Embed Size (px)
Citation preview

Presenter Disclosure Information
Diane Bild, MD, MPHScreening for Subclinical Atherosclerosis as a Strategy for CVD Prevention
FINANCIAL DISCLOSURE:None
UNLABELED/UNAPPROVED USES DISCLOSURE:None

Screening for Subclinical Atherosclerosis as a Strategy for CVD Prevention
AHA Quality and OutcomesMay 21, 2010
Diane Bild, MD, MPHAssociate Director, Prevention and Population Sciences Program
Division of Cardiovascular Sciences
The views expressed are not necessarily those of NHLBI.

Prevent morbidity and mortality due to CVD◦Identify disease before it becomes symptomatic.
◦Prevent disease progression.
The Goals of Subclinical CVD Screening
Footnote: “Screening” is a standardized population or case-finding approach, not an individualized strategy.

It may be costly. It may cause undue psychological
stress. Coronary artery calcium detection
requires CT scanning and radiation, which may induce cancer.
CT scans may uncover other subclinical disease (such as pulmonary nodules) that requires further work-up.
Possible Harms of Subclinical CVD Screening

Hundreds of risk factors Countless analyses from observational studies
Recent progress in modeling risk prediction, particularly with clinical relevance◦ Discrimination◦ Calibration ◦ Reclassification
Prediction

Theoretical pathway from screening to prevention
http://lifebeat.pt/en2.php
Identify high risk
Further diagnosis
Treatment Rx? statins? aspirin? antihypertensives
Long-term adherence
Risk lowered

Atherosclerosis Test
Very Low Risk3
Negative Test• CACS =0• CIMT <50th percentile
LowerRisk
ModerateRisk
Positive Test• CACS ≥1• CIMT 50th percentile or Carotid Plaque
ModeratelyHigh Risk
HighRisk
VeryHigh Risk
No Risk Factors5 + Risk Factors • CACS <100 & <75th%• CIMT <1mm & <75th%
& no Carotid Plaque
• Coronary Artery Calcium Score (CACS)or
• Carotid IMT (CIMT) & Carotid Plaque4
• CACS 100-399 or >75th%• CIMT 1mm or >75th%
or <50% Stenotic Plaque
• CACS >100 & >90th%or CACS 400
• 50% Stenotic Plaque6
IndividualizedIndividualizedIndividualized5-10 years5-10 yearsRe-test Interval
<70 mg/dl<100 mg/dl<70 Optional
<130 mg/dl<100 Optional
<130 mg/dl<160 mg/dlLDL Target
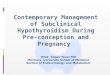
All >75y receive unconditional treatment2
Apparently Healthy Population Men>45y Women>55y1
ExitExit
MyocardialIschemiaTest
NoAngiography
Follow Existing Guidelines
Yes
The 1st S .H .A .P .E . GuidelineTowards the National Screening for Heart Attack Prevention and Education (SHAPE) Program
Step 1
Step 2
Step 3Optional
CRP>4mg
ABI<0.9
1: No history of angina, heart attack, stroke, or peripheral arterial disease.2: Population over age 75y is considered high risk and must receive therapy without testing for atherosclerosis.3: Must not have any of the following: Chol>200 mg/dl, blood pressure >120/80 mmHg, diabetes, smoking, family history, metabolic syndrome.4: Pending the development of standard practice guidelines.5: High cholesterol, high blood pressure, diabetes, smoking, family history, metabolic syndrome.6: For stroke prevention, follow existing guidelines.

How do we decide when screening is valuable?
Wilson JM. J R Coll Gen Pract 1968;16 Suppl 2:48 –57.

How do we decide when screening is valuable?
Wilson JM. J R Coll Gen Pract 1968;16 Suppl 2:48 –57.

Criteria for Evaluation of Novel Markers of Cardiovascular Risk
Hlatky, et al. Circulation 2009; 119:2408-2416.
??
CAC?

U.S. Preventive Services Task ForceGrade
DefinitionSuggestions for Practice
A The USPSTF recommends the service. There is high certainty that the net benefit is substantial.
Offer or provide this service.
B The USPSTF recommends the service. There is high certainty that the net benefit is moderate or there is moderate certainty that the net benefit is moderate to substantial.
Offer or provide this service.
C The USPSTF recommends against routinely providing the service. There may be considerations that support providing the service in an individual patient. There is at least moderate certainty that the net benefit is small.
Offer or provide this service only if other considerations support the offering or providing the service in an individual patient.

U.S. Preventive Services Task ForceGrade
DefinitionSuggestions for Practice
D The USPSTF recommends against the service. There is moderate or high certainty that the service has no net benefit or that the harms outweigh the benefits.
Discourage the use of this service
I State
ment
The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of the service. Evidence is lacking, of poor quality, or conflicting, and the balance of benefits and harms cannot be determined.
Read the clinical considerations section of USPSTF Recommendation Statement. If the service is offered, patients should understand the uncertainty about the balance of benefits and harms.

Condition Explanation Grade
Abdominal aortic aneurysm (2005)
One-time screening for AAA by ultrasonography in men aged 65 to 75 who have ever smoked.
B
No recommendation for or against screening for AAA in men aged 65 to 75 who have never smoked.
C
The USPSTF recommends against routine screening for AAA in women.
D
CV screening recommendations per USPSTF

Condition Explanation Grade
Carotid artery stenosis (2007)
Recommends against screening for asymptomatic carotid artery stenosis in the general adult population.
D
Peripheral artery disease (2005)
The USPSTF recommends against routine screening for peripheral arterial disease.
D
CV screening recommendations per USPSTF, continued

Condition Explanation Grade
Coronary heart disease (2004)
Recommends against routine screening with resting electrocardiography (ECG), exercise treadmill test (ETT), or electron-beam computerized tomography (EBCT) scanning for coronary calcium for either the presence of severe coronary artery stenosis (CAS) or the prediction of coronary heart disease (CHD) events in adults at low risk for CHD events.
D
Insufficient evidence to recommend for or against routine screening with ECG, ETT, or EBCT scanning for coronary calcium for either the presence of severe CAS or the prediction of CHD events in adults at increased risk for CHD events.
I
CV screening recommendations per USPSTF, continued

Condition Explanation Grade
Risk assessment, nontraditional risk factors (2009)
Evidence is insufficient to assess the balance of benefits and harms of using the nontraditional risk factors discussed in this statement to screen asymptomatic men and women with no history of CHD to prevent CHD events
I
CV screening recommendations per USPSTF, continued
The nontraditional risk factors included in this recommendation are high-sensitivity C-reactive protein (hs-CRP), ankle-brachial index (ABI), leukocyte count, fasting blood glucose level, periodontal disease, carotid intima-media thickness (carotid IMT), coronary artery calcification (CAC) score on electron-beam computed tomography (EBCT), homocysteine level, and lipoprotein(a) level.

Condition Explanation Grade
Lipid disorders in adults (2008) - Men
The U.S. Preventive Services Task Force (USPSTF) strongly recommends screening men aged 35 and older for lipid disorders.
The USPSTF recommends screening men aged 20 to 35 for lipid disorders if they are at increased risk for coronary heart disease.
A
B
Lipid disorders in adults (2008) – Women at increased risk
The USPSTF strongly recommends screening women aged 45 and older for lipid disorders if they are at increased risk for coronary heart disease.
The USPSTF recommends screening women aged 20 to 45 for lipid disorders if they are at increased risk for coronary heart disease.
A
B
CV screening recommendations per USPSTF, continued

Condition Explanation Grade
Lipid disorders in Adults --Young Men and All Women Not at Increased Risk
The USPSTF makes no recommendation for or against routine screening for lipid disorders in men aged 20 to 35, or in women aged 20 and older who are not at increased risk for coronary heart disease.
C
Blood pressure
The U.S. Preventive Services Task Force (USPSTF) recommends screening for high blood pressure in adults aged 18 and older.
A
CV screening recommendations per USPSTF, continued

Level of evidence A: recommendation based on evidence from multiple randomized trials or meta-analyses
Level of evidence B: recommendation based on evidence from a single randomized trial or nonrandomized studies
Level of evidence C: recommendation based on expert opinion, case studies, or standards of care
The ACC/AHA guidelines grading scheme – Results for CAC
Tricoci, et al. JAMA 2009;301:831-841.

CAC improves CHD risk prediction, calibration, and classification
Polonsky, et al. JAMA 2010;303:1610-16.

Efficacy of cholesterol-lowering treatment:prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins
Source: Cholesterol Treatment Trials Collaborators. Lancet 2005:366:1267–78
“Treatment better”~25% risk reduction

Randomized, placebo-controlled trial of cholestyramine
Lipid Research Clinics Program. JAMA 1984;251:351-64.

Published in 1967 N=143
Randomized placebo-controlled trial of diuretics in severe hypertension
VA Cooperative Study Group on Antihypertensive Agents. JAMA 1967;202:116-21.

We have come only so far . . .

Call for trials of imaging
Douglas, et al. Outcomes Research in Cardiovascular Imaging: Report of a Workshop Sponsored by the National Heart, Lung, and Blood Institute. JACC Cardiovasc Imaging 2009;2:897-907.

Guidelines may need to be changed due to:◦Emergence of new evidence◦Changes in disease prevalence◦Consideration of new risk groups◦Development of new therapies◦Changes in the cost of treatment
Re-evaluating Screening Guidelines

Goals are laudable; some candidate screening markers have promising characteristics.
Harms of screening need to be carefully considered, especially for coronary artery calcium detection.
Few screening targets in cardiovascular disease prevention are deemed beneficial -- most notably, BP and lipids.
Much work has been performed in estimating prediction; little in estimating outcomes.
Any screening guidelines need periodic re-evaluation.
Summary – Subclinical CVD Screening