Embed Size (px)
Citation preview

Gynecologic Oncology 122 (2011) 595–599
Contents lists available at ScienceDirect
Gynecologic Oncology
j ourna l homepage: www.e lsev ie r.com/ locate /ygyno
Predicting gestational trophoblastic neoplasia (GTN): Is urine hCG the answer?
Mo'iad Alazzam a,e,⁎, Tracey Young c, Robert Coleman b,d, Barry Hancock b,d, David Drew b,Perm Wilson b, John Tidy a,b,⁎⁎a Sheffield Gynaecological Cancer Centre, Sheffield Teaching Hospitals NHS Trust, Glossop Road, UKb Sheffield Trophoblastic Disease Centre, Sheffield, UKc School of Health and Related Research (ScHARR), University of Sheffield NIHR Research Design Service for Yorkshire and Humber, Sheffield, UKd Department of Oncology, University of Sheffield, Sheffield, UKe The Galway Clinic, Galway, Ireland
⁎ Correspondence to: M. Alazzam, Department of GyDoughiska, Galway, Ireland.⁎⁎ Correspondence to: J. Tidy, Sheffield Gynaeco
Hallamshire Hospital, Glossop Road, Sheffield S10 4JL, UE-mail addresses: [email protected] (M.' Alazza
(J. Tidy).
0090-8258/$ – see front matter © 2011 Elsevier Inc. Aldoi:10.1016/j.ygyno.2011.05.035
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 9 April 2011Accepted 27 May 2011Keywords:Human chorionic gonadotrophin (hCG)Urine hCGMolar pregnancyGestational trophoblastic neoplasia (GTN)
Background. Previous studies on the significance of hCG to predict gestational trophoblastic neoplasia(GTN) have been too small for robust conclusions to be reached. Our aim in this study was to analyse thesignificance of urine hCG in predicting GTN in a large population.
Methods. Details of 3926 patients were available for analysis. Information regarding age, dates of diagnosisand registration, urine hCG levels, antecedent pregnancy and chemotherapy were prospectively collectedand used for analyses. Patients were stratified into different groups according to urine hCG level (IU/L); b 50,50–99, 100–249, 250–499, 500–999, 1000–9999 and≥10,000. Multivariate analyses were used to identify theprognostic indicators of GTN.
Results. Urine hCG and antecedent pregnancy were the most powerful indicators for developing GTN(Pb0.01). None of the patients with partial mole and urine hCG b50 IU/L (Normal level=40 IU/L) developedGTN. The risk of GTN was N35% in all patients with urine hCG ≥500 IU/L. GTN developed in 70% of patientswith complete mole and urine hCG ≥10,000 IU/L.
Conclusion. Urine hCG is sensitive test for GTN. Urine hCG level is a powerful prognostic indicator for theGTN. Patients with partial mole could be safely discharged from the surveillance programme once their hCGhave normalised. Patients with urine hCG≥249 IU/L, whether partial or complete molar pregnancy, appear tobenefit from intensive surveillance. Prophylactic chemotherapy could be considered when there are problemswith surveillance.
© 2011 Elsevier Inc. All rights reserved.
Introduction
Gestational trophoblastic disease (GTD) is a term used to describe avariety of pathological subtypes, all of which arise from humantrophoblastic tissue. It includes complete and Partial HydatidiformMole, choriocarcinoma, placental site trophoblastic tumour andepithelioidtrophoblast tumour.
The majority of hydatidiform moles resolve spontaneously afterevacuation of the uterus. However, in the remainder the diseasepersists and requires chemotherapy [1,2]. Almost all patients arepotentially curable if they are correctly diagnosed and treated [1].
Women diagnosed with complete molar pregnancy are typicallycounselled that the risk of developing GTN is in the range of 6–30%
naecology, The Galway Clinic,
logical Cancer Centre, RoyalK.m), [email protected]
l rights reserved.
[2,3], compared to a 0.5–3% risk faced by women who had partialmolar pregnancy [4,5].
Persistent GTD, now referred to as GTN, manifests either clinically,or more commonly, as persistently elevated or rising hCG levels. Incountries where surveillance is available, patients are registeredat specialist centres for follow up once the diagnosis of molar preg-nancy is confirmed. Themethod of follow-up using blood or urine hCGvaries depending on the specialist centre, as does the frequency ofassessment. In Sheffield, patients are routinely followed upwith serialurine hCG until they undergo spontaneous resolution or there isevidence of persistent disease requiring further investigation andtreatment. Until 2007, the length of surveillance varied according tothe original histological diagnosis of the disease; in cases of CompleteHydatidiform Mole (CHM) patients were followed up for two yearscompared with one year following Partial Hydatidiform Mole (PHM).Following review of the registration and follow up process, ashortened period of follow up was introduced both in Sheffield andthe Charing Cross in London. Women with either CHM or PHM arenow followed for only 6 months from the first normal hCG followinguterine evacuation [6,7].

Table 1Multivariate analysis for factors predicting persistent disease (GTN) — all patients.
Variable Coefficientvalue
Pvalue
95% confidence interval
Age 0.013 0.24 −0.01 0.36CHM −1.60 0.001 −2.03 −1.17PHM −0.11 0.79 −0.91 0.69UhCG (test result) 0.00005 0.0001 0.00004 0.00006Reduced time interval betweendiagnosis and registration
−0.016 0.001 –0.03 −0.01
596 M.' Alazzam et al. / Gynecologic Oncology 122 (2011) 595–599
Several investigators have attempted to identify factors that mightpredict either disease remission or persistence [6–10]. Accurateprediction may provide a means to reduce the duration or intensityof surveillance, enable better counselling of patients and providereassurance for those at low risk of developing persistent disease.Conversely, reliable prediction of GTN may also allow the provision ofprophylactic chemotherapy treatment for patients who are at a higherrisk of developing persistent disease or in countries where there areproblems with follow up and/or adherence to the follow-up protocol.
The extended surveillance schemes adopted by many specialistcentres allow the adoption of a conservative treatment philosophyby minimising the effects of cytotoxic chemotherapy without com-promising patient care and treatment cure rates. However, theextended “follow up” is resource demanding and associated withsignificant practical complications including compliance and patientanxiety.
The aim of this study was to assess if urine hCG, measured inwomen registered with the Sheffield Trophoblastic Disease Centre,could be reliably used to predict disease remission and thus determineif follow up could be abbreviated further. We also assessed the needfor chemotherapy based on hCG levels at different time points, asthis could inform us when counselling women during follow up.
Methods
Women referred to the Sheffield Trophoblastic Disease Centrewith a diagnosis of molar pregnancy are prospectively registered on acomputerised database. Using this database we collected informationof patients age, histological diagnosis, date of first uterine evacuation,date of registration, date and level of serial urine hCG, and the date ofany further treatment for those who developed GTN.
Once patients are registered on the database, those who needurine hCG follow-up are identified. A sample tube (containing a smallamount of preservative) and request form labelled with patient name,hospital number and a unique barcode is sent to the patient togetherwith a pre-paid envelope. Instructions for sample taking and postingback to lab are on reverse of form.
A competitive protein binding radioimmune assay is used for hCGdetermination. The hCG competes with 125Iodine-hCG for bindingsites on a polyclonal antibody (raised in a rabbit). When the reactionhas reached equilibrium (approximately 16 h), the antibody/antigen(Ab/Ag) complexes are precipitated by the addition of a secondantibody (anti-rabbit IgG covalently coupled to micro-fine celluloseparticles). The precipitate is compacted by centrifugation and excessliquid removed. The amount of radioactivity in each precipitate isinversely proportional to the concentration of hCG in the sample.Result are reported as hCGIU/L and also hCG/creatinine ratio (log10(hCG/creatinine)) to compensate for urineconcentration.
At our centre, we have stringent criteria for the definition andtreatment of persistent disease [11]. Patients included in this reportrepresent the subgroup that underwent treatment as a result of eitherhCG plateau or rise during the follow-up period. Women with aninitial diagnosis of choriocarcinoma, placental site trophoblastictumour (PSTT) or epitheloid trophoblastic tumour (ETT), and thosewho required treatment coincident with the time of registration werenot included. Although we do not perform central pathology reviewwhen patients undergo surveillance; central pathology review ismandatory for patients with suspected GTN and for those who needchemotherapy.
Based on their clinical outcome, patients were categorised intotwo groups; GTN (patients who received chemotherapy) or sponta-neous resolution. Patients were then divided into different groupsusing specific numerical ranges for urine hCG: 0–49, 50–99, 100–249,250–499, 500–999, 1000–9999 and ≥10,000 IU/L. Using these nu-merical values, we then calculated the number and the proportion ofpatients who developed GTN at weekly intervals for the first eight
weeks, with reference to both registration and diagnosis dates. As therisk of developing GTN varies between CHM and PHM, we analysedeach histological group separately.
Using the results of the first urine hCG for all included patients, weperformed multivariate analyses to identify factors that might in-fluence disease persistence and subsequently administration of che-motherapy. We, initially, analysed all patients as one group. Then werepeated the same analysis after dividing the sample subjects intotwo groups; using the value of urinehCG 500 IU/L as a cut off point.Age, urinehCG level, histological diagnosis and time interval betweentime of first evacuation and registration were included. All analyseswere performed using STATA software package version 10.1 (2009)StataCorp LP, Texas, USA.
Local institutional review board approval was obtained for thisstudy. This studywas donewith anonymised patient records and henceinformed consent was not needed.
Results
4071 patientswere identifiedwhounderwent urine hCGmonitoringbetween September 1989 and February 2008; 2333 patients with adiagnosis of PHM, 1593 with CHM and in 145 patients the primaryhistology was unknown. Of these, 169 patients (4.2%) developed GTNand received chemotherapy; 127 (8.0%)with CHM, 35 (1.5%)with PHM,whilst in 7 patients theprimary histologywas unknown. The groupwithunknown primary histology was excluded from the study resulting in3926 eligible patients.
The mean age of all registered women was 28.8 years (standarddeviation (SD)=7.0). Women who developed GTN (Mean=29.6,SD=7.8 years) were slightly older than those who had spontaneousresolution (Mean=28.7, SD=7.0 years), although this difference didnot reach statistical significance.
The type of antecedent molar pregnancy and the numerical valueof urine hCG were the most significant factors to predict thedevelopment of GTN. Women with CHM had a significantly higherrisk for developing GTN when compared with those who have PHM(P=0.01).
The mean interval between uterine evacuation of the molarpregnancy and registration was 46.7 days (SD=32.2). Women whosubsequently developed GTN had a shorter interval between uterineevacuation and registration (Mean=35.8 days, SD=23.1 days), com-pared to women who had spontaneous resolution (Mean=47.2 days,SD=32.5 days, Pb0.001) (Table 1 and Table 2).
Complete Hydatidiform Mole (CHM)
127 patients of 1593 patients included in the study (8%) developedGTN as result of persistently elevated urine hCG and received che-motherapy (Table 2). At all time points, the risk of developing GTNprogressively increased with the level of urine hCG levels (Fig. 1A). Atone extreme, in patients with urine hCG b50 IU/L, the risk of devel-oping GTNwas less than 1% irrespective ofwhen this level was reached,whereas, in patients with urine hCG≥10,000 IU/L or more, irrespectiveof when this level was reached, the risk of developing GTN was at least
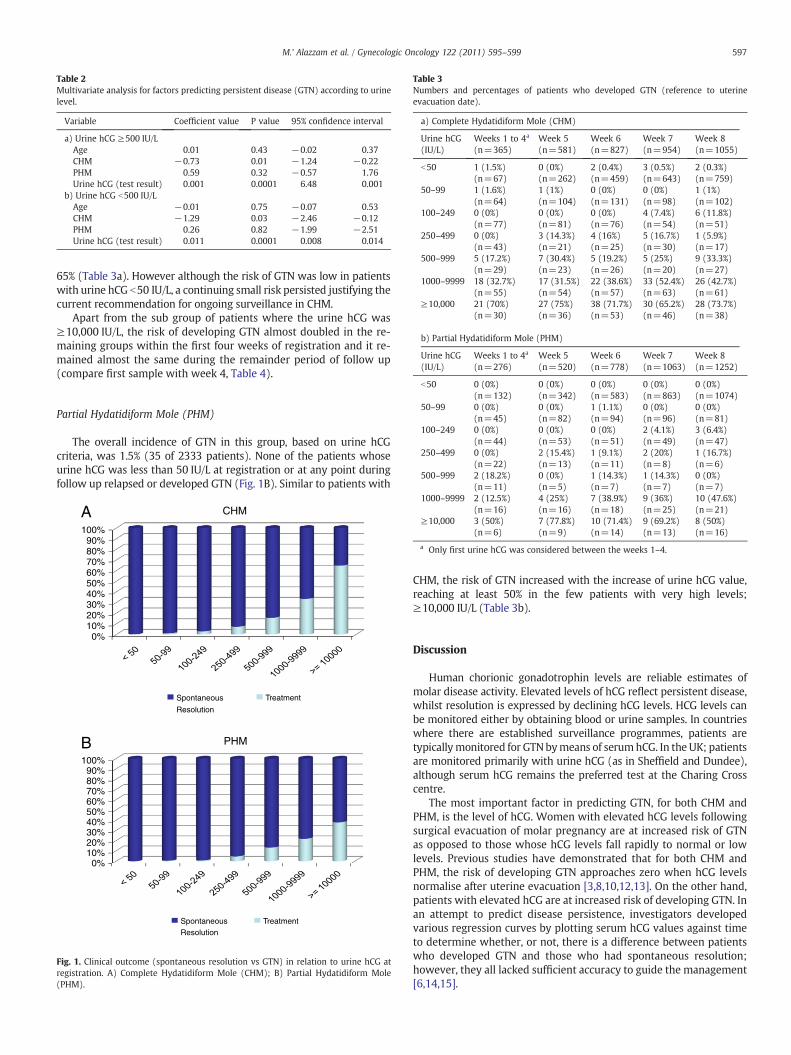
Table 2Multivariate analysis for factors predicting persistent disease (GTN) according to urinelevel.
Variable Coefficient value P value 95% confidence interval
a) Urine hCG ≥500 IU/LAge 0.01 0.43 −0.02 0.37CHM −0.73 0.01 −1.24 −0.22PHM 0.59 0.32 −0.57 1.76Urine hCG (test result) 0.001 0.0001 6.48 0.001
b) Urine hCG b500 IU/LAge −0.01 0.75 −0.07 0.53CHM −1.29 0.03 −2.46 −0.12PHM 0.26 0.82 −1.99 −2.51Urine hCG (test result) 0.011 0.0001 0.008 0.014
Table 3Numbers and percentages of patients who developed GTN (reference to uterineevacuation date).
a) Complete Hydatidiform Mole (CHM)
Urine hCG(IU/L)
Weeks 1 to 4a
(n=365)Week 5(n=581)
Week 6(n=827)
Week 7(n=954)
Week 8(n=1055)
b50 1 (1.5%)(n=67)
0 (0%)(n=262)
2 (0.4%)(n=459)
3 (0.5%)(n=643)
2 (0.3%)(n=759)
50–99 1 (1.6%)(n=64)
1 (1%)(n=104)
0 (0%)(n=131)
0 (0%)(n=98)
1 (1%)(n=102)
100–249 0 (0%)(n=77)
0 (0%)(n=81)
0 (0%)(n=76)
4 (7.4%)(n=54)
6 (11.8%)(n=51)
250–499 0 (0%)(n=43)
3 (14.3%)(n=21)
4 (16%)(n=25)
5 (16.7%)(n=30)
1 (5.9%)(n=17)
500–999 5 (17.2%)(n=29)
7 (30.4%)(n=23)
5 (19.2%)(n=26)
5 (25%)(n=20)
9 (33.3%)(n=27)
1000–9999 18 (32.7%)(n=55)
17 (31.5%)(n=54)
22 (38.6%)(n=57)
33 (52.4%)(n=63)
26 (42.7%)(n=61)
≥10,000 21 (70%)(n=30)
27 (75%)(n=36)
38 (71.7%)(n=53)
30 (65.2%)(n=46)
28 (73.7%)(n=38)
b) Partial Hydatidiform Mole (PHM)
Urine hCG(IU/L)
Weeks 1 to 4a
(n=276)Week 5(n=520)
Week 6(n=778)
Week 7(n=1063)
Week 8(n=1252)
597M.' Alazzam et al. / Gynecologic Oncology 122 (2011) 595–599
65% (Table 3a). However although the risk of GTN was low in patientswith urine hCG b50 IU/L, a continuing small risk persisted justifying thecurrent recommendation for ongoing surveillance in CHM.
Apart from the sub group of patients where the urine hCG was≥10,000 IU/L, the risk of developing GTN almost doubled in the re-maining groups within the first four weeks of registration and it re-mained almost the same during the remainder period of follow up(compare first sample with week 4, Table 4).
b50 0 (0%)(n=132)
0 (0%)(n=342)
0 (0%)(n=583)
0 (0%)(n=863)
0 (0%)(n=1074)
50–99 0 (0%)(n=45)
0 (0%)(n=82)
1 (1.1%)(n=94)
0 (0%)(n=96)
0 (0%)(n=81)
100–249 0 (0%)(n=44)
0 (0%)(n=53)
0 (0%)(n=51)
2 (4.1%)(n=49)
3 (6.4%)(n=47)
250–499 0 (0%)(n=22)
2 (15.4%)(n=13)
1 (9.1%)(n=11)
2 (20%)(n=8)
1 (16.7%)(n=6)
500–999 2 (18.2%)(n=11)
0 (0%)(n=5)
1 (14.3%)(n=7)
1 (14.3%)(n=7)
0 (0%)(n=7)
Partial Hydatidiform Mole (PHM)
The overall incidence of GTN in this group, based on urine hCGcriteria, was 1.5% (35 of 2333 patients). None of the patients whoseurine hCG was less than 50 IU/L at registration or at any point duringfollow up relapsed or developed GTN (Fig. 1B). Similar to patients with
CHM
0%10%20%30%40%50%60%70%80%90%
100%
Spontaneous
Resolution
Treatment
PHM
0%10%20%30%40%50%60%70%80%90%
100%
Spontaneous Resolution
Treatment
A
B
Fig. 1. Clinical outcome (spontaneous resolution vs GTN) in relation to urine hCG atregistration. A) Complete Hydatidiform Mole (CHM); B) Partial Hydatidiform Mole(PHM).
1000–9999 2 (12.5%)(n=16)
4 (25%)(n=16)
7 (38.9%)(n=18)
9 (36%)(n=25)
10 (47.6%)(n=21)
≥10,000 3 (50%)(n=6)
7 (77.8%)(n=9)
10 (71.4%)(n=14)
9 (69.2%)(n=13)
8 (50%)(n=16)
a Only first urine hCG was considered between the weeks 1–4.
CHM, the risk of GTN increased with the increase of urine hCG value,reaching at least 50% in the few patients with very high levels;≥10,000 IU/L (Table 3b).
Discussion
Human chorionic gonadotrophin levels are reliable estimates ofmolar disease activity. Elevated levels of hCG reflect persistent disease,whilst resolution is expressed by declining hCG levels. HCG levels canbe monitored either by obtaining blood or urine samples. In countrieswhere there are established surveillance programmes, patients aretypicallymonitored for GTNbymeans of serumhCG. In the UK; patientsare monitored primarily with urine hCG (as in Sheffield and Dundee),although serum hCG remains the preferred test at the Charing Crosscentre.
The most important factor in predicting GTN, for both CHM andPHM, is the level of hCG. Women with elevated hCG levels followingsurgical evacuation of molar pregnancy are at increased risk of GTNas opposed to those whose hCG levels fall rapidly to normal or lowlevels. Previous studies have demonstrated that for both CHM andPHM, the risk of developing GTN approaches zero when hCG levelsnormalise after uterine evacuation [3,8,10,12,13]. On the other hand,patients with elevated hCG are at increased risk of developing GTN. Inan attempt to predict disease persistence, investigators developedvarious regression curves by plotting serum hCG values against timeto determine whether, or not, there is a difference between patientswho developed GTN and those who had spontaneous resolution;however, they all lacked sufficient accuracy to guide the management[6,14,15].

Table 4Suggested guidelines for the management molar pregnancy based on urine hCGlevelsat registration.
a) Partial Hydatidiform MoleUrine hCG b50 IU/L (no risk group)
Reassure and discharge from follow up.Urine hCG 50–249 IU/L (low risk group)
Risk of GTN is b10%.Monitor Bi-weekly urine hCG.Discharge once fallen to b50 IU/L (normalised) in two subsequent readings.Investigate for GTN if plateau or rising.
Urine hCG ≥250 IU/L (high risk group)Risk of GTN up to 38%.Monitor with weekly urine hCG.Discharge once fallen to b50 IU/L (normalised) in two subsequent readings.Investigate for GTN if Plateau or rising.Consider prophylactic chemotherapy if there are problems with follow up.
b) Complete Hydatidiform Mole (CHM)Urine hCG b50 IU/L (very low risk group)
Reassure, risk of GTN b1%.Monitor bi-weekly urine hCGDischarge after six months if remained b50 IU/L.
Urine hCG 50–249 IU/L (low risk group)Risk of GTN is ≤10%.Monitor Bi-weekly urine hCG.Discharge six months after fallen to b50 IU/L.Investigate for GTN if plateau or rising.
Urine hCG ≥250 IU/L (high risk group)Risk of GTN up to 65%.Monitor with weekly urine hCG.Discharge six months after fallen to b50 IU/LInvestigate for GTN if Plateau or rising.Consider prophylactic chemotherapy if there are problems with follow up.
598 M.' Alazzam et al. / Gynecologic Oncology 122 (2011) 595–599
Spontaneous normalisation group
In 1986 the Charing Cross group reported 27 patients with molarpregnancy who relapsed after hCG normalisation [16]. They definedtwo groups of patients who had spontaneous resolution; those whoreached normal levels within 56 days of evacuation and all remainedfree of disease. Of the remaining group who became normal after56 days, 27 (1%) relapsed and developed GTN. These findings sub-sequently formed the basis of the current surveillance strategy inthe UK. Studies from other centres, including our centre, showedsimilar results [9,13,17]. However, none of these studies differentiatedbetween complete molar pregnancy in which the reported risk fordeveloping GTN is within the range of 6–30% and partial mole wherethe risk is around 1%.
The results of our study clearly demonstrate that none of thepatients who had PHM and urine hCG b50 IU/L after uterine evac-uation relapsed or developed GTN, irrespective of when this levelwas reached during the follow up period. Although we use UhCG asthe main surveillance assay in our centre, our results are consistentwith those from other centreswho use different hCG assays; urine andserum [8,12,18].
The distinction between PHM and CHM can be difficult for thenonspecialist pathologist, with some early CHM being erroneouslydiagnosed as PHM. Although we do not routinely review histology inpatients with molar pregnancies who do not require further inves-tigation or treatment, even if some misclassifications had occurred,the fact that not a single patient with a normal hCG associated withPHM reported by the local pathologist developed GTN is reassuringand supports a policy of reducing follow-up in PHM.
However, women with CHM and urine hCG levelb50 IU/L duringthe follow up period continue to carry a small risk (b1%) for devel-oping GTN. Our findings are similar to the study from Wolfberg et al.in which two out of 876 (0.2%) patients with CHM developed GTN [3].
The definition of normal is always difficult and at times con-troversial. Definition of normal level varies between different regions
of the world and even between centres within the same country. Weacknowledge that the use of 50 IU/L as the lower cut-off level wasentirely arbitrary; it is higher than the conventional normal levels lessthan 40 IU/L at Sheffield and less than 25 IU/24 h at Charring Cross.The same can be said for the definition of normal with serum hCG.Besides, there are no prospective studies to determine the clinicaloutcome with the level of urine hCG. We, therefore, opted to move alittle away from the higher sensitivity concept and used a slightlyhigher cut-off point to demonstrate that patients can still be managedsafely even if a less sensitive test is used. Indeed only one patient witha urine hCG level of b100 developed GTN indicating the exact level ofthe cut off chosen is not critical to individual patient management.This is particularity important in regions where the pregnancy testsused are less sensitive than those used in more developed countries.
Persistently elevated urine hCG group
We observed a clear difference in the risk of GTN according tothe level of urine hCG, with risk of persistent disease rising with thelevel of urine hCG. We identified a subgroup of patients, a group whohad CHM and urine hCG ≥10,000 IU/L, in whom the risk fordeveloping GTN exceeded 65%. This subgroup requires intensivesurveillance, and prophylactic chemotherapy could be an option forthis group whenever follow up is unreliable or difficult for variousreasons.
This study illustrates that type of antecedent molar pregnancyand urine hCG values are the most significant factors in determiningwhether patients will either develop GTN or undergo spontaneousresolution. The observation that GTN patients are registered earlierthan those with spontaneous resolution may reflect clinical practice.Reasons for variability in registration practices are unknown but itseems, most probably, that gynaecologists are registering patients inwhom they have some clinical concern more rapidly.
We note that the published literature has applied, so far, the conceptof “one-size-fits-all” in either the adoption or rejection of surveillanceprogrammes or using various regression curves to predict patients'outcome [6,8,10]. However, and in light of the accumulated knowledgeover the last few decades, we now have sufficient information to un-derstand that molar pregnancy, both complete and partial, behaves insimilar fashion to other conditions where the risk of malignant trans-formation varies according to a number of factors.
We propose classifying patients into three risk groups based on theirurine hCG level and type of antecedentmolar pregnancy. The “no risk ornegligible risk” group have urine hCG levels below 50 IU/L; this grouppatients can be safely discharged if they have PHM. Patients with CHMand urine hCG b50 IU/L should be reassured that their risk of GTN is lessthan 1%, they can undergo less intensive follow up and be discharged6 months after hCG normalisation, (see suggested guidelines). The “lowrisk group” group whose urine hCG ranges between 50 and 249 IU/Land in whom the risk of developing GTN is around 10%. This low riskgroup could benefit from a less intensive surveillance scheme. The “highrisk” group includes those women whose urine hCG exceeds 249 IU/L.Patients in this group should be counselled for their increased risk ofdeveloping GTN and the need to undergo intensive surveillance. Thisgroup represents the majority of patients who develop GTN and whereprophylactic chemotherapymay be a reasonable optionwhen there areproblems with surveillance or patient compliance (Table 4).
Conclusion
Wehavedemonstrated that urinehCGcanbe safelyused to triage andfollow up women diagnosed with complete and partial molar pregnan-cies. We also show that patients with partial mole could be safelydischarged from the surveillance programme once their hCG havenormalised regardless of the hCG test used; urine or serum. Furthermore,we propose that women could safely undergo different surveillance

599M.' Alazzam et al. / Gynecologic Oncology 122 (2011) 595–599
protocols dependent on the type of molar pregnancy and the urine hCGlevel (Table 4a and b). Finally, we have identified a potential subgroup ofpatients who may benefit from prophylactic chemotherapy.
Authors contribution
MA and JT conceived and designed the study. MA collected thedata. DD and PW performed urine hCG assays. BWH, REC and JTtreated the patients. MA and TY performed data analysis. MA, JT, BWHand REC interpreted the data and wrote the manuscript. All authorshave seen and approved the final version of the report.
Conflict of interestThe authors declare they have no conflict of interest.
References[1] Hancock B. Differences in management and treatment: critical appraisal. In:
Hancock B, Newlands ES, Berkwitz RS, Cole LA, et al, editors. GestationalTrophoblastic Disease2nd ed. ; 2003. p. 337–47.
[2] Paradinas FJ. The histological diagnosis of hydatidiform moles. Curr Diag Path1994:24–31.
[3] Wolfberg AJ, Feltmate C, Goldstein DP, Berkowitz RS, Lieberman E. Low risk ofrelapse after achieving undetectable HCG levels in women with complete molarpregnancy. Obstet Gynecol 2004;104:551–4.
[4] Seckl MJ, Fisher RA, Salerno G, Rees H, Paradinas FJ, Foskett M, et al.Choriocarcinoma and partial hydatidiform moles. Lancet 2000;356:36–9.
[5] Berkowitz RS, Goldstein DP, Bernstein MR. Natural history of partial molarpregnancy. Obstet Gynecol 1985;66:677–81.
[6] van Trommel NE, Ngo Duc H, Massuger LF, Schijf CP, Sweep CG, Thomas CM. Earlyidentification of persistent trophoblastic disease with serum hCG concentrationratios. Int J Gynecol Cancer 2008;18:318–23.
[7] Behtash N, Ghaemmaghami F, Honar H, Riazi K, Nori A, Modares M, et al. Is normalbeta-hCG regression curve helpful in the diagnosis of persistent trophoblasticdisease? Int J Gynecol Cancer 2004;14:980–3.
[8] Wielsma S, Kerkmeijer L, Bekkers R, Pyman J, Tan J, Quinn M. Persistenttrophoblast disease following partial molar pregnancy. Aust N Z J Obstet Gynaecol2006;46:119–23.
[9] Pisal N, Tidy J, Hancock B. Gestational trophoblastic disease: is intensive follow upessential in all women? Bjog 2004;111:1449–51.
[10] Sebire NJ, Foskett M, Short D, Savage P, Stewart W, Thomson M, et al. Shortenedduration of human chorionic gonadotrophin surveillance following complete orpartial hydatidiform mole: evidence for revised protocol of a UK regionaltrophoblastic disease unit. Bjog 2007;114:760–2.
[11] http://www.chorio.group.shef.ac.uk/index.html In.[12] Lavie I, Rao GG, Castrillon DH, Miller DS, Schorge JO. Duration of human chorionic
gonadotropin surveillance for partial hydatidiform moles. Am J Obstet Gynecol2005;192:1362–4.
[13] Kerkmeijer LG, Wielsma S, Massuger LF, Sweep FC, Thomas CM. Recurrentgestational trophoblastic disease after hCG normalization following hydatidiformmole in The Netherlands. Gynecol Oncol 2007;106:142–6.
[14] Schlaerth JB, Morrow CP, Kletzky OA, Nalick RH, D'Ablaing GA. Prognosticcharacteristics of serum human chorionic gonadotropin titer regression followingmolar pregnancy. Obstet Gynecol 1981;58:478–82.
[15] Shigematsu T, Kamura T, Saito T, Kaku T, Nakano H, Kinugawa N. Identificationof persistent trophoblastic diseases based on a human chorionic gonadotro-pin regression curve by means of a stepwise piecewise linear regressionanalysis after the evacuation of uneventful moles. Gynecol Oncol 1998;71:376–80.
[16] Bagshawe KD, Dent J, Webb J. Hydatidiform mole in England and Wales 1973–83.Lancet 1986;2:673–7.
[17] Batorfi J, Vegh G, Szepesi J, Szigetvari I, Doszpod J, Fulop V. How long shouldpatients be followed after molar pregnancy? Analysis of serum hCG follow-updata. Eur J Obstet Gynecol Reprod Biol 2004;112:95–7.
[18] Wolfberg AJ, Growdon WB, Feltmate CM, Goldstein DP, Genest DR,Chinchilla ME, et al. Low risk of relapse after achieving undetectable HCGlevels in women with partial molar pregnancy. Obstet Gynecol 2006;108:393–6.





























