Embed Size (px)
Citation preview

Clinical Studies
Predicting Responses to NeoadjuvantChemotherapy in Breast Cancer: ACRIN 6691 Trialof Diffuse Optical Spectroscopic ImagingBruce J. Tromberg1, Zheng Zhang2, Ana€�s Leproux1, Thomas D. O'Sullivan1,Albert E. Cerussi1, Philip M. Carpenter3, Rita S. Mehta4, Darren Roblyer5,Wei Yang6,Keith D. Paulsen7, Brian W. Pogue7, Shudong Jiang7, Peter A. Kaufman8, Arjun G. Yodh9,So Hyun Chung9, Mitchell Schnall10, Bradley S. Snyder11, Nola Hylton12, David A. Boas13,Stefan A. Carp13, Steven J. Isakoff14, and David Mankoff10, on behalf of theACRIN 6691 investigators
Abstract
The prospective multicenter ACRIN 6691 trial was designedto evaluate whether changes from baseline to mid-therapy in adiffuse optical spectroscopic imaging (DOSI)–derived imagingendpoint, the tissue optical index (TOI), predict pathologiccomplete response (pCR) in women undergoing breast cancerneoadjuvant chemotherapy (NAC). DOSI instruments wereconstructed at the University of California, Irvine (Irvine, CA),and delivered to six institutions where 60 subjects with newlydiagnosed breast tumors (at least 2 cm in the longest dimen-sion) were enrolled over a 2-year period. Bedside DOSI imagesof the tissue concentrations of deoxy-hemoglobin (ctHHb),oxy-hemoglobin (ctHbO2), water (ctH2O), lipid, and TOI(ctHHb � ctH2O/lipid) were acquired on both breasts up tofour times during NAC treatment: baseline, 1-week, mid-point,
and completion. Of the 34 subjects (mean age 48.4 � 10.7years) with complete, evaluable data from both normal andtumor-containing breast, 10 (29%) achieved pCR as deter-mined by central pathology review. The percent change intumor-to-normal TOI ratio (%TOITN) from baseline to mid-therapy ranged from �82% to 321%, with a median of �36%.Using pCR as the reference standard and ROC curve method-ology, %TOITN AUC was 0.60 (95% CI, 0.39–0.81). In thecohort of 17 patients with baseline tumor oxygen saturation(%StO2) greater than the 77% population median, %TOITNAUC improved to 0.83 (95% CI, 0.63–1.00). We conclude thatthe combination of baseline functional properties and dynamicoptical response shows promise for clinical outcome predic-tion. Cancer Res; 76(20); 5933–44. �2016 AACR.
IntroductionNeoadjuvant chemotherapy (NAC), or preoperative systemic
therapy, offers unique opportunities for patient care and cancerdrug development (1). In addition to improving breast tissueconservation and cosmetic outcome, NAC can cause down-staging of the presurgical tumor and reduce the required extentof axillary dissection (2). Studies have shown that pathologiccomplete response (pCR) predicts patient survival (3, 4), andthe FDA now allows use of the pCR endpoint to supportaccelerated approval of drugs for high-risk early-stage breastcancer (5). Importantly, NAC enables tumor response andchemotherapy effectiveness to be assessed on an individualpatient basis, allowing oncologists to optimize treatment strat-egy and improve patient outcome.
In current clinical practice, NAC response assessment is deter-mined predominantly by serial physical examination, mammog-raphy, and/or ultrasound. Yeh and colleagues (6) showed thatpalpation, mammography, ultrasound, and MRI had 19%, 26%,35%, and 71% agreement, respectively, with final pathologicresponse. These and other studies have shown that anatomicchanges in tumor presentation are not reliable predictors of finalpathologic state (7–9). Functional measurements of tumors fromcontrast-enhanced MRI (10), magnetic resonance spectroscopy(MRS; refs. 11, 12), and PET (13, 14) have shown substantial
1Beckman Laser Institute and Medical Clinic, University of CaliforniaIrvine, Irvine, California. 2Department of Biostatistics and Center forStatistical Sciences, Brown University School of Public Health, Prov-idence, Rhode Island. 3Department of Pathology, University of South-ern California, California. 4Department of Medicine, University of Cali-fornia Irvine, Irvine, California. 5Department of Biomedical Engineer-ing, Boston University, Boston, Massachusetts. 6Department of Diag-nostic Radiology, University of Texas MD Anderson Cancer Center,Houston, Texas. 7Thayer School of Engineering, Dartmouth College,Hanover, New Hampshire. 8Section of Hematology and Oncology,Dartmouth-Hitchcock Medical Center, Norris Cotton Cancer Center,Lebanon, New Hampshire 9Department of Physics and Astronomy,University of Pennsylvania, Philadelphia, Pennsylvania. 10Departmentof Radiology, University of Pennsylvania, Philadelphia, Pennsylvania.11Center for Statistical Sciences, Brown University School of PublicHealth, Providence, Rhode Island. 12Department of Radiology, Univer-sityofCalifornia, SanFrancisco,California. 13DepartmentofRadiology,Massachusetts General Hospital, Harvard Medical School, Boston,Massachusetts. 14Hematology Oncology, Massachusetts General Hos-pital, Harvard Medical School, Boston, Massachusetts.
Note: Supplementary data for this article are available at Cancer ResearchOnline (http://cancerres.aacrjournals.org/).
Corresponding Author: Bruce J. Tromberg, Beckman Laser Institute and Med-ical Clinic, University of California, Irvine, 1002 Health Sciences Road, Irvine, CA92612. Phone: 949-824-8705; Fax: 949-824-8413; E-mail: [email protected]
doi: 10.1158/0008-5472.CAN-16-0346
�2016 American Association for Cancer Research.
CancerResearch
www.aacrjournals.org 5933
on June 25, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 15, 2016; DOI: 10.1158/0008-5472.CAN-16-0346

improvement over conventional anatomic imaging.However, thecost, radiation exposure, and/or potential toxicities of contrastagents limit the frequency of these scans. Optical imaging offers alow-cost, risk-free approach that could be used as a "bedside"adjunct to these methods.
Currently, morphologic criteria are the only clinical care stan-dards for evaluating therapeutic efficacy of NAC. Prior studieshave indicated that functional and molecular measures mayprovide an early indicator of breast cancer therapy response inthe neo-adjuvant setting. Studies support the potential value ofproliferation biomarkers, including imaging markers (15), aspredictors of therapeutic response (16, 17).Other imaging studiesindicate that early changes in blood flow and tumor metabolismpredict subsequent response and provide an early marker forcellular response to treatment (10–12, 18). Taken together, evi-dence suggests that early (24 to 72 hours) tumor biochemicalchanges precede volumetric changes in response to cancer ther-apies (19, 20). These early biochemical changes may provide apathway for predicting final pathologic outcome (20). Earlyclassification of therapeutic effectiveness could increase patientsurvival and minimize unnecessary damage to sensitive tissues(e.g., heart, liver, brain) caused by ineffective therapeutic strate-gies. This opportunity motivates the development of accurateimaging predictors of pCR and pathologic nonresponse.
Diffuse optical imaging (DOI) technology, a potential candi-date to address this clinical need, uses red and near-infrared (NIR)light (�600–1,000 nm) to probe tissue absorption and scatteringproperties at depths up to several centimeters (21). Absorptionand scattering properties in this regime characterize tissue struc-ture and function. Analogous to MRS and MRI, diffuse opticalspectroscopic imaging (DOSI) is a specialized DOI technologythat performshigh-resolution spectroscopy from650 to 1000nm,where oxy- and deoxy-hemoglobin, water, and lipid have prom-inent absorption features. These endogenous components varysignificantly in abundance and molecular state between breastcancer and normal tissue (22–26) and unique cancer-specificabsorption signatures not found in normal breast have beenobserved (27). DOSI-measured tumor water concentration andwater binding state were shown to scale with the NottinghamBloom–Richardson histopathology score and appear to be pro-portional to tissue cellularity and extracellular matrix composi-tion (22, 28). Hemoglobin, water, and bulk lipid componentshave been shown to be sensitive to microvasculature, cellularmetabolism, angiogenesis, edema, hypoxia, and necrosis in sev-eral single-center studies and provide tumor contrast thatcan change significantly with the growth and regression of tumors(22, 29–35). Quantitative, optical functional endpoints are easyto interpret and offer objective measures to predict therapeuticoutcome and minimize patient toxicity. For instance, tissueoptical index (TOI; compound function of deoxy-hemoglobin,water, and lipid tissue concentrations), which describes tissuemetabolism, structure, and cellularity, has been shown to be apromising imaging endpoint that significantly decreases by mid-therapy and can be used for predicting NAC response (36).Response to chemotherapy significantly correlatedwith adecreasein TOI by mid-therapy. The biological origins of this TOI signalchange are NAC-induced reductions in tumor cellular density andedema (reduced water content), re-normalization of breast adi-pose displaced by the tumor (increased lipid fraction), anddecreased levels of deoxyhemoglobin due to a loss of metabol-ically active tumor cells. Any DOI instrument that uses the
appropriate wavelength bands to retrieve hemoglobin, water, andlipid information can calculate TOI. Because DOSI is a relativelyinexpensive, portable, risk-free technology, it can be used fre-quently at the bedside, potentially creating new opportunities forpatients to receive personalized treatment and for physicians togain insight into response mechanisms. These features have beenhighlighted in several single-center studies and they motivatedAmerican College of Radiology Imaging Network (ACRIN)6691, which was designed to evaluate whether quantitativeDOSI measurements can be conducted in a prospective, mul-ticenter trial setting to predict therapeutic response in breastcancer patients undergoing NAC. The primary aim was toevaluate whether the baseline to mid-therapy change of theDOSI-derived TOI could predict pCR. The secondary aimsinvestigate the utility of additional DOSI measurements oftumor biochemical composition, obtained both at baselineand other time-points, for predicting pCR.
Patients and MethodsSubject eligibility and enrollment
Seven institutions were approved to enroll a total of 60 femalebreast cancer patients: Dartmouth Hitchcock Medical Center(Dartmouth), Massachusetts General Hospital (MGH), Univer-sity of California Irvine (UCI), University of California SanFrancisco (UCSF), University of Pennsylvania (UPenn), BostonUniversity (BU), and MD Anderson Cancer Center (MDACC).Enrollment began in June 2011 and completed in June 2013. Allinstitutions activated concurrently, exceptMDACCandBU,whichjoined the study in January and May 2013, respectively.
Eligible subjects were females age 18 years or olderwith biopsy-proven invasive breast cancer of at least 2 cm in the greatestdimension (as measured by palpation or standard breast imagingtechniques), whoplanned to receiveNAC followedby surgery.Norestrictions were placed on menopausal status, tumor stage, ortumor subtype/pathology. For this study, the chemotherapy reg-imen was determined by the treating oncologist, and regimenscontaining at least one cytotoxic chemotherapeutic agent wererequired. Neoadjuvant hormonal therapy or other targeted agentsalone in the absence of cytotoxic chemotherapy was not allowed.Potential subjects who received previous treatments, such aschemotherapy, endocrine therapy, radiation, or surgery (exclud-ing breast augmentation) to the involved breast were excludedfrom the study. In addition,womenwhowere pregnant or nursingwere excluded. All subjects provided written informed consent.The HIPAA-compliant protocol and informed consent wereapproved by the American College of Radiology InstitutionalReview Board, the NCI Cancer Therapy Evaluation Program(CTEP), and each site's Institutional Review Board.
DOSIInstrumentation. DOSI measurements were performed with sys-tems that combine frequency domain photonmigration (FDPM)and broadband NIR (650–1000 nm) spectroscopy for quantita-tive, model-based measurement of tissue absorption and scatter-ing properties and recovery of tissue oxy-hemoglobin (ctHbO2),deoxy-hemoglobin (ctHHb), water, and lipid. The full technicaldetails of the system are described elsewhere (37). Standardizedprocedures were developed for data collection and to monitorinstrument performance. Three sets of three calibration measure-ments on two custom-fabricated solid breast-tissue simulating
Tromberg et al.
Cancer Res; 76(20) October 15, 2016 Cancer Research5934
on June 25, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 15, 2016; DOI: 10.1158/0008-5472.CAN-16-0346

phantoms (InstitutNational d'Optique,Quebec, Canada; andUCIrvine Beckman Laser Institute, CA) and on one reflectance stan-dard (SRS-99-020, Labsphere Inc.) were performed before, mid-way and after each subject measurement. The breast tissue sim-ulating phantoms and reflectance standards used at all sites wereidentical. These measurements were used for determining instru-ment response-function, cross-calibration between instruments,andmonitoring instrument performance over the duration of thestudy (38). Dartmouth, MGH, UCI, UCSF, and UPenn usedidentical DOSI instruments. MDACC and BU, which joined thetrial about 1.5 years after the first patient enrollment, used asmaller, portable version with equivalent features and perfor-mance to the original five DOSI instruments. The handheld DOSIprobe that is scanned on the breast for data collection wasidentical for all instruments. A group of trainers from UCI, whodeveloped the DOSI instruments, traveled to each site for initialinstrument setup and training.
Spectroscopy. The approach to DOSI data acquisition and analysishas been previously described (22), and is briefly summarizedhere. Concentrations of oxy-hemoglobin (ctHbO2), deoxy-hemo-globin (ctHHb), water (ctH2O), and bulk lipid were calculated byfitting a linear combination of their known molar extinctioncoefficient spectra to the tissue ma values derived from model-based fits of DOSI data (22). From these quantities, the totalblood volume (THb ¼ ctHHb þ ctHbO2), percent oxygen satu-ration (StO2), and TOI were calculated. The StO2 is the ratio ofctHbO2 to THb. TOI is defined as TOI ¼ ctHHb � ctH2O/lipid.Prior single-center studies have shown that TOI can provide hightumor to normal (T/N) tissue contrast and that changes in T/NTOI are sensitive to chemotherapy response (22, 36).Quantitativeimages of these local tissue concentrations and contrast function
were formed on a generic three-dimensional (3D) breast surfacefor visualization.
Imaging proceduresDOSI scans were performed prior to the start of the chemo-
therapy treatment (baseline), 5 to 10 days after the first cycle(early-), at a change in chemotherapy regimens or mid-waythrough a single regimen protocol (mid-), and within 3 weeksafter completion of the chemotherapy treatment but prior tosurgery (post-therapy). The mid-therapy DOSI measurement wasperformed at least 5 days after the completion of the last cycleprior to the mid-point, and prior to the first cycle after the mid-point. Early- and post-therapy scans were optional as they werenot required to analyze the primary aim.
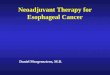
DOSI measurements were performed using a standard proto-col. Subjects were measured in a supine or reclining position. TheDOSI probe was placed against the breast tissue, and sequentialmeasurements were recorded in a rectangular grid pattern using10-mm spacing. Both breasts were specified to be measuredat each visit. The dimension of the grids ranged from 7 � 7 to15� 16 cm2 (i.e., 49 to 240measurement locations). The grid sizewas chosen to fully encompass the tumor anatomical extent (byultrasound or palpation) and to capture surrounding normaltissue. The grid on the noncancerous contralateral breast (normalside) was mirrored from the grid on the cancerous breast (tumorside). An example of DOSI imaging grid locations and theresulting images is provided in Fig. 1. For consecutive DOSI visits,individual static landmarks such as moles or freckles wererecorded on a transparency sheet and provided a fixed referenceto coregister the imaging grid at follow-up DOSI sessions. Afterinitial processing performed centrally by the UCI/ACRIN core lab(see section "Image Analysis"), DOSI data from each session were
Figure 1.
Example of DOSI measurement gridsand the corresponding TOI images(Subject 6691-21).
Optical Imaging of Breast Cancer Chemotherapy Response
www.aacrjournals.org Cancer Res; 76(20) October 15, 2016 5935
on June 25, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 15, 2016; DOI: 10.1158/0008-5472.CAN-16-0346

plotted using grid coordinates and heatmap functions inMATLAB. Linear interpolation was used to account for 10-mmspacing of grid points. The colored 2Dmapswere thenoverlaid ona 3D textured mesh of a realistic breast anatomic model with gridpoints drawn on it. The initial 3D image was obtained by using anX-box Kinect scanner for windows and accompanying SoftwareDevelopment Kit (Microsoft). Colored heatmaps obtained fromMATLAB were warped and overlaid on the textured mesh usingPhotoshop CS6 Extended (Adobe) to create the final images.
Histopathologic assessmentHistopathologic analysis of surgical specimens was performed
locally by each institution's pathologist. One central pathologist(UCI core) then reviewed all pathologic reports to assess individ-ual tumor response. The binary determination of pCRor non-pCRwas made based on evaluation of the pathology reports, and ifneeded, standard-of-care imaging reports. All determinationswere made blinded to DOSI imaging data. pCR was standardizedand defined as no residual of invasive disease present in thesurgically resected tissue (breast and lymph nodes) as perFDA guidelines (http://www.fda.gov/downloads/drugs/guidan-cecomplianceregulatoryinformation/guidances/ucm305501.pdf).Non-pCR included both partial and nonresponders. For the pur-poses of this report, only pCR status (0 or 1) was used to evaluateclinical outcome. Partial response characteristics will be furthercharacterized in future analyses of secondary aims.
Image analysisA single analyst fromUCI processed the deidentified raw DOSI
data centralized from all participating institutions, and recoveredthe mean and SD in tumor and normal tissue of all DOSIparameters. All DOSI data processing, including model-basedfits to raw data, calculation of breast tissue composition, andimage generation, was performed blinded with respect to clinicaloutcome on deidentified data by the UCI data core team. Theseprocessed data were transferred to the central ACRIN facility forfurther statistical analysis by the ACRIN Biostatistics Center. Fromthe DOSI images, two regions of interest (ROI) representingtumor and normal tissue were defined using an automatedalgorithm. DOSI parameters were determined by calculating themean of the measurement locations in each ROI. In this work, wefocus on the T/N ratio, which accounts for chemotherapy-inducedchanges in normal tissue.
As described in previous studies, the tumorROI consisted of thefull-width-at-half-maximum(FWHM) region around thebaselineTOI tumor peak (36). The DOSI measurement locations that hadgreater TOI values than a threshold equal to half the peak wereincluded in the tumor ROI. In addition, a continuity rule wasimplemented to define the tumor ROI: any location calculated aspart of the ROI but spatially disconnected (>2 cm away) wasexcluded from the ROI, and any location not meeting the thresh-old but surrounded by at least three other included points wasincorporated. The tumorROI sizewasfixed for all time-points, butthe tumor ROI could be translated up to 2 cm at later time-pointsto account for a shift in tumor TOI enhancement (due to asym-metric tumor shrinkage or grid misplacement on the breast). Thismethod was designed to capture the entire tumor region, butbecause the tumor size was longitudinally fixed, it overestimatesthe tumor extent at later time-points in responders. The normaltissue ROI was selected in the contralateral breast to mirror theipsilateral tumor ROI.
Statistical analysisSummary statistics including the mean, SD, median, and range
were computed for all DOSI markers. Logistic regression was usedtomodel the association between percent change in T/N TOI ratio(%TOITN) from baseline to mid-therapy and pathologic responsestatus (pCR vs. non-pCR). The resulting OR and 95% CI werereported. In addition, a receiver operating characteristic (ROC)curve was derived for %TOITN with pathologic response status asthe reference standard. Area under the ROC curve (AUC) and theassociated 95% confidence interval were computed empirically. Ifthe lower limit of the 95% CI for AUC was at least 0.50, then themarkerwas considered capableof differentiating pCRvs. non-pCR.
To account for the heterogeneous cohort, the predictive powerof %TOITN was evaluated further on two subsets of patientsstratified by baseline tumor tissue oxygen saturation (StO2),which is an optical parameter reflective of the tumor biophysicalstate. Tumor baseline StO2 has been shown to be a promisingpredictor for pCR at early time-points (33, 39). The median valueof baseline StO2 was used to stratify the subsets, with ROC curveand corresponding AUC reported for each subset. Evaluation ofbaseline StO2 alone and in combination with midpoint %TOITNwas a planned secondary aim of the study.
ACRIN 6691 was powered to detect an odds ratio of 3.0 using atwo-sided hypothesis test, a type I error rate of 0.05, and 90%power (PASS 2008). The resulting sample size was determined tobe 47 evaluable subjects. All tests were two-sided with P value<0.05 considered statistically significant. Statistical computationswere done using SAS 9.3 (SAS Institute) and R v3.1.0 (R project,http://www.r-project.com).
ResultsEnrollment information
The target accrual was met with 60 subjects enrolled in ACRIN6691. As depicted in Fig. 2, three subjects withdrew from thestudy. An additional 12 subjects were not included in the imaginganalysis because of the following DOSI scan issues: mandatorybaseline DOSI not performed (n ¼ 1), baseline DOSI non-evaluable (n ¼ 8), mandatory mid-therapy DOSI not performed(n ¼ 3). A DOSI scan was considered nonevaluable in case ofunrealistic physiological values, or incorrect instrument configu-ration. This decision was made on blinded, de-identified datausing instrument calibration and raw data QC reports. Of the 45eligible subjects with evaluable DOSI scans, one surgical pathol-ogy report after chemotherapy was not available. For another 10subjects, the DOSI scan of the contralateral breast was not per-formed due to insufficient time during the measurement sessionto complete the normal side breast scan, which was required inthis analysis for T/N values. The analysis, therefore, included 34subjects with evaluable DOSI scans and available pathologicresponse data from five different institutions (SupplementaryTable S1). Measurements at the two mandatory time-points toassess the primary aim, baseline, and mid-therapy were per-formed in 97% and 88% of all enrolled subjects, respectively(Supplementary Table S2). Despite being optional, measure-ments at early-therapy and post-therapy were performed in73% and 82% of all enrolled subjects, respectively.
Subject and tumor characteristicsTable 1 presents the characteristics of all enrolled subjects (n¼
60), and those subjects included in the analysis of the primary aim
Tromberg et al.
Cancer Res; 76(20) October 15, 2016 Cancer Research5936
on June 25, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 15, 2016; DOI: 10.1158/0008-5472.CAN-16-0346

(n ¼ 34). Among analyzed subjects, the average age was 48.4 �10.7 years (range 30–67 years), with 50% premenopausal, 3%perimenopausal, and 47% postmenopausal. The racial distribu-tion was 56%White, 24% Black, 12%Asian, and 9% of unknownrace; 15% of analyzed subjects were of Hispanic or Latino eth-nicity. Prechemotherapy tumor characteristics are also reportedin Table 1. IDC accounted for approximately 85% of the tumors(with or without a DCIS component, and including 6% of casesmixed with an ILC component) in the analysis group. Notably,approximately 71% of the tumors in the analysis group were ERþ.
The chemotherapy protocols undergone by the subjects werenot controlled in this study and, as a result, were highlyheterogeneous. Treatments for all subjects were based on cyto-toxic therapies. Targeted agents, such as Avastin (bevacizumab)or Herceptin (trastuzamab), could be used in combination ofthe cytotoxic agents. Hormonal therapies were not allowed. Atotal of 17 different chemotherapy protocols, including 12different drugs, were administered in the 34 evaluable cases.HER2 status was known in 25 of 34 (74%) analyzable subjects.Trastuzamab was administered to 10 of 11 (91%) HER2þ
tumors, and bevacizumab was administered to 1 of 2 (50%)triple-negative tumors.
Pathologic outcome statisticsAt surgery, 10 (29%) pCR and 24 (71%) non-pCRs were
included in the analysis group. A similar distribution of 15
(25%) pCRs was observed in all 60 enrolled subjects, with 5(8%) not undergoing surgery/lost to follow-up.
DOSI during NACFigure 3 presents two typical examples of a pCR and a non-
pCR measured using DOSI during NAC. The corresponding%TOITN is shown across NAC for both responses. Both subjectsexhibited relatively high baseline TOI levels of approximatelythree to four at tumor and arealor regions. The pCR subjectdemonstrated a greater %TOITN decrease at midpoint than thenon-pCR subject (�46% and �14%, respectively). Peak areolarTOI levels for subjects remained approximately the samethroughout therapy.
Response prediction—TOIT/N change from baseline tomid-therapy
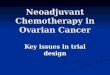
Among analyzable subjects, the distribution of %TOITN frombaseline to mid-therapy ranged from �82.4% to 320.8%, with amedian of �36.2%. The corresponding mean (SD) was �25.9%(67.2%). Figure 4A presents the distribution of %TOITN frombaseline to mid-therapy by pathologic response category. Onaverage, the pCR group exhibited a greater decrease in %TOITNthan the non-pCR group; however, large variability occurred in%TOITN in the non-pCR group.
The protocol-planned logistic regression analysis demonstrat-ed anOR for pCRpredictionof 1.4 (95%CI, 0.7–2.9;P¼0.40)per
Figure 2.
Enrollment to analysis flowchart.
Optical Imaging of Breast Cancer Chemotherapy Response
www.aacrjournals.org Cancer Res; 76(20) October 15, 2016 5937
on June 25, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 15, 2016; DOI: 10.1158/0008-5472.CAN-16-0346

SD increase in %TOITN. As strong evidence of model lack of fitexisted using continuous %TOITN, we explored using �40% todichotomize the population for the purpose of logistic regression,which was approximately equal to the median %TOITN across allsubjects. Patients who had a 40%or larger decrease in TOITN frombaseline to mid-therapy were more likely to be complete respon-ders than patients who experienced smaller decreases or increases,with an estimated odds ratio for pCR prediction of 4.7 (95% CI,0.9–23.0; P ¼ 0.059; see Table 2). The ROC AUC for pCR using%TOITN was 0.60 (95% CI, 0.39–0.81), suggesting this marker
does not exhibit good discriminatory ability for pCR in the entirecohort (Fig. 5A).
In the subset analysis, subjects were further stratified using themedian tumor StO2 at baseline (76.9%) as another binarymarker.Note that this median baseline tumor StO2 is similar to thethreshold value reported by Ueda and colleagues (39), 76.7%,whichhasbeen shown to correlatewithNAC response. Fig. 4B andC shows the distributions of %TOITN from baseline to mid-therapy by pathologic response category in each subset. Although%TOITN in patients with low baseline tumor StO2 did not cor-relate with pathologic response, a large decrease in %TOITN frombaseline tomid-therapy inpatientswith highbaseline tumor StO2
was associated with pCR. For 17 subjects with baseline StO2
greater than 76.9%, AUC was 0.83 (95% CI, 0.63–1.00; Fig.5C). These subjects were more likely to be complete respondersthanpatientswhoexperienced smaller decreases or increases,withan estimated OR for pCR prediction of 16.5 (95% CI, 1.1–250.2;P ¼ 0.043; see Table 2).
DiscussionACRIN6691 is thefirstmulticenter breast imaging trial utilizing
DOSI technology. As its primary aim, the trial was designed toevaluate whether %TOITN from baseline to mid-therapy waspredictive of the final pathologic response of breast cancer duringNAC. DOSI measurements were successfully performed longitu-dinally throughout NAC at six different institutions across theUnited States.
Standard-of-care NAC response is currently assessed usingchanges in anatomic tumor size. However, anatomic assessmenthas been shown to be an unreliablemetric of pathologic responseand arises after a measurable change in functional characteristics(7, 19, 20). Functional imaging techniques, such as dynamiccontrast enhanced (DCE) MRI and PET have shown better pre-dictive value than anatomic imaging methods (10, 40), but theyare costly, involve lengthy scan times, and require injection of acontrast agent,which limit availability andmeasurement frequen-cy. DOSI is a portable, noninvasive intrinsic-signal technique thatmonitors functional tumor response duringNACandmaypredictearly clinical outcome. Frequent longitudinal DOSI measure-ments were first reported to reveal dynamic tumor physiology(41), and validated the TOI endpoint in a single-site 34-subjectstudy by showing%TOITN is significantly different atmid-therapyfor pCR versus non-pCRNACpatients (36). Additional studies byseveral groups have confirmed the sensitivity of diffuse opticalmethods to breast cancer NAC response using both baseline anddynamic response measures (30–32, 42–48). Although thesestudies were completed with different instruments and NACprotocols, their common findings indicate that tumor cell metab-olism and vascularity are significantly altered during chemother-apy and optical methods are sensitive to several markers of thesechanges. For example, NAC-induced cellular damage alters tumoroxygen consumption and lowers tumor ctHHb; vascular damagecauses a decrease in tumor ctHbO2, and progressive loss ofcellularity and edema results in a decrease in tumorwater content.
The current multicenter clinical trial was devised to evaluateNAC response using a single, standardized DOSI platform andTOI endpoint. Extensive validation and performance assessmentfeatures were built into the study to evaluate the potential use ofDOSI technologies in patient management. As expected, weobserved that the 10 subjects achieving pCR exhibited dramatic
Table 1. Subject and tumor characteristics from initial pathology
Analysisgroup
All enrolledsubjects
N ¼ 34 N ¼ 60
Age, yearsMean � SD (range) 48.4 � 10.7
(30–67)48.9 � 11.0(28–69)
Menopausal status, n (%)Pre- 17 (50) 29 (48)Peri- 1 (3) 4 (7)Post- 16 (47) 26 (43)Unknown 0 (0) 1 (2)
Race, n (%)White 19 (56) 37 (62)Black/African-American 8 (24) 12 (20)Asian 4 (12) 7 (12)Native Hawaiian/Pacific Islander 0 (0) 1 (2)Unknown 3 (9) 3 (5)
Ethnicity, n (%)Hispanic/Latino 5 (15) 7 (12)Non-Hispanic/Latino 29 (85) 53 (88)
Histologic findings, n (%)IDC 16 (47) 34 (57)ILC 3 (9) 3 (5)DCIS/IDC 11 (32) 16 (27)IDC/ILC 2 (6) 2 (3)Other/not available 2 (6) 5 (8)
ER status, n (%)Positive 24 (71) 41 (68)Negative 7 (21) 13 (22)Unknown 3 (9) 5 (8)Not available 0 (0) 1 (2)
PR status, n (%)Positive 19 (56) 34 (57)Negative 12 (35) 20 (33)Unknown 3 (9) 5 (8)Not available 0 (0) 1 (2)
Ki67 status, n (%)Positive 17 (50) 23 (38)Negative 2 (6) 3 (5)Unknown 15 (44) 33 (55)Not available 0 (0) 1 (2)
Her2 status, n (%)0 4 (12) 9 (15)1 8 (24) 14 (23)2 8 (24) 12 (20)3 4 (12) 6 (10)Unknown/not available 10 (29) 19 (32)
Fish status, n (%)Amplified 7 (21) 9 (15)Nor amplified 14 (41) 29 (48)Unknown/not available 13 (38) 22 (37)
Areolar tumor, n (%)Areolar tumor 17 (50) 31 (52)Nonareolar tumor 17 (50) 27 (45)N/A (DOSI not performed) 0 (0) 2 (3)
NOTE: Data are numbers of subjects, with percentages in parentheses.
Tromberg et al.
Cancer Res; 76(20) October 15, 2016 Cancer Research5938
on June 25, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 15, 2016; DOI: 10.1158/0008-5472.CAN-16-0346

decreases in TOITN from baseline to mid-therapy. However,although many non-pCR tumors exhibited lesser TOITN changes,significant TOITN decreases were, nonetheless, observed in someof the non-pCR tumors. Although a previous single-site studyusing identical DOSI technology showed %TOITN was signifi-cantly different at mid-therapy for pCR versus non-pCR patients(36), the variability among non-pCR subjects limited the abilityof %TOITN to discriminate between pCR and non-pCR in themulticenter setting. This outcomemay be due to factors that werenot controlled for in this study including diverse tumor biology,widely varying chemotherapy regimens, and the fact that patho-logic response is performed on a microscopic level. Nevertheless,pCR has been recognized by the FDA as a validated endpoint forevaluatingdrug efficacy and it is a surrogate for 5-year survival. ThepCR endpoint has been used in a similar manner to test andvalidate several imaging technologies including PET, MRI, andultrasound for monitoring and predicting NAC response. Several
previous ACRIN NAC trials of experimental imaging endpointshave been based on pCR including ACRIN 6657 for MRI andACRIN 6688 for PET.
The importance of studying individual NAC treatmentresponse is supported by recent work, which suggests that pCRmay not be correlated with disease-free survival in certain NACagents (49). The %TOITN variability we observe is primarily aresult of the diverse responses observed in the non-pCR group,which includes subjects who have a significant tumor burden,as well as subjects with only small clusters of remaining tumorcells. A more refined clinical assessment of the non-pCR groupusing a continuously variable endpoint, such as the residualcancer burden (50) or the Miller-Payer system (51), could leadto a better understanding of the non-pCR TOITN changes, andto a better separation of %TOITN between response groups. Thetotal number of non-pCR subjects is too small, however, toconduct such an examination in this study. In addition, 17 out
Figure 3.
A, DOSI images throughout NAC for a pCR (6691-08) and a non-pCR (6691-13) subject. Scale bar illustrates TOI values. B, percent change in TOITN, HHbTN, H2OTN,LipidTN from baseline for both subjects. Error bars represent the SD of multiple measurement locations defined by the ROI for each subject (25 and 28 locations for6691-08 and 6691-13, respectively).
Optical Imaging of Breast Cancer Chemotherapy Response
www.aacrjournals.org Cancer Res; 76(20) October 15, 2016 5939
on June 25, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 15, 2016; DOI: 10.1158/0008-5472.CAN-16-0346

of the 34 evaluable tumors were involved to some degree in theareolar complex. In premenopausal females, the areolar regionis metabolically active, and, in some cases, it has been shown toexhibit NAC induced changes in metabolism measured usingDOSI (52). Our results suggest that there is a trend towarddifferential performance of %TOITN in areolar versus nonar-eolar tumors, with better discriminatory ability in non-areolar
tumors (ROC AUC ¼ 0.52; 95% CI, 0.18–0.85 vs. ROC AUC ¼0.70; 95% CI, 0.43–0.97); however, given the small sample sizein each subset (N ¼ 17), there was large variability in the pointestimates and this difference was not statistically significant(P ¼ 0.41). A larger sample size would be needed to confirmthis trend. Nevertheless, the large magnitude of tumor changesobserved in non-pCR subjects with retroareolar tumors may, inpart, be due to the response of metabolically active areolarbreast tissue combined with adjacent involved tumor. Thesefactors impact the magnitude of the tumor response measuredusing DOSI and they underscore the importance of controllingthe environment (tumor type, chemotherapy protocol, etc.) tooptimally predict therapeutic response.
Hypoxia, characterized in part by low StO2 levels, is oftenpresent in locally advanced breast tumors due to a combinationof abnormal tumor microvessels, elevated tumor metabolism,and high tumor osmotic pressures (53). Previous studies haveshown that prechemotherapy tumor oxygen saturation (39)and total hemoglobin (48) may be good prognostic tools for
Overall (n = 34) Baseline tumor SAT ≤ median (n = 17) Baseline tumor SAT > median (n = 17)
Pathologic response Pathologic response Pathologic response
n = 24 n = 12 n = 12n = 5 n = 5n = 10
Non-CR Non-CR Non-CRCR CR CR
–50
0
50
–50
0
50
–50
0
50
% C
hang
e in
TO
I rat
io (T
/N):
mid
-ther
apy
% C
hang
e in
TO
I rat
io (T
/N):
mid
-ther
apy
% C
hang
e in
TO
I rat
io (T
/N):
mid
-ther
apy
A B C
Figure 4.
Boxplot of percent change from baseline to mid-therapy in TOITN (%TOITN) by final pathologic status, dichotomized as pCR vs. non-pCR. A, in the overallevaluable dataset. B, in the subset of evaluable cases with baseline tumor oxygenation lower than the median value. C, in the subset of evaluable cases withbaseline tumor oxygenation greater than the median value.
Table 2. Summary of odds ratios and significance for predicting pCR fromlogistic regression using percent change from baseline to mid-therapy in TOITN(%TOITN)
DOSI endpoint binarymarker
Numberof subjects OR (95% CI) P
(A) %TOITN � �40% 34 4.7 (0.9–23.0) 0.059(B) %TOITN � �40% andbaseline StO2 >76.9%
17 16.5 (1.1–250.2) 0.043
NOTE: (A), %TOITN dichotomized at�40%; (B), %TOITN dichotomized at�40%for the subset of evaluable subjects with baseline tumor StO2 > 76.9%. (i.e.,population median).
Tromberg et al.
Cancer Res; 76(20) October 15, 2016 Cancer Research5940
on June 25, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 15, 2016; DOI: 10.1158/0008-5472.CAN-16-0346

predicting therapeutic outcome. Here, the data also suggest thattumor oxygen saturation plays an important role in predictingpCR. Improved pCR prediction was observed when performingthe primary analysis on tumors with baseline tumor oxygensaturation greater than the median value (77%). This predic-tion was not possible in subjects with baseline tumor oxygensaturation <77%. These results suggest that baseline tumoroxygen saturation may be important in stratifying the popu-lation for evaluating DOSI response. Overall, baseline tumorStO2 appears to be an important imaging biomarker that can beused in combination with dynamic changes to predict clinicaloutcome. However, the underlying origin of this response is notyet known. The predictive power of the %TOITN dynamicresponse may be restricted to well-oxygenated tumors becauseof technical reasons related to DOSI, or because of the biolog-ical advantage of oxygenation. Establishing threshold criteriafor baseline DOSI measurements could play an important rolein interpreting the tumor dynamic response and, ultimately,employing DOSI to improve patient outcome. Establishingpredictive thresholds is expected to be sensitive to both thetechnology employed and the patient population. Their prac-tical use in clinical management and outcome prediction willdepend on whether baseline parameters can be clearly definedboth within and across technology platforms and this shouldbe the focus of future studies.
To assess the uniqueness of DOSI endpoints, our results wereevaluated for the possible confounders of pretreatmentmolecularsubtype and tumor size. Both have beenusedpreviously to stratifypatient therapeutic response predictions (54, 55). No associationwas found between baseline tumor oxygen saturation andmolec-ular subtype in the 31 of 34 evaluable patients where these datawere available (P ¼ 0.41 for ER status and P ¼ 1.0 for PR statusfrom Fisher exact test). Low correlation also occurred betweenbaseline tumor oxygen saturation and tumor size (measured byultrasound) in the 19 of the 34 patients where baseline tumor sizewas available (Spearman correlation ¼ �0.39, P ¼ 0.10).
Studies have shown that diffuse optical techniques are sen-sitive to breast tissue composition changes during the men-strual cycle (56–58). To account for these biological changesand for chemotherapy-induced changes in normal tissue, thetumor-to-normal ratio was reported. This resulted in 10 sub-jects excluded from the analysis due to the absence of contra-lateral tissue measurement. As part of the secondary aims,changes of tumor values rather than T/N ratio will be reportedin future analysis. However, the preliminary results were not aspromising as the ratiometric analysis.
Study limitationsImportant study limitations were the diversity of the patient
population, heterogeneity of tumor molecular subtypes, and
Figure 5.
A–C, ROC curves for pCR usingpercent change from baseline to mid-therapy in TOITN (%TOITN) in theoverall evaluable dataset (A), in thesubset of evaluable cases withbaseline tumor saturation lower thanthemedian value (B), and in the subsetof evaluable caseswith baseline tumorsaturation greater than the medianvalue (C). The reference standard iscoded as follows: 0 ¼ pCR and1 ¼ non-pCR.
Optical Imaging of Breast Cancer Chemotherapy Response
www.aacrjournals.org Cancer Res; 76(20) October 15, 2016 5941
on June 25, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 15, 2016; DOI: 10.1158/0008-5472.CAN-16-0346

lack of standardized chemotherapy regimens. In addition, theadequate sample size was determined to be 47 subjects; how-ever, only 34 of the 60 enrolled cases were assessed as analyz-able. Because this study was the first multicenter trial that testedlongitudinal DOSI measurements during NAC, much effortwas focused on instrument and procedure standardization.Each instrument was fabricated and tested at University ofCalifornia Irvine, using a common set of tissue-simulatingphantoms before delivery to the study site. Preliminary analysisdemonstrated <1% variability in broadband DOSI over 1 hour(typical patient measurement time-frame), <5% variability over4 months (typical chemotherapy measurement time-frame),and <6% variability over the 2-year study duration. Althoughoperators at all institutions were trained to perform standardmeasurement procedures, clinical DOSI data were in general ofpoor quality for the first few subjects. Data quality improvedwith more practice and feedback, nevertheless, the number ofnonevaluable cases was primarily due to operator error that ledto incorrect instrument settings and poor data quality, as well asclinical work-flow time pressures that resulted in lack of normalside data on several subjects. Also, a large disparity in subjectenrollment occurred across institutions: UCI and MDACCenrolled about two thirds of the subjects, whereas MGH andUCSF enrolled a total of three and two subjects, respectively. Asthe technique and instrument become more standardized, andthrough the experience gained with this study, ease-of-use isexpected to improve, and the number of nonevaluable cases isexpected to decline in future multicenter studies. Finally, tumordimensions by ultrasound matching the DOSI scan date at �2weeks (at baseline and mid-therapy) were available for only 12subjects. Of those, only two were pCR, limiting our ability tomake a DOSI–ultrasound comparison.
Future analysisAnalysis of ACRIN 6691 secondary aims is ongoing, including
examining other DOSI dynamic response endpoints, baselineparameters, and molecular subtype. Further analyses will alsoexplore the development of new indices to report tumor changes.Finally, the tumor ROI used in this study was obtained with analgorithm based on the FWHM around the baseline (preche-motherapy) TOI peak. Although some groups have explored theimpact of different ROIs on NAC prediction of DOI (31, 32),currently no standardized method exists to determine tumor ROIinDOSI data. The effect of ROI choicewill, therefore, be examinedin future work.
ConclusionAs an experimental cancer imaging technology, DOSI has
been tested for the first time in ACRIN 6691, an independently-executed, prospective multicenter trial of breast cancer NAC.The results demonstrated that although a range of responses toNAC were observed in this heterogeneous patient population,subjects exhibiting a greater drop in %TOITN from baseline tomid-therapy were more likely to have a pCR to NAC. Althoughthis change alone was not a strong predictor of clinical outcomefor the full patient population, its performance was substan-tially improved when patients were stratified according tobaseline tumor oxygen saturation levels. Importantly, the samedynamic %TOITN change was unable to predict pCR in subjectswith baseline tumor oxygen saturation lower than the median
value. This finding suggests that stratification using baselinetumor properties, especially oxygenation, can be used toimprove DOSI therapy response predictions for individualsubjects, particularly among diverse patient populations andNAC treatment strategies.
Disclosure of Potential Conflicts of InterestB.J. Tromberg reports receiving a commercial research grant from LG
Electronics, has ownership interest (including patents) in intellectual prop-erty related to breast imaging assigned to UC Regents, and is a consultant/advisory board member for Hamamatsu Photonics. A.E. Cerussi has own-ership interest (including patents) in intellectual property related to breastimaging assigned to UC Regents. W. Yang is a is a consultant/advisoryboard member for General Electric Healthcare and Devicor. K.D. Paulsenhas ownership interest (including patents) in Intellectual Property relatedto breast imaging, CairnSurgical, and MIST, Inc. No potential conflicts ofinterest were disclosed by the other authors.
Authors' ContributionsConception and design: B.J. Tromberg, Z. Zhang, A.E. Cerussi, R.S. Mehta,D. Roblyer, K.D. Paulsen, A.G. Yodh, S.H. Chung, M. Schnall, S.J. Isakoff,D. MankoffDevelopment of methodology: B.J. Tromberg, T.D. O'Sullivan, A.E. Cerussi,D. Roblyer, K.D. Paulsen, A.G. YodhAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): A. Leproux, T.D. O'Sullivan, R.S. Mehta, W. Yang,K.D. Paulsen, B.W. Pogue, S. Jiang, P.A. Kaufman, A.G. Yodh, N. Hylton,D.A. Boas, S.A. Carp, S.J. IsakoffAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): Z. Zhang, A. Leproux, T.D. O'Sullivan, P.M. Carpen-ter, D. Roblyer, S. Jiang, P.A. Kaufman, B.S. Snyder, S.J. Isakoff, D. MankoffWriting, review, and/or revision of the manuscript: B.J. Tromberg, Z. Zhang,A. Leproux, T.D. O'Sullivan, P.M. Carpenter, R.S. Mehta, W. Yang, K.D. Paulsen,P.A. Kaufman, A.G. Yodh, S.H. Chung, M. Schnall, B.S. Snyder, N. Hylton,S.A. Carp, S.J. Isakoff, David MankoffAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): Z. Zhang, A. Leproux, T.D. O'Sullivan,A.E. Cerussi, B.W. Pogue, S.H. Chung, M. Schnall, S.A. CarpStudy supervision: B.J. Tromberg, A. Leproux, T.D. O'Sullivan, A.E. Cerussi,R.S. Mehta, D. Roblyer, W. Yang, P.A. Kaufman, A.G. Yodh, D. MankoffOther (review and analysis of pathology reports, contribution of studydefinitions): P.M. Carpenter
AcknowledgmentsThe authors thank the entire ACRIN staff for their generous support in
completing this study, including Donna Hartfeil, Sharon Mallet, and DunstanHorng; UCI coordinatorsMontana Compton, Erin Sullivan, and Jennifer Ehren;UCI engineers Amanda Durkin and Brian Hill; clinical coordinators at all sites,and the patients who generously volunteered their time for this study.
Grant SupportThis research was supported by the American College of Radiology Imaging
Network, ACRIN, which receives funding from the National Cancer Institute(NCI) through the grants U01 CA079778 and U01 CA080098 (clinical trialinformation: NCT01217385), theNational Institute of Biomedical Imaging andBioengineering (P41EB015890), the National Cancer Institute (R01CA142989,U54CA136400), and the Chao Family Comprehensive Cancer Center(P30CA62203), and programmatic support from the Arnold and Mabel Beck-man Foundation.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received February 8, 2016; revised June 9, 2016; accepted July 3, 2016;published OnlineFirst August 15, 2016.
Tromberg et al.
Cancer Res; 76(20) October 15, 2016 Cancer Research5942
on June 25, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 15, 2016; DOI: 10.1158/0008-5472.CAN-16-0346

References1. Gralow JR, Zujewski JA, Winer E. Preoperative therapy in invasive breast
cancer: reviewing the state of the science and exploring new researchdirections. J Clin Oncol 2008;26:696–7.
2. Sledge GW, Mamounas EP, Hortobagyi GN, Burstein HJ, Goodwin PJ,Wolff AC. Past, present, and future challenges in breast cancer treatment.J Clin Oncol 2014;32:1979–86.
3. Esserman LJ, Berry DA, Cheang MC, Yau C, Perou CM, Carey L, et al.Chemotherapy response and recurrence-free survival in neoadjuvant breastcancer depends on biomarker profiles: results from the I-SPY 1 TRIAL(CALGB 150007/150012; ACRIN 6657). Breast Cancer Res Treat 2012;132:1049–62.
4. Rastogi P, Anderson SJ, Bear HD, Geyer CE, Kahlenberg MS, Robidoux A,et al. Preoperative chemotherapy: updates of national surgical adjuvantbreast and bowel project protocols B-18 and B-27. J Clin Oncol2008;26:778–85.
5. U.S. Food and Drug Administration. Available from: http://www.fda.gov/downloads/drugs/guidancecomplianceregulatoryinformation/guidances/ucm305501.pdf.
6. Yeh E, Slanetz P, Kopans DB, Rafferty E, Georgian-Smith D, Moy L, et al.Prospective comparison of mammography, sonography, and MRI inpatients undergoing neoadjuvant chemotherapy for palpable breast cancer.Am J Roentgenol 2005;184:868–77.
7. Vinnicombe SJ, MacVicar AD, Guy RL, Sloane JP, Powles TJ, Knee G, et al.Primary breast cancer: mammographic changes after neoadjuvant chemo-therapy, with pathologic correlation. Radiology 1996;198:333–40.
8. Helvie MA, Joynt LK, Cody RL, Pierce LJ, Adler DD, Merajver SD, et al.Locally advanced breast carcinoma: accuracy of mammography versusclinical examination in the prediction of residual disease after chemother-apy. Radiology 1996;198:327–32.
9. Feldman LD, Hortobagyi GN, Buzdar AU, Ames FC, Blumenschein GR.Pathological assessment of response to induction chemotherapy in breastcancer. Cancer Res 1986;46:2578–81.
10. Hylton NM, Blume JD, Bernreuter WK, Pisano ED, Rosen MA, Morris EA,et al. Locally advancedbreast cancer:MR imaging for predictionof responseto neoadjuvant chemotherapy—results from ACRIN 6657/I-SPY TRIAL.Radiology 2012;263:663–72.
11. Chenevert TL, Stegman LD, Taylor JM, Robertson PL, Greenberg HS,Rehemtulla A, et al. Diffusion magnetic resonance imaging: an earlysurrogate marker of therapeutic efficacy in brain tumors. J Natl CancerInst 2000;92:2029–36.
12. Meisamy S, Bolan PJ, Baker EH, Bliss RL, Gulbahce E, Everson LI, et al.Neoadjuvant chemotherapy of locally advanced breast cancer: predictingresponsewith in vivo 1HMRspectroscopy—apilot study at 4 T 1. Radiology2004;233:424–31.
13. Mankoff DA, Dunnwald LK, Gralow JR, Ellis GK, Schubert EK, Tseng J, et al.Changes in blood flow and metabolism in locally advanced breast cancertreated with neoadjuvant chemotherapy. J Nucl Med 2003;44:1806–14.
14. McDermott GM,Welch A, Staff RT, Gilbert FJ, Schweiger L, Semple SI, et al.Monitoring primary breast cancer throughout chemotherapy using FDG-PET. Breast Cancer Res Treat 2007;102:75–84.
15. Kostakoglu L, Duan F, Idowu MO, Jolles PR, Bear HD, Muzi M, et al. Aphase II study of 30-Deoxy-30-18F-fluorothymidine PET in the assessmentof early response of breast cancer to neoadjuvant chemotherapy: resultsfrom ACRIN 6688. J Nucl Med 2015;56:1681–9.
16. Bozzetti C, Musolino A, Camisa R, Bisagni G, Flora M, Bassano C, et al.Evaluation of HER-2/neu amplification and other biological markers aspredictors of response to neoadjuvant anthracycline-based chemotherapyin primary breast cancer: the role of anthracycline dose intensity. Am J ClinOncol 2006;29:171–7.
17. Burcombe R, Wilson GD, Dowsett M, Khan I, Richman PI, Daley F, et al.Evaluation of Ki-67 proliferation and apoptotic index before, during andafter neoadjuvant chemotherapy for primary breast cancer. Breast CancerRes 2006;8:31–3.
18. Dose-Schwarz J, TilingR, Avril-Sassen S,Mahner S, LebeauA,WeberC, et al.Assessment of residual tumour by FDG-PET: conventional imaging andclinical examination following primary chemotherapy of large and locallyadvanced breast cancer. Br J Cancer 2009;102:35–41.
19. SymmansWF, VolmMD, Shapiro RL, Perkins AB, KimAY, Demaria S, et al.Paclitaxel-induced apoptosis and mitotic arrest assessed by serial fine-
needle aspiration: implications for early prediction of breast cancerresponse to neoadjuvant treatment. Clin Cancer Res 2000;6:4610–7.
20. Archer C, PartonM, Smith IE, Ellis PA, Salter J, Ashley S, et al. Early changesin apoptosis and proliferation following primary chemotherapy for breastcancer. Br J Cancer 2003;89:1035–41.
21. O'Sullivan TD, Cerussi AE, CucciaDJ, Tromberg BJ. Diffuse optical imagingusing spatially and temporally modulated light. J Biomed Opt 2012;17:0713111–4.
22. Cerussi A, Shah N, Hsiang D, Durkin A, Butler J, Tromberg BJ. In vivoabsorption, scattering, and physiologic properties of 58 malignant breasttumors determined by broadband diffuse optical spectroscopy. J BiomedOpt 2006;11:044005.
23. Srinivasan S, Pogue BW, Brooksby B, Jiang S, Dehghani H, Kogel C, et al.Near-infrared characterization of breast tumors in vivo using spectrally-constrained reconstruction. Technol Cancer Res Treat 2005;4:513–26.
24. Spinelli L, Torricelli A, Pifferi A, Taroni P, Danesini G, Cubeddu R.Characterization of female breast lesions from multi-wavelength time-resolved optical mammography. Phys Med Biol 2005;50:2489–502.
25. Taroni P, Danesini G, Torricelli A, Pifferi A, Spinelli L, Cubeddu R. Clinicaltrial of time-resolved scanning optical mammography at 4 wavelengthsbetween 683 and 975 nm. J Biomed Opt 2004;9:464–73.
26. Wang J, Jiang S, Li Z, diFlorio-Alexander RM, Barth RJ, Kaufman PA, et al.In vivo quantitative imaging of normal and cancerous breast tissue usingbroadband diffuse optical tomography. Med Phys 2010;37:3715–24.
27. Kukreti S, Cerussi A, Tromberg B, Gratton E. Intrinsic tumor biomarkersrevealed by novel double-differential spectroscopic analysis of near-infra-red spectra. J Biomed Opt 2007;12:020509.
28. Chung SH, Cerussi AE, Klifa C, Baek HM, Birgul O, Gulsen G, et al. In vivowater state measurements in breast cancer using broadband diffuse opticalspectroscopy. Phys Med Biol 2008;53:6713–27.
29. Cerussi A, Hsiang D, Shah N, Mehta R, Durkin A, Butler J, et al. Predictingresponse to breast cancer neoadjuvant chemotherapy using diffuse opticalspectroscopy. Proc Natl Acad Sci U S A 2007;104:4014–9.
30. ChoeR,CorluA, LeeK,Durduran T, Konecky SD,Grosicka-KoptyraM, et al.Diffuse optical tomography of breast cancer during neoadjuvantchemotherapy: a case study with comparison to MRI. Med Phys 2005;32:1128–39.
31. Falou O, SolimanH, Sadeghi-Naini A, Iradji S, Lemon-Wong S, Zubovits J,et al. Diffuse optical spectroscopy evaluation of treatment response inwomen with locally advanced breast cancer receiving neoadjuvant che-motherapy. Transl Oncol 2012;5:238.
32. Jiang S, Pogue BW, Carpenter CM, Poplack SP, Wells WA, Kogel CA, et al.Evaluation of breast tumor response to neoadjuvant chemotherapy withtomographic diffuse optical spectroscopy: case studies of tumor region-of-interest changes. Radiology 2009;252:551–60.
33. Roblyer D, Ueda S, Cerussi A, TanamaiW, Durkin A,Mehta R, et al. Opticalimaging of breast cancer oxyhemoglobin flare correlates with neoadjuvantchemotherapy response one day after starting treatment. ProcNatl Acad SciU S A 2011;108:14626–31.
34. Soliman H, Gunasekara A, Rycroft M, Zubovits J, Dent R, Spayne J, et al.Functional imaging using diffuse optical spectroscopy of neoadjuvantchemotherapy response in women with locally advanced breast cancer.Clin Cancer Res 2010;16:2605–14.
35. ZhuQ, TannenbaumS,HegdeP, KaneM,XuC, Kurtzman SH.Noninvasivemonitoring of breast cancer during neoadjuvant chemotherapy usingoptical tomography with ultrasound localization. Neoplasia 2008;10:1028–40.
36. Cerussi AE, Tanamai VW, Hsiang D, Butler J, Mehta RS, Tromberg BJ.Diffuse optical spectroscopic imaging correlates with final pathologicalresponse in breast cancer neoadjuvant chemotherapy. Philos Trans AMathPhys Eng Sci 2011;369:4512–30.
37. Bevilacqua F, Berger AJ, Cerussi AE, Jakubowski D, Tromberg BJ. Broad-band absorption spectroscopy in turbid media by combined frequency-domain and steady-state methods. Appl Opt 2000;39:6498–507.
38. Cerussi A, Durkin A, Kwong R, Quang T, Hill B, Tromberg BJ, et al. Qualitycontrol and assurance for validation of DOS/I measurements. BiOSConference 2010. p. 756703.
39. Ueda S, RoblyerD,Cerussi A,DurkinA, LeprouxA, Santoro Y, et al. Baselinetumor oxygen saturation correlates with a pathologic complete response in
Optical Imaging of Breast Cancer Chemotherapy Response
www.aacrjournals.org Cancer Res; 76(20) October 15, 2016 5943
on June 25, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 15, 2016; DOI: 10.1158/0008-5472.CAN-16-0346

breast cancer patients undergoing neoadjuvant chemotherapy. Cancer Res2012;72:4318–28.
40. Kurland BF,Gadi VK, Specht JM,AllisonKH, LivingstonRB, Rodler ET, et al.Feasibility study of FDG PET as an indicator of early response to aromataseinhibitors and trastuzumab in a heterogeneous group of breast cancerpatients. EJNMMI Res 2012;2:34.
41. Jakubowski DB, Cerussi AE, Bevilacqua F, Shah N, Hsiang D, Butler J, et al.Monitoring neoadjuvant chemotherapy in breast cancer using quantitativediffuse optical spectroscopy: a case study. J Biomed Opt 2004;9:230–8.
42. Carp S,WanyoCM, FangQ, BoasD, Isakoff SJ. Neoadjuvant chemotherapymonitoring using dynamic breast compression imaging. BiomedicalOptics Conference 2012. p. BW3A-7.
43. Enfield L, Cantanhede G, Douek M, Ramalingam V, Purushotham A,Hebden J, et al. Monitoring the response to neoadjuvant hormone therapyfor locally advanced breast cancer using three-dimensional time-resolvedoptical mammography. J Biomed Opt 2013;18:56012.
44. Jiang S, PogueBW,KaufmanPA,Gui J, JermynM, Frazee TE, et al. Predictingbreast tumor response to neoadjuvant chemotherapy with Diffuse OpticalSpectroscopic Tomography prior to treatment. Clin Cancer Res 2014;20:6006–15.
45. Pakalniskis MG, Wells WA, Schwab MC, Froehlich HM, Jiang S, Li Z, et al.Tumor angiogenesis change estimated by using diffuse optical spectro-scopic tomography: demonstrated correlation in women undergoingneoadjuvant chemotherapy for invasive breast cancer. Radiology 2011;259:365–74.
46. Schaafsma BE, van de GiessenM, Charehbili A, Smit VT, Kroep JR, LelieveldtBP, et al. Optical mammography using diffuse optical spectroscopy formonitoring tumor response to neoadjuvant chemotherapy in women withlocally advanced breast cancer. Clin Cancer Res 2015;21:577–84.
47. Xu C, Vavadi H, Merkulov A, Li H, Erfanzadeh M, Mostafa A, et al.Ultrasound-guided diffuse optical tomography for predicting and moni-toring neoadjuvant chemotherapy of breast cancers: recent progress. Ultra-son Imaging 2016;38:5–18.
48. Zhu Q,Wang L, Tannenbaum S, Ricci A Jr, DeFusco P, Hegde P. Pathologicresponse prediction to neoadjuvant chemotherapy utilizing pretreatmentnear-infrared imaging parameters and tumor pathologic criteria. BreastCancer Res 2014;16:456.
49. Berruti A, Amoroso V, Gallo F, Bertaglia V, Simoncini E, Pedersini R, et al.Pathologic complete response as a potential surrogate for the clinicaloutcome in patients with breast cancer after neoadjuvant therapy: ameta-regression of 29 randomized prospective studies. J Clin Oncol2014;32:3883–91.
50. Symmans WF, Peintinger F, Hatzis C, Rajan R, Kuerer H, Valero V, et al.Measurement of residual breast cancer burden to predict survival afterneoadjuvant chemotherapy. J Clin Oncol 2007;25:4414–22.
51. Ogston KN, Miller ID, Payne S, Hutcheon AW, Sarkar TK, Smith I, et al. Anew histological grading system to assess response of breast cancers toprimary chemotherapy: prognostic significance and survival. Breast2003;12:320–7.
52. O'Sullivan TD, Leproux A, Chen JH, Bahri S, Matlock A, Roblyer D, et al.Optical imaging correlateswithmagnetic resonance imaging breast densityand reveals composition changes during neoadjuvant chemotherapy.Breast Cancer Res 2013;15:R14.
53. Vaupel P, Briest S, H€ockel M. Hypoxia in breast cancer: pathogenesis,characterization and biological/therapeutic implications hypoxie beimmammakarzinom: pathogenese, charakterisierung und biologische/ther-apeutische Konsequenzen. Wien Med Wochenschr 2002;152:334–42.
54. Lips E, Mulder L, de Ronde JJ, Mandjes IA, Vincent A, Vrancken Peeters MT,et al. Neoadjuvant chemotherapy in ERþ HER2� breast cancer: responseprediction based on immunohistochemical and molecular characteristics.Breast Cancer Res Treat 2012;131:827–36.
55. Song I-H, LeeHJ, GongG. Pathologic response pattern of breast cancer afterneoadjuvant chemotherapy: its correlation with molecular subtypes. Can-cer Res 2014;74(19 Suppl):1880.
56. Shah N, Cerussi A, Eker C, Espinoza J, Butler J, Fishkin J, et al. Noninvasivefunctional optical spectroscopy of human breast tissue. Proc Natl Acad SciU S A 2001;98:4420–5.
57. Pogue BW, Jiang S, Dehghani H, Kogel C, Soho S, Srinivasan S, et al.Characterization of hemoglobin, water, andNIR scattering in breast tissue:analysis of intersubject variability and menstrual cycle changes. J BiomedOpt 2004;9:541–52.
58. CubedduR,D'AndreaC, Pifferi A, Taroni P, Torricelli A, Valentini G. Effectsof themenstrual cycle on the red and near-infrared optical properties of thehuman breast. Photochem Photobiol 2000;72:383–91.
Cancer Res; 76(20) October 15, 2016 Cancer Research5944
Tromberg et al.
on June 25, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 15, 2016; DOI: 10.1158/0008-5472.CAN-16-0346

2016;76:5933-5944. Published OnlineFirst August 15, 2016.Cancer Res Bruce J. Tromberg, Zheng Zhang, Anaïs Leproux, et al. Cancer: ACRIN 6691 Trial of Diffuse Optical Spectroscopic ImagingPredicting Responses to Neoadjuvant Chemotherapy in Breast
Updated version
10.1158/0008-5472.CAN-16-0346doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerres.aacrjournals.org/content/suppl/2016/08/13/0008-5472.CAN-16-0346.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerres.aacrjournals.org/content/76/20/5933.full#ref-list-1
This article cites 55 articles, 16 of which you can access for free at:
Citing articles
http://cancerres.aacrjournals.org/content/76/20/5933.full#related-urls
This article has been cited by 2 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/76/20/5933To request permission to re-use all or part of this article, use this link
on June 25, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 15, 2016; DOI: 10.1158/0008-5472.CAN-16-0346