Embed Size (px)
DESCRIPTION
Prevention of Venous Thromboembolism (VTE) Andrew Nicolaides Emeritus Professor of Vascular Surgery Imperial College, London UK. VTE mortality per year in 25 EU countries. Deaths due to VTE : 543,454 1 More than double the combined deaths due to: AIDS 5,860 2 - PowerPoint PPT Presentation
Citation preview

1
Prevention of Venous Thromboembolism (VTE)
Andrew Nicolaides
Emeritus Professor of Vascular Surgery
Imperial College, London UK

2
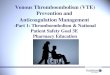
VTE mortality per year in 25 EU countries
1Cohen AT. Presented at the 5th Annual Congress of the European Federation of Internal Medicine; 2005.2Eurostat statistics on health and safety 2001. Available from: http://epp.eurostat.cec.eu.int.
Deaths due to VTE : 543,4541 More than double the combined deaths
due to: AIDS 5,8602
breast cancer 86,8312
prostate cancer 63,6362
transport accidents 53,5992

3
Risk by Patient Group in the Absence of Prophylaxis
Patient group Studies DVT incidence 95% CI
Stroke 8 56% 51-61%
THR 17 51% 48-54%
Multiple trauma 4 50% 46-55%
TKR 7 47% 42-51%
Hip fracture 15 44% 40-47%
Spinal cord inj. 9 35% 31-39%
Retrop. prostatectomy 8 32% 27-37%
Patients in ICU 3 25% 19-32%
General Surgery 20 25% 24-26%
Neurosurgery 5 22% 17-27%
Gynecol. (malignancy) 4 22% 17-26%
Gynecol. Surgery 4 15% 11-17%
General medical 10 8.1% 7-9.1%
Knee arthroscopy 7 8% 6-10%
Nicolaides A et al Intern Angiol 2013 (In Press)

4
ENDORSE Survey
Multinational, cross-sectional survey of:
(a) prevalence of VTE risk and
(b) prophylaxis use in hospital

5
Patient Enrollment Criteria
Inclusion Criteria
Acute medical patients age 40 or older
Surgical patients age 18 or older
Exclusion Criteria
Admitted for treatment of VTE
Not evaluable because of missing data

6
Criteria for VTE Risk and Recommendations for Prophylaxis
2004 American College of Chest Physicians Recommendations1
Patients at risk and appropriate types of prophylaxis
1 Geerts WH, et al. Chest. 2004; 126 (Suppl 3):338S-400S

7
ENDORSE : A worldwide study
32 countries - 358 hospitals32 countries - 358 hospitalsFirst patient enrolled August 2, 2006Last patient enrolled January 4, 2007

8
Patients at risk for VTE in 32 countries
N= 68,183
0
10
20
30
40
50
60
70
80
90
100
%
Mean = 52%

9
Patients at risk for VTE receiving recommended prophylaxis in 32 countries
0
10
20
30
40
50
60
70
80
90
100
Algeria
Austra
lia
Bangla
desh
Brazil
Bulgar
ia
Colombia
Czech
Rep
Egypt
Franc
e
Germ
any
Greec
e
Hungar
yIn
dia
Irelan
d
Kuwait
Mex
ico
Pakist
an
Poland
Portu
gal
Romania
Russia
Saudi
Arabia
Slovakia
Spain
Switzer
land
Thaila
nd
Tunisi
a
Turke
yUAE UK
USA
Venez
uela
%
Mean = 50%
N= 35,329

10
Surgical Patients at risk for VTE and receiving recommended prophylaxis
Primary objectives
52 % at Risk for VTE
50 % receiving ACCP
Rec. Px
Overall( N= 68,183 )
Secondary objectives
64 % at Risk for VTE
59 % receiving
ACCP Rec. Px
Surgical( n = 30,827 )
Medical( n = 37,356 )
42 % at Risk for VTE
40 % receiving
ACCP Rec. Px

11
Conclusions
ENDORSE demonstrates:
the high prevalence of patients at risk for VTE and
the need to improve the rate of prophylaxis use.

12
(a) Implement hospital-wide strategies
(b) Assess patient risk for VTE routinely
(c) Provide appropriate prophylaxis
(d) Educate the public to ask for prophylaxis when admitted to hospital
These data reinforce the rationale to :These data reinforce the rationale to :

13

14
The International Guidelines on Prevention of VTE (2013)

15
Developed under the auspices of the:
Cardiovascular Disease Educational and Research Trust (UK)European Venous ForumNorth American Thrombosis ForumInternational Union of Angiology andUnion Internationale du Phlebologie
PREVENTION AND TREATMENTPREVENTION AND TREATMENTOF VENOUS THROMBOEMBOLISMOF VENOUS THROMBOEMBOLISM
International Consensus Statement 2013Guidelines According to Scientific Evidence

16
Prevention and Treatment of Venous Thromboembolism Consensus Statement
Aim Provide a concise account of the evidence of efficacy or
harm for various methods available to prevent and treat venous thromboembolism (VTE)
Provide recommendations based on critical evaluation of the evidence

17
EDITORIAL COMMITTEE
Chairman: AN Nicolaides,
Cochairmen: J Fareed, AK Kakkar
Members: AJ Comerota, SZ Goldhaber, R Hull, K Myers, M Samama, J Fletcher
Editorial Secretary: E Kalodiki

18
Faculty
D Bergqvist (Sweden) J Bonnar (Ireland) JA Caprini (USA) C Carter (USA) AJ Comerota (USA) J Conard (France) B Eklof (Sweden) I Elalamy (France) J Fareed (USA) J Fletcher (Australia) G Gerotziafas (France) G Geroulakos (UK) A Giannoukas (Greece) SZ Goldhaber (USA) I Greer (UK) M Griffin (UK)
R Hull (USA) A K Kakkar (UK) S Kakkos (Greece) E Kalodiki (UK) MR Lassen (Denmark) GDO Lowe (UK) A Markel (Israel) K Myers (Australia) A Nicolaides (Cyprus) P Prandoni (Italy) G Raskob (USA) M Samama (France) AC Spyropoulos (USA) AG Turpie (Canada) JM Walenga (USA) D Warwick (UK)

19

20
Corresponding Faculty
C Allegra (Italy)
J Arcelus (Spain)
N Baekgaard (Denmark)
G Belcaro (Italy)
H Bjarnason (USA)
MA Cairols (Spain)
M Catalano (Italy)
D Christopoulos (Greece)
D Clement (Belgium)
F Corvalán (Chile)
E Diamantopoulos (Greece)
J Fernandes e Fernandes (Portugal)
C Fisher (Australia)
A Gasparis (USA)
H Gibbs (Australia)
V Hadjianastassiou (Cyprus)
K Ivancev (UK)
CP Hsien (Thaiwan)
JT Hobbs (UK)
D Hoppenstead (USA)
EA Hussein (Egypt)
O Iqbal (USA)
K Ivancev (Russia)
R Kistner (USA)
TK Kim (Korea)
M Kurtoglou (Turkey)
T Kölbel (Germany)
N Labropoulos (USA)
LH Lee (Singapore)
BB Lee (USA)
Y-J Li (China)
NC Liew (Malaysia)
A Llinas (Colombia)
M Nakamura (Japan)
P Neglen (Cyprus)
L Norgren (Sweden)
H Partsch (Austria)
N Ramakrishnan (India)
G Rao (USA)
J-B. Ricco (France)
N Rich (USA)
P Robless (Singapore)
W Schobersberger (Austria)
M Seed (UK)
S Schellong (Germany)
A Scuderi (Brazil)
R Sexana (India)
E Shaydakov (Russia)
A Shevela (Russia)
R Simkin (Argentina)
W Toff (UK)
JM Trabal (Puerto Rico)
M Vandendriessche (Belgium)
M Veller (South Africa)
L Villavincencio (USA)
R Wahi (USA)
C Wittens (TheNetherlands)
R Wong (Hong Kong)

21
Levels of Evidence
High level of evidence was considered to be provided by RCTs with consistent results, or
systematic reviews that were directly applicable to the target population
also, by single randomized trials which have been rigorously performed, methodologically reliable, and sufficiently large to give clear results that are applicable to most patients in most circumstances

22
Levels of Evidence
Moderate level of evidence was considered to be provided by RCT with less consistent results, limited power or other
methodological problems, which were directly applicable to the target population
Also, by RCT extrapolated to the target population from a different group of patients.

23
Levels of Evidence
Low level of evidence was considered to be provided by well-conducted observational studies with consistent results that
were directly applicable to the target population.
Lack of evidence ? Lack of evidence or low level evidence resulted in a number of key
questions that require to be addressed by future studies
These key questions are stated throughout the document and are summarised in the final section (Chapter 24).

24
Outcomes
Evidence is presented for the following outcomes asymptomatic DVT at screening
symptomatic DVT or PE,
fatal PE,
overall mortality and
development of the post-thrombotic syndrome (PTS) when available

25
Recommendations
Low risk patients (minor general surgery, no risk factors)
Graduated elastic compression
Avoid dehydration
Level of evidence (LE): low (extrapolation from moderate risk)

26
Effect of GEC (8 studies: moderate risk general surgery)
0
5
10
15
20
25
DVT (%)
Control (n=637) GEC (n=653)
Groups
68% Reduction in DVT Incidence
p < 0.001

27
Effect of LDUH: 32 Studies in General Surgery
0
5
10
15
20
25
DVT (%)
Control (n=2567) LDUH (n=2655)
Groups
68% Reduction in DVT Incidence
p < 0.001

28
LMWH vs Placebo in General Surgery (1 study)
0
2
4
6
8
10
12
14
16
DVT (%)
Placebo (n = 91) LMWH (n = 92)
74% Reduction in DVT Incidence
p < 0.025

29
LMWH vs LDUH in General Surgery (17 Studies)
0
1
2
3
4
5
6
7
DVT (%)
LDUH (n = 3411) LMWH (n = 3467)
21% Reduction in DVT Incidence
p < 0.025

30
LMWH vs LDUH in General Surgery (14 Studies)
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
PE (%)
LDUH (n = 2644) LMWH (n = 2798)
56% Reduction in PE Incidence
p < 0.001

31
LMWH vs LDUH in General Surgery
LMWH
is more effective in preventing PE
has a lower risk of HIT than LDUH
requires one injection per day

32
Effect of IPC in General Surgery (11 studies)
0
5
10
15
20
25
30
DVT (%)
Control (n = 658) IPC (n=660)
69% Reduction in DVT Incidence
p < 0.001

33
Recommendations
Moderate risk patients (major general surgery, age >40, no additional risk factors)
(LDUH) or LMWH LE: high
IPC + GEC LE: high

34
Fondaparinux (Arixtra)
Dalteparin
% V
TE
Relative Risk Reduction= 25%
p = 0.14
6.1%4.6%
0
1
2
3
4
5
6
7
Fondaparinux (Arixtra) in prevention of VTE in General Surgery (n= 2858)
47/1027
62/1021
British Journal of Surgery 2005, G Agnelli et al

35
Relative Risk Reduction= 39% (95 %CI : 59.6; 6.7%)
p = 0.02
55/712
9
Fondaparinux (ARIXTRA)
Dalteparin0
1
2
3
4
5
6
7
8
7.7%
4.7%
33/696
% V
TE
Cancer Surgery (n= 1941)
British Journal of Surgery 2005, G Agnelli et al

36
Recommendations
High risk patients (major general surgery, age > 60 or age > 40 with at least one additional risk factor)
(LDUH) LMWH LE: high
IPC + GEC LE: high
Fondaparinux (one study) LE: moderate
IPC + GEC with LMWH LE: high

37
Orthopedics

38
Efficacy in Elective Hip Replacement(Historical progression)
Control vs LDUH 50% reduction in DVT (20 sudies)
Control vs IPC 52% reduction in DVT (4 studies)
LDUH vs LMWH 54% further red. in DVT (10 studies)
LMWH vs Fondaparinux 24% further red. In DVT (2 studies)
50% further red. In PE (2 studies)
LMWH vs LMWH+IPC 28% vs 0% DVT (1 study)

39
Fondaparinuxbetter
Enoxaparin better
Homogeneity test: ns
95% CI
-100 -80 -60 -40 -20 200 40 60 80 100
Hip replacementn=3,411 (2 studies)
-45.3% [-58.9; -27.4]
Knee replacementn=724 -63.1% [-75.5; -
44.8]
Hip fracturen=1,250 [-73.4; -
45.0]-61.6%
Overall odds reduction -55.2% [-63.1; -
45.8]p=10-17
Odds reduction (%)
Efficacy of Fondaparinux vs Enoxaparin
Turpie et al. Arch Intern Med 2002;162:1833-40

40
New Oral Anticoagulants

41
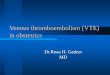
Figure 1: Site of Actions for Conventional and Newer Oral AnticoagulantsSite of Actions for Conventional and Newer Oral Anticoagulants
Antithrombin
Fibrinogen
Factor II(Prothrombin)
Fibrin
Factor IIa(Thrombin)
Factor X
Factor IX Factor VII
Anti-Xa drugs
Anti-IIa drugs
Factor Xa
Dabigatran
ApixabanBetrixabanEdoxabanRivaroxaban
VKA drugs
Warfarin
FVIIa
FIXa

42

43
Recommendationsfor Elective Hip Replacement (2013)
Fondaparinux LE: high (Most effective)
LMWH LE: high
IPC + GEC LE: high (Equivalent to LMWH)
IPC+GEC+LMWH LE: high (More effective than either)
Rivaroxaban, Dabigatran LE: high
Initiation
LMWH: before or after operation LE: high
Fondaparinux: at least 6 hours after operation

44
Recommendations
Neurosurgery
IPC + GEC LE: High
Acutely ill medical patients
(LDUH) or LMWH LE: High
IPC + GEC LE: Moderate
Fondaparinux LE: Moderate

45
Duration of thromboprophylaxis
Total hip replacement patients (Hull et al1)
‒ 4-5 weeks vs 1-2 weeks LMWH – 64% RRR for symptomatic VTE
Cancer surgery (ENOXACAN II) 2
‒ 4 weeks vs 1 week LMWH – 60% RRR for VTE
Major abdominal surgery (Rasmussen et al3)
‒ 4 weeks vs 1 week LMWH – 55% RRR for VTE
Medical patients ?
1 Hull RD, et al. Ann Intern Med. 2001; 135:858-69.2 Bergqvist D, et al. NEJM. 2002; 346:975-980. 3 Rasmussen MS, et al. J Thromb Haemost. 2006; 4:2384-2390.

46 46
Study design Multicenter, Prospective, Randomized, Double-blind, Placebo-controlled study
to demonstrate superiority of enoxaparin 40 mg sc qd for 28 days + 4 days compared
with placebo both following 10 + 4 days of initial treatment with enoxaparin 40 mg sc qd
10 + 4
Mandatory ultrasonography
0
R
Enoxaparin 40 mg sc od
Placebo
38 ± 4Day
Follow-up
Enoxaparin40 mg sc od
Open-label Double-blind
180 ± 10
qd = once a day, SC = subcutaneous

47
Enrolment per country
Belgium0.6%
Argentina0.5%
Austria0.3%
Israel1.1%
India2.2%
Brazil1.6%
Tunisia2.6%
Italy2.7%
Colombia2.8%
Russia3.1%
Spain3.7%
Poland4.0%
Canada4.1%
Australia/NZ4.6%
U.K.6.5%
Germany7.4%
South Africa7.5%
Mexico7.9%
France8.7%
USA28.2%

48
Baseline: Primary enrolment diagnosis
Primary Primary enrollmentenrollment diagnosis diagnosis (%)(%)
Enoxaparin N = 2013
PlaceboN = 2027
Acute infection
Acute respiratory insufficiency
Heart failure
Acute ischemic stroke
Acute rheumatic disorder
Active cancer
Fractures (non surgical)
Active episode of infl. bowel disease
Multiple diagnosis
Other
30.5
26.6
21.2
8.3
2.7
2.3
1.0
0.2
0.9
6.3
31.0
27.6
21.5
7.8
2.8
2.1
0.8
0.1
0.4
5.8

49
Efficacy – all VTE until Day 90
Day 38 Day 90
Inci
den
ce (
%)
4.9
2.8
5.2
3.0
p = 0.0011 p = 0.0115
- 44%
RRR- 42%
RRR
Placebo
Enoxaparin

50
Safety – Bleeding
p = 0.007 p = 0.019
p = 0.024
Inci
den
ce
(%
)
3.80
5.70
0.150.60
5.20
3.70
Total Bleeding Major Bleeding Minor Bleeding
Placebo
Enoxaparin

51
Conclusions
Extended-duration prophylaxis reduced the rate of VTE by 44%
This benefit was for proximal DVT and symptomatic VTE, reducing the rate by 34% and 73%, respectively
The overall rate of major bleeding was higher in the active treatment arm.
The benefit of extended-duration prophylaxis translates in a NNT to avoid one VTE of 46, versus a NNT to cause major bleeding of 224

52
Combined Modalities

53
IPC + Heparin vs IPC or Anticoagulant alone (DVT) (14 Studies)
Combined IPC or Anticoag.
TOTAL 63/3074 200/3238
2.05% 6.18% p < 0.001
OR 0.31 (95% CI 0.23 to 0.43) or 69% reduction
Kakkos S et al Cochrane Database Syst Rev 2008:CD005258

54
IPC + Heparin vs IPC or Anticoagulant (Symptomatic PE) ( 16 Studies)
Combined IPC or Anticoag.
TOTAL 33/3838 122/4313
0.86% 2.83% p < 0.001
OR 0.34 (95% CI 0.23 to 0.50) or 67% reduction
Kakkos S et al Cochrane Database Syst Rev 2008:CD005258

55
Conclusion
Compared to single modalities, combined
prophylactic modalities significantly decrease the
incidence of both postoperative DVT and PE in a
variety of specialties, including orthopedic, general
and cardiac surgery.
The results support their use, especially in high risk
patients (e.g. thrombophilia or previous VTE)