Embed Size (px)
Citation preview

Archives of Disease in Childhood 1994; 71: 433-436
Prevalence of cardiovascular malformations andassociation with karyotypes in Turner's syndrome
C-O G0tzsche, B Krag-Olsen, J Nielsen, K E S0rensen, B 0 Kristensen
AbstractThe aim of the study was to establish theprevalence of cardiovascular malforma-tions in females with Turner's syndromeand analyse possible associations withthe various karyotypes. One hundredand seventy nine of 393 females whohad Turner's syndrome diagnosed inDenmark were examined. Completechromosome analysis was available inall cases. Clinical examination, electro-cardiography, and echocardiographyincluding Doppler were performed.The distribution of the various karyo-
types was 45,X, 58%; mosaic monosomyX, 35%/o; and structural abnormalities ofthe X chromosome, 7%. In 46 (26%) ofthefemales a total of 69 cardiovascularmalformations were found; aortic valveabnormality (18%) and aortic coarctation(10%) being the most common. There wasa significant difference in the prevalenceof cardiovascular malformations between45,X and mosaic monosomy X (38% v11%), primarily due to a significant differ-ence in the prevalence of aortic valveabnormalities and aortic coarctation.Pulmonary valve abnormalities were seenonly in females with mosaic monosomyX but the prevalence was low (3%). Nopatient with structural abnormalities ofthe X chromosome had cardiovascularmalformations.(Arch Dis Child 1994; 71: 433-436)
Aarhus UniversityHospital, Departnentof Cardiology, Skejby,DK-8200 Arhus N,DenmarkC-O GotzscheK E SorensenB 0 Kristensen
The Turner Centerand CytogeneticLaboratory, Instituteof Biological.Psychiatry, ArhusPsychiatric Hospital,DenmarkB Krag-OlsenJ Nielsen
Correspondence to:Dr Kristensen.
Accepted 17 August 1994
Turner's syndrome is a genetic abnormality infemales and the karyotype can be monosomyX (45,X), mosaic monosomy X, or a structuralabnormality of the X chronosome. Thesyndrome is characterised by shdrt stature andgonadal dysgenesis, and is associated with a
number of congenital abnormalities includingcardiovascular malformations. In publishedseries of Turner's syndrome the percentage ofthose with cardiovascular malformations hasranged from 17% to 47%; aortic coarctationand bicuspid aortic valve being the mostcommon lesions. 1-3 However, these studieshave all been relatively small hospital basedseries from departments of paediatrics, cardio-logy, or endocrinology. Due to possible selec-tion bias, these data may not truly reflect theprevalence of cardiovascular malformations inTurner's syndrome.An association of aortic valve disease and
aortic coarctation with 45,X karyotype andpulmonary stenosis with mosaic monosomy Xhas previously been suggested,4 but prevalencestudies are not available.
Since 1963, all females with Turner's syn-drome diagnosed in Denmark have been listedin the Danish National Cytogenetic Register.The presence of this register made it possiblefor us to examine a large and relativelyunselected group of females with Turner's syn-drome. The introduction of echocardiographywith the application of Doppler techniques hasmade non-invasive detection of cardiovascularmalformations possible, including identifica-tion of minor cardiac lesions that may other-wise remain asymptomatic for years. Dopplerultrasonographic modalities have not beenused in previous studies of females withTurner's syndrome.The purpose of our study was to establish
the prevalence of cardiovascular malforma-tions and investigate any possible associationsbetween the various genotypes and cardio-vascular malformations.
Patients and methodsIn March 1988, 393 females with Turner'ssyndrome were registered in the DanishNational Cytogenetic Register. We were ableto obtain contact with 223 through directcontact, through the family doctor, or throughthe National Association of Turner ContactGroups, and 179 agreed to participate. Themean age of the females examined was 23 years(range 6 months to 46 years). Results fromchromosome analysis were available in all.
In each case a history was taken concerningcardiovascular symptoms and former opera-tions. Clinical examination, electrocardio-graphy, and echocardiography were performedby a cardiologist blinded to the specifickaryotype.
Echocardiography including Doppler studieswas performed using a Toshiba 60 or 65A.Pulsed and continuous wave Doppler as well ascolour flow mapping was performed with a2-5 MHz transducer. The echocardiographyincluded standard M mode measurements andtwo dimensional evaluation from all standardplanes. Flow velocities across the aortic, mitral,pulmonary, and tricuspid valve as well as in theascending and descending thoracic aorta wereobtained using pulsed and continuousDoppler modalities.5 All echocardiograms wererecorded on videotape and later reviewedblindly by another cardiologist. The diagnosisof bicuspid aortic valve and mitral valveprolapse followed standard criteria.2 6The x2 test with the Yates's correction and
Fisher's exact test were used in comparisonbetween the 45,X group and the mosiacmonosomy X group; p<0 05 was consideredsignificant.
433
group.bmj.com on October 27, 2014 - Published by http://adc.bmj.com/Downloaded from
Gotzsche, Krag-Olsen, Nielsen, Sorensen, Kristensen
45,X
45,X/46,XX45,X/46,X,r(X)45,X/46,X,i(Xq)45,X146,XY45,X146,X+mar45,X147,XXX45,X/46,X,dic(Xq)45,X/46,X,i(Xq)/47,X,i(Xq),i(Xq)45,X146,X,del(X)(pl 1)45,X/46,X,del(X)(ql 1)45,X/46,X,i(Yp)45,X146,X,dic(X;X)(p22;p22)45,X146,Xinv(X)(p22;q24)45,X/46,X,i(Xq)/46,X,r(X)46,XX/46,X,i(Xq)
46,XX,i(Xq)46,X,del(X)(pl 1)46,X,del(X)(q25)46,X,del(X)(ql3)46,X,+mar46,X,dic(X;X)(p2 l;p21)
The study was approved by the local ethicalcommittee for medical science.
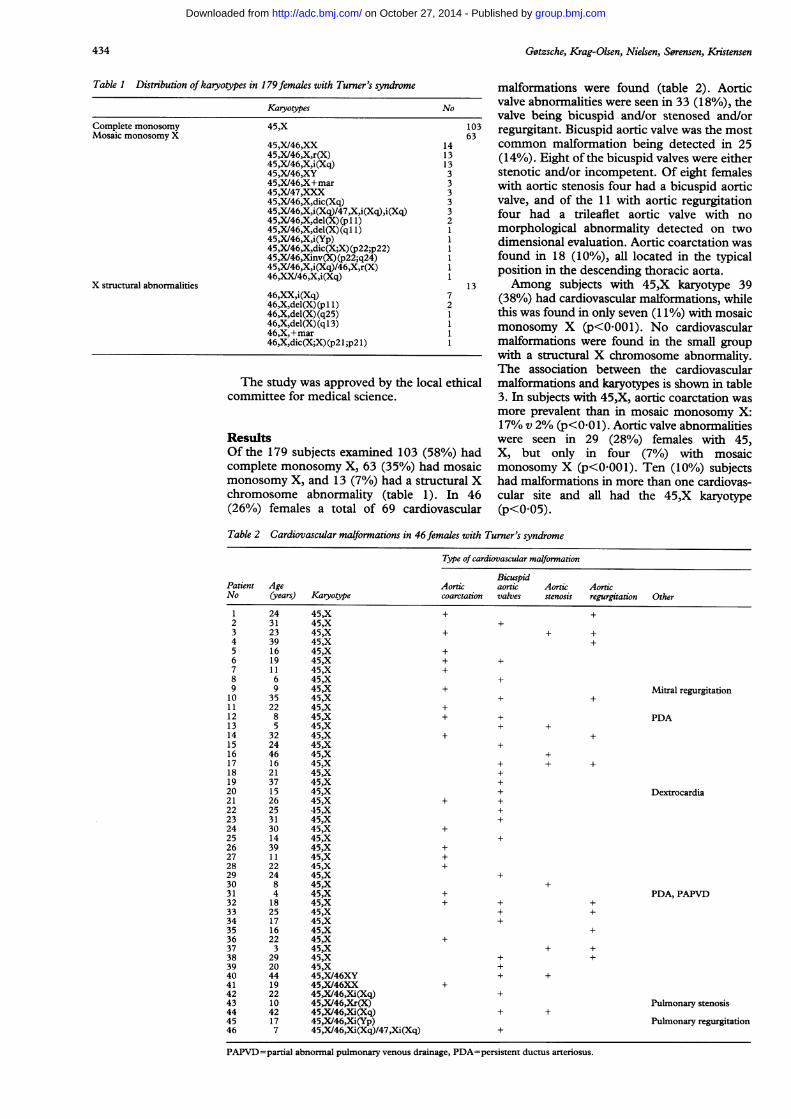
ResultsOf the 179 subjects examined 103 (58%) hadcomplete monosomy X, 63 (35%) had mosaicmonosomy X, and 13 (7%) had a structural Xchromosome abnormality (table 1). In 46(26%) females a total of 69 cardiovascular
malformations were found (table 2). Aorticvalve abnormalities were seen in 33 (18%), thevalve being bicuspid and/or stenosed and/orregurgitant. Bicuspid aortic valve was the mostcommon malformation being detected in 25(14%). Eight of the bicuspid valves were eitherstenotic and/or incompetent. Of eight femaleswith aortic stenosis four had a bicuspid aorticvalve, and of the 11 with aortic regurgitationfour had a trileaflet aortic valve with nomorphological abnormality detected on twodimensional evaluation. Aortic coarctation wasfound in 18 (10%), all located in the typicalposition in the descending thoracic aorta.Among subjects with 45,X karyotype 39
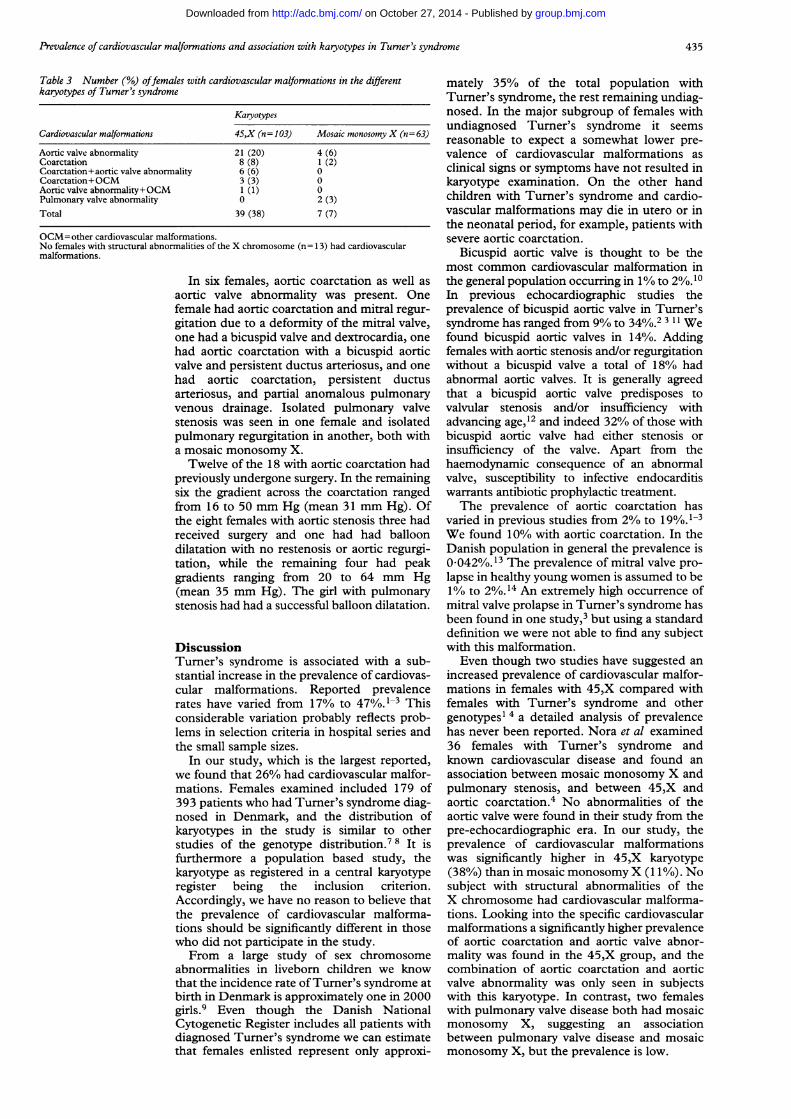
(38%) had cardiovascular malformations, whilethis was found in only seven (11%) with mosaicmonosomy X (p<00 01). No cardiovascularmalformations were found in the small groupwith a structural X chromosome abnormality.The association between the cardiovascularmalformations and karyotypes is shown in table3. In subjects with 45,X, aortic coarctation wasmore prevalent than in mosaic monosomy X:17% v 2% (p<0 01). Aortic valve abnormalitieswere seen in 29 (28%) females with 45,X, but only in four (7%) with mosaicmonosomy X (p<0001). Ten (10%) subjectshad malformations in more than one cardiovas-cular site and all had the 45,X karyotype(p<0 05).
Table 2 Cardiovascular malformations in 46 females with Turner's syndrome
Type ofcardiovascular malformation
BicuspidPatient Age Aortic aortic Aortic AorticNo (years) Karyotype coarctation valves stenosis regurgitation Other
1 24 45,X + +2 31 45,X +3 23 45,X + + +4 39 45,X +5 16 45,X +6 19 45,X + +7 11 45,X +8 6 45,X +9 9 45,X + Mitral regurgitation10 35 45,X + +11 22 45,X +12 8 45,X + + PDA13 5 45,X + +14 32 45,X + +15 24 45,X +16 46 45,X +17 16 45,X + + +18 21 45,X +19 37 45,X +20 15 45,X + Dextrocardia21 26 45,X + +22 25 45,X +23 31 45,X +24 30 45,X +25 14 45,X +26 39 45,X +27 11 45,X +28 22 45,X +29 24 45,X +30 8 45,X +31 4 45,X + PDA, PAPVD32 18 45,X + + +33 25 45,X + +34 17 45,X +35 16 45,X +36 22 45,X +37 3 45,X + +38 29 45,X + +39 20 45,X +40 44 45,X/46XY + +41 19 45,X/46XX +42 22 45,X146,Xi(Xq) +43 10 45,X/46,Xr(X) Pulmonary stenosis44 42 45,X/46,Xi(Xq) + +45 17 45,X/46,Xi(Yp) Pulmonary regurgitation46 7 45,X/46,Xi(Xq)/47,Xi(Xq) +
PAPVD=partial abnormal pulmonary venous drainage, PDA-persistent ductus arteriosus.
Table 1 Distribution ofkaryotypes in 179females with Turner's syndrome
Karvotypes
Complete monosomyMosaic monosomy X
X structural abnormalities
434
group.bmj.com on October 27, 2014 - Published by http://adc.bmj.com/Downloaded from
Prevalence of cardiovascular malformations and association with karyotypes in Turner's syndrome
Table 3 Number (%o) offemales with cardiovascular malformations in the differentkaryotypes of Turner's syndrome
Karyotypes
Cardiovascular malformations 45,X (n= 103) Mosaic monosomny X (n= 63)
Aortic valve abnormality 21 (20) 4 (6)Coarctation 8 (8) 1 (2)Coarctation+aortic valve abnormality 6 (6) 0Coarctation+OCM 3 (3) 0Aortic valve abnormality+OCM 1 (1) 0Pulmonary valve abnormality 0 2 (3)Total 39 (38) 7 (7)
OCM=other cardiovascular malformations.No females with structural abnormalities of the X chromosome (n= 13) had cardiovascularmalformations.
In six females, aortic coarctation as well asaortic valve abnormality was present. Onefemale had aortic coarctation and mitral regur-gitation due to a deformity of the mitral valve,one had a bicuspid valve and dextrocardia, onehad aortic coarctation with a bicuspid aorticvalve and persistent ductus arteriosus, and onehad aortic coarctation, persistent ductusarteriosus, and partial anomalous pulmonaryvenous drainage. Isolated pulmonary valvestenosis was seen in one female and isolatedpulmonary regurgitation in another, both witha mosaic monosomy X.Twelve of the 18 with aortic coarctation had
previously undergone surgery. In the remainingsix the gradient across the coarctation rangedfrom 16 to 50 mm Hg (mean 31 mm Hg). Ofthe eight females with aortic stenosis three hadreceived surgery and one had had balloondilatation with no restenosis or aortic regurgi-tation, while the remaining four had peakgradients ranging from 20 to 64 mm Hg(mean 35 mm Hg). The girl with pulmonarystenosis had had a successful balloon dilatation.
DiscussionTurner's syndrome is associated with a sub-stantial increase in the prevalence of cardiovas-cular malformations. Reported prevalencerates have varied from 17% to 470/o.l-3 Thisconsiderable variation probably reflects prob-lems in selection criteria in hospital series andthe small sample sizes.
In our study, which is the largest reported,we found that 26% had cardiovascular malfor-mations. Females examined included 179 of393 patients who had Turner's syndrome diag-nosed in Denmark, and the distribution ofkaryotypes in the study is similar to otherstudies of the genotype distribution.7 8 It isfurthermore a population based study, thekaryotype as registered in a central karyotyperegister being the inclusion criterion.Accordingly, we have no reason to believe thatthe prevalence of cardiovascular malforma-tions should be significantly different in thosewho did not participate in the study.From a large study of sex chromosome
abnormalities in liveborn children we knowthat the incidence rate ofTurner's syndrome atbirth in Denmark is approximately one in 2000girls.9 Even though the Danish NationalCytogenetic Register includes all patients withdiagnosed Turner's syndrome we can estimatethat females enlisted represent only approxi-
mately 35% of the total population withTurner's syndrome, the rest remaining undiag-nosed. In the major subgroup of females withundiagnosed Turner's syndrome it seemsreasonable to expect a somewhat lower pre-valence of cardiovascular malformations asclinical signs or symptoms have not resulted inkaryotype examination. On the other handchildren with Turner's syndrome and cardio-vascular malformations may die in utero or inthe neonatal period, for example, patients withsevere aortic coarctation.
Bicuspid aortic valve is thought to be themost common cardiovascular malformation inthe general population occurring in l% to 2%.10In previous echocardiographic studies theprevalence of bicuspid aortic valve in Turner'ssyndrome has ranged from 9% to 34%.2 3 11 Wefound bicuspid aortic valves in 14%. Addingfemales with aortic stenosis and/or regurgitationwithout a bicuspid valve a total of 18% hadabnormal aortic valves. It is generally agreedthat a bicuspid aortic valve predisposes tovalvular stenosis and/or insufficiency withadvancing age,'2 and indeed 32% of those withbicuspid aortic valve had either stenosis orinsufficiency of the valve. Apart from thehaemodynamic consequence of an abnormalvalve, susceptibility to infective endocarditiswarrants antibiotic prophylactic treatment.The prevalence of aortic coarctation has
varied in previous studies from 2% to 19%.1-3We found 10% with aortic coarctation. In theDanish population in general the prevalence is0.042%./13 The prevalence of mitral valve pro-lapse in healthy young women is assumed to be1% to 2%.14 An extremely high occurrence ofmitral valve prolapse in Turner's syndrome hasbeen found in one study,3 but using a standarddefinition we were not able to find any subjectwith this malformation.Even though two studies have suggested an
increased prevalence of cardiovascular malfor-mations in females with 45,X compared withfemales with Turner's syndrome and othergenotypesl 4 a detailed analysis of prevalencehas never been reported. Nora et al examined36 females with Turner's syndrome andknown cardiovascular disease and found anassociation between mosaic monosomy X andpulmonary stenosis, and between 45,X andaortic coarctation.4 No abnormalities of theaortic valve were found in their study from thepre-echocardiographic era. In our study, theprevalence of cardiovascular malformationswas significantly higher in 45,X karyotype(38%) than in mosaic monosomy X (1 1%). Nosubject with structural abnormalities of theX chromosome had cardiovascular malforma-tions. Looking into the specific cardiovascularmalformations a significantly higher prevalenceof aortic coarctation and aortic valve abnor-mality was found in the 45,X group, and thecombination of aortic coarctation and aorticvalve abnormality was only seen in subjectswith this karyotype. In contrast, two femaleswith pulmonary valve disease both had mosaicmonosomy X, suggesting an associationbetween pulmonary valve disease and mosaicmonosomy X, but the prevalence is low.
435
group.bmj.com on October 27, 2014 - Published by http://adc.bmj.com/Downloaded from

Gotzsche, Krag-Olsen, Nielsen, Sorensen, Kristensen
In a selected group of females with Turner'ssyndrome, Price et al found a reduction in lifeexpectancy, particularly because of death dueto cardiovascular malformations.'5 Further-more, a few young women with Turner's syn-drome and no evidence of cardiovasculardisease who died from dissection of the aortahave been reported.16 This may indicate anassociation between Turner's syndrome andweakness of the aortic wall. We conclude thatTurner's syndrome is associated with a sub-stantial increase in the prevalence of cardiovas-cular malformations primarily related to the45,X karyotype. Aortic valve disease and aorticcoarctation are the most common malforma-tions and they are significantly more frequentin 45,X karyotype. Because of the therapeuticand prophylactic implications we recom-mend a cardiological examination includingDoppler echocardiography in all females withTurner's syndrome, once the diagnosis isestablished.The study was supported by a grant from the Danish HeartFoundation. We are also grateful to members of the NationalAssociation of Turner Contact Groups who assisted in thestudy.
1 Rainer-Pope CR, Cunningham RD, Nadas AS, Crigler JF.Cardiovascular malformations in Turner's syndrome.Pediatnics 1964; 19: 919-25.
2 Mazzanti L, Prandstaller D, Tassinara D, et al. Heart
disease in Turner's syndrome. Helv Paediatr Acta 1988;43: 25-31.
3 Bastianon V, Pasquino AM, Giglioni E, et al. Mitral valveprolapse in Turner syndrome. Eur J Pediatr 1989; 148:533-4.
4 Nora JJ, Torres FG, Sinha AK, McNamara DG.Characteristic cardiovascular anomalies of XO Turnersyndrome, XX and XY phenotype and XO/XX Turnermosaic. Am J Cardiol 1970; 25: 639-41.
5 Goldberg SJ, Allen HD, Marx GR, Donnerstein RL.Doppler echocardiography. 2nd Ed. Philadelphia: Lea andFebiger, 1988.
6 Perloff JK, Child JS, Edwards JE. New guidelines for theclinical diagnosis of mitral valve prolapse. Am Jf Cardiol1986; 57: 1124-9.
7 Palmer CG, Reichmann A. Chromosomal and clinical find-ings in 110 females with Tumer syndrome. Hum Genet1976; 35: 35-49.
8 Hall JG, Gilchrist DM. Tumer syndrome and its variants.Pediat Clin North Am 1990; 37: 1421-40.
9 Nielsen J, Wohlert M. Sex chromosome abnormalitiesfound among 34 910 newborn children: results from a 13-year incidence study in Arhus, Denmark. Birth Defects1991; 26: 209-23.
10 Roberts WC. The congenitally bicuspid aortic valve. Astudy of 85 autopsy cases. Am Jf Cardiol 1970; 26: 72-83.
11 Miller MJ, Geffner ME, Lippe BM, et al. Echocardiographyreveals a high incidence of bicuspid aortic valve in Turnersyndrome. JPediatr 1983; 102: 47-50.
12 Braunwald E. Valvular heart disease. In: Brunwald W, ed.Heart disease. A textbook ofcardiovascular medicine. 4th Ed.Philadelphia: WB Saunders, 1992: 1035.
13 Bzkgaard-Laursen H. Congenital heart disease inDenmark. 1963-73. An epidemiological investigation.[Thesis.] Copenhagen: FADL's forlag, 1979.
14 Wann LS, Grove JR, Hess TR, et al. Prevalence of mitralprolapse by two dimensional echocardiography in healthyyoung women. Br HeartJ7 1983; 49: 334-40.
15 Price WH, Clayton JF, Collyer S, deMey R, Wilson J.Mortality ratios, life expectancy, and causes of death inpatients with Turner's syndrome. J Epidemiol CommunityHealth 1986; 40: 97-102.
16 Price WH, Wilson J. Dissection of the aorta in Turner'ssyndrome. JMed Genet 1983; 20: 61-3.
436
group.bmj.com on October 27, 2014 - Published by http://adc.bmj.com/Downloaded from
syndrome.and association with karyotypes in Turner's Prevalence of cardiovascular malformations
KristensenC O Gøtzsche, B Krag-Olsen, J Nielsen, K E Sørensen and B O
doi: 10.1136/adc.71.5.4331994 71: 433-436 Arch Dis Child
http://adc.bmj.com/content/71/5/433Updated information and services can be found at:
serviceEmail alerting
box at the top right corner of the online article. Receive free email alerts when new articles cite this article. Sign up in the
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on October 27, 2014 - Published by http://adc.bmj.com/Downloaded from