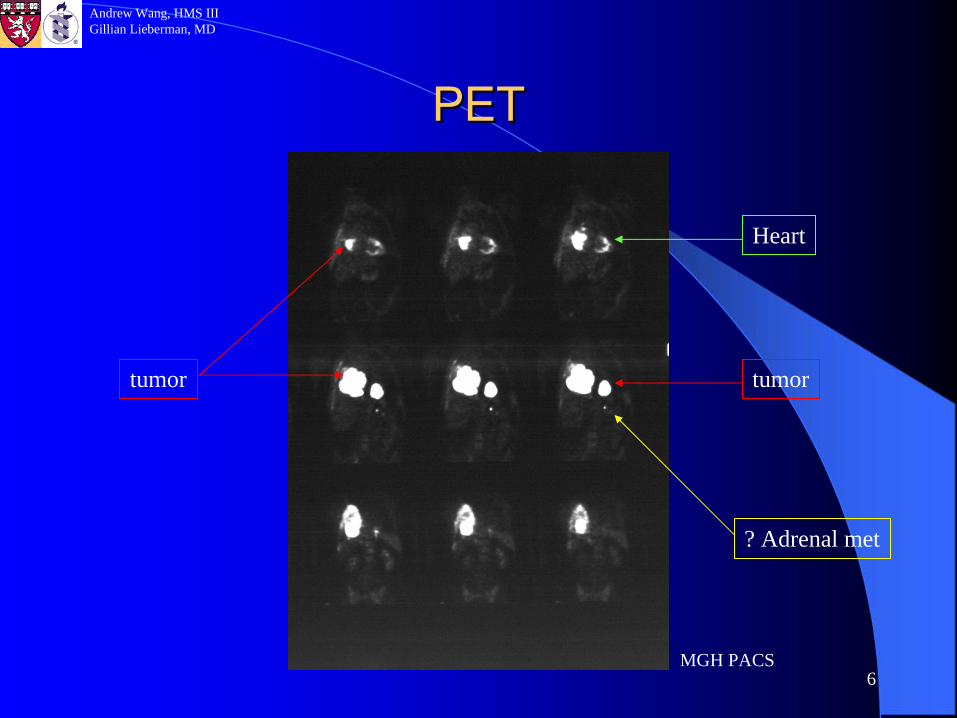
Chest tube-large empyemaBronchoscopy/biopsy-large soft tissue mass occluding right bronchus intermedius, preliminary path is SCLC.Cancer staging
–
CT-
7.5 X 10.5cm soft tissue mass in the right hilar
region. Soft tissue mass in the left posterior mediastinum
which may be contiguous with the stomach. 2.1 X 1.5 left adrenal nodule.
–
Head MRI-no mets–
Bone scan-
no bone mets–
PET for staging as well as assessing left hilar
mass and adrenal nodule. Results showed a large right lung mass and left retrocardiac
mass, right hilar
lymph node mets
and 2 left adrenal increased uptake.
6
Andrew Wang, HMS IIIGillian Lieberman, MD
PETPET
MGH PACS
tumor tumor
Heart
? Adrenal met
7
Andrew Wang, HMS IIIGillian Lieberman, MD
Our patientOur patient
Final pathology: small cell lung cancer.Stage: extensive.Treatment: –
Systemic chemotherapy–
Radiation therapy to open occluded right bronchus intermedius
PET imaging was unnecessary in this caseQuestion: when is PET indicated in evaluating lung cancer and how is it used?
8
Andrew Wang, HMS IIIGillian Lieberman, MD
Positron Emission TomographyPositron Emission Tomography
Physics–
e+
+ e-
γ
+γγ–
Photons (511 keV) leave the annihilation site in opposite direction
–
Simultaneous detection of the photons allow localization of annihilation location
–
Common positron emitters: 11C, 15O, 13N and 18F.Type of detectors–
PET-several thousand ring detectors, more signal, better resolution
–
SPECT-retrofitter with coincidence detectors, cheaper
–
PET/CT-more accurate location of cancer
9
Andrew Wang, HMS IIIGillian Lieberman, MD
PETPET
Physiology for imaging of cancers–
Cancer cells have high metabolism, and rich in hexokinases.
–
Most commonly used molecule for cancer imaging is FDG (2-18F-2-deoxy-D-glucose)
–
FDG is phosphorylated
in the cell. It cannot be degraded nor can be excreted quickly after phosphorylation.
–
FDG labels cells with high metabolism-cancers
10
Andrew Wang, HMS IIIGillian Lieberman, MD
PETPET
Patient preparation–
Fasting for at least 4 hoursPhysiologic positives: brain, myocardium, urinary system, recently exercised muscle.False positives: Inflammation and benign neoplasms.False negatives: slow growing tumors-bronchoalveolarcarcinoma, carcinoids, prostate cancer, etc.PET is approved for imaging of lung, thyroid, lymphoma, colon and melanoma cancers.PET is not indicated in SCLC (staging is only based on size) and slow growing tumors (low signal) such as bronchoalveolarcarcinoma.
11
Andrew Wang, HMS IIIGillian Lieberman, MD
Indications for PET inIndications for PET in
lung cancerlung cancer
Diagnosis: malignant vs. benign. Especially in the evaluation of solitary pulmonary nodules (SPN)
Cancer staging
Post-therapy evaluation and recurrence assessment
12
Andrew Wang, HMS IIIGillian Lieberman, MD
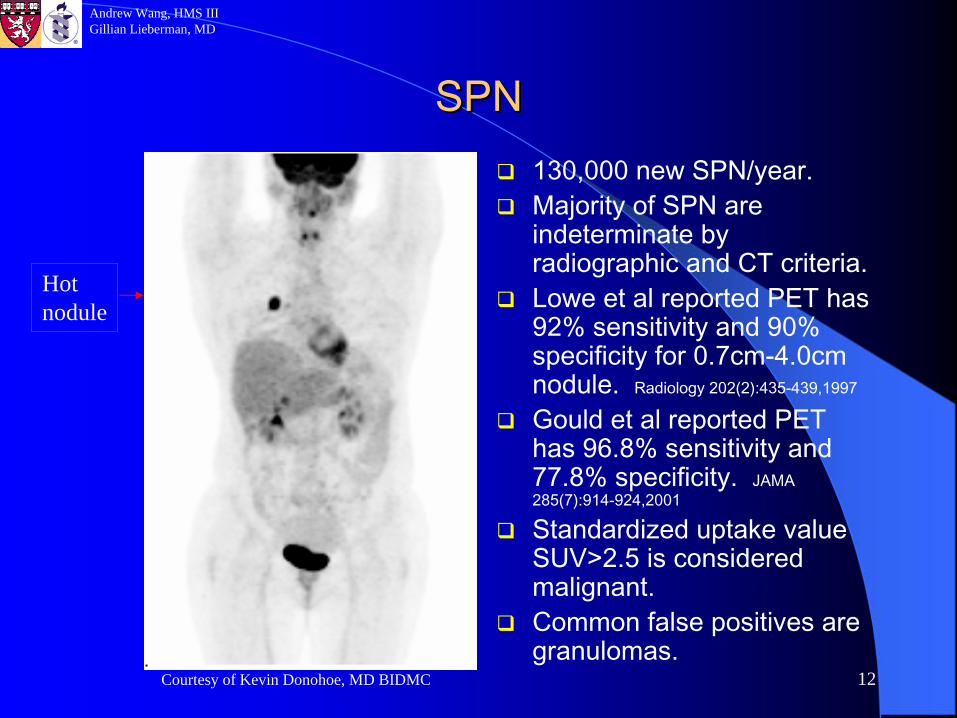
SPNSPN130,000 new SPN/year.Majority of SPN are indeterminate by radiographic and CT criteria.Lowe et al reported PET has 92% sensitivity and 90% specificity for 0.7cm-4.0cm nodule. Radiology 202(2):435-439,1997
Gould et al reported PET has 96.8% sensitivity and 77.8% specificity. JAMA 285(7):914-924,2001
Standardized uptake value SUV>2.5 is considered malignant.Common false positives are granulomas.
Hot nodule
Courtesy of Kevin Donohoe, MD BIDMC
13
Andrew Wang, HMS IIIGillian Lieberman, MD
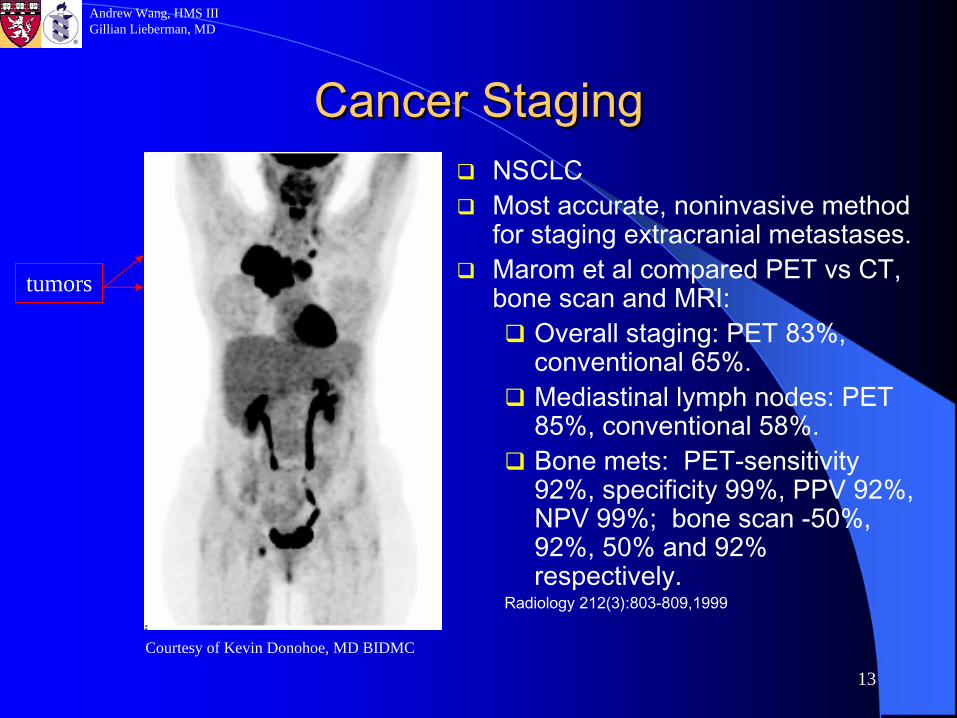
Cancer StagingCancer StagingNSCLCMost accurate, noninvasive method for staging extracranial metastases.Marom et al compared PET vs CT, bone scan and MRI:
Overall staging: PET 83%, conventional 65%.Mediastinal lymph nodes: PET 85%, conventional 58%.Bone mets: PET-sensitivity 92%, specificity 99%, PPV 92%, NPV 99%; bone scan -50%, 92%, 50% and 92% respectively.
Radiology 212(3):803-809,1999
tumors
Courtesy of Kevin Donohoe, MD BIDMC
14
Andrew Wang, HMS IIIGillian Lieberman, MD
PostPost--therapy Evaluationtherapy Evaluation
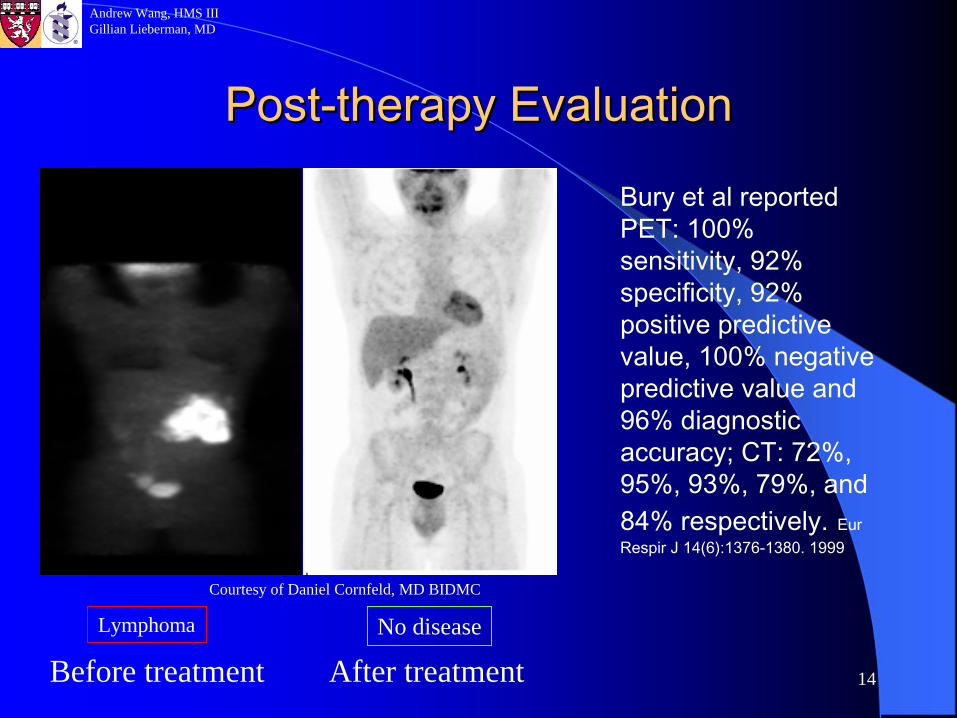
Bury et al reported PET: 100% sensitivity, 92% specificity, 92% positive predictive value, 100% negative predictive value and 96% diagnostic accuracy; CT: 72%, 95%, 93%, 79%, and 84% respectively.
Eur
Respir
J 14(6):1376-1380. 1999
Before treatment After treatmentLymphoma No disease
Courtesy of Daniel Cornfeld, MD BIDMC
15
Andrew Wang, HMS IIIGillian Lieberman, MD
SummarySummary
PET is a powerful noninvasive diagnostic tool in lung cancer imaging.It is indicated in evaluation of SPN, staging of NSCLC, and in evaluating treatment effects.It is not indicated in SCLC, and bronchoalveolar cancer.Bone mets should be evaluated with PET, not bone scan in lung cancer.
16
Andrew Wang, HMS IIIGillian Lieberman, MD
ReferencesReferencesTurkington TG, Coleman RE. Clinical Oncologic Positron Emission Tomography: An introduction. Seminars in Roentgenology 37(2):102-109. 2002.Hagge RJ, Coleman RE. Positron Emission Tomography: Lung Cancer. Seminars in Roentgenology 37(2):110-117. 2002.Lowe VJ et al. Pulmonary abnormalities and PET Data analysis : a retrospective study. Radiology 202(2):435-439,1997Gould MK et al: Accuracy of positron emission tomography for diagnosis of pulmonary nodules and mass lesions. JAMA 285(7):914-924,2001Marom EM et al. Staging non-small cell lung cancer with whole-body PET. Radiology 212(3):803-809,1999Bury T et al: Value of FDG-PET in detecting residual or recurrent nonsmall cell lung cancer. Eur Respir J 14(6):1376-1380. 1999
17
Andrew Wang, HMS IIIGillian Lieberman, MD
AcknowledgementsAcknowledgements
Kevin Donohoe, MDDaniel Cornfeld, MD
Gillian Lieberman, MDPamela Lepkowski
Larry Barbaras and Cara Lyn D’amour