Embed Size (px)
Citation preview
Label indications (87/140): primary immunodeficiencies (68/87), idiopatic thrombocytopenic purpura(7/87), Guillain-Barré syndrome (5/87), secondary immunodeficiency (5/87), Kawasaki disease (2/87).
Off-label indications supported by clinical evidence (28/140): myasthenia gravis (9/28), chronicinflammatory demyelinating polyradiculoneuropathy (5/28), inflammatory myopathies (5/28), multifocalmotor neuropathy (2/28), stiff person syndrome (2/28), renal transplant rejection mediated byantibodies (2/29), Lambert-Eaton syndrome (1/28), autoimmune hemolytic anemia (1/28),staphylococcal toxic shock (1/28).
Off-label indications not sufficiently supported by clinical evidence (17/140): systemic lupuserythematosus (6/17), systemic vasculitis (6/17), paraneoplastic syndrome (3/17), acute disseminatedencephalomyelitis (1/17), refractory childhood epilepsy (1/17).Indication wasn´t properly established in 6% (8/140) of the cases.
Objective
Material and methods
Results
Disclosing the use of intravenous immunoglobulin (IVIg) in a tertiary hospital: adequacy to label indications and economic impact.
• Retrospective study (January-2015 to December-2015).• Collected data, from medical records: sex, age, IVIg indication, posology, cumulative dose and treatment
cost per patient.• Descriptive analysis of IVIg use per patient and indication and associated cost.
Off-label IVIg indications are frequent in our hospital (32%), with an important economic impact (52%),higher than label indications. It would be useful implementing an updated IVIg protocol, listing indicationssupported by scientific evidence to facilitate application of IVIg treatment in off-label indications.
Conclusion
age 62.6[3.1 to 91.8] years old 59.3% 40.7%140 patients received IVIg
No conflict of interest ATC: l-04 Immune sera and immunoglobulins
PosologyReplacement therapy: 100 – 400 mg/kg every 3–5 weeks
56% hospitalizedImmunomodulatory: 1-2 g/kg single dose – monthly adm.
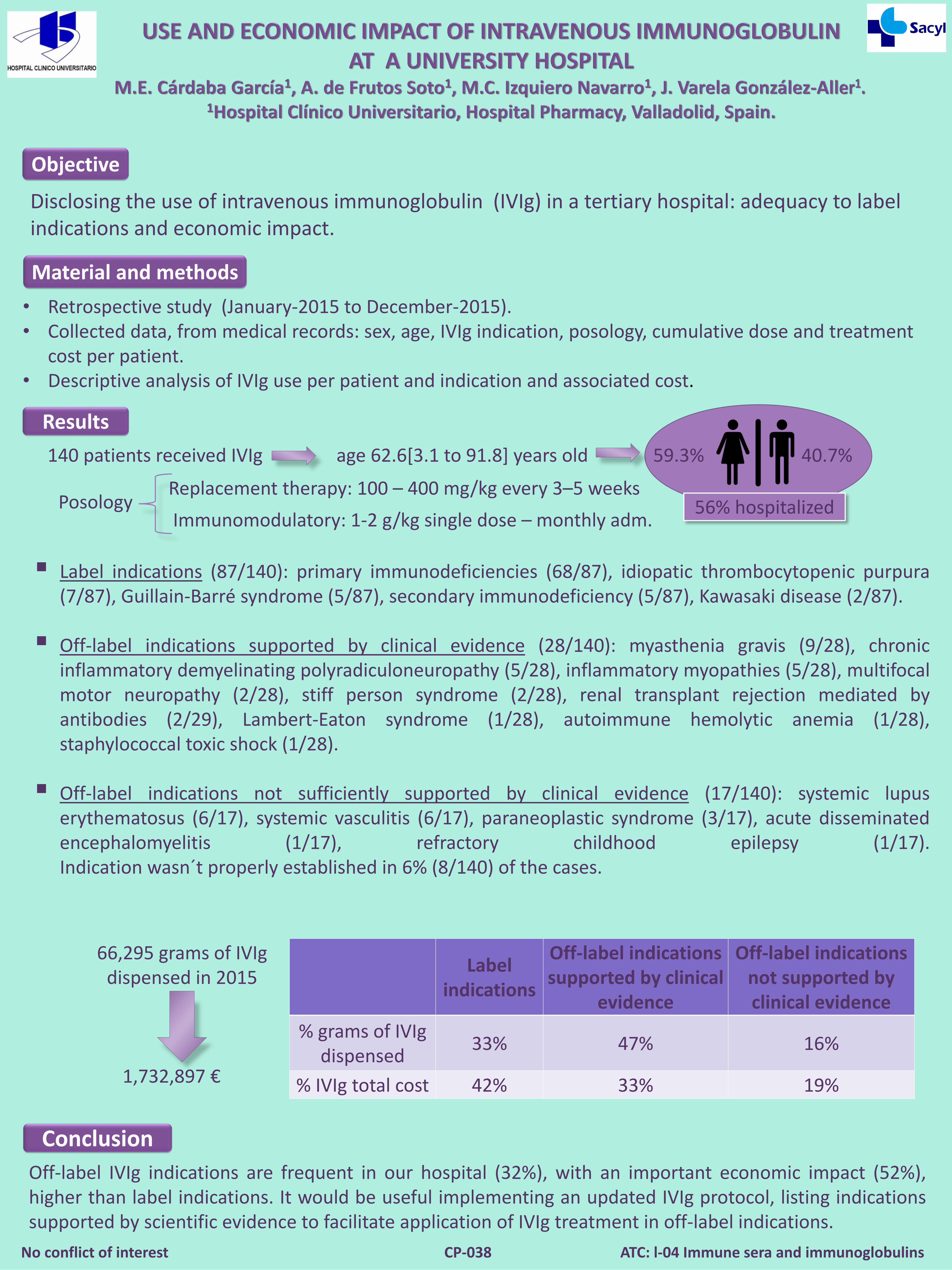
66,295 grams of IVIgdispensed in 2015
1,732,897 €
Labelindications
Off-label indications supported by clinical
evidence
Off-label indications not supported by clinical evidence
% grams of IVIgdispensed
33% 47% 16%
% IVIg total cost 42% 33% 19%
CP-038