Embed Size (px)
Citation preview

C H A P T E R
1
Growth: Importance and Implicationsof Variations
Jaya Sujatha Gopal-Kothandapani, Indraneel Banerjee, Leena Patel
P
h
O U T L I N E
Part 1: Normal Growth and Puberty
1Part 2: Variations in Linear Growth
11Specific Conditions Presenting with ShortStature and Growth Failure
12ractical Pediatric Endocrinology in a Limited Resource Setting
ttp://dx.doi.org/10.1016/B978-0-12-407822-2.00001-3 1
Tall Stature
24Specific Conditions Presenting with TallStature
25References and Further Reading
26PART 1: NORMAL GROWTHAND PUBERTY
Introduction
Growth is a complex dynamic process bywhich the body and various structures withinthe body increase in size. Normal growth resultsfrom the careful co-ordination of three cellularprocesses: (1) an increase in the number of cellsor cell hyperplasia, (2) increase in the size ofcells or cell hypertrophy and (3) programmedcell death or apoptosis. It involves tissues,organs, body parts and the whole body, andany or all of these can be affected when growthis disrupted. Although the term ’growth’ has
a wide definition, we have restricted its use togrowth in height or linear growth for thepurpose of this chapter. The growth pattern ofa child and adolescent is a good indicator of:
• health and general well-being• nutritional status• disease activity and response to treatment of
any underlying illness.
Commonly Used Terms
Interpreting growth measurements for anyindividual child requires comparing with refer-ence values. The reference can be the child’sprevious measurements and/or those derived
Copyright � 2013 Elsevier Inc. All rights reserved.

1. GROWTH: IMPORTANCE AND IMPLICATIONS OF VARIATIONS2
from measurements of a sample of healthy chil-dren in a population. For example, a child’sheight at a particular age can be comparedwith the child’s height measurements atprevious time points, if available, as well aswith a height reference such as the WHO ChildGrowth Standards. The height reference may beavailable as a table or as a growth chart.
A histogram of height measurements froma reference sample shows a bell-shaped orGaussian distribution, also conventionallydescribed as a ’normal’ distribution (Figure 1.1).This is because a greater proportion of themeasurements will cluster around the averageand the number ofmeasurements that are furtheraway from the average are fewer. Themean is theaverage value for a bell-shaped distribution andstandard deviation describes the spread ofvalues. Percentiles, or centiles, represent thepercentage of the population that falls belowthat point. Thus in a bell-shaped distributionthe mean represents the 50th centile and thissimply indicates that 50% of the values will fallbelow while 50% will be above the mean. The3rd, 15th, 50th, 85th and 97th centiles are shownin the WHO growth charts (Figure 1.2).
A ’normal’ curve with a mean of 0 and a stan-dard deviation of 1 is called a standard normalcurve (Figure 1.2; Table 1.1). The Empirical Rulecan be applied to this, such that approximately:
3rdcentile
15thcentile
50thcentile
85thcentile
97thcentile
0 mean
I -1 SD
I -2 SD
I +1 SD
I +2 SD
FIGURE 1.1 ’Normal’, bell-shaped or Gaussian distri-bution from smoothed out histogram of height measure-ments from a reference population sample.
• 68% of the values will fall within 1 standarddeviation of the mean in either direction
• 95% of the values will fall within 2 standarddeviations of the mean in either direction
• 99.7% of the values fall within 3 standarddeviations of the mean in either direction.
Since only 5% of measurements from healthychildren fall outside the range between e2 andþ2 standard deviations, a height below or abovethis range is more likely to be abnormal thannormal. In the absence of a defined cut-off forabnormal growth measurements, the proba-bility of whether a measurement is likely to benormal or abnormal is useful in clinical practice.
Any ’normal’ distribution can be standardisedby converting the mean to zero and the standarddeviation to one. For a measured value (e.g.height), the standard deviation score (SDS) orz-score can be calculated (measured value minusmean value/standard deviation), and then thecorresponding percentile can be obtained fromprobability tables (found in textbooks on statis-tics). Converting observed growth measure-ments into SDS is useful in clinical research andallows comparisons to be made irrespective ofage, gender and ethnic background.
Types of Growth Charts
Gender specific height, weight and headcircumference centile charts are widely used inclinical practice. They represent age on the hori-zontal axis and include selected centiles forreference populations from different countries(Figure 1.2 shows the WHO length/height-for-age chart for girls). These are described asdistance charts. The centile lines on a distancechart show the normal pattern of growththrough childhood and adolescence. Charts forother growth measurements (such as sittingheight and subischial leg length) and disease-specific growth charts (e.g. Turner syndrome,Down syndrome) are also available. Growthvelocity charts illustrate the rate of change inmeasurements per year on the vertical axis

452 4 6 8 10 2 4 6 8 10 2 4 6 8 10 2 4 6 8 10 2 4 6 8 10
50
60
70
80
90
100
105
110
115
120
85
95
55
65
75
45
50
60
70
80
90
100
105
110
115
120
85
95
55
65
75
Birth 1 year 2 years 3 years 4 years 5 years
Age (completed months and years)
Leng
th/H
eigh
t (cm
)
Months
Length/height-for-age GIRLS
Birth to 5 years (percentiles)
WHO Child Growth Standards
97th
85th
50th
15th
3rd
FIGURE 1.2 Length/height distance chart showing 3rd, 15th, 50th, 85th and 97th centile lines for the referencepopulation.
TABLE 1.1 Approximate Relationships Between Perc-entiles and Standard Deviations for a Sta-ndard Normal Distribution
Standard deviation Percentile
þ3 99.9
þ2.5 99
þ2 97.7
þ1 84.1
0 50
e1 15.9
e2 2.3
e2.5 1
e3 0.1
PART 1: NORMAL GROWTH AND PUBERTY 3
and age on the horizontal axis (Figure 1.3).However, theymay not be available for differentpopulations worldwide.
Problems can arise with use of a growthchart derived from different population data.Previously, WHO data were derived from theNational Centre for Health Statistics (NCHS)standards from North America. The mostrecent WHO growth charts are derived fromlongitudinal growth data in optimally nour-ished children from six different countries,including those that are relatively underdevel-oped. While these charts are not necessarilyrepresentative of undernourished children indeveloping countries, they aim to providea common international reference standard,which may be adopted for use in countries

Height velocity
Age
GirlsBoys
FIGURE 1.3 Height velocity chart showing the 50thcentile for girls (light grey) and boys (dark grey).
1. GROWTH: IMPORTANCE AND IMPLICATIONS OF VARIATIONS4
where recent national standards are not avail-able. If possible, the development of a localnational standard should be encouraged. Thesestandards should be updated over time to takeinto account secular trends and shiftingeconomic and nutritional status in thosecountries.
Phases of Linear Growth
Normal growth is a continuous process witha predictable pattern. It starts prenatally andcontinues until the epiphyses at the ends oflong bones are fused. The latter occurs whenfull pubertal maturation is achieved. Deviationsfrom the normal pattern of growth provide cluesto the state of health of a child and possibleunderlying pathology.
The period of growth can be subdivided intoa phase before birth and three phases after birth:
1 Fetal phase: During this phase a singlefertilised egg grows and develops over 9months into an infant with an average lengthof about 50 cm. Thus the growth rate or
height velocity during this phase is the fastest(approximately 70 cm/year).
2 Infancy phase: Although considerablegrowth occurs initially and length increasesby about 23e25 cm in the first year, the rate ofgrowth rapidly declines to about 9 cm/yearby age 2 years and 7 cm/year by age 4 years.
3 Childhood phase: Through mid-childhoodfrom age 4 years and until the onset ofpuberty, growth velocity remains relativelysteady at around 5e7 cm/year.
4 Puberty phase: This phase begins with theonset of puberty and ends when adult heightis attained. It is characterised by thedevelopment of secondary sex characteristicsand a pubertal growth spurt when the peakgrowth rate increases dramatically to anaverage of 8 cm/year in girls and 10 cm/yearin boys. The timing of the onset of puberty,peak growth rate and cessation of growthoccurs earlier in girls compared to boys, andcontributes to men being nearly 12.5 cm tallerthan women.
Key Factors which Regulate Growth andBasic Requirements for Normal Growth
Genes, nutrition and hormones have impor-tant effects on fetal and postnatal growth. Fetalgrowth is determined by the availability ofglucose in utero and influenced by the IGFsystem. Nutrition, insulin and IGF-I regulategrowth in early infancy and growth hormonebegins to have an effect from the second 6months of life. During puberty, growth is regu-lated by both growth hormone and sexsteroids. Other hormones necessary for normalgrowth but which do not directly controlgrowth are:
• thyroid hormones• vitamin D• insulin• leptin• glucocorticoids.

TABLE 1.2 Basic Requirements for Normal Growthand Examples of Conditions When theseare not Available and Growth is AdverselyAffected
Basic requirements
Conditions when basic
requirements are not available
Happiness Emotional neglect andpsychosocial deprivation
Health Any chronic illness
Nutrients Malnutrition from any cause
Normal cellsand bones
Genetic conditions includingskeletal dysplasia, i.e.conditions in which bones areincapable of normal growth
Hormones Hormone deficiencies or excesssuch as hypothyroidism orglucocorticoid excess
TABLE 1.3 Key Components of the History forthe Assessment of Growth
• Presenting complaint: short or tall; early, delayed or arrested
puberty; associated symptoms such as weight loss or weight
gain.
• Duration of the problem and progress.
• Past history: symptoms associated with specific syndromes,
hypothalamic-pituitary lesions, systemic illness.
• Dietetic history: estimated food energy and protein intake,
history suggestive of vitamin or mineral deficiency, missed
meals, lean periods, diarrhoea, vomiting, skin changes
suggestive of malnutrition.
• Medications: prolonged corticosteroid treatment.
• Antenatal details: maternal health, illness, medications, alcohol,
recreational drugs.
• Fetal monitoring history: ultrasound scan, fetal movements.
• Birth details: gestation at birth, mode of delivery, need for
resuscitation, birth weight, length, head circumference.
• Postnatal period: hypoglycaemia, jaundice, feeding difficulties,
floppiness, surgery in the neonatal period, unusual features such
as puffy feet, hands and neck.
• Neurodevelopment: problems with speech, hearing, learning,
vision, behaviour.
• Family history: consanguinity, mother’s and father’s height,
mother’s and sister’s age at menarche, father’s and brother’s age
at pubertal growth spurt and starting to shave, family members
with growth disorders, known inherited or auto-immune
conditions.
• Social background: parents’ education, employment, income,
stress in family.
• School and social activities: academic performance, behaviour,
friends; physical and/or psychological impact such as bullying
and emotional problems.
PART 1: NORMAL GROWTH AND PUBERTY 5
In addition to these factors, there are somebasic requirements for normal growth andwithout them growth is adversely affected(Table 1.2).
Clinical Assessment of Growth
Clinical assessment of growth requiresthorough:
• history• growth measurements• pubertal staging• clinical examination.
History
A history from the child who is able tocommunicate and carers provides valuableinformation about their specific concerns,beliefs and expectations. The key componentsare presented in Table 1.3.
Growth Measurements: Anthropometry
For any growth measurement, repeatedmeasurements over time are more informative
than single measurements as they show thepattern of growth and growth velocity.
WEIGHT
Infants should be weighed naked and chil-dren with minimal clothing using accuratelycalibrated scales. Weight should be recorded inkilograms and to the nearest 100 grams.
A number of formulae are available for esti-mating average weight for a healthy child by

1. GROWTH: IMPORTANCE AND IMPLICATIONS OF VARIATIONS6
age (Table 1.4). The weight derived from theseformulae is only a rough guide to the estimatedweight. It is advisable to weigh accurately andto plot on reference standards, such as theWHO centiles.
SUPINE LENGTH AND STANDING HEIGHT
Supine length should be measured from birthto 2 years and older children who are unable tostand independently. Standing height ismeasured in children older than age 2 yearswho can stand independently. The instrumentsavailable for measuring length range fromsimple, relatively cheap boards, light portablemeasuring mats which can be rolled up tomore sophisticated equipment such as the Har-penden neonatometer. For standing height,fixed wall-mounted stadiometers as well asportable equipment can be used (such as Mini-metre and the Leicester Height Metre). Therange of error is greater with wall chartscompared to a stadiometer. It must be appreci-ated that even stadiometers may be susceptibleto error. Error can arise from:
• inappropriate installation of equipment,positioned incorrectly
• incorrect use, such as faulty setting of thedigital counter of a stadiometer owing torough handling
• incorrect technique of positioning the child• unco-operative child.
TABLE 1.4 Formulae for Estimating Average Weightand Standing Height
Age Formula
Weight in kg Birth 3.5 kg
1e12 months 0.5 � Age in months þ 4
1e5 years 2 � Age in years þ 8
6e12 years 3 � Age in years þ 7
Standingheight in cm
2e12 years (Age in years � 6) þ 77
A solid rod of known length should be usedto calibrate the equipment. The most importantaspect of measuring length and height is thetechnique of positioning the child. This remainsuniform irrespective of the equipment used(Figure 1.4). Although height can be measuredby one person, length requires two people.
The measurements should be recorded incentimetres and to the nearest millimetre.Whenever possible, serial measurements shouldbe made with the interval between measure-ments at least 3 months or more.
INTERPRETING LENGTH AND HEIGHT
MEASUREMENTS
A child’s growth measurements should beplotted on centile charts so that comparisonscan be made with the reference population. Inaddition, the child’s height needs to be inter-preted in the context of parents’ heights(Figure 1.5). When possible, parents’ heightsshould be obtained by direct measurementrather than relying on reported values, whichare likely to be error prone. Midparental heightis an indicator of the child’s growth potentialbased on the genetic background. Midparentalheight is calculated as:
½ðfathers height in cm
þmothers height in cmÞO2� � 7 for a girl
½ðfathers height in cm
þmothers height in cmÞO2� þ 7 for a boy
This formula is derived from children in theUK but is also applicable for children in otherparts of the world. The target centile range is thestandard error on either side of the midparentalheight. This is approximately 10 cm in boysand 8.5 cm in girls. The midparental heightformula is applicable in those where parentalheights are not wide apart. In those wherematernal and paternal heights are widelydiscrepant, a midparental height may not be reli-able as a marker of genetic growth potential. In

1. Height metre accurately calibrated
the wall3. Shoulders relaxed, back and bottoms against the wall, legs
straight4. Eyes looking straight ahead and in the same plane as the external
auditory meati5. Ensure headboard is on top of the head
mastoid processes as the child breathes out; arms by the side7. Read height to the nearest millimetre
accurately calibrated2. One person positions head correctly in contact with
headboard3. Another person ensures back and legs are straight and
4. Read length to nearest millimetre
(A) Supine length – if child under 2 years or not able to stand
(B) Standing height
1
1
2
2
3
3
3
3
4
45
6
7
Frankfurt’s plane
FIGURE 1.4 Techniques for measuring (A) supine length and (B) standing height.
PART 1: NORMAL GROWTH AND PUBERTY 7
such cases, the child’s height usually tends tofollow the centile line for either of the parents’heights.
Parents’ heights are plotted on the right-hand side on growth charts as illustrated inFigure 1.5. As the charts are gender specific,subtract 14 cm from father’s height to plot iton a girl’s chart and add 14 cm to mother’sheight to plot it on a boy’s chart.
Height measurements can also usefully beexpressed as standard deviation scores (SDS),where a child’s height is compared with themean of other children of matched age andsex. It can be then used to compare children ofdifferent ages and sex. Height SDS is derivedby the formula:
Child0s height measurement�mean height forage from a reference chart
1 SD of height for age on a reference chart
HEIGHT VELOCITY
The increment in height between two timepoints can be used to estimate the rate of changeor height velocity:
Height velocity in cm=year ¼ðHeight at time point 2 ½cm��Height at time point 1 ½cm�Þ
ðAge at time 2 ½years� �Age at time 1 ½years�Þ
The reliability of an estimated height velocitydepends on:
• the time interval between the two heightmeasurements
• the reliability with which the two heightmeasurements are made.
The error in measuring height can be about0.15 cm even with an experienced observer.Since an estimate of height velocity from

Height-for-age Boys
5 to 19 years (percentiles)
190
180
170
160
150
140
130
120
110
100Months Years
3 6 9 3 6 9 3 6 9 3 6 9 3 6 9 3 6 9 3 6 9 3 6 9 3 6 9 3 6 9 3 6 9 3 6 9 3 6 9 3 6 95 6 7 8 9 10 11 12 13 14 15 16 17 18 19
110
100
120
130
140
150
160
170
180
190
F1
M1
F2
M2
Age (completed months and years)
Hei
ght (
cm)
3rd
15th
50th
85th
87th
World Health
Organization
A
B
2007 WHO Reference
FIGURE 1.5 Height distance chart for boys.Note: The reference centile lines as well as parents’ heights are useful for interpreting the growth of a child. A growthtrajectory that is parallel to the reference centiles indicates normal height velocity. Deviation downwards suggests poorlinear growth (A), and upwards suggests rapid growth (B). The initial height of child A and child B would be consideredappropriate for father 1 (F1) and mother 1 (M1) but short for parents F2 and M2.
1. GROWTH: IMPORTANCE AND IMPLICATIONS OF VARIATIONS8
intervals less than 12 months requires extrapo-lating, the error will be magnified. Thus theerror is lower when height velocity is estimatedfrom measurements taken 12 months apart andgreater with shorter intervals between the twoheight measurements.
A child’s rate of growth in height can be inter-preted from a height distance chart and withouta height velocity chart. Serial height measure-ments from a child plotted on a distance chartwill reveal the child’s growth trajectory. Fora healthy child, this trajectory will be reasonablyparallel to the reference centile lines on the
growth chart. An individual’s growth trajectorythat deviates downwards from the referencescentile lines suggests poor linear growth.When it deviates upwards, the growth trajectoryindicates rapid growth (Figure 1.5).
Obtaining records of past height measure-ments from additional sources can be valuable.These include maternal and child health recordsand records retained by the family from serialmeasurements at home. Parental observationsof increasing divergence in growth patternsbetween children in the same family may alsobe useful for growth assessment.

PART 1: NORMAL GROWTH AND PUBERTY 9
SITTING HEIGHT (CROWN RUMP LENGTH)
AND SUBISCHIAL LEG LENGTH
Sitting height should be measured whenthere appears to be disproportion between thetrunk and limbs or if there are any features tosuggest a skeletal dysplasia. An alternative tothe expensive Harpenden sitting height table isa narrow table positioned against the standingheight measuring equipment. The child sits onthe table with the back straight and flat againstthe wall, shoulders relaxed and legs hangingloosely from the edge of the table. The headshould be positioned as for standing height.Gentle upward pressure is applied behind themastoids and a headboard lowered to obtainthe reading. Subtracting the height of the tablefrom this value gives the sitting height. Subis-chial leg length is calculated by subtractingsitting height from the standing height. Thevalues for sitting height and subischial leglength can be interpreted by plotting them oncorresponding centile charts.
HEAD CIRCUMFERENCE
Head circumference is measured as themaximal occipito-frontal circumference. Anon-stretch tape measure should be used. Itshould encircle the head above the ears,midway between the eyebrows and the hairline,and over the occipital prominence at the back ofthe head. The value should be recorded in centi-metres and to the nearest millimetre.
Testes 4 mL
Testes andpenile growth
Shavingfacial hair
Breast buds
BODY MASS INDEX
Body mass index (BMI) provides a crudeestimate of adiposity and should be calculatedif a child appears overweight or weight is ona higher centile compared to height on agrowth chart. It is calculated from weightand height:
BMI in kg=m2 ¼ weight in kgOheight in m2
BMI should be plotted on age specific referenceranges, if locally available.
Pubertal Staging
Assessment of pubertal development isimportant when there are concerns aboutpuberty and is also essential when there areany concerns about growth. There is consider-able normal variation in the timing and pacewith which physical changes and the growthspurt occur during puberty. However, thesequence of events remains fixed (Figure 1.6).Assessing pubertal status entails obtaininga history as well as physical examination usingTanner’s stages (Figure 1.7). Enquire about thetiming of events such as start of breast develop-ment, voice breaking, growth spurt and startingto shave facial hair. However, the history maynot correspond with examination findings.Early breast development in girls and thechanges in testicular volumes in boys are subtleand may go unnoticed.
Menarche
FIGURE 1.6 The sequence ofphysical changes during puberty inrelation to the growth spurt.

FIGURE 1.7 Tanner stages of pubertal development in (A) girls and (B) boys. Reprinted with permission from Carel J-C,
Leger J. Precocious Puberty. New Engl J Med 2008;358:2366e77.
1. GROWTH: IMPORTANCE AND IMPLICATIONS OF VARIATIONS10
Onset of and rate of change of some featuresof puberty differs markedly between differentethnic groups. For example, pubic hair devel-opment in children of Chinese or Vietnameseorigin can be minimal until an otherwise latestage of puberty, in comparison with a childof Mediterranean or Middle Eastern origin,where onset of pubic hair is an early featureof puberty.
Peak height velocity occurs relatively early ingirls, usually before age 12 years and beforemenarche. Following menarche, height velocityslows down and the child reaches a near-finaladult height in another 2 years. The averageage of menarche in girls in the UK and in mostWestern countries is around 13 years. There isa trend to earlier menarche in most populations,the reasons for which are not fully clear. It ispossible that an improved nutritional statusmay be partly responsible for this trend. Inboys, peak height velocity occurs on averagebetween 13 and 14 years. At this time, testicularvolumes are between 10 and 12 mL. The laterpubertal growth spurt translates to taller staturein boys compared to girls.
Clinical Examination
Specific growth concerns and potential expla-nations or differential diagnoses for these deter-mine the focus of the clinical examination. Both
general and systemic examination can providevaluable clues. For example, in a child withconcerns about short stature, general examina-tion needs to focus on:
• head, face and neck for dysmorphic features(as in Turner or Noonan syndrome)
• limbs, hands and feet for unusualappearances (e.g. Madelung deformity inSHOX haploinsufficiency ordyschondrosteosis; abnormal thumbs inFanconi anaemia)
• disproportional length measurementsbetween the limbs and trunk, other skeletalabnormalities suggestive of skeletaldysplasias
• weight centile and subcutaneous fat inrelation to height centile (e.g. truncaladiposity in growth hormone deficiency)
• features to suggest deficiencies of growthhormone, thyroxine, cortisol or sexsteroids.
In addition, systemic examination willinclude identifying any systemic illness, cardiacdefects and neurodevelopment problems.
BONE AGE
Bone age is used to assess skeletal maturityand growth potential. Bone age is assessedfrom the appearances of epiphyses, usually

PART 2: VARIATIONS IN LINEAR GROWTH 11
froma radiographof thenon-dominant handandwrist. Since epiphyses determine linear growth,bone age reflects bone maturation and correlatesbetter with linear growth than chronological age.A number of methods are available for deter-mining bone age. In the Greulich and Pylemethod, using photographic reproductions ofhand X-rays, the individual ossification centresare compared with published age-matched stan-dards derived from healthy children. In the Tan-nereWhitehouse 2 or 3 (TW2 or TW3) method,the maturity of each epiphyses is scored anda bone age is derived from the total score.
Bone age is an important component ofgrowth assessment as many growth disordersare accompanied by a delay in bone maturation,particularly hypothyroidism, growth hormonedeficiency and pubertal delay. However, thebone age results can be subjective and may notbe accurate, particularly in those under 5 yearsof age. Nonetheless, bone age X-rays are readilyavailable and serve as a useful additional tool ingrowth assessment.
PART 2: VARIATIONS IN LINEARGROWTH
Short Stature and Growth Failure:Definition and Implications
Short stature can be a normal variant in somechildren and a symptom of underlyingpathology in others. Although a height lessthan two standard deviations below the meanfor age and gender at a single point, irrespectiveof a child’s growth rate and/or ethnic origin, isfrequently used as an arbitrary cut-off, this isnot an absolute definition of short stature.
For an individual, the definition of shortstature requires taking into consideration thestage of pubertal development, parents’ heights,ethnic background and the growth performanceof the reference population. For example, achild with height on the 2nd centile would be
considered to be short if the midparental heightwere on the 50th centile. However, if the mid-parental height were on the 9th centile, thischild would be relatively short for the referencepopulation but not short for parents’ heights.Conversely, a child with height on the 50th cen-tile would not be considered short for the refer-ence population but would be short for parentsif midparental height were on the 98th centile.
Growth failure or faltering growth impliesthat a child fails to grow at a normal heightvelocity. This is independent of initial heightand is not restricted to children who are short.By this definition, a boy whose height was onthe 85th centile at 6.5 years and 50th centile at8 years would have faltering growth despiteboth height measurements being within the’normal’ range. This pattern of growth isusually pathological and warrants carefulevaluation. It would not be appropriate tomake any sensible assessment of a child’sheight without plotting the midparental heighton the growth chart and thus placing the childin the context of the family. Whenever pos-sible, parental heights should be included inassessment.
School age children and adolescents who areshort may have a negative perception abouttheir physical appearance and may suffer morepsychosocial limitations than physical disabil-ities. They can experience feelings of depres-sion, anxiety, bullying at school and socialisolation leading to behavioural problems,poor interpersonal skills, low academic perfor-mance and a poor quality of life. The physicalimpact of short stature depends on the aetiologyand may include interference with independentactivities of daily living such as opening doors,reaching objects, gaining access to public trans-port or even problems with walking if lowerlimb deformity is present. Some conditionsmay be associated with chronic pain whichmay further limit activity and increase distress.These problems need to be recognised andappropriate support provided.

1. GROWTH: IMPORTANCE AND IMPLICATIONS OF VARIATIONS12
Clinical Classification of Short Stature
Short stature can be broadly classified accord-ing to the dominant clinical feature (Table 1.5).
Epidemiology of Short Stature
A height measurement more than two stan-dard deviations below the mean is onlyexpected in 2.5% of healthy children accordingto the Empirical Rule. Thus, the shorter the childthe greater the likelihood of organic disease(Table 1.6).
Clinical Assessment of a Child withShort Stature
It is important to consider common condi-tions in the population that may be associatedwith short stature. These include chronicmalnutrition and energy deficiency in manydeveloping countries. Chronic illnesses such asrecurrent malaria, haemolytic anaemia, giardi-asis and intestinal worm infestations should beexcluded first before considering rarer condi-tions such as coeliac disease, cystic fibrosis andinflammatory bowel disease. Endocrine causesof short stature are relatively rare, but notimpossible. These include examples presentedin Table 1.6, such as growth hormone deficiency,Turner syndrome and glucocorticoid excess.
Therefore, specific history and examinationin children with short stature should be focusedon likely causes, as follows:
• Maternal nutrition, birth size and history ofpoorgrowth in utero (small forgestational age).
• Postnatal events: prolonged jaundice(congenital hypothyroidism, congenitalhypopituitarism), neonatal hypoglycaemia(congenital hypopituitarism), floppiness withfeeding difficulties (PradereWilli syndrome),puffy hands and feet (Turner syndrome).
• A detailed medical history for features ofchronic energy deficiency and chronicsystemic illness, recurrent infections
(malaria, respiratory tract infections, urinarytract infections, gastroenteritis), bloodtransfusions (haemolytic anaemia), problemswith hearing, vision, speech and learning;treatments such as corticosteroids.
• Family history of consanguinity, similarcondition in a family member, parents andsiblings’ height and puberty.
• General examination: head size, bodyproportions, evidence of malnutrition, signsof chronic systemic illness,hepatosplenomegaly (chronic haemolyticanaemia), dysmorphic features, midlinedefects, visual defects.
SPECIFIC CONDITIONSPRESENTING WITH SHORT
STATURE AND GROWTH FAILURE
Familial short stature and constitutionaldelay in puberty are the most common physio-logic causes of short stature when nutrition isadequate and general health is satisfactory.They must be considered in the context of anyshort child presenting for assessment and mayindeed be part contributors where a pathologiccause also exists.
Undernutrition
Undernutrition, usually secondary to proteincalorie malnutrition, is the most importantcause of short stature worldwide, is usuallyaccompanied by mineral and vitamin defi-ciencies and is associated with pubertal delay,aggravating the problem of short stature. Itspresence can be assessed as a low weight forheight as well as low weight for age and sex-matched peers. Short stature due to undernutri-tion is complicated by zinc deficiency whichalone can cause short stature and delayedpuberty. It results in low IGF1 and has beenconsidered as an adaptive mechanism for anenergy-restricted environment.

TABLE 1.5 Clinical Classification of Short Stature According to Dominant Clinical Feature
Growth failure
Endocrine disorder
Small for gestational
age
Dysmorphic features in
face and/or limbs
Disproportion between
trunk and limbs
Chronic systemic
disease
Apparently healthy,
normal looking and
growth rate normal for
stage of puberty
Hypothyroidism
• Growth
hormone
deficiency
• Corticosteroid excess
• Primary IGF-I
deficiency
Normal or apparently
large head (preserved
head size)
• Intrauterine
growth
retardation
(RusselleSilver
syndrome)
• 3-M syndrome
Small head
• Fetal alcohol
spectrum
disorder
• Fanconi
syndrome
Girls
• Turner syndrome
• SHOX deficiency
(LerieWeill
dyschondrosteosis or
Langer mesomelia)
Girls or boys
Noonan syndrome
Down syndrome
PradereWilli syndrome
Boys
• Aarskog syndrome
• Short limbs
• Skeletal dysplasia:
hypochondroplasia,
achondroplasia
• Rickets
Short limbs/back
• Muco-
polysaccharidosis
Overt features
• Malnutrition
• Chronic
infection
• Chronic renal failure
• Cyanotic
congenital
heart disease
• Juvenile
chronic
arthritis
Silent or asymptomatic
Coeliac disease
Chronic
inflammatory
bowel disease
Renal tubular
defects
Bone age not
delayed and
parents short
• Familial short stature
• Bone age delayed
• Constitutional delay in
growth
and puberty
SPECIFIC
CONDITIO
NSPRESENTIN
GWITH
SHORT
STATUREAND
GROWTH
FAILURE
13

TABLE 1.6 Estimated Frequency of Short Stature and Organic Cause to Indicate the Scale of these Problems inWestern Settings
Criteria Frequency Population
Height below 3rd centile 1 in 80 14,346 Prepubertal children at school entry in theUK [Voss. BMJ 1992]
Height below 3rd centile and heightvelocity less than 5 cm/year
• Endocrine disorder
• Systemic illness
• CDGP and FSS
1 in 20
5%
10%
75%
114,881 Elementary school age children in USA[Lindsay. J Pediatr 1994]
GHDCDGPFSSTurner syndromePrimordial short stature
10%8%04%2%
49 Prepubertal short children with height morethan e2.5 SD below the mean and referred forevaluation of short stature [Moore. J. Pediatr. 1993]
Notes: CDGP e constitutional delay in growth and puberty; GHD e growth hormone deficiency; FSS efamilial short stature.
1. GROWTH: IMPORTANCE AND IMPLICATIONS OF VARIATIONS14
Chronic Disease
Many disorders of chronic illness result inshort stature and frequent but not inevitablepubertal delay. Those disorders associatedwith malabsorption in the upper gastrointes-tinal tract are more likely to cause slow growth,due to a combination of poor nutrition, neces-sary medications such as corticosteroids and toactive inflammation with high inflammatorycytokines.
In countries where access to healthcare maybe limited by distance, financial constraint orlack of knowledge concerning normal growth,other conditions commonly interfere withnormal growth. These include cardiac disease,chronic anaemia and vitamin deficiency, chronicasthma, liver and renal disease.
Type 1 diabetes mellitus with chronic poorcontrol, due to lack of access to or use ofadequate insulin, results in Mauriac syndrome,characterised by severe growth failure, thick-ened skin and hepatosplenomegaly.
Coeliac disease may be a hidden cause ofgrowth failure, with very few or no symptoms
after infancy, other than growth and pubertalfailure.
Intrauterine Growth Retardation andSmall for Gestational Age
Most intrauterine growth retardation (IUGR)worldwide is due to problems of maternal nutri-tion, particularly in the first trimester of preg-nancy. There are multiple factors operative,including protein calorie malnutrition, vitamindeficiencies, smoking and intrauterine infec-tions. Epigenetic programming is now wellestablished to occur as a result of maternal andfeto-placental factors, with long-term and some-time transgenerational adverse effects on thefetus and child. Some of these effects can bedelayed in expression to the second and thirddecade of life. A strong association is seenbetween past IUGR, metabolic syndrome andearly ischaemic heart disease, diabetes mellitus,and hyperlipidaemia. Reduced fertility due tomultiple hormone resistance may also occur.
The major challenge to be met is to reducematernal factors predisposing to this condition.

SPECIFIC CONDITIONS PRESENTING WITH SHORT STATURE AND GROWTH FAILURE 15
Education and service availability need tofocus on access to better antenatal care andimproved peri-conceptual maternal nutritionand support.
RusselleSilver Syndrome
Characteristic Features
The RusselleSilver syndrome (RSS) isa particular condition within the IUGR range.The estimated incidence is 1 in 3000 to 100,000.
RSS is a heterogeneous condition character-ised by some or all of the following features:
• severe prenatal and postnatal growth failure• feeding difficulties from birth• short stature and no disproportion between
trunk and limbs• poor weight gain• hemi-atrophy resulting in limb length
asymmetry• normal head circumference and large
forehead; head appears relatively large incomparison to face and body
• small triangular lower face, narrow chin,small jaw, downturned corners of themouth
• clinodactyly• pubertal onset at normal age which
contributes to compromised adult height• cafe-au-lait patches.
Diagnosis is usually clinical and can beconfirmed by gene testing.
Genetics of RusselleSilver Syndrome
About 40% of cases are sporadic. Abnormali-ties in the imprinted genes on chromosomes 7and 11 have been identified in some cases andinclude:
• loss of paternal methylation of the centraltelomeric imprinting centre region I (ICR1)on chromosome 11p15 which disrupts theregulation of H19 and IGF-II (up to 60%reported)
• maternal uniparental disomy of chromosome7 and therefore absence of the genes that arenormally active on the paternal copy ofchromosome 7 (7%).
Management
Untreated average adult height is 140 cm forfemales and 150 cm for males. Growth hormonetreatment is beneficial in improving childhoodlinear growth, where available.
Endocrine Disorders: Hypothyroidism
Causes
• Undiagnosed congenital hypothyroidismin countries where there is no neonatalscreening programme: untreated severecongenital hypothyroidism is likely tohave a significant impact onneurodevelopment and is unlikely topresent with short stature in the absenceof other features. However, in those withmild and previously compensatedcongenital hypothyroidism, short staturemay be a presenting feature. Intellectualdevelopment may be normal if theunderlying problem is of a lingualthyroid, where sufficient thyroxine hasbeen produced to protect the brain in thefirst 2 years of life. In later childhood,thyroid function may becomedecompensated to cause significant shortstature.
• Acquired hypothyroidism:
e autoimmune due to Hashimoto’sthyroiditis
e iodine deficiency
Characteristic Features of Hypothyroidism
These include:
• growth failure• relatively overweight for height

1. GROWTH: IMPORTANCE AND IMPLICATIONS OF VARIATIONS16
• lack of concentration and poor schoolperformance may be present but the childmay apparently be seen as a diligent student,conforming to rules but being methodicallyslow.
Classical features of lethargy, tiredness,sleepiness, cold intolerance, mottled skin, con-stipation, coarse features, hoarse voice, slowpulse, goitre and delayed relaxation of deeptendon reflexes are seen less commonly as isdelayed bone age which may be severe if thehypothyroidism is congenital.
Investigations When Hypothyroidism isSuspected and Management
These include:
• blood samples for thyroid function (TSH, freethyroxine) and thyroid antibodies
• replacement with levothyroxine anddose adjusted according to clinicalresponse and regular monitoring of thyroidfunction.
(See Chapter 3, Thyroid Disorders, for details.)
TABLE 1.7 Organic Causes of Growth Hormone Deficien
1. Congenital e associated with developmental abnormalities of the h
early childhood
Eye features such as nystagmus, squint, impaired vision: septo-opti
Other midline brain and facial abnormalities: holoprosencephaly, si
2. Defects in genes necessary for pituitary development and function
Isolated familial GHD
• Severe short stature and autosomal recessive: GH1 defects
• Moderate short stature and autosomal recessive or dominant: G
• Short stature with agammaglobulinaemia and X-linked recessiv
• Combined pituitary hormone deficiency
• PIT1/POU1F1, PROP1, LHX3, LHX4, HESX1, SOX3, SOX2, GLI
3. Acquired
Tumours within the hypothalamic-pituitary axise craniopharyngiom
Cranial irradiation e leukaemia, medulloblastoma, astrocytoma/gli
Trauma to the hypothalamus/pituitary e perinatal or postnatal
Infiltration e Langerhans cell histiocytosis
Central nervous systems infections
Endocrine Disorders: Growth HormoneDeficiency
Growth hormone (GH) is secreted from theanterior pituitary gland in a pulsatile manner.Its secretion is controlled by the hypothalamusthrough an interaction between its releasinghormones, GHRH and ghrelin, and the inhibi-tory hormone somatostatin. GH secretion is alsoregulated by insulin-like growth factor (IGF-1).
Causes of Growth Hormone Deficiency
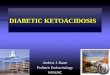
Growth hormone deficiency (GHD) can bebroadly classified into congenital or geneticconditions and acquired defects (Table 1.7).Although the aetiology remains obscurein many cases of isolated GHD, abnormal pitu-itary morphology may be seen on MRI(Figure 1.8).
Clues from the History that Suggest GrowthHormone Deficiency
• Neonatal history: hypoglycaemia, prolongedjaundice, microphallus.
cy
ypothalamus/pituitary, characterised by presentation in infancy or
c dysplasia and optic nerve hypoplasia
ngle central incisor, cleft lip/palate
H1 or GHRHR defects
e
2, GLI3
a, germinoma, teratoma
oma, ependymoma, nasal rhabdomyosarcoma

FIGURE 1.8 MRI scan showing small anterior pituitary,absent stalk and ectopic posterior pituitary.
SPECIFIC CONDITIONS PRESENTING WITH SHORT STATURE AND GROWTH FAILURE 17
• Breech delivery: a high incidence reported inretrospective studies, up to 65%.
• Childhood history: head injury, infection,cranial irradiation.
• Family history: consanguinity, severe shortstature.
• Symptoms suggesting intracranial lesion:headache, vomiting, visual loss e up to 25%.
• Craniofacial and midline abnormalities:nystagmus, squint, visual impairment, opticnerve hypoplasia, cleft lip/palate, singlecentral incisor.
• Other causes of short stature and growthfailure excluded (e.g. small for gestationalage, hypothyroidism, chronic systemicdisease, Turner syndrome, skeletaldysplasia).
Clinical Features of Growth HormoneDeficiency
These include:
• short stature, frequently below -3 SD forreference population, but no disproportionbetween the trunk and limbs
• growth failure and progressive decline inheight velocity
• high-pitched voice• cherubic face with crowding of mid-facial
structures• normal head circumference and frontal
bossing• delayed dentition• chubbiness with more subcutaneous fat
compared to muscle bulk• anterior abdominal adiposity with dimpling
of fat• small phallus (where gonadotrophin
deficiency is co-existent)• delayed bone age• delayed puberty• any associated features to suggest an
acquired cause, e.g. visual loss, diabetesinsipidus.
Investigations When Growth HormoneDeficiency is Suspected
These tests may not be available but anattempt to make a definite diagnosis of GH defi-ciency should be undertaken for the followingreasons:
• to investigate for a possible brain tumour asa cause for pituitary dysfunction
• if there is any consideration for use of GHtreatment.
Investigation with dynamic growth hormonetesting should be considered when a child isshort, below the 3rd centile, growing slowly,fallingawayfromthegrowthcurve,withagrowthvelocity less than the 25th centile for bone age,with associated risk factors as above and withoutany features to suggest a chronic disease.
If the growth velocity is normal and an IGF1is normal for age-matched peers, dynamictesting may not be required. However, on itsown, neither a normal growth velocity nor anIGF-I in the normal range would sufficientlyexclude the diagnosis of growth hormonedeficiency.

1. GROWTH: IMPORTANCE AND IMPLICATIONS OF VARIATIONS18
To diagnose GHD:
• Single random plasma IGF-1 and IGFBP3levels: In the absence of undernutrition, lowlevels (below -2 SD) for gender, age and stageof puberty strongly support GHD but normallevels do not exclude it.
• GH stimulation tests: As GH is secreted ina pulsatile manner, GH measured fromsingle random blood samples cannot beinterpreted. GH secretion can be stimulatedby exogenous agents such as arginine,which reduces endogenous inhibitorysomatostatin tone. Glucagon injections maylower blood glucose levels and also havea direct stimulatory effect on GH release.Insulin is a powerful stimulant of GHsecretion and acts by inducinghypoglycaemia. However, hypoglycaemiamay be dangerous and hence the insulintolerance test should only be considered ifadequate medical supervision is available.Other agents that are less commonly usedto test GH secretion includepyridostigmine, clonidine, levodopa andpropranolol. Although useful, GHstimulation tests are never a ’gold standardtest’ and can be biased by false positive andfalse negative results. Peak GH levels canbe falsely low in children who areperipubertal and those who are overweight.Children older than 8 years who areprepubertal or in early puberty should haveGH stimulation tests after sex steroidpriming (testosterone 100 mg intramuscular3e9 days before the test in boys; ethinyloestradiol 10 mg daily for 3 days issometimes used in girls). Twopharmacological stimulation tests arerecommended in patients suspected to haveisolated GHD and one test in those withacquired pathology, multiple pituitaryhormone deficiencies or genetic defects.
To identify whether GHD is isolated orassociated with other pituitary hormone
deficiencies, the following tests are recommen-ded in order of usefulness to the patient:
• Thyroid function tests including both freeT4 and TSH.
• A TRH test (measurement of TSH followinginjection of TRH) might help if available butis not essential for diagnosis. A low fT4without rise in TSH will usually providesufficient information.
• 8 am cortisol levels. Similarly, a low cortisolwithout rise in ACTH may be helpful. TheACTH level is less likely to be available and isof less value. The standard dose synacthentest (measurement of cortisol following aninjection of synthetic ACTH) can be used todetect whether the adrenal has not beenstimulated for a prolonged time and istherefore unable to respond. It does notdifferentiate between primary and secondaryhypo-adrenalism in the absence of an ACTHlevel.
• Plasma urea and electrolytes; plasma andurine osmolality in the morning afterovernight fast (food and water) will definemany cases of diabetes insipidus of centralaetiology. The presence of diabetes insipidusmay indicate a space-occupying lesion in thehypothalamic-pituitary area.
• Basal FSH and LH levels; and a GnRH testmay be of some use in an adolescent or inearly infancy but are of no value at all in mid-childhood as the gonadal axis is quiescentand stimulated gonadotrophin levels will benormally low. Time of onset into puberty andnormality of pubertal progress as physicalfeatures are far more useful for evaluating thehypothalamic-pituitary-gonadal axis.
• Prolactin level might be of minor interest ifthere has been a tumour or radiation to thehypothalamus but is unlikely to be diagnosticexcept if a prolactinoma is suspected as thecause for growth failure. In rare cases,children with Pit1 gene defects may havevery low prolactin levels.

SPECIFIC CONDITIONS PRESENTING WITH SHORT STATURE AND GROWTH FAILURE 19
To define the cause of GHD the followingare needed:
• Neuroradiological evaluation with magneticresonance imaging (MRI) of thehypothalamic-pituitary region: hypoplasticanterior pituitary, interrupted or hypoplasticstalk, ectopically placed posterior lobe(Figure 1.8).
• WhereMRI is not available, CTwith a requestto focus on the hypothalamic-pituitary areamay help but definition is less satisfactory. Alateral skull X-ray will demonstrate sellarerosion or enlargement, if that is the onlyavailable test.
• Other MRI findings may help define midlinelesions. These include midline abnormalitiessuch as: optic nerve/chiasm hypoplasia,which can be detected by a goodophthalmologic assessment. An MRI isrequired to demonstrate absent septumpellucidum and abnormalities in the corpuscallosum, often present in the septo-opticdysplasia spectrum.
• Genetic studies in patients with isolatedfamilial GHD, if facilities exist.
Management of Growth HormoneDeficiency where Available
Children with GHD need replacement dosesof recombinant human GH (rhGH) (25e50mg/kg/day or 0.7e1 mg/m2/day). Dosesshould be adjusted according to the growthresponse and IGF-I levels maintained in thenormal range. Final height outcome is betterwith younger age at start of treatment, longerduration of treatment, smaller height deficitat start of treatment and greater catch-up inheight in the first year of treatment. rhGH iscontinued until near-final height (HV lessthan 2 cm/year) when GH secretory statusshould be reassessed to identify patients likelyto benefit from continuing rhGH replacementinto adulthood.
Hypopituitarism (Combined PituitaryHormone Deficiencies)
Hypopituitarism or combined pituitaryhormonedeficiencies is defined as adeficiency oftwo or more pituitary hormones. Deficiency ofall anterior and posterior pituitary hormones isreferred to as panhypopituitarism.
Causes of Hypopituitarism
The congenital and acquired causes ofgrowth hormone deficiency (Table 1.7) can alsocause hypopituitarism. Genetic defects thataffect pituitary development and differentiationinclude mutations in the transcription factorsPROP1 (deficiency of all anterior pituitaryhormones) and PIT1 (deficiency of GH, TSHand prolactin).
Clinical Features of Hypopituitarism
The age at presentation and the spectrum ofclinical features are determined by the under-lying cause and hormone deficiencies. Somato-trophs appear to be most vulnerable and arefollowed by gonadotrophs, thyrotrophs andcorticotrophs. Thus GH deficiency is mostcommon and is followed by deficiency of LHand FSH, TSH and finally ACTH. The numberof hormone deficiencies can evolve as the childgets older. This means that children with hypo-pituitarism can develop additional hormonedeficiencies at any age and therefore requireregular follow-up and re-evaluation of pituitaryfunction.
Congenital hypopituitarism presents in theneonatal period often with non-specific (leth-argy, poor feeding, poor weight gain) features.These include:
• symptoms of hypoglycaemia (jitteriness,apnoea, convulsions)
• jaundice which may be prolonged(unconjugated due to TSH deficiency andconjugated due to ACTH deficiency)

1. GROWTH: IMPORTANCE AND IMPLICATIONS OF VARIATIONS20
• undescended testes, underdevelopedscrotum and micropenis.
Congenital hypopituitarism can be associ-ated with a history of breech or traumaticdelivery. Some cases are secondary to defi-ciencies in embryonic pituitary transcriptionfactors, as outlined in Table 1.8.
A particular form of hypopituitarism in earlylife is septo-optic dysplasia. Unlike congenitalhypopituitarism, children with septo-optic dys-plasia may develop central diabetes insipidusandare thereforeprone todehydrationandhyper-natraemia. The spectrum and severity of clinicalfeatures is wide and includes the following.
• Optic nerve hypoplasia e this is identified byophthalmoscopy. The eye manifestationsrange from normal vision to total blindnessand can be associated with nystagmus andsquint. The intracranial part of the opticnerve is best visualised on MRI scanning.
• Pituitary hormone deficiencies e these aremore likely in children with anatomicalabnormalities of the pituitary gland and otherstructures in the brain including the corpuscallosum and septum pellucidum.
• Other midline brain abnormalities (thincorpus callosum and absent septumpellucidum).
TABLE 1.8 Clinical Classification of GH Insensitivity
1. Congenital GH insensitivity
Normal birth weight and normalhead circumference
Small for gestationhead
GH receptor defects
• Low GHBP: mutation in
extracellular domain
• Normal or high GHBP: mutation
in intracellular domain
GH signalling defects
• STAT5B
• Noonan syndrome: PTPN11
• Low IGF-I and l
difficulties: IGF-
• High IGF-I: IGF-
• Epilepsy e due to a more global brainabnormality in severe septo-optic dysplasia.
During childhood, hypopituitarism shouldbe suspected in any child with poor lineargrowth and clinical features suggestive ofhypothyroidism with or without adrenal insuf-ficiency. An additional clue during adolescenceis delayed puberty. Craniopharyngiomas arethe commonest hypothalamic tumours of child-hood that cause hypopituitarism. They aredevelopmental tumours which arise fromremnants of the Rathke’s pouch and are charac-teristically slow growing. They usually presentin school-age children and teenagers but canpresent at any age. The clinical features of cra-niopharyngiomas and other tumours close tothe pituitary and hypothalamus are due to:
• compression of the pituitary gland and thuspituitary hormone deficiencies
• compression of the hypothalamus edisturbance of appetite and excessive weightgain; hypothalamic dysfunction can alsocontribute to pituitary hormone deficiencies
• compression of optic chiasm with defects invisual fields and visual acuity
• raised intracranial pressure e morningheadaches, vomiting and cranial nerve palsy(6th nerve).
2. Acquired GH insensitivity
al age, small • Malnutrition
• Chronic inflammation
• Liver disease and other chronic
systemic diseases
• Severe infections
earning
I gene defects
I receptor defects

SPECIFIC CONDITIONS PRESENTING WITH SHORT STATURE AND GROWTH FAILURE 21
Investigations for SuspectedHypopituitarism
Depending on the availability of laboratoryand radiological facilities, investigations shouldbe directed to:
• assess the spectrum of anterior and posteriorpituitary hormone deficiencies (see sectionon growth hormone deficiency)
• identify intracranial pathology andanatomical abnormalities of the pituitary andbrain.
Management of Hypopituitarism
The principles of management of hypopitu-itarism are to:
• replace the hormones that are deficient and• treat the underlying cause (such as a tumour)
when possible.
When there are multiple pituitary hormonedeficiencies, glucocorticoid replacement mustbe prioritised before replacing thyroxine andgrowth hormone. For guidance on hormonereplacement, see the sections on GH deficiency,gonadotrophin deficiency, hypothyroidism,adrenal insufficiency and central diabetesinsipidus.
Growth Hormone Insensitivity
Definition
Children with congenital GH insensitivity areexceptionally short and have clinical featuressimilar to GHD. However, they differ fromGHD in that they have high GH levels to stimu-lation tests. They do not respond to GH treat-ment and the availability of recombinanthuman IGF-I makes this the treatment of choice.
Classification of GH Insensitivity Based onClinical and Biochemical Features
GH insensitivity can be either congenital oracquired (Table 1.8).
Cushing Syndrome
The mechanisms by which excess exogenousor endogenous corticosteroids lead to growthimpairment are complex and include disruptionof the GHeIGF axis at various levels, directeffects on the epiphyseal growth plate, andinhibitory effects on gonadotrophin secretionand adrenal steroid production.
Causes
• Exogenous: iatrogenic secondary to long-term treatment with pharmacological dosesof corticosteroids as immunosuppressive andanti-inflammatory agents, for example forasthma and nephrotic syndrome.
• Endogenous: adrenal pathology, excesspituitary ACTH secretion (Cushing’s disease)and non-pituitary ectopic ACTH syndromeeall rare in childhood.
Characteristic Features of CushingSyndrome
These include growth failure, excessiveweightgain and obesity, tiredness, lack of energy, behav-iour and sleep problems, truncal obesity andnuchal fat pad, rounded plethoric face, thinskin, striae, easy bruising, hirsutism, hyperten-sion, proximal muscle weakness and delayedmotormilestones, delayedbone age, osteopaenia.
The diagnosis of Cushing syndrome is relianton the demonstration of excess cortisol secretiondue to altered circadian rhythmicity. In addi-tion, in children with Cushing’s disease, wherethe lesion is due to a pituitary adenoma,ACTH levels are high, but suppressible withhigh-dose dexamethasone. The specific investi-gations for Cushing syndrome are outlinedelsewhere in this book. (See Chapter 4, AdrenalDisorders.)
Management of Cushing Syndrome
Management depends on the cause ofCushing syndrome and includes both medical

1. GROWTH: IMPORTANCE AND IMPLICATIONS OF VARIATIONS22
and surgical options. Specialist advice isrecommended.
Turner Syndrome
All girls with Turner syndrome do not havethe classical textbook features. Therefore Turnersyndrome should be considered in any girl pre-senting with short stature as well as in anyadolescent girl presenting with delayed orarrested puberty. The diagnosis of Turnersyndrome is confirmed by peripheral bloodlymphocyte karyotyping. The estimated inci-dence is 1 in 2500 live female births and there-fore relatively common.
Treatment with growth hormone is beneficialin improving adult height. A woman withTurner syndrome is on average 20 cm shorterthan other adult women and untreated finaladult height is 136e147 cm.
(See Chapter 2, Puberty, for details.)
Noonan Syndrome
Characteristic Clinical Features
Some of the characteristic clinical features ofNoonan syndrome resemble Turner syndrome.However, Noonan syndrome affects boys aswell as girls. The estimated incidence is 1 in1000 to 2500 live births.
Features include:
• short stature and growth failure• delayed puberty• facial dysmorphism with ptosis,
hypertelorism, downward-slanting eyes,low-set abnormal ears, grooved philtrum,broad nasal tip
• neck webbing• pectus carinatum often with combined
pectus excavatum• cardiac abnormalities: pulmonary valve
stenosis (PS), atrial septal defect (ASD),ventricular septal defect (VSD), patent ductus
arteriosus (PDA), hypertrophiccardiomyopathy
• undescended testes• mild learning difficulties which are
sometimes due to or compounded byunrecognised hearing or visual problems
• bleeding tendency due to one or more defectsof the coagulation cascade important.
The genetics of Noonan Syndrome
Mutations in a number of genes on differentchromosomes have been identified in childrenwith Noonan syndrome. The most commondefect is found in the PTPN11 gene on chromo-some 12q and is inherited as autosomal domi-nant. Other genes involved include:
• KRAS e more severe form of the disease• RAF1 e dilated cardiomyopathy• SOS1 e heart defects• NFNS e neurofibromatosis-like features.
Management
The diagnosis is essentially clinical. Genetictesting, where available, can provide confirma-tion. Growth hormone treatment can be usedto improve linear growth in childhood but haslittle effect on adult height achieved. Somestudies suggest modest increments in height inthe short term. However, long-term studies donot show convincing evidence to justify growthhormone treatment in children with Noonansyndrome. Moreover, some forms of theNoonan syndrome spectrum, such as Costellosyndrome, are prone to malignancy. In suchcases, growth hormone treatment may not beadvisable.
Recognition and identification of a bleedingdisorder is important particularly in girls withNoonan syndrome. The problems are of oozingblood loss in an exposed area of tissue such asafter tooth extraction or birth. Postpartum hae-morrhage is common and may result in theneed for an emergency hysterectomy. These

SPECIFIC CONDITIONS PRESENTING WITH SHORT STATURE AND GROWTH FAILURE 23
problems may be avoided if prior diagnosis ofa bleeding disorder has been established.
PradereWilli Syndrome
Characteristic Clinical Features
The estimated incidence is 1 in 15,000 and 1 in25,000 live births. Features include:
• short stature• floppiness and feeding difficulties from birth
and necessitating nasogastric tube feeding ininfancy
• failure to thrive infancy• voracious appetite emerges in childhood
between age 2 and 8 years. This is due to anabnormality in the secretion of ghrelin fromthe stomach. Ghrelin stimulates appetite andGH secretion.
• progressive obesity with greater fat masscompared to lean mass
• sleep disorders• characteristic facial appearance with almond-
shaped eyes and fair hair• small hands and feet• mild learning difficulties• speech delay• behavioural problems including skin self-
mutilation• scoliosis• small penis and undescended testes• delayed puberty.
The Genetics of Prader-Willi Syndrome
Anumber of genes in the region 15q11-q13 areaffected in PradereWilli syndrome. Normally,the paternal inherited genes in this region arefunctioning and maternal genes are switchedoff (this is called genomic imprinting). The pater-nally derived genes can be affected in a numberof ways:
• deletion of the critical part of the paternallyderived chromosome e 70% of cases
• maternal uniparental disomy when bothcopies of chromosome 15 are inherited fromthe mother e 25% of cases
• imprinting defect inherited from the fatherwhich affects functioning of the paternalgenes e 5% of cases.
Management
The diagnosis is essentially clinical. Genetictesting, where available, can provide confirma-tion. Without treatment, average final adultheight is about 154 cm in men and 145e159 cmin women. Growth hormone treatment can beused to improve linear growth and adult heightas well as to normalise body composition.
3-M Syndrome
Characteristic Features
3-M syndrome is an autosomal recessiveprimordial growth disorder characterised byprenatal and post growth restriction, significantshort stature, facial dysmorphism and promi-nent heels.
Genetics of 3-M Syndrome
A significant proportion of children with 3-Msyndrome have a genetic aetiologye genes suchas CUL7 and OBSL1, in growth hormone signal-ling pathways, have been implicated.
Management
Children with 3-M syndrome have relativeGH insensitivity with normal GH levels to stim-ulation tests and relatively low IGF-I levels.There is no significant improvement in lineargrowth with growth hormone treatment.
Skeletal Dysplasias
A skeletal dysplasia should be suspected inpatients who have disproportionate shortstature with unusually short limbs or short

1. GROWTH: IMPORTANCE AND IMPLICATIONS OF VARIATIONS24
trunk and a positive family history. The skeletaldysplasias are broadly classified based on theregion of bone involved such as epiphysis,metaphysis and diaphysis.
Hypochondroplasia and achondroplasia aremost common. These children grow normallybut fail to have a normal pubertal growth spurtdespite appropriate pubertal development. Asitting and standing height along with full skel-etal survey should be undertaken to confirmdiagnosis. There is no significant improvementin lineargrowthwith growthhormone treatment.
TALL STATURE
Definition and Implications
Asfor short stature, thedefinitionof tall statureis relative. Children who are above 99.6th centileand/or above their parental target centile rangeare considered exceptionally tall for the referencepopulation. Tall stature can have significantpsychosocial impact leading to low self-esteem,depression, social isolation and bullying.However, social perceptions around tall statureare not as negative as for short stature and ingeneral it appears to arouse considerably lessanxiety among individuals and their families.
TABLE 1.9 Clinical Classification of Tall Stature
Tall and normal
height velocity
Tall and increased
height velocity
Dysmo
no disp
trunk a
• Familial tall
stature if
parents tall
• Obesity
• Precocious puberty if prepubertal age
group and signs of puberty present
• Hyperthyroidism
• Familial glucocorticoid deficiency
• GH excess (very rare)
• Asym
Beck
synd
• Sym
Soto
Some children who are very tall in earlychildhood may have advanced bone age witha normal adult height outcome.
Assessment of any child who is unusually tallfor his or her family must consider pathologiccauses of excessive growth rate.
Clinical Classification of Tall Stature
Tall stature can be classified according to thedominant clinical features as shown in Table 1.9.
Clinical Assessment of a Child with TallStature
In addition to the history and examinationdetailed in Part 1, specific features useful inthe assessment of a child with tall statureinclude arm span, sitting and standing height,height velocity and pubertal staging.
Management of Tall Stature
Investigations and treatment should betailored according to the clinical diagnosis.Although high-dose oestrogen for girls andhigh-dose testosterone for boys has been usedto attenuate final height in pubertal age
rphic features and
roportion between
nd limbs
Characteristic features and
relatively long limbs
metrical overgrowth:
witheWiedemann
rome
metrical overgrowth:
s syndrome
Autosomal dominant, characteristicfeatures and normal intelligence
• Marfan syndrome
Learning and behaviour problems
• Klinefelter syndrome
• XYY boys
• Homocystinuria
Anosmia
• Gonadotrophin deficiency

SPECIFIC CONDITIONS PRESENTING WITH TALL STATURE 25
children, the side effects and possible adverselate effects of therapy should be borne in mindas these may outweigh the benefits. Manycentres no longer offer treatment for tall stature,solely to hasten epiphyseal closure, althoughthere may be individual exceptions.
SPECIFIC CONDITIONSPRESENTING WITH TALL
STATURE
Idiopathic or Familial Tall Stature
Characteristics include:
• commonest cause of tall stature• one or both parents are tall• the child’s height is within the parental target
centile• bone age corresponds to the chronological
age• concordant pubertal growth.
Exogenous Obesity
In general, a child with exogenous obesitywill be tall compared to the midparental expec-tation but will have an advanced bone age, withrelatively early puberty resulting in normalisa-tion of adult height. Judicious weight reductionusually slows growth rate.
Endocrine Conditions
Precocious Puberty
Sudden onset of abnormal growth accelera-tion in comparison with siblings and peers,combined with pubertal changes, providesa diagnosis. Advanced bone age will variablyreduce final height.
Growth Hormone Excess
This is very rare in childhood, perhaps less sowhen associated with the McCuneeAlbright
syndrome. If an affected child has significantfacial changes due to sphenoid wing fibrousdysplasia and/or when gonadotrophin inde-pendent precocious puberty is also present,onset of GH excess can be extremely difficultto detect clinically. A high index of suspiciontogether with IGF1 levels and a glucose toler-ance test to measure growth hormone levelsare required, for diagnosis.
Klinefelter Syndrome
This may be suspected in a child who haslearning problems, social isolation, testicularmaldescent or in an adolescent with pubertalfailure or arrest gynaecomastia or behaviouralproblems. Unusually tall stature within thefamily may be seen.
(See Chapter 2, Puberty, for details.)
Marfan Syndrome
This should be suspected when there is anunusually tall child in a family, with some ofthe following features:
• A family history of early death or lensdislocation should be sought.
• Clinical assessment of arm span greater than5 cm more than the height, lower segmentgreater than the upper segment, long slenderfingers, upward and outwards dislocatedlens, high arched palate and pectusexcavatum or carinatum, among others.
• An important component of Marfansyndrome is aortic root widening, which hasa high risk for aortic dissection withprogressive dilatation.
Marfan syndrome is an autosomal dominantcondition due to a mutation in the fibrillin gene(FBN1) on chromosome 15q, but genetic confir-mation is rarely required. It is important toconsider the diagnosis of Marfan syndrome inchildren with tall stature, as progressive aorticroot dilatation may be prevented with cardiac

1. GROWTH: IMPORTANCE AND IMPLICATIONS OF VARIATIONS26
medication, such as b-blockers. It is prudent toseek a cardiac opinion if Marfan syndrome issuspected but not all physical signs are present.
A diagnostic tool based on the revised Ghentcriteria is available on the web site: www.marfan.org
Management
Management includes:
• annual echocardiographs irrespective of thecardiac involvement at the time of diagnosis
• b-blockers should be started for children toprevent aortic complications
• advice given not to take part in contact sports• annual eye assessment is recommended for
lens dislocation and or myopia• orthopaedic monitoring andmanagement are
indicated for kyphoscoliosis.
BeckwitheWiedemann Syndrome
Cardinal features include fetal macrosomia,neonatal hypoglycaemia secondary to hyperin-sulinism, which varies from mild and short-lived to extremely severe, hemihypertrophyand omphalocoele.
Early diagnosis is important for hypoglycae-mia management and for surveillance forincreased risk for Wilm’s tumour and adrenalcarcinoma.
Soto Syndrome or Cerebral Gigantism
This is an autosomal dominant conditionfrom a mutation in the NSD I gene on chromo-some 5q. Clinical features include intrauterineexcessive growth, large birth weight and growth
from infancy, large head and prominent fore-head, downward-slanting palpebral fissures,high arched palate, a long pointed chin, largehands and feet, scoliosis, developmental delay,and behavioural problems including attentiondeficit hyperactivity disorder (ADHD).
Advanced bone age is present. Children withthis condition may not be exceptionally tall asadults. No specific treatment is indicated.
References and Further Reading
Gluckman PD, Hanson MA, Cooper C, Thornburg KL.Effect of in utero and early-life conditions on adulthealth and disease. N Engl J Med 2008;359:61e73.Review.
Lindsay R, Feldkamp M, Harris D, Robertson J, Rallison M.Utah Growth Study: growth standards and the preva-lence of growth hormone deficiency. J Pediatr1994;125:29e35.
Moore KC, Donaldson DL, Ideus PL, Gifford RA, MooreWV. Clinical diagnoses of children with extremely shortstature and their response to growth hormone. J Pediatr1993;122:687e92.
Voss LD, Mulligan J, Betts PR, Wilkin TJ. Poor growth inschool entrants as an index of organic disease: theWessex growth study. BMJ 1992;305:1400e02.
Wit JM, Ranke MB, Kelnar CJH. ESPE Classification ofpaediatric endocrine diagnoses. Horm Res 2007;68(Suppl 2): S1-120.
Wit JM, Kiess W, Mullis P. Genetic evaluation of shortstature. Best Pract Res Clin Endocrinol Metab 2011;25:1e17.
Resources
The WHO Child Growth Standards. Available at URL:www.who.int/growthref/en/ (Growth reference chartsand tables for length/height, weight and BMI for chil-dren under age 5 years and age 5e19 years.)