Embed Size (px)
Citation preview
Vol. 47 No. 1 January 2014 Journal of Pain and Symptom Management 57
Review Article
Prevalence of Breakthrough Cancer Pain:A Systematic Review and a Pooled Analysisof Published LiteratureSilvia Deandrea, MD, PhD, Oscar Corli, MD, Dario Consonni, MD, PhD,Walter Villani, BSc, Maria Teresa Greco, MD, and Giovanni Apolone, MDCenter for the Evaluation and Research on Pain (CERP) (S.D., O.C., W.V.), IRCCS Istituto di
Ricerche Farmacologiche ‘‘Mario Negri,’’ Milan; Istituto di Statistica Medica e Biometria ‘‘G. A.
Maccacaro,’’ (S.D., M.T.G.), Universit�a degli Studi di Milano, Milan; Unit of Epidemiology (D.C.),
Fondazione IRCCS Ca’ GrandadOspedale Maggiore Policlinico, Milan; and Direzione Scientifica
(G.A.), IRCCS Arcispedale Santa Maria Nuova, Reggio-Emilia, Italy
Abstract
Context. Despite the large body of literature on breakthrough cancer pain(BTcP), an accurate estimate of BTcP prevalence is still not available.Objectives. To provide an estimate of BTcP prevalence and investigate
the association between different prevalence rates and possible determinants.Methods. We conducted MEDLINE and EMBASE searches for studies
published from 1990 to 2012 reporting data on BTcP prevalence in adult cancerpopulations. Pooled prevalence rates from observational studies with anacceptable methodological quality were computed. The association between BTcPprevalence and possible predictors was investigated using subgroup analyses andmeta-regression.
Results. Twenty-seven observational studies were identified. When qualitycriteria were applied, only 19 studies were included in the pooled analysis. Theoverall pooled prevalence was 59.2%, with high heterogeneity. The lowestprevalence rates were detected in studies conducted in outpatient clinics (39.9%),and the highest prevalence was reported in studies conducted in hospice (80.5%).The association between BTcP prevalence and other determinants such aspublication year, age, gender, metastatic disease prevalence, or baseline painintensity did not reach statistical significance.
Conclusion. In the context of a large between-studies heterogeneity, more thanone in two patients with cancer pain also experiences BTcP, with some variabilityaccording to clinical and organizational variables. J Pain Symptom Manage2014;47:57e76. � 2014 U.S. Cancer Pain Relief Committee. Published by Elsevier Inc. Allrights reserved.
Address correspondence to: Silvia Deandrea, MD, PhD,Center for the Evaluation and Research on Pain(CERP), IRCCS Istituto di Ricerche Farmacologiche
‘‘Mario Negri,’’ Via La Masa 19, 20156 Milan, Italy.E-mail: [email protected]
Accepted for publication: February 22, 2013.
� 2014 U.S. Cancer Pain Relief Committee.Published by Elsevier Inc. All rights reserved.
0885-3924/$ - see front matterhttp://dx.doi.org/10.1016/j.jpainsymman.2013.02.015

58 Vol. 47 No. 1 January 2014Deandrea et al.
Key Words
Breakthrough cancer pain, prevalence, systematic review, pooled analysisIntroductionBreakthrough cancer pain (BTcP) has been
defined by the Association for Palliative Medi-cine of Great Britain and Ireland (APM) taskgroup1 as ‘‘a transient exacerbation of painthat occurs either spontaneously, or in relationto a specific predictable or unpredictable trig-ger, despite relatively stable and adequatelycontrolled background pain’’ a definitionshared by the European Association for Pallia-tive Care recommendations on opioids in can-cer pain.2
Despite the large body of literature on BTcPand the recent development of new pharmaco-logic strategies,3e8 its actual prevalence is notwell known, with reported estimates varyinglargely across studies and settings.9,10 Theremay be several reasons for such variability, in-cluding different conceptual and operationaldefinitions across studies and countries, differ-ent study designs, and different settings. Qual-itative and quantitative reviews9e13 havehighlighted the need to increase the quantityand quality of evidence on BTcP. A recent sys-tematic review evaluating the definition andclassification of BTcP concluded that there isneither a widely accepted classification systemnor a definitive and well-validated tool for as-sessment.14 We carried out a systematic reviewof published literature and a statistical poolingof the study results in an attempt to obtainmore accurate figures on BTcP prevalenceand identify reasons for such variability.
MethodsStudy Selection and BTcP Definition
We started our analysis with two reviews re-porting articles published before 2004: oneconducted by the Cochrane Collaboration12
and one by Svendsen et al.15 We then per-formed MEDLINE and EMBASE searches toupdate the list of articles from January 2004to December 2012, scanned the references ofarticles identified in the previous steps, includ-ing more recently published reviews,16e19 andconsulted experts in the field. The literature
search strategy used the following terms:(breakthrough or episodic or transient or tran-sitory or incident or flare) AND (cancer or ma-lignant or neoplasm or neoplasia or tumor ortumour) AND pain. Only articles written inEnglish involving humans and adults were con-sidered. Two investigators (W.V. and S.D.) in-dependently reviewed titles and abstracts,selecting articles addressing pain in adult can-cer patients. Disagreements were resolved bydiscussion and consensus.Finally, we selected the final sample from
the studies retrieved according to the follow-ing inclusion criteria: 1) original studies and2) reporting data about prevalence of break-through pain in adult cancer populations.Both observational and experimental studieswere included. At this step, we included allstudies on transitory pain exacerbation orpain flare, irrespective of the type of definitionused by any single author.
Study CharacteristicsOn a data extraction sheet developed with
a pilot-tested procedure, we recorded the fol-lowing relevant details of study design: aim ofthe study (BTcP prevalence or other), samplesize, participants’ characteristics (age, sex,type of cancer, and presence of metastasis), set-ting, background cancer pain characteristics(prevalence, intensity, and treatments), BTcPcharacteristics (definition, prevalence, num-ber of episodes/day, duration of episodes,and intensity), and method of BTcP data col-lection (patient or proxy questionnaire, pa-tient or proxy interview, medical record, anduse of validated or nonvalidated instruments).Disagreements were resolved by discussion andconsensus. When data were not available fromthe full-text article, the authors of the originalarticles were contacted to provide the missinginformation. The prevalence of BTcP couldbe reported either as a proportion of the totalnumber of cancer patients included in thesample, even if not experiencing cancer painat all or for whom the presence of cancerpain was not clearly reported, or as a propor-tion of patients with baseline pain greater

Vol. 47 No. 1 January 2014 59Prevalence of BTcP
than zero. Thus, our operational definition ofBTcP prevalence was ‘‘the number of patientswith background cancer pain also experienc-ing BTcP, according to the articles’ definition.’’Articles were grouped according to the type ofBTcP definition (Table 1).
Quality AssessmentObservational studies were evaluated using
the methodological criteria for prevalencestudies developed by Leboeuf-Yde and Laurit-sen20 and Walker,21 later adapted to cancerpain by van den Beuken-van Everdingenet al.22 In this analysis, the cancer pain ques-tions were substituted with BTcP questions(Table 2). This process resulted in a qualityscore that ranged from 0 to 19 points for stud-ies in which all the criteria were applicable andfrom 0 to 15 when some criteria were not ap-plicable. The cutoff level for methodologicalacceptability was set at 75% of the total pointsthat could be achieved, corresponding to 14points in the first case and 11 points in the sec-ond case. The quality score was used to selecta subgroup of articles suitable for subgroupanalysis after the pooling of data. One article23
was excluded from the quality assessment be-cause it did not report the prevalence ofBTcP in cancer patients with backgroundpain, according to the prevalence rate defini-tion. Quality scores for each article are avail-able as Appendix.
Pooling of DataFor longitudinal studies including more
than one BTcP prevalence rate accordingto the follow-up duration, only the earliestestimate was considered. Central tendencymeasures (mean and median) and a raw prev-alence, computed dividing the sum of subjectswith BTcP by the total number of subjects en-rolled in the studies, were computed for threesubsets: all the studies initially included, obser-vational studies only, and observational studieswith acceptable quality. We estimated thepooled BTcP prevalence and its 95% CI usinga random-effects model.24 Only the lattergroup was considered eligible for subgroupanalysis: publication year, context of care (on-cology, palliative, and mixed), setting (inpa-tients, outpatients, hospice, and home care),mean age of the sample (>median and # me-dian), male prevalence in the sample
(>median and # median), presence of metas-tases (>median and # median), BTcP de-finition using the classification previouslydescribed, background worst pain (mild, mod-erate, and severe), and average pain (mild,moderate, and severe). Mild pain was definedby numerical rating scale (NRS) Scores 1e4,moderate pain by NRS Scores 5e6, and severepain by NRS Scores 7e10.25 To investigatewhether the variation in prevalence rates be-tween studies was more than could be attrib-uted to chance alone, the I-square test26 andc2 test for homogeneity were calculated.
To further explore whether study-levelcharacteristics could explain between-studyheterogeneity, we performed a univariate meta-regression analysis. Themeta-regression analysiswas performed for continuous variables and forsetting categorized according to an ascendingorder: outpatients, mixed, inpatients, homecare, and hospice. All the analyses were per-formed using Stata 11 (2009, StataCorp LP,College Station, TX).
ResultsSixty-one studies were identified from the
previously published reviews and 70 morethrough consultation with experts in the field.The searches of MEDLINE and EMBASE pro-duced 781 citations. After removing dupli-cates, 752 citations remained. Of these, 557citations were discarded because after review-ing the abstracts, they did not meet the inclu-sion criteria. The full text of each of theremaining 195 citations was examined inmore detail. Two publications11,27 reporteddata from the same sample, and we selectedthe more recent article27 because it focusedon BTcP data. Thirty-three studies11,23,27e58
met all the inclusion criteria, and the selectedcharacteristics are reported in Tables 3 and 4.The flowchart of study selection is shown inFig. 1. Publication dates ranged from 1988 to2012 (median year, 2005); 10studies33,34,37,38,41,43,44,51e53 were from NorthAmerica, 19 studies23,29,32,35,36,39,40,42,45e50,54e58
from Europe, one study from Australia,28 andone study from India.30 Two were multicenterand multinational studies.27,31 Twenty-seven23,27e33,35e40,42,43,47e53,55e58 were obser-vational studies and six34,41,44e46,54 were
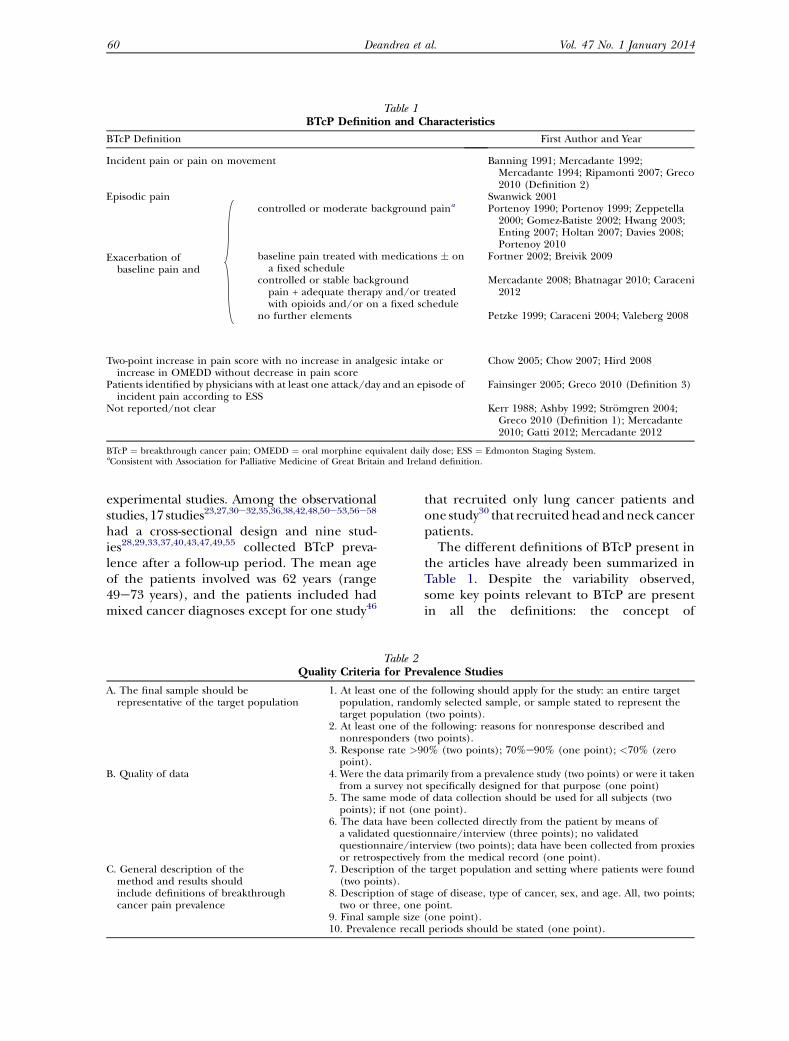
Table 1BTcP Definition and Characteristics
BTcP Definition First Author and Year
Incident pain or pain on movement Banning 1991; Mercadante 1992;Mercadante 1994; Ripamonti 2007; Greco2010 (Definition 2)
Episodic pain Swanwick 2001
Exacerbation ofbaseline pain and
controlled or moderate background paina Portenoy 1990; Portenoy 1999; Zeppetella2000; Gomez-Batiste 2002; Hwang 2003;Enting 2007; Holtan 2007; Davies 2008;Portenoy 2010
baseline pain treated with medications � ona fixed schedule
Fortner 2002; Breivik 2009
controlled or stable backgroundpain + adequate therapy and/or treatedwith opioids and/or on a fixed schedule
Mercadante 2008; Bhatnagar 2010; Caraceni2012
no further elements Petzke 1999; Caraceni 2004; Valeberg 2008
Two-point increase in pain score with no increase in analgesic intake orincrease in OMEDD without decrease in pain score
Chow 2005; Chow 2007; Hird 2008
Patients identified by physicians with at least one attack/day and an episode ofincident pain according to ESS
Fainsinger 2005; Greco 2010 (Definition 3)
Not reported/not clear Kerr 1988; Ashby 1992; Str€omgren 2004;Greco 2010 (Definition 1); Mercadante2010; Gatti 2012; Mercadante 2012
BTcP ¼ breakthrough cancer pain; OMEDD ¼ oral morphine equivalent daily dose; ESS ¼ Edmonton Staging System.aConsistent with Association for Palliative Medicine of Great Britain and Ireland definition.
60 Vol. 47 No. 1 January 2014Deandrea et al.
experimental studies. Among the observationalstudies, 17 studies23,27,30e32,35,36,38,42,48,50e53,56e58
had a cross-sectional design and nine stud-ies28,29,33,37,40,43,47,49,55 collected BTcP preva-lence after a follow-up period. The mean ageof the patients involved was 62 years (range49e73 years), and the patients included hadmixed cancer diagnoses except for one study46
Table 2Quality Criteria for Pre
A. The final sample should berepresentative of the target population
1. At least one of thpopulation, randotarget population
2. At least one of thnonresponders (t
3. Response rate >9point).
B. Quality of data 4. Were the data primfrom a survey not
5. The same mode opoints); if not (on
6. The data have bea validated questiquestionnaire/intor retrospectively
C. General description of themethod and results shouldinclude definitions of breakthroughcancer pain prevalence
7. Description of th(two points).
8. Description of statwo or three, one
9. Final sample size10. Prevalence recal
that recruited only lung cancer patients andone study30 that recruitedhead andneck cancerpatients.The different definitions of BTcP present in
the articles have already been summarized inTable 1. Despite the variability observed,some key points relevant to BTcP are presentin all the definitions: the concept of
valence Studies
e following should apply for the study: an entire targetmly selected sample, or sample stated to represent the(two points).e following: reasons for nonresponse described andwo points).0% (two points); 70%e90% (one point); <70% (zero
arily from a prevalence study (two points) or were it takenspecifically designed for that purpose (one point)f data collection should be used for all subjects (twoe point).en collected directly from the patient by means ofonnaire/interview (three points); no validatederview (two points); data have been collected from proxiesfrom the medical record (one point).e target population and setting where patients were found
ge of disease, type of cancer, sex, and age. All, two points;point.(one point).l periods should be stated (one point).
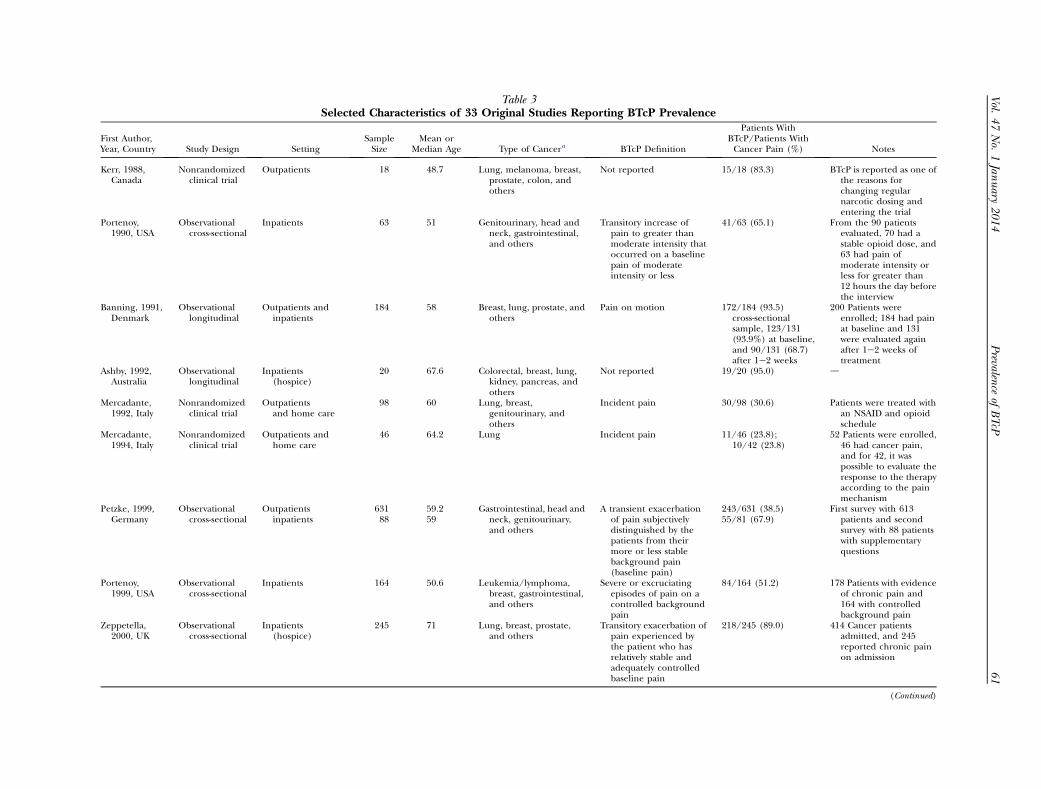
Table 3Selected Characteristics of 33 Original Studies Reporting BTcP Prevalence
First Author,Year, Country Study Design Setting
SampleSize
Mean orMedian Age Type of Cancera BTcP Definition
Patients WithBTcP/Patients WithCancer Pain (%) Notes
Kerr, 1988,Canada
Nonrandomizedclinical trial
Outpatients 18 48.7 Lung, melanoma, breast,prostate, colon, andothers
Not reported 15/18 (83.3) BTcP is reported as one ofthe reasons forchanging regularnarcotic dosing andentering the trial
Portenoy,1990, USA
Observationalcross-sectional
Inpatients 63 51 Genitourinary, head andneck, gastrointestinal,and others
Transitory increase ofpain to greater thanmoderate intensity thatoccurred on a baselinepain of moderateintensity or less
41/63 (65.1) From the 90 patientsevaluated, 70 had astable opioid dose, and63 had pain ofmoderate intensity orless for greater than12 hours the day beforethe interview
Banning, 1991,Denmark
Observationallongitudinal
Outpatients andinpatients
184 58 Breast, lung, prostate, andothers
Pain on motion 172/184 (93.5)cross-sectionalsample, 123/131(93.9%) at baseline,and 90/131 (68.7)after 1e2 weeks
200 Patients wereenrolled; 184 had painat baseline and 131were evaluated againafter 1e2 weeks oftreatment
Ashby, 1992,Australia
Observationallongitudinal
Inpatients(hospice)
20 67.6 Colorectal, breast, lung,kidney, pancreas, andothers
Not reported 19/20 (95.0) d
Mercadante,1992, Italy
Nonrandomizedclinical trial
Outpatientsand home care
98 60 Lung, breast,genitourinary, andothers
Incident pain 30/98 (30.6) Patients were treated withan NSAID and opioidschedule
Mercadante,1994, Italy
Nonrandomizedclinical trial
Outpatients andhome care
46 64.2 Lung Incident pain 11/46 (23.8);10/42 (23.8)
52 Patients were enrolled,46 had cancer pain,and for 42, it waspossible to evaluate theresponse to the therapyaccording to the painmechanism
Petzke, 1999,Germany
Observationalcross-sectional
Outpatientsinpatients
631 59.2 Gastrointestinal, head andneck, genitourinary,and others
A transient exacerbationof pain subjectivelydistinguished by thepatients from theirmore or less stablebackground pain(baseline pain)
243/631 (38.5)55/81 (67.9)
First survey with 613patients and secondsurvey with 88 patientswith supplementaryquestions
88 59
Portenoy,1999, USA
Observationalcross-sectional
Inpatients 164 50.6 Leukemia/lymphoma,breast, gastrointestinal,and others
Severe or excruciatingepisodes of pain on acontrolled backgroundpain
84/164 (51.2) 178 Patients with evidenceof chronic pain and164 with controlledbackground pain
Zeppetella,2000, UK
Observationalcross-sectional
Inpatients(hospice)
245 71 Lung, breast, prostate,and others
Transitory exacerbation ofpain experienced bythe patient who hasrelatively stable andadequately controlledbaseline pain
218/245 (89.0) 414 Cancer patientsadmitted, and 245reported chronic painon admission
(Continued)
Vol.
47No.
1Jan
uary
2014
61
Prevalen
ceof
BTcP
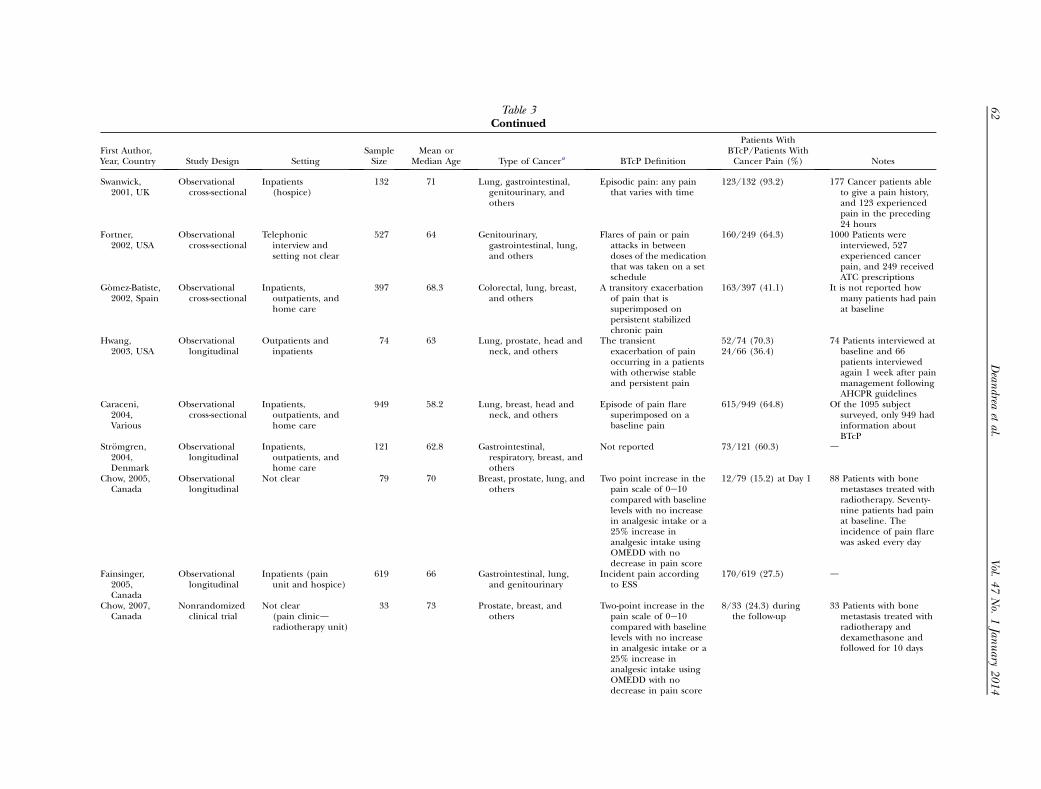
Table 3Continued
First Author,Year, Country Study Design Setting
SampleSize
Mean orMedian Age Type of Cancera BTcP Definition
Patients WithBTcP/Patients WithCancer Pain (%) Notes
Swanwick,2001, UK
Observationalcross-sectional
Inpatients(hospice)
132 71 Lung, gastrointestinal,genitourinary, andothers
Episodic pain: any painthat varies with time
123/132 (93.2) 177 Cancer patients ableto give a pain history,and 123 experiencedpain in the preceding24 hours
Fortner,2002, USA
Observationalcross-sectional
Telephonicinterview andsetting not clear
527 64 Genitourinary,gastrointestinal, lung,and others
Flares of pain or painattacks in betweendoses of the medicationthat was taken on a setschedule
160/249 (64.3) 1000 Patients wereinterviewed, 527experienced cancerpain, and 249 receivedATC prescriptions
G�omez-Batiste,2002, Spain
Observationalcross-sectional
Inpatients,outpatients, andhome care
397 68.3 Colorectal, lung, breast,and others
A transitory exacerbationof pain that issuperimposed onpersistent stabilizedchronic pain
163/397 (41.1) It is not reported howmany patients had painat baseline
Hwang,2003, USA
Observationallongitudinal
Outpatients andinpatients
74 63 Lung, prostate, head andneck, and others
The transientexacerbation of painoccurring in a patientswith otherwise stableand persistent pain
52/74 (70.3)24/66 (36.4)
74 Patients interviewed atbaseline and 66patients interviewedagain 1 week after painmanagement followingAHCPR guidelines
Caraceni,2004,Various
Observationalcross-sectional
Inpatients,outpatients, andhome care
949 58.2 Lung, breast, head andneck, and others
Episode of pain flaresuperimposed on abaseline pain
615/949 (64.8) Of the 1095 subjectsurveyed, only 949 hadinformation aboutBTcP
Str€omgren,2004,Denmark
Observationallongitudinal
Inpatients,outpatients, andhome care
121 62.8 Gastrointestinal,respiratory, breast, andothers
Not reported 73/121 (60.3) d
Chow, 2005,Canada
Observationallongitudinal
Not clear 79 70 Breast, prostate, lung, andothers
Two point increase in thepain scale of 0e10compared with baselinelevels with no increasein analgesic intake or a25% increase inanalgesic intake usingOMEDD with nodecrease in pain score
12/79 (15.2) at Day 1 88 Patients with bonemetastases treated withradiotherapy. Seventy-nine patients had painat baseline. Theincidence of pain flarewas asked every day
Fainsinger,2005,Canada
Observationallongitudinal
Inpatients (painunit and hospice)
619 66 Gastrointestinal, lung,and genitourinary
Incident pain accordingto ESS
170/619 (27.5) d
Chow, 2007,Canada
Nonrandomizedclinical trial
Not clear(pain clinicdradiotherapy unit)
33 73 Prostate, breast, andothers
Two-point increase in thepain scale of 0e10compared with baselinelevels with no increasein analgesic intake or a25% increase inanalgesic intake usingOMEDD with nodecrease in pain score
8/33 (24.3) duringthe follow-up
33 Patients with bonemetastasis treated withradiotherapy anddexamethasone andfollowed for 10 days
62
Vol.
47No.
1Jan
uary
2014
Dean
dreaetal.
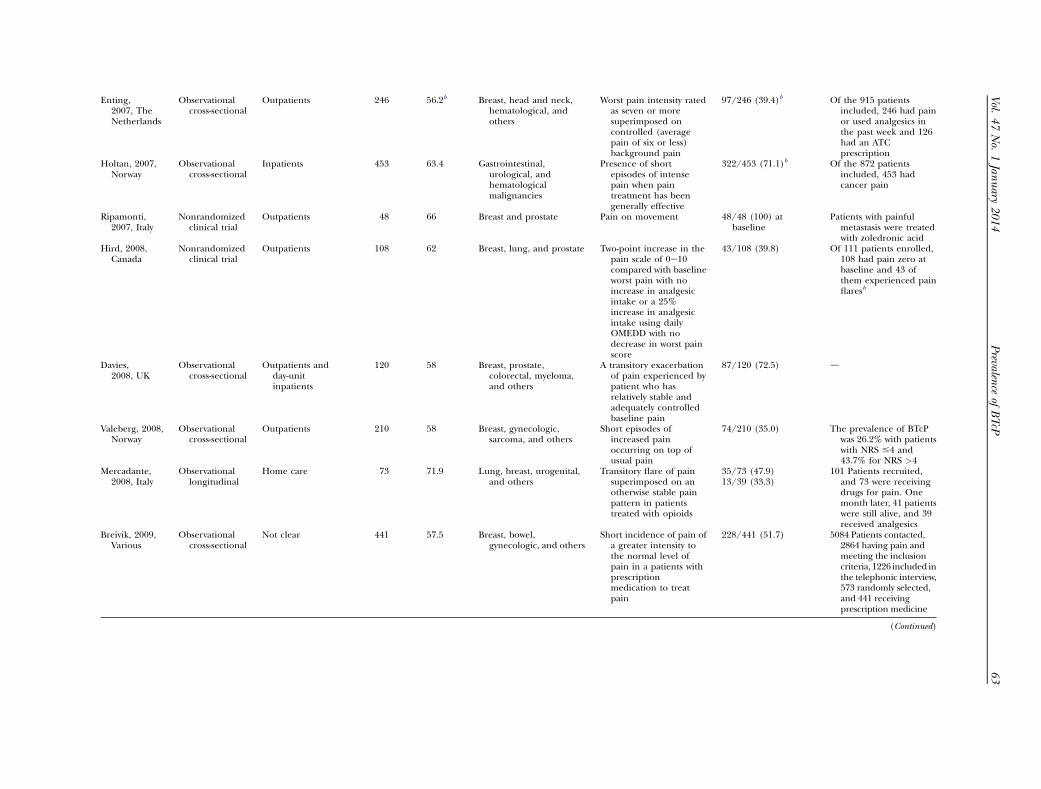
Enting,2007, TheNetherlands
Observationalcross-sectional
Outpatients 246 56.2b Breast, head and neck,hematological, andothers
Worst pain intensity ratedas seven or moresuperimposed oncontrolled (averagepain of six or less)background pain
97/246 (39.4)b Of the 915 patientsincluded, 246 had painor used analgesics inthe past week and 126had an ATCprescription
Holtan, 2007,Norway
Observationalcross-sectional
Inpatients 453 63.4 Gastrointestinal,urological, andhematologicalmalignancies
Presence of shortepisodes of intensepain when paintreatment has beengenerally effective
322/453 (71.1)b Of the 872 patientsincluded, 453 hadcancer pain
Ripamonti,2007, Italy
Nonrandomizedclinical trial
Outpatients 48 66 Breast and prostate Pain on movement 48/48 (100) atbaseline
Patients with painfulmetastasis were treatedwith zoledronic acid
Hird, 2008,Canada
Nonrandomizedclinical trial
Outpatients 108 62 Breast, lung, and prostate Two-point increase in thepain scale of 0e10compared with baselineworst pain with noincrease in analgesicintake or a 25%increase in analgesicintake using dailyOMEDD with nodecrease in worst painscore
43/108 (39.8) Of 111 patients enrolled,108 had pain zero atbaseline and 43 ofthem experienced painflaresb
Davies,2008, UK
Observationalcross-sectional
Outpatients andday-unitinpatients
120 58 Breast, prostate,colorectal, myeloma,and others
A transitory exacerbationof pain experienced bypatient who hasrelatively stable andadequately controlledbaseline pain
87/120 (72.5) d
Valeberg, 2008,Norway
Observationalcross-sectional
Outpatients 210 58 Breast, gynecologic,sarcoma, and others
Short episodes ofincreased painoccurring on top ofusual pain
74/210 (35.0) The prevalence of BTcPwas 26.2% with patientswith NRS #4 and43.7% for NRS >4
Mercadante,2008, Italy
Observationallongitudinal
Home care 73 71.9 Lung, breast, urogenital,and others
Transitory flare of painsuperimposed on anotherwise stable painpattern in patientstreated with opioids
35/73 (47.9)13/39 (33.3)
101 Patients recruited,and 73 were receivingdrugs for pain. Onemonth later, 41 patientswere still alive, and 39received analgesics
Breivik, 2009,Various
Observationalcross-sectional
Not clear 441 57.5 Breast, bowel,gynecologic, and others
Short incidence of pain ofa greater intensity tothe normal level ofpain in a patients withprescriptionmedication to treatpain
228/441 (51.7) 5084 Patients contacted,2864 having pain andmeeting the inclusioncriteria, 1226 included inthe telephonic interview,573 randomly selected,and 441 receivingprescription medicine
(Continued)
Vol.
47No.
1Jan
uary
2014
63
Prevalen
ceof
BTcP
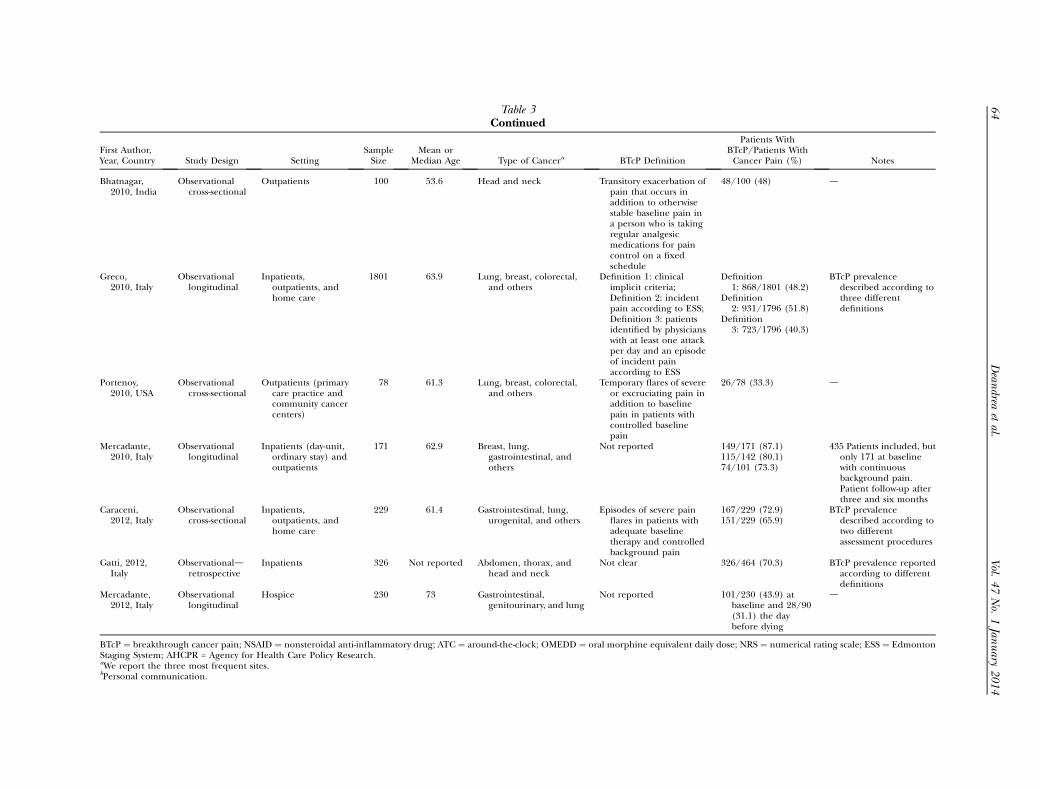
Table 3Continued
First Author,Year, Country Study Design Setting
SampleSize
Mean orMedian Age Type of Cancera BTcP Definition
Patients WithBTcP/Patients WithCancer Pain (%) Notes
Bhatnagar,2010, India
Observationalcross-sectional
Outpatients 100 53.6 Head and neck Transitory exacerbation ofpain that occurs inaddition to otherwisestable baseline pain ina person who is takingregular analgesicmedications for paincontrol on a fixedschedule
48/100 (48) d
Greco,2010, Italy
Observationallongitudinal
Inpatients,outpatients, andhome care
1801 63.9 Lung, breast, colorectal,and others
Definition 1: clinicalimplicit criteria;Definition 2: incidentpain according to ESS;Definition 3: patientsidentified by physicianswith at least one attackper day and an episodeof incident painaccording to ESS
Definition1: 868/1801 (48.2)
Definition2: 931/1796 (51.8)
Definition3: 723/1796 (40.3)
BTcP prevalencedescribed according tothree differentdefinitions
Portenoy,2010, USA
Observationalcross-sectional
Outpatients (primarycare practice andcommunity cancercenters)
78 61.3 Lung, breast, colorectal,and others
Temporary flares of severeor excruciating pain inaddition to baselinepain in patients withcontrolled baselinepain
26/78 (33.3) d
Mercadante,2010, Italy
Observationallongitudinal
Inpatients (day-unit,ordinary stay) andoutpatients
171 62.9 Breast, lung,gastrointestinal, andothers
Not reported 149/171 (87.1)115/142 (80.1)74/101 (73.3)
435 Patients included, butonly 171 at baselinewith continuousbackground pain.Patient follow-up afterthree and six months
Caraceni,2012, Italy
Observationalcross-sectional
Inpatients,outpatients, andhome care
229 61.4 Gastrointestinal, lung,urogenital, and others
Episodes of severe painflares in patients withadequate baselinetherapy and controlledbackground pain
167/229 (72.9)151/229 (65.9)
BTcP prevalencedescribed according totwo differentassessment procedures
Gatti, 2012,Italy
Observationaldretrospective
Inpatients 326 Not reported Abdomen, thorax, andhead and neck
Not clear 326/464 (70.3) BTcP prevalence reportedaccording to differentdefinitions
Mercadante,2012, Italy
Observationallongitudinal
Hospice 230 73 Gastrointestinal,genitourinary, and lung
Not reported 101/230 (43.9) atbaseline and 28/90(31.1) the daybefore dying
d
BTcP ¼ breakthrough cancer pain; NSAID ¼ nonsteroidal anti-inflammatory drug; ATC ¼ around-the-clock; OMEDD ¼ oral morphine equivalent daily dose; NRS ¼ numerical rating scale; ESS ¼ EdmontonStaging System; AHCPR = Agency for Health Care Policy Research.aWe report the three most frequent sites.bPersonal communication.
64
Vol.
47No.
1Jan
uary
2014
Dean
dreaetal.
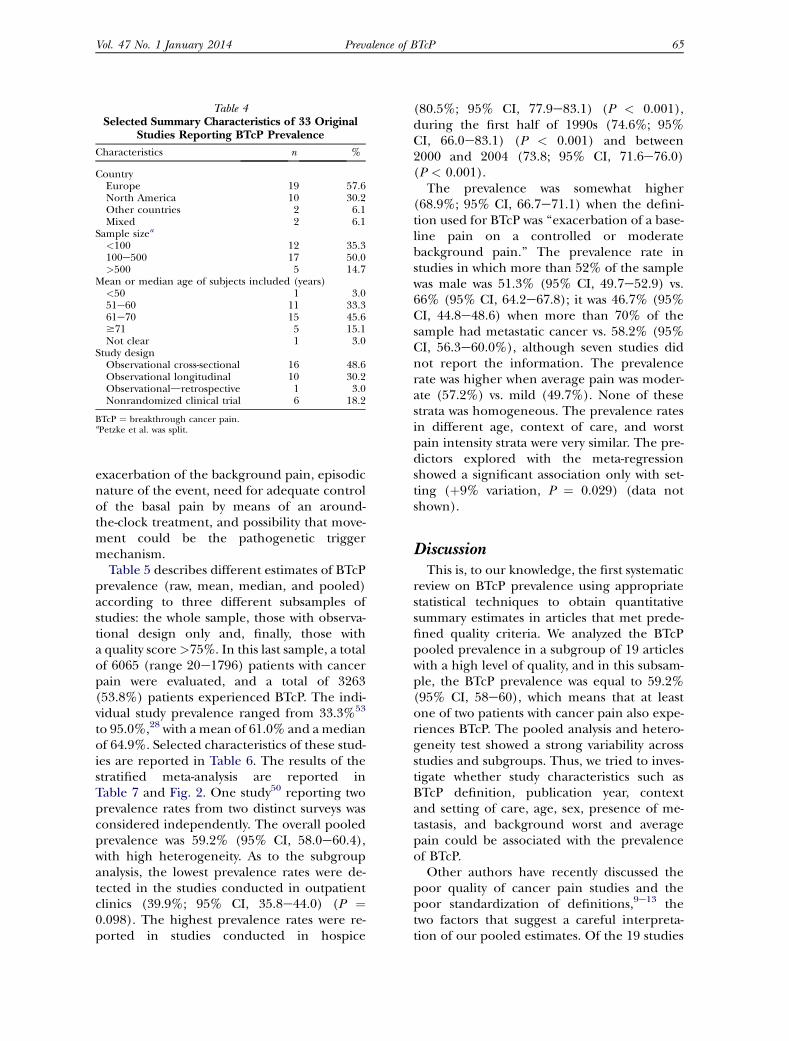
Table 4Selected Summary Characteristics of 33 Original
Studies Reporting BTcP Prevalence
Characteristics n %
CountryEurope 19 57.6North America 10 30.2Other countries 2 6.1Mixed 2 6.1
Sample sizea
<100 12 35.3100e500 17 50.0>500 5 14.7
Mean or median age of subjects included (years)<50 1 3.051e60 11 33.361e70 15 45.6$71 5 15.1Not clear 1 3.0
Study designObservational cross-sectional 16 48.6Observational longitudinal 10 30.2Observationaldretrospective 1 3.0Nonrandomized clinical trial 6 18.2
BTcP ¼ breakthrough cancer pain.aPetzke et al. was split.
Vol. 47 No. 1 January 2014 65Prevalence of BTcP
exacerbation of the background pain, episodicnature of the event, need for adequate controlof the basal pain by means of an around-the-clock treatment, and possibility that move-ment could be the pathogenetic triggermechanism.
Table 5 describes different estimates of BTcPprevalence (raw, mean, median, and pooled)according to three different subsamples ofstudies: the whole sample, those with observa-tional design only and, finally, those witha quality score>75%. In this last sample, a totalof 6065 (range 20e1796) patients with cancerpain were evaluated, and a total of 3263(53.8%) patients experienced BTcP. The indi-vidual study prevalence ranged from 33.3%53
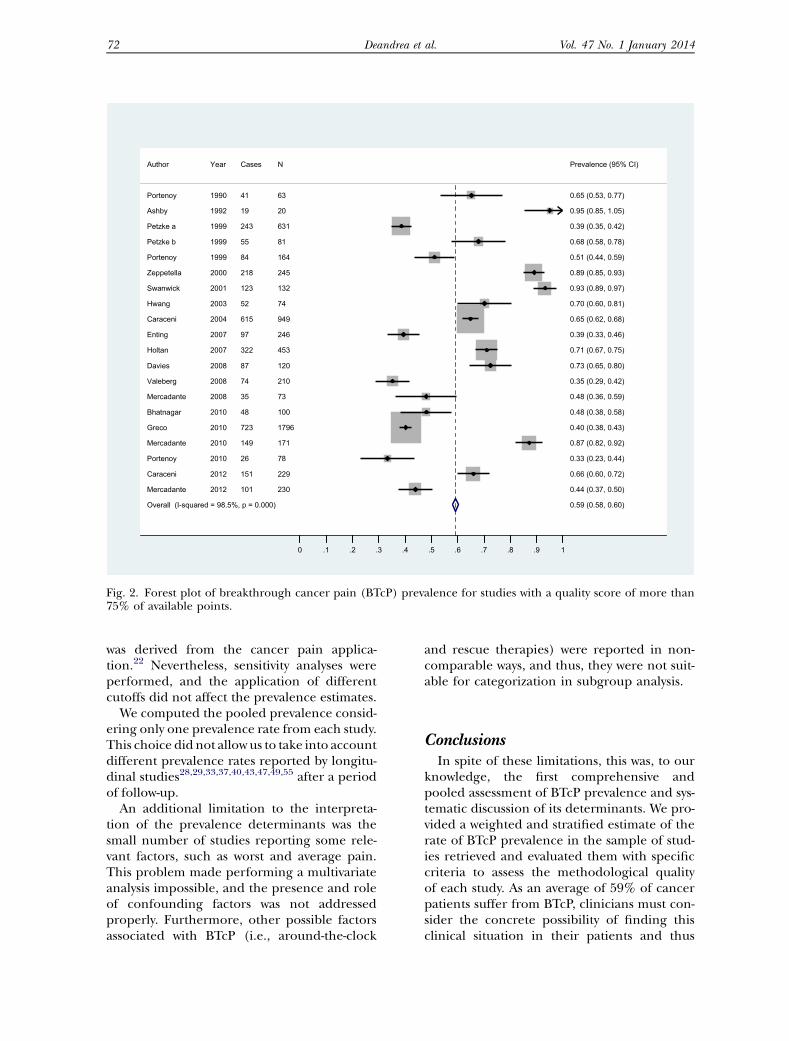
to 95.0%,28 with a mean of 61.0% and a medianof 64.9%. Selected characteristics of these stud-ies are reported in Table 6. The results of thestratified meta-analysis are reported inTable 7 and Fig. 2. One study50 reporting twoprevalence rates from two distinct surveys wasconsidered independently. The overall pooledprevalence was 59.2% (95% CI, 58.0e60.4),with high heterogeneity. As to the subgroupanalysis, the lowest prevalence rates were de-tected in the studies conducted in outpatientclinics (39.9%; 95% CI, 35.8e44.0) (P ¼0.098). The highest prevalence rates were re-ported in studies conducted in hospice
(80.5%; 95% CI, 77.9e83.1) (P < 0.001),during the first half of 1990s (74.6%; 95%CI, 66.0e83.1) (P < 0.001) and between2000 and 2004 (73.8; 95% CI, 71.6e76.0)(P < 0.001).
The prevalence was somewhat higher(68.9%; 95% CI, 66.7e71.1) when the defini-tion used for BTcP was ‘‘exacerbation of a base-line pain on a controlled or moderatebackground pain.’’ The prevalence rate instudies in which more than 52% of the samplewas male was 51.3% (95% CI, 49.7e52.9) vs.66% (95% CI, 64.2e67.8); it was 46.7% (95%CI, 44.8e48.6) when more than 70% of thesample had metastatic cancer vs. 58.2% (95%CI, 56.3e60.0%), although seven studies didnot report the information. The prevalencerate was higher when average pain was moder-ate (57.2%) vs. mild (49.7%). None of thesestrata was homogeneous. The prevalence ratesin different age, context of care, and worstpain intensity strata were very similar. The pre-dictors explored with the meta-regressionshowed a significant association only with set-ting (þ9% variation, P ¼ 0.029) (data notshown).
DiscussionThis is, to our knowledge, the first systematic
review on BTcP prevalence using appropriatestatistical techniques to obtain quantitativesummary estimates in articles that met prede-fined quality criteria. We analyzed the BTcPpooled prevalence in a subgroup of 19 articleswith a high level of quality, and in this subsam-ple, the BTcP prevalence was equal to 59.2%(95% CI, 58e60), which means that at leastone of two patients with cancer pain also expe-riences BTcP. The pooled analysis and hetero-geneity test showed a strong variability acrossstudies and subgroups. Thus, we tried to inves-tigate whether study characteristics such asBTcP definition, publication year, contextand setting of care, age, sex, presence of me-tastasis, and background worst and averagepain could be associated with the prevalenceof BTcP.
Other authors have recently discussed thepoor quality of cancer pain studies and thepoor standardization of definitions,9e13 thetwo factors that suggest a careful interpreta-tion of our pooled estimates. Of the 19 studies
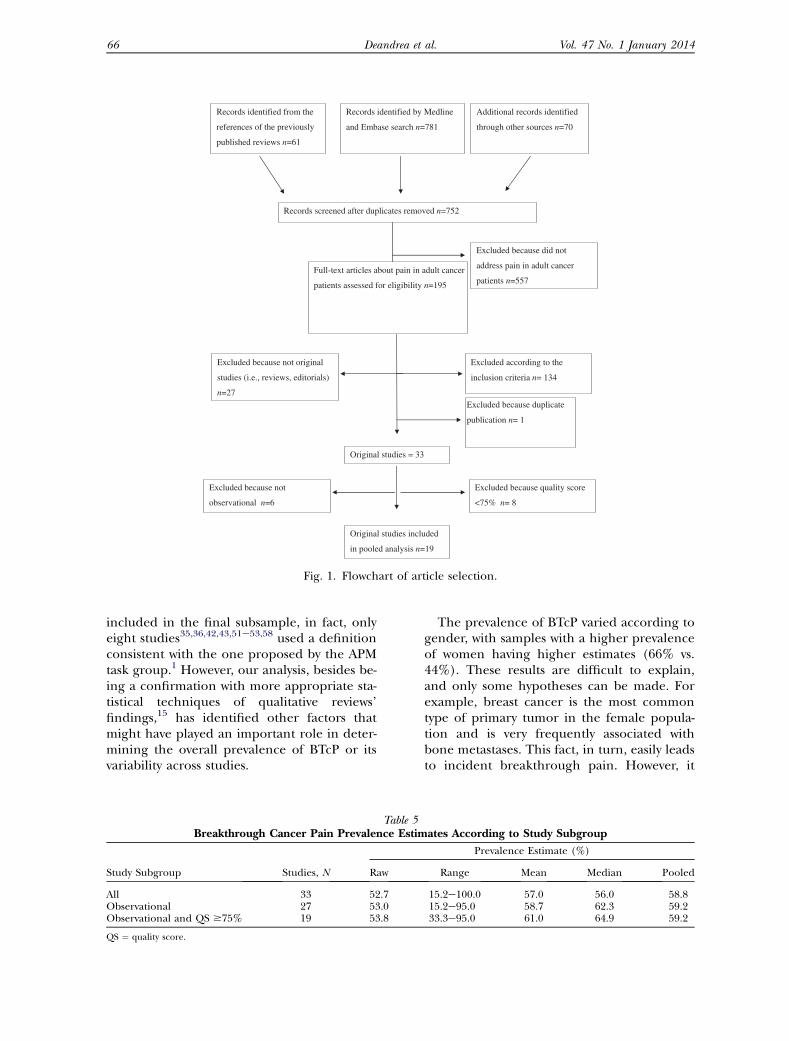
Records identified by Medline
and Embase search n=781
Records screened after duplicates removed n=752
Full-text articles about pain in adult cancer
patients assessed for eligibility n=195
Records identified from the
references of the previously
published reviews n=61
Original studies = 33
Excluded because did not
address pain in adult cancer
patients n=557
Additional records identified
through other sources n=70
Excluded according to the
inclusion criteria n= 134
Excluded because not original
studies (i.e., reviews, editorials)
n=27Excluded because duplicate
publication n= 1
Original studies included
in pooled analysis n=19
Excluded because quality score
<75% n= 8
Excluded because not
observational n=6
Fig. 1. Flowchart of article selection.
66 Vol. 47 No. 1 January 2014Deandrea et al.
included in the final subsample, in fact, onlyeight studies35,36,42,43,51e53,58 used a definitionconsistent with the one proposed by the APMtask group.1 However, our analysis, besides be-ing a confirmation with more appropriate sta-tistical techniques of qualitative reviews’findings,15 has identified other factors thatmight have played an important role in deter-mining the overall prevalence of BTcP or itsvariability across studies.
Table 5Breakthrough Cancer Pain Prevalence Estim
Study Subgroup Studies, N Raw
All 33 52.7Observational 27 53.0Observational and QS $75% 19 53.8
QS ¼ quality score.
The prevalence of BTcP varied according togender, with samples with a higher prevalenceof women having higher estimates (66% vs.44%). These results are difficult to explain,and only some hypotheses can be made. Forexample, breast cancer is the most commontype of primary tumor in the female popula-tion and is very frequently associated withbone metastases. This fact, in turn, easily leadsto incident breakthrough pain. However, it
ates According to Study Subgroup
Prevalence Estimate (%)
Range Mean Median Pooled
15.2e100.0 57.0 56.0 58.815.2e95.0 58.7 62.3 59.233.3e95.0 61.0 64.9 59.2
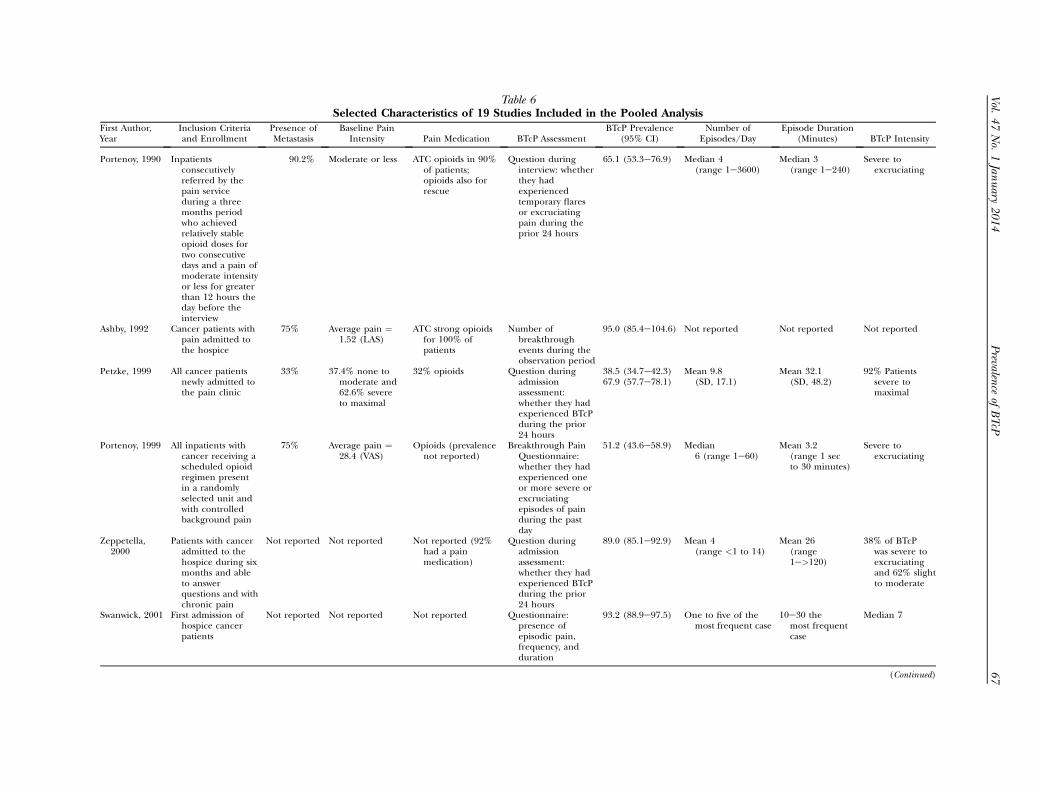
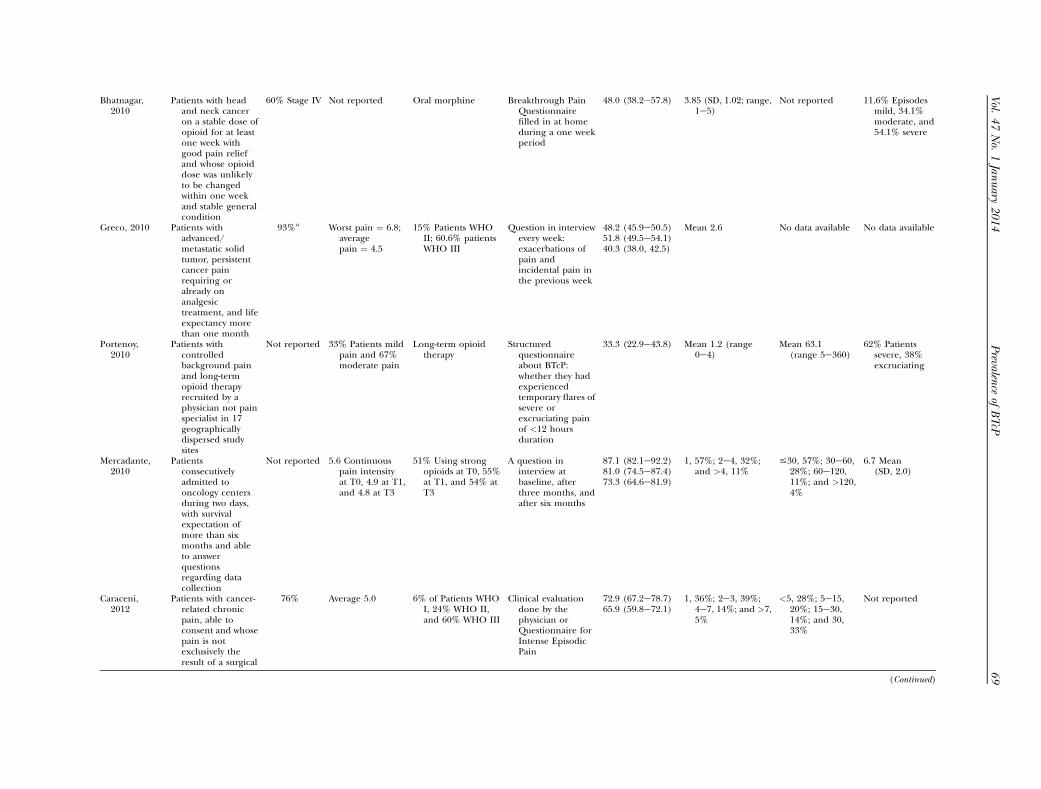
Table 6Selected Characteristics of 19 Studies Included in the Pooled Analysis
First Author,Year
Inclusion Criteriaand Enrollment
Presence ofMetastasis
Baseline PainIntensity Pain Medication BTcP Assessment
BTcP Prevalence(95% CI)
Number ofEpisodes/Day
Episode Duration(Minutes) BTcP Intensity
Portenoy, 1990 Inpatientsconsecutivelyreferred by thepain serviceduring a threemonths periodwho achievedrelatively stableopioid doses fortwo consecutivedays and a pain ofmoderate intensityor less for greaterthan 12 hours theday before theinterview
90.2% Moderate or less ATC opioids in 90%of patients;opioids also forrescue
Question duringinterview: whetherthey hadexperiencedtemporary flaresor excruciatingpain during theprior 24 hours
65.1 (53.3e76.9) Median 4(range 1e3600)
Median 3(range 1e240)
Severe toexcruciating
Ashby, 1992 Cancer patients withpain admitted tothe hospice
75% Average pain ¼1.52 (LAS)
ATC strong opioidsfor 100% ofpatients
Number ofbreakthroughevents during theobservation period
95.0 (85.4e104.6) Not reported Not reported Not reported
Petzke, 1999 All cancer patientsnewly admitted tothe pain clinic
33% 37.4% none tomoderate and62.6% severeto maximal
32% opioids Question duringadmissionassessment:whether they hadexperienced BTcPduring the prior24 hours
38.5 (34.7e42.3) Mean 9.8(SD, 17.1)
Mean 32.1(SD, 48.2)
92% Patientssevere tomaximal
67.9 (57.7e78.1)
Portenoy, 1999 All inpatients withcancer receiving ascheduled opioidregimen presentin a randomlyselected unit andwith controlledbackground pain
75% Average pain ¼28.4 (VAS)
Opioids (prevalencenot reported)
Breakthrough PainQuestionnaire:whether they hadexperienced oneor more severe orexcruciatingepisodes of painduring the pastday
51.2 (43.6e58.9) Median6 (range 1e60)
Mean 3.2(range 1 secto 30 minutes)
Severe toexcruciating
Zeppetella,2000
Patients with canceradmitted to thehospice during sixmonths and ableto answerquestions and withchronic pain
Not reported Not reported Not reported (92%had a painmedication)
Question duringadmissionassessment:whether they hadexperienced BTcPduring the prior24 hours
89.0 (85.1e92.9) Mean 4(range <1 to 14)
Mean 26(range1e>120)
38% of BTcPwas severe toexcruciatingand 62% slightto moderate
Swanwick, 2001 First admission ofhospice cancerpatients
Not reported Not reported Not reported Questionnaire:presence ofepisodic pain,frequency, andduration
93.2 (88.9e97.5) One to five of themost frequent case
10e30 themost frequentcase
Median 7
(Continued)
Vol.
47No.
1Jan
uary
2014
67
Prevalen
ceof
BTcP
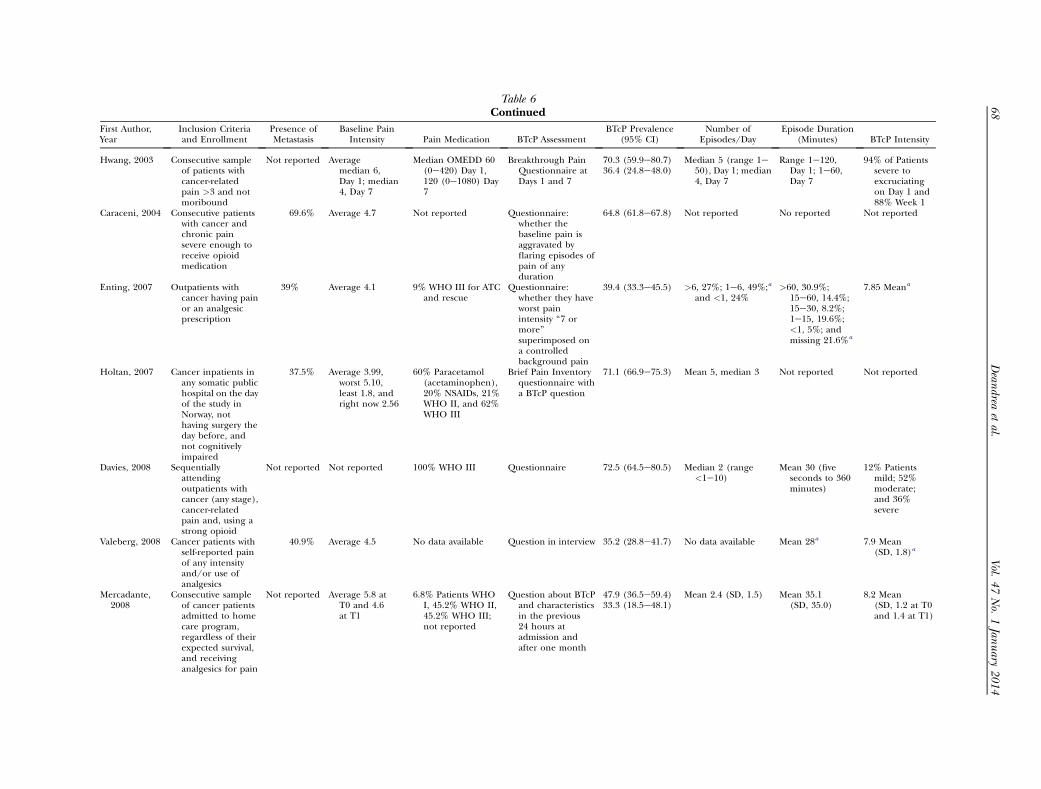
Table 6Continued
First Author,Year
Inclusion Criteriaand Enrollment
Presence ofMetastasis
Baseline PainIntensity Pain Medication BTcP Assessment
BTcP Prevalence(95% CI)
Number ofEpisodes/Day
Episode Duration(Minutes) BTcP Intensity
Hwang, 2003 Consecutive sampleof patients withcancer-relatedpain >3 and notmoribound
Not reported Averagemedian 6,Day 1; median4, Day 7
Median OMEDD 60(0e420) Day 1,120 (0e1080) Day7
Breakthrough PainQuestionnaire atDays 1 and 7
70.3 (59.9e80.7) Median 5 (range 1e50), Day 1; median4, Day 7
Range 1e120,Day 1; 1e60,Day 7
94% of Patientssevere toexcruciatingon Day 1 and88% Week 1
36.4 (24.8e48.0)
Caraceni, 2004 Consecutive patientswith cancer andchronic painsevere enough toreceive opioidmedication
69.6% Average 4.7 Not reported Questionnaire:whether thebaseline pain isaggravated byflaring episodes ofpain of anyduration
64.8 (61.8e67.8) Not reported No reported Not reported
Enting, 2007 Outpatients withcancer having painor an analgesicprescription
39% Average 4.1 9% WHO III for ATCand rescue
Questionnaire:whether they haveworst painintensity ‘‘7 ormore’’superimposed ona controlledbackground pain
39.4 (33.3e45.5) >6, 27%; 1e6, 49%;a
and <1, 24%>60, 30.9%;
15e60, 14.4%;15e30, 8.2%;1e15, 19.6%;<1, 5%; andmissing 21.6%a
7.85 Meana
Holtan, 2007 Cancer inpatients inany somatic publichospital on the dayof the study inNorway, nothaving surgery theday before, andnot cognitivelyimpaired
37.5% Average 3.99,worst 5.10,least 1.8, andright now 2.56
60% Paracetamol(acetaminophen),20% NSAIDs, 21%WHO II, and 62%WHO III
Brief Pain Inventoryquestionnaire witha BTcP question
71.1 (66.9e75.3) Mean 5, median 3 Not reported Not reported
Davies, 2008 Sequentiallyattendingoutpatients withcancer (any stage),cancer-relatedpain and, using astrong opioid
Not reported Not reported 100% WHO III Questionnaire 72.5 (64.5e80.5) Median 2 (range<1e10)
Mean 30 (fiveseconds to 360minutes)
12% Patientsmild; 52%moderate;and 36%severe
Valeberg, 2008 Cancer patients withself-reported painof any intensityand/or use ofanalgesics
40.9% Average 4.5 No data available Question in interview 35.2 (28.8e41.7) No data available Mean 28a 7.9 Mean(SD, 1.8)a
Mercadante,2008
Consecutive sampleof cancer patientsadmitted to homecare program,regardless of theirexpected survival,and receivinganalgesics for pain
Not reported Average 5.8 atT0 and 4.6at T1
6.8% Patients WHOI, 45.2% WHO II,45.2% WHO III;not reported
Question about BTcPand characteristicsin the previous24 hours atadmission andafter one month
47.9 (36.5e59.4) Mean 2.4 (SD, 1.5) Mean 35.1(SD, 35.0)
8.2 Mean(SD, 1.2 at T0and 1.4 at T1)
33.3 (18.5e48.1)
68
Vol.
47No.
1Jan
uary
2014
Dean
dreaetal.
Bhatnagar,2010
Patients with headand neck canceron a stable dose ofopioid for at leastone week withgood pain reliefand whose opioiddose was unlikelyto be changedwithin one weekand stable generalcondition
60% Stage IV Not reported Oral morphine Breakthrough PainQuestionnairefilled in at homeduring a one weekperiod
48.0 (38.2e57.8) 3.85 (SD, 1.02; range,1e5)
Not reported 11.6% Episodesmild, 34.1%moderate, and54.1% severe
Greco, 2010 Patients withadvanced/metastatic solidtumor, persistentcancer painrequiring oralready onanalgesictreatment, and lifeexpectancy morethan one month
93%a Worst pain ¼ 6.8;averagepain ¼ 4.5
15% Patients WHOII; 60.6% patientsWHO III
Question in interviewevery week:exacerbations ofpain andincidental pain inthe previous week
48.2 (45.9e50.5) Mean 2.6 No data available No data available51.8 (49.5e54.1)40.3 (38.0, 42.5)
Portenoy,2010
Patients withcontrolledbackground painand long-termopioid therapyrecruited by aphysician not painspecialist in 17geographicallydispersed studysites
Not reported 33% Patients mildpain and 67%moderate pain
Long-term opioidtherapy
Structuredquestionnaireabout BTcP:whether they hadexperiencedtemporary flares ofsevere orexcruciating painof <12 hoursduration
33.3 (22.9e43.8) Mean 1.2 (range0e4)
Mean 63.1(range 5e360)
62% Patientssevere, 38%excruciating
Mercadante,2010
Patientsconsecutivelyadmitted tooncology centersduring two days,with survivalexpectation ofmore than sixmonths and ableto answerquestionsregarding datacollection
Not reported 5.6 Continuouspain intensityat T0, 4.9 at T1,and 4.8 at T3
51% Using strongopioids at T0, 55%at T1, and 54% atT3
A question ininterview atbaseline, afterthree months, andafter six months
87.1 (82.1e92.2) 1, 57%; 2e4, 32%;and >4, 11%
#30, 57%; 30e60,28%; 60e120,11%; and >120,4%
6.7 Mean(SD, 2.0)81.0 (74.5e87.4)
73.3 (64.6e81.9)
Caraceni,2012
Patients with cancer-related chronicpain, able toconsent and whosepain is notexclusively theresult of a surgical
76% Average 5.0 6% of Patients WHOI, 24% WHO II,and 60% WHO III
Clinical evaluationdone by thephysician orQuestionnaire forIntense EpisodicPain
72.9 (67.2e78.7) 1, 36%; 2e3, 39%;4e7, 14%; and >7,5%
<5, 28%; 5e15,20%; 15e30,14%; and 30,33%
Not reported65.9 (59.8e72.1)
(Continued)
Vol.
47No.
1Jan
uary
2014
69
Prevalen
ceof
BTcP
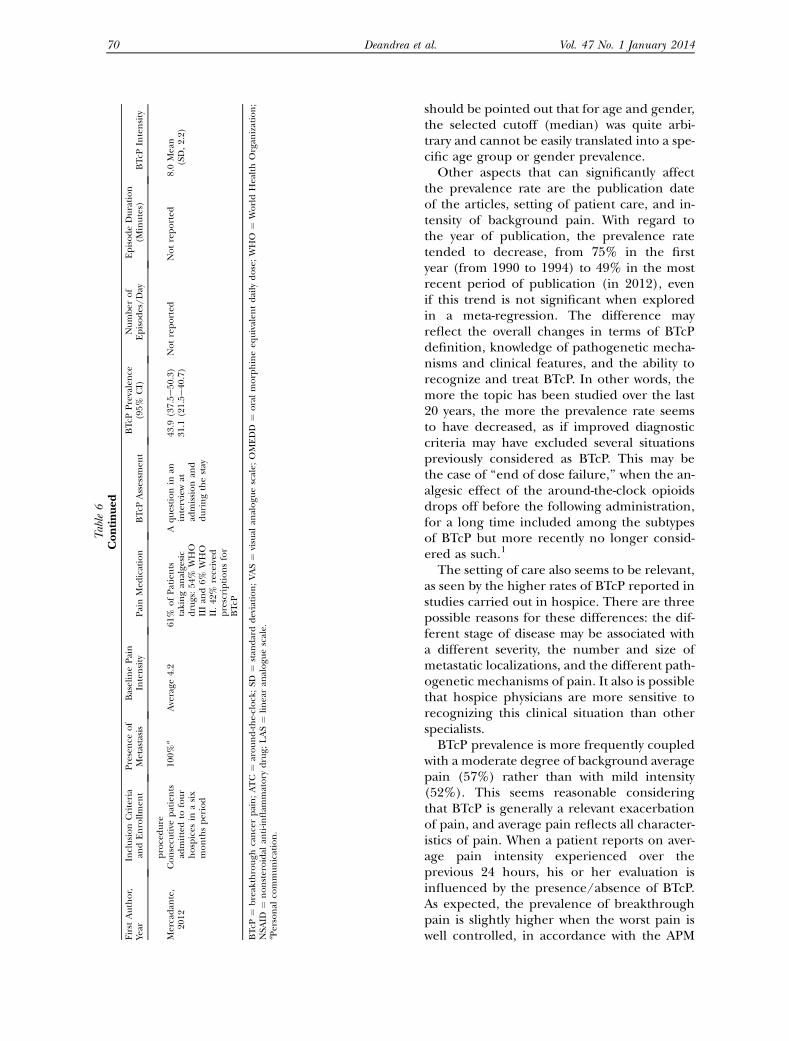
Table6
Continued
First
Author,
Year
InclusionCriteria
andEnrollmen
tPresence
of
Metastasis
BaselinePain
Intensity
PainMed
ication
BTcP
Assessm
ent
BTcP
Prevalence
(95%
CI)
Number
of
Episodes/Day
EpisodeDuration
(Minutes)
BTcP
Intensity
procedure
Mercadan
te,
2012
Consecu
tive
patients
admittedto
four
hospices
inasix
monthsperiod
100%
aAverage
4.2
61%
ofPatients
takingan
alge
sic
drugs:54
%WHO
IIIan
d6%
WHO
II.42
%received
prescriptionsfor
BTcP
Aquestionin
aninterviewat
admissionan
dduringthestay
43.9
(37.5e50
.3)
Notreported
Notreported
8.0Mean
(SD,2.2)
31.1
(21.5e40
.7)
BTcP
¼breakthrough
cancerpain;ATC
¼around-the-clock;SD
¼stan
darddeviation;VAS¼
visual
analogu
escale;
OMEDD
¼oralmorphineeq
uivalen
tdaily
dose;WHO
¼WorldHealthOrgan
ization;
NSA
ID¼
nonsteroidal
anti-in
flam
matory
drug;
LAS¼
linearan
alogu
escale.
aPersonal
communication.
70 Vol. 47 No. 1 January 2014Deandrea et al.
should be pointed out that for age and gender,the selected cutoff (median) was quite arbi-trary and cannot be easily translated into a spe-cific age group or gender prevalence.Other aspects that can significantly affect
the prevalence rate are the publication dateof the articles, setting of patient care, and in-tensity of background pain. With regard tothe year of publication, the prevalence ratetended to decrease, from 75% in the firstyear (from 1990 to 1994) to 49% in the mostrecent period of publication (in 2012), evenif this trend is not significant when exploredin a meta-regression. The difference mayreflect the overall changes in terms of BTcPdefinition, knowledge of pathogenetic mecha-nisms and clinical features, and the ability torecognize and treat BTcP. In other words, themore the topic has been studied over the last20 years, the more the prevalence rate seemsto have decreased, as if improved diagnosticcriteria may have excluded several situationspreviously considered as BTcP. This may bethe case of ‘‘end of dose failure,’’ when the an-algesic effect of the around-the-clock opioidsdrops off before the following administration,for a long time included among the subtypesof BTcP but more recently no longer consid-ered as such.1
The setting of care also seems to be relevant,as seen by the higher rates of BTcP reported instudies carried out in hospice. There are threepossible reasons for these differences: the dif-ferent stage of disease may be associated witha different severity, the number and size ofmetastatic localizations, and the different path-ogenetic mechanisms of pain. It also is possiblethat hospice physicians are more sensitive torecognizing this clinical situation than otherspecialists.BTcP prevalence is more frequently coupled
with a moderate degree of background averagepain (57%) rather than with mild intensity(52%). This seems reasonable consideringthat BTcP is generally a relevant exacerbationof pain, and average pain reflects all character-istics of pain. When a patient reports on aver-age pain intensity experienced over theprevious 24 hours, his or her evaluation isinfluenced by the presence/absence of BTcP.As expected, the prevalence of breakthroughpain is slightly higher when the worst pain iswell controlled, in accordance with the APM
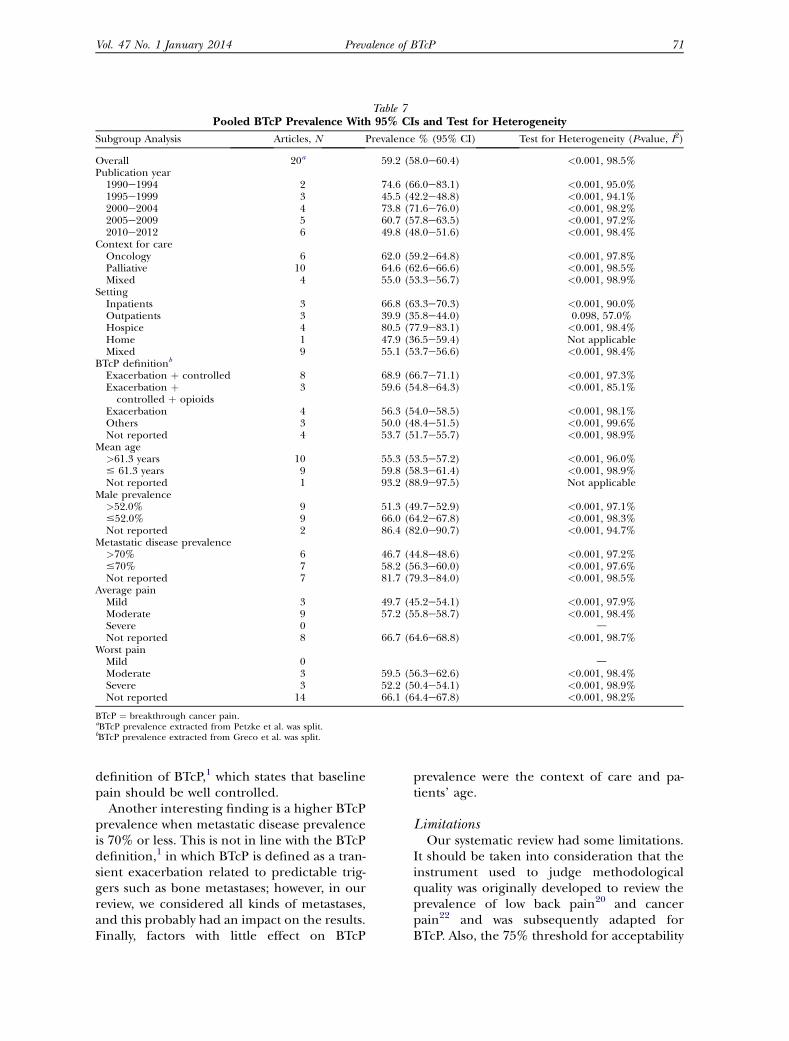
Table 7Pooled BTcP Prevalence With 95% CIs and Test for Heterogeneity
Subgroup Analysis Articles, N Prevalence % (95% CI) Test for Heterogeneity (P-value, I2)
Overall 20a 59.2 (58.0e60.4) <0.001, 98.5%Publication year
1990e1994 2 74.6 (66.0e83.1) <0.001, 95.0%1995e1999 3 45.5 (42.2e48.8) <0.001, 94.1%2000e2004 4 73.8 (71.6e76.0) <0.001, 98.2%2005e2009 5 60.7 (57.8e63.5) <0.001, 97.2%2010e2012 6 49.8 (48.0e51.6) <0.001, 98.4%
Context for careOncology 6 62.0 (59.2e64.8) <0.001, 97.8%Palliative 10 64.6 (62.6e66.6) <0.001, 98.5%Mixed 4 55.0 (53.3e56.7) <0.001, 98.9%
SettingInpatients 3 66.8 (63.3e70.3) <0.001, 90.0%Outpatients 3 39.9 (35.8e44.0) 0.098, 57.0%Hospice 4 80.5 (77.9e83.1) <0.001, 98.4%Home 1 47.9 (36.5e59.4) Not applicableMixed 9 55.1 (53.7e56.6) <0.001, 98.4%
BTcP definitionb
Exacerbation þ controlled 8 68.9 (66.7e71.1) <0.001, 97.3%Exacerbation þcontrolled þ opioids
3 59.6 (54.8e64.3) <0.001, 85.1%
Exacerbation 4 56.3 (54.0e58.5) <0.001, 98.1%Others 3 50.0 (48.4e51.5) <0.001, 99.6%Not reported 4 53.7 (51.7e55.7) <0.001, 98.9%
Mean age>61.3 years 10 55.3 (53.5e57.2) <0.001, 96.0%# 61.3 years 9 59.8 (58.3e61.4) <0.001, 98.9%Not reported 1 93.2 (88.9e97.5) Not applicable
Male prevalence>52.0% 9 51.3 (49.7e52.9) <0.001, 97.1%#52.0% 9 66.0 (64.2e67.8) <0.001, 98.3%Not reported 2 86.4 (82.0e90.7) <0.001, 94.7%
Metastatic disease prevalence>70% 6 46.7 (44.8e48.6) <0.001, 97.2%#70% 7 58.2 (56.3e60.0) <0.001, 97.6%Not reported 7 81.7 (79.3e84.0) <0.001, 98.5%
Average painMild 3 49.7 (45.2e54.1) <0.001, 97.9%Moderate 9 57.2 (55.8e58.7) <0.001, 98.4%Severe 0 dNot reported 8 66.7 (64.6e68.8) <0.001, 98.7%
Worst painMild 0 dModerate 3 59.5 (56.3e62.6) <0.001, 98.4%Severe 3 52.2 (50.4e54.1) <0.001, 98.9%Not reported 14 66.1 (64.4e67.8) <0.001, 98.2%
BTcP ¼ breakthrough cancer pain.aBTcP prevalence extracted from Petzke et al. was split.bBTcP prevalence extracted from Greco et al. was split.
Vol. 47 No. 1 January 2014 71Prevalence of BTcP
definition of BTcP,1 which states that baselinepain should be well controlled.
Another interesting finding is a higher BTcPprevalence when metastatic disease prevalenceis 70% or less. This is not in line with the BTcPdefinition,1 in which BTcP is defined as a tran-sient exacerbation related to predictable trig-gers such as bone metastases; however, in ourreview, we considered all kinds of metastases,and this probably had an impact on the results.Finally, factors with little effect on BTcP
prevalence were the context of care and pa-tients’ age.
LimitationsOur systematic review had some limitations.
It should be taken into consideration that theinstrument used to judge methodologicalquality was originally developed to review theprevalence of low back pain20 and cancerpain22 and was subsequently adapted forBTcP. Also, the 75% threshold for acceptability
Overall (I-squared = 98.5%, p = 0.000)
Portenoy
Portenoy
Caraceni
Mercadante
Mercadante
Greco
Holtan
Petzke a
Author
Valeberg
Enting
Petzke b
Caraceni
Ashby
Mercadante
Portenoy
Hwang
Bhatnagar
Davies
Zeppetella
Swanwick
1990
2010
2004
2010
2012
2010
2007
1999
Year
2008
2007
1999
2012
1992
2008
1999
2003
2010
2008
2000
2001
41
26
615
149
101
723
322
243
Cases
74
97
55
151
19
35
84
52
48
87
218
123
63
78
949
171
230
1796
453
631
N
210
246
81
229
20
73
164
74
100
120
245
132
0.59 (0.58, 0.60)
0.65 (0.53, 0.77)
0.33 (0.23, 0.44)
0.65 (0.62, 0.68)
0.87 (0.82, 0.92)
0.44 (0.37, 0.50)
0.40 (0.38, 0.43)
0.71 (0.67, 0.75)
0.39 (0.35, 0.42)
Prevalence (95% CI)
0.35 (0.29, 0.42)
0.39 (0.33, 0.46)
0.68 (0.58, 0.78)
0.66 (0.60, 0.72)
0.95 (0.85, 1.05)
0.48 (0.36, 0.59)
0.51 (0.44, 0.59)
0.70 (0.60, 0.81)
0.48 (0.38, 0.58)
0.73 (0.65, 0.80)
0.89 (0.85, 0.93)
0.93 (0.89, 0.97)
0 .1 .2 .3 .4 .5 .6 .7 .8 .9 1
Fig. 2. Forest plot of breakthrough cancer pain (BTcP) prevalence for studies with a quality score of more than75% of available points.
72 Vol. 47 No. 1 January 2014Deandrea et al.
was derived from the cancer pain applica-tion.22 Nevertheless, sensitivity analyses wereperformed, and the application of differentcutoffs did not affect the prevalence estimates.
We computed the pooled prevalence consid-ering only one prevalence rate from each study.This choice did not allowus to take into accountdifferent prevalence rates reported by longitu-dinal studies28,29,33,37,40,43,47,49,55 after a periodof follow-up.
An additional limitation to the interpreta-tion of the prevalence determinants was thesmall number of studies reporting some rele-vant factors, such as worst and average pain.This problem made performing a multivariateanalysis impossible, and the presence and roleof confounding factors was not addressedproperly. Furthermore, other possible factorsassociated with BTcP (i.e., around-the-clock
and rescue therapies) were reported in non-comparable ways, and thus, they were not suit-able for categorization in subgroup analysis.
ConclusionsIn spite of these limitations, this was, to our
knowledge, the first comprehensive andpooled assessment of BTcP prevalence and sys-tematic discussion of its determinants. We pro-vided a weighted and stratified estimate of therate of BTcP prevalence in the sample of stud-ies retrieved and evaluated them with specificcriteria to assess the methodological qualityof each study. As an average of 59% of cancerpatients suffer from BTcP, clinicians must con-sider the concrete possibility of finding thisclinical situation in their patients and thus
Vol. 47 No. 1 January 2014 73Prevalence of BTcP
must apply standardized definitions and classi-fication systems of BTcP to prescribe the mostappropriate treatments. This finding also mayguide researchers in better designing futurestudies and consistently collecting importantvariables for the interpretation of BTcP preva-lence figures (i.e., baseline pain intensity andtherapies).
Disclosures and AcknowledgmentsThis work was supported by an uncondi-
tional grant from Grunenthal-Italy. Dr. Apol-one and Dr. Corli have received consultingand lecture fees from Grunenthal-Italy. Allthe remaining authors declare no conflicts ofinterest.
The authors thank Alessandra Favero andIlir Ileshi for their assistance in the literaturesearch.
References1. Davies AN, Dickman A, Reid C, et al. ScienceCommittee of the Association for Palliative Medi-cine of Great Britain and Ireland. The managementof cancer-related breakthrough pain: recommenda-tions of a task group of the Science Committee ofthe Association for Palliative Medicine of Great Brit-ain and Ireland. Eur J Pain 2009;13:331e338.
2. Caraceni A, Hanks G, Kaasa S, et al. for theEuropean Palliative Care Research Collaborative(EPCRC), on behalf of the European Associationfor Palliative Care (EAPC). Use of opioid analgesicin the treatment of the cancer pain: evidence-based recommendations from the EAPC. LancetOncol 2012;13:e58ee68.
3. Mercadante S, Radbruch L, Davies A, et al.A comparison of intranasal fentanyl spray with oraltransmucosal fentanyl citrate for the treatment ofbreakthrough cancer pain: an open-label, random-ized, crossover trial. Curr Med Res Opin 2009;25:2805e2815.
4. Rauck RL, Tark M, Reyes E, et al. Efficacy andlong-term tolerability of sublingual fentanyl orallydisintegrating tablet in the treatment of break-through cancer pain. Curr Med Res Opin 2009;25:2877e2885.
5. Zeppetella G. Sublingual fentanyl (Abstral) forbreakthrough cancer pain. Eur Oncol 2009;1:10e13.
6. Delgado-Guay MO. Efficacy and safety of fentan-yl buccal for cancer pain management by adminis-tration through a soluble film: an update. CancerManag Res 2010;2:303e306.
7. Fisher A, Watling M, Smith A, Knight A. Phar-macokinetics and relative bioavailability of fentanylpectin nasal spray 100-800 mg in healthy volunteers.Int J Clin Pharmacol Ther 2010;48:860e867.
8. Kaasa S, Moksnes K, Nolte T, et al. Pharmacoki-netics of intranasal fentanyl spray in patients withcancer and breakthrough pain. J Opioid Manag2010;6:17e26.
9. Mercadante S, Radbruch I, Caraceni A, et al. Ep-isodic (breakthrough) pain: consensus conferenceof an expert working group of the European Associ-ation for Palliative Care. Cancer 2002;94:832e839.
10. Zeppetella G, Ribeiro MDC. The pharmacother-apy of cancer-related episodic pain. Expert OpinPharmacother 2003;4:493e502.
11. Caraceni A, Portenoy R, on behalf of the Work-ing Group of the IASP Task Force on Cancer Pain.An international survey of cancer pain characteris-tics and syndromes. Pain 1999;82:263e274.
12. Zeppetella G, Ribeiro MDC. Opioids for themanagement of breakthrough (episodic) pain incancer patients. Cochrane Database Syst Rev 2006;1:CD004311.
13. Zeppetella G. Impact and management ofbreakthrough pain in cancer. Curr Opin SupportPalliat Care 2009;3:1e6.
14. Haugen DF, Hjermstad MJ, Hagen N, et al. onbehalf of the European Palliative Care ResearchCollaborative (EPCRC). Assessment and classifica-tion of cancer breakthrough pain: a systematic liter-ature review. Pain 2010;149:476e482.
15. Svendsen KB, Andersen S, Arnason S, et al.Breakthrough pain in malignant and non-malignant diseases: a review of prevalence, charac-teristics and mechanisms. Eur J Pain 2005;9:195e206.
16. Smith H. A comprehensive review of rapid-onset opioids for breakthrough pain. CNS Drugs2012;26:509e535.
17. Davis MP. Fentanyl for breakthrough pain: a sys-tematic review. Expert Rev Neurother 2011;11:1197e1216.
18. Zeppetella G. Opioids for the management ofbreakthrough cancer pain in adults: a systematic re-view undertaken as part of an EPCRC opioid guide-lines project. Palliat Med 2011;25:516e524.
19. Nicholson B, Agarwala SS. Opioid delivery inthe treatment of cancer breakthrough pain: a reviewof routes of administration. J Opioid Manag 2011;7:69e79.
20. Leboeuf-Yde C, Lauritsen JM. The prevalence oflow back pain in the literature. A structured reviewof 26 Nordic studies from 1954 to 1993. Spine1995;20:2112e2118.
21. Walker BF. The prevalence of low back pain:a systematic review of the literature from 1966 to1998. J Spinal Disord 2000;13:205e217.
74 Vol. 47 No. 1 January 2014Deandrea et al.
22. van den Beuken-van den Everdingen MH, deRijke JM, Kessels AG, et al. Prevalence of pain in pa-tients with cancer: a systematic review of the past 40years. Ann Oncol 2007;18:1437e1449.
23. G�omez-Batiste X, Madrid F, Moreno F, et al.Breakthrough cancer pain: prevalence and charac-teristics in patients in Catalonia, Spain. J Pain Symp-tom Manage 2002;24:45e52.
24. DerSimonian R, Laird N. Meta-analysis in clini-cal trials. Control Clin Trials 1986;7:177e188.
25. Oldenmenger WH, de Raaf PJ, de Klerk C, vander Rijt CC. Cut points on 0-10 numeric ratingscales for symptoms included in the EdmontonSymptom Assessment Scale in cancer patients: a sys-tematic review. J Pain Symptom Manage 2013;45:1083e1093.
26. Higgins JP, Thompson SG, Deeks JJ,Altman DG. Measuring inconsistency in meta-analy-ses. BMJ 2003;327:557e560.
27. Caraceni A, Martini C, Zecca E. Breakthroughpain characteristics and syndrome in patients withcancer pain. An international survey. Palliat Med2004;18:177e183.
28. Ashby MA, Fleming BG, Brooksbank M, et al.Description of a mechanistic approach to pain man-agement in advanced cancer. Preliminary report.Pain 1992;51:153e161.
29. Banning A, Sjogren P, Henriksen H. Treatmentoutcome in a multidisciplinary cancer pain clinic.Pain 1991;47:129e134.
30. Bhatnagar S, Upadhyay S, Mishra S. Prevalenceand characteristics of breakthrough pain in patientswith head and neck cancer: a cross-sectional study.J Palliat Med 2010;13:291e295.
31. Breivik H, Cherny N, Collett B, et al. Cancer-re-lated pain: a pan-European survey of prevalence,treatment, and patient attitudes. Ann Oncol 2009;20:1420e1433.
32. Caraceni A, Bertetto O, Labianca R. Episodic(breakthrough) pain prevalence in a populationof cancer pain patients. Comparison of clinical diag-noses with the QUDEIdItalian questionnaire for in-tense episodic pain. J Pain Symptom Manage 2012;43:833e841.
33. Chow E, Ling A, Davis L, et al. Pain flare follow-ing external beam radiotherapy and meaningfulchange in pain scores in the treatment of bone me-tastases. Radiother Oncol 2005;75:64e69.
34. Chow E, Loblaw A, Harris K, et al. Dexametha-sone for the prophylaxis of radiation inducedpain flare after palliative radiotherapy for bonemetastasesda pilot study. Support Care Cancer2007;15:643e647.
35. Davies AN, Vriens J, Kennett A, McTaggart M.An observational study of oncology patients’ utiliza-tion of breakthrough pain medication. J Pain Symp-tom Manage 2008;35:406e411.
36. Enting RH, Oldenmenger WH, Van Gool AR,van der Rijt CC, Sillevis Smitt PA. The effects of an-algesic prescription and patient adherence on painin a Dutch outpatient cancer population. J PainSymptom Manage 2007;35:523e531.
37. Fainsinger RL, Nekolaichuk CL, Lawlor OG,et al. A multicenter study of the revised EdmontonStaging System for classifying cancer pain in ad-vanced cancer patients. J Pain Symptom Manage2005;29:224e237.
38. Fortner BR, Okon TA, Portenoy RK. A survey ofpain-related hospitalizations, emergency depart-ment visits, and physician office visits reported bycancer patients with and without a history of break-through pain. J Pain 2002;3:38e44.
39. Gatti A, Mediati RD, Reale C, et al. Break-through pain in patients referred to pain clinics:the Italian pain network retrospective study. AdvTher 2012;29:464e472.
40. Greco MT, Corli O, Montanari M, et al. Epide-miology and pattern of care of breakthrough cancerpain in a longitudinal sample of cancer patients: re-sults from the cancer pain outcome research studygroup. Clin J Pain 2011;27:9e18.
41. Hird A, Chow E, Zhang L, et al. Determiningthe incidence of pain flare following palliative radio-therapy for symptomatic bone metastases: resultsfrom three Canadian cancer centers. Int J RadiatOncol Biol Phys 2009;75:193e197.
42. Holtan A, Aass N, Nordoy T, et al. Prevalence ofpain in hospitalised cancer patients in Norway: a na-tional survey. Palliat Med 2007;21:7e13.
43. Hwang SS, Chang VT, Kasimis B. Cancer break-through pain characteristics and responses to treat-ment at a VA medical center. Pain 2003;101:55e64.
44. Kerr IG, Sone M, Deangelis C, et al. Continuousnarcotics infusion with patient-controlled analgesiafor chronic cancer pain in outpatients. Ann InternMed 1988;108:554e557.
45. Mercadante S, Maddaloni S, Roccella S,Salvaggio L. Predictive factors in advanced cancerpain treated only by analgesics. Pain 1992;50:151e155.
46. Mercadante S, Armata M, Salvaggio L. Paincharacteristics of advanced lung cancer patients re-ferred to a palliative care service. Pain 1994;59:141e145.
47. Mercadante S, Intravaia G, Villari P, et al. Intra-venous morphine for breakthrough (episodic) painin an acute palliative care unit: a confirmatory study.J Pain Symptom Manage 2008;35:307e313.
48. Mercadante S, Zagonel V, Breda E, et al. Break-through pain in oncology: a longitudinal study.J Pain Symptom Manage 2010;40:183e190.
49. Mercadante S, Valle A, Sabba S. Pattern andcharacteristics of advanced cancer patients admittedto hospices in Italy. Support Care Cancer 2013;21:935e939.
Vol. 47 No. 1 January 2014 75Prevalence of BTcP
50. Petzke F, Radbruch L, Zech D, et al. Temporalpresentation of chronic cancer pain: transitorypains on admission to a multidisciplinary painclinic. J Pain Symptom Manage 1999;17:391e401.
51. Portenoy KR, Hagen NA. Breakthrough pain:definition, prevalence and characteristics. Pain1990;41:273e281.
52. Portenoy RK, Payne D, Jacobsen P. Break-through pain: characteristics and impact in patientswith cancer pain. Pain 1999;81:129e134.
53. Portenoy RK, Bruns D, Shoemaker B,Shoemaker SA. Breakthrough pain in community-dwelling patients with cancer pain and noncancerpain, part1: prevalence and characteristics.J Opioid Manag 2010;6:97e108.
54. Ripamonti C, Fagnoni E, Campa T, et al. De-creases in pain at rest and movement-related painduring zoledronic acid treatment in patients withbone metastases due to breast or prostate cancer:
a pilot study. Support Care Cancer 2007;15:1177e1184.
55. Str€omgren AS, Groenvold M, Petersen MA,et al. Pain characteristics and treatment outcomefor advanced cancer patients during the first weekof specialized palliative care. J Pain Symptom Man-age 2004;27:104e113.
56. Swanwick M, Haworth M, Lennard RF. Theprevalence of episodic pain in cancer: a survey ofhospice patients on admission. Palliat Med 2001;15:9e18.
57. Valeberg BT, Miaskowski C, Hanestad BR, et al.Demographic, clinical, and pain characteristics areassociated with average pain severity groups in a sam-ple of oncology outpatients. J Pain 2008;9:873e882.
58. Zeppetella G, O’Doherty CA, Collins S. Preva-lence and characteristics of breakthrough pain incancer patients admitted to a hospice. J Pain Symp-tom Manage 2000;20:87e92.
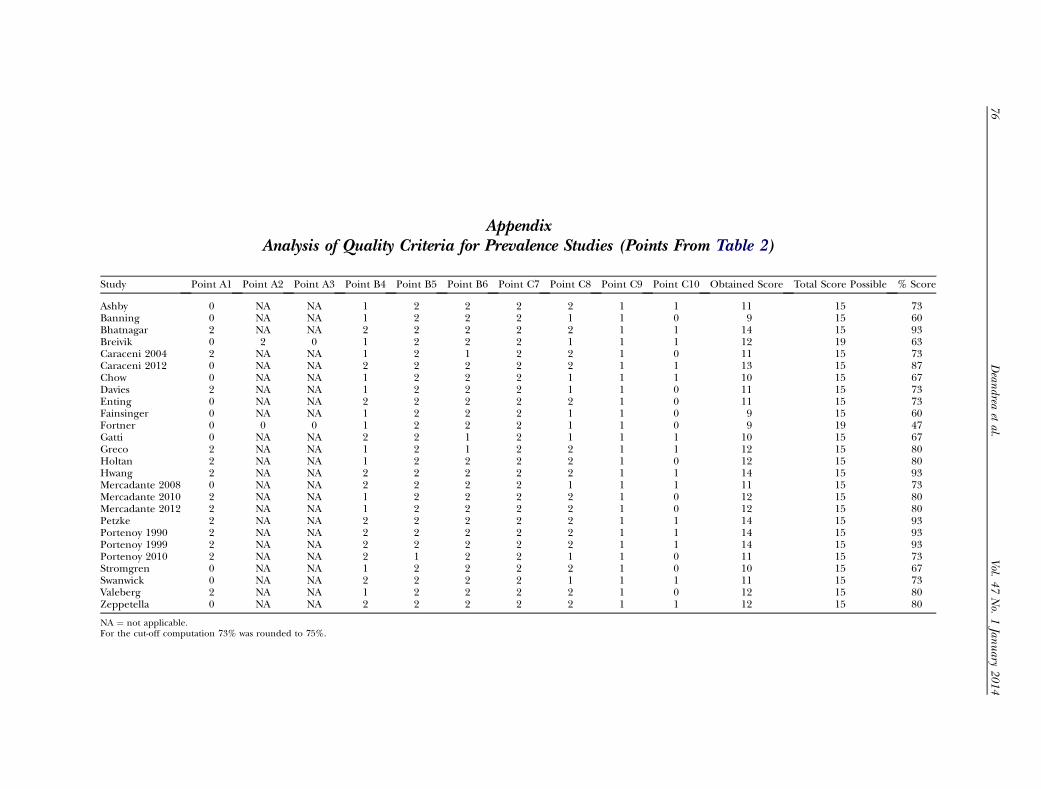
AppendixAnalysis of Quality Criteria for Prevalence Studies (Points From Table 2)
Study Point A1 Point A2 Point A3 Point B4 Point B5 Point B6 Point C7 Point C8 Point C9 Point C10 Obtained Score Total Score Possible % Score
Ashby 0 NA NA 1 2 2 2 2 1 1 11 15 73Banning 0 NA NA 1 2 2 2 1 1 0 9 15 60Bhatnagar 2 NA NA 2 2 2 2 2 1 1 14 15 93Breivik 0 2 0 1 2 2 2 1 1 1 12 19 63Caraceni 2004 2 NA NA 1 2 1 2 2 1 0 11 15 73Caraceni 2012 0 NA NA 2 2 2 2 2 1 1 13 15 87Chow 0 NA NA 1 2 2 2 1 1 1 10 15 67Davies 2 NA NA 1 2 2 2 1 1 0 11 15 73Enting 0 NA NA 2 2 2 2 2 1 0 11 15 73Fainsinger 0 NA NA 1 2 2 2 1 1 0 9 15 60Fortner 0 0 0 1 2 2 2 1 1 0 9 19 47Gatti 0 NA NA 2 2 1 2 1 1 1 10 15 67Greco 2 NA NA 1 2 1 2 2 1 1 12 15 80Holtan 2 NA NA 1 2 2 2 2 1 0 12 15 80Hwang 2 NA NA 2 2 2 2 2 1 1 14 15 93Mercadante 2008 0 NA NA 2 2 2 2 1 1 1 11 15 73Mercadante 2010 2 NA NA 1 2 2 2 2 1 0 12 15 80Mercadante 2012 2 NA NA 1 2 2 2 2 1 0 12 15 80Petzke 2 NA NA 2 2 2 2 2 1 1 14 15 93Portenoy 1990 2 NA NA 2 2 2 2 2 1 1 14 15 93Portenoy 1999 2 NA NA 2 2 2 2 2 1 1 14 15 93Portenoy 2010 2 NA NA 2 1 2 2 1 1 0 11 15 73Stromgren 0 NA NA 1 2 2 2 2 1 0 10 15 67Swanwick 0 NA NA 2 2 2 2 1 1 1 11 15 73Valeberg 2 NA NA 1 2 2 2 2 1 0 12 15 80Zeppetella 0 NA NA 2 2 2 2 2 1 1 12 15 80
NA ¼ not applicable.For the cut-off computation 73% was rounded to 75%.
76
Vol.
47No.
1Jan
uary
2014
Dean
dreaetal.




























