Embed Size (px)
Citation preview

PRENATAL DIAGNOSIS, VOL. 13,87-91 (1993)
PRENATAL DIAGNOSIS OF DANDY-WALKER MALFORMATION IN A FAMILY DISPLAYING
X-LINKED INHERITANCE
T. COWLES, P. FURMAN AND I. WILKINS Department of Obstetrics. Gynecology, and Reproductive Sciences, University of Texas,
Medical School at Houston, Houston, TX 77030, U.S.A.
SUMMARY The diagnosis of Dandy-Walker malformation was made on the ultrasonographic evaluation of a 33-week male fetus. Pedigree analysis revealed a family history of isolated Dandy- Walker malformation in three other males, suggesting an X-linked recessive inheritance pattern.
KEY WORDS Dandy-Walker malformation X-Linked recessive inheritance Prenatal diagnosis
INTRODUCTION Dandy-Walker malformation (DWM) is a developmental abnormality of the central nervous system that includes hydrocephalus, partial or complete absence of the cerebellar vermis, and a posterior fossa cyst (Hart et al., 1972). DWM can occur as an isolated disorder, or in association with single gene disorders, chromosomal aberrations, or multiple malformation syndromes. We report a Dedigree which includes four males affected with isolated DWM and four obligate female carriers.
CASE REPORT The mother of the proband, a 19-year-old primigravida, presented for first-trimester genetic counselling at another centre with a family history of Down syndrome. Her karyotype was 46,XX without evidence of a translocation. She also gave a family history of hydrocephalus. Accordingly, the patient was encouraged to have a second-trimester ultrasound examination, which she did not obtain.
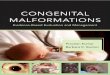
At 33 weeks’ gestation, she was referred to our centre because of suspected hydramnios. Ultrasound examination confirmed this finding and revealed a 33-week male fetus with DWM and associated severe hydrocephalus (Figure 1). A fetal blood sample was obtained and the karyotype was found to be 46,XY. Additional family history and medical records revealed three other males in the previous two gener- ations who had isolated DWM (Figure 2). CT scans on 111-5 revealed hydrocephalus and a posterior fossa cyst consistent with DWM; both 111-5 and 111-9 have required ventriculoperitoneal shunt placement. Although 11-6 had only limited care in Mexico, it is likely that he had a similar malformation, as he died at 1 year of age with an enlarging head.
Addressee for correspondence: Tracy Cowles, MD, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Texas, Medical School at Houston, 6431 Fannin, Suite 3.204, Houston, TX 77030, U.S.A.
0 197-385 1/93/020087-05$07.50 0 1993 by John Wiley & Sons, Ltd.
Received 5 March 1992 Revised 5 July 1992
Accepted 28 July 1992

88 T. COWLES ET AL.
Figure 1. Ultrasound demonstrating severe hydrocephalus and cerebellar hypoplasia
I
I1
I11
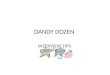
' I ' I- f-! DANDY-WALKER MALFORMATION
DOWN SYNDROME
Figure 2. Pedigree
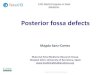
The male proband was delivered at 38 weeks by Caesarean section. He weighed 4820 g and had an extremely large frontal-occipital diameter of 54 cm (Figure 3). On the day of birth, an ultrasound evaluation of the cranial structures revealed massive dilatation of the lateral ventricles, a markedly thinned cerebral mantle, a large posterior fossa cyst, and small hypoplastic cerebellar hemispheres with absence of the cerebellar vermis. Computed tomographic studies the following day confirmed these findings. In addition, an inversion of the normal relationship of the torcular and lambdoidal sutures was noted. The corpus callosum was present. All of these findings were consistent with the diagnosis of severe DWM. A ventriculoperitoneal shunt was placed soon after birth and was revised at age 3 months.

PRENATAL DIAGNOSIS OF DANDY-WALKER MALFORMATION 89
Figure 3. Newborn with extreme macrocephaly
Table 1. Associations of DWM with other abnormalities
Mendelian syndromes Chromosomal abnormalities Environmental risk factors Multifactorial inheritance Sporadic associations
No dysmorphic features were identified; the testes were undescended and a small left inguinal hernia was noted. Original ophthalmological examinations noted a marked exotropia with up-gaze paralysis. Over the following months, this spontaneously reverted to an esotropic gaze that persisted despite shunt revision. At age 15 months, he underwent surgical correction. There is no evidence of optic atrophy and vision appears to be near normal. Although follow-up has not been consistent, examination by a paediatric neurologist suggests developmental delay.
DISCUSSION The advent of high-quality ultrasonographic equipment and an increase in experience have allowed the prenatal diagnosis of a number of central nervous system (CNS) malformations, including DWM. The presence of a posterior fossa cyst and partial or complete absence of the cerebellar vermis are diagnostic of DWM in the fetus. The onset of hydrocephalus associated with DWM is variable and may not develop until the newborn period or later in life (Hirsch et al., 1984; Bordarier and Aicardi, 1990).
DWM is associated with other abnormalities in a significant proportion of cases (see Table 1). CNS malformations most commonly include agenesis of the corpus callosum and occipital encephaloceles (Hirsch et al., 1984; Russ et al., 1989).

90 T. COWLES ETAL.
Extracranial malformations, including cleft lip and palate, cardiac malformations, urinary tract abnormalities, facial angiomas, and minor facial anomalies, are present in approximately 20-30 per cent of cases (Hart et al., 1972; Hirsch et al., 1984; Russ et al., 1989).
A variety of reports link DWM to environmental factors. The malformation has been noted following prenatal exposure to rubella, cytomegalovirus, toxoplasmosis, coumadin, and alcohol (Murray et al., 1985). These agents most likely provide a non-specific insult at a critical time in embryogenesis.
More complicated Mendelian disorders may have DWM as a manifestation. DWM has been reported as part of the Aicardi syndrome, an X-linked dominant disorder (Philips et al., 1978). There are reports of DWM in association with trisomies 9, 18, and 21; triploidy; Turner syndrome; and chromosomal abnormali- ties in which additional 5p, 8p, or 8q material is present (Hirsch et al., 1984; Murray et al., 1985; Russ et al., 1989). DWM has been described in rare chromosomal abnormalities such as 17q duplication and in two unrelated children homozygous for the 9qh+ heteromorphism (Murray et al., 1985).
Autosomal recessive syndromes which can have DWM as a feature include Warburg, Coffin-Siris, Joubert-Boltshauser, and Meckel-Gruber (Murray et al., 1985). Chemke et al. (1975), described a sibship of seven in which three inherited a constellation of malformations including DWM, lissencephaly, and occular malfor- mations in an apparently autosomal recessive pattern. More recently, Lehman (198 1) presented a family in which three consecutive siblings were affected with hindbrain malformations. The findings of DWM were noted only on CT scan when the third, apparently normal, child underwent evaluation following the death of the second sibling.
While some X-linked CNS abnormalities such as X-linked mental retardation with aqueductal stenosis have been well described (Howard et al., 1981), other reports of X-linked CNS abnormalities are less clear. Prior to this report, only two families have been described who display similar malformations occurring in an X-linked pattern of inheritance. The first family contained a sibship of three brothers; two of these were affected and died shortly after birth with congenital hydrocephalus, cerebellar agenesis, and enlargement of the fourth ventricle. A maternal male relative, three generations prior to the proband, also died of con- genital hydrocephalus (Riccardi and Marcus, 1978). Another family, less similar to ours, has been described in which two brothers and a maternal uncle were found to have communicating hydrocephalus and mental retardation. Agenesis of the vermis was not noted on CT scanning (Renier et al., 1983).
The present family includes four males affected with isolated DWM apparently inherited in an X-linked recessive fashion. 11-6 died in infancy; the others, 111-5, 111-9, and IV-2, required ventriculoperitoneal shunt placement. Four females, 1-2, 11-2, 11-5, and 111-3, are obligate carriers of the responsible gene. The proband’s mother and grandmother, 111-3 and 11-2, were Hispanic women with normal appear- ance and intelligence. No radiographic study has been made of these women. Karyotypic analysis of IV-2 and 111-3 is normal; linkage studies have not been obtained because of a lack of cooperation from the family.
Because of the heterogeneous nature of the DWM, genetic counselling of families with a previously affected child can be difficult. When DWM is associated with

PRENATAL DIAGNOSIS OF DANDY-WALKER MALFORMATION 91
Mendelian syndromes or chromosomal abnormalities, then the recurrence risk is that of the particular disorder. In the absence of an associated disorder, the recurrence risk of isolated DWM appears to be similar to multifactorial disorders (about 5 per cent after one affected child is born to unrelated, unaffected parents) (Murray et al., 1985). Thorough pedigree analysis is essential, however, as some families may be at much higher risk for affected offspring. Rare families appear to transmit the disorder in an X-linked recessive fashion, with a recurrence risk of 25 per cent.
REFERENCES Bordarier, C., Aicardi, J. (1999). Dandy-Walker syndrome and agenesis of the cerebellar
vermis: diagnostic problems and genetic counselling, Dev. Med. Child Neurol., 32,285-294. Chemke, J . , Czernobilsky, B., Mundel, G., Barishak, Y.R. (1975). A familial syndrome of
central nervous system and ocular malformations, Clin. Genet., 7 , 1-7. Hart, M.N., Malamud, N., Ellis, W.G. (1972). The Dandy-Walker syndrome, Neurology, 22,
771-780. Hirsch, J.F., Peirre-Kahn, A., Renier, D., Sainte-Rose, C., Hoppe-Hirsch, E. (1984). The
Dandy-Walker malformation, J. Neurosurg., 61,5 15-522. Howard, F.M., Till, K., Carter, C.O. (1981). A family study of hydrocephalus resulting from
aqueduct stenosis, J. Med. Genet., 18,252-255. Lehman, R.M. (198 1). Dandy-Walker syndrome in consecutive siblings: familial hindbrain
malformation, Neurosurgery, 8,7 17-719. Murray, J.C., Johnson, J.A., Bird, T.D. (1985). Dandy-Walker malformation: etiologic
heterogeneity and empiric recurrence risks, Clin. Genet., 28,272-283. Philips, H.E., Carter, A.P., Kennedy, J.L., Rasman, N.P., OConnor, J.F. (1978). Aicardi’s
syndrome: radiologic manifestations, Radiology, 127,453455. Renier, W.O., Gabreels, F. J.M., Hustinx, T.W.J., Thijssen, J.O.M., Ter Haar, B.G.A., Kroll,
E.W., Beckers, H. (1983). Cerebellar hypoplasia, communicating hydrocephalus and mental retardation in two brothers and a maternal uncle, Brain. Dev., 5 , 4 1 4 5 .
Riccardi, V.M., Marcus, E.S. (1978). Congenital hydrocephalus and cerebellar agenesis, Clin. Genet., 13,443447.
Russ, P.D., Pretorius, D.H., Johnson, M.J. (1989). Dandy-Walker syndrome: a review of fifteen cases evaluated by prenatal sonography, Am. J . Obstet. Gynecol., 161,401406.