Embed Size (px)
Citation preview

Preoperatíve Preoperatíve anesthesiologic assesmentanesthesiologic assesment
Risk of anesthesiaRisk of anesthesia
Preadmission Preadmission clinic (PAC)clinic (PAC)
PremedicationPremedication

The operatíve/anesthesiologic riskThe operatíve/anesthesiologic risk
Operation/anesthesia effects the entire Operation/anesthesia effects the entire organism, and carries certainorganism, and carries certain risks risks for the for the patient.patient.
The patient should be in the possible best The patient should be in the possible best condition for an elective operation to condition for an elective operation to reduce the risk of the procedure.reduce the risk of the procedure.
The risk of the operation/anesthesia The risk of the operation/anesthesia should never exceed the benefits of the should never exceed the benefits of the procedure!procedure!

Evaluation of riskEvaluation of risk
Benefits of the operation
What does the patient win?
Risk of complications
or death(What can he
loose?)

The anesthesia riskThe anesthesia risk
MortalityMortality associated with anesthesia: associated with anesthesia:Anesthesia and surgical mortalityAnesthesia and surgical mortality
- In many cases it is difficult to distinguish - In many cases it is difficult to distinguish
MorbidityMorbidity associated with anesthesia associated with anesthesia– Immediate complications/ Late complicationsImmediate complications/ Late complications– Reversible, short live complicationsReversible, short live complications– Permanent damagesPermanent damages (brain, palsy, etc.) (brain, palsy, etc.)

One anesthesia-death is one more than One anesthesia-death is one more than acceptable!acceptable!
The statistical probability of anesthesia The statistical probability of anesthesia death is 100 000:1 (2-4?) -”acceptable”??death is 100 000:1 (2-4?) -”acceptable”??
..and if the one person is my near relative ..and if the one person is my near relative …?…?
Sometimes it is difficult to see the real Sometimes it is difficult to see the real cause;cause;
Sometimes the media are creating a Sometimes the media are creating a „crime” „crime” - default/negligence where there is - default/negligence where there is none.none.
The most important question: is the structure we are working safe enough???

Factors influencing the risk of Factors influencing the risk of anesthesiaanesthesia
Physical state of the patient, agePhysical state of the patient, ageSpecial risk factors Special risk factors (cardiorespiratory and other complications)(cardiorespiratory and other complications)Urgency of the operation Urgency of the operation (immediate, urgent, scheduled, elective)(immediate, urgent, scheduled, elective)The degree of the surgical stress –The degree of the surgical stress –
– Type of operationType of operation– Length of operationLength of operation
Technical conditions/equipment, monitoring, Technical conditions/equipment, monitoring, essential servicesessential services
Subjective circumstances and conditions:Subjective circumstances and conditions:Training and experience of the anesthetistTraining and experience of the anesthetistReadiness, fatique of the physiciansReadiness, fatique of the physicians

Risk according to the severity of the Risk according to the severity of the operationoperation
Low riskLow risk– Small interventions, blood loss Small interventions, blood loss <<200ml 200ml (pl.inquinal hernia, (pl.inquinal hernia,
arthroscopy)arthroscopy)
Medium riskMedium risk– Medium severe surgical intervention, Medium severe surgical intervention, (laparoscopic (laparoscopic
cholecystectomy, tonsillectomy,TUR) cholecystectomy, tonsillectomy,TUR) blood loss blood loss <<1000 ml1000 ml
High riskHigh risk– Long abdominal, thoracic, intracranial surgery with more Long abdominal, thoracic, intracranial surgery with more
than 1000ml blood loss, than 1000ml blood loss, high quality postoperative therapy necessaryhigh quality postoperative therapy necessary
(morbidity, mortality (morbidity, mortality elevated)elevated)

Risk according to urgencyRisk according to urgency
Vital urgencyVital urgency„„Simple” urgencySimple” urgencyElective - hospitalisedElective - hospitalised
day casesday cases
The minimum of necessary surgical information:The minimum of necessary surgical information:Surgical status, previous findings, surgical plan Surgical status, previous findings, surgical plan
(type of operation), plan of postoperative (type of operation), plan of postoperative rehabilitationrehabilitation

Sürgős beavatkozásokSürgős beavatkozásokImmediate (vital) urgency (periculum in vita)Immediate (vital) urgency (periculum in vita)
No preparation is possible (e.g. liver rupture)No preparation is possible (e.g. liver rupture)
„„Simple” urgency Simple” urgency (short preparation possible)(short preparation possible)
Has to be done within a couple of hoursHas to be done within a couple of hours (acute abdomen, arterial (acute abdomen, arterial
obstruction) obstruction) Has to be done on the same day (e.g. open fractures)Has to be done on the same day (e.g. open fractures)
Has to be done in a couple of daysHas to be done in a couple of days
Relative uregency (weeks?)Relative uregency (weeks?)Proper preparation is possible and necessaryProper preparation is possible and necessary
(e.g. tumor (e.g. tumor surgery)surgery)

Classification of the physical status of the patient Classification of the physical status of the patient
according to theaccording to the American Society of AnesthesiologistsAmerican Society of Anesthesiologists (ASA)(ASA)
ASA 1 (I) ”Normal”, healthy patientASA 1 (I) ”Normal”, healthy patientASA 2 (II) Mild systemic diseasesASA 2 (II) Mild systemic diseasesASA 3 (III) Severe systemic disease ASA 3 (III) Severe systemic disease
that limits activitythat limits activityASA 4 (IV) Incapacitating disease ASA 4 (IV) Incapacitating disease
(constant treat to life)(constant treat to life)ASA 5 (V) Moribund patientASA 5 (V) Moribund patient
For For emergency cases an „E”emergency cases an „E” is added before classification is added before classification (e.g. ASA class EIV)(e.g. ASA class EIV)

Mortality and ASA risk categoriesMortality and ASA risk categories
ASAASA 11 22 33 44 55
Mortality Mortality inin>>6000 pts 6000 pts (Germany)(Germany)
0,1%0,1% 0,7%0,7% 3,5%3,5% 18,3%18,3% 93,3%93,3%
The preoperative preparation of the patient may be a very important factor of anesthesia risk!
With good preparation also the physical state can be influenced.

Special risk factors not included in Special risk factors not included in ASA categoriesASA categories
UrgencyUrgency
ObesityObesity
Full stomachFull stomach !!!!! !!!!!
Rithm disturbancesRithm disturbances
Electrolite/acid-base Electrolite/acid-base imbalance, imbalance, metabolic disturbancesmetabolic disturbances
Drog abuseDrog abuse
Alcohol abuse, smokingAlcohol abuse, smoking
Inadequate preparation, lack of informationInadequate preparation, lack of information

USA closed clames USA closed clames Caplan 1994
ComplicationComplication %-of all %-of all claimsclaims
Paid sum Paid sum $$
$$ (from-to) (from-to)
Death
Nerve injuryLasting cerebral injury
Airway injuries
Newborn - complications
Pneumothorax
Eye injury
Aspiration
Awakening during surgery
37
15
12
4
4
3
3
3
3
171.000
17.500
700.000
14.250
325.500
26.250
25.000
150.000
18.000
750.000-4.000.000
188.000-2.100.000
10.000-6.000.000
15 - 200.000
25.000- 5.400.000
500 – 4.000.000
145 - 1.000.000
25.000 -4.500.000
430 - 305.100
The incidence of respiratory problems was 34% - these were found responsible for 85% of lethal cases!!!
(cardiovascular complications 6%)

„„Near accidents” - the whole therapeutic Near accidents” - the whole therapeutic chain has to be checked!chain has to be checked!
ActiveActive human error?human error?
Latent Latent negligence?negligence? System error?System error?
– Lack of attentionLack of attention– Lack of knowledgeLack of knowledge– Violation of rulesViolation of rules
•Failures of the training•Jujdgement of competence•Tiredness, overwork•Working place atmospheraStrategies for controlling risk!!!
Rami L, Grimaud D. Aneszteziológia és Intenzív Terápia 2005/3

The most important decision:The most important decision:
Advantages of the planned surgery?Advantages of the planned surgery? (What does the patient gain -
surgical point of view)
How high is the risk of cancelling / postponing the operation?How high is the risk of cancelling / postponing the operation?
Risk of the operation? Risk of the operation? (anesthesiologic points of view)
How high is the risk of complications?How high is the risk of complications?
Could we improve the situation?Could we improve the situation?

Aim of preoperative assesment and Aim of preoperative assesment and of the preparation of the patientof the preparation of the patient
Operation of the patient at the best timepoint in Operation of the patient at the best timepoint in the possible best conditionthe possible best condition
Selection of the optimal anesthesiologic methodSelection of the optimal anesthesiologic method
Reduction of hospitalisation timeReduction of hospitalisation time
Rational, economic proceduresRational, economic procedures
Reduction of the perioperative risk factors Reduction of the perioperative risk factors (mortality and morbidity reduction)(mortality and morbidity reduction)

Risk because of urgencyRisk because of urgency
Full stomach – risk of aspirationFull stomach – risk of aspiration
Lack of preparationLack of preparation– Physical, laboratory, radiologic, cardiologic, etc. Findings?Physical, laboratory, radiologic, cardiologic, etc. Findings?
Risk caused by the basic problemRisk caused by the basic problem– e.g. severe bleeding, shock state…e.g. severe bleeding, shock state…
Insufficient personal conditions, missing team Insufficient personal conditions, missing team members and eguipment members and eguipment
e.g. monitors, competent doctors …e.g. monitors, competent doctors …
We have to find the balance between the grade of urgency and We have to find the balance between the grade of urgency and the „acceptable” deficiencies + risk factors!the „acceptable” deficiencies + risk factors!

A preoperative NPOA preoperative NPOMendelson (1946)!
Hours before Hours before surgerysurgery
Allowed orally:Allowed orally:
2-32-3 Clear liquids (except: alcohol, milk, coffe)
44 Mother milk
66 Milk, light solid food
88 Normal solid food (meat, fat…)
CAVE: protracted emptying – trauma, stress, DM, alkoholism, GI problems!

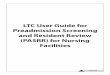
Patterns of Gastric Emptying in Healthy People and in Patients with Diabetic Gastroparesis
Camilleri M. N Engl J Med 2007;356:820-829

Preoperative assesmentPreoperative assesment
HistoryHistoryPhysical examinationPhysical examinationPrevious documentationPrevious documentationLaboratory and special diagnostic proceduresLaboratory and special diagnostic proceduresConsultation with colleguages of other Consultation with colleguages of other specialitiesspecialitiesPlan for the preoperative anesthesiologic Plan for the preoperative anesthesiologic preparation/therapeutic interventionspreparation/therapeutic interventionsDesign of the anesthesiologic method and of the Design of the anesthesiologic method and of the postoperative carepostoperative careInformation of the patient, informed consentInformation of the patient, informed consent

Preoperative anesthesiologic Preoperative anesthesiologic preparation I.preparation I.
Site: Site: Preadmission anesthesiology clinic (or unfortunately Preadmission anesthesiology clinic (or unfortunately
sometimes the ward or even OR)sometimes the ward or even OR)
Time:Time:In ideal case some (5-14) days before the scheduled In ideal case some (5-14) days before the scheduled
intervention (sufficient time for the necessary intervention (sufficient time for the necessary investigations, therapy)investigations, therapy)
Responsible person: Responsible person: Anesthetist in cooperation with consultants of other Anesthetist in cooperation with consultants of other
specialitiesspecialities

Preoperative anesthesiologic Preoperative anesthesiologic preparation II.preparation II.
Methods:Methods:HistoryHistory
Questioning of the patientDocuments of previous investigations, hospital treatmentsSpecial anamnestic questions (bleeding disorders, possible gravidity, etc)MedicationAlcohol, tobacco abuse
Physical investigationPhysical investigation– General– Special (eg. Intubation difficulties, venous access, etc.)– Measured parameters (BP, HR, temperature)
Laboratory investigationsLaboratory investigationsIndividual decisions Blood group crossmatching
Imageing methods – e.g. chest X ray, sonography, CT…Imageing methods – e.g. chest X ray, sonography, CT…Functional tests – e.g. stress ECG, respiratory function testFunctional tests – e.g. stress ECG, respiratory function testSpecialist consiliumSpecialist consilium

Individual planning of the Individual planning of the necessary investigationsnecessary investigations
Minimum (routine) investigations Minimum (routine) investigations (short, (short, small operation ASA class I patient)small operation ASA class I patient)
History, physical examinationHistory, physical examinationurine, quantitative blood chemistry, (crossmatching)urine, quantitative blood chemistry, (crossmatching)
Maximum investigation (serious operation, ASA III-V)Maximum investigation (serious operation, ASA III-V)History, physical examinationHistory, physical examinationUrin, routine laboratory, qualitative/quantitative blood chemistryUrin, routine laboratory, qualitative/quantitative blood chemistryIonogramm, hepatic and renal function tests, blood sugar, se. proteinsIonogramm, hepatic and renal function tests, blood sugar, se. proteinsBood group crossmatched, blood gases, acid/base statusBood group crossmatched, blood gases, acid/base statusChest X ray, ECG, respiratory funcion testsChest X ray, ECG, respiratory funcion tests
Additional investigations according to the diagnosis Additional investigations according to the diagnosis and accompanying diseasesand accompanying diseases
Screening testsScreening testsBreast, rectal, stool, gravidity test, etc.Breast, rectal, stool, gravidity test, etc.

Preoperative anesthesiologic Preoperative anesthesiologic preparation III.preparation III.
Competency of the anesthesiologistCompetency of the anesthesiologist::– Assessment of anesthesia tolerance of the Assessment of anesthesia tolerance of the
patientpatient– Planning of the anesthesia preparationPlanning of the anesthesia preparation– Discussion with the patient, informed consentDiscussion with the patient, informed consent– Choice of the anesthesia methodChoice of the anesthesia method– Plan of the postoperative anesthesia care Plan of the postoperative anesthesia care
(RR, ICU?(RR, ICU?))– Perioperative analgesiaPerioperative analgesia

Preoperative anesthesiologic Preoperative anesthesiologic preparation IV.preparation IV.
Competency of the consultant specialist:Competency of the consultant specialist:– Specialist opinion about the status of the Specialist opinion about the status of the
patient, diagnosis, therapeutic advicepatient, diagnosis, therapeutic advice;;– Help in order to optimize the conditions…Help in order to optimize the conditions…– … …and reduce the operative riskand reduce the operative risk

Indication for preoperative chest x Indication for preoperative chest x rayray
Cardiorespiratory disease, metastatic cancer,
Big operaqtion, age over 40 years
X ray necessary for proper X ray necessary for proper assesment of the patientassesment of the patient
Good results at chest X Good results at chest X ray within one yearray within one year
Worsening since the last examination
Chest X ray necessary
Chest X ray not necessary
yes
yes
yesyes
no
no no
no

Indication for perioperative ECGIndication for perioperative ECG
Age: men <40y, women< 50y
IHD, vascular disease, big IHD, vascular disease, big operation, rhythm disturbancesoperation, rhythm disturbances
Negative ECG within 1 Negative ECG within 1 yearyear
Worsening of status
ECG necessary
ECG not necessaryyes
yes
yesyes
no
no
no
no

Indication for preoperative Indication for preoperative respiratory function testsrespiratory function tests
COPD, chr.bronchitis, asthma
Chest deformities, neuromuscular diseases, dyspnoea
Thoracotomy? Fresh results (within 3 months
Pulmonary function test
indicated
Pulmonary function test unnecessary
yes
yes
yes
no
no
no

Premedication I.Premedication I.
AimAim of premedication of premedication::
Anxiolysis, sedationAnxiolysis, sedation
Reduction of the dose of indunction anestheticsReduction of the dose of indunction anesthetics
Reduction of secretionsReduction of secretions
Attenuation of vagal and sympathoadrenal refllexesAttenuation of vagal and sympathoadrenal refllexes
Elevation of gastric pH valuesElevation of gastric pH values
Prevention pf postoperative nausea and emesis (PONV)Prevention pf postoperative nausea and emesis (PONV)
AmnesiaAmnesia

Premedication IIPremedication IIPrescription of medicamentsPrescription of medicaments
– Benzodiazepines Benzodiazepines (anxiolysis, sedation, amnesia)(anxiolysis, sedation, amnesia)
diazepam, temazepam, lorazepam, midazolamdiazepam, temazepam, lorazepam, midazolam– Opioids Opioids (analgesia, sedation)(analgesia, sedation)
fentanyl, pethidin, alfentanil sufentanilfentanyl, pethidin, alfentanil sufentanil– Butyrofenons Butyrofenons (sedation, antiemesis)(sedation, antiemesis)
dehydrobenzperidol (DHBP)dehydrobenzperidol (DHBP)– Anticholinergic agents Anticholinergic agents (antisialague, amnestic, antivagal)(antisialague, amnestic, antivagal)
atropin, glycopyrrolat, (hyoscin)atropin, glycopyrrolat, (hyoscin)– Antacids Antacids
Sodium citricum, HSodium citricum, H22 antagonists, omeprazol, metoclopramid antagonists, omeprazol, metoclopramid• -receptor blockers -receptor blockers (antinocicepcion)(antinocicepcion)
atenolol, esmololatenolol, esmolol
• 22 receptor agonists receptor agonists (anesthesia potenciation, (anesthesia potenciation, reduction of central NE effectsreduction of central NE effects
clonidin, dexmedetomidinclonidin, dexmedetomidin• Phenotiazins Phenotiazins (central antiemesis, sedation, antiallergic, anticholinerg)(central antiemesis, sedation, antiallergic, anticholinerg)
!

Risk of venous thromboembolismRisk of venous thromboembolismLow riskLow risk Medium riskMedium risk High risk High risk (DVT(DVT>>10-10-
20%, PE 1-5%)20%, PE 1-5%)
Short surgical Short surgical interventions interventions whithout other whithout other risk factors (RF)risk factors (RF)
Medium or long general-, Medium or long general-, urologic, gynecologic, neuro-, urologic, gynecologic, neuro-, cardiac-, vascular-, thoracic- cardiac-, vascular-, thoracic- surgery, surgery, >>40 years, RF 40 years, RF >>22
Pelvic fractures-Pelvic fractures-traumatol., ortop. surgerytraumatol., ortop. surgery
Medium long Medium long surgery, surgery, whithout other whithout other RFsRFs
Serious trauma, burnsSerious trauma, burns
AnticoncipientsAnticoncipients
Obesitas, smokingObesitas, smoking
Pelvic tumor operations Pelvic tumor operations
Extended surgery, Extended surgery, traumatrauma
Medical disease + Medical disease + thrombophilia thrombophilia
Paresis, immobilityParesis, immobility
Small trauma, Small trauma, medical diseasesmedical diseases
Medical disease + DVT, PE in Medical disease + DVT, PE in the pt’s historythe pt’s history
Small trauma + immobilisationSmall trauma + immobilisation
Critical lower limb Critical lower limb ischaemiaischaemia

Perioperative patient carePerioperative patient care
SimpleSimpleContinuous observationContinuous observation
Knowledge of surgical processesKnowledge of surgical processes
MonitoringMonitoringPatient’s parameters: circulation, breathing, Patient’s parameters: circulation, breathing, temperature, muscle relaxation, CNS activity…temperature, muscle relaxation, CNS activity…
Parameters on the anesthesia machine, ventillatorParameters on the anesthesia machine, ventillator

DocumentationDocumentationAnesthesia recordAnesthesia record
– Graphic plotsGraphic plots: continuously registered parameters: continuously registered parameters
– BP, pulse, CVPy…..BP, pulse, CVPy…..– OO22 saturation, ETCO2, pressures…… saturation, ETCO2, pressures……
– Intra- and postoperative investigations, samplingIntra- and postoperative investigations, sampling
– Medication, infusionsMedication, infusions
– Urine outputUrine output
– Important eventsImportant events– ComplicationsComplications

Cheer up! Break is near!