Embed Size (px)
Citation preview
50ème Séminaire Interrégional de Réanimation Médicale Clermont-Ferrand, 7 & 8 Décembre 2006
Prise en charge du syndrome post-arrêt cardiaque
Alain CariouRéanimation Médicale
Cochin - Université Paris 5
« The post-resuscitation disease is a specific pathophysiologic state that should be considered an independent nosological entity » P. Safar & W. Negovski
Post-resuscitation care
ROSC must be the beginning of a complex treatment
Aims of post-resuscitation care are:• To stabilize cardio-respiratory status in order to improve tissue perfusion
(particularly cerebral and splanchnic)
• To find the cause of CA, to treat it and to prevent recurrence
• To manage the post-resuscitation syndrome
Post-resuscitation care should permit: • To reach neurological evaluation in the best conditions
• To improve the prognosis?

Pronostic de l’arrêt cardiaque
350000 morts subites par an
100000 tentatives de RCP
Période pré-hospitalière40000 patients
réanimés…
…et hospitalisés
Mortalité hospitalière:
Choc → décès précoce
Lésions neurologiques
20000 survivants
10000 sans séquelles neuro. majeures
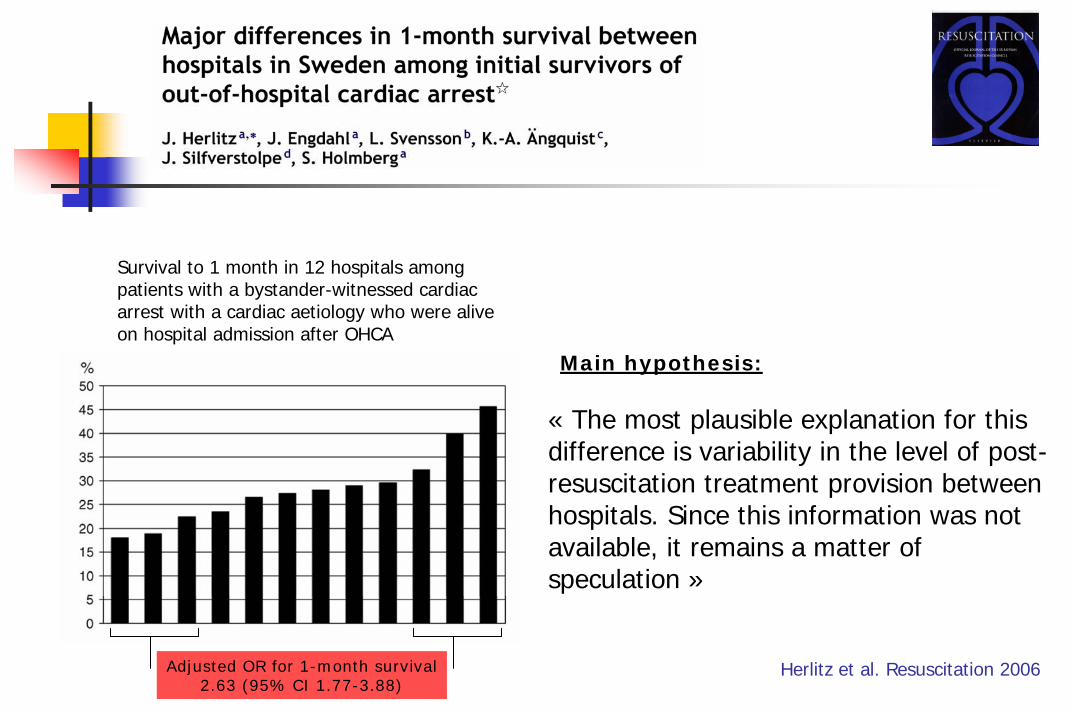
Survival to 1 month in 12 hospitals among patients with a bystander-witnessed cardiac arrest with a cardiac aetiology who were alive on hospital admission after OHCA
Main hypothesis:
« The most plausible explanation for this difference is variability in the level of post-resuscitation treatment provision between hospitals. Since this information was not available, it remains a matter of speculation »
Adjusted OR for 1-month survival2.63 (95% CI 1.77-3.88)
Herlitz et al. Resuscitation 2006
ut
1. Ischemia and reperfusion syndrome2. Inflammatory response3. Myocardial dysfunction4. Adrenal dysfunction5. Coagulopathy
Current Opinion in Crit Care. 2004
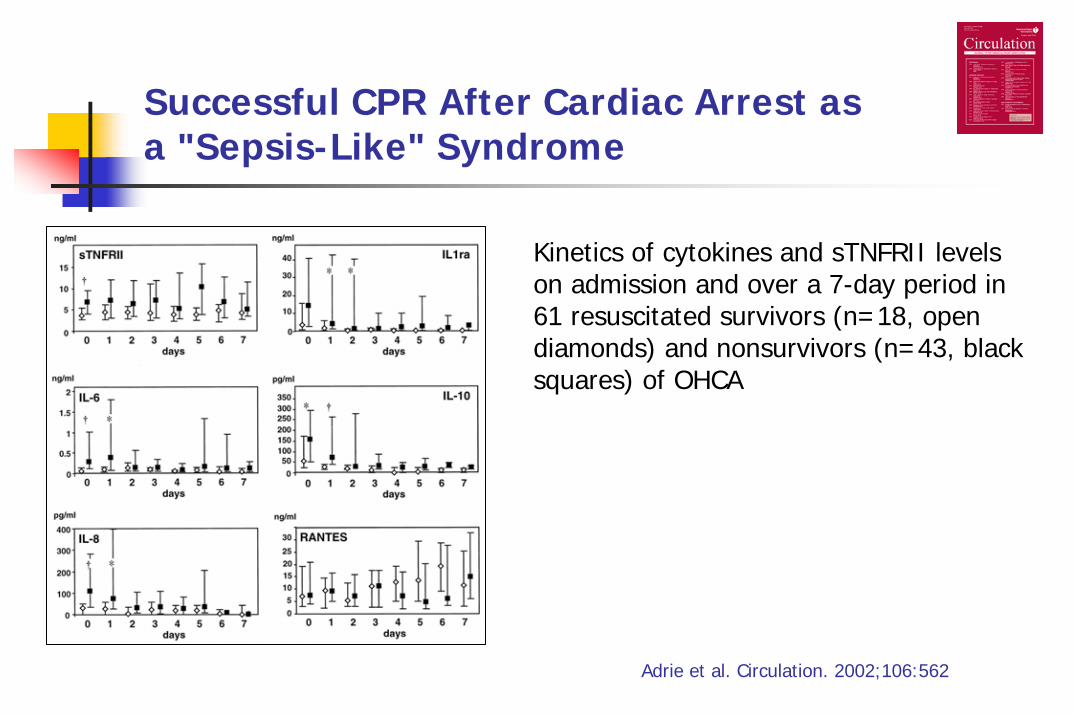
Successful CPR After Cardiac Arrest as a "Sepsis-Like" Syndrome
Kinetics of cytokines and sTNFRII levels on admission and over a 7-day period in 61 resuscitated survivors (n=18, open diamonds) and nonsurvivors (n=43, black squares) of OHCA
Adrie et al. Circulation. 2002;106:562
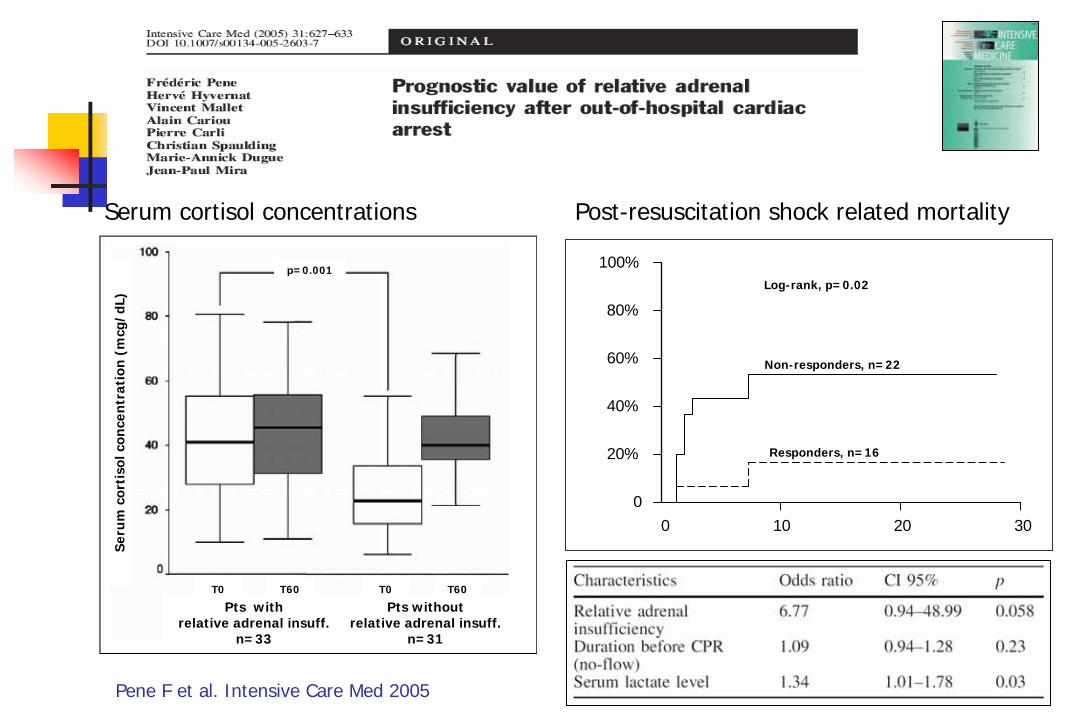
Pene F et al. Intensive Care Med 2005
T0 T60
Pts with relative adrenal insuff.
n=33
Pts without relative adrenal insuff.
n=31
Seru
m c
orti
solc
once
ntr
atio
n (m
cg/d
L)
T0 T60
p=0.001
Non-responders, n=22
Responders, n=16
Log-rank, p=0.02
Post-resuscitation shock related mortalitySerum cortisol concentrations
0 10 20 300
20%
40%
60%
80%
100%
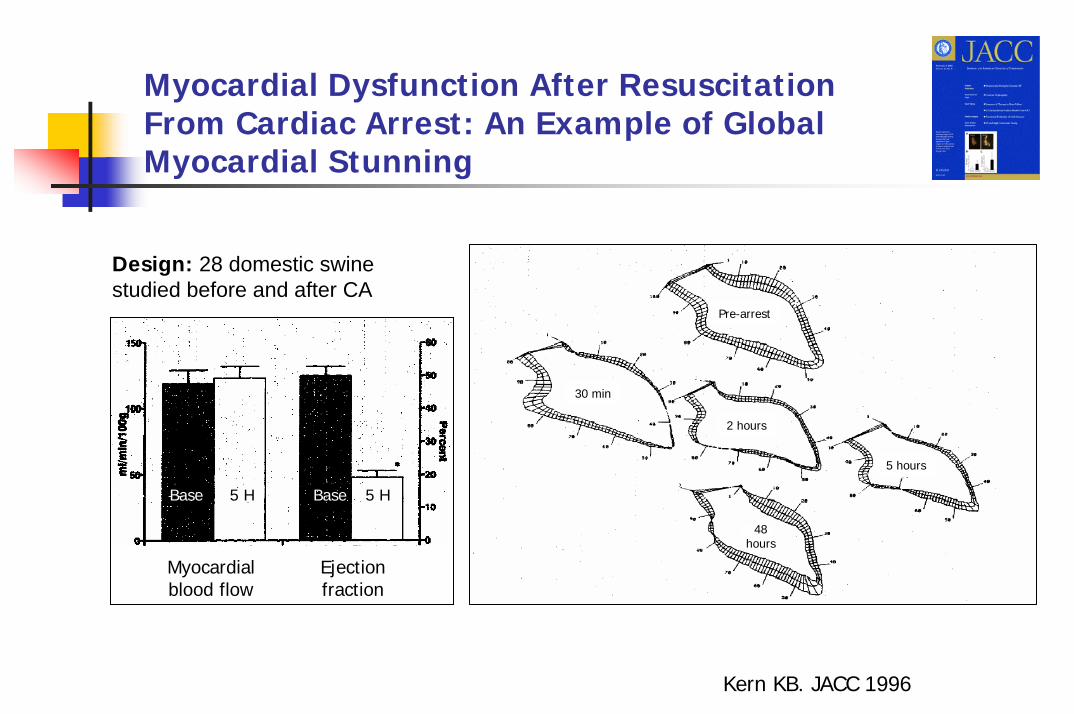
Myocardial Dysfunction After Resuscitation From Cardiac Arrest: An Example of Global Myocardial Stunning
Design: 28 domestic swine studied before and after CA
Pre-arrest
30 min
2 hours
5 hours
48 hours
Myocardialblood flow
Ejection fraction
Base Base5 H 5 H
Kern KB. JACC 1996
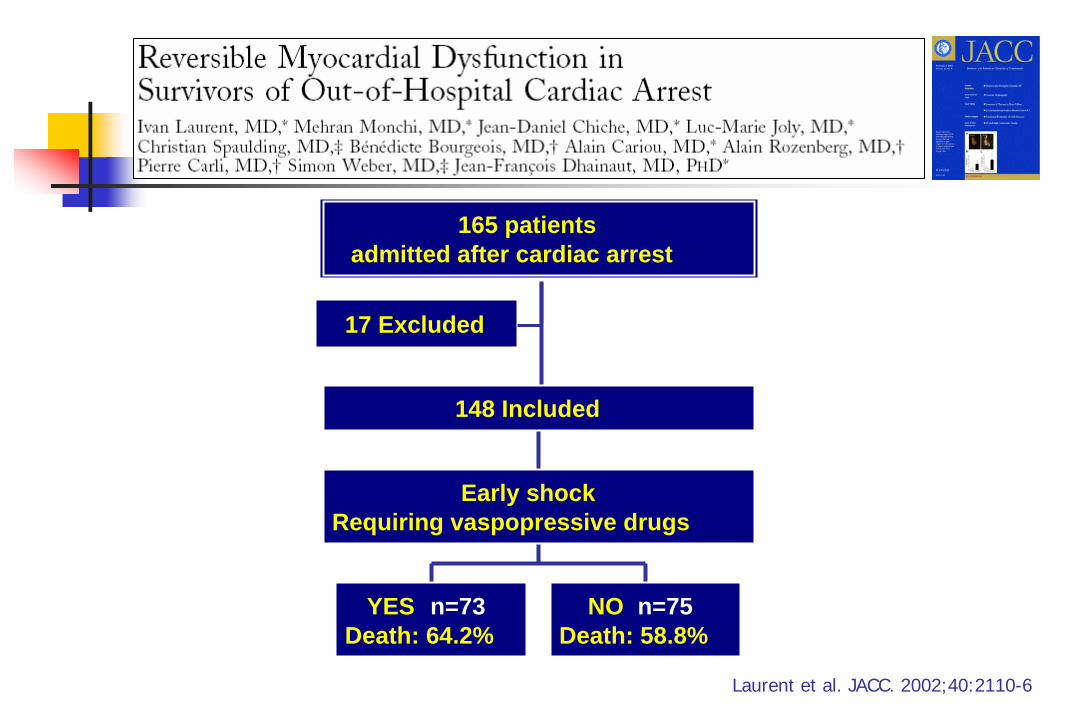
17 Excluded
YES n=73Death: 64.2%
NO n=75Death: 58.8%
Early shockRequiring vaspopressive drugs
148 Included
165 patientsadmitted after cardiac arrest
Laurent et al. JACC. 2002;40:2110-6
LA PHASE INITIALE : Une défaillance multi-viscérale sévère
Tenir jusqu ’à…
… une évaluation neurologique fiable
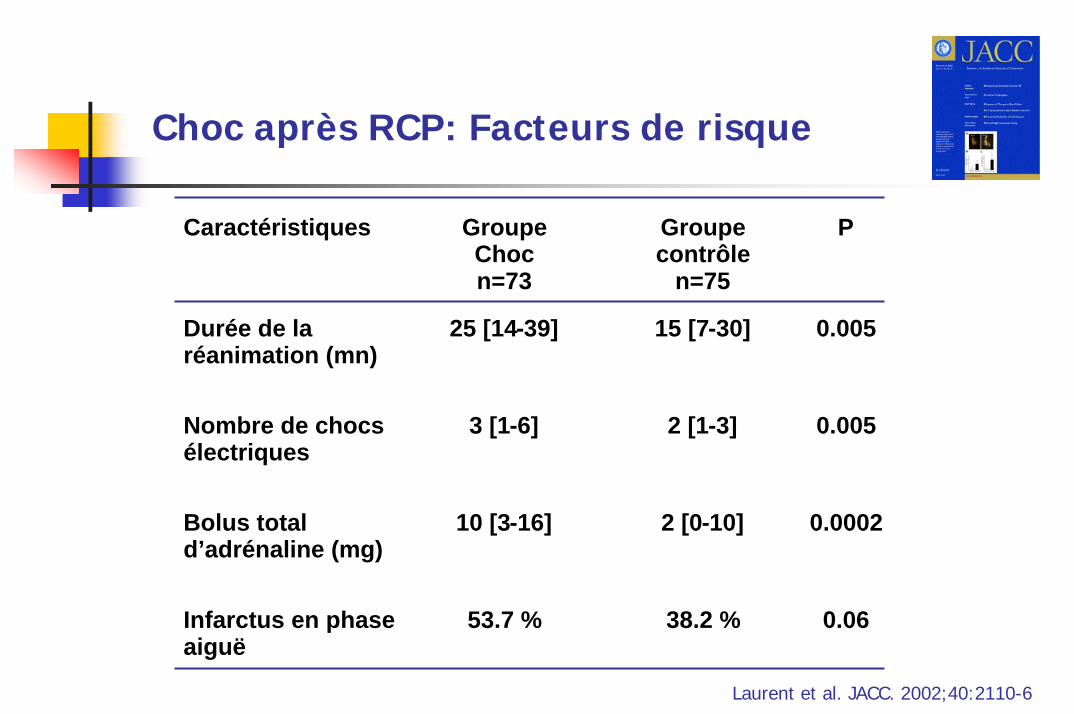
Choc après RCP: Facteurs de risque
Caractéristiques GroupeChocn=73
Groupe contrôle
n=75
P
Durée de la réanimation (mn)
25 [14-39] 15 [7-30] 0.005
Nombre de chocs électriques
3 [1-6] 2 [1-3] 0.005
Bolus total d’adrénaline (mg)
10 [3-16] 2 [0-10] 0.0002
Infarctus en phase aiguë
53.7 % 38.2 % 0.06
Laurent et al. JACC. 2002;40:2110-6

0
20
40
0 20 40 60heures après l'ACR
mmHg
0
2
4
L/min/m²
POD PAPO IC
**** ****
** p< 0.05p< 0.05
**
**** p< 0.01p< 0.01
Laurent et al. JACC. 2002;40:2110-6
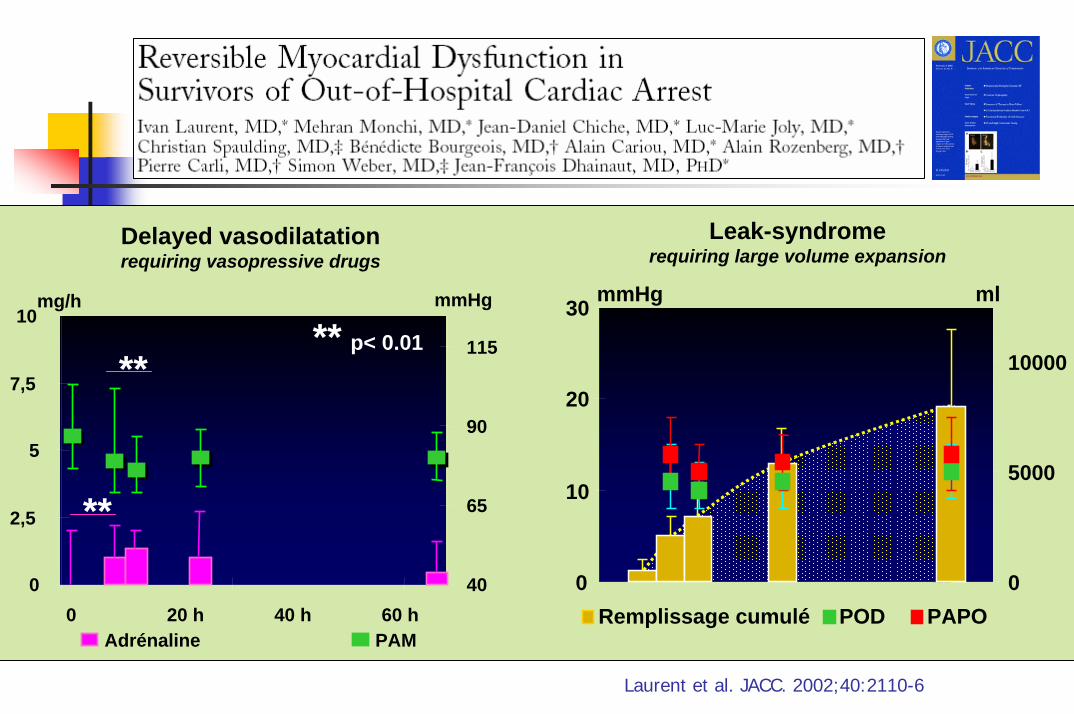
0
10
20
30 mmHg
0
5000
10000
ml
Remplissage cumulé POD PAPO0
2,5
5
7,5
10
0 20 h 40 h 60 h
mg/h
40
65
90
115
mmHg
Adrénaline PAM
Delayed vasodilatationrequiring vasopressive drugs
Leak-syndromerequiring large volume expansion
**
**
** p< 0.01
Laurent et al. JACC. 2002;40:2110-6
Prise en charge : Points particuliers
Monitorage précis et completCorrection des troubles métaboliques
DyskaliémiesAcidose métabolique
Adaptation de la ventilation mécaniquePressions bassesNomocapnie
Thérapeutiques d’exceptionCoronarographie ?Hémofiltration ?Assistance circulatoire ?
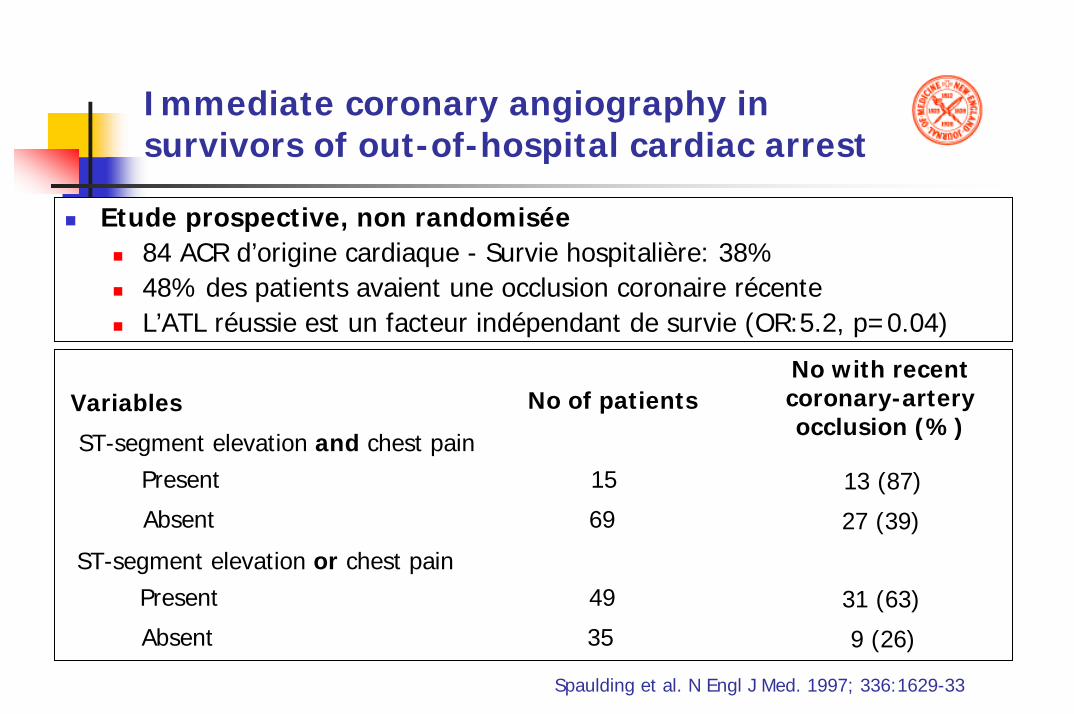
Immediate coronary angiography in survivors of out-of-hospital cardiac arrest
Variables
ST-segment elevation and chest painPresent
Absent
ST-segment elevation or chest painPresent
Absent
No of patients
15
69
49
35
No with recentcoronary-arteryocclusion (%)
13 (87)
27 (39)
31 (63)
9 (26)
Etude prospective, non randomisée84 ACR d’origine cardiaque - Survie hospitalière: 38%48% des patients avaient une occlusion coronaire récenteL’ATL réussie est un facteur indépendant de survie (OR:5.2, p=0.04)
Spaulding et al. N Engl J Med. 1997; 336:1629-33
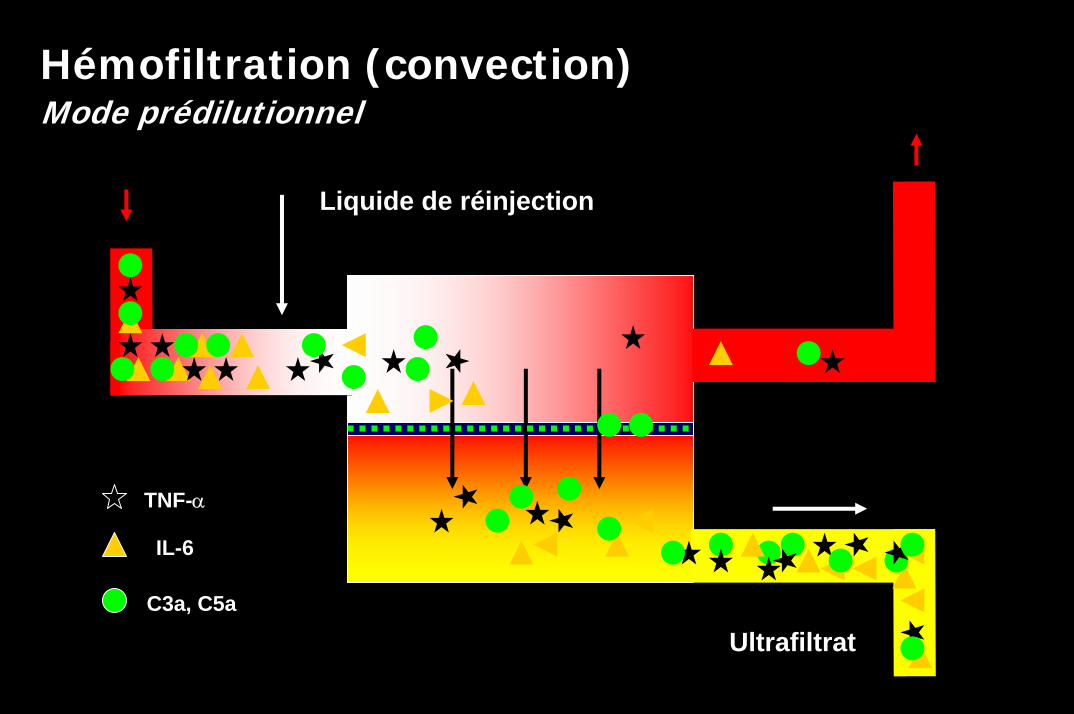
Hémofiltration (convection)Mode prédilutionnel
Ultrafiltrat
Liquide de réinjection
TNF-α
IL-6
C3a, C5a
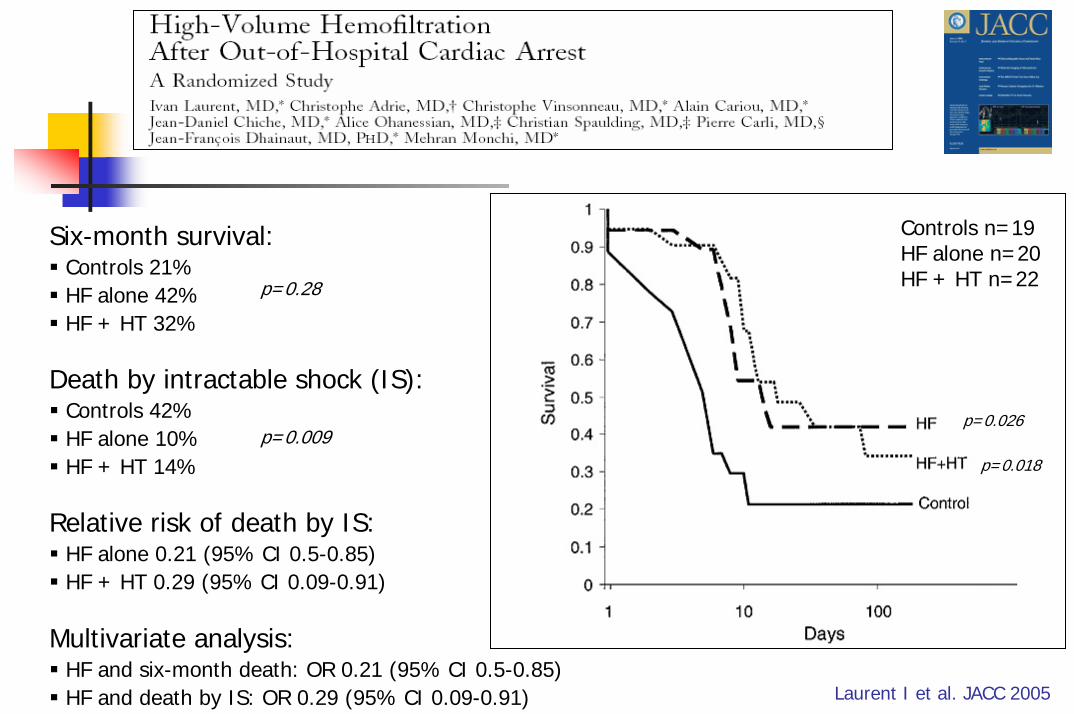
Six-month survival: Controls 21%HF alone 42%HF + HT 32%
p=0.28
Death by intractable shock (IS): Controls 42%HF alone 10%HF + HT 14%
p=0.009
Laurent I et al. JACC 2005
p=0.026
p=0.018
Controls n=19HF alone n=20HF + HT n=22
Multivariate analysis: HF and six-month death: OR 0.21 (95% CI 0.5-0.85)HF and death by IS: OR 0.29 (95% CI 0.09-0.91)
Relative risk of death by IS: HF alone 0.21 (95% CI 0.5-0.85)HF + HT 0.29 (95% CI 0.09-0.91)
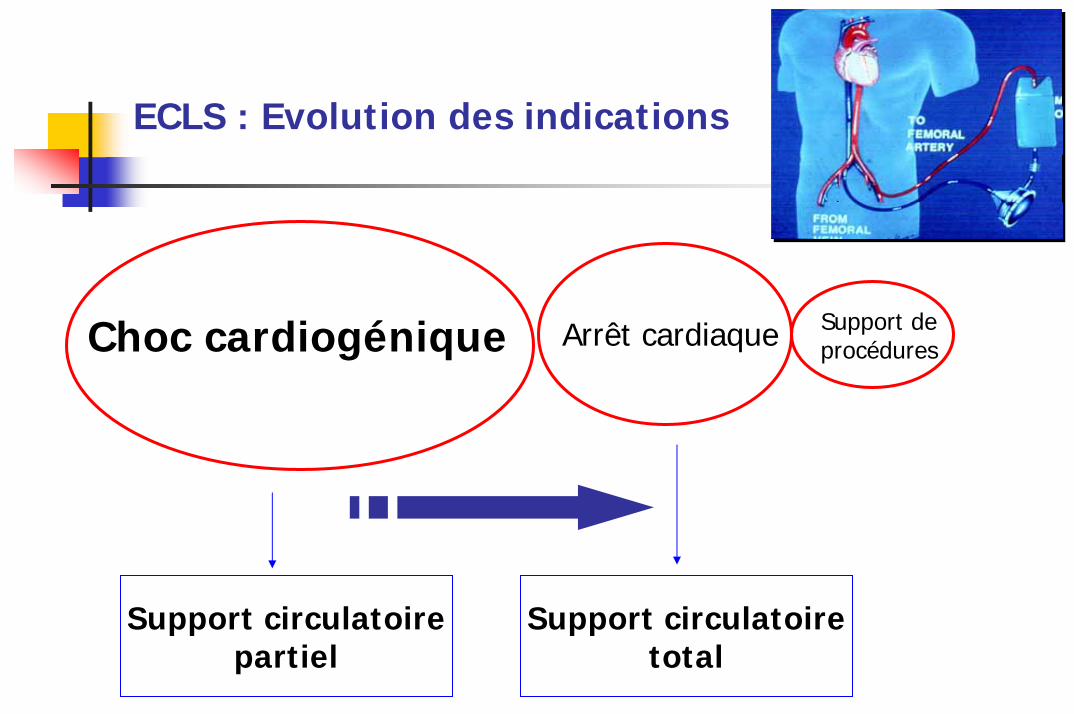
Support circulatoirepartiel
Support circulatoiretotal
Choc cardiogénique Arrêt cardiaque Support de procédures
ECLS : Evolution des indications
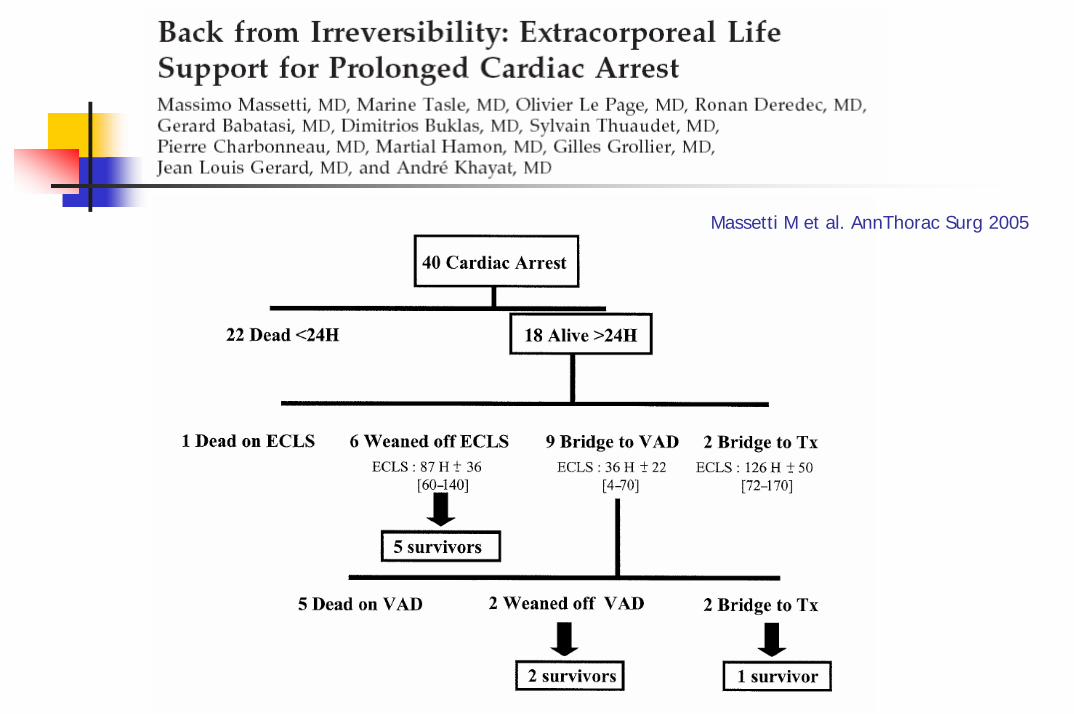
Massetti M et al. AnnThorac Surg 2005

En salle de KT, on ne fait pas que des coros….
LA PHASE TARDIVEL’évaluation du pronostic neurologique
Savoir jeter l’éponge…
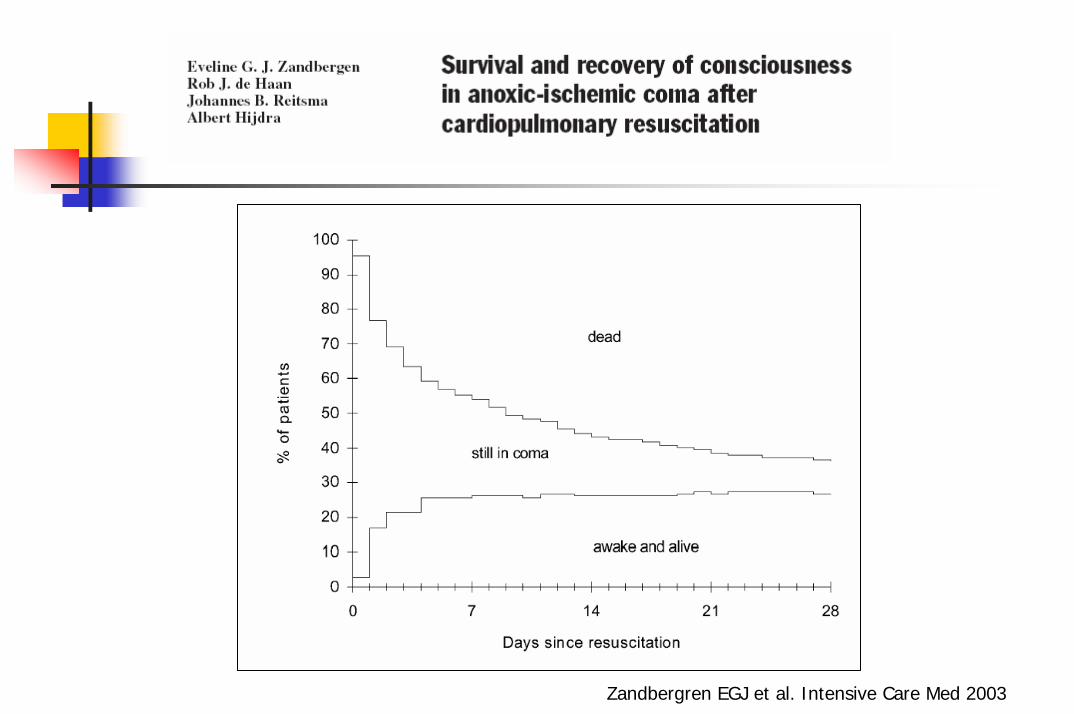
Zandbergren EGJ et al. Intensive Care Med 2003
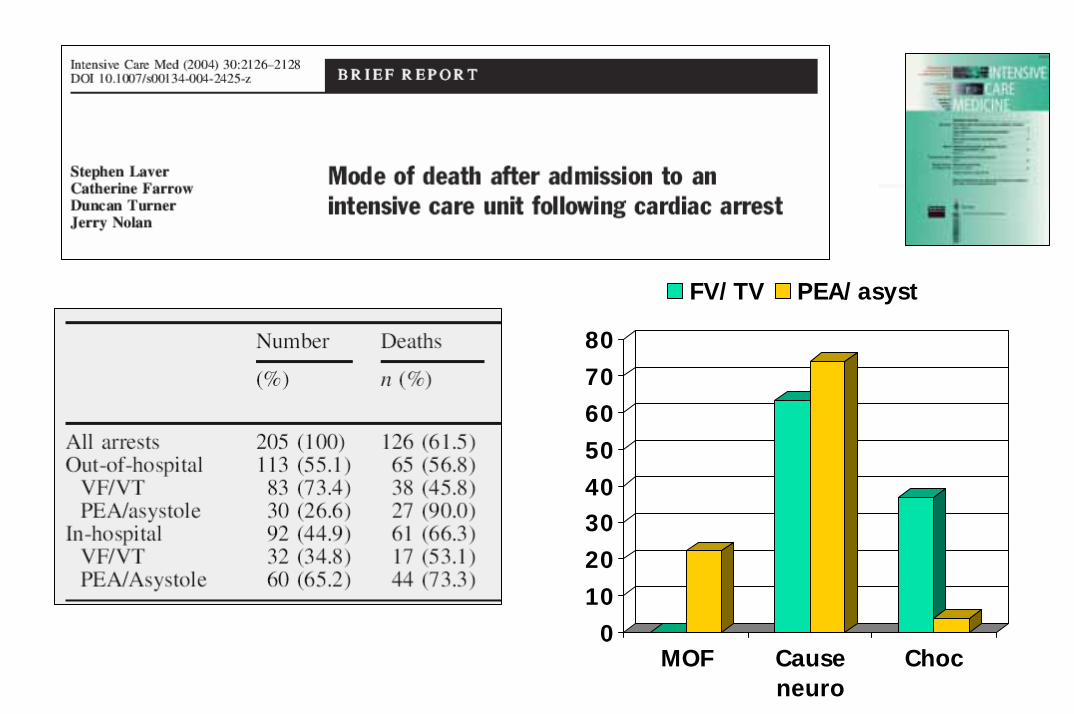
01020304050607080
MOF Causeneuro
Choc
FV/TV PEA/asyst
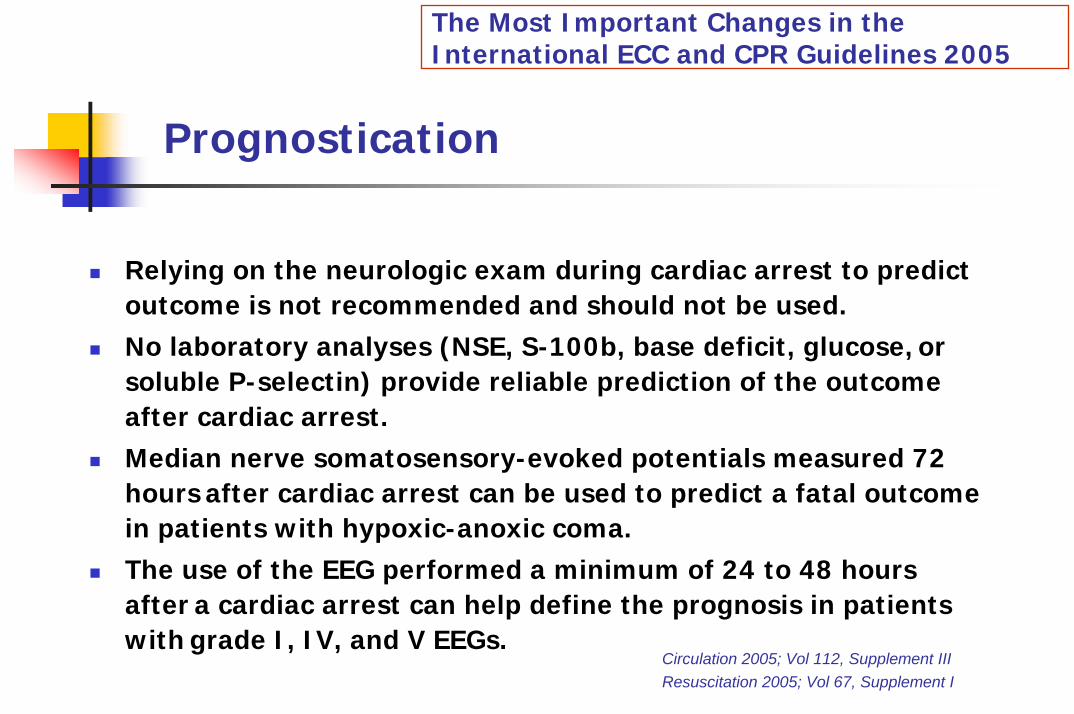
The Most Important Changes in the International ECC and CPR Guidelines 2005
Prognostication
Relying on the neurologic exam during cardiac arrest to predictoutcome is not recommended and should not be used.No laboratory analyses (NSE, S-100b, base deficit, glucose, or soluble P-selectin) provide reliable prediction of the outcomeafter cardiac arrest.Median nerve somatosensory-evoked potentials measured 72 hours after cardiac arrest can be used to predict a fatal outcomein patients with hypoxic-anoxic coma.The use of the EEG performed a minimum of 24 to 48 hours after a cardiac arrest can help define the prognosis in patients with grade I, IV, and V EEGs.
Circulation 2005; Vol 112, Supplement IIIResuscitation 2005; Vol 67, Supplement I
I must say … Brain ismy second favouriteorgan…
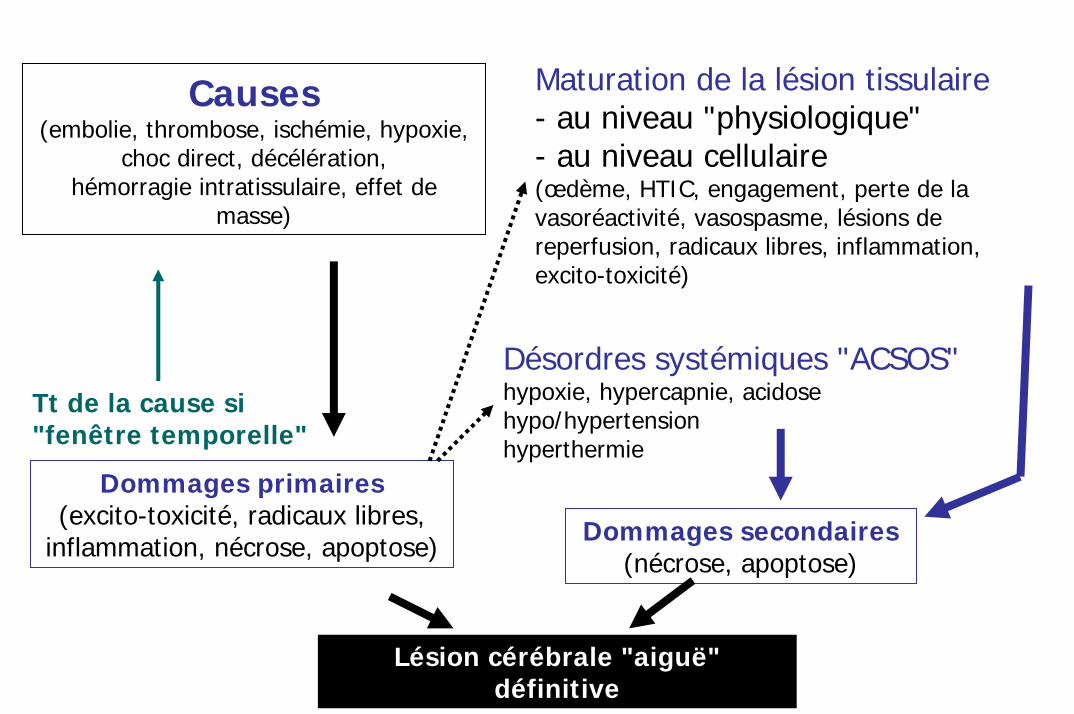
Causes(embolie, thrombose, ischémie, hypoxie,
choc direct, décélération,hémorragie intratissulaire, effet de
masse)
Dommages primaires(excito-toxicité, radicaux libres,
inflammation, nécrose, apoptose)
Tt de la cause si "fenêtre temporelle"
Maturation de la lésion tissulaire- au niveau "physiologique"- au niveau cellulaire(œdème, HTIC, engagement, perte de la vasoréactivité, vasospasme, lésions de reperfusion, radicaux libres, inflammation, excito-toxicité)
Désordres systémiques "ACSOS"hypoxie, hypercapnie, acidosehypo/hypertensionhyperthermie
Dommages secondaires(nécrose, apoptose)
Lésion cérébrale "aiguë" définitive
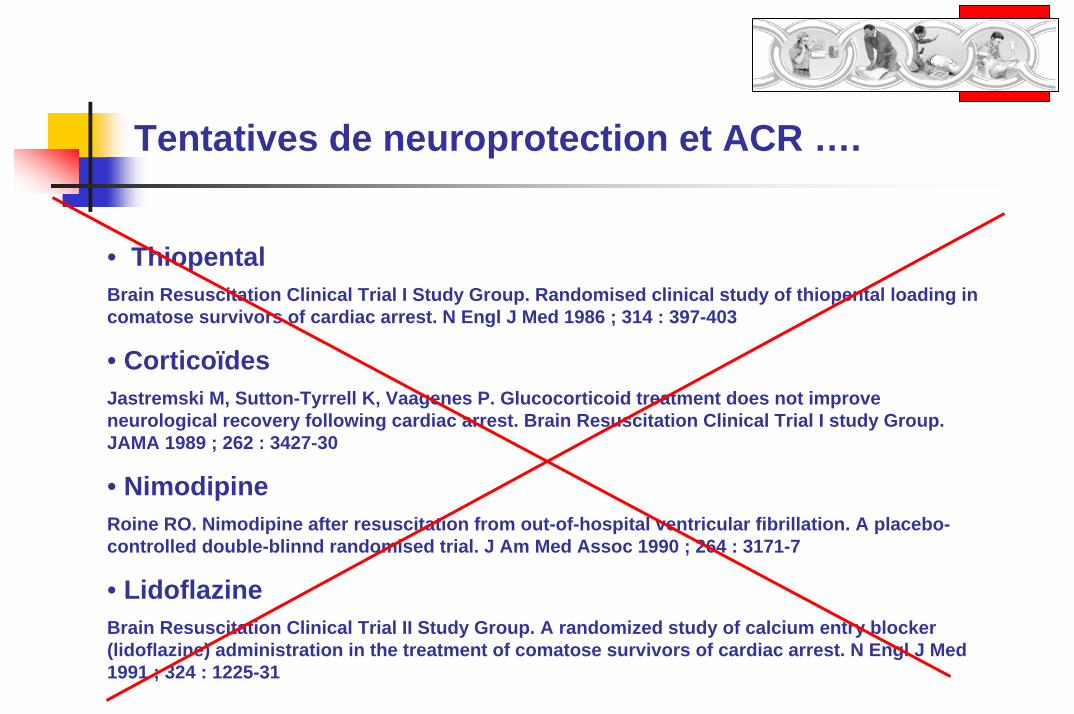
Tentatives de neuroprotection et ACR ….
• ThiopentalBrain Resuscitation Clinical Trial I Study Group. Randomised clinical study of thiopental loading in comatose survivors of cardiac arrest. N Engl J Med 1986 ; 314 : 397-403
• CorticoïdesJastremski M, Sutton-Tyrrell K, Vaagenes P. Glucocorticoid treatment does not improveneurological recovery following cardiac arrest. Brain Resuscitation Clinical Trial I study Group. JAMA 1989 ; 262 : 3427-30
• NimodipineRoine RO. Nimodipine after resuscitation from out-of-hospital ventricular fibrillation. A placebo-controlled double-blinnd randomised trial. J Am Med Assoc 1990 ; 264 : 3171-7
• LidoflazineBrain Resuscitation Clinical Trial II Study Group. A randomized study of calcium entry blocker(lidoflazine) administration in the treatment of comatose survivors of cardiac arrest. N Engl J Med1991 ; 324 : 1225-31
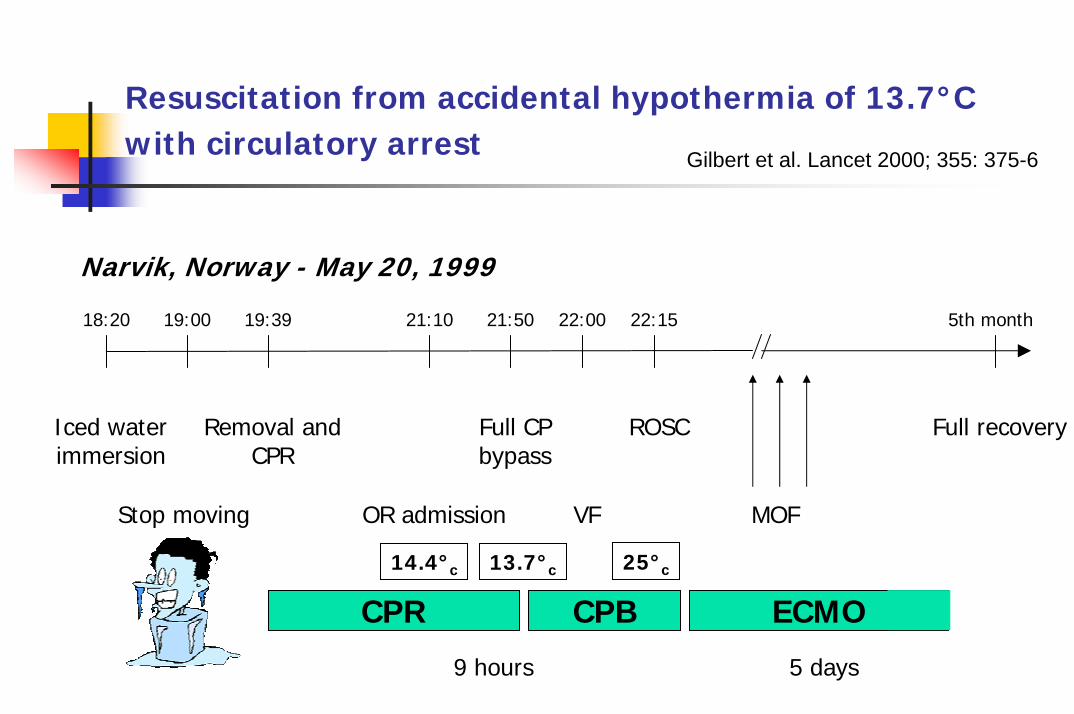
Resuscitation from accidental hypothermia of 13.7°C with circulatory arrest Gilbert et al. Lancet 2000; 355: 375-6
Narvik, Norway - May 20, 1999
18:20 19:00 19:39 21:10 21:50 22:00 22:15 5th month
Iced waterimmersion
Removal andCPR
Full CP bypass
ROSC Full recovery
Stop moving OR admission VF MOF
25°c14.4°c 13.7°c
CPR CPB ECMO
9 hours 5 days
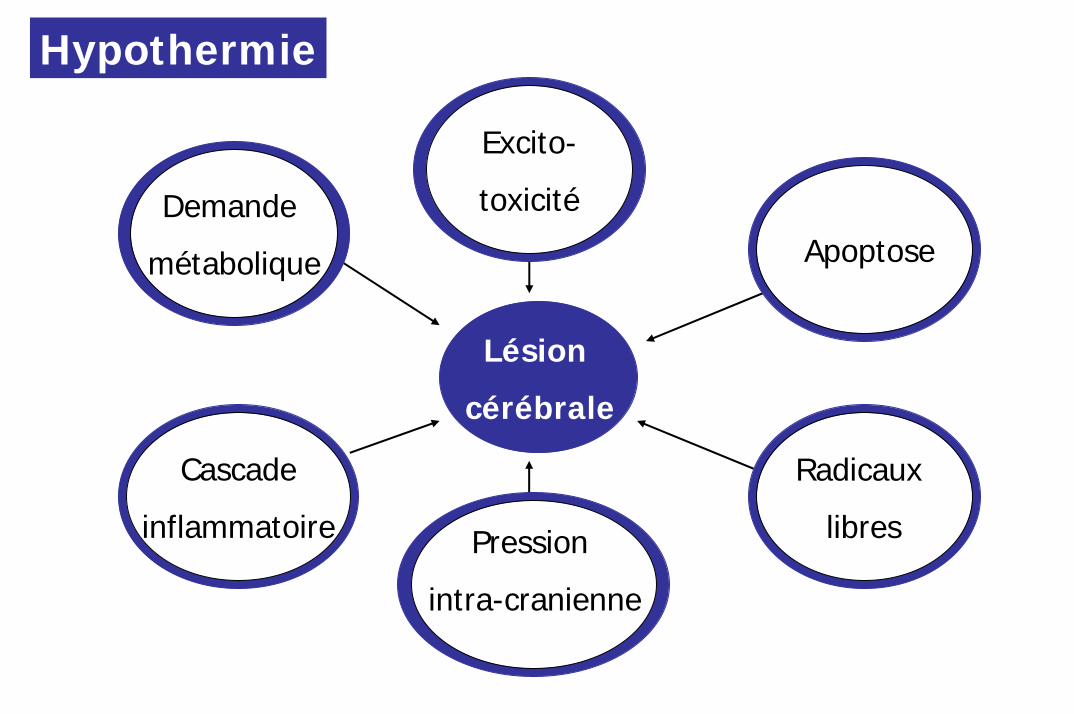
Lésion
cérébrale
Radicaux
libres
Apoptose
Pression
intra-cranienne
Cascade
inflammatoire
Excito-
toxicitéDemande
métabolique
Hypothermie
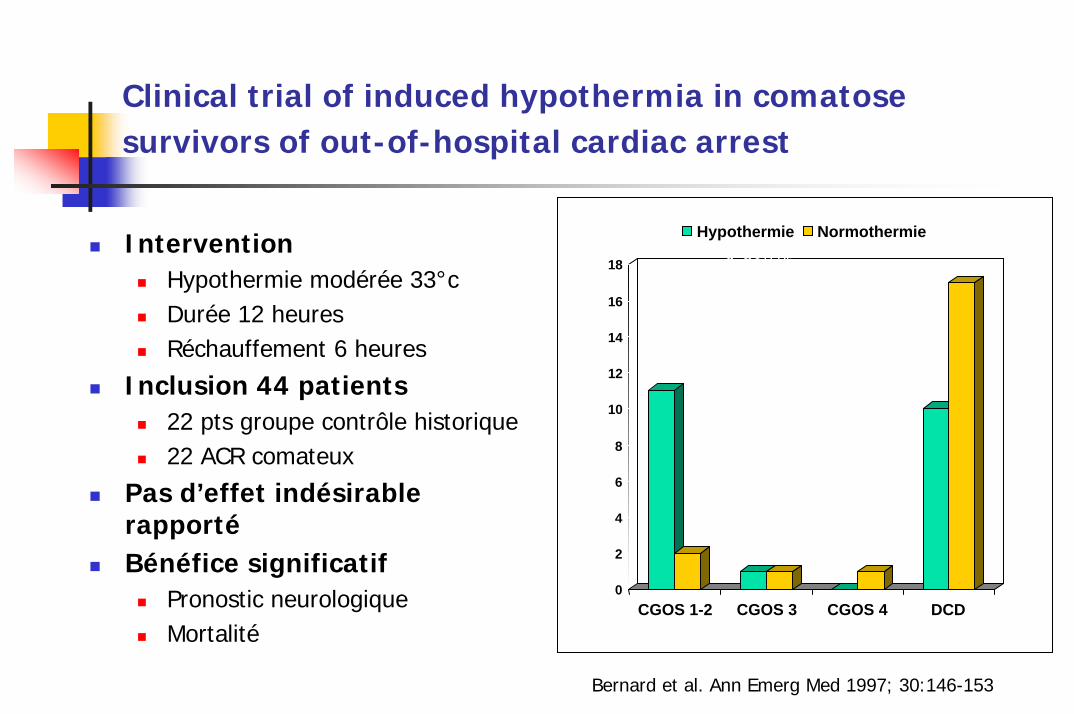
Clinical trial of induced hypothermia in comatose survivors of out-of-hospital cardiac arrest
0
2
4
6
8
10
12
14
16
18
CGOS 1-2 CGOS 3 CGOS 4 DCD
Hypothermie Normothermie
* p<0.05
*
*
InterventionHypothermie modérée 33°cDurée 12 heuresRéchauffement 6 heures
Inclusion 44 patients22 pts groupe contrôle historique22 ACR comateux
Pas d’effet indésirable rapportéBénéfice significatif
Pronostic neurologique Mortalité
Bernard et al. Ann Emerg Med 1997; 30:146-153
P. Safar & PM Kochanek.
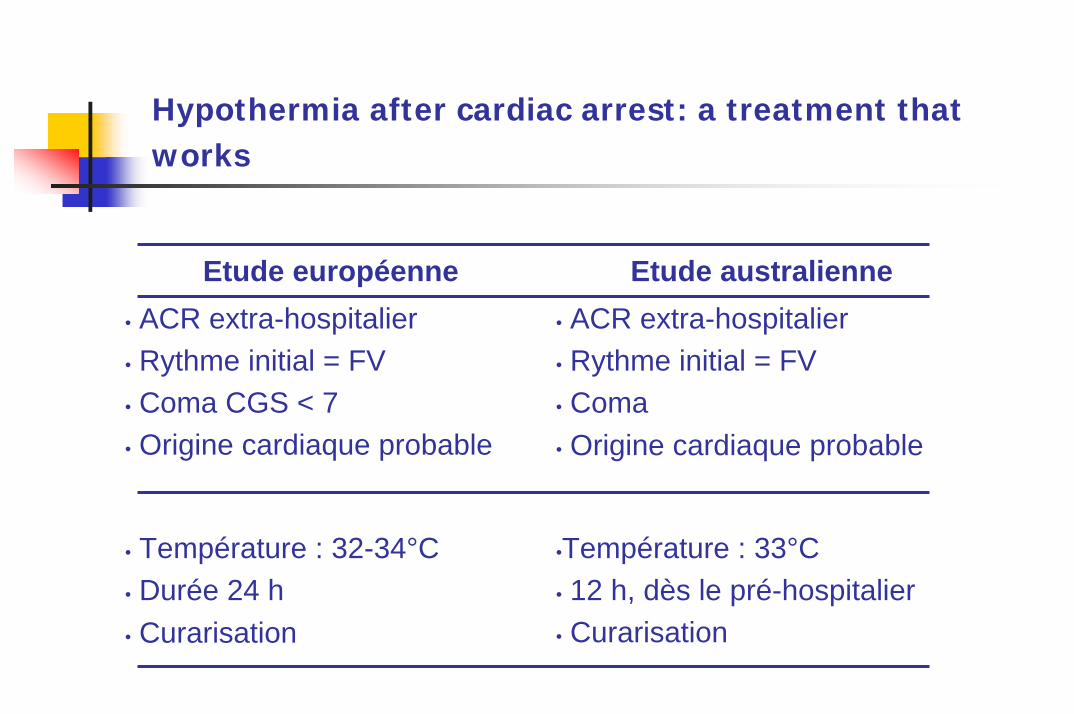
Hypothermia after cardiac arrest: a treatment thatworks
Etude européenne Etude australienne• ACR extra-hospitalier• Rythme initial = FV• Coma CGS < 7• Origine cardiaque probable
• ACR extra-hospitalier• Rythme initial = FV• Coma• Origine cardiaque probable
• Température : 32-34°C • Durée 24 h• Curarisation
•Température : 33°C • 12 h, dès le pré-hospitalier• Curarisation
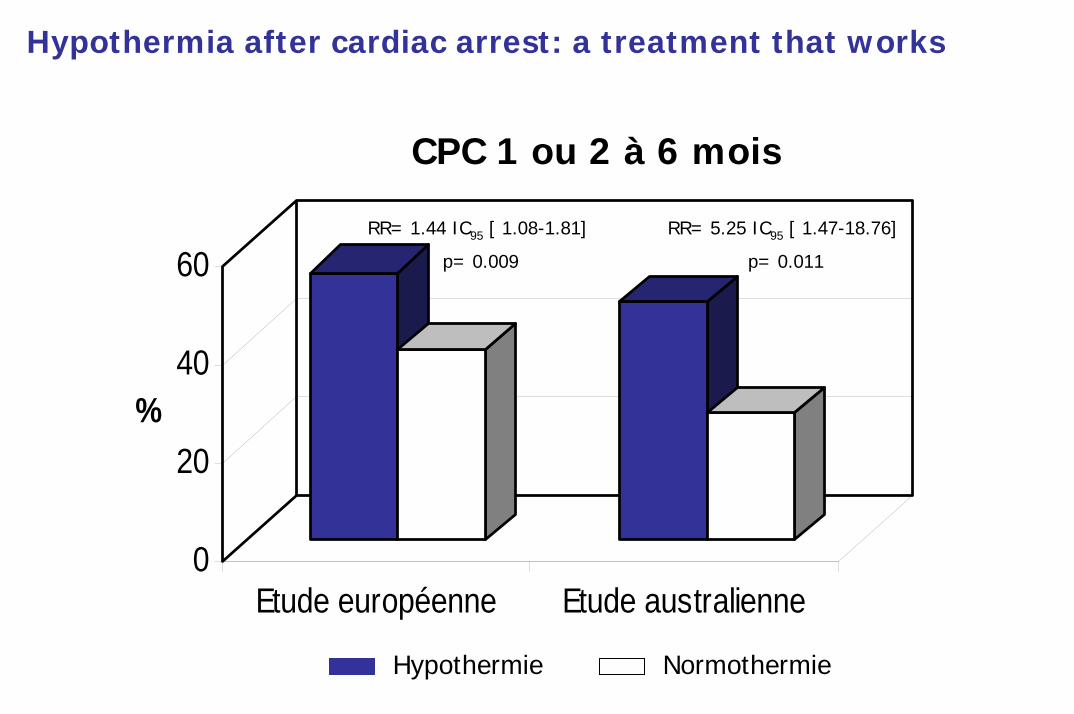
0
20
40
60
%
Etude européenne Etude australienne
RR= 1.44 IC95 [ 1.08-1.81]
p= 0.009
RR= 5.25 IC95 [ 1.47-18.76]
p= 0.011
CPC 1 ou 2 à 6 mois
Hypothermie Normothermie
Hypothermia after cardiac arrest: a treatment that works
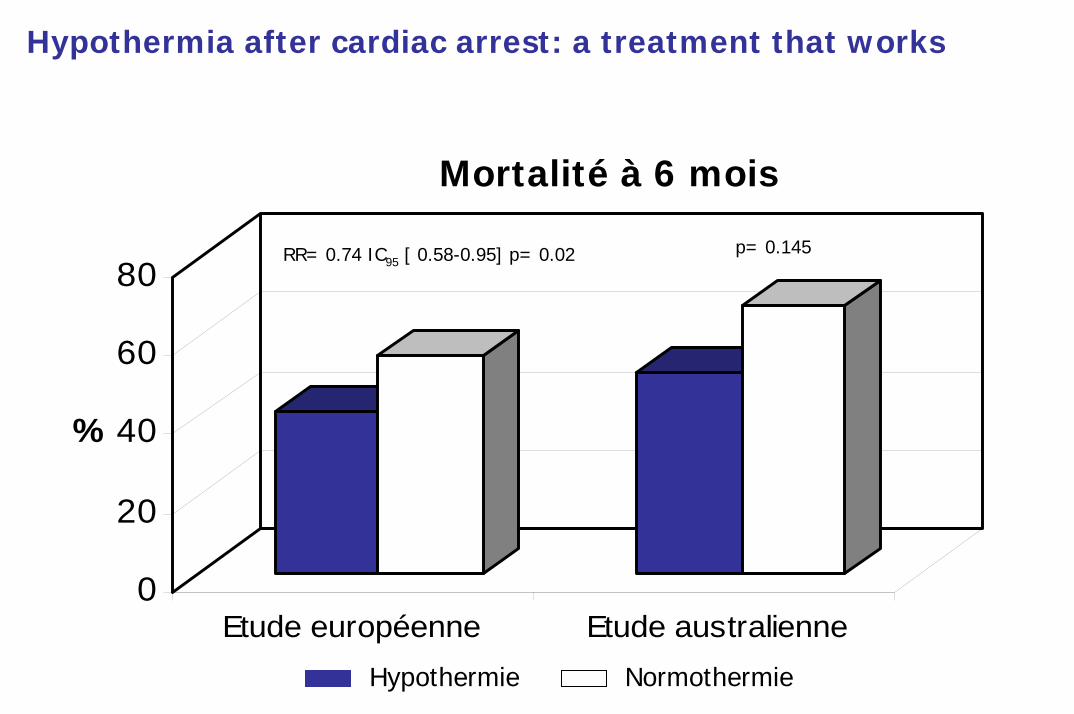
0
20
40
60
80
%
Etude européenne Etude australienneHypothermie Normothermie
p= 0.145
Mortalité à 6 mois
RR= 0.74 IC95 [ 0.58-0.95] p= 0.02
Hypothermia after cardiac arrest: a treatment that works
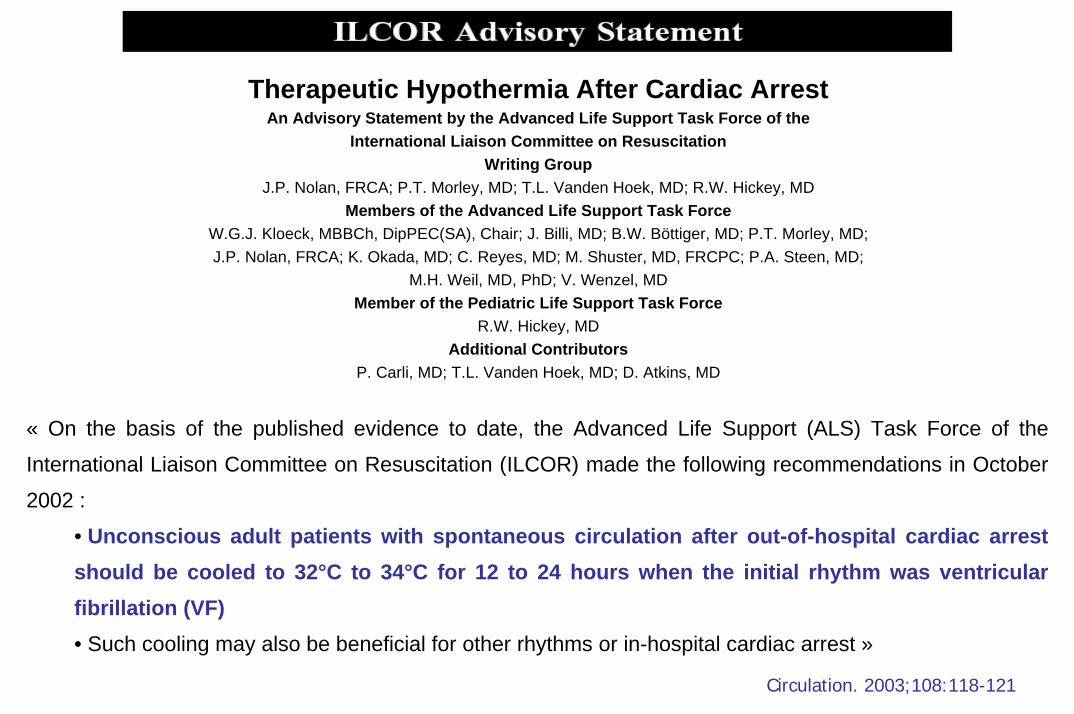
Therapeutic Hypothermia After Cardiac ArrestAn Advisory Statement by the Advanced Life Support Task Force of the
International Liaison Committee on ResuscitationWriting Group
J.P. Nolan, FRCA; P.T. Morley, MD; T.L. Vanden Hoek, MD; R.W. Hickey, MDMembers of the Advanced Life Support Task Force
W.G.J. Kloeck, MBBCh, DipPEC(SA), Chair; J. Billi, MD; B.W. Böttiger, MD; P.T. Morley, MD;J.P. Nolan, FRCA; K. Okada, MD; C. Reyes, MD; M. Shuster, MD, FRCPC; P.A. Steen, MD;
M.H. Weil, MD, PhD; V. Wenzel, MDMember of the Pediatric Life Support Task Force
R.W. Hickey, MDAdditional Contributors
P. Carli, MD; T.L. Vanden Hoek, MD; D. Atkins, MD
« On the basis of the published evidence to date, the Advanced Life Support (ALS) Task Force of the
International Liaison Committee on Resuscitation (ILCOR) made the following recommendations in October
2002 :
• Unconscious adult patients with spontaneous circulation after out-of-hospital cardiac arrestshould be cooled to 32°C to 34°C for 12 to 24 hours when the initial rhythm was ventricularfibrillation (VF)• Such cooling may also be beneficial for other rhythms or in-hospital cardiac arrest »
Circulation. 2003;108:118-121
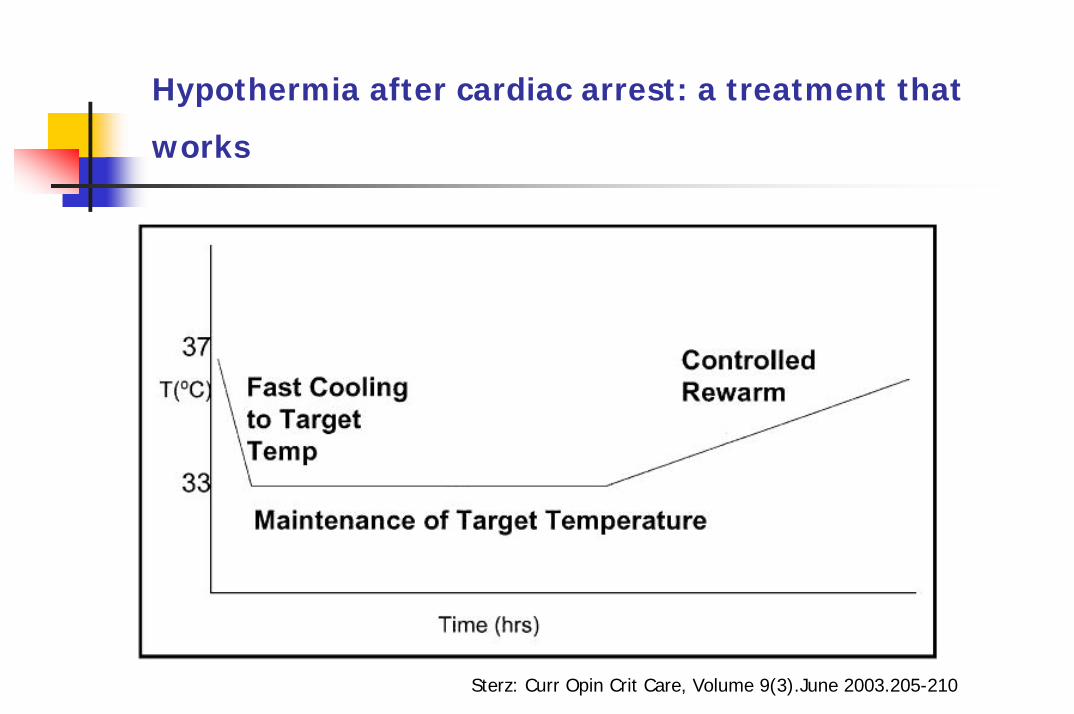
Hypothermia after cardiac arrest: a treatment that
works
Sterz: Curr Opin Crit Care, Volume 9(3).June 2003.205-210
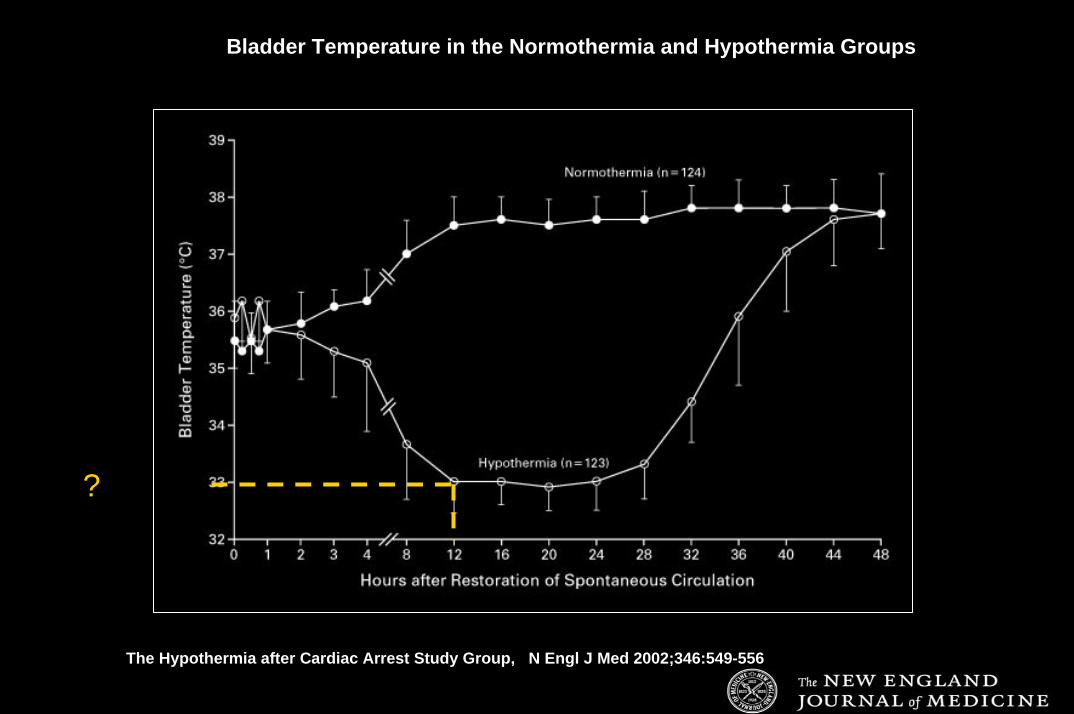
?
The Hypothermia after Cardiac Arrest Study Group, N Engl J Med 2002;346:549-556
Bladder Temperature in the Normothermia and Hypothermia Groups
?
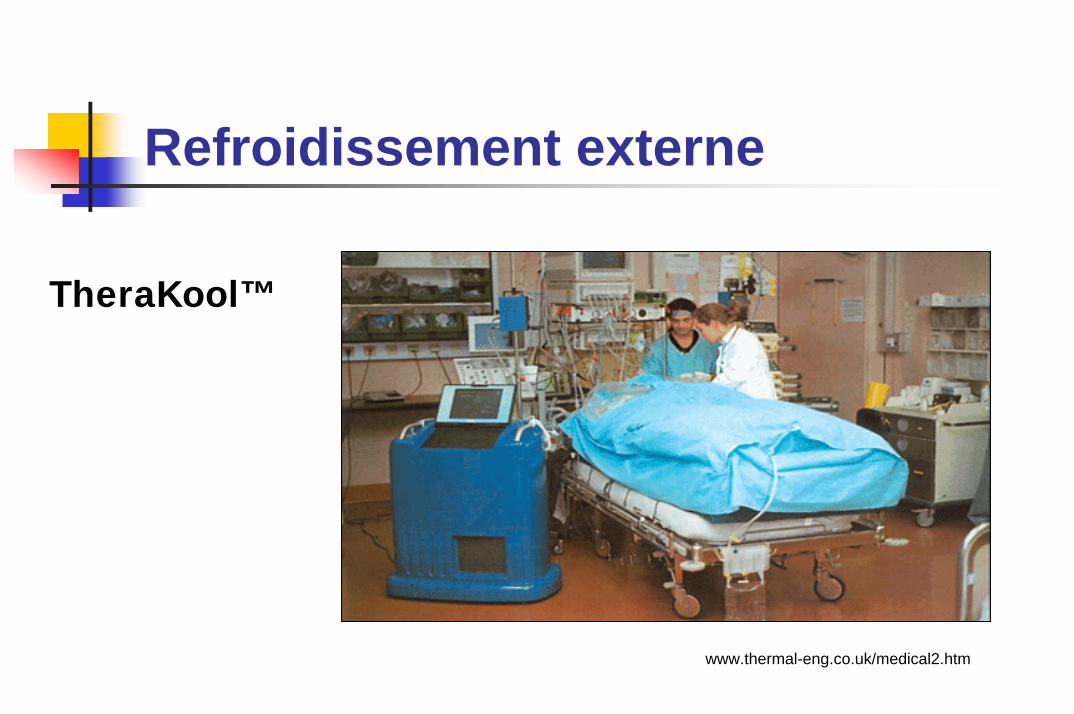
Refroidissement externe
TheraKool™
www.thermal-eng.co.uk/medical2.htm
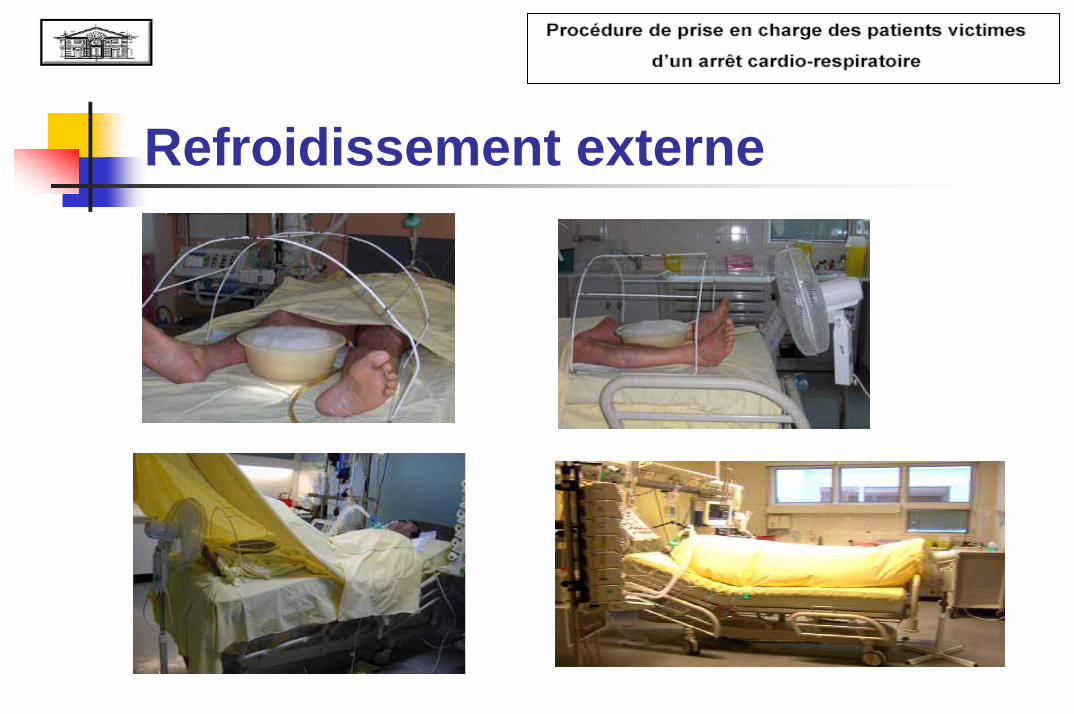
Refroidissement externe
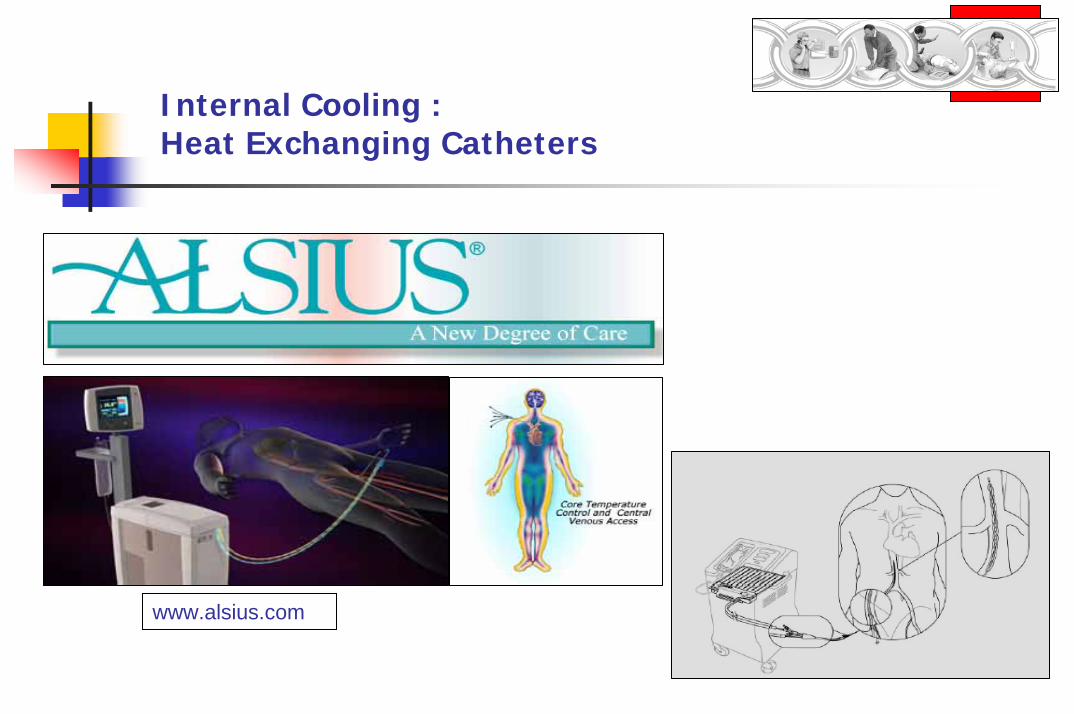
Internal Cooling : Heat Exchanging Catheters
www.alsius.com
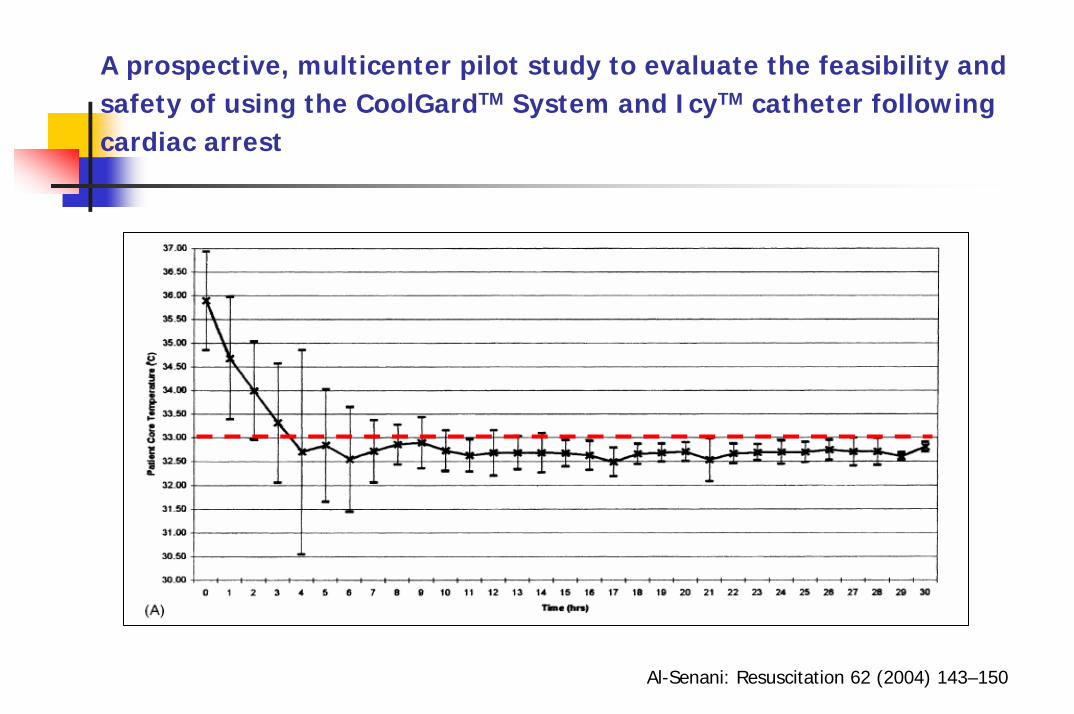
A prospective, multicenter pilot study to evaluate the feasibility andsafety of using the CoolGardTM System and IcyTM catheter followingcardiac arrest
Al-Senani: Resuscitation 62 (2004) 143–150
Intérêt clinique du refroidissement par cathétérisme endovasculaire à la phase précoce de l’arrêt cardiaque : impact
sur la mortalité et impact médico-économique
Investigateur Coordonnateur: Pr F. BaudInvestigateurs associés : Dr N. Deye & A. CariouMéthodologie et Statistique & Monitoring : Pr E. VicautEconomiste : Pr R. LaunoisPromoteur : AP-HP
PHRC 2005
Objectif principal : Amélioration du pronostic à l’aide du refroidissement endovasculaire comparativement à la technique conventionnelle externe de refroidissement
Neuroprotection post-arrêt cardiaque
Dessin : Étude prospective multicentrique randomisée
Calendrier : Début des inclusions 2ème semestre 2006
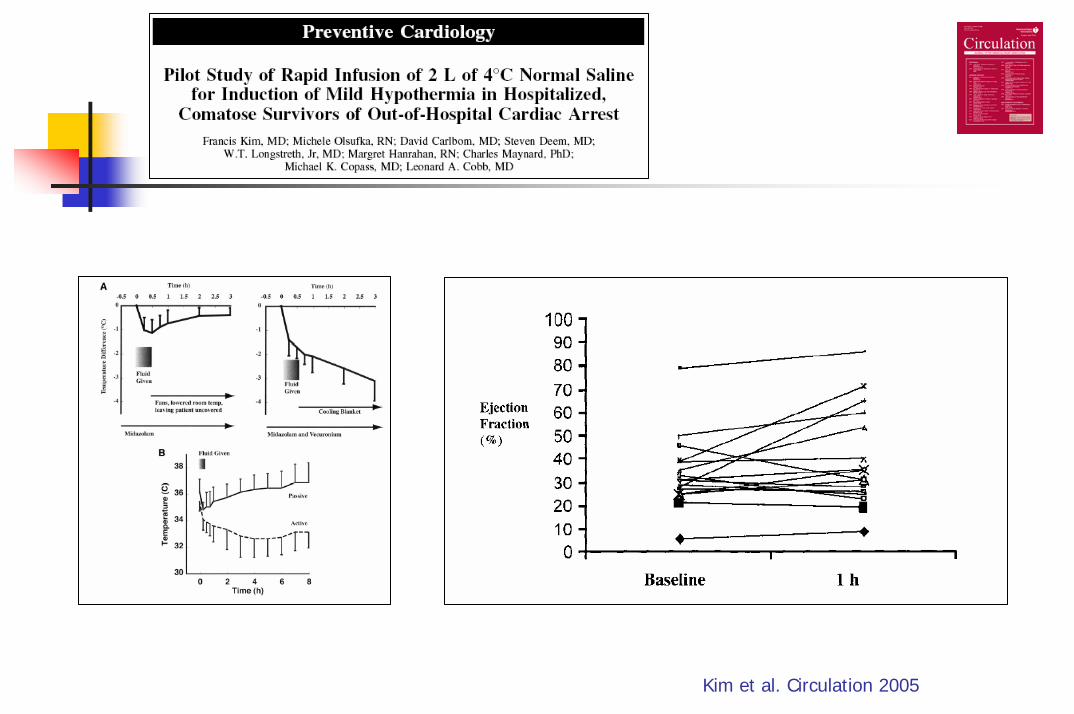
Kim et al. Circulation 2005
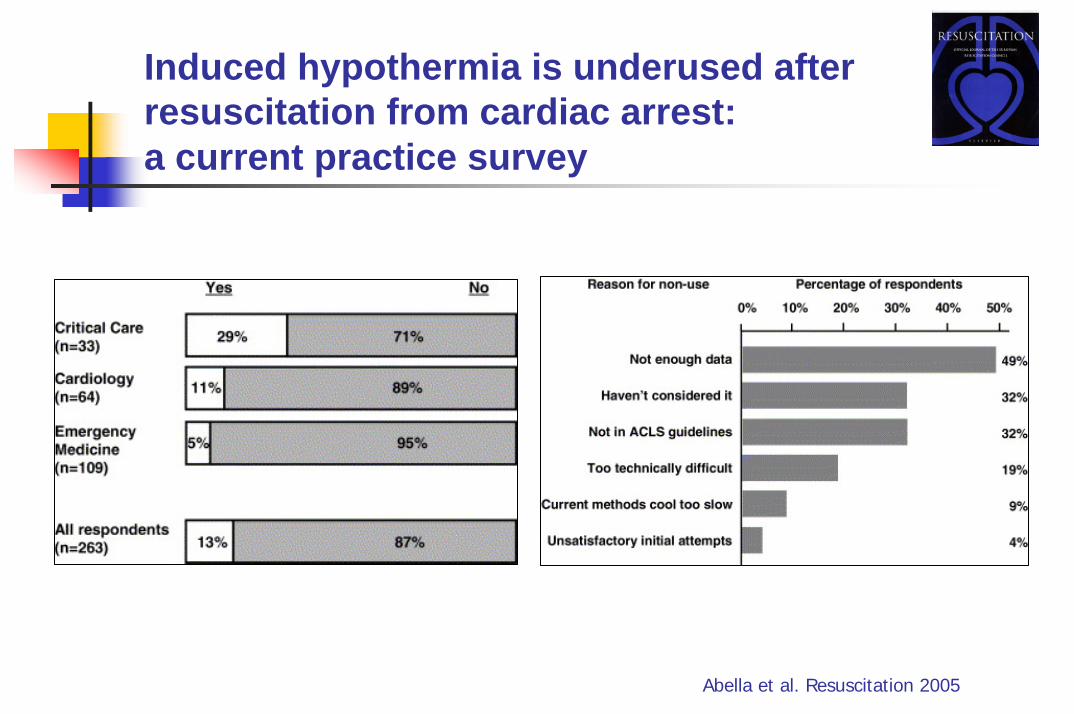
Induced hypothermia is underused after resuscitation from cardiac arrest: a current practice survey
Abella et al. Resuscitation 2005
Langhelle et al. Resuscitation 2005