-
Prise en charge des congénitauxScanner cardiaque
pédiatrique:
consensus d’experts 2019
Karine Warin Fresse MD1
Isorni MA, MD2, Dacher JN, MDPHD3, Pontana F, MDPHD4, Gorincour
G MDPHD5, MD, Raimondi F, MD6
1Imagerie cardiovasculaire, Fédération des cardiopathies
congénitales, CHU Nantes2Cardiologie, CCML, Paris, 3Radiologie, CHU
Rouen, 4Radiologie CHU Lille; 5Radiologie CHU Marseilles,
6Cardiopédiatrie Necker-enfants malades, Paris
-
Introduction
• Cardiac Computed Tomography Angiography (CTA):
– has progressively replaced cardiac catheterization
– is now often used as a diagnostic tool complementary to
echocardiography.
• Challenge:
–breath-holding issues,
–uncontrolled movement
–high heart rate,
–complex anatomy and small structures
-
• Indications
• Patient preparation
• CTA techniques
• Dose reduction
• Post processing
• Structured report
-
Indications
• Coronary arteries
• Systemic vessels– Aortic coarctation
– Complex arch anomalies
– Supra valvular aortic stenosis
– Aorto-pulmonary window
– Pulmonary arteries
• Pulmonary venous anomalies
• Transposition of great arteries
• Intracardiac anatomy : complex congenital heart disease– for
surgical strategy
– 3D modeling from CT data may be reconstructed and eventually
printed to help in planning surgical strategy Raimondi F, Warin
Fresse K. Arch Cardiovasc Dis. 2016;109(2):150-7
Han BK et al. J Cardiovasc Comput Tomogr. 2015; 9(6):493-513Han
BK et al. J Cardiovasc Comput Tomogr. 2015; 9(6):475-492
-
Coronary Artery Imaging
Han BK et al. J Cardiovasc Comput Tomogr. 2015; 9(6):475-492
-
11 month 9 kgTGV
136 bpmDLP 25 mGy.cm / 0.6 msv
-
14 month 10 kgTGV
155 bpmDLP 31.4 mGy.cm : 0.8msv
-
Coronary arteries
ARCAPA
-
Co-arctation
• At the time of the diagnosis as a complement TTE
• During follow up:
–After surgical correction
–Before catheter intervention
• Restenosis,
• Residual stenosis,
• Aneurysm or pseudoaneurysm
–Aortic arch hypoplasia
15 yoProspective acquisition
80 cc Visipaque 320 40 cc saline flush
HR: 93 bpm. No prémédication. PDL : 56 mGy.cm
-
Complex arch anomalies
-
Double Aortic Arch
-
Pulmonary venous anomalies
6 month, 6 kgatrial septal defect
VPARHR 110 bpm
DLP 16.1 mGy.cm
-
Transposition of Great Arteries
-
Complex Congenital heart diseaseCriss Cross Heart
-
Patient preparation
• Good injection site (peripheral vein of arm, foot or head)
(1,5cc/s power injector )
• ECG electrode on the chest outside the exam zone to avoid
artefact• comfortably installed in specially designed bed with
blanket and bands to
avoid movement and keep warm• > 5-6 yo:
• Exam and breath should be explained • Apnea
• < 6 yo:• BB < 3-6 mois: baby bottle• 6 mois- 6 ans:
light sedation
-
Booij R et al. J Cardiovasc Comput Tomogr. 2016; 10(6):13-21
-
CTA technique
• Abandoned technique:
–Non-ECG- synchronized helical scan
–Retrospectively ECG- gated scan
• 2 CT scan acquisition depending on:
–Prospectively ECG triggered sequential acquisition
–One shot acquisition.
-
ECG triggered sequential acquisition
• Step-and-shoot acquisition
• Any heart rate condition and even in free breathing
• Biphasic injection of iodinated contrast followed by a saline
flush (1cc/kg) using a power injector :
– 270-300 mgI/L < 40 kg,
– 320-350 mgI/L > 40kg
• Beta-blockers could be used not to decrease the heart rate but
to stabilize it.
-
Prospective Acquisition
-
One shot acquisition
allows to acquire the whole heart within one single heart
beat
Heart rate (bpm)any heart rate
ECG Synchronisation/acquisition Prospective/ Axial Cardiac
Weight (kg)any Weight until 50 Kg
kV max70-80
mA Smart mA 150-450
Exposure Window0,25-0,5 s
Collimation16 cm
Target phase 40-50% if HR > 65 bpm 75% si < 65 bpm
Rotation time (ms) 0.28 sec
Lenght (mm)120-140 mm
Field of Vue (SFOV) small
Slice Thickness (mm)0.625 mm
Reconstruction algorythm ASIR 40%
Motion correction algorythm Freeze if HR variation
Heart rate (bpm) 30 to 180
ECG Synchronisation/acquisitionProspective target auto /one shot
acquisition / one
beat
Weight (kg) any Weight until 50 Kg
kVp 80kV
mA mA Modulation (SUREExposure)
Exposure Window 350-400 ms
Collimation (mm) 0.5x240 to 0.5x320 (adapted to the heart)
Target phase Auto target phase (75% if HR70 bpm
Rotation time (ms) 0,275 s
Lenght (mm) 120-160 mm
Field of Vue (SFOV) 240 mm
Slice Thickness and interval (mm) 0.5 - 0.25
Reconstruction algorythm iterative
Motion correction algorythm PhaseExact (best phase)
REVO CT General Electric ACQUILLION ONE GENESIS Canon Medical
system
-
Dose reduction
• First step :
–to choose the more adapted scanning protocol for the
patient
–and his clinical characteristics
• Second step:
–Reconstruction algorithms (specific /vendors)
–Iterative reconstructions
-
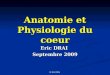
Dose
E (mSv) = DLP (mGy.cm) x fDLP (mSv/mGy.cm)
-
Dose
• Pas de NRD (Niveau Référence Diagnostic) en cardiopédiatrie•
NRD scanner pédiatrique
0,78 mSv 1,17 mSv 1,82 mSv
www.nrd.irsn.fr
-
CHU Nantes
Nouveau nés (n=12)
1 -12 mois (n=22)
13-60 mois(n=22)
61-120 mois (n=23)
>120 mois(n=18)
DLP moyenne (mGy.cm) 15,55 21, 45 29,91 40,08 55,52
Dose (mSv) 0,6 0,56 0,54 0,52 0,72
NRD 0,78 0,78 1,17 1,17 1,82
< 10 KG (35) 10-20 KG (23) 20-30 kg (12) >30 kg (27)
DLP moyenne (mGy.cm) 20,69 35,56 36,74 55,02
NRD (mGy.cm)
-
Acquisition prospective Acquisition rétrospective
270mgI/L 320mgI/L 320mgI/L
Liu Z et al. Int J Clin Pract 2016
N = 90
-
• Diagnostic accuracy:
– Extra-cardiaque: 100% in 3 groups
– Intra-cardiaque: A-C: 100% for A, B: 96%
• Low dose, Low concentrationLiu Z et al. Int J Clin Pract
2016
Bouchra HG et al. Eur Radiol 2015
-
Post-processing
• Best cardiac phase
• Motion correction
• Windowing
• Multiplanar recontructions
• Maximum intensity projection
• Volume Rendering
-
Best cardiac phase 72%
3 years old22 cc VISIPAQUE 270, 10 cc saline flush
145 bpm.PDL : 37.9 mGy.cm
-
Best cardiac phase 41%
3 years old22 cc VISIPAQUE 270, 10 cc saline flush
145 bpm.PDL : 37.9 mGy.cm
-
Best cardiac phase 51%
3 years old22 cc VISIPAQUE 270, 10 cc saline flush
145 bpm.PDL : 37.9 mGy.cm
-
Best cardiac phase 61%
3 years old22 cc VISIPAQUE 270, 10 cc saline flush
145 bpm.PDL : 37.9 mGy.cm
-
Windowing
-
Windowing
-
Windowing
-
MIP
3 month, PAVSD Type 18 cc VISIPAQUE 270, 4 cc saline flush
146 bpm.DLP : 13.6 mGy.cm
-
Volume Rendering
6 years old40 cc Visipaque 270, 20 cc saline flush.
105bpmDLP 37.8mGy.cm
-
Structured report
• First Name, Last Name• Date of birth• Identification number•
Scanner date
• Indication : • Age at the date of the CT scanner• Clinical
context• Question
• Technique :• CT scan date of commissioning• Acquisition
technique• Contrast volume, contrast name• Heart rate•
Premedication• DLP (mgy.cm)
• Results :• Image quality• Segmental analysis:• Heart:• Situs
abdominal (when possible) solitus or inversus• Situs atrial solitus
or inversus or ambiguus• Levo/dextro/meso- cardia• Systemic veins
(connection, stenosis, anatomy)• Atrio-ventricular connection,
ventriculo-arterial connection• Cardiac chambers•• Great vessels:•
Aorta (right or left, supra-aortic vessels, size, coarctation,
injury…)• Pulmonary arteries`(size, stenosis)• Post surgical
anatomy (conduit, stent etc)• Arteriosus ductus (presence or not,
size, course)• Coronary• Position of coronary ostia• Course•
Stenosis / aneurysm (size, localisation)• Diameter (aneurysm,
fistula)• Dominance (if possible)•• Pericardium• Thrombus••
Mediastinum / lung / oesophagus/ trachea• Associated other
malformation (squelettae…)
Conclusion:Synthetic answer to the question
-
In summary
• Increase:
–Spatial and temporal resolution of CCT with
–Speed of data acquisition
• Decrease in radiation dose.
• Benefit/risk balance
• CT scan
–Newborns and infants: second line after echocardiography
–Adolescents: in complementary of cardiac MRI
• ALARA
-
Merci de votre attention