Embed Size (px)
Citation preview

www.elsevier.com/locate/yebeh
Epilepsy & Behavior 9 (2006) 535–540
Case Report
Postictal autoscopy in a patient with partial epilepsy
Yukari Tadokoro *, Tomohiro Oshima, Kousuke Kanemoto
Department of Psychiatry, School of Medicine, Aichi Medical University, Karimata 21, Yazako, Nagakute-cho, Aichi-gun, Aichi-ken 480-1195, Japan
Received 20 June 2006; revised 11 July 2006; accepted 11 July 2006Available online 14 August 2006
Abstract
Autoscopy is an experience of seeing oneself in external space, viewed from within one’s own physical body. It is a complex psycho-sensorial hallucinatory perception of one’s own body image projected into external visual space, with epilepsy one of the common dis-orders reported to be associated with the experience. A survey of the literature revealed that there are few case reports of postictal auto-scopic phenomena. Herein, we report a case of a patient with partial epilepsy who has experienced postictal autoscopy for nearly 30years. Although the neurological mechanisms that cause autoscopic phenomena are not fully understood, wish-fulfilling fantasiesreleased as a result of a shaken integrity regarding personal bodily image may contribute to the shaping of the symptoms, at least inthe case of postictal autoscopy.� 2006 Elsevier Inc. All rights reserved.
Keywords: Epilepsy; Autoscopy; Hallucination; Postictal; Release phenomenon
1. Introduction
Autoscopy is the experience of seeing oneself in exter-nal space, viewed from within one’s own physical body[1]. During the experience, the subject remains withinthe boundaries of his or her physical body, or conscious-ness is perceived within the physical body [2,3]. It is acomplex psycho-sensorial hallucinatory perception ofone’s own body image projected into external visualspace [4]. Both autoscopy and out-of-body experiencesare classified as autoscopic phenomena [3], during whichthe subject sees himself or herself as a part of the extra-personal world [2].
Autoscopic phenomena occur not only in patients withneurological illnesses or in those with psychiatric disorders,but also in normal persons, in certain circumstances [3,5–7]. Epilepsy, more specifically temporal lobe epilepsy, isone of the most common disorders in which autoscopicexperiences are reported [1,8], and these phenomena com-
1525-5050/$ - see front matter � 2006 Elsevier Inc. All rights reserved.
doi:10.1016/j.yebeh.2006.07.003
* Corresponding author. Fax: +81 561 63 8270.E-mail address: [email protected] (Y. Tadokoro).
monly occur as auras prior to complex partial seizures orgeneralized tonic–clonic seizures in those patients [3].
During autoscopic experiences associated with epilepsy,the double may appear as if the subject is looking at his orher own reflection in a mirror [9,10], or the subject may seehis or her own self in a retrospective scene in a dreamy state[10]. Along with the above, postictal autoscopic experienceshave been reported in the literature [3,10,11]; however, oursurvey revealed that there are few reported cases of postic-tal autoscopic phenomena. Herein, we report a case of apatient with epilepsy who has experienced postictal auto-scopic phenomena for nearly 30 years.
2. Case
The patient, a right-handed woman, was 37 years oldwhen first referred to us for medically intractable complexpartial seizures. Tonic seizures of an unidentified natureoccurred frequently at 1 year of age, and she first experi-enced a generalized seizure at the age of 2. An EEG, atthe age of 4, revealed an abnormality, and the patientbegan taking antiepileptic drugs at that time. At the ageof 10, she noted seeing herself following seizures, beforebecoming fully conscious.

536 Case Report / Epilepsy & Behavior 9 (2006) 535–540
At the time of referral, she was experiencing complexpartial seizures several times a month, sometimes with sec-ondary generalization. Her habitual seizures occurred thesame way each time, as follows. Prior to experiencing acomplex partial seizure, the patient reported feeling a sen-sation originating from her stomach and traveling up to herthroat, or she noticed her heart beating fast for a moment.These autonomic auras sometimes recurred several timeswithin a day. Vomiting often followed and occasionallycontinued for more than 24 h, and afterward, she wasobserved to have a stony stare and tonic posturing of theright upper limb. Then, the patient bent her right armand subsequently lost consciousness, after which sherepeatedly vomited. Sometimes she passed her hands overher clothes or moved things around on a table, duringwhich oral automatisms were occasionally seen. Immedi-ately after the seizures, she experienced autoscopic phe-nomena and saw herself in external space while beingfully aware of her own physical body. In other words,her consciousness was perceived as being within her phys-ical body and she saw her second self as a separate personin front of her.
Three different types of autoscopic phenomena havebeen reported by this patient. In one type, she saw herwhole body, in normal size and color, in front of her abouta meter away. In addition, she would see her second self ina beautiful flower field with several other women, allunknown to her, and they all looked very happy and satis-fied. Her double would smile and wave to her, and ask herto come and join them. She wanted to do so, but was notable to move, as if glued to the spot. This scene would last
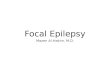
Fig. 1. Cerebral MR
a few seconds to a few minutes. Sometimes the scene wouldcontinue into another episode, in which the double wouldsay to her, ‘‘Why didn’t you come last time when I invitedyou?’’ This type of autoscopy began when she was 10 yearsold and still occurs after nearly every seizure.
At the age of 15, the patient had her first autoscopic expe-rience of the second type, which recurred repetitively fornearly 10 years. Her own double would take her by the armsaying: ‘‘Come, come! Hurry! We will be in trouble if some-body finds us having a seizure. We’ve got to hide somewhereright away.’’ Every time she experienced this type of episode,she found herself behind furniture or in a bathroom when sheregained consciousness, as if she were trying to hide.
The third type of autoscopic phenomenon was slightlydifferent from the other two. During these episodes, thepatient saw her second self either from behind or from asuperior point of view, instead of facing and interactingwith the double. At these times, the double was wearinga uniform that the patient had never worn before andwas working in an office unfamiliar to her, along with afemale supervisor. The double did not seem to notice herpresence and never turned toward her, though the patientinsisted it was herself. This type of episode began in her latetwenties and continued for about 10 years.
Interictal EEG findings demonstrated irregular back-grounds with intermittent beta and theta waves, while posi-tive sharp waves were once detected from the righthemisphere. Slight atrophy in the left hippocampus wasobserved in a cerebral MRI examination (Fig. 1). In addi-tion, interictal cerebral SPECT revealed hypoperfusion inthe bilateral frontal lobes and left temporal lobe (Fig. 2).
I (FLAIR) scan.

Fig. 2. Interictal cerebral SPECT image.
Case Report / Epilepsy & Behavior 9 (2006) 535–540 537
Although seizures continued to occur despite trials withall available antiepileptic drugs, the frequency decreasedsignificantly after increasing the carbamazepine dose andadding clobazam.
3. Discussion
Autoscopic phenomena are classified among the phe-nomena of duplication. These are visual experiences, notsimply the feeling or sense of a double being present. Thisinvisible double, which is felt to be present but not seen,may also be called a somatesthetic double [7,8,12–14]. Bothautoscopy and out-of-body experiences are classified asautoscopic phenomena. However, during the latter, thesubject sees his or her own physical body and the worldfrom a location other than that of the actual physical body(parasomatic body and visuospatial perspective), whereasduring autoscopy, conscious awareness remains withinthe boundaries of the physical body (physical visuospatialperspective) [2]. Cases of autoscopic phenomena associatedwith epileptic activity reported to date can be classified,according to their pathophysiological backgrounds, intothree main types: mirror-image type, reminiscence type,and drama type (Table 1).
3.1. Mirror-image type
In the mirror-image autoscopic experience, the patientsees his or her own body ahead, as if it were a reflectionin a mirror. Irritative phenomena of the occipital lobe seemto have a close relationship with this type of autoscopy[15,16]. Selective excitement of the occipital lobe alonecould produce visual hallucinations; however, such anexperience is normally limited to elementary hallucinationssuch as twinkling spots and whirling, colored circles [17].Autoscopy is quite a complicated phenomenon; thus, it is
Table 1Characteristics of autoscopy with epileptic activity
Type of autoscopy Clinical features
1. Mirror-image As if being reflected in a mirror
2. Reminiscence Dreamy stateTransfiguration of familiarity
3. Drama Fulfilling fantasies
more likely that other regions of the brain besides theoccipital lobe are involved. The parieto-occipital and tem-poral lobes are reported to have great influence on formedhallucinations [10,17,18]. Further, the parietal lobe mayplay an important role, as it organizes the body schema[3,10]. Maillard et al. discussed the case of a patient whoexperienced palinopsia and macrosomatognosia as ictalsymptoms in addition to mirror-image type autoscopy [9],and hypothesized that paroxysmal autoscopy in patientswith epilepsy occurs because of an ictal disturbance ofthe normal process of integration of body representationwithin the parieto-occipital networks. The coexistence ofpalinopsia with mirror-image type autoscopy in the samepatient led us to speculate that there is a relationshipbetween the two experiences.
3.2. Reminiscence type
The reminiscence type of autoscopy is typically experi-enced as an aura originating from temporal lobe epilepsyand is a feature of the dreamy state in psychomotor sei-zures [10]. This dreamy state often consists of images, rep-resenting vivid memories and deja vu, although it is an ictalwaking event with no reference to dreams [19]. Jacksonused the word reminiscence as a clinical feature of thedreamy state, commonly called intellectual aura, which hecharacterized as an elaborate mental state and distin-guished from crude sensations such as noise in the ear,strong smell in the nose, and other types of sensual input[20,21]. Janz analyzed Jackson’s studies and presentedtransfiguration of familiarity as an essential symptom ofthe dreamy state [21,22].
Devinsky et al. described a 32-year-old man born fol-lowing trauma to the left temporal region caused by for-ceps delivery [3]. The patient had experienced simple andcomplex partial seizures, as well as generalized tonic–clonic
Symptoms Localization
Aura Parieto-occipitalTemporal
Aura Temporal
Postictal Undetermined Release phenomena?

538 Case Report / Epilepsy & Behavior 9 (2006) 535–540
seizures since the age of 8. His first episode of autoscopy,which preceded a generalized tonic–clonic seizure, occurredat the age of 16. The patient was awake at the time, but feltlike he was in a dream when suddenly he saw his double forthe first time, who was about 5 feet in front of him andmowing the lawn, an activity that he should have beendoing at that time. The patient had more than a dozenautoscopic episodes immediately before complex or sec-ondary generalized tonic–clonic seizures, as well as numer-ous episodes unrelated to other seizure phenomena. Hisdouble was usually engaged in an activity that he felt heshould have been doing. The EEGs revealed left temporalepileptiform discharges.
Devinsky et al. cited two cases of Hecaen and Green[3,23]. One, a 34-year-old man with a left temporal astrocy-toma, experienced both deja vu and seeing his double. Theother, an 18-year-old man whose illness was not reported,also experienced deja vu and seeing himself since his youth.Lukinowicz’s case was a 38-year-old architect who had losthis right leg in battle at the age of 25 [4]. Eight years later,he developed seizures, preceded by a sensory aura in theform of excruciating pain in the missing limb. In thisrespect, the latter case is similar to cases of phantom limb.The first episode of autoscopy occurred 5 years after theonset of epilepsy. While talking to a builder/contractor,the patient suddenly felt very sad and weary, then sawhis double coming through a closed door. The doublewas absolutely identical to him except for one detail: thedouble did not manifest the slight limp caused by the pros-thesis. The phantom limb pain and the observation of hisdouble walking without a limp led to speculation that theremay be the same aspect of wish fulfillment in both autosco-py and phantom limb cases [4,14].
Epstein’s case was a woman whose seizure content con-tained the unpleasant visual image of seeing herself beingdrowned or trapped by fire [24]. She had recurrent dreamsthat were identical in content to her seizures. He alsodescribed a 35-year-old woman, for whom data indicatedan abnormal right temporal discharge that occurred simul-taneously with REM sleep and influenced the nature of theaccompanying dream [25]. Further, Kanemoto et al.reported that some patients with temporal lobe epilepsyexperience recurrent dreams in which they see themselveswith feelings of familiarity [26]. Recurrent, stereotypeddreams may have a close affinity to the reminiscence typeof autoscopy among patients with temporal lobe epilepsy.
Table 2Reported cases of postictal autoscopic phenomena
Patient source Seizure types and symptoms Typ
1. Fere (1891)a [10,11] CPS,GTC Dou2. Sengoku et al. (1981) [10] CPS, SPS, GTC Dou3. Devinsky et al. (1989) [3] CPS OBE4. Present case CPS, GTC, Autonomic aura Dou
a Year published.
3.3. Drama type
In the drama type of autoscopic phenomena, the sub-ject sees herself or himself playing a role, mostly the lead,in a brief story, and the scenario tends to fulfill fantasies.Some authors have speculated that autoscopy may serveas a mechanism for the expression of latent wishes[3,27,28]. Thus far, this type of epileptic autoscopy hasbeen reported to occur only during postictal states, andonly a few case reports have been published. Casesreported as postictal autoscopic phenomena are listed inTable 2.
In Fere’s case, a man who experienced autoscopy of thedrama type during transient hemiparalysis of the right sideafter a seizure [10,11], the double appeared to his rightwhile he was lying on the bed and he was himself at thetime, even though he was affected by postparoxysmalparalysis on the right side. The patient would shout out:‘‘Give him a cigarette! Light it up, the poor man has noright hand. Rub his hand, his fingers are prickly.’’ Lher-mitte mentioned, quoting Fere’s case, that the visionalways appeared in the same manner and with the sameshape for the same patient, and sometimes the subjecttransferred his own sensation to the double [11]. The auto-scopic experience in that case is classified as the dramatype; however, the autoscopic experience may have beenclosely associated with his paralyzed half-body. Further,somatoparaphrenic aspects should be considered in inter-preting his symptoms.
Sengoku et al. reported a 33-year-old woman who twiceexperienced drama-type autoscopy [10]. In the first episode,she saw her own self having a seizure when her second selfcame toward her with a handkerchief, then she fully recov-ered. The patient always dribbled from her mouth duringseizures and had to wipe the saliva with a handkerchief.In the second episode, she saw her double being chasedby a bear and was running away to get a glass of water,while she again saw her own self having a seizure at thesame time. When she regained consciousness, the patientfound herself at the sink, where water was running fromthe faucet. In addition, Devinsky reported a 27-year-oldman who had focal motor seizures involving the rightextremities that progressed to complex partial seizures [3].The man had an out-of-body experience during the postic-tal period, and the feeling of drifting out of his own bodylasted for 15–20 min.
e of episode Clinical findings
ble Left-sidedble EEG: right temporal epileptiform discharges
EEG: intermittent theta in left frontotemporal regionble SPECT: hypoperfusion

Case Report / Epilepsy & Behavior 9 (2006) 535–540 539
3.4. Present case
The first two types of autoscopy experienced by ourpatient are typical of the drama type. However, the thirdtype of autoscopic phenomenon is slightly different fromthe other two, as she saw the double either from behindor from a superior point of view. Superficially, it wouldseem to be more of an out-of-body experience than autos-copy. Nevertheless, she still viewed the double from withinher own physical body. Therefore, we consider that herthird type is also the drama type of autoscopy.
For a differential diagnosis of our case, the possibility ofdissociative reaction must be considered. Her habitual sei-zures are relatively brief, normally lasting only 10–15 mineach time, and repetitively occur in the same way everytime, a few times each month. In a few instances, she waswalking across the street against a red light during the sei-zure and was nearly hit by a car. At other times, the patientrolled down stairs and got injured. Without exception, theautoscopic phenomena are exclusively coupled with com-plex partial seizures and have never occurred prior to com-plex partial seizures. In view of these findings as well asMRI and SPECT results, we conclude that her seizuresare complex partial seizures and not dissociative reactions,and believe that epilepsy is the underlying cause of her par-oxysmal, transient autoscopy.
Laterality and localization remain to be determined inthe present case. Although ictal vomiting has often beendiscussed in association with right-sided temporal lobe epi-lepsy [30,31], though with some exceptions [32], the dyston-ic posturing of the right upper limb during the initial phaseof complex partial seizures, as well as MRI and SPECTfindings, suggest the opposite with respect to sidedness. Abroad disturbance of the brain including the temporallobes, more dominantly on the left side, is assumed tooccur in this case.
Although the neurological mechanisms that cause auto-scopic phenomena remain open to question, both the mir-ror-image and reminiscence types seem to corresponddirectly to localized ictal discharges, and can be consid-ered to represent focal irritation of the brain. In contrast,drama-type autoscopy, which seems to occur only duringa postictal period, cannot be simply reduced to ictal activ-ity. One possible explanation might be that it is equivalentto Todd’s paralysis. Postictal exhaustion of the temporalor possibly temporoparietal junction plus partiallyimpaired consciousness, which many recent papers havesuggested are prerequisites for the genesis of autoscopicphenomena, are a perfect match to the condition. Howev-er, this explanation of autoscopic phenomena as a doublefailure to integrate proprioceptive, tactile, and visualinformation with respect to one’s own body (disintegra-tion in personal space), along with an additional vestibu-lar dysfunction leading to disintegration betweenpersonal (vestibular) space and extrapersonal (visual)space, can be accepted only with reservation in cases ofdrama-type autoscopy, because the complex and consis-
tently repeated experiences typical of these patients cannotbe well explained as a result of the mere mechanical dis-connection between vestibular and visual perceptions ofspace.
Cogan presumed that hallucinations of a continuous,nonstereotype variety represented release phenomenaresulting from loss or suppression of normal visual input,in contrast to episodic hallucinations, which represent irri-tative phenomena [29]. Further, he noted that a major fac-tor in releasing hallucinations is loss of normally inhibitedvisual control through blindness, hemianopia, or loss ofcognitive functions.
The parents of the present patient divorced when shewas 5 years old, and she was raised by her grandparents,during which time her grandmother physically abusedher. When she was 10 years old, her mother returned homewith a new husband and their son. Thereafter, she marriedat the age of 22 and divorced after 10 years, because herhusband did not understand her seizures and her need totake antiepileptic medication. She remarried a year afterthe divorce and claims to have lived a happy life since.These experiences may be contributory to the prominentwish-fulfilling aspects of the present case. Indeed, even inthe drama type, deranged temporal (or temporoparietal)lobe function coupled with partially impaired conscious-ness, which shakes the fundamental body integrity of anindividual, seems to be a prerequisite. However, releasedfantasies resulting from shaken personal integrity may havegreat impact on the shaping of the symptoms. Additionalintensive studies of postictal autoscopic phenomena mayprovide clues leading to a better understanding of the con-nections between the brain and traumatic psychologicalexperiences.
References
[1] Dening TR, Berrios GE. Autoscopic phenomena. Br J Psychiatry1994;165:808–17.
[2] Blanke O, Landis T, Spinelli L, Seeck M. Out-of-body experience andautoscopy of neurological origin. Brain 2004;127:243–58.
[3] Devinsky O, Feldmann E, Burrowes K, Bromfield E. Autoscopicphenomena with seizures. Arch Neurol 1989;46:1080–8.
[4] Lukianowicz N. Autoscopic phenomena. Arch Neurol Psychiatry1958;80:199–220.
[5] Brugger P, Agosti R, Regard M, Wieser HG, Landis T. Heautoscopy,epilepsy and suicide. J Neurol Neurosurg Psychiatry 1994;57:838–9.
[6] Collacott RA. Autoscopy, mental handicap and epilepsy: a casereport. Br J Psychiatry 1998;153:825–7.
[7] Ishifuku T. Clinical psychopathology of the double. Psychiatr NeurolJpn 1979;81:33–61.
[8] Grusser OJ, Landis T. The splitting of ’I’ and ’me’: heautoscopy andrelated phenomena. Vision and visual dysfunction. Visual agnosiasand other disturbances of visual perception and cognition, vol.12. Basingstoke, Hampshire: Macmillan Press, Scientific & Medical;1991. p. 297–303.
[9] Maillard L, Vignal JP, Anxionnat R, Taillandier L, Vespignani H.Semiologic value of ictal autoscopy. Epilepsia 2004;45:391–4.
[10] Sengoku A, Kawai I, Ohashi H, Fujinawa A. Paroxysmal autoscopy.Seishin Igaku (Clin Psychiatry) 1981;23:239–43.
[11] Lhermitte J. Visual hallucination of the self. Br Med J1951;1:431–4.

540 Case Report / Epilepsy & Behavior 9 (2006) 535–540
[12] Brugger P, Regard M, Landis T. Unilaterally felt ‘‘presences’’: theneuropsychiatry of one’s invisible Doppelganger. NeuropsychiatryNeuropsychol Behav Neurol 1996;9:114–22.
[13] Brugger P, Regard M, Landis T. Illusory reduplication of one’s ownbody: phenomenology and classification of autoscopic phenomena.Cogn Neuropsychiatry 1997;2:19–38.
[14] Takayanagi I. Doppelganger: evaluation of Capgras syndrome, bodyimage, ego disturbances and depersonalization. Psychiatr Neurol Jpn1971;73:42–51.
[15] Commission on Classification and Terminology of the InternationalLeague Against Epilepsy. Proposal for revised classification ofepilepsies and epileptic syndromes. Epilepsia 1989;30:389–99.
[16] Hara S. Ictal ‘‘Doppelganger’’ experience. Nou To Seishin No Igaku(Brain Sci Mental Disord) 1999;10:195–200.
[17] Kolmel HW. Die homonymen Hemianopsien—Klinik undPathophysiologie zentraler Sehstorunge. Berlin: Springer-Verlag;1988.
[18] Dewhurst K, Pearson J. Visual hallucinations of the self in organicdisease. J Neurol Neurosurg Psychiatry 1955;18:53–7.
[19] Epstein AW, Freeman NR. The uncinate focus and dreaming.Epilepsia 1981;22:603.
[20] Jackson JH. Lectures on the diagnosis of epilepsy (1879). In: TaylorJ, editor. Selected writings of John Hughlings Jackson, vol. 1. NewYork: Basic Books; 1958. p. 276–307.
[21] Sengoku A, Seino M, Kawai I. About a dreamy state in psychomotorseizures. Seishin Igaku (Clin Psychiatry) 1982;24:699–705.
[22] Janz D. Die Epilepsien. Stuttgart: Georg Thieme Verlag; 1969.[23] Hecaen H, Green A. Sur I’heautoscopie. Encephale 1957;46:581–94.[24] Epstein AW. Recurrent dreams: their relationship to temporal lobe
seizures. Arch Gen Psychiatry 1964;10:25.[25] Epstein AW, Hill W. Ictal phenomena during REM sleep of a
temporal lobe epileptic. Arch Neurol 1966;15:367.[26] Kanemoto K, Kawai I. Temporal lobe epilepsy and recurrent dreams.
Seishin Igaku (Clin Psychiatry) 1992;34:739–44.[27] Grotstein JS. Autoscopy: the experience of oneself as a double.
Hillside J Clin Psychiatry 1983;5:259–304.[28] Todd J, Dewhurst K. The double: its psycho-pathology and psycho-
physiology. J Nerv Ment Dis 1955;122:47–55.[29] Cogan DG. Visual hallucinations as release phenomena. Albrecht
von Graefe’s Arch Clin Exp Ophthalmol 1973;188:139–50.[30] Devinsky O, Frasca J, Pacia SV, et al. Ictus emeticus: further
evidence of nondominant temporal involvement. Neurology1995;45:1158–60.
[31] Kanemoto K. Ictus emeticus status epilepticus as an aura continua ina patient with temporal lobe epilepsy. Neurol Med 1996;45:255–7.
[32] Schauble B, Britton JW, Mullan BP, et al. Ictal vomiting inassociation with left temporal lobe seizures in a left hemispherelanguage-dominant patient. Epilepsia 2002;43:1432–5.