Embed Size (px)
Citation preview

Primary Care Practice: Surprise & Uncertainty
Benjamin F. CrabtreeUMDNJ-RWJMSDept Family Medicine

Overview
Translating evidence into practice
Results from two studies of family practices
Practices as complex systems
Implications of complexity science for
managing uncertainty

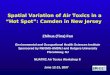
1000 persons
800 report symptoms
327 consider seeking medical care
217 visit a physician’s office (113 visit a primary care physician’s office)
65 visit a complementary or alternative medical care provider
21 visit a hospital outpatient clinic
14 receive home health care
13 visit an emergency dept
8 are hospitalized
<1 is hospitalized in an academic medical center
Fig. Results of a reanalysis of the monthly prevalence of illness in the community and the roles of various sources of health care. (Green LA et al., N Engl J Med 2001, 344:2021-2024)

Background
Recent advances in diagnostic and treatment technologies have produced great opportunities to decrease morbidity and mortality from many common diseases.
Clinical trials and evidence-based reviews have established widely accepted clinical guidelines for the management and prevention of diseases.

The Uncertainty & SurpriseDissemination of these advances into clinical
practice has been disappointing, resulting in disparity between scientific evidence and actual practice.
There is an ongoing onslaught of new information and technology resulting in the need for continual learning in practice.
Current models of organizational change limit change in clinical practices and do not anticipate uncertainty.

Dissemination StrategiesContinuing medical educationEvidence-based guidelinesOpinion leadersAudit and feedbackIncentives & disincentivesAcademic detailingPatient and/or consumer activationOffice system innovationsContinuous quality improvement

Difficulty with current approaches
Each has demonstrated some success under certain circumstances, but none is effective in a generalizable manner.
Combination of approaches are more effective than individual approaches.
Each assumes that physician and practice change is a linear process and fails to account for the complexity of practice systems.


Two Studies of Practices
Direct Observation of Primary Care (DOPC)
Funded by grant from NCI (1 R01 CA60862)
Prevention & Competing Demands in Primary Care (P&CD)
Funded by grant from AHRQ (R01 HS08776)

Direct Observation of Primary Care
Cross-sectional observation of 84 family practices & 4454 patient visits to 138 physicians in Ohio
Direct ObservationDavis Observation CodeChecklists
Medical Record ReviewsPatient Exit questionnaireBilling DataPractice Environment ChecklistEthnographic Fieldnotes

Prevention & Competing DemandsIn-depth multimethod comparative case study of
18 family practices & 1,600 visits to 56 clinicians in Nebraska
Prolonged direct observation of practice environment recorded in checklists and field notes
Direct observation of 30 encounters/clinician recorded in checklists and field notes
Chart audits of patients who were observed
Interviews of all clinicians and most staff

Variation in Practice
Physicians provide integrated, prioritized care within an ongoing personal relationship. Stange KC, Jaen CR, Flocke SA, Miller WL, Crabtree BF. The value
of a family physician. J Fam Pract 1998; 46:363-368.
Services are tailored to meet risk factors, patient preferences, and teachable moments. Jaen CR, Crabtree BF, Zyzanski SJ, Stange KC. Making time for
tobacco counseling. J Fam Pract 1998; 46:425-428.

Variation in PracticeAntibiotics are prescribed inappropriately for
acute URI despite evidence. Scott J, Cohen D, DiCicco-Bloom B, Orzano J, Jaen C, Crabtree B.
Antibiotics use in acute respiratory infections and the ways patients pressure physicians for a prescription. J Fam Pract, 2001; 50(10): 853-8.
Smoking cessation counseling rates of physicians vary considerably. Jaen C, McIlvain H, Pol L, Phillips R, Flocke S, Crabtree BF.
Tailoring tobacco counseling to the competing demands in the clinical encounter. J Fam Pract, 2001; 50(10): 859-63.
Management of emotional distress varies considerably among physicians. Robinson D, Prest L, Susman J, Rouse J, Crabtree B. Technician,
friend, detective, and healer: family physicians’ responses to emotional distress. J Fam Pract, 2001; 50(10): 864-70.

Variation in Practice
Patient care staff roles in practices often do not match professional training. Aita V, Dodendorf D, Lebsack J, Tallia A, Crabtree B. Patient care
staffing patterns and roles in community-based family practices. J Fam Pract, 2001; 50(10): 889.
Geographic location of practice influences the delivery of services. Pol L, Rouse J, Zyzanski S, Rasmussen D, Crabtree B. Rural, urban,
and suburban comparisons of preventive services in family practice clinics. J Rural Health, 2001; 17(2): 114-121.

Practices are complexForced discontinuity of care results in 24% of
patients with managed care insurance changing physicians over a 2 year period, impacting quality of care. Flocke S, et al. The impact of insurance type and forced discontinuity
on the delivery of primary care. J Fam Pract, 1997; 45: 129-135.
Visits are complex with a large variety of problems & multiple problems/visit that are covered in visits of 10 minute average duration. Stange KC, et al. Illuminating the “black box:” A description of 4454
patient visits to 138 family physicians. J Fam Pract, 1998; 46: 377-389.

Practice are complexMultiple family members are treated in 18% of
visits making visits longer, but with no difference in billing. Flocke S, et al. The effect of a secondary patient on the family practice
visit. J Fam Pract, 1998; 46: 429-434.
Many patients have emotional distress (19% of patients seeing a family physician) with dramatic differences in time use (10 min no distress vs. 11.5 min distress & no dx vs. 12.8 min distress & dx) Callahan EJ, et al. The impact of a recent emotional distress and
diagnosis of depression or anxiety on the physician-patient encounter. J Fam Pract, 1998; 46410-418.

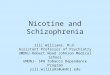
How can you make sense of all this variation and complexity?
5Local Community
3Clinical
Encounter
2Clinician
1Patient
4Practice
6Health System

Practices as Complex Adaptive SystemsPractices co-evolve locally with communities to
meet the particular needs of patients. Miller WL, Crabtree BF, McDaniel R, Stange KC. Understanding
change in primary care practice using complexity theory. J Fam Pract 1998; 46:369-376.
Important features of practices that make them unique:• History and initial condition• Particular agents and patterns of nonlinear interaction• Local fitness landscape• Regional and global influences Miller WL, McDaniel RR, Crabtree BF, Stange KC. Practice jazz:
understanding variation in family practices using complexity science. J Fam Pract, 2001; 50(10): 872-8.

Three Properties of Complex SystemsSelf-organization
Spontaneous development of structures and forms of behavior according to non-linear interactions among agents seeking a better position in the local fitness landscape.
Co-evolutionEach system evolves over time in relationship to
other systems in the local fitness landscape.Emergence
The system that evolves is greater than the sum of its parts and cannot be understood just by understanding the individual parts.

Franchise Family Practice
Suburban practice created by a hospital system to serve an insured middle-class population.
Focus is on providing efficient medical services and maximizing financial success.
Internal processes related to patient care, office operations, income generation, and physician style all work towards this focus and related goals.

Dusty Garden Family Practice
Four physician inner-city practice serving a local indigent population.
Vision is to empower its underserved community and to improve the community’s health.
Founding physician has strong beliefs about caring for the underserved.
Internal processes related to patient care, office operations, preventive service delivery, and physician style all work towards this vision.

Observation Intervention
DOPC
STEP-UPDirectObservation of PrimaryCare Study To
Enhance Prevention by Understanding
Practice
P&CDPrevention & Competing Demands in Primary Care

Study To Enhance Prevention by Understanding Practice
STEP-UPRandomized clinical trial of 80 family practices
in Ohio
Multimethod assessment (MAP) of values, structures, and processes Crabtree B, Miller W, Stange K. Understanding practice from the
ground up. J Fam Pract, 2001; 50(10): 881-887.
Tailored change strategies Goodwin M, Zyzanski S, Zronek S, et al. A clinical trial of tailored office
systems for preventive service delivery. The Study to Enhance Prevention by Understanding Practice (STEP-UP). Am J Prev Med, 2001; 21: 20-8.

Practice Assessment Methods
Direct observation of practice and clinical encounters (2-5 days)• Participant observation fieldnotes• Structured and unstructured checklists• Chart reviews and billing data• Informal and formal interviews
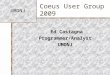
Physician, staff, and patient surveysPractice Genogram

Practice GenogramMcIlvain HE, Crabtree BF, Medder J, et al. Using “practice genograms” to understand and describe practice configurations. Fam Med, 1998; 30:490-6.
EMD
1992Age: 30's
CMD
1987Age: 50's
DMD
1990Age: 40's
HBusinessManager
promoted 1992
GHead Nurse
F(C's wife)
CollectionsPart time
BMD
1987-92
IAide
Part time
KAide
Part time
JOld timer
MFront Desk
4 years
LFront Desk
1987
NInsurance
5 years
OTranscriptionist
4 years
AMD
1987-89
HFront Desk
1987-92
GHead Nurse3 days/week

Feedback & FacilitationPractice report & genogram generated
and shared with practice stakeholdersValues, structures, processes, and
outcomes shared along with reflection points
Negotiated intervention• Instrumental approaches• Motivational approaches
Follow-up & facilitation

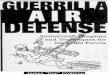
Global Preventive Service Delivery Rates
Per
cen
t of
Eli
gib
le S
ervi
ces
Up
to
Dat
e
0.43
0.41
0.39
0.37
0.35
0.33
0.31
0.29
0.27
0.25Baseline 6 months 12 months 18 months 24 months
Intervention Control
Goodwin MA, Zyzanski SJ, Zronek S, Ruhe M, Weyer SM, Konrad N,Esola D, Stange KC. A clinical trial of tailored office systems for preventive service delivery: The Study to Enhance Prevention by Understanding Practice (STEP-UP). Am J Prev Med, 2001; 21:20-8.

Implications of STEP-UP
Assessments for tailoring interventions to fit local fitness landscapes
Facilitate interventions to identify and maximize practice capacity to change
Practice and clinician self-reflection for ongoing learning

Observation Intervention
DOPC
STEP-UP
IMPACT
DirectObservation of PrimaryCare Study To
Enhance Prevention by Understanding
Practice
Insights from Multimethod Practice Assessment of Change over Time
P&CDPrevention & Competing Demands in Primary Care
ULTRAUsing Learning Teams for Reflective Adaptation

Multi-method Assessment Process (MAP)/ Reflective Adaptive Process (RAP):
an iterative assessment and reflective change approach that uses complexity science as a conceptual framework to guide the processes.
Emergent Quality

ULTRANHLBI funded group randomized clinical
trial of 60 practices in NJ and PAIntervention focused on interrelationships of
key stakeholders (agents)Two week practice assessment (MAP),
followed by a practice summary report and 3-6 months of facilitated reflective practice teams (RAP)
Outcome measures: smoking screening; management of hyperlipidemia, hypertension, diabetes, and asthma; and practice culture and capacity for change

Intervention OverviewMAP
Collected by facilitator first two weeks in practicePractice information form (Completed by Practice Mgr)General observation & key informant interviews &
DocumentsPractice genogram
RAPBased on MAP, facilitator helps identify team leader
and members with the goal of diversity among agentsTeam meets for 1 hour weekly, with initial focus on team
skills and collaboration Using MAP assessment as starting point, team identifies
problems with system level implications and begins improvement cycle

A Last Word From Yogi
“In theory, there is no difference between theory and practice. In practice there is.”