Embed Size (px)
Citation preview
Pain, 45 (1991) 299-306 10 1991 Elsevier Science Publishers B.V. 0304-3959/91/$03.50 ADONIS 0304395991001384
299
PAIN 01789
Preparing children for venous blood sampling
Ann Harrison
department of Co~~u~~ty medicine and ~eha~~orui Sciences, Faculty of ~ed~cjne, Kuwait U~i~er~jty, Kuwait Cig ~K~~ajt~
(Received 8 January 1990, revision received 15 November 1990. accepted 20 November 1990)
Summary A convenience sample of 100 children, aged 6-12 years, attending Kuwait government hospital laboratories for venous blood sampling was studied. A picture book was used to prepare half of the children for the procedure. Preparation was carried out just prior to sampling and took less than 5 min. The story provided a simple description of venous blood sampling, and why it is carried out; it stressed that the pain is noticeable but not unbearable, and that children will experience less pain if they relax their arm and cooperate with the technician. Prepared children reported sig~~cantly less pain, and radial pulse rates confirmed that they were less distressed by the procedure. Observers’ and parents’ evaluations also indicated that prepared children coped better. Various explanations for the benefits observed are discussed, together with requirements for managing the pain, fear and stress experienced by children during medical treatment.
Key words: Venepuncture; Stress; (Child); (Pain)
Venous blood sampling is acknowledged to be a potentially very frightening and painful experience for children [4,5,17]. If a child is tense or struggles, vene- puncture is more difficult to complete, and the risks of accidental injury are greater ]2]. There is a need, there- fore, to find ways of encouraging children to be less anxious and more cooperative during venous blood sampling. This should also lessen the chances of children becoming unduly fearful of a procedure which they are likely to face again [11,12,19].
The aim of the present study was to establish whether young children benefit from being read a short prepara- tion story while waiting for a blood sample to be taken. Parents and care staff often have very little warning that venepuncture will be carried out, and so only a short time in which to prepare the child. While debate con- tinues about how far in advance it is best to prepare children for painful procedures [18], there are prece- dents for the effectiveness of late preparation [19].
Correspondence to: Dr. Ann Harrison. Faculty of Medicine and Health Science, United Arab Emirates University, P.O. Box 17666. Al-Ain, U.A.E.
Based on previous research, the preparation story attempted to improve children’s knowledge about venous blood sampling and extend their strategies for coping with the procedure, with the aims of reducing the amount of fear, stress and pain experienced by them [13,21--231. Specifically, the story sought: (i) to provide young children with accurate and intelligible informa- tion about what happens during venous blood sampling, and what pain to expect; (ii) to forestall misconceptions which have been shown to increase children’s fear of blood sampling [4,5]; (iii) to foster cooperation with, and trust in, the person performing the procedure, and (iv) to provide a model of a child who copes during blood sampling, who relaxes and does not struggle. The preparation story offered a simple description of the venous blood sampling procedure, why it is carried out, and what happens to the blood after it has been col- lected. It emphasised that the procedure creates a brief period of pain, and that the pain is noticeable but not unbearable. The story also stressed that venepuncture is less painful if a child relaxes his arm and cooperates with the technician. In order to increase the likelihood of children modelling the behaviour of the child fea- tured in the story, sex- and age-appropriate models of average appearance were used, and local children, parents and hospital settings were photographed [18].

The study was carried out in the central laboratories of general hospitals in Ku\h;ait. Central laboratories
collect venepunctute blood samples from mobile inpa- tients. outpatients, and adults and children referred
from community clinics. Laboratories are designed around a common waiting area. with rooms at the
periphery specialised for different procedures. After a
procedure has been completed, patients pass back
through the waiting area. One disadvantage of this
arrangement is that children hear the reactions of pa- tients ahead of them, and witness any distress they show
when leaving. Initial observations revealed that labora- tory technicians generally made no attempt to prepare
children for venepuncture or to talk them through the procedure; if children protested and struggled, their strategy was to physically restrain the child and com-
plete the procedure. Often, parents were recruited to
help. A variety of indices were used to compare prepured
and non-prepared children’s reactions to venous blood
sampling. Children rated the intensity of the pain they had experienced using a visual analog scale (VAS) and were asked to comment on how painful and frightening
the procedure had been. Parents provided VAS ratings of their child’s fear and pain, and experimenters evaluated the child’s behaviour during blood sampling, and measured radial pulse rates immediately before and
after the procedure.
Methods
Subjects A convenience sample of 100 children (49 girls, 50
boys; mean age 8.4 years) reporting to 4 hospital laboratories was studied. The only selection criterion
used was that a child should be aged 6612 years old.
Procedure Ethical clearance was received from the Ministry of
Health, State of Kuwait. The data were collected by
nursing students in the second year of a 4 year degree programme. The design called for 3 experimenters. Ex- perimenter 1 approached accompanying adults for in-
formed consent. Participating children were assigned
Fig. 1. The preparation story. Eman is feeling sick, and so her mother takes her to the doctor (photograph A). The doctor is not sure what is wrong, and so he sends Eman to the hospital to have a blood sample taken (photograph B). In the laboratory, they will check a small amount of Eman’s
blood and see if they can discover why she is feeling sick (photograph C), Miss Sanaa is the lady who takes the blood samples (photograph D).
Eman is a bit frightened, but Miss Sanaa tells her that although it will hurt, it will not be too bad, and it will soon be over. Miss Sanaa asks Eman
to keep her arm still and relaxed, and not to move. Miss Sanaa tells Eman that if she keeps her arm still and relaxed, the needle will hurt less. When
Eman is comfortable, Miss Sanaa puts a rubber band around her arm and sticks a needle in to remove some blood (photograph E). Miss Sanaa says
‘Eman you were really good, you kept your arm very still and relaxed which made it easy for me. ’ Eman replied ‘You were right. it did hurt, but it
was soon over.’ (photograph F).
301
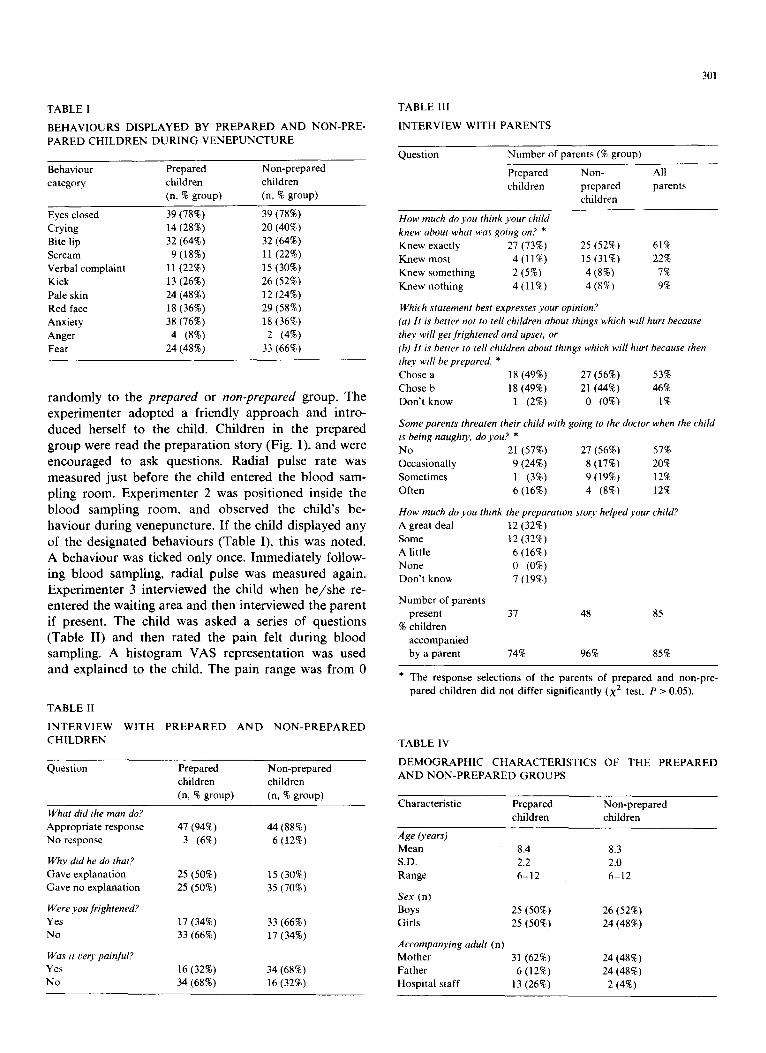
TABLE 1
BEHAVIOURS DISPLAYED BY PREPARED AND NON-PRE-
PARED CHILDREN DURING VENEPUNCTURE
Behaviour category
Prepared Non-prepared children children (n, % group) (n, % group)
Eyes closed 39 (78%) 39 (78%)
Crying Bite lip
Scream
Verbal complaint
Kick
Pale skin
Red face
Anxiety
Anger
Fear
14 (28%)
32 (64%)
9 (18%)
11(22%)
13 (26%)
24 (48%)
18 (36%)
38 (76%)
4 (8%) 24 (48%)
20 (40%)
32 (64%)
11 (22%)
15 (30%)
26 (52%)
12 (24%)
29 (58%)
18 (36%)
2 (4%) 33 (66%)
randomly to the prepared or non-prepared group. The experimenter adopted a friendly approach and intro-
duced herself to the child. Children in the prepared group were read the preparation story (Fig. I), and were encouraged to ask questions. Radial pulse rate was measured just before the child entered the blood sam-
pling room. Experimenter 2 was positioned inside the blood sampling room, and observed the child’s be-
haviour during venepuncture. If the child displayed any of the designated behaviours (Table I), this was noted. A behaviour was ticked only once. Immediately follow- ing blood sampling, radial pulse was measured again. Experimenter 3 interviewed the child when he/she re- entered the waiting area and then interviewed the parent if present. The child was asked a series of questions (Table II) and then rated the pain felt during blood sampling. A histogram VAS representation was used and explained to the child. The pain range was from 0
TABLE II
INTERVIEW WITH PREPARED AND NON-PREPARED
CHILDREN
Question Prepared
children
(n, % group)
Non-prepared
children
(n, % group)
What did the man do?
Appropriate response
No response
Why did he do that?
Gave explanation
Gave no explanation
Were you frightened?
Yes
No
Was it oery painful?
Yes
No
47 (94%)
3 (6%)
25 (50%)
25 (50%)
17 (34%)
33 (66%)
16 (32%)
34 (68%)
44 (88%)
6 (12%)
15 (30%)
35 (70%)
33 (66%)
17 (34%)
34 (68%)
16 (32%)
TABLE III
INTERVIEW WITH PARENTS
Question Number of parents (% group)
Prepared
children
Non-
prepared
children
All
parents
How much do you think your chrld
knew about what was going on? *
Knew exactly 27 (73%)
Knew most 4 (11%)
Knew something 2 (5%) Knew nothing 4 (11%)
25 (52%) 61%
15 (31%) 22%
4 (8%) 7%
4 (8%) 9%
Which statement best expresses your opinion?
(a) It is better not to tell children about things which will hurt because
they will get frightened and upset, or
(b) It is better to tell children about thmgs which will hurt because then
they will be prepared. *
Chose a 18 (49%) 27 (56%) 53%
Chose b 18 (49%) 21(44%) 46%
Don’t know l (2%) 0 (0%) 1%
Some parents threaten their child with going to the doctor when the child
is being naughty, do you? *
No 21 (57%) 27 (56%) 57%
Occasionally 9 (24%) 8 (17%) 20%
Sometimes l (3%) 9 (19%) 12%
Often 6 (16%) 4 (8%) 12%
How much do you think the preparation stoty helped your child?
A great deal 12 (32%)
Some 12 (32%)
A little 6 (16%)
None 0 (0%) Don’t know 7 (19%)
Number of parents
present 37 48 85
% children
accompanied
by a parent 74% 96% 85%
* The response selections of the parents of prepared and non-pre-
pared children did not differ significantly (x2 test, P > 0.05).
TABLE IV
DEMOGRAPHIC CHARACTERISTICS OF THE PREPARED
AND NON-PREPARED GROUPS
Characteristic Prepared
children Non-prepared
children
Age (years) Mean 8.4 S.D. 2.2 Range 6-12
Sex (n) Boys 25 (50%) Girls 25 (50%)
Accompanyrng adult (n) Mother 31(62%) Father 6 (12%) Hospital staff 13 (26%)
8.3
2.0
6-12
26 (52%)
24 (48%)
24 (48%)
24 (48%)
2 (4%)
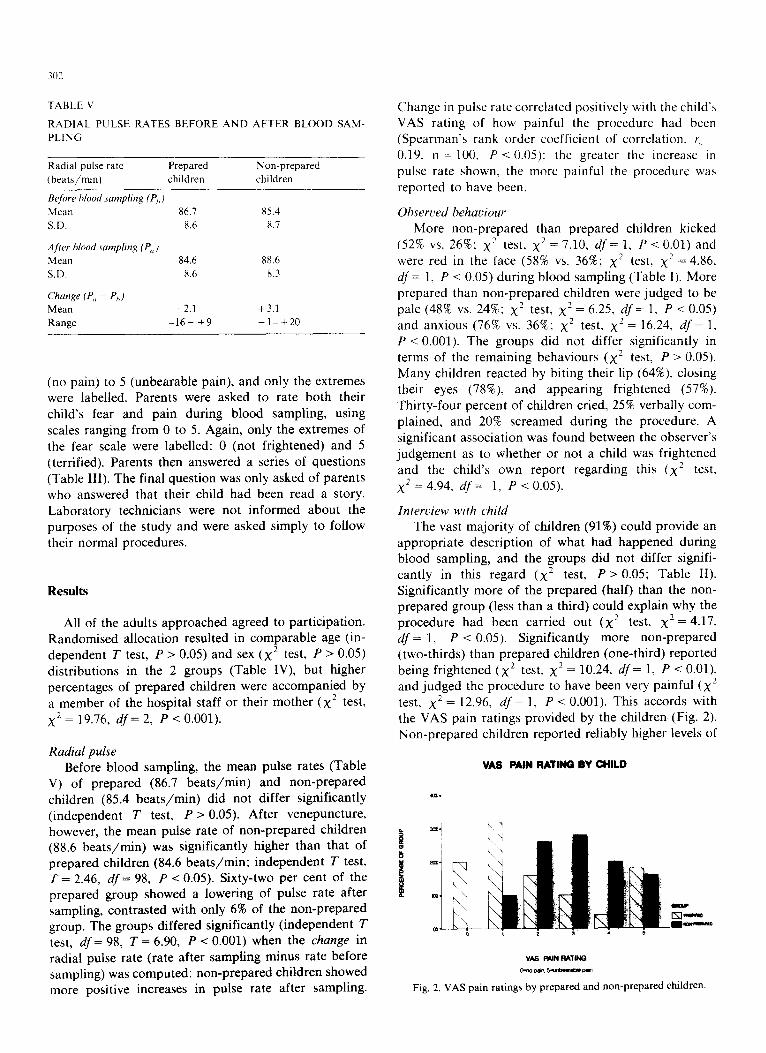
302
1 ABLE \’
RADIAL PULSE RATES BEFORE AND AFTER BLOOD SAM-
PLING
Radial pulse rate Prepared Non-prepared (beats/min) children children
Be/ore blood sumpling (P,>)
Mean 86.7 x5.4
SD. 8.6 x.7
..4frer blood sampbng (PC,)
Mean 84.6 88.6
S.1). 8.6 x.3
C‘hunge (P<, - P,,)
Mean -2.1 +3.1
Range -16- +9 -l-+20
(no pain) to 5 (unbearable pain), and only the extremes were labelled. Parents were asked to rate both their
child’s fear and pain during blood sampling, using scales ranging from 0 to 5. Again, only the extremes of the fear scale were labelled: 0 (not frightened) and 5
(terrified). Parents then answered a series of questions
(Table III). The final question was only asked of parents who answered that their child had been read a story. Laboratory technicians were not informed about the purposes of the study and were asked simply to follow their normal procedures.
Results
All of the adults approached agreed to participation. Randomised allocation resulted in comparable age (in- dependent T test, P > 0.05) and sex (x2 test, P > 0.05)
distributions in the 2 groups (Table IV), but higher percentages of prepared children were accompanied by a member of the hospital staff or their mother (x2 test,
x2 = 19.76, df= 2, P < 0.001).
Radial pulse Before blood sampling, the mean pulse rates (Table
V) of prepared (86.7 beats/min) and non-prepared children (85.4 beats/min) did not differ significantly
(independent T test, P > 0.05). After venepuncture, however, the mean pulse rate of non-prepared children (88.6 beats/min) was significantly higher than that of prepared children (84.6 beats/min; independent T test, T = 2.46, df = 98, P < 0.05). Sixty-two per cent of the prepared group showed a lowering of pulse rate after sampling, contrasted with only 6% of the non-prepared group. The groups differed significantly (independent T test, df = 98, T = 6.90, P < 0.001) when the change in
radial pulse rate (rate after sampling minus rate before sampling) was computed: non-prepared children showed more positive increases in pulse rate after sampling.
Change in pulse rate correlated positively with the child’s
VAS rating of how painful the procedure had been (Spearman’s rank order coefficient of correlation, r, z=
0.19. n = 100. P < 0.05): the greater the increase in pulse rate shown, the more painful the procedure was
reported to have been.
Observed hehaviour
More non-prepared than prepared children kicked (52% vs. 26%: x’ test, x2 = 7.10, df = 1, P-C 0.01) and were red in the face (58% vs. 36%; x2 test, xz = 4.86,
df = 1, P < 0.05) during blood sampling (Table I). More
prepared than non-prepared children were judged to be pale (48% vs. 24%; x2 test, xz = 6.25, df = 1, P < 0.05) and anxious (76% vs. 36%: x2 test, x2 = 16.24, df = 1, P < 0.001). The groups did not differ significantly in terms of the remaining behaviours (x’ test, P > 0.05). Many children reacted by biting their lip (64%), closing
their eyes (78%), and appearing frightened (57%). Thirty-four percent of children cried, 25% verbally com- plained, and 20% screamed during the procedure. A
significant association was found between the observer’s judgement as to whether or not a child was frightened and the child’s own report regarding this (x’ test.
x2 = 4.94, df = 1, P < 0.05).
Interview with child
The vast majority of children (91%) could provide an appropriate description of what had happened during blood sampling, and the groups did not differ signifi-
cantly in this regard (x’ test, P > 0.05; Table II). Significantly more of the prepared (half) than the non- prepared group (less than a third) could explain why the procedure had been carried out (x2 test, x2 = 4.17,
df= 1, P < 0.05). Significantly more non-prepared (two-thirds) than prepared children (one-third) reported
being frightened (x’ test, xz = 10.24, df = 1, P < 0.01).
and judged the procedure to have been very painful (x” test. x2 = 12.96, df = 1. P < 0.001). This accords with
the VAS pain Non-prepared
"1
ratings provided by the children (Fig. 2). children reported reliably higher levels of
VAS MN RATING BY CHILD
VAS RUN RA”
Fig. 2. VAS pain ratings by prepared and non-prepared children.
303
PARENTS’ RATING CF CHILD’S PAIN
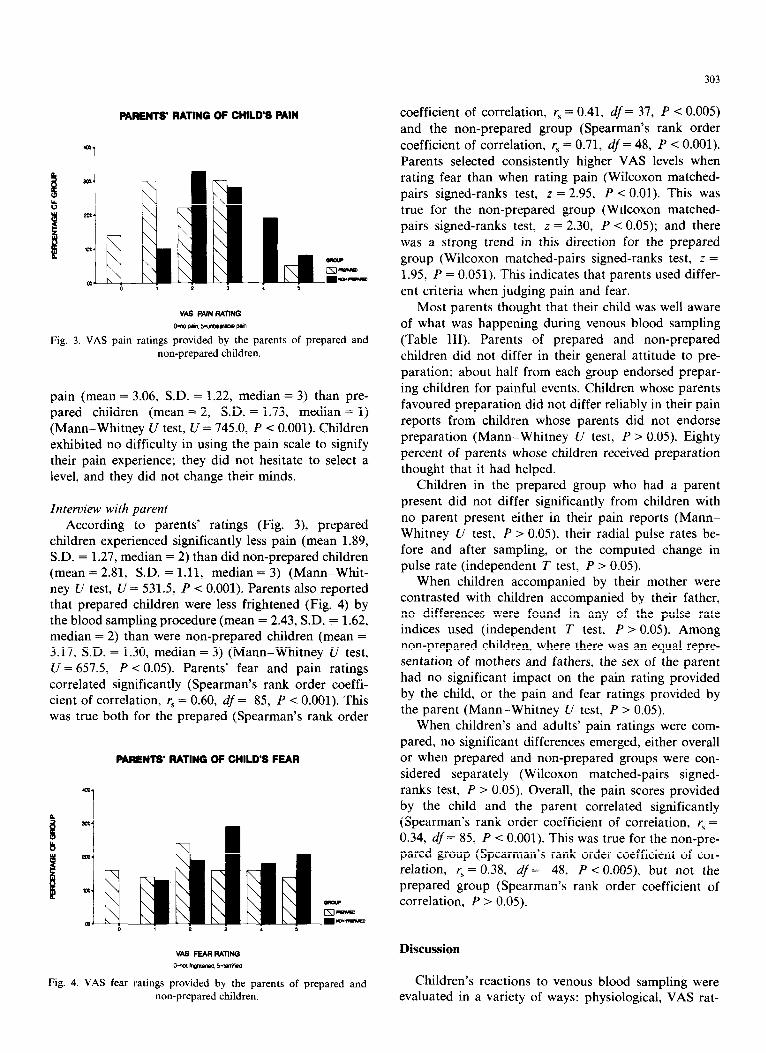
Fig. 3. VAS pain ratings provided by the parents of prepared and non-prepared children.
pain (mean = 3.06, S.D. = 1.22, median = 3) than pre- pared children (mean = 2, S.D. = 1.73, median = 1)
(Mann-Whitney U test, CT = 745.0, P < 0.001). Children exhibited no difficulty in using the pain scale to signify
their pain experience; they did not hesitate to select a level, and they did not change their minds.
Interview with parent According to parents’ ratings (Fig. 3), prepared
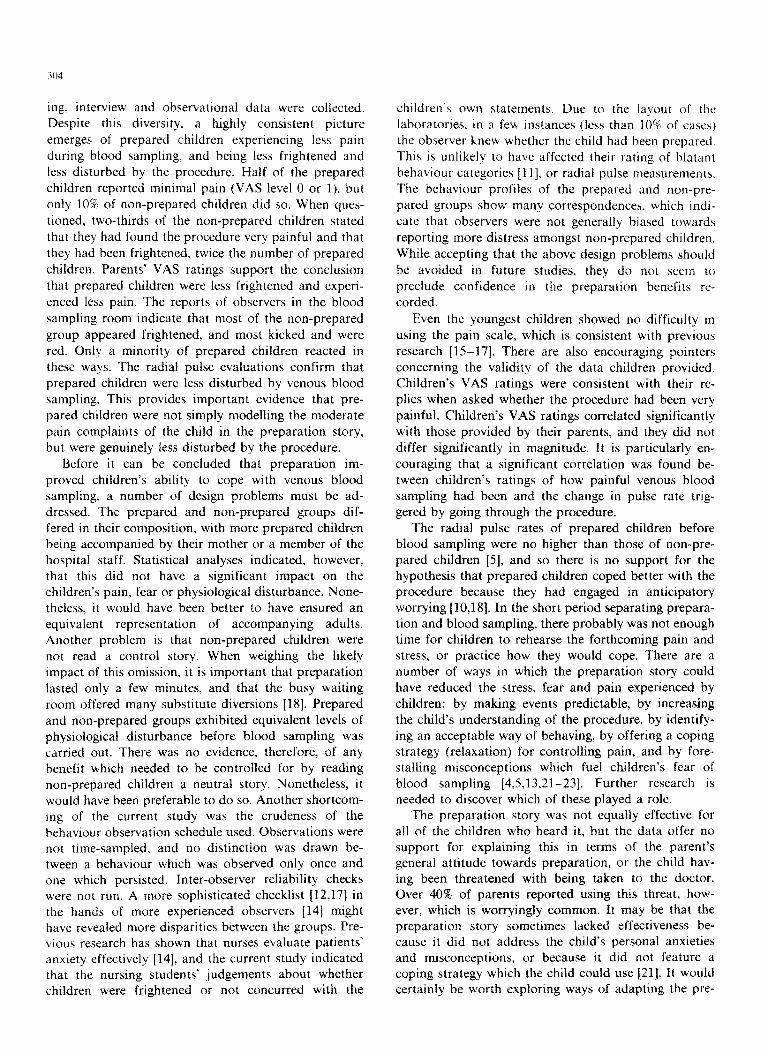
children experienced significantly less pain (mean 1.89, SD. = 1.27, median = 2) than did non-prepared children (mean = 2.81, S.D. = 1.11, median = 3) (Mann-Whit- ney U test, U = 531.5, P -e 0.001). Parents also reported that prepared children were less frightened (Fig. 4) by the blood sampling procedure (mean = 2.43, S.D. = 1.62, median = 2) than were non-prepared children (mean = 3.17, S.D. = 1.30, median = 3) (Mann-Whitney U test,
U = 657.5, P < 0.05). Parents’ fear and pain ratings correlated significantly (Spearman’s rank order coeffi- cient of correlation, r, = 0.60, df = 85, P -c 0.001). This was true both for the prepared (Spearman’s rank order
PARENTS’ RATING OF CHILD’S FEAR
Fig. 4. VAS fear ratings provided by the parents of prepared and non-prepared children.
coefficient of correlation, r, = 0.41, df = 37, P < 0.005) and the non-prepared group (Spearman’s rank order
coefficient of correlation, r, = 0.71, df = 48, P < 0.001).
Parents selected consistently higher VAS levels when rating fear than when rating pain (Wilcoxon matched-
pairs signed-ranks test, z = 2.95, P < 0.01). This was
true for the non-prepared group (Wilcoxon matched- pairs signed-ranks test, z = 2.30, P < 0.05); and there
was a strong trend in this direction for the prepared
group (Wilcoxon matched-pairs signed-ranks test, z =
1.95, P = 0.051). This indicates that parents used differ-
ent criteria when judging pain and fear.
Most parents thought that their child was well aware
of what was happening during venous blood sampling
(Table III). Parents of prepared and non-prepared children did not differ in their general attitude to pre-
paration: about half from each group endorsed prepar-
ing children for painful events. Children whose parents favoured preparation did not differ reliably in their pain
reports from children whose parents did not endorse
preparation (Mann-Whitney U test, P > 0.05). Eighty
percent of parents whose children received preparation thought that it had helped.
Children in the prepared group who had a parent present did not differ significantly from children with
no parent present either in their pain reports (Mann-
Whitney U test, P > 0.05), their radial pulse rates be- fore and after sampling, or the computed change in pulse rate (independent T test, P > 0.05).
When children accompanied by their mother were contrasted with children accompanied by their father, no differences were found in any of the pulse rate indices used (independent T test, P > 0.05). Among non-prepared children, where there was an equal repre- sentation of mothers and fathers, the sex of the parent
had no significant impact on the pain rating provided
by the child, or the pain and fear ratings provided by the parent (Mann-Whitney U test, P > 0.05).
When children’s and adults’ pain ratings were com-
pared, no significant differences emerged, either overall
or when prepared and non-prepared groups were con- sidered separately (Wilcoxon matched-pairs signed-
ranks test, P > 0.05). Overall, the pain scores provided by the child and the parent correlated significantly (Spearman’s rank order coefficient of correlation, r, = 0.34, df = 85, P < 0.001). This was true for the non-pre- pared group (Spearman’s rank order coefficient of cor- relation, [\ = 0.38, df = 48, P -c O.OOS), but not the prepared group (Spearman’s rank order coefficient of correlation, P > 0.05).
Discussion
Children’s reactions to venous blood sampling were evaluated in a variety of ways: physiological, VAS rat-
304
ing, interview and observational data were collected. Despite this diversity. a highly consistent picture emerges of prepared children experiencing less pain
during blood sampling, and being less frightened and less disturbed by the procedure. Half of the prepared
children reported minimal pain (VAS level 0 or 1). but
only 10% of non-prepared children did so. When ques-
tioned, two-thirds of the non-prepared children stated
that they had found the procedure very painful and that
they had been frightened, twice the number of prepared
children. Parents’ VAS ratings support the conclusion that prepared children were less frightened and experi-
enced less pain. The reports of observers in the blood
sampling room indicate that most of the non-prepared
group appeared frightened, and most kicked and were
red. Only a minority of prepared children reacted in these ways. The radial pulse evaluations confirm that
prepared children were less disturbed by venous blood sampling. This provides important evidence that pre-
pared children were not simply modelling the moderate pain complaints of the child in the preparation story, but were genuinely less disturbed by the procedure.
Before it can be concluded that preparation im-
proved children’s ability to cope with venous blood sampling, a number of design problems must be ad- dressed. The prepared and non-prepared groups dif-
fered in their composition, with more prepared children being accompanied by their mother or a member of the
hospital staff. Statistical analyses indicated, however, that this did not have a significant impact on the children’s pain, fear or physiolo~cal disturbance. None-
theless, it would have been better to have ensured an equivalent representation of accompanying adults. Another problem is that non-prepared children were not read a control story. When weighing the likely impact of this omission. it is important that preparation
lasted only a few minutes, and that the busy waiting room offered many substitute diversions [18]. Prepared
and non-prepared groups exhibited equivalent levels of physiological disturbance before blood sampling was carried out. There was no evidence, therefore, of any benefit which needed to be controlled for by reading non-prepared children a neutral story. Nonetheless, it would have been preferable to do so. Another shortcom- ing of the current study was the crudeness of the behaviour observation schedule used. Observations were not time-sampled, and no distinction was drawn be- tween a behaviour which was observed only once and one which persisted. Inter-observer reliability checks were not run. A more sophisticated checklist [12,17] in the hands of more experienced observers [14] might have revealed more disparities between the groups. Pre- vious research has shown that nurses evaluate patients’ anxiety effectively [14], and the current study indicated that the nursing students’ judgements about whether children were frightened or not concurred with the
children’s own statements. Due to the layout t,f the laboratories, in a few instances {less than lo%! of case>)
the observer knew whether the child had been prepared.
This is unlikely to have affected their rating of blatant
behaviour categories [II], or radial pulse measurements. The behaviour profiles of the prepared and non-pre-
pared groups show many correspondences. which indi-
cate that observers were not generally biased towards
reporting more distress amongst non-prepared children.
While accepting that the above design problems should
be avoided in future studies, they do not seem to preclude confidence in the preparation benefits re- corded.
Even the youngest children showed no difficulty in using the pain scale, which is consistent with previous
research [15-171. There are also encouraging pointers concerning the validity of the data children provided. Children’s VAS ratings were consistent with their re- plies when asked whether the procedure had been very
painful. Children’s VAS ratings correlated significantly with those provided by their parents, and they did not
differ significantly in magnitude. It is particularly en-
couraging that a significant correlation was found be- tween children’s ratings of how painful venous blood
sampling had been and the change in pulse rate trig- gered by going through the procedure.
The radial pulse rates of prepared children before blood sampling were no higher than those of non-pre- pared children [5], and so there is no support for the hypothesis that prepared children coped better with the procedure because they had engaged in anticipatory worrying [10,18]. In the short period separating prepara- tion and blood sampling, there probably was not enough time for children to rehearse the forthcoming pain and stress, or practice how they would cope. There are a number of ways in which the preparation story could have reduced the stress, fear and pain experienced by children: by making events predictable, by increasing
the child’s understanding of the procedure, by identify- ing an acceptable way of behaving, by offering a coping strategy (relaxation) for controlling pain, and by fore- stalling misconceptions which fuel children’s fear of blood sampling [4,5,13.21--231. Further research is needed to discover which of these played a role.
The preparation story was not equally effective for all of the chifdren who heard it, but the data offer no support for explaining this in terms of the parent’s general attitude towards preparation, or the child hav- ing been threatened with being taken to the doctor. Over 40% of parents reported using this threat, how- ever, which is worryingIy common. It may be that the preparation story sometimes lacked effectiveness be- cause it did not address the child’s personal anxieties and misconceptions, or because it did not feature a coping strategy which the child could use [21]. It would certainly be worth exploring ways of adapting the pre-

paration story so as to increase its overall effectiveness, but without making it impracticably long. It would also be worth exploring the benefits, and feasibility, of using adjunct techniques during sampling, such as auditory
distraction or skin coolants, which would not prolong
the procedure or the preparation [3,6]. There may well be a subset of children who are so
fearful of venous blood sampling that brief, late pre- paration will not help them. Excessive fear could have
its origins in the child’s past experience, or reflect a parent’s attitudes and fears [4]. In order to help such children cope with clinical procedures, it will be neces-
sary to develop effective techniques for identifying them, and for moderating their fears, stress and pain. One
model would be to provide such children with more extensive preparation, tailored to meet their particular
fears and arm them with effective coping strategies. Such an investment is probably only practical with a child who will have to face medical interventions re-
peatedly and, certainly, would be impractical if a venous blood sample is needed immediately. Another option is to use pharmacological pain blockers. EMLA cream, a topical anaesthetic containing prilocaine and lignocaine, has been shown to be effective for alleviating venepunc- ture pain in young children [e.g., 11, and no serious side
effects have been noted. Significant anaesthesia is not achieved until about 1 h after application [7-91, which would limit the practicality of using it for routine venous
blood sampling. It does, however, represent a valuable option when there is insufficient time for effective pre- paration, or when preparation cannot make the proce- dure tolerable.
The reactions of non-prepared children in the current study confirm that venous blood sampling can be a very frightening and painful experience for children. Among the local conditions which may have contributed to the distress children showed were the physical arrangement of the laboratory, and the lack of preparation given by parents and technicians. The central waiting area meant that children were exposed to the distress of patients
ahead of them. It might be counterproductive, however, for patients to use a different exit route; for it is not
clear what interpretation children would place on hear-
ing an upset patient ahead of them and never seeing that person re-emerge. A far more effective solution would be to help children cope with venepuncture, and so provide waiting patients with a positive model to follow. The current study highlighted the need to pro- vide local technicians with more training in ways of minimising children’s distress. Their current strategy of physically restraining upset children seemed merely to feed the child’s anxiety and increase struggling. It is certainly possible that being physically restrained re- duces how much control children feel they have over
events, thereby adding to their stress [22]. Only about half of the parents interviewed thought that children
generally should be prepared for painful events, al- though 80% thought that the current preparation had
been beneficial. Previous research has shown that
parents who have witnessed the clinical benefits of preparation do not always go on to adopt preparation
as a general strategy [20]. For the future, it might be possible to address this issue, and that of dissuading
parents from threatening their children with taking them to the doctor when they are naughty, using public
education programmes. In the meantime, the present study offers an example of a simple and brief prepara- tion technique which helped children to cope with a
common, invasive medical procedure.
There is a clear need to try and ensure that children do not find medical procedures intolerably painful and
frightening. This is not to suggest that all procedures should be made pain-free, however, for children do
benefit from learning that they can cope with stress and
pain [18]. The challenges for the future are to develop
effective tools for predicting how a given child will react
to a given clinical procedure, and how that child can most effectively be helped to cope, and to develop a rich
range of options for alleviating stress, fear and pain.
Acknowledgements
The study was conducted by the following students from the Faculty of Allied Health Sciences and Nursing as part of course 211AH ‘The Psychology of Medical Care’: L. Al-Ghussien, R. Al-Hassan, A. Al-Kandari, R. Al-Methen, M. Al-Otaibi, F. Al-Serry, N. Hussan, A. Ibrahim, F. Ibrahim and H. Mohammed. The expert help of Mrs. Fawsia Yousif and Miss Zenas Mundegar
is also gratefully acknowledged. This work was supported by Kuwait University Pro-
ject MU072.
References
1 Cooper, C.M., Gerrish, S.P., Hardwick, M. and Kay, R., EMLA cream reduces the pain of venepuncture in children, Eur. J.
Anaesthesiol., 4 (1987) 441-448.
2 Dahlquist, L.M., Gil, K.M., Armstrong, F.D., Ginsberg, A. and
Jones, B., Behavioral management of children’s distress during
chemotherapy, J. Behav. Ther. Exp. Psychiat., 16 (1985) 32.5-329.
3 Eland, J.M., Minimizing pain associated with prekindergarten
intramuscular injections, Iss. Comprehens. Pediat. Nurs., 5 (1981)
361-372.
4 Fassler, D., The fear of needles in children, Am. J. Orthopsychiat.,
53 (1985) 371-377.
5 Fassler, D. and Wallace, N., Children’s fear of needles, Clin.
Pediat., 21 (1982) 59-60.
6 Fowler-Kerry, S. and Lander, J.R., Management of injection pain
in children, Pain, 30 (1987) 169-175.
7 Hallen, B., Olsson, G.L. and Uppfeldt, A., Pain-free venepuncture,
Anaesthesia, 39 (1984) 969-972.
8 Hallperin, D.L., Koren, G., Attias, D., Pellegrini, E., Greenberg,

M.L. and Wyss, M., Topical skin anesthesia for venous. suhcuta-
neous drug reservoir and lumbar punctures in children. Pediatrics.
84 (1989) 281-284.
9 Hopkins. C.S.. Buckley. C.J. and Bush. G.H.. Pain-free injection in
infants, Anaesthesia, 43 (1988) 198~201,
10 Janis. I.L.. Psychological Stress, Wiley. New York. 1958.
11
12
13
14
15
Jay, S.M.. Elliott, C.H., Ozolins, M., Olson, R.A. and Pruitt. SD.,
Behavioral management of children’s distress during painful medi-
cal procedures, Behav. Res. Ther., 23 (1985) 513-520.
Jay, S.M.. Ozolins. M., Elliott, C.H. and Caldwell. S., Assessment
of children’s distress during painful medical procedures, Hlth
Psycho].. 2 (1983) 133-147.
Keefe. F.J. and Gil, KM., Behavioral concepts in the analysis of
chronic pain syndromes. J. Consult. Clin. Psychoi.. 54 (1986)
776-783.
LeBaron. S. and Zeltzer, L.. Assessment of acute pain and anxiety
in children and adolescents by self-reports. observer reports, and a
behavior checklist, J. Consult. Clin. Psycho]., 52 (1984) 729-738.
McGrath, P.A.. An assessment of children’s pain: a review of
behavioral. physiological and direct scaling techniques. Pain, 31
(1987) 147-176.
16 McGrath. P.J.. Cunningham, S.J.. Goodman. J.‘l md Ilnruh. A..
The clinical measurement of pain in children: a revie\ls, <‘lln. .1
Pam. I (19X6) 221-227.
I7 McGrath. P.J. and Unruh. A.. Pain in Children and Adolescents.
Elsevler. Amsterdam. 1987.
18 Melamed, B.G.. Psychological preparation for hoapitahzation. In:
S. Rachman (Ed.). Contributions to Medical Psychology. Vol. I.
Pergamon. Oxford. 1977, pp. 43.-74.
19 Nocella. J. and Kaplan. R.M.. Training children to cope with
dental treatment. J. Pediat. Psycho]., 7 (1982) 17% 178.
20 Peterson. L. and Shigetomi. C., One-year follow-up of elective
surgery child patients receiving preoperative preparation. J. Pediat.
Psycho]., 7 (1982) 43-48.
21 Reissland. N.. Cognitive maturity and the experience of fear and
pain in hospital. Sot. Sci. Med., 17 (1983) 1389-1395.
22 Tan. S.-Y., Cognitive and cognitive-behavioral methods for pain
control: a selective review. Pain. 12 (1982) 201-228.
23 Vernon, D.T.A.. Foley. J.M.. Sipowicz. R.R. and Schulman, J.L..
The Psychological Responses of Children to Hospitalization and
Illness. Thomas. Springfield. IL. 1965.