Embed Size (px)
Citation preview
7/12/2014
1
Be sure to convert to your own time zone at www.worldhealthwebinars.com.au
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Ankle Injury Management and Rehabilitation
Presented by: Paul Hermann
Andrew Ellis BSc (Ex. Sci), M. Phty
Paul Hermann B.Sc.(Cli.Sc.), M.H.Sc.(Osteo), M.Ex.Sc(S&C), Member AOA
Ankle
Injury Management and Rehabilitation
Paul Hermann
Osteopath & Exercise Scientist B.Sc.(Clin.Sc), M.H.Sc.(Osteo), M.H.Sc.(S&C)
7/12/2014
2
What we will cover today… 1. Some epidemiology of ankle injuries and what commonly presents in
clinic
2. Structuring a stage based approach to ankle rehabilitation
3. Identifying and addressing imbalances that may have predisposed
patient to injury and/or increase potential for re injury
4. Restoring patient specific function
Ankle Injury Incidence
• In Australian Sport - 16% of all injuries with less than 20% of those being a primarily medial injury
• In AFL 2013 - 3.7 new injuries per club last year (compared to 2.6 in 2012) causing 12.1 games missed per club (10.5 in 2012)
• Anecdotally in clinic it seems recurrence is high
22nd Annual Australian Football League Injury Report 2013
The Western Australian Sports Injury Study, Stevenson et al, 2001 (Deakin University)
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
What do we want to know?? This may be very important for late stage rehab and for injury recurrence prevention • History of the injury:
• Site of pain • Onset • Mechanism of Injury - very important
• Inversion injury? • Eversion injury? • Forced Dorsiflexion with rotation - ? injury to syndesmosis • Compressive forces involved - ? osteochondral injury
• Previous History of injury
• Contact vs non contact injury • Direction of forces involved • Speed or degree of impact
What do we want to know??
• When did injury occur? • Gradual or acute onset? • Aggravation of pre - existing condition? • Was something heard or felt? • Associated sounds or sensations? • Pops, cracks, buckling, giving way……? • Localised injury site versus generalised area • What are the pain characteristics? • What is the behaviour of the symptoms?
What do we want to know??
• What is the level of irritability? • Etiological factors and biomechanical
considerations: • Training surface, training regime and changes
made to it • What footwear was being worn? • Equipment used? • Requirements of competition……? • Training stage/period
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
GAIT
• Step length
• Weight bearing
• Pain - if present where and when? What exactly reproduces it?
• Range of motion during gait
• Balance
• Alterations in foot posture
• Try different gait styles
7/12/2014
3
EXAMINATIONS
• Active/Passive Movements: • Plantarflexion / dorsiflexion
• Inversion / Eversion
• Resisted Movements: • Eversion – if possible (in acute ankle injuries
resisted movements may not be possible)
• In cases of persistent pain following ankle injury, weakness of the peroneal muscles should be assessed
EXAMINATIONS
• Functional Tests: • Lunge test
• Single leg standing balance - knee locked and unlocked -what reacts?
• Standing leg swings – results may surprise you
• Hopping - if appropriate
PALPATION • Distal fibula
• Lateral malleolus
• Lateral ligaments
• Talus
• Peroneal tendon(s)
• Base of 5th metatarsal
• Dome of talus
• Medial ligament
• Sustentaculum tali
• Sinus tarsi
• Anteroinferior tibiofibular ligament (AITFL)
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
SPECIAL TESTS
• Anterior Draw:
• Lateral talar tilt:
• Balance/Proprioception:
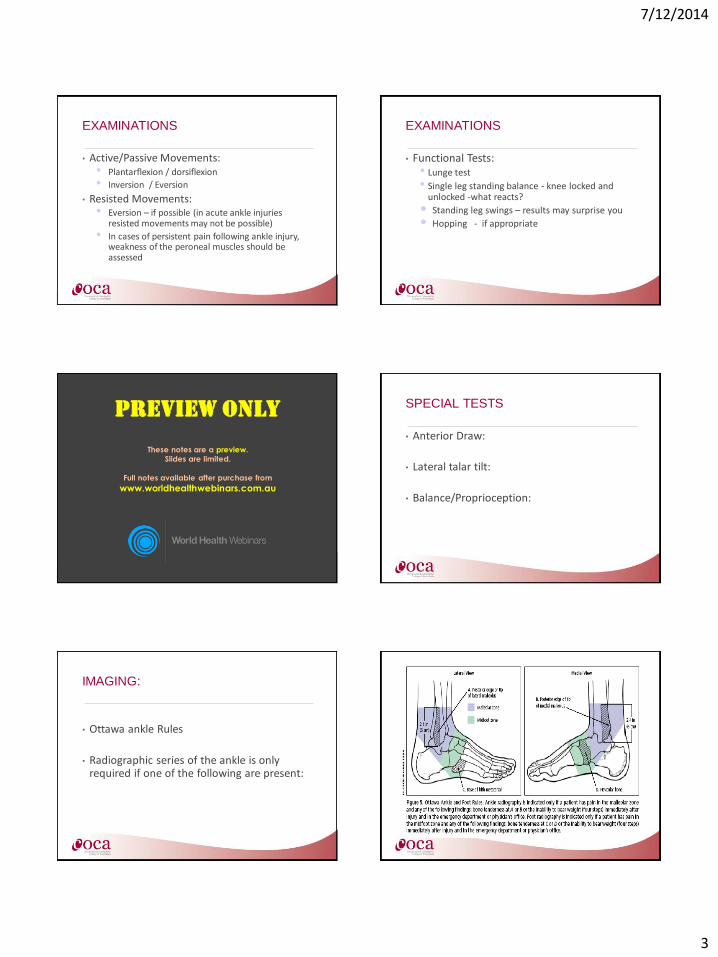
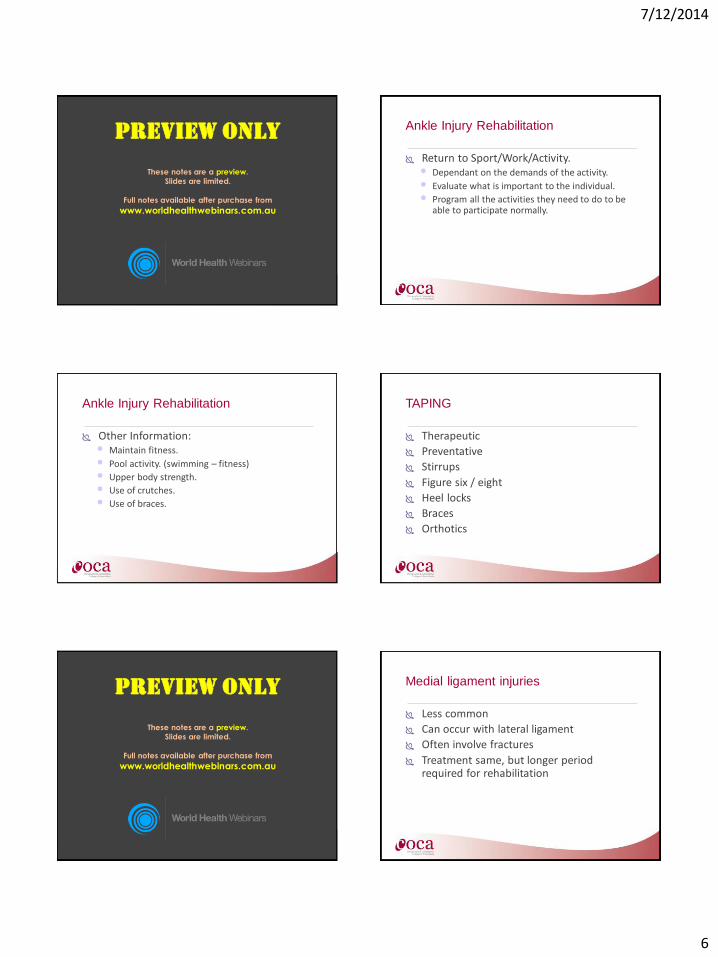
IMAGING:
• Ottawa ankle Rules
• Radiographic series of the ankle is only required if one of the following are present:
7/12/2014
4
Ottawa Rules
• Bone tenderness @ posterior edge of the distal 6cm of the medial malleolus
• Bone tenderness @ posterior edge of the distal 6cm of the lateral malleolus
• Totally unable to WB both immediately after injury & (for 4 steps) in the emergency department
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Ottawa Foot Rules
• Bone tenderness of the navicular
• Bone tenderness at the base of the 5th MT
• Totally unable to WB both immediately after injury & (for 4 steps) in the emergency department
LATERAL LIGAMENT INJURIES
• Often occur in activities with changes in direction, uneven surfaces: netball, football, basketball…
• Usually inversion and PF
• Usually ATFL before the CFL
LATERAL LIGAMENT INJURIES
• GRADE 1: mild stretching and no instabilities / abnormal laxity (compare)
• GRADE 2: partial but incomplete tear with mild instability & firm end point
• GRADE 3: a complete tear of the ATF and CF ligaments with gross laxity and instability
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Ankle Injury Rehabilitation • Stages:
• Early/Initial
• Intermediate
• Advanced
• Return to Sport/Function
Brukner, Peter & Khan, Karim (1999) Clinical Sports Medicine. Mc Graw - Hill Book Company: Australia.
What I commonly see in recurrence is that patients did the following: Injury
Initial Care
Basic Rehab – PROM, AROM & Strength (isolated)
7/12/2014
5
What I commonly see in recurrence is that patients did the following: Standing Balance (wobble
board)
Back to work, sport, life
Re injury
Problem?? Recurrence? Why? Non Specific
Incomplete
No Functional Re Introduction Stage
Only Static Balance Ex’s - no dynamic
Didn’t address previous imbalances…etc etc etc
Ankle Injury Rehabilitation
Acute: • RICE:
• Bracing/Taping:
• Determination of Grade of damage (I, II, or III).
• 24-48 hrs non-weight bearing (dependant).
• Progression to partial weight bearing then full.
• Passive mobilisation (esp dorsi flexion - towel)
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Ankle Injury Rehabilitation
Early Stage: • Starts when partial weight bearing is achievable.
• Can be completed sitting or standing dependent on damage.
• ROM: seated dorsi/plantar flexion, inversion/eversion using a towel.
• Wobble Board seated using above movement patterns.
Ankle Injury Rehabilitation
Early Stage: • Loaded ROM - standing (lunge dorsiflexion).
• Static Standing wobble board or Stability Disc/Matt (AROM + Balance).
• Strengthening (eversion/inversion using resistance band).
• Normally things stop here….
Ankle Injury Rehabilitation
Strengthening Exercises: • Squatting – various angles
• Calf raises – uni & bilateral – full pain free ROM
• Toe and Heel Walking
• The Moon Walk
7/12/2014
6
Ankle Injury Rehabilitation
Return to Activity Exercises: • Landing – lunge to land, lunge with leap to land –
toe landing, heel landing, sideways leap to land, 1 foot to 2 foot landing, 2 foot to 1 foot landing, landing eyes closed THEN….
• Jogging, Hopping, Skipping
• Progress to change surfaces also
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Ankle Injury Rehabilitation
Return to Sport/Work/Activity. • Dependant on the demands of the activity.
• Evaluate what is important to the individual.
• Program all the activities they need to do to be able to participate normally.
Ankle Injury Rehabilitation
Other Information: • Maintain fitness.
• Pool activity. (swimming – fitness)
• Upper body strength.
• Use of crutches.
• Use of braces.
TAPING
Therapeutic
Preventative
Stirrups
Figure six / eight
Heel locks
Braces
Orthotics
Grade 3 injuries
Surgery versus conservative
Trial of initial conservative at least over 6 weeks
Recurrent episodes of instability or persistent pain may warrant surgery or at the least a referral for opinion
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Medial ligament injuries
Less common
Can occur with lateral ligament
Often involve fractures
Treatment same, but longer period required for rehabilitation
7/12/2014
7
The “Problem Ankle”
Patient continues to complain of pain and recurrent instability
Persistent swelling and impaired function three to six weeks post injury
Accurate diagnosis is essential
Possible Problems
Undiagnosed fracture
Other bony abnormalities
Ligament, tendon, synovial or neurological dysfunction (or all the above!!)
Missed syndesmosis injury
Sinus Tarsi Syndrome
Osteochondral damage
An injury or small fracture of the cartilage surface of the talus Not uncommon in compressive injuries
Injury with actual loss of part of the chondral surface and underlying subchondral bone,
Injury to the superficial cartilage surface with a crush cartilage injury or shear tear of the cartilage surface,
Subchondral cyst type injury with a cyst formation deep to the cartilage surface but an intact overlying cartilage and bone surface.
Examine the foot at 45º PF and attempt to rotate the talus out of the ankle mortis
Try and reveal tenderness of the dome of the talus MRI / isotopic bone scan
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Avulsion fracture base of the 5th
Metatarsal Can occur with avulsion injuries Results from avulsion of the peroneus brevis
tendon from it’s attachment to the 5th metatarsal
X-ray should show it Immobilisation for pain relief (1-2 weeks) Protected mobilisation and rehabiliation
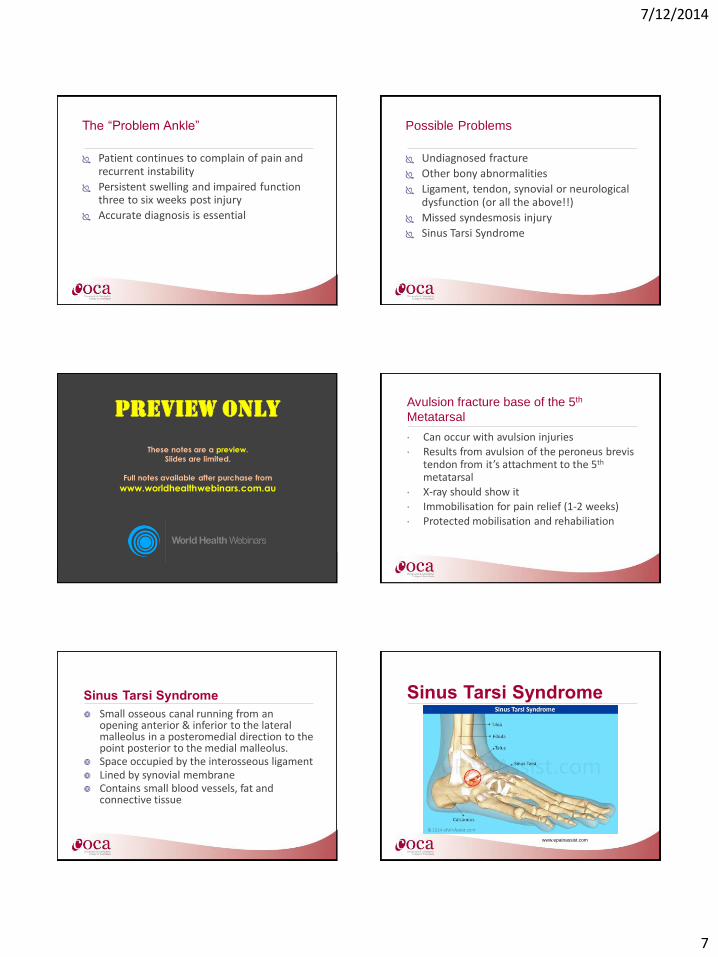
Sinus Tarsi Syndrome
Small osseous canal running from an opening anterior & inferior to the lateral malleolus in a posteromedial direction to the point posterior to the medial malleolus.
Space occupied by the interosseous ligament Lined by synovial membrane Contains small blood vessels, fat and
connective tissue
Sinus Tarsi Syndrome
www.epainassist.com
7/12/2014
8
Sinus Tarsi Syndrome
May occur secondary to an ankle injury
May occur as an overuse injury secondary to excessive subtalar pronation
Pain is experienced at the anterolateral opening of the sinus tarsi
Often worse in the morning but improves with loading
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Causes
Chronic overuse secondary to poor biomechanics (excessive pronation)
Often secondary to inversion injury
The joint is prone to synovitis both in the acute situation and also in the chronic situations such as gout, inflammatory arthropathies and osteoarthritis
Clinical features:
Poorly localised pain, more over the anterolateral aspect of the lateral malleolus
Greater pain in the morning May decrease with exercise Difficulty with uneven ground and perturbations Often full ROM in the ankle joint, however the
subtalar ROM is restricted May reproduce pain on either passive inversion
or eversion
In The Journal of Sports and Physical Therapy, Japanese
researchers discovered, individuals with chronic ankle instability
(CAI) had a distal fibula positioned more lateral compared with
healthy individuals with no CAI. In effect, those who had suffered
serious syndesmosis injuries in the past and ended up with a wider
distance between the fibula and the tibia, suffered more ongoing
ankle pain than those without a tibfib separation.*
Research says even a 1mm displacement of the talus within the
mortise (due to a wider placed fibula) can reduce the contact area in
the talocrural joint by 42% (Ramsey and Hamilton 1976).
Kobayashi et al (2014). 'Fibular malalignment in individuals with chronic ankle instability.' JOPST. 44(11); pp 841-910.
Ramsey and Hamilton (1976). J Bone and J Surgery Am. 58(3); 356-357.
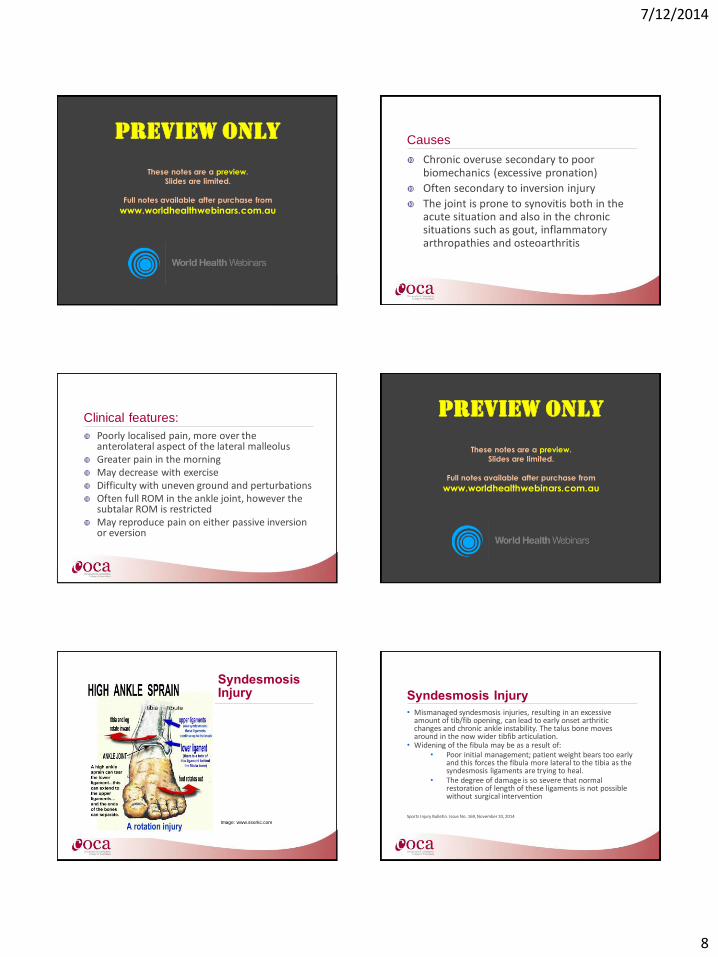
Syndesmosis Injury PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Image: www.ssorkc.com
Syndesmosis Injury Syndesmosis Injury
• Mismanaged syndesmosis injuries, resulting in an excessive amount of tib/fib opening, can lead to early onset arthritic changes and chronic ankle instability. The talus bone moves around in the now wider tibfib articulation.
• Widening of the fibula may be as a result of: • Poor initial management; patient weight bears too early
and this forces the fibula more lateral to the tibia as the syndesmosis ligaments are trying to heal.
• The degree of damage is so severe that normal restoration of length of these ligaments is not possible without surgical intervention
Sports Injury Bulletin. Issue No. 169, November 10, 2014
7/12/2014
9
Compliance • Why don’t patients follow all the way
through with their rehab?
• Pain is a strong motivator – remove the pain and you remove the motivation
• We need to educate it simply, so they can understand completely: • What has been damaged, how to heal it,
what imbalances are present and WHY it is important to address the imbalances for THAT person.
Educate, Empower, Motivate PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Seek to understand their motivators
• Find the thing that motivates THEM.
• Show them a plan visually and show them where they are on that plan – you need “buy in” to the plan early on for the best results.
• What is it that they LOVE doing - sport, walking, hiking, dancing, playing golf when they are 90 years old, gardening. Explain what they need to do reduce the chance of injury so they can keep doing those activities
Prochaska, J. O., & DiClemente, C. C. Transtheoretical therapy: Toward a more integrative model of change. Psychotherapy: theory, research and practice, 1982,19, 276-288.
Thank you
World Health Webinars
http://worldhealthwebinars.com.au