Embed Size (px)
Citation preview

Prof. Saeed Abuel Makarem
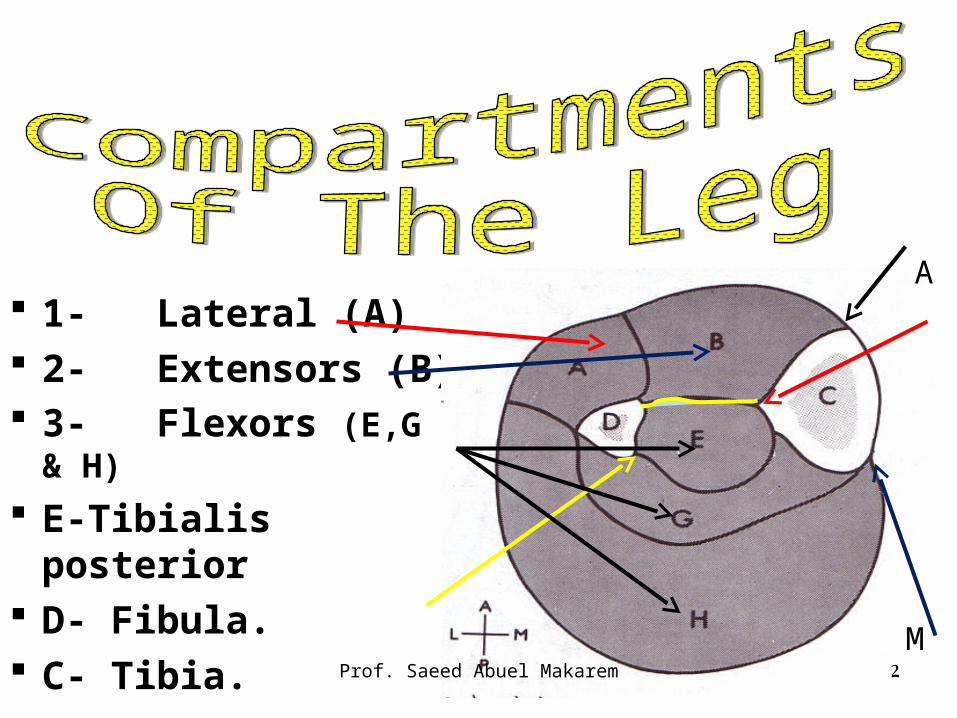
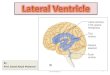
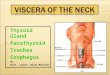
1- Lateral (A) 2- Extensors (B) 3- Flexors (E,G & H)
E-Tibialis posterior D- Fibula. C- Tibia.
2Prof. Saeed Abuel Makarem
A
M
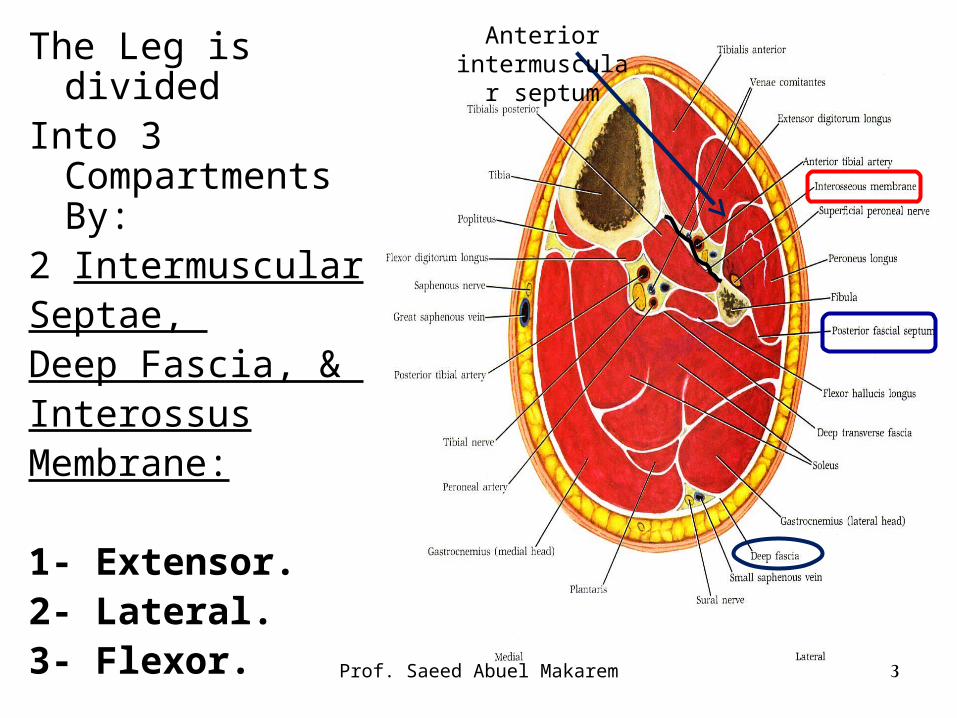
The Leg is dividedInto 3
Compartments By:
2 IntermuscularSeptae, Deep Fascia, & InterossusMembrane:
1- Extensor.2- Lateral.3- Flexor.
3Prof. Saeed Abuel Makarem
Anterior intermuscular
septum
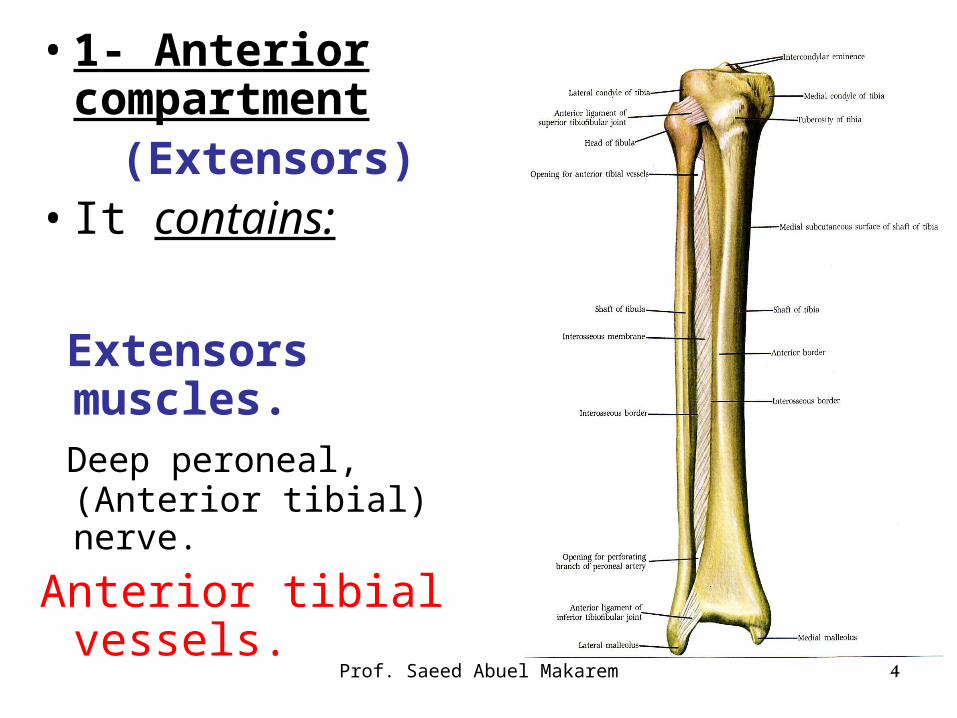
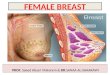
• 1- Anterior compartment
(Extensors)• It contains:
Extensors muscles.
Deep peroneal, (Anterior tibial) nerve.
Anterior tibial vessels.
4Prof. Saeed Abuel Makarem
Prof. Saeed Abuel Makarem 5
2- Lateral compartment (Peroneal)
It contains:
Peroneus Longus and brevis muscles.
Superficial peroneal, (musculocutaneous) nerve.
Branches from peroneal artery.
Prof. Saeed Abuel Makarem 6
3- Posterior compartment (Flexors)
It contains:
Flexors muscles.
Posterior tibial vessels,
Posterior tibial nerve (tibial nerve).
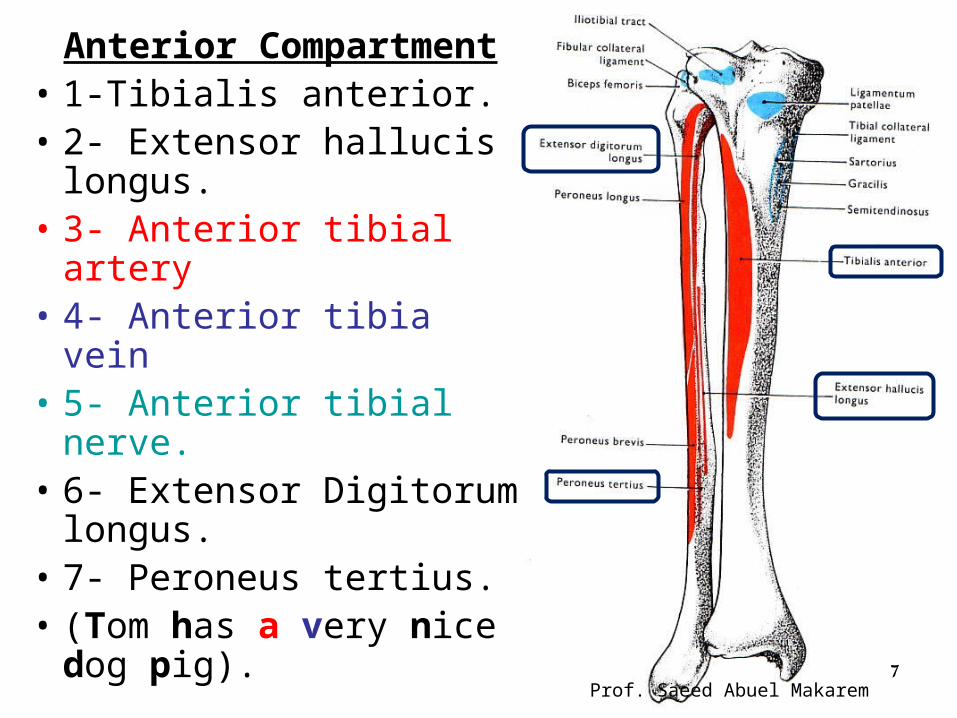
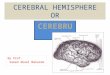
Anterior Compartment• 1-Tibialis anterior.• 2- Extensor hallucis
longus.• 3- Anterior tibial artery• 4- Anterior tibia vein• 5- Anterior tibial nerve.• 6- Extensor Digitorum
longus.• 7- Peroneus tertius.• (Tom has a very nice
dog pig).7
Prof. Saeed Abuel Makarem
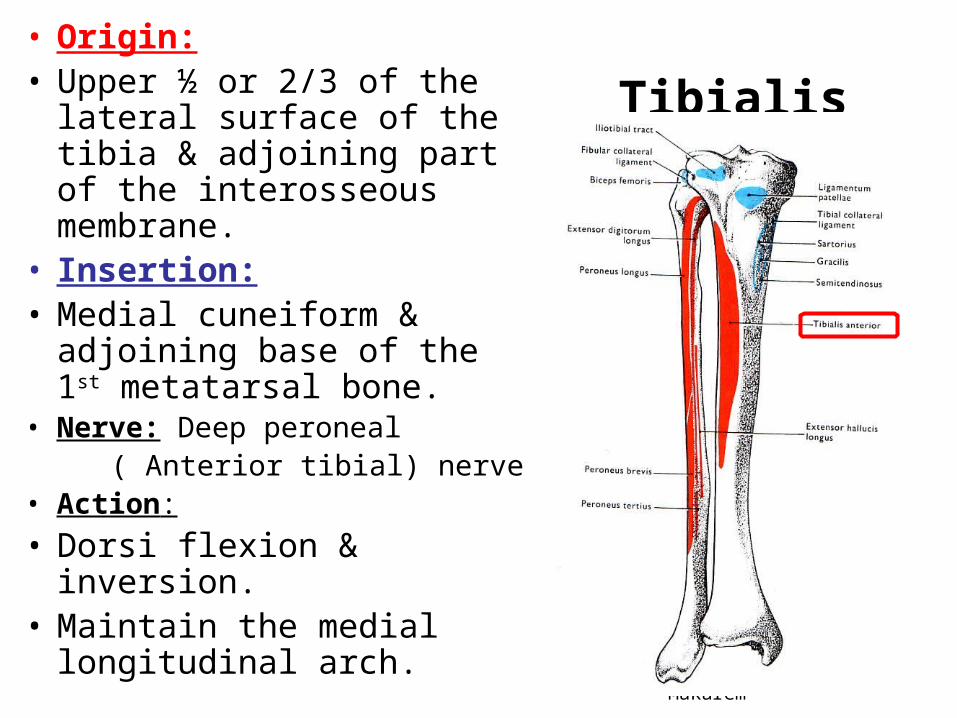
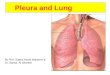
Tibialis Anterior• Origin: • Upper ½ or 2/3 of the lateral
surface of the tibia & adjoining part of the interosseous membrane.
• Insertion: • Medial cuneiform &
adjoining base of the 1st metatarsal bone.
• Nerve: Deep peroneal ( Anterior tibial) nerve• Action:
• Dorsi flexion & inversion.• Maintain the medial
longitudinal arch.Prof. Saeed Abuel Makarem 8
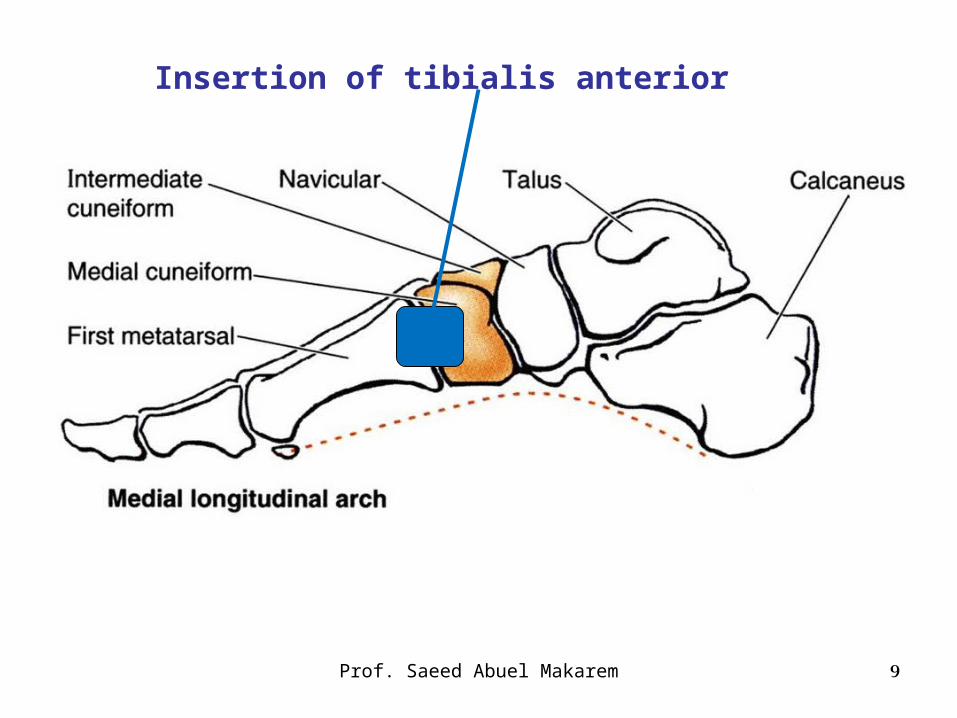
Prof. Saeed Abuel Makarem 9
Insertion of tibialis anterior
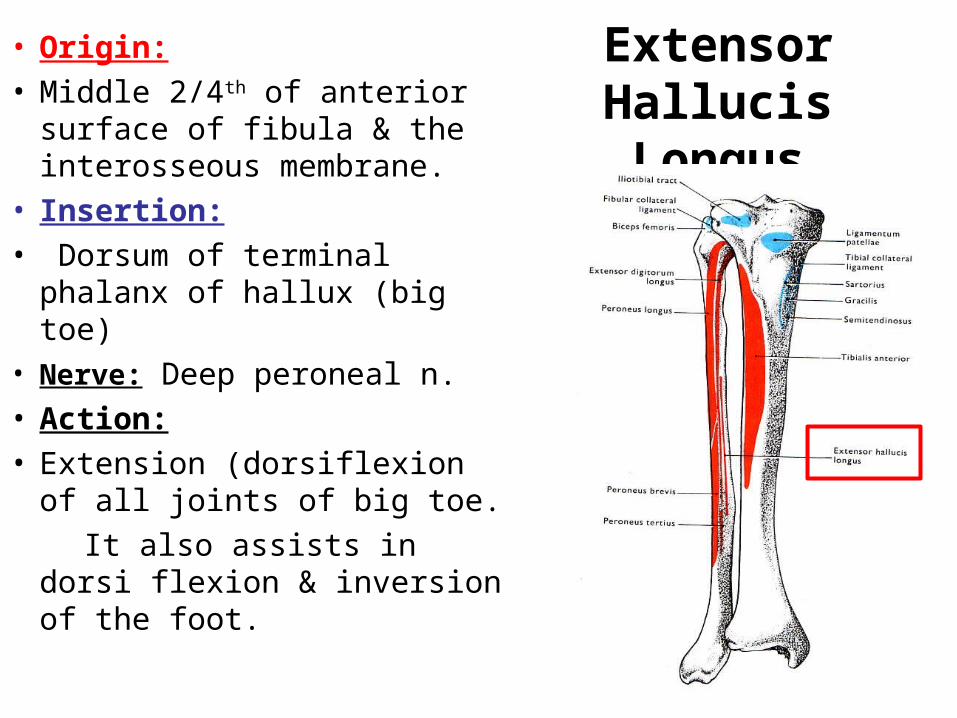
Extensor Hallucis Longus
• Origin: • Middle 2/4th of anterior
surface of fibula & the interosseous membrane.
• Insertion: • Dorsum of terminal phalanx
of hallux (big toe)• Nerve: Deep peroneal n.• Action:• Extension (dorsiflexion of all
joints of big toe.
It also assists in dorsi flexion & inversion of the foot.
10
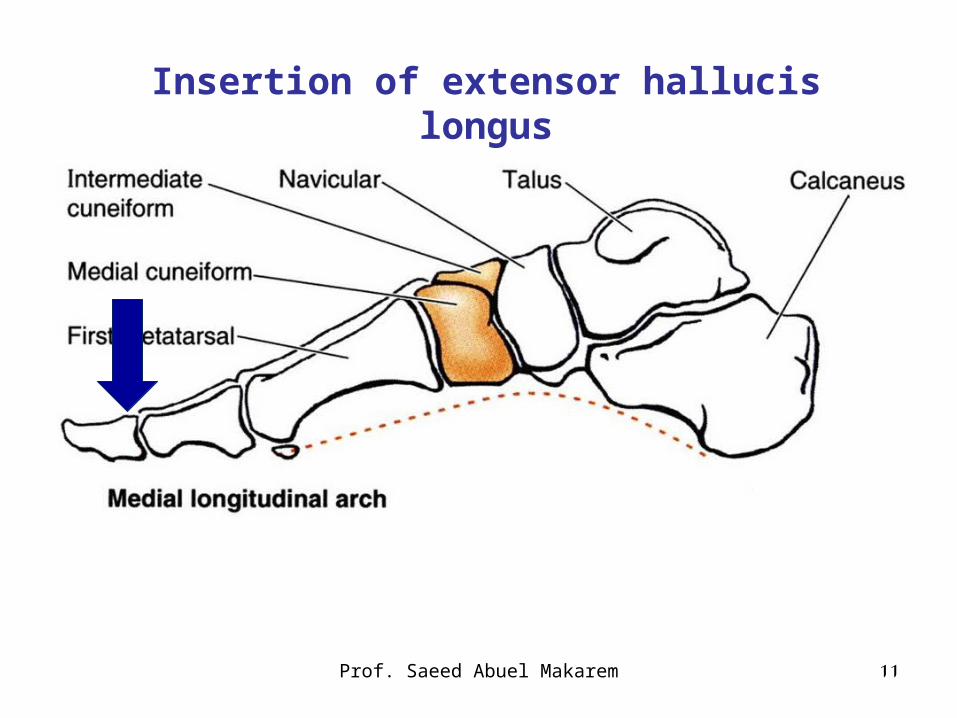
Prof. Saeed Abuel Makarem 11
Insertion of extensor hallucis longus
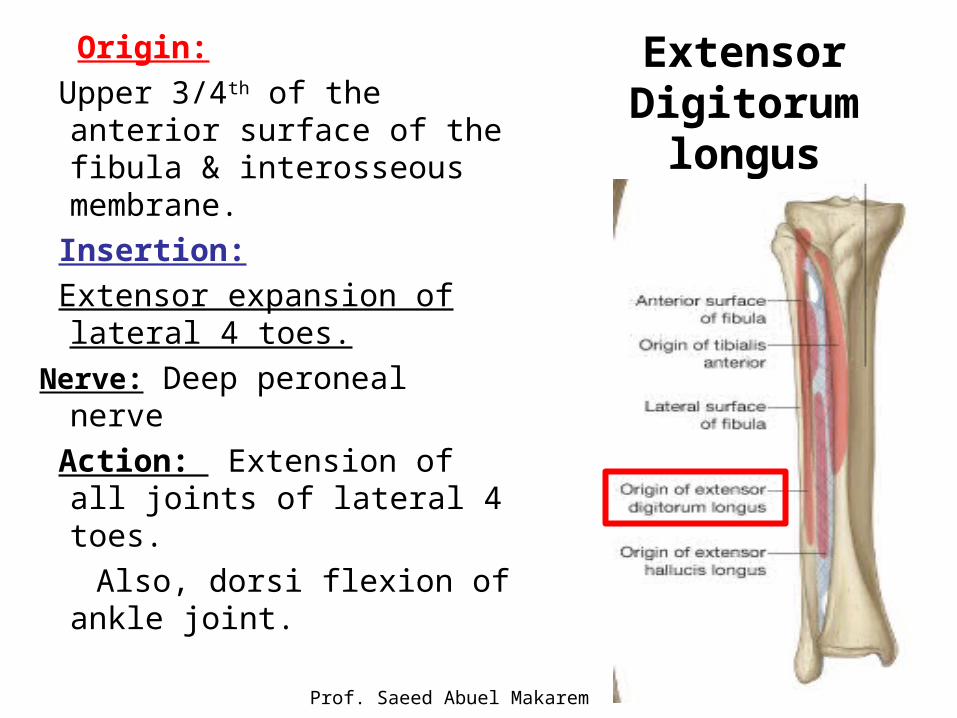
Extensor Digitorum longus
Origin:
Upper 3/4th of the anterior surface of the fibula & interosseous membrane.
Insertion:
Extensor expansion of lateral 4 toes.
Nerve: Deep peroneal nerve
Action: Extension of all joints of lateral 4 toes.
Also, dorsi flexion of ankle joint.
Prof. Saeed Abuel Makarem
12
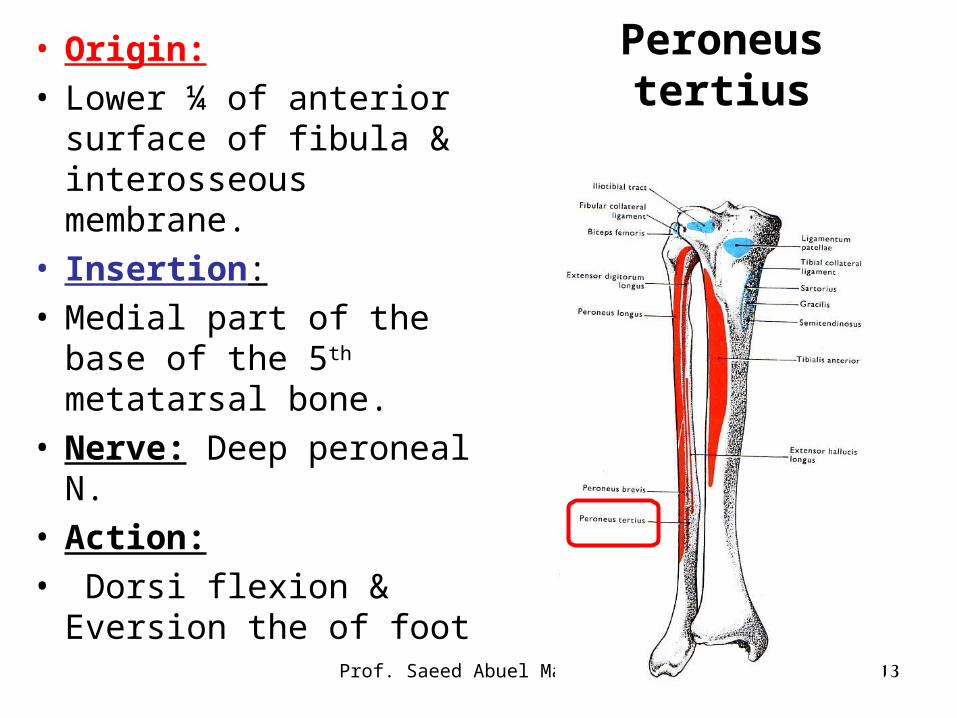
Peroneus tertius• Origin: • Lower ¼ of anterior
surface of fibula & interosseous membrane.
• Insertion: • Medial part of the base of
the 5th metatarsal bone.• Nerve: Deep peroneal N.• Action:• Dorsi flexion & Eversion
the of foot
Prof. Saeed Abuel Makarem 13
Prof. Saeed Abuel Makarem 14
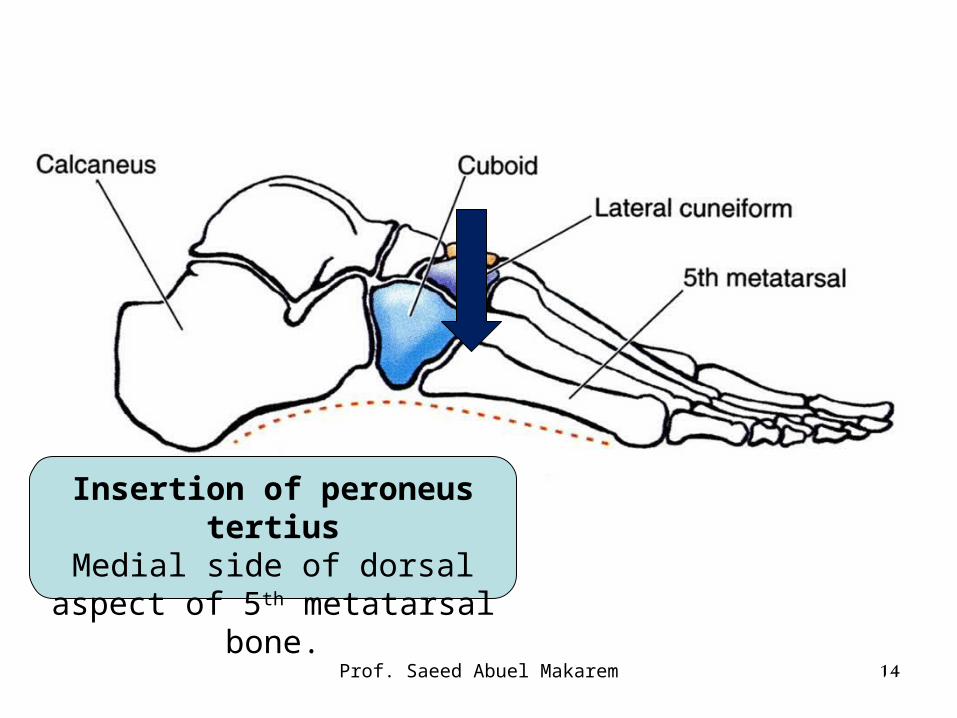
Insertion of peroneus tertiusMedial side of dorsal aspect of
5th metatarsal bone.
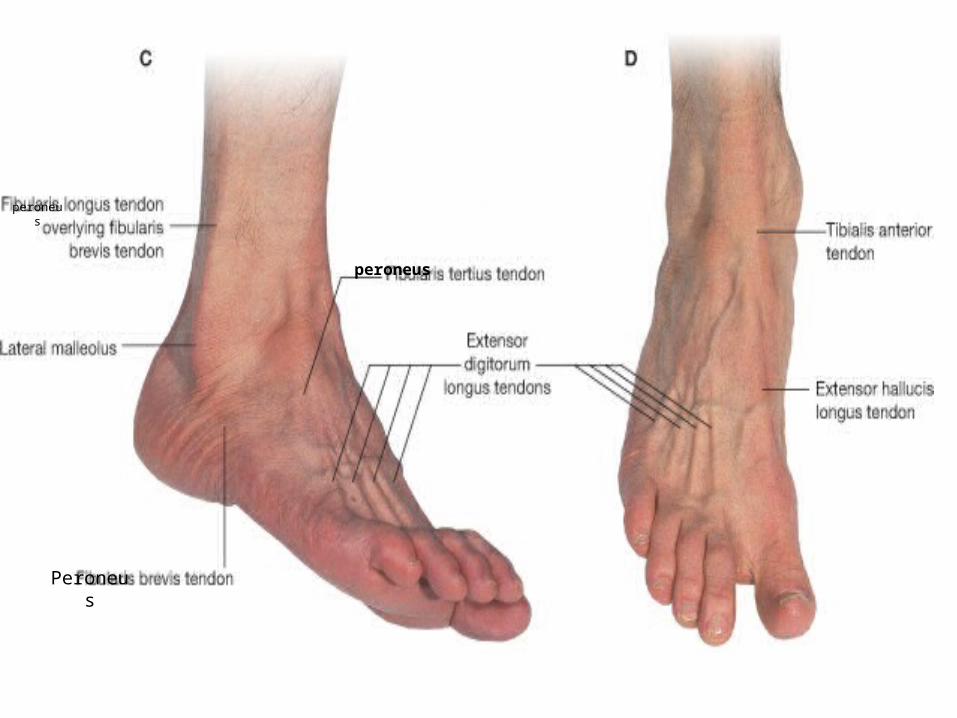
peroneus
Peroneus
peroneus
Prof. Saeed Abuel Makarem 16
NB.Dorsi flexion & Planter flexion occur in the ankle joint.
While Eversion & Inversion occur in the subtalar & transverse tarsal joints or (Tallo-calcenio-navicular joints).
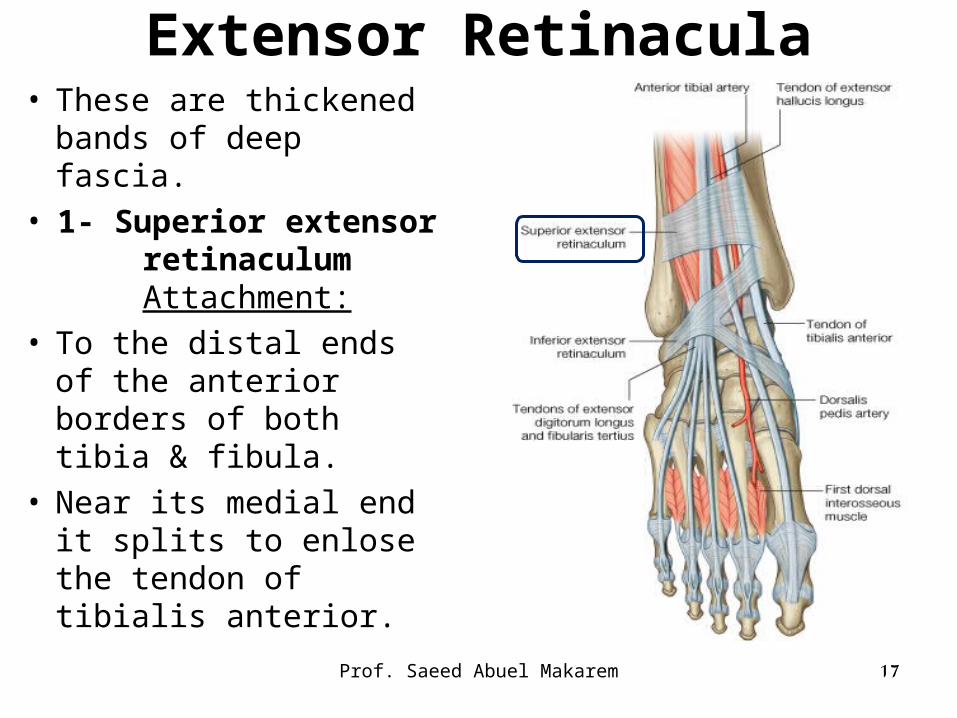
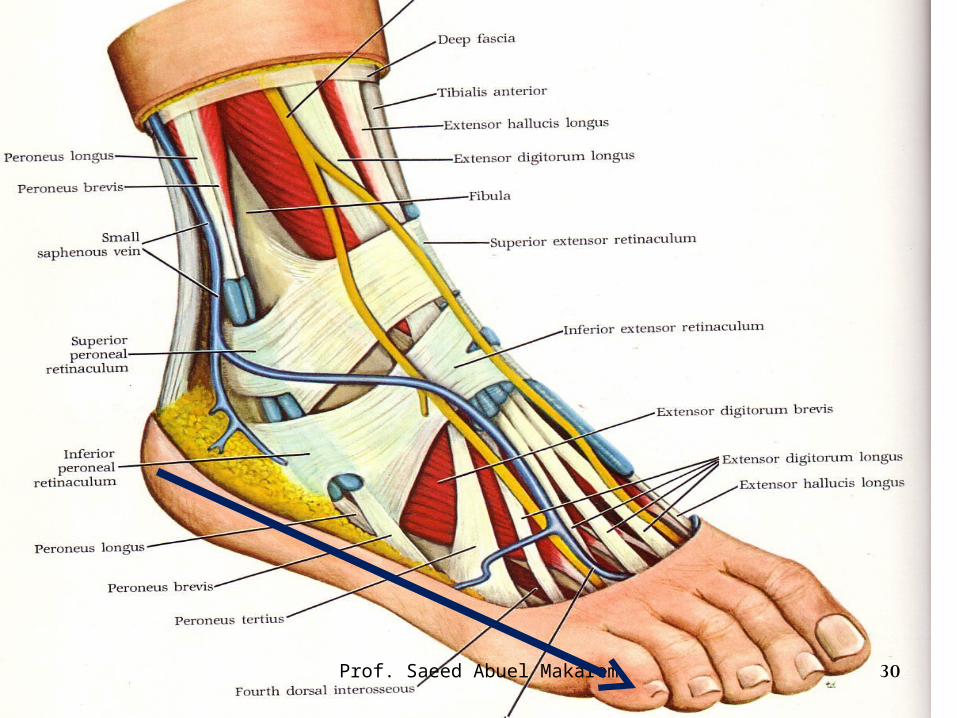
Extensor Retinacula• These are thickened
bands of deep fascia.• 1- Superior extensor
retinaculum Attachment:
• To the distal ends of the anterior borders of both tibia & fibula.
• Near its medial end it splits to enlose the tendon of tibialis anterior.
Prof. Saeed Abuel Makarem 17
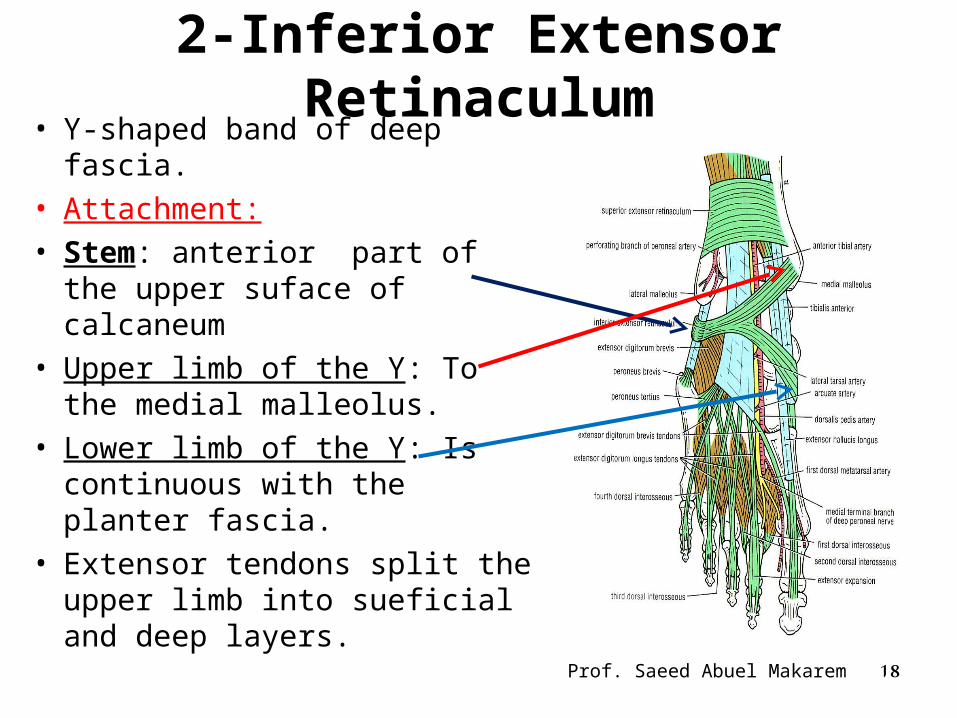
2-Inferior Extensor Retinaculum• Y-shaped band of deep fascia.• Attachment:• Stem: anterior part of the
upper suface of calcaneum• Upper limb of the Y: To the
medial malleolus.• Lower limb of the Y: Is
continuous with the planter fascia.
• Extensor tendons split the upper limb into sueficial and deep layers.
Prof. Saeed Abuel Makarem 18
19Prof. Saeed Abuel Makarem
Lateral Compartment
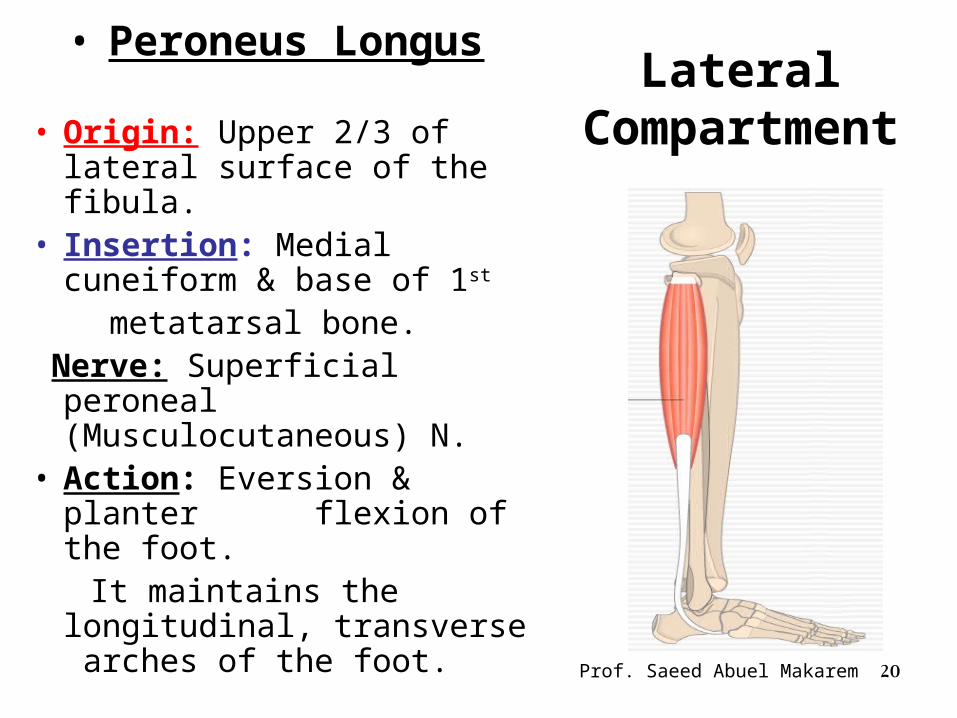
• Peroneus Longus
• Origin: Upper 2/3 of lateral surface of the fibula.
• Insertion: Medial cuneiform & base of 1st
metatarsal bone. Nerve: Superficial peroneal
(Musculocutaneous) N.• Action: Eversion & planter
flexion of the foot. It maintains the longitudinal,
transverse arches of the foot.
Prof. Saeed Abuel Makarem 20
Lateral Compartment
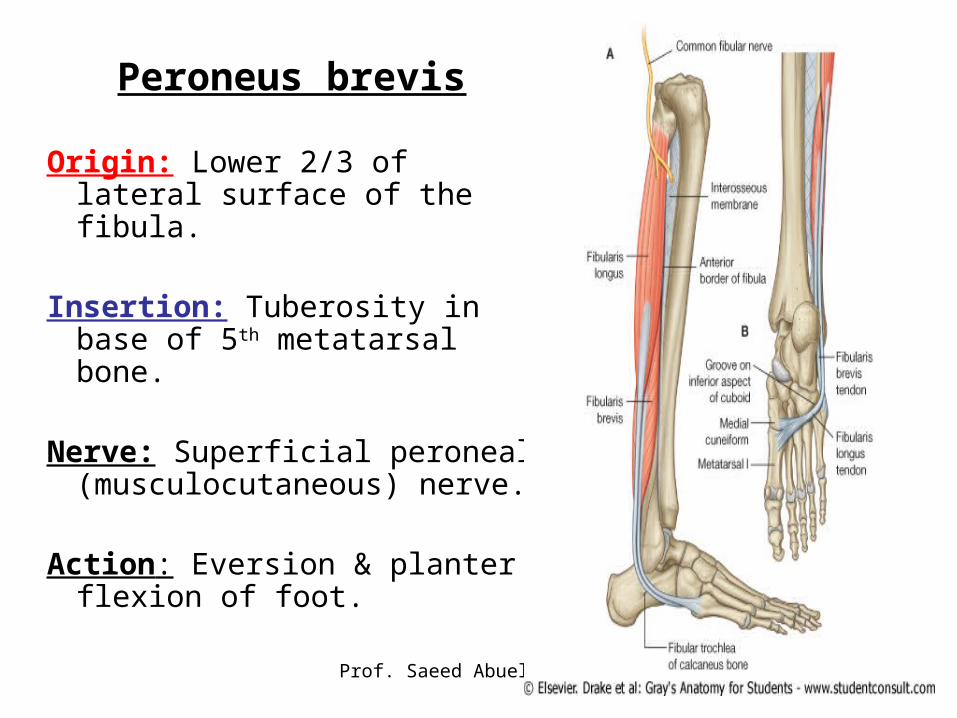
Peroneus brevis
Origin: Lower 2/3 of lateral surface of the fibula.
Insertion: Tuberosity in base of 5th metatarsal bone.
Nerve: Superficial peroneal (musculocutaneous) nerve.
Action: Eversion & planter flexion of foot.
Prof. Saeed Abuel Makarem 21
22Prof. Saeed Abuel Makarem
23Prof. Saeed Abuel Makarem
Superficial peroneal Nerve (Musculocutaneous)
• One of the two terminal branches of the common peroneal nerve.
• It arises at the lateral side of the neck of fibula.• In upper 1/3rd of the leg it descends within the
Peroneus Longus• In middle 1/3rd it runs between Peroneus Longus and
brevis.• In lower 1/3rd it pierces deep fascia and runs in the
superficial fascia crossing superficial to superior and inferior extensor retinaculae to the dorsum of the foot
24Prof. Saeed Abuel Makarem
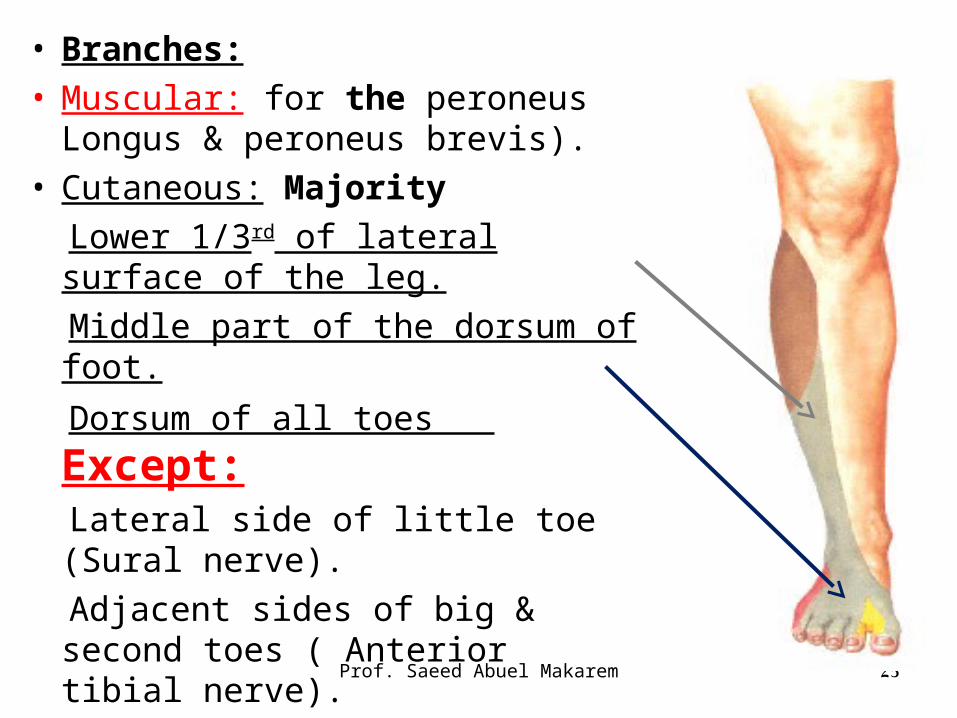
• Branches:• Muscular: for the peroneus Longus
& peroneus brevis).• Cutaneous: Majority
Lower 1/3rd of lateral surface of the leg.
Middle part of the dorsum of foot.
Dorsum of all toes Except: Lateral side of little toe (Sural
nerve).
Adjacent sides of big & second toes ( Anterior tibial nerve).
25Prof. Saeed Abuel Makarem
26
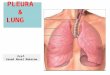
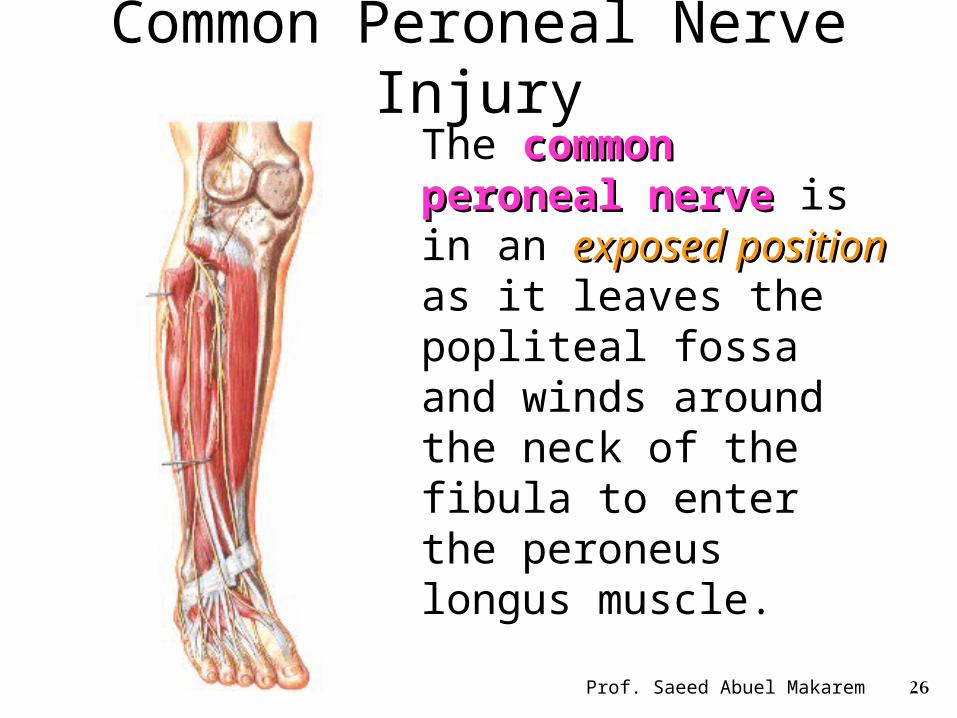
Common Peroneal Nerve Injury
The common peroneal common peroneal nervenerve is in an exposed exposed positionposition as it leaves the popliteal fossa and winds around the neck of the fibula to enter the peroneus longus muscle.
Prof. Saeed Abuel Makarem
27
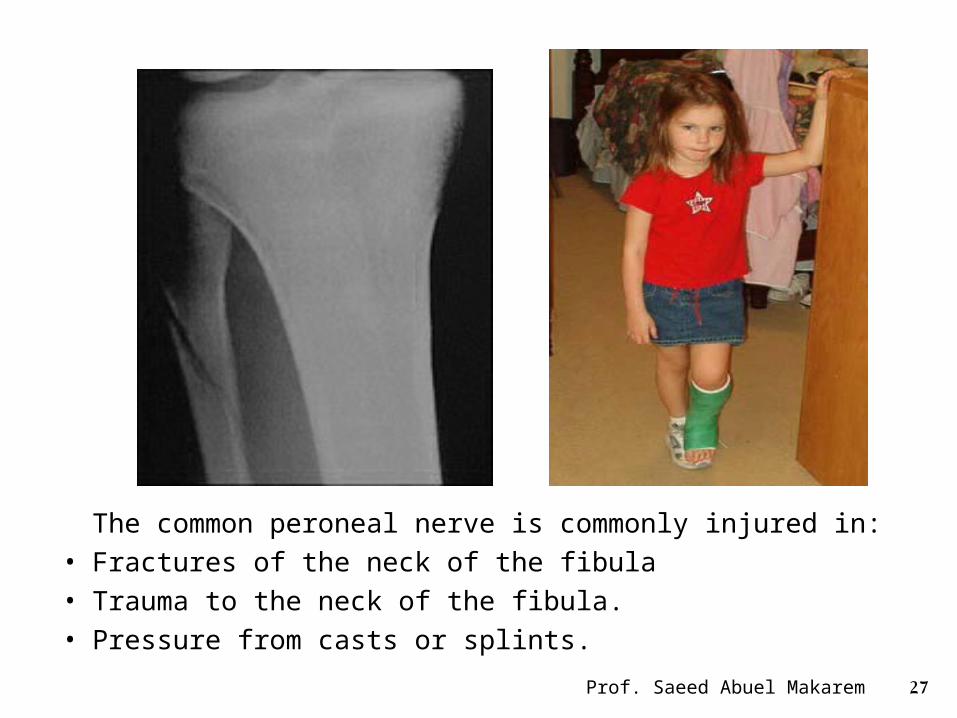
The common peroneal nerve is commonly injured in: • Fractures of the neck of the fibula• Trauma to the neck of the fibula.• Pressure from casts or splints.
Prof. Saeed Abuel Makarem

28
• The following clinical features are present in Common Peroneal Nerve Injury
Motor: Motor:
• The muscles of the anterior and The muscles of the anterior and lateral compartments of the leg are lateral compartments of the leg are paralyzed,paralyzed,
• As a result, the opposing muscles, the plantar flexors of the ankle joint and the invertors of the subtalar and transverse tarsal joints,
• cause the foot to be plantar flexed (foot drop) and inverted, an attitude
referred to as equinovarus.equinovarus.
Prof. Saeed Abuel Makarem
29
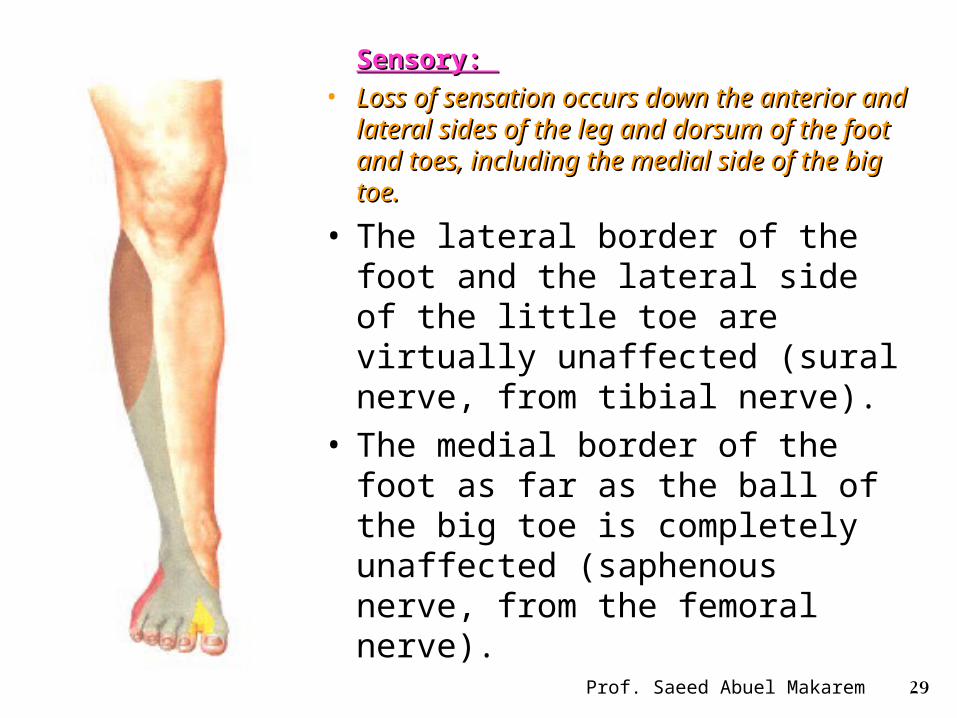
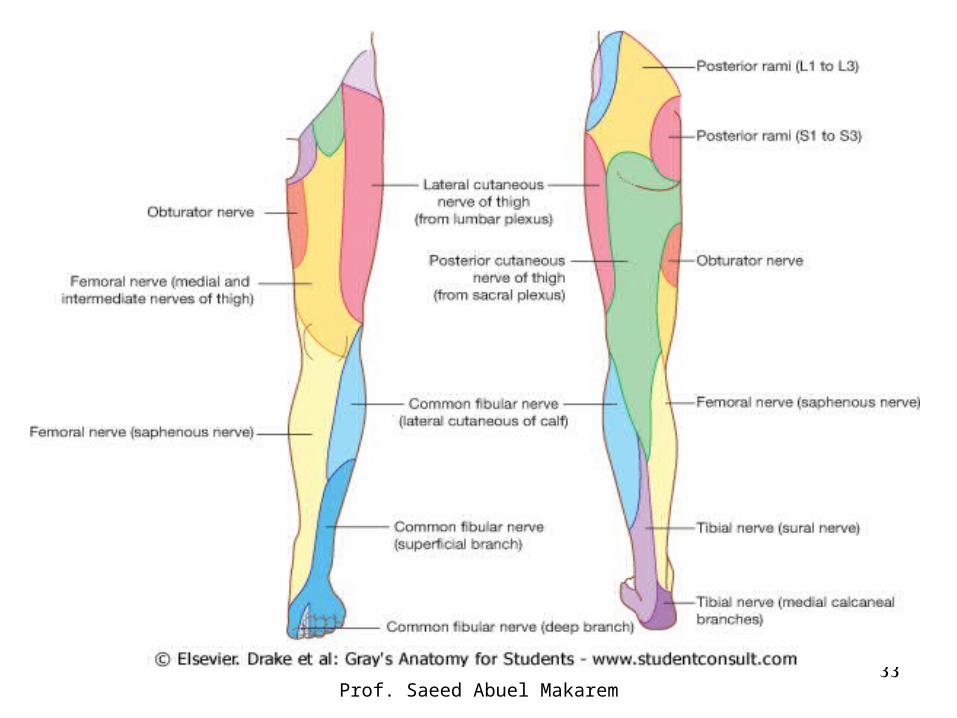
Sensory: Sensory:
• Loss of sensation occurs down the anterior Loss of sensation occurs down the anterior and lateral sides of the leg and dorsum of and lateral sides of the leg and dorsum of the foot and toes, including the medial side the foot and toes, including the medial side of the big toe. of the big toe.
• The lateral border of the foot and the lateral side of the little toe are virtually unaffected (sural nerve, from tibial nerve).
• The medial border of the foot as far as the ball of the big toe is completely unaffected (saphenous nerve, from the femoral nerve).
Prof. Saeed Abuel Makarem
30Prof. Saeed Abuel Makarem
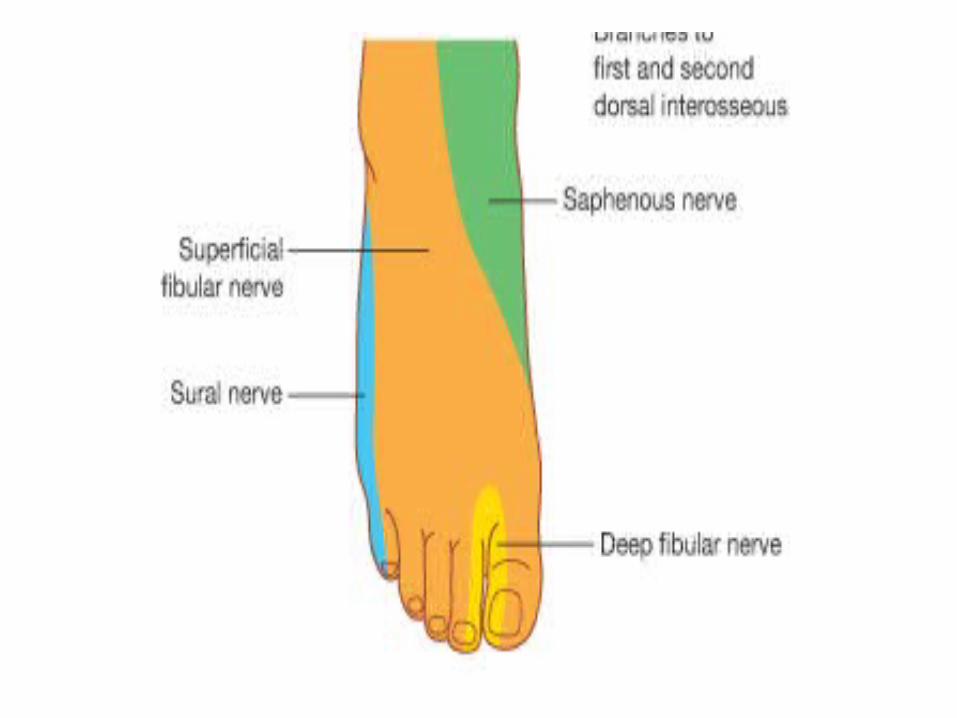
• Cutaneous nerve supply• I- On the dorsum of foot:• Medial part: Saphenous nerve.• Intermediate part: Superficial peroneal nerve.• Lateral part: Sural nerve.• II- On the dorsum of toes:• Sural nerve, lateral side of little toe.• Deep peroneal nerve, Adjacent sides of the big
and 2nd toes.• Superficial peroneal, to all remaining toes.
31
33Prof. Saeed Abuel Makarem
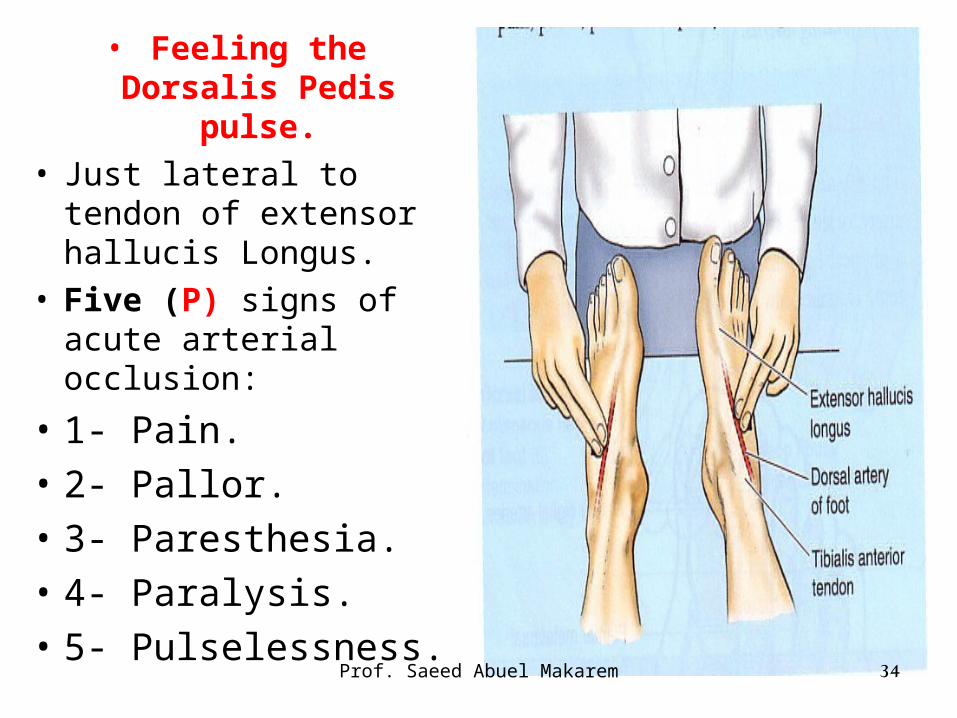
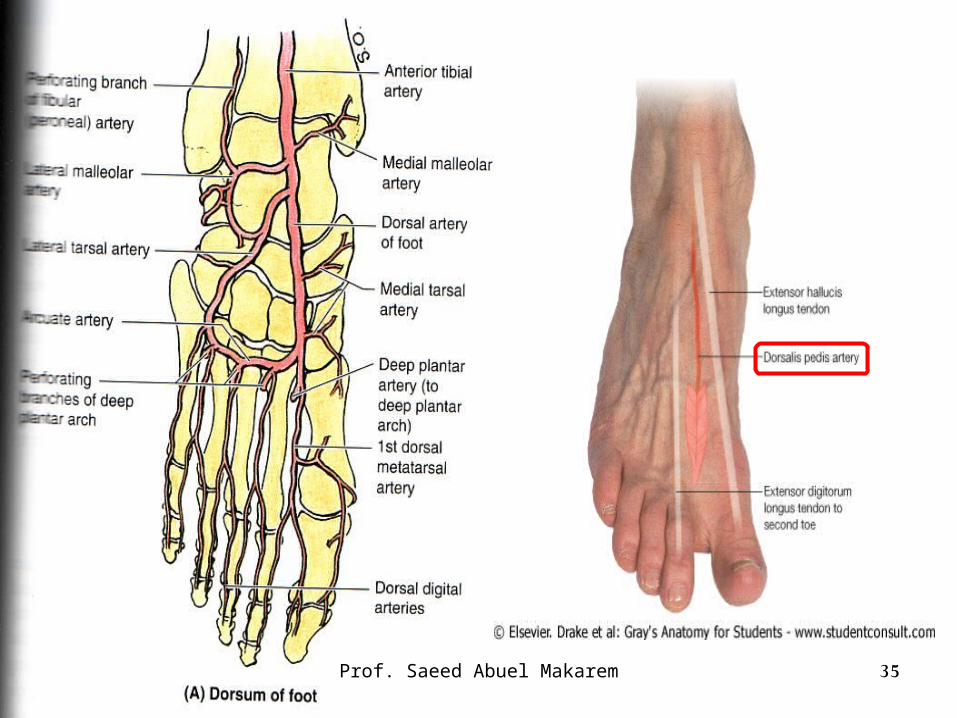
• Feeling the Dorsalis Pedis pulse.
• Just lateral to tendon of extensor hallucis Longus.
• Five (P) signs of acute arterial occlusion:
• 1- Pain.
• 2- Pallor.
• 3- Paresthesia.
• 4- Paralysis.
• 5- Pulselessness.34Prof. Saeed Abuel Makarem
35Prof. Saeed Abuel Makarem
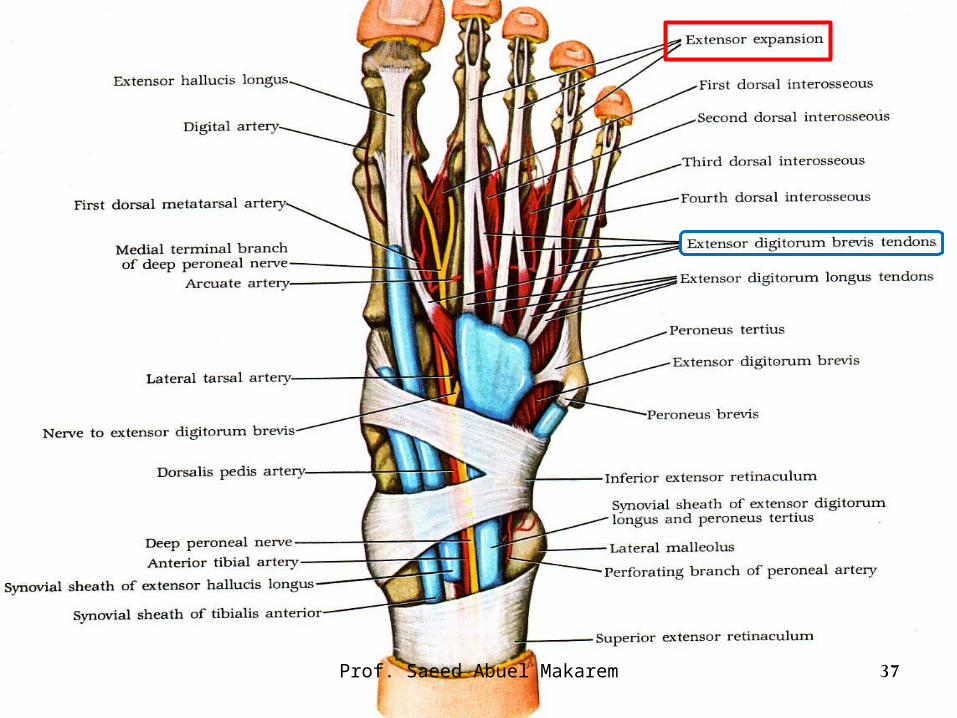
• Extensor Digitorum brevis:• The only muscle on the dorsum of the foot
Origin: anterior part of upper surface of calcaneus ???????
Insertion: Medial, medial, medial, 4 toes.
The medial slip is called extensor hallucis brevis.
It is inserted into proximal phalanx of big toe.
Each of the lateral 3 slips joins the extensor expansion of the 2nd,3rd & 4th toes.
Nerve supply: anterior tibial nerve.
NB. No tendon of Extensor Digitorum brevis reaches the little toe. 36
Prof. Saeed Abuel Makarem
37Prof. Saeed Abuel Makarem
38Prof. Saeed Abuel Makarem
Prof. Saeed Abuel Makarem 39
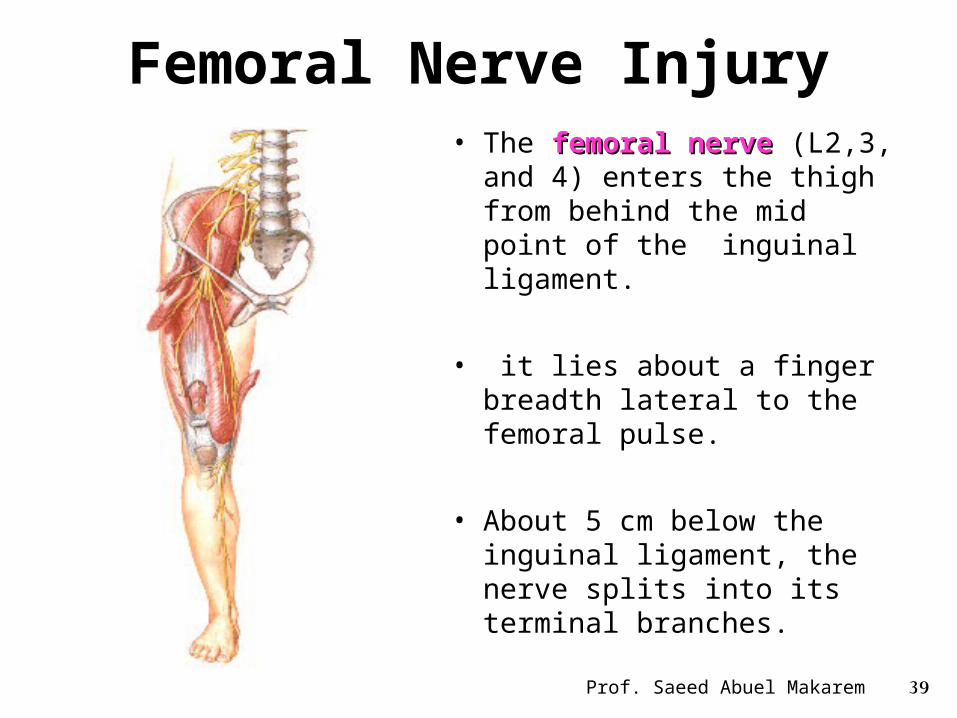
Femoral Nerve Injury• The femoral nervefemoral nerve (L2,3,
and 4) enters the thigh from behind the mid point of the inguinal ligament.
• it lies about a finger breadth lateral to the femoral pulse.
• About 5 cm below the inguinal ligament, the nerve splits into its terminal branches.
40
The following clinical features are present when the nerve is completely divided:
• Motor:Motor: The quadriceps femoris muscle is paralyzed,The quadriceps femoris muscle is paralyzed, and the knee cannot be extended.
• Is walking possible?Is walking possible?
- Yes. In walking, this is compensated for to some extent by use of the adductor muscles.
Prof. Saeed Abuel Makarem
Prof. Saeed Abuel Makarem 41
Femoral Nerve Injury
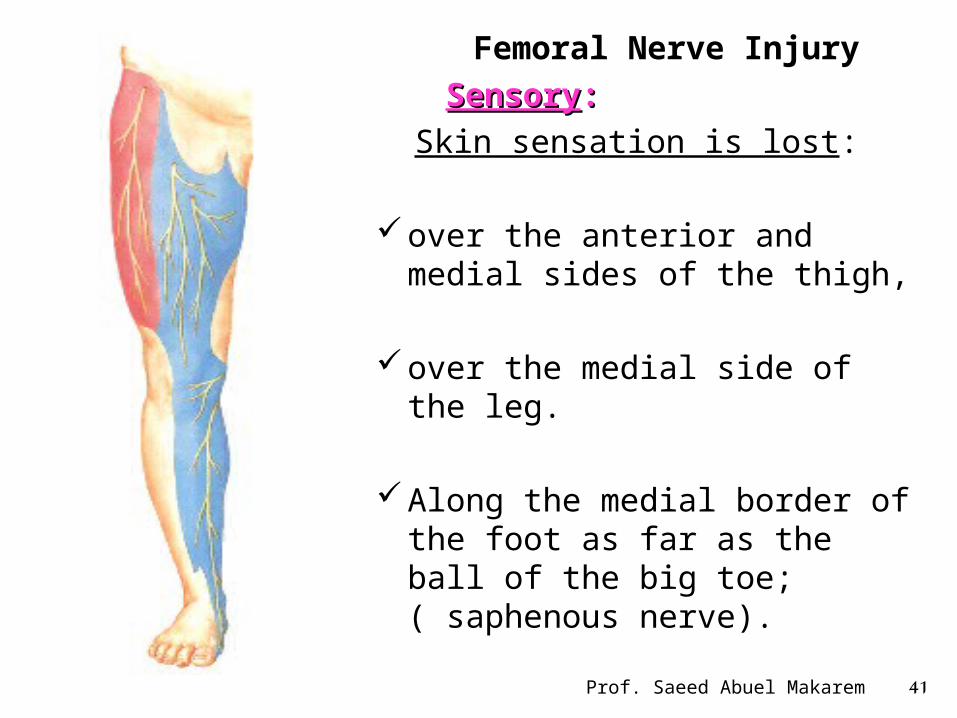
SensorySensory::
Skin sensation is lost:
over the anterior and medial sides of the thigh,
over the medial side of the leg.
Along the medial border of the
foot as far as the ball of the big toe; ( saphenous nerve).
Prof. Saeed Abuel Makarem 42
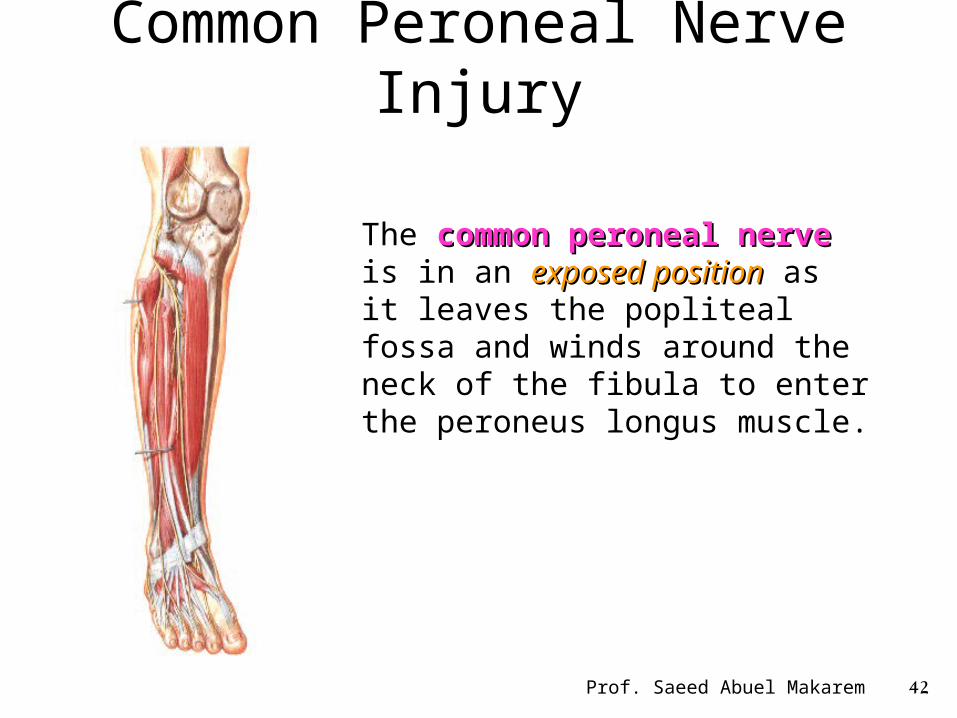
Common Peroneal Nerve Injury
The common peroneal nervecommon peroneal nerve is in an exposed positionexposed position as it leaves the popliteal fossa and winds around the neck of the fibula to enter the peroneus longus muscle.
Prof. Saeed Abuel Makarem 43
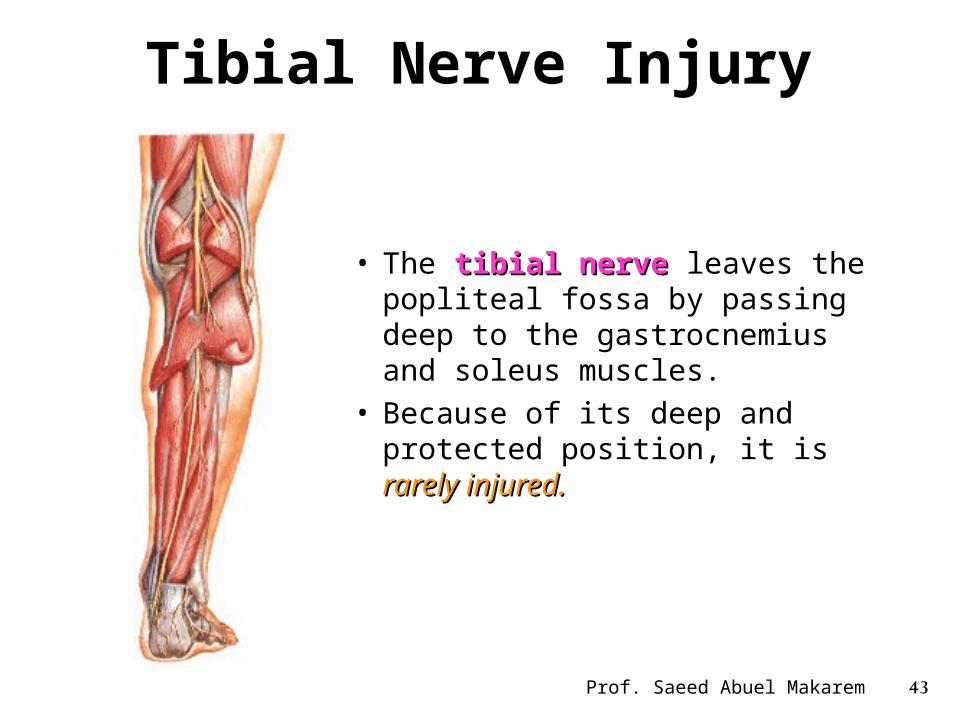
Tibial Nerve Injury
• The tibial nervetibial nerve leaves the popliteal fossa by passing deep to the gastrocnemius and soleus muscles.
• Because of its deep and protected position, it is rarely rarely injured. injured.
Prof. Saeed Abuel Makarem 44
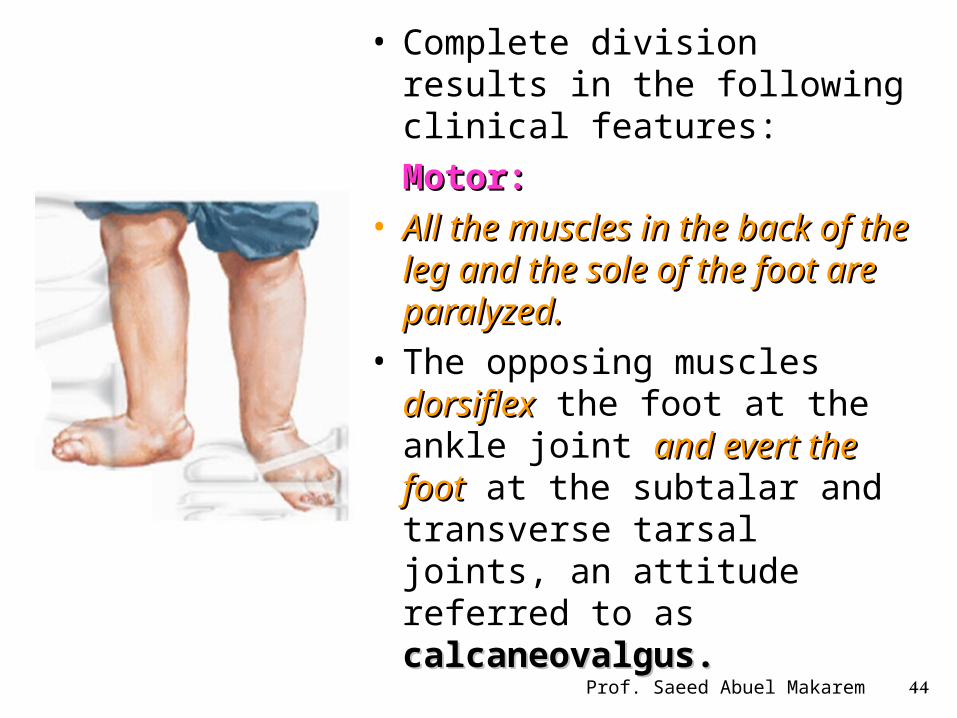
• Complete division results in the following clinical features:
Motor: Motor: • All the muscles in the back of All the muscles in the back of
the leg and the sole of the foot the leg and the sole of the foot are paralyzed. are paralyzed.
• The opposing muscles dorsiflexdorsiflex the foot at the ankle joint and evert the footand evert the foot at the subtalar and transverse tarsal joints, an attitude referred to as calcaneovalgus.calcaneovalgus.