Embed Size (px)
Citation preview
Journal of Medical Virology 42151-157 (1994)
Presence of Hepatitis B and C Viral Genomes in US Blood Donors as Detected by Polymerase Chain Reaction Amplification T. Jake Liang, Henry C. Bodenheimer, Jr., Ronald Yankee, Nancy V. Brown, Kenneth Chang, Jiakang Huang, and Jack R. Wands Gastrointestinal Unit, Massachusetts General Hospital, Boston, Molecular Hepatology Laboratory, Massachusetts General Hospital Cancer Center, Charlestown, and Department of Medicine, Haruard Medical School, Boston, Massachusetts (T.J.L., N.V.B., J.H., J.R. W,) , and Mt. Sinai School of Medicine, New York, New York (H.C.B.) and Rhode Island Blood Center, Brown University (R.Y., K.C.), Providence, Rhode Island
Hepatitis C virus (HCV) represents a major cause of posttransfusion hepatitis worldwide. Post- transfusion hepatitis associated with hepatitis B virus (HBV) continues to occur. HBsAg-negative donor sera from the Rhode Island Blood Center between 1987 and 1988 were screened using more sensitive techniques to assess the preva- lence of low level HBV infection. Group I consists of 866 healthy blood donors without HBV sero- logic markers, group II consists of 377 donors with ALT elevations (>45 IU/L), group II consists of 148 donors positive for anti-HBc, and group IV consists of eight donors positive for both surro- gate markers. A sensitive monoclonal immuno- radiometric assay (M-IRMA) was employed for detection of HBsAg-associated epitopes (detec- tion limit of 20 pg/mI) in serum. A subset of sera were analyzed for the presence of HBV DNA us- ing the method of anti-HBs capture of HBV re- lated virions in serum followed by polymerase chain reaction (PCR) amplification. Using these techniques, 0.8% and 1.7% of donors were posi- tive for HBsAg and HBV DNA respectively in group 1. In contrast, 0.9% and 9.5% in group II and 0.7% and 18.1% in group Ill were positive, respectively. There were eight donors with both ALT elevation and anti-HBc; and four (50°/0) of these were positive for HBV DNA. In the group with anti-HBc, the majority (80%) of donors with HBV DNA had either no or low (signal to noise ratio <lo) anti-HBs titer. Using anti-HCV testing and reverse transcription-PCR for detection of HCV genomes, we detected evidence of HCV in- fection in nine of the 49 donors with low level HBV DNA.
We demonstrate that low level HBV viremia otherwise undetectable by conventional method are prevalent in donor grups with either or both of the surrogate and HCV infection either alone or as co-infecting agent are also common in this population. Q 1994 Wi~ey-Liss, Inc.
Q 1994 WILEY-LISS, INC.
KEY WORDS: posttransfusion hepatitis, sur- rogate markers, anti-HBc, ALT elevation
INTRODUCTION Posttransfusion hepatitis remains a significant
health care problem in the United States. The recent identification and characterization of hepatitis C virus (HCV) has led to a diagnostic test to detect presumed HCV infection [Choo et al., 1989; Kuo et al., 19891. Blood donor screening with this test is expected to be effective in eliminating the majority of posttransfusion non-A, non-B hepatitis cases [Van der Poel et al., 1989, 1990; Alter et al., 1989; Stevens et al., 19901. In cotrast, hepatitis B virus (HBV)-associated posttransfusion hepatitis continued to occur despite the implementa- tion of screening test for HBsAg in blood donors [Hoofnagle et al., 1978; Stevens et al., 1984; Dienstag et al., 1986; Polesky et al., 19891. Several studies con- ducted in the late 1970s reported that 5-20% of post- transfusion hepatitis were HBV-related [Stevens et al., 1984; Dienstag et al., 1986; Poelsky et al., 19891. Com- bining polymerase chain reaction (PCR) technology and a highly specific monoclonal anti-HBs antibody, we have developed a rapid, sensitive, and specific method to detect encapsidated low level HBV in serum [Liang et al., 19891. This method involves the capture of viral particles from serum using a high affinity anti-HBs monoclonal antibody directed against a common do- main epitope on the HBV envelope protein and the subsequent amplification of viral DNA by polymerase
Accepted for publication May 18, 1993. Address reprint requests to Dr. T.J. Liang, Gastrointestinal
Unit, Jackson 812, Massachusetts General Hospital, Fruit St., Boston, MA 02114.
Presented in part a t the annual meeting of the American Asso- ciation for Study of Liver Diseases on Nov. 5,1990.

152 Liang et al.
PCR Detection of HBV and HCV Genomes The method of anti-HBs capture-PCR detection of
HBV DNA in serum has been described previously [Li- ang et al., 19891. Four sets of primers spanning the precorelcore, preSlsurface, and X region of the HBV genome were used. Their sequences were described pre- viously [Liang et a]., 1989, 1990a, 1991aI. Since we have previously established that the precorelcore prim- ers are the most sensitive primers for HBV amplifica- tion, we routinely amplified with this set of primers first and then confirm the positivity with other sets of primers LLiang et al., 1989, 1990a, 1991al. Isolation of serum HCV RNA and detection of HCV RNA by the reverse transcription-PCR method have also been de- scribed previously LLiang et al., 19931. Three sets of HCV primers spanning the 5’ untranslated region, NS3, and NS5 were used.
Serologic Tests for Hepatitis B and C The presence of HBsAg in blood donors was also mea-
sured by Auzyme (Abbott Laboratories, North Chicago, IL). Anti-HBs antibodies were measured by Ausab (Ab- bott Laboratories, North Chicago, IL). The anti-HBc status was initially determined by Corzyme and later repeated with the Corab test. Only Corab positive sam- ples were included in the anti-HBc positive group in this study. The M-IRMA to detect low level HBsAg in serum was performed as described previously [Ben- Porath et al., 19851. First generation enzyme-linked immunosorbent assay (ELISA) to detect antibodies to HCV (C-100 antigen) (Abbott Laboratories, North Chi- cago, IL) and a second generation recombinant immu- noblot assay (RIBA 11) to detect anti-HCV [Ebeling et al., 19901 were performed as described. The general prevalence rates of anti-HCV positivity in the donor population from the Providence area with respect to the surrogate markers since May 1990 were 0.9%, 9%, 8%, and 40% for groups I, 11,111, and IV respectively. More than 5,000 donor units were tested for anti-HCV during this period. These data are consistent with what others have reported for United States blood donors [Stevens et al., 19901.
chain reaction. The amplification is initiated using “ge- neric” primers derived from the core and precore se- quences, which are highly conserved amongst the hep- adnaviruses. This rapid technique detects fewer than ten infections virions per 200 ~1 of serum [Liang et al., 19891.
We and others using a similar technique of PCR am- plification of DNA extracted from serum have impli- cated HBV as the possible etiologic factor in some HBsAg-negative individuals with chronic liver disease [Thiers et al., 1988; Kaneko et al., 1989; Liang et al., 1990, 19911. Serum from some of these subjects has been shown to be infectious and transmit acute hepati- tis infection to chimpanzees [Wands et al., 1986; Thiers et a]., 1988; Liang et a]., 1990a,bl. In this report, we have extended our observations and studied serum samples from a large cohort of blood donors with and without ALT elevations and anti-HBc antibodies (the surrogate markers for non-A, non-B hepatitis) from the Rhode Island Blood Center. We also investigated the significance of HCV infection in selected subjects with evidence of low level HBV infection from this pop- ulation using the anti-HCV tests and reverse transcrip- tion(RT)-PCR detection of HCV genomes.
MATERIALS AND METHODS Subjects
Serum samples from 1,407 volunteer blood donors who were negative for HBsAg by Auzyme were selected as random batches from the Rhode Island Blood Center between 1987 and 1988; 866 had no HBV serologic markers or ALT elevations (group I), 377 had elevated ALT values (>45 IU/L) (group 111,148 were positive for anti-HBc (Group 1111, and eight were positive for both surrogate markers (group IV). All donors were asked to complete a brief questionnaire regarding their health and medical conditions prior to donation and this infor- mation was retrieved during this study. Among the anti-HBc positive donors, all were negative for IgM anti-HBC and 41 (35.4%) were negative for anti-HBs. All the donors were tested for HBsAg by M-IRMA, and 293,126,105, and 8 HBsAg-negative donors who were randomly selected from groups I, 11,111, and IV respec- tively were assayed for HBV DNA by anti-HBs capture1 PCR. These samples were stored frozen at -70°C and tested for HBsAg and HBV DNA under code. All donors with circulating HBsAg and/or HBV DNA were ana- lyzed for the co-existence of anti-HCV and HCV RNA, as well as 25 sera selected randomly from each surro- gate marker group. Samples positive for HBsAg by monoclonal immunoradiometric assay (M-IRMA), HBV DNA by anti-HBs capturelPCR amplification, or HCV RNA by RT-PCR were retested independently for con- firmation of positive results. We maintained rigorous precautions to minimize PCR contamination by HBV and HCV as previously described [Liang et al., 1991a; Kwok and Higuchi, 19891.
Statistical Analysis The prevalence rates of various serologic markers
were analyzed for statistical significance by the two- tailed Fisher’s Exact test or Chi-square test with Yates’ correction.
RESULTS Using the methods described above, we studied se-
rum of blood donors from Providence, RI, during 1988 and 1989. Table I illustrates the results. Similar to a previous study [Ben-Porath et al., 19841, we identified additional reactive blood donors with circulating HBsAg by the more sensitive M-IRMA. HBsAg was detected in 71866 (0.8%) donors with no other HBV sero- logic markers. In addition, we detected HBsAg in 31377 (0.970) of donors with ALT elevations, and in 1/148

HBV and HCV in Blood Donors 153
TABLE I. Prevalence of Serum HBV DNA by Anti-HBs Capture1PCR in Blood Donors
Group HBsAg (M-IRMA)" HBV DNA (PCR)
I. No markers 71866 (0.8%) 51293 (1.7%) 11. ALT elevation (>45 IUIL) 31377 (0.9%) 121126 (9.5%)"
111. Anti-HBc 11148 (0.7%) 191105 (18.1%)"" 418 (50%)"" IV. ALT elevation and 018 (0%)
anti-HBc
"Nine of 11 donors with HBsAg by M-IRMA were a1 *P < 0.002 comparing to group I. **P < 0.0005 comparing to group I. Blood donors were divided into three groups accordj (ALT elevation and anti-HBc positivity).
TABLE 11. Prevalence of Serum HBV DNA in Blood Donors With Anti-HBc
Grow Anti-HBc Anti-HBs HBV DNA (PCR)
I. (n = 40) + - 12 (30.0%) 11. (n = 9) + + (SIN < 10) 6 (66.7%)"
111. (n = 64) + + (S1N > 10) 5 (7.8%)""
*P < 0.005 comparing to group I. **P < 0.0001 comparing to group I.
(0.7%) of donors with anti-HBc antibodies. We analyzed these 11 donors by anti-HBs capture/PCR method and nine were positive for HBV DNA as well. Additional randomly selected specimens from each of the three groups (no surrogate markers, positive anti-HBc, or ALT elevations were tested by anti-HBs capture/PCR. We identified circulating virion-associated HBV DNA in 5/293 (1.7%) blood donors with no HBV serologic markers. In contrast, we found a significantly higher percentage of donors with either of the surrogate mark- ers reactive for HBV DNA in their serum (9.5% of do- nors with ALT elevations and 18.1% of donors with anti-HBc positivity). Four of eight blood donors (50%) with both surrogate markers were positive for circulat- ing HBV DNA. Therefore, the prevalence rates of low level HBV carriers in these blood donors will be more accurately reflected by the sum of the results from both tests.
The prevalence rates of HBV DNA in serum of blood donors with anti-HBc antibodies with respect to anti- HBs status are shown in Table 11. Thirty-five percent of serum samples from anti-HBc positive blood donors contained anti-HBc alone whereas the remainder con- tained both anti-HBc and anti-HBs. There was a signif- icantly higher number of donors with no (30%, P < 0.005) or low level anti-HBs (66.7%, P < 0.0001) with HBV DNA in their serum as compared to donors with high titer anti-HBs (7.8%). Blood donors with ALT elevations were also analyzed for the presence of HBV DNA as a function of the magnitude of ALT values (Table 111). Regardless of the anti-HBc status, the prev- alence of circulating HBV DNA was significantly higher in donors with ALT elevation than those with- out.
All the donors with circulating HBsAg and/or HBV DNA with the exception of two (n = 49) were analyzed for the presence of anti-HCV and HCV RNA, as well as
so positive for HBV DNA by PCR.
ing to the presence or absence of surrogate markers
25 sera selected randomly from each surrogate marker group (Table IV). One of the two had no surrogate markers and the other had ALT elevation; their sera were not tested because of inadequate volumes. Six do- nors had co-existence of HBV DNA and anti-HCV: four donors were with both ALT elevations and anti-HBc, the fifth with ALT, and the final one with anti-HBc. In our cohort of blood donors there were a total of eight donors with both surrogate markers, and six of them were positive for anti-HCV. Among these six donors with anti-HCV, four were also positive for HBV DNA in their serum by PCR. Since the presence of anti-HCV antibodies may not indicate active HCV infection, we employed a reverse transcription-PCR (RT-PCR) method using three sets of primers spanning different regions of the HCV genome. Again, all the available donor units with circulating HBsAg and/or HBV DNA were analyzed by this RT-PCR method. We found that five of six donors who previously tested positive for anti-HCV contained HCV RNA in their serum (Fig. 1); three of these five were positive for both surrogate markers, the fourth had anti-HBc, and the fifth had ALT elevation. One donor who had anti-HCV but tested negative for HCV RNA was positive for both markers. Three additional donors of the remaining 38 without anti-HCV were shown to harbor HCV genomes (Fig. 1). Of these three donors, one had no serologic marker, the second had an ALT elevation and the third carried anti- HBc; none of them were positive or indeterminate for anti-HCV in RIBA 11. Five of the 25 randomly selected samples from each group were positive (three with ALT elevation and two with anti-HBc). They were also ana- lyzed for HCV RNA in their serum. Only two of the donors with ALT elevations and one with anti-HBc con- tained HCV RNA in serum (Table IV). ALL three were also positive for anti-HCV. In contrast to the group of donors with HBV DNA, none of the donor controls who were anti-HCV negative were positive for HCV RNA.
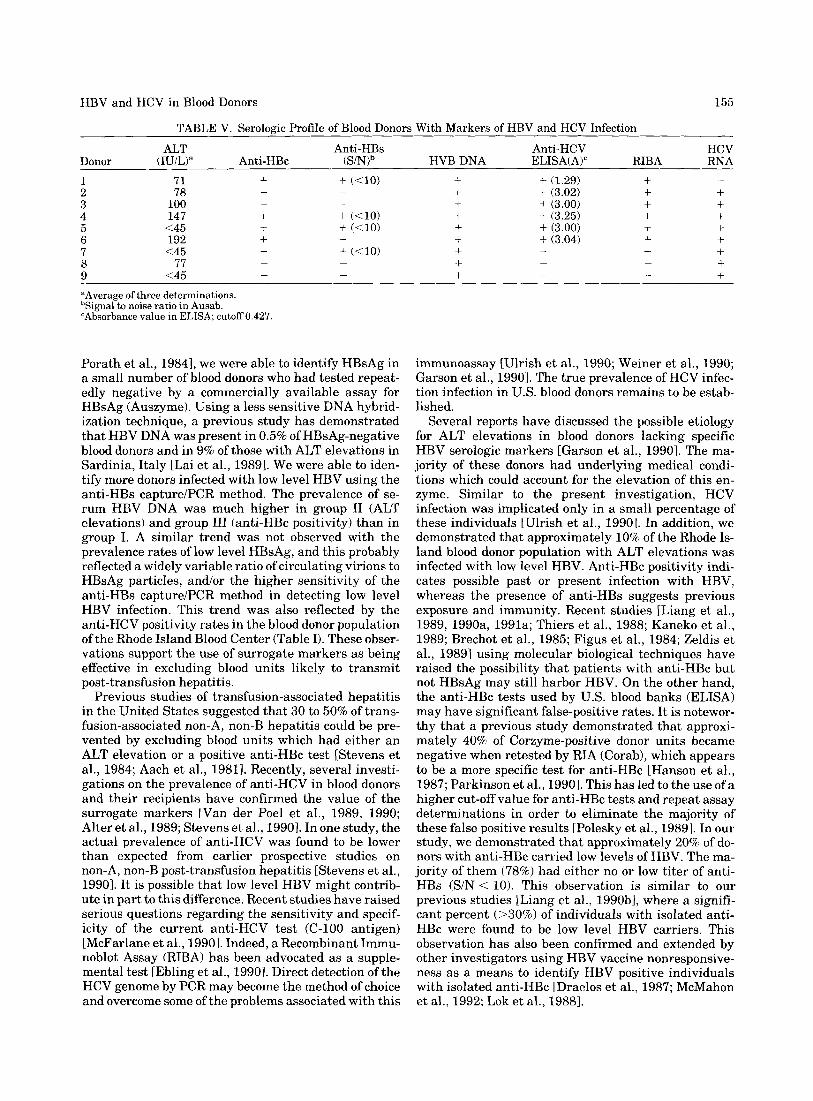
The serologic profiles and PCR results for HBV and HCV of the donors with both serum HBV DNA and anti-HCV (or HCV RNA) are summarized in Table V. All except for donor no. 9 had either one or both of the surrogate markers. None had a history of jaundice or hepatitis and there was no history of prior transfusion or intravenous drug abuse. The six donors with anti- HCV all had high signals in the ELISA assay (>3.0 O.D.) and the anti-HCV status of all six were confirmed
154 Liang et al.
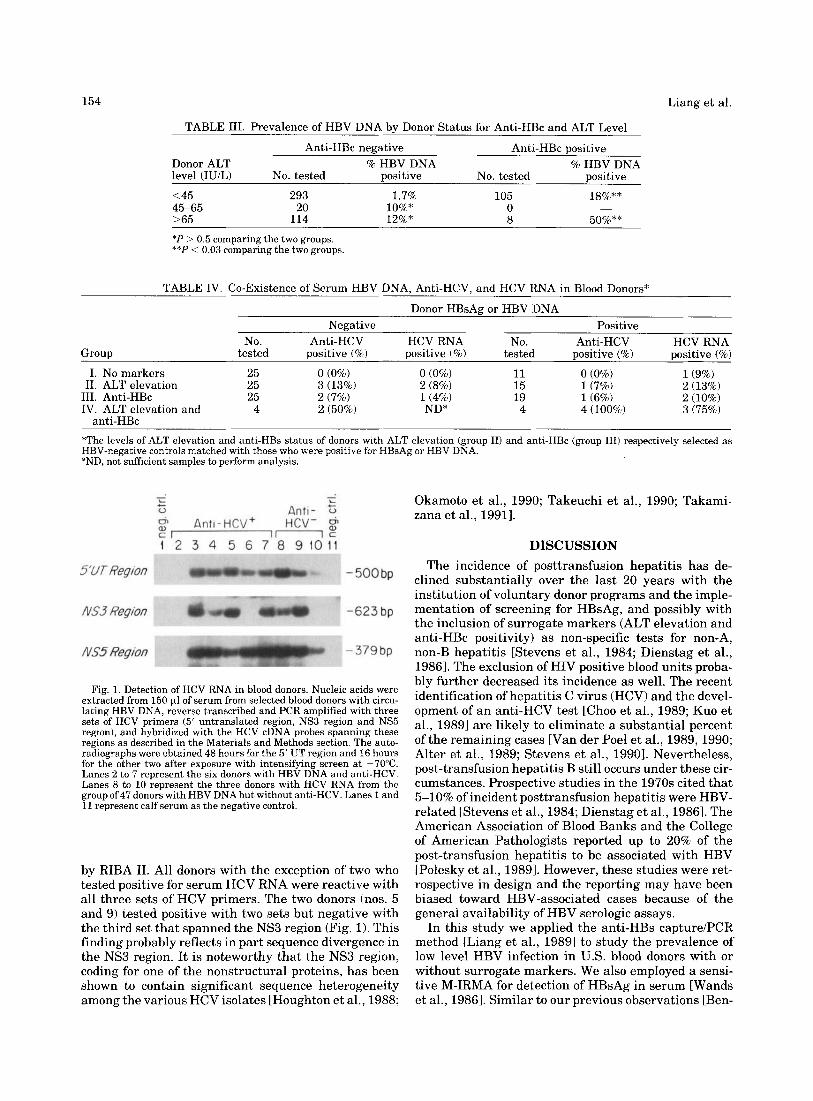
TABLE 111. Prevalence of HBV DNA by Donor Status for Anti-HBc and ALT Level
Anti-HBc negative Anti-HBc positive Donor ALT % HBV DNA % HBV DNA level (IUiL) No. tested positive No. tested positive <45 293 1.7% 105 la%** 45-65 20 lo%* 0 >65 114 12%" 8 50%** *P > 0.5 comparing the two groups. **P < 0.03 comparing the two groups.
-
TABLE IV. Co-Existence of Serum HBV DNA, Anti-HCV, and HCV RNA in Blood Donors"
Donor HBsAg or HBV DNA Negative Positive
No. Anti-HCV HCV RNA No. Anti-HCV HCV RNA Group tested positive (%) positive (%) tested positive (%) positive (%)
I. No markers 25 0 (0%) 0 (0%) 11 0 (0%) 1(9%) 11. ALT elevation 25 3 (13%) 2 (8%) 15 1(7%) 2 (13%)
111. Anti-HBc 25 2 (7%) 1(4%) 19 1(6%) 2 (10%) IV. ALT elevation and 4 2 (50%) ND" 4 4 (100%) 3 (75%)
anti-HBc *The levels of ALT elevation and anti-HBs status of donors with ALT elevation (group 11) and anti-HBc (group 111) respectively selected as HBV-negative controls matched with those who were positive for HBsAg or HBV DNA. "ND, not sufficient samples to perform analysis.
Okamoto et al., 1990; Takeuchi et al., 1990; Takami- zana et al., 19911.
DISCUSSION The incidence of posttransfusion hepatitis has de-
clined substantially over the last 20 years with the institution of voluntary donor programs and the imple- mentation of screening for HBsAg, and possibly with the inclusion of surrogate markers (ALT elevation and anti-HBc positivity) as non-specific tests for non-A, non-B hepatitis [Stevens et al., 1984; Dienstag et al., 19861. The exclusion of HIV Dositive blood units Droba- bly further decreased its incidence as well. The ;ecent identification Of hepatitis virus (HCV) and the devel- opment of an anti-HCV test [Choo et al., 1989; Kuo et al., 19891 are likely to eliminate a substantial percent ofthe remaining cases [Van der Pod et al., 1989, 1990; Alter e t al., 1989; Stevens et al., 19901. Nevertheless, post-transfusion hepatitis B still occurs under these cir- cumstances. Prospective studies in the 1970s cited that
related [Stevens et al., 1984; Dienstag et al., 19861. The
Fig. 1. Detection of HCV RNA in blood donors. Nucleic acids were extracted from 150 p,1 of serum from selected blood donors with circu- lating HBV DNA, reverse transcribed and PCR amplified with three sets of HCV primers (5' untranslated region, NS3 region and NS5 region), and hybridized with the HCV cDNA probes spanning these regions as described in the Materials and Methods section. The auto- radiographs were obtained 48 hours for the 5' UT region and 16 hours for the other two after exposure with intensifying screen at -70°C. Lanes to represent the six donors with HBV DNA and anti-HCV, Lanes 8 to 10 represent the three donors with HCV RNA from the group of 47 donors with HBV DNA but without anti-HCV. Lanes 1 and 11 represent calf serum as the negative control.
5-10% of incident posttransfusion hepatitis were HBV-
by RIBA 11. All donors with the exception of two who tested positive for serum HCV RNA were reactive with all three sets of HCV primers. The two donors (nos. 5 and 9) tested positive with two sets but negative with the third set that spanned the NS3 region (Fig. 1). This finding probably reflects in part sequence divergence in the NS3 region. It is noteworthy that the NS3 region, coding for one of the nonstructural proteins, has been shown to contain significant sequence heterogeneity among the various HCV isolates [Houghton et al., 1988;
American Association of Blood Banks and the College of American Pathologists reported up to 20% of the post-transfusion hepatitis to be associated with HBV [Polesky et al., 19891. However, these studies were ret- rospective in design and the reporting may have been biased toward HBV-associated cases because of the general availability of HBV serologic assays.
In this study we applied the anti-HBs capture/PCR method [Liang et al., 19891 to study the prevalence of low level HBV infection in U.S. blood donors with or without surrogate markers. We also employed a sensi- tive M-IRMA for detection of HBsAg in serum [Wands et al., 19861. Similar to our previous observations [Ben-
HBV and HCV in Blood Donors 155
TABLE V. Serologic Profile of Blood Donors With Markers of HBV and HCV Infection ALT Anti-HBs
Donor (IU/L)" Anti-HBc 1 71 + + ((10) 2 78 3 100 + 4 147 + + (< lo)
<45 + + (< lo) 5 6 192 +
<45 + + (< lo) 7 77 8
9 <45
"Average of three determinations. bSignal to noise ratio in Ausab. 'Absorbance value in ELISA; cutoff 0.427.
- ~
-
-
- -
- -
Porath et al., 19841, we were able to identify HBsAg in a small number of blood donors who had tested repeat- edly negative by a commercially available assay for HBsAg (Auszyme). Using a less sensitive DNA hybrid- ization technique, a previous study has demonstrated that HBV DNA was present in 0.5% of HBsAg-negative blood donors and in 9% of those with ALT elevations in Sardinia, Italy [Lai e t al., 19891. We were able to iden- tify more donors infected with low level HBV using the anti-HBs capture/PCR method. The prevalence of se- rum HBV DNA was much higher in group I1 (ALT elevations) and group 111 (anti-HBc positivity) than in group I. A similar trend was not observed with the prevalence rates of low level HBsAg, and this probably reflected a widely variable ratio of circulating virions to HBsAg particles, andlor the higher sensitivity of the anti-HBs capturelPCR method in detecting low level HBV infection. This trend was also reflected by the anti-HCV positivity rates in the blood donor population of the Rhode Island Blood Center (Table I). These obser- vations support the use of surrogate markers as being effective in excluding blood units likely to transmit post-transfusion hepatitis.
Previous studies of transfusion-associated hepatitis in the United States suggested that 30 to 50% of trans- fusion-associated non-A, non-B hepatitis could be pre- vented by excluding blood units which had either an ALT elevation or a positive anti-HBc test [Stevens et al., 1984; Aach et al., 19811. Recently, several investi- gations on the prevalence of anti-HCV in blood donors and their recipients have confirmed the value of the surrogate markers [Van der Poel et al., 1989, 1990; Alter et al., 1989; Stevens et al., 19901. In one study, the actual prevalence of anti-HCV was found to be lower than expected from earlier prospective studies on non-A, non-B post-transfusion hepatitis [Stevens et al., 19901. It is possible that low level HBV might contrib- ute in part to this difference. Recent studies have raised serious questions regarding the sensitivity and specif- icity of the current anti-HCV test (C-100 antigen) [McFarlane et al., 19901. Indeed, a Recombinant Immu- noblot Assay (RIBA) has been advocated as a supple- mental test [Ebling et al., 19901. Direct detection of the HCV genome by PCR may become the method of choice and overcome some of the problems associated with this
Anti-HCV HCV HVB DNA ELISA(AF RIBA RNA
- + + (1.29) + + + (3.02) + + + + (3.00) + + + + (3.25) + + + + (3.00) + + + + (3.04) + +
+ + +
- - + + +
- -
- -
immunoassay [Ulrish et al., 1990; Weiner et al., 1990; Garson et al., 19901. The true prevalence of HCV infec- tion infection in U.S. blood donors remains to be estab- lished.
Several reports have discussed the possible etiology for ALT elevations in blood donors lacking specific HBV serologic markers [Garson et al., 19901. The ma- jority of these donors had underlying medical condi- tions which could account for the elevation of this en- zyme. Similar to the present investigation, HCV infection was implicated only in a small percentage of these individuals [Ulrish et al., 19901. In addition, we demonstrated that approximately 10% of the Rhode Is- land blood donor population with ALT elevations was infected with low level HBV. Anti-HBc positivity indi- cates possible past or present infection with HBV, whereas the presence of anti-HBs suggests previous exposure and immunity. Recent studies [Liang et al., 1989, 1990a, 1991a; Thiers et al., 1988; Kaneko et al., 1989; Brechot et al., 1985; Figus et al., 1984; Zeldis et al., 19891 using molecular biological techniques have raised the possibility that patients with anti-HBc but not HBsAg may still harbor HBV. On the other hand, the anti-HBc tests used by U S . blood banks (ELISA) may have significant false-positive rates. It is notewor- thy that a previous study demonstrated that approxi- mately 40% of Corzyme-positive donor units became negative when retested by RIA (Corab), which appears to be a more specific test for anti-HBc [Hanson et al., 1987; Parkinson et al., 19901. This has led to the use of a higher cut-off value for anti-HBc tests and repeat assay determinations in order to eliminate the majority of these false positive results [Polesky et al., 19891. In our study, we demonstrated that approximately 20% of do- nors with anti-HBc carried low levels of HBV. The ma- jority of them (78%) had either no or low titer of anti- HBs (SlN < 10). This observation is similar to our previous studies [Liang et al., 1990b1, where a signifi- cant percent (>30%) of individuals with isolated anti- HBc were found to be low level HBV carriers. This observation has also been confirmed and extended by other investigators using HBV vaccine nonresponsive- ness as a means to identify HBV positive individuals with isolated anti-HBc [Draelos e t al., 1987; McMahon et al., 1992; Lok et al., 19881.

156 Liang et al.
could be misclassified as non-A, non-B hepatitis [Thiers et al., 1988; Wands et al., 1986; Coursaget et al., 19871. More recent studies suggest that there are HBV vari- ants that may exhibit unusual biologic and serologic behavior [Carman et al., 1989, 1990; Brunetto et al., 1990; Liang et al., 1991bI. In order to establish the clinical significance of low level HBV infection, i t will be necessary to analyze prospectively followed donors and recipients with respect to the occurrence of transfu- sion-associated hepatitis.
ACKNOWLEDGMENTS We are grateful for the excellent secretarial assis-
tance of Ms. Kristin Cambria and the expert technical help of Rolf Carlson. We also thank Ms. Jane Petrucci and her staff a t the Rhode Island Blood Center for per- forming anti-HCV ELISA tests and Dr. Mitchell Nelles at Ortho Diagnostics for carrying out second generation anti-HCV RIBA tests. This work was supported by grants DK01952, CA-54524, AA-02666, CA-35711, and AA-08169 from the National Institutes of Health, USA.
Four of eight donors with ALT elevation and anti- HBc positivity harbored circulating HBV DNA as well as anti-HCV antibodies. The co-infection of HBV and HCV may suppress HBV replication, thus contributing to the low level of HBV DNA in serum which is only detectable by a highly sensitive method, such as the PCR. Suppression of HBV replication by HCV co-infec- tion has also been suggested by others [Brotman et al., 19831 and this phemonenon has been well-described in HBV and HDV co-infection [Hoofnagle e t al., 19891. Using RT-PCR detection as a means of identifying HCV genomes in serum, we were able to confirm that the majority of donors with anti-HCV do indeed harbor the HCV virus in their blood. Since an equivalent of 50 pl of serum was used in each RT-PCR for the detection of HCV genomes, it is possible that some donors carrying very low level HCV may have been missed. This could indeed be the case in donor no. 1 (Table V), who was positive for anti-HCV by RIBA I1 but negative for HCV RNA by RT-PCR. Others have reported that by using a higher volume of serum, HCV sequences may be de- tected in additional patients [Ulrish et al., 19901. Un- fortunately, we did not have any more serum from do- nor no. 1 for additional testing. In addition, HCV RNA was identified in three HBV DNA-positive donors who were negative for anti-HCV even by the second-genera- tion RIBA. This finding is consistent with other reports comparing the presence of anti-HCV with HCV RNA as detected by RT-PCR [Ulrish et al., 1990; Garson et al., 1990; Katkov et al., 1989; Sugitani et al., 19921 and raises doubts regarding the sensitivity of first and sec- ond generation anti-HCV assays. These observations suggest that co-infection by both HBV and HCV may be common.
Using the anti-HBs captureiPCR method, we were able to detect the presence of virion-associated HBV DNA in 1.7% of healthy blood donors from Providence, RI. However, the true prevalence rate remains to be established since the number of donors studied was small. At present, we have no direct evidence that low level HBV in these healthy blood donors are clinically significant, i.e., whether they are infectious. We were unable to obtain follow-up data on the recipients of these donor units containing low level HBV in order to address this question. We can only speculate regarding the clinical significance of this low level HBV carrier state with respect to the transmission of post-transfu- sion hepatitis. Fewer than 100 HBV virions could cause hepatitis B infection in chimpanzees [Prince et al., 19831. HBsAg-negative serum with low level HBV DNA derived from patients with or without HBV sero- logic markers has been shown to transmit hepatitis in chimpanzees [Liang et al., 1989, 1990a; Thiers et al., 1988; Wands et al., 1986J. Therefore, we are led to be- lieve that some of these donor units are probably infec- tious.
Transfusion of donor units with low level HBV DNA could be associated with acute transfusion-associated hepatitis B or HBV-associated hepatitis without con- ventional HBV serologic markers. The latter cases
REFERENCES Aach R, Szmuness W, Mosley JW, Hollinger FB, Kahn RA, Stevens
CE, Edwards VM, Werch J (1981): Serum alamine aminotrans- ferase of donors in relation to the risk of non-A, non-B hepatitis in recipients. The transfusion-transmitted viruses study. New En- gland Journal of Medicine 304:989-994.
Alter H, Purcell R, Shih JW, Melpolder JC, Houghton M, Choo G-L, Kuo G (1989): Detection of antibody to hepatitis C virus in prospec- tively followed transfusion recipients with acute and chronic non-A, non-B hepatitis. New England Journal of Medicine 321: 1494-1500.
Ben-Porath E, Wands J , Gruia M, Isselbacher K (1984): Clinical sig- nificance of enhanced detection of HBsAg by a monoclonal radio- immunoassay. Hepatology 4303-807.
Ben-Porath E, Wands JR, Bar-Shany S, Huggins SC, Isselbacher KJ (1985): Improved detection of hepatitis B surface antigen (HBsAg) in blood donors by monoclonal radioimmunoassay. Transfusion 2510-16.
Brechot C, Degos F, Lugassy C, Thiers V, Safrani S, France D, Bis- muth H, Trepo C, Benhamou J-P, Wands JR, Isselbacher KJ, Tiol- lais P, Berthelot P (1985): Hepatitis B virus DNA in patients with chronic liver disease and negative tests for hepatitis B surface antigen. New England Journal of Medicine 312:270-276.
Brotman B, Prince AM, Huima T, Richardson MC, van den Ende MC, Pfeifer U (1983): Interference between non-A, non-B and hepatitis B virus infection in Chimpanzees. Journal of Medical Virology 11:191-205.
Brunetto MR, Stemler M, Bonino F, Schodel F, Oliveri F, Rizzetto M, Verme G, Will H (1990): A new hepatitis B virus strain in patients with severe anti-HBe positive chronic hepatitis B. Journal of He- patology 10:258-261.
Carman WF, Jacyna MR, Hadziyannis S, Karayiannis P, McGarvey MJ, Makris A, Thomas HC (1989): Mutation preventing formation ofhepatitis e antigen in patients with chronic hepatitis B infection. Lancet 11:588-591.
Carman WF, Zanetti AR, Karayiannis P, Waters J, Manzillo G, Tanzi E, Zuckerman AJ, Thomas HC (1990): Vaccine-induced escape mu- tant of hepatitis B virus. Lancet 336:325-329.
Choo Q-L, Kuo G, Weinger AJ, Overby LR, Bradley DW, Houghton M (1989): Isolation of a cDNA clone derived from a blood borne non-A non-B viral genome. Science 244:359-362.
Coursaget P, Yvonnet B, Bourdil C, Mevelec MN, Adamonicz P, Barres JL, Chotard J, NDoye R, DiopMar I, Chiron J P (1987): HBsAg positive reactivity in man not due to hepatitis B virus. Lancet ii:1354-1357.
Dienstag JL, Alter H J (1986): Non-A, non-B hepatitis: Evolving epide- miologic and clinical perspective. Seminars in Liver Disease 6:67- 81.
HBV and HCV in Blood Donors
Draelos M, Morgan T, Schifman RB, Sampliner RE (1987): Signifi- cance of isolated antibody to hepatitis B core antigen determined by immune response to hepatitis B vaccination. JAMA 258:1193- 1195.
Ebeling F,Naukkarinen R, Leikola J (1990): Recombinant immuno- blot assay for hepatitis C virus antibody as predictor of infectivity. Lancet 335:982-983.
Figus A, Blum HE, Vyas GN, De Virgullis SO, Cao A, Lippi M, Lai E, Lippi M, Lai E, Balestrieri A (1984): Hepatitis B viralnucleotide sequences in non-A, non-B hepatitis B related chronic liver dis- ease. Hepatology 4:364-368.
Garson JA, Tedder RS, Briggs M, Tuke P, Glazebrook JA, Trute A, Parker D, Barbara JA, Contreras M, Aloysius S (1990): Detection of hepatitis C viral sequences in blood donations by “nested poly- merase chain reaction and prediction of infectivity. Lancet 335: 1419-1422.
Hanson MR, Polesky HF (1987): Evaluation of routine anti-HBc screening of volunteer blood donors: A questionable surrogate test for non-A, non-B hepatitis. Transfusion 27:107-108.
Hoofnagle J H (1989): Delta hepatitis and the hepatitis delta virus. In Seeff LB, Lewis J H (eds): “Current Perspectives in Hepatology .” New York: Plenum Publishing Corp., pp 47-62.
Hoofnagle JH, Seeff LB, Bales ZB, Zimmerman HJ, and the Veterans Administration Hepatitis Cooperative Study Group (1978): Type B hepatitis after transfusion with blood containing antibody to hepa- titis B core antigen. New England Journal of Medicine 25:1379- 1383.
Houghton M, Choo Q-L, Kuo G (1988): European Patent Publication 318,46.
Kaneko S, Miller RH, Feinstone SM, Unoura M, Kobayashi K, Hattori N, Purcell RH (1989): Detection of serum hepatitis B virus DNA using the polymerase chain reaction assay. Proceedings of the Na- tional Academy of Sciences USA 86:312-316.
Katkov WN, Friedman LS, Cody H, Evans AA, Kuo G, Choo Q-L, Hougbton M, Huggins CE, Dienstag J L (1989): Elevated serum alanine aminotransferase in blood donors: The contribution of hep- atitis C virus. Hepatology 10:581.
Kuo G, Choo Q-L, Alter HJ, Gitnik RG, Purcell RH, Miyamura T, Dienstag JL, Alter MJ, Stevens CE, Tegtmeier GE, Bonino F, Colombo M, Lee W-S, Kuo C, Berger K, Shuster JR, Overby LR, Bradley DW, Houghton M (1989): An assay for circulating antibod- ies to a major etiologic virus of human non A, non B hepatitis. Science 244:362-364.
Kwok S, Higuchi R (1989): Avoiding false positives with PCR. Nature 339:237-238.
Lai ME, Farci P, Figus A, Balestrieri A, Arnone M, Vyas GN (1989): Hepatitis B virus DNA in the serum of Sardinian blood donors negative for the hepatitis B surface antigen. Blood 73:17-19.
Liang TJ, Isselbacher KJ, Wands JR (1989): Rapid identification of low level hepatitis B related viral genome in serum. Journal of Clinical Investigation 84: 1367-1371.
Liang TJ, Blum HE, Wands JR (1990a): Characterization and biologi- cal properties of a hepatitis B virus isolated from a patient without HBV serologic markers. Hepatology 12:20&212.
Liang TJ, Blum HE, Hasegawa K, Takahashi H, Galun E, Wands JR (1990b): Detection and transmission of low level hepatitis B re- lated virus in HBsAg-negative individuals. In Hollinger FB, Lemon SM, Margolis HS (eds): “Viral Hepatitis and Liver Dis- ease.” Baltimore: Williams & Wilkins.
Liang TJ, Baruch Y, Ben-Porath E, Enat R, Bassan L, Brown NV, Rimon N, Blum HE, Wands JR (1991a): Hepatitis B virus infection in patients with idiopathic liver disease. Hepatology 13:104P 1051.
Liang TJ, Hasegawa K, Ramon N, Wands JR, Ben-Porath E (1991b): A hepatitis B virus mutant associated with an epidemic of fulminan- thepatitis. New England Journal of Medicine 324:1705-1709.
Liang TJ, Jeffers L, Reddy RK, Silva MO, Cheinquer H, Findor A, De Medina M, Yarbough PO, Reyes GR, Schiff ER (1993): Fulimant or subfulimant non-A, non-B viral hepatitis: The role of hepatitis C and E viruses. Gastroenterology 104:55&562.
Lok ASF, Lai C-L, Wu P-C (1988): Prevalence of isolated antibody to hepatitis B core antigen in an area endemic for hepatitis B virus infection: Implication in hepatitis B vaccination program. Hepatol- ogy 8:766770.
157
McFarlane IG, Smith HM, Johnson PJ, Bray GP, Vergani D, Williams R (1990): Hepatitis C virus antibodies in chronic active hepatitis: Pathogenetic factor or false-positive results. Lancet 335:75&757.
McMahon BJ, Parkinson AJ, Helminiak C, Wainwright RB, Bulkow L, Kellerman-Douglas AJ, Schoenberg S, Ritter D (1992): Re- sponses to hepatitis B vaccine of persons positive for antibody to hepatitis B core antigen. Gastroenterology 103:590-594.
Okamoto H, Okada S, Sagiyama Y, Yotsumoto S, Tanaka T, Yoshi- zana H, Tsuda F, Miyakawa Y, Mayumi M (1990): The 5‘-terminal sequence of hepatitis C virus genome. Japanese Journal of Experi- mental Medicine 60:167-177.
Parkinson AJ, McMahon BJ, Hall D, Ritter D, Fitzgerald MA (1990): Comparison of enzyme immunoassay with radioimmunoassay for the detection of antibody to hepatitis B core antigen as the only marker of hepatitis B infection in a population with a high preva- lence of hepatitis B. Journal of Medical Virology 30:253-257.
Polesky HF, Hanson MR (1989): Transfusion-associated hepatitis C virus infection. Archives of Pathology and Laboratory Medicine 113:232-235.
Prince AM, Stephan W, Brotman B (1983): Beta-propiolactone/ ultraviolet irradiation: A review of its effectiveness for inactiva- tion of its effectiveness for inactivation of viruses in blood deriva- tives. Review of Infections Diseases 5:92-107.
Stevens CE, Aach RD, Hollinger FB, Mosley JW, Szmuness W, Kahn R, Werch J , Edwards V (1984): Hepatitis B virus antibody in blood donors and the occurrence of non-A, non-B hepatitis in transfusion recipients: An analysis of the transfusion-transmitted viruses study. Annals of International Medicine 101:733-738.
Stevens CE, Taylor PE, Pindyck J, Choo A-L, Bradley DW, Kuo G, Houghton M (1990): Epidemiology of hepatitis C virus: A prelimi- nary study in volunteer blood donors. JAMA 263:49-53.
Sugitani M, Inchauspe G, Shindo M, Prince AM (1992): Sensitivity of serological assays to identify blood donors with hepatitis C vi- raemia. Lancet 339:1018-1019.
Takamizana A, Mori C, Fuke I, Manabe S, Murakami S, Fujita J , Onishi F, Andoh T, Yoshida I, Okayama H (1991): Structure and organization of the hepatitis C virus genome isolated from human carriers. Journal of Virology 65:llOl-1113.
Takeuchi K, Kubo Y, Boonmai S, Watanabe Y, Katayama T, Choo Q-L, Kuo G, Houghton M, Saito I, Miyamura T (1990): The puta- tive nucleocapsid and envelope protein genes of hepatitis C virus determined by comparison of the nucleotide sequences of two iso- lates derived from an experimentally infected chimpanzee and healthy human carriers. Journal of General Virology 71:3027- 3033.
Thiers V, Nakajima E, Kremsdorf D, Macke D, Schellekens H, Driss F, Goudeau A, Wards JR, Sninsky J, Tiollais P, Brechot C (1988): Transmission of hepatitis B from hepatitis B seronegative subjects. Lancet 2:1273-1276.
Ulrish PP, Romeo JM, Lane PK, Kelly I, Daniel U, Vyas GN (1990): Detection, semiquantitation, and genetic variation in hepatitis C virus sequences amplified from the plasma of blood donors with elevated alanine aminotransferase. Journal of Clinical Investiga- tion 86:1609-1614.
Van der Poel CL, Reesink HW, LeLie PN, Leentvaar-Kuypers A, Choo G-L, Kuo G, Houghton M (1989): Anti-hepatitis C antibodies and non-A non-B post-transfusion hepatitis in the Netherlands. Lancet 2:297-299.
Van de Poel CL, Reesink HW, Schaasberg W, Leentvaar-Kuypers A, Bakker E, Exel-Oehlers PJ, Lelie PN 11990): Infectivity of blood seropositive for hepatitis C virus antibodies. Lancet 335:558-560.
Wands JR, Fujity YK, Isselbacher KJ, Degott C, Schellekens H, Dazza MC, Thiers V (1986): Identification and transmission of hepatitis B virus-related variant. Proceedings of the National Academy of Sci- ences USA 3:6608-6612.
Weiner A, Kuo G, Bradley D, Bonino F, Saracco G, Lee C, Rosenblatt J , e t al. (1990): Detection of hepatitis C viral sequences in non-A, non-B hepatitis. Lancet 335:l-3.
Zeldis JB, Lee JH , Manish D, Finegold DJ, Sircar R, Ling Q, Knudsen PJ, Kuramoto ZK, Mimms LT (1989): Direct method for detecting small quantities of hepatitis B virus DNA in serum and plasma using the polymerase chain reaction. Journal of Clinical Investiga- tion 84:1503-1508.







![Recombinase Polymerase Amplification-Based Assay to ... · Giardia assay (recombinase polymerase amplification-based Giardia [RPAG] assay) that is capable of detecting the pres ence](https://img.pdfslide.net/doc/110x75/60328fc63d35af025c01a9a2/recombinase-polymerase-amplification-based-assay-to-giardia-assay-recombinase.jpg)





















