Embed Size (px)
Citation preview

www.emwa.org Volume 26 Number 4 | Medical Writing December 2017 | 5
Jennifer HonekHonek Communications Consulting & MedicalWriting, Stockholm, Sweden
Correspondence to:Honek Communications Consulting & Medical WritingStockholm, [email protected]
AbstractThe process of developing a novel drug is timeconsuming and costly. To increase thechances of successfully completing a clinicaltrial leading to the approval of a new drug, thechoice of appropriate preclinical models is ofutmost importance. Identifying a safe, potent,and efficacious drug requires thoroughpreclinical testing, which evaluates aspects ofpharmacodynamics, pharmacokinetics, andtoxicology in in vitro and in vivo settings.Nevertheless, merely a small fraction ofinvestigational new drugs tested in clinicaltrials after passing preclinical evaluationeventually lead to a marketed product. Hence,there is a need for optimising current standardpreclinical approaches to better mimic thecomplexity of human disease mechanisms.
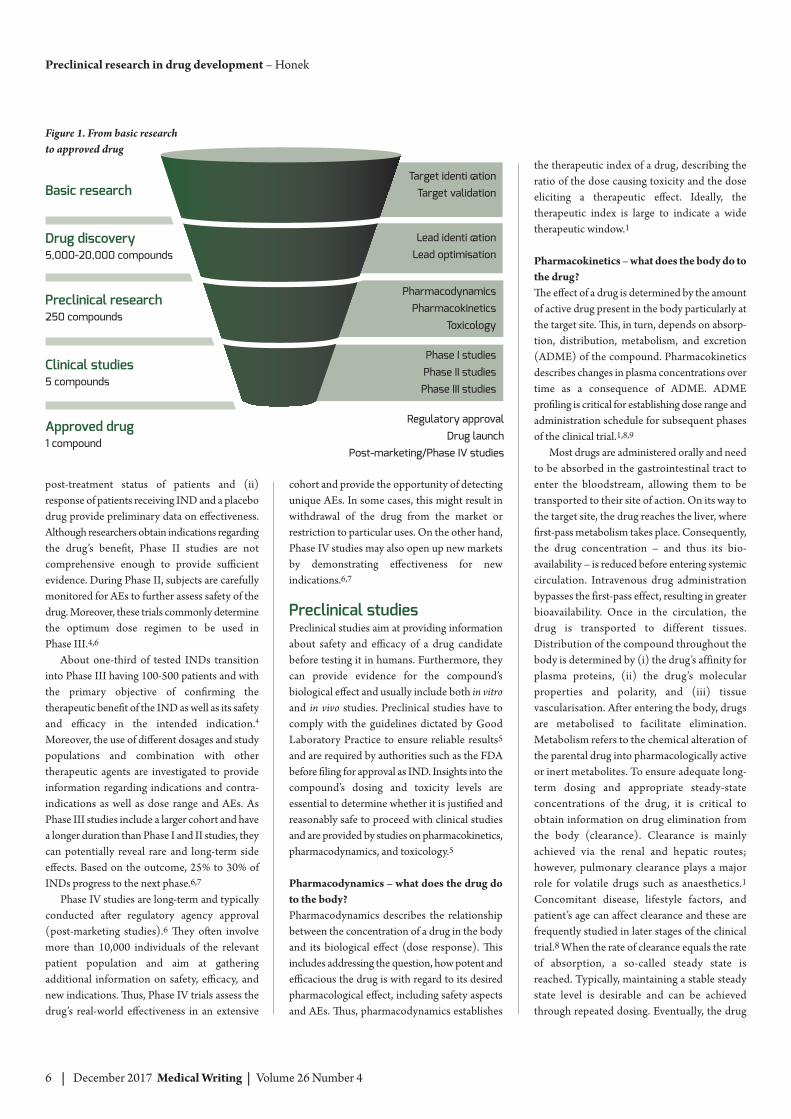
From bench to bedside – thelong journey from the lab intothe clinicDeveloping a novel drug is an interdisciplinaryendeavour involving a multitude of competencesfrom biologists, chemists, computer scientists,medical staff, statisticians, and regulatory experts.Taking a compound from bench to bedsiderequires up to 12 years at an average estimatedcost exceeding US $1 billion.1 Figure 1 sum -marises this long-term process (see overleaf).
Drug development starts with the iden ti -fication of a “druggable” target. Bio informatics,genetic association studies, and phenotypescreening are valuable tools in the discovery ofnovel targets. To validate the relevance of theidentified target for a particular disease, studiesare performed to investigate whether targetmodulation is disease modifying.2 Eventually,lead compounds are obtained and their potentialto interact with the target as well as their effecton the biological system is evaluated. Thousandsof modifications and variations of these leadcompounds are synthesised and tested duringpreclinical activities. Once an optimisedcompound is identified, this investigational newdrug (IND) becomes a candidate for clinicaltrials involving human subjects.
Clinical trials are conducted over differentphases (Phase I-IV), starting from a smallnumber of subjects and extending to large
cohorts.1 In Phase I studies, the IND isadministered to humans for the first time.3 EarlyPhase I studies (previously Phase 0) describefirst-in-human studies where a small group ofsubjects, usually 10 to 15 individuals, received asingle, sub-therapeutic dose to obtain pharma -cokinetic information without inducing pharma -cological effects. The goal of these exploratorystudies is to investigate whether the drugcandidate performs as expected based onpreclinical studies. If successful, further studiesassess safety and tolerance of the IND in humansubjects. These studies typically involve 20–50healthy volunteers. Apart from determining thedrug’s maximum tolerated dose by increasing thetreatment dose until dose-limiting toxicity isreached (dose escalation), the drug’s mostcommon and serious adverse effects (AEs) aswell as pharmacological, pharmacodynamic, andpharmacokinetic properties are evaluated.4
Approximately 70% of drug candidates movefrom Phase I to Phase II, in which therapeuticefficacy of the IND in patients is assessed.5 PhaseII studies typically involve several hundredpatients. The study population is well defined byinclusion and exclusion criteria, and based on thedose or dose range determined in Phase I, dose
response in patients and thedrug’s biological activity are
evaluated. Comparison of(i) pre- and
Preclinical research in drugdevelopment
6 | December 2017 Medical Writing | Volume 26 Number 4
post- treatment status of patients and (ii)response of patients receiving IND and a placebodrug provide preliminary data on effectiveness.Although researchers obtain indications regardingthe drug’s benefit, Phase II studies are notcomprehensive enough to provide sufficientevidence. During Phase II, subjects are carefullymonitored for AEs to further assess safety of thedrug. Moreover, these trials commonly determinethe optimum dose regimen to be used in Phase III.4,6
About one-third of tested INDs transitioninto Phase III having 100-500 patients and withthe primary objective of confirming thetherapeutic benefit of the IND as well as its safetyand efficacy in the intended indication.4
Moreover, the use of different dosages and studypopulations and combination with othertherapeutic agents are investigated to provideinformation regarding indications and contra -indications as well as dose range and AEs. AsPhase III studies include a larger cohort and havea longer duration than Phase I and II studies, theycan potentially reveal rare and long-term sideeffects. Based on the outcome, 25% to 30% ofINDs progress to the next phase.6,7
Phase IV studies are long-term and typicallyconducted after regulatory agency approval(post-marketing studies).6 They often involvemore than 10,000 individuals of the relevantpatient population and aim at gatheringadditional information on safety, efficacy, andnew indications. Thus, Phase IV trials assess thedrug’s real-world effectiveness in an extensive
cohort and provide the opportunity of detectingunique AEs. In some cases, this might result inwithdrawal of the drug from the market orrestriction to particular uses. On the other hand,Phase IV studies may also open up new marketsby demonstrating effectiveness for newindications.6,7
Preclinical studies Preclinical studies aim at providing informationabout safety and efficacy of a drug candidatebefore testing it in humans. Furthermore, theycan provide evidence for the compound’sbiological effect and usually include both in vitroand in vivo studies. Preclinical studies have tocomply with the guidelines dictated by GoodLaboratory Practice to ensure reliable results5
and are required by authorities such as the FDAbefore filing for approval as IND. Insights into thecompound’s dosing and toxicity levels areessential to determine whether it is justified andreasonably safe to proceed with clinical studiesand are provided by studies on pharmacokinetics,pharmacodynamics, and toxicology.5
Pharmacodynamics – what does the drug doto the body?Pharmacodynamics describes the relationshipbetween the concentration of a drug in the bodyand its biological effect (dose response). Thisincludes addressing the question, how potent andefficacious the drug is with regard to its desiredpharmacological effect, including safety aspectsand AEs. Thus, pharmacodynamics establishes
Preclinical research in drug development – Honek
Figure 1. From basic researchto approved drug
Basic research
Drug discovery5,000-20,000 compounds
Preclinical research250 compounds
Clinical studies5 compounds
Approved drug1 compound
Target identi cation
Target validation
Lead identi cation
Lead optimisation
Pharmacodynamics
Pharmacokinetics
Toxicology
Phase I studies
Phase II studies
Phase III studies
Regulatory approval
Drug launch
Post-marketing/Phase IV studies
the therapeutic index of a drug, describing theratio of the dose causing toxicity and the doseeliciting a therapeutic effect. Ideally, thetherapeutic index is large to indicate a widetherapeutic window.1
Pharmacokinetics – what does the body do tothe drug?The effect of a drug is determined by the amountof active drug present in the body particularly atthe target site. This, in turn, depends on absorp -tion, distribution, metabolism, and excretion(ADME) of the compound. Pharmacokineticsdescribes changes in plasma concentrations overtime as a consequence of ADME. ADMEprofiling is critical for establishing dose range andadministration schedule for subsequent phasesof the clinical trial.1,8,9
Most drugs are administered orally and needto be absorbed in the gastrointestinal tract toenter the bloodstream, allowing them to betransported to their site of action. On its way tothe target site, the drug reaches the liver, wherefirst-pass metabolism takes place. Consequently,the drug concentration – and thus its bio -availability – is reduced before entering systemiccirculation. Intravenous drug administrationbypasses the first-pass effect, resulting in greaterbioavailability. Once in the circulation, thedrug is transported to different tissues.Distribution of the compound throughout thebody is determined by (i) the drug’s affinity forplasma proteins, (ii) the drug’s molecularproperties and polarity, and (iii) tissuevascularisation. After entering the body, drugsare metabolised to facilitate elimination.Metabolism refers to the chemical alteration ofthe parental drug into pharmacologically activeor inert metabolites. To ensure adequate long-term dosing and appropriate steady-stateconcentrations of the drug, it is critical toobtain information on drug elimination fromthe body (clearance). Clearance is mainlyachieved via the renal and hepatic routes;however, pulmonary clearance plays a majorrole for volatile drugs such as anaesthetics.1Concomitant disease, lifestyle factors, andpatient’s age can affect clearance and these arefrequently studied in later stages of the clinicaltrial.8 When the rate of clearance equals the rateof absorption, a so-called steady state isreached. Typically, maintaining a stable steadystate level is desirable and can be achievedthrough repeated dosing. Eventually, the drug

www.emwa.org Volume 26 Number 4 | Medical Writing December 2017 | 7
and its metabolites are excreted from the bodymainly through urine or faeces.
Toxicology – it is potent, but is it safe?To determine whether a drug is safe for testing inhuman subjects, preclinical toxicology studies areperformed to identify the treatment regimenassociated with the least degree of toxicity andthus determine a suitable and safe starting dosefor clinical trials. Additionally, they can be usedto establish biomarkers for monitoring potentialAEs later. Starting with single-dose studies toidentify organs that might be subject to drugtoxicity, preclinical in vivo studies continue withrepeated-dose approaches. The treatmentregimen ideally mimics the intended clinicaldesign with respect to treatment duration,schedule, and route of administration. Otherstudies evaluate carcinogenicity, genotoxicity,and reproductive toxicity. While the drug’sgenotoxic effect is usually studied based on itspotential to induce mutations in yeast-based invitro systems, carcinogenicity and reproductivetoxicity studies typically involve rats. As thetumorigenic effect of a drug may only becomeevident after prolonged exposure, carcinogenicitystudies comprise continuous drug administrationfor a minimum of six months.
The ideal preclinical modelaccurately mimics humandiseaseObtaining relevant results from preclinicalstudies with a high degree of generalisabilityrequires appropriate preclinical models that areas comparable to the target population aspossible. Typically, this involves a series ofexperiments using in vitro, in vivo, and morerecently, also in silico models.
In vitro models – studying the drug in a petridishIn vitro studies are a relatively fast, simple, andcost efficient way of preclinical testing. Thosestudies utilise cell, tissue, and organ cultures, orfocus on particular cell components such asproteins or other biological macromolecules. In vitro studies permit tight control and monitoringof experimental settings and often providemechanistic evidence for the investigationalcompound’s mode of action. While having thepotential to provide mechanistic insights, in vitromodels are constrained by the fact that isolatedcells may not behave in a petri dish as they would
within the body where they partake in crosstalkand interaction with millions of other cells.Consequently, more sophisticated preclinicalmodels are required to establish the inves ti -gational compound’s safety profile beforetransitioning to a clinical setting.
In vivo models – is the mouse the bestexperimental animal?In vivo studies consider the complete organismbased on various animal models. Similar tostudies in humans, animal testing is tightlyregulated in most countries and permission fromlocal ethical review boards is required to ensurethat no unnecessary harm is done to theexperimental subjects. Recent advances haverefined the use of animal models in drugdevelopment through non-invasive imagingtechnologies, microsampling, and telemetricmonitoring.10 Naturally, controlling experimentalsettings is far more complicated for in vivostudies and, due to the complexity of the livingorganism, compounds may behave differentlyfrom what is expected based on results obtainedin a test tube.
The choice of appropriate animal modelsdepends on myriad criteria and requiresunderstanding of species-specific physiology andsimilarity with regard to the target organ,metabolic pathways as well as financial,regulatory, and ethical considerations. Typically,in vivo studies are performed in a rodent (e.g,mouse, guinea pig, hamster) and non-rodentmodel to comply with FDA requirements. Mice,rats, and dogs are among the most frequentlyused animal models while testing in primates(e.g., monkeys, apes, etc.) is performedoccasionally and typically for larger molecules.9One of the most popular animal models in
pharmaceutical testing is the mouse. The genomes of mouse and man are highly
similar: 99% of all mouse genes overlap withthose of humans. Additionally, genomicmanipulation in this organism has become fairlysimple. Nevertheless, species-specific differencesin host immune response, drug metabolism, andtumour heterogeneity affect therapeutic out -comes. Differences in pharmacokinetics andpharmacodynamics among species are also notnegligible and thus, mouse models often sufferfrom poor predictive power regarding clinicalefficacy.11 However, lack of superior alternativesmakes mouse models the gold standard fortesting cancer-targeting drugs.
Classically, such mouse cancer models werelimited to transplantation of cultured humantumour cells (cell lines) to immunodeficient micesuch as nude or severe combined immuno -deficiency (SCID) mice.12 Transplantation ofcells, tissue, or organs from one species toanother is called xenografting. In these cell line-derived xenograft (CDX) models, cancer cells areinjected subcutaneously and tumour growthcurves are established by measuring the size ofthe tumour in regular intervals. Treatment oftumour-bearing mice with a drug candidateprovides information regarding its potential toreduce tumour growth and thus its in vivoefficacy. However, these cell lines have beenpassaged under artificial conditions that do notrecapitulate the natural tumour micro environ -ment. Consequently, CDX models may lacksimilarity with human disease.11,13 To improveclinical relevance, a range of different mousemodels has been developed and is used in in vivoexperiments:� Patient-derived xenograft (PDX) models:
Tissue from a patient’s primary tumour isdirectly implanted into the animal. Thisstrategy omits in vitro adaptation of tumourcells and, thus, these models are more similarto human disease in terms of stromalcomposition and tumour heterogeneity, incontrast to classical CDX models. The PDXapproach is challenging; however, recentadvances in sample retrieval and transplan -tation technology made this method feasible.To date, PDX models consist of almostexclusively subcutaneous transplants.
� Orthotopic tumour models: Tumours areimplanted into the organ of origin (i.e.orthotopically) to better mimic the micro -environment and recapitulate metastasis
Honek – Preclinical research in drug development

8 | December 2017 Medical Writing | Volume 26 Number 4
Preclinical research in drug development – Honek
pathways of human tumours.11,13 Conse -quently, orthotopic models are moreclinically relevant. Orthotopic PDX modelsare technically challenging and thusuncommon, while orthotopic transplantationis widely used for CDX models.11
� Genetically engineered mice (GEM):Genetic engineering has given rise tohumanised mouse models and providesvaluable tools for translational research.Through genetic manipulation, mutations inoncogenes or tumour suppressor genesassociated with human malignancies areintroduced. In GEM, tumours developorthotopically from initiation throughprogression in their native microenvironmentrecapitulating human tumourigenesis.11
Hence, preclinical studies in GEM have thepotential to provide more relevant data forsubsequent clinical trials.
In silico models – the computer’s role in drugdevelopmentProgress in bioinformatics over the past decadeshas made in silico studies attractive so that theyoften precede or complement in vitro and in vivostudies. In silico models are based on computersimulations and provide information on how aninvestigational compound might behave insubsequent in vitro and in vivo experiments.14
Apart from technological requirements, thesecomputer simulations demand expert knowledgein biochemistry and molecular biology.
Preclinical research isindispensableDespite all efforts to identify relevant animalmodels to ensure a significant translational value,drugs often show different pharmacodynamiccharacteristics when administered to humansubjects. Thus, merely one out of fiveinvestigational drugs tested in clinical trialseventually gains approval for clinical use. Somestudies even report that only nine percent ofcompounds passing preclinical efficacy
evaluation are approved by the FDA.11 The factthat most anti-cancer drugs do not pass efficacyevaluation in Phase II and III studies suggeststhat currently used preclinical models fail atappropriately mimicking tumour heterogeneity,host factors, and drug resistance mech -anisms.15,16 Nevertheless, preclinical research isindispensable to protect human subjects inclinical trials. Adequate design of preclinicalstudies and careful choice of model systems arevital to ensure relevant results that translate intoapplicability in clinical settings.
Conflicts of InterestThe author declares no conflicts of interest.
References 1. Ng R. Drugs: From discovery to approval.
3rd ed. New Jersey: Wiley-Blackwell; 2015. 2. Hughes JP, Rees S, Kalindjian SB, Philpott
KL. Principles of early drug discovery. Br JPharmacol. 2011;162(6):1239–49.
3. European Medicines Agency. ICH Topic E8 General Considerations for ClinicalTrials. 1998 [cited 2017 September 10].Available from: http://www.emea.eu.int.Published 1998.
4. Friedman LM, Furberg CD, Demets DL.Fundamentals of clinical trials. 4th ed. New York: Springer Science+BusinessMedia LLC; 2010.
5. U.S. Food & Drug Administration. The Drug Development Process – Step 2:Preclinical Research. 2017. [cited 2017September 10]. Available from:https://www.fda.gov/forpatients/approvals/drugs/ucm405658.htm.
6. U.S. Food & Drug Administration. The Drug Development Process - Step 3:Clinical Research. 2017. [cited 2017September 10]. Available from:https://www.fda.gov/ForPatients/Approvals/Drugs/ucm405622.htm.
7. Waller DG, Sampson T. Medicalpharmacology and therapeutics E-Book.
Elsevier Health Sciences; 2017.8. Fitzpatrick S. The clinical trial protocol.
Buckinghamshire: Institute of ClinicalResearch; 2005.
9. Faqi AS, ed. A comprehensive guide totoxicology in preclinical drug development.Waltham, MA: Elsevier; 2013.
10. Everitt JI. The future of preclinical animalmodels in pharmaceutical discovery anddevelopment: A need to bring in cerebro tothe in vivo discussions. Toxicol Pathol.2015;43(1):70–7.
11. Herter-Sprie GS, Kung AL, Wong KK. Newcast for a new era: Preclinical cancer drugdevelopment revisited. J Clin Invest.2013;123(9):3636–45.
12. Vandamme T. Use of rodents as models ofhuman diseases. J Pharm Bioallied Sci.2014;6(1):2.
13. Hoffman RM. Patient-derived orthotopicxenografts: Better mimic of metastasis thansubcutaneous xenografts. Nat Rev Cancer.2015;15(8):451–2.
14. Amberg A. In silico methods. In: VogelHG, Maas J, Hock FJ, Mayer D, eds. DrugDiscovery and Evaluation: Safety andPharmacokinetic Assays. Berlin,Heidelberg: Springer; 2013:1273–96.
15. Day CP, Merlino G, Van Dyke T. Preclinicalmouse cancer models: A maze ofopportunities and challenges. Cell.2015;163(1):39–53.
16. Al-Lazikani B, Banerji U, Workman P.Combinatorial drug therapy for cancer inthe post-genomic era. Nat Biotechnol.2012;30(7):679–92.
Author informationJennifer Honek has a background inmolecular biotechnology and holds a PhD inMedicine. She has been active as a freelancemedical writer since 2015 and also works fora medtech company as a clinical trial lead.





























