Embed Size (px)
Citation preview
ORIGINAL PAPER
Prognostic factors, long-term survival, and outcome of cancerpatients receiving chemotherapy in the intensive care unit
Philipp Wohlfarth & Thomas Staudinger & Wolfgang R. Sperr & Andja Bojic & Oliver Robak &
Alexander Hermann & Klaus Laczika & Alexander Carlström & Katharina Riss &Werner Rabitsch & Marija Bojic & Paul Knoebl & Gottfried J. Locker & Maria Obiditsch &
Valentin Fuhrmann & Peter Schellongowski & Arbeitsgruppe für hämato-onkologischeIntensivmedizin der Österreichischen Gesellschaft für Internistische und AllgemeineIntensivmedizin und Notfallmedizin (ÖGIAIN)
Received: 10 March 2014 /Accepted: 11 June 2014 /Published online: 6 July 2014# Springer-Verlag Berlin Heidelberg 2014
Abstract Prognostic factors and outcomes of cancer patientswith acute organ failure receiving chemotherapy (CT) in theintensive care unit (ICU) are still incompletely described. Wetherefore retrospectively studied all patients who received CTin any ICU of our institution between October 2006 andNovember 2013. Fifty-six patients with hematologic (n=49;87.5 %) or solid (n=7; 12.5 %) malignancies, of which 20(36 %) were diagnosed in the ICU, were analyzed [m/f ratio,33:23; median age, 47 years (IQR 32 to 62); CharlsonComorbidity Index (CCI), 3 (2 to 5); Simplified AcutePhysiology Score II (SAPS II), 50 (39 to 61)]. The mainreasons for admission were acute respiratory failure, acutekidney failure, and septic shock. Mechanical ventilation andvasopressors were employed in 34 patients (61 %) respective-ly, hemofiltration in 22 (39 %), and extracorporeal life supportin 7 (13 %). Twenty-seven patients (48 %) received their firstCT in the ICU. Intention of therapy was cure in 46 patients
(82 %). Tumor lysis syndrome (TLS) developed in 20 patients(36 %). ICU and hospital survival was 75 and 59 %. Hospitalsurvivors were significantly younger; had lower CCI, SAPSII, and TLS risk scores; presented less often with septic shock;were less likely to develop TLS; and received vasopressors,hemofiltration, and thrombocyte transfusions in lower propor-tions. After discharge, 88 % continued CT and 69 % of 1-yearsurvivors were in complete remission. Probability of 1- and 2-year survival was 41 and 38 %, respectively. Conclusively,administration of CT in selected ICU cancer patients wasfeasible and associated with considerable long-term survivalas well as long-term disease-free survival.
Keywords Chemotherapy . Acute leukemia .
Lymphoma . Cancer . Intensive care unit . Tumor lysissyndrome
Introduction
Short- and long-term survival of critically ill cancer patientshas improved markedly over the last decades [1–4]. Forpatients with both, hematological or solid malignancies,achievements have been reported in the therapy of acuterespiratory failure [5–7], acute kidney failure [8, 9], and sepsis[10–12]. Moreover, quality of life after intensive care may notsignificantly differ in patients with hematologic malignancieswhen compared to the general ICU population [13].Numerous well-established prognostic factors allowed forproposing a framework of evidence-based admission criteria[14]. Accordingly, unlimited intensive care seems to be ben-eficial in a significant proportion of selected patients withmalignant diseases.
P. Wohlfarth : T. Staudinger :W. R. Sperr :A. Bojic :O. Robak :A. Hermann :K. Laczika :A. Carlström :K. Riss :W. Rabitsch :M. Bojic : P. Knoebl :G. J. Locker : P. Schellongowski (*)Department of Medicine I, Intensive Care Unit 13i2, ComprehensiveCancer Center, Medical University of Vienna, Waehringer Guertel18-20, 1090 Vienna, Austriae-mail: [email protected]
M. ObiditschPharmacy Department, Vienna General Hospital,Waehringer Guertel18-20, 1090 Vienna, Austria
V. FuhrmannDepartment of Medicine III, Intensive Care Unit 13h1, MedicalUniversity of Vienna, Waehringer Guertel 18-20, 1090 Vienna,Austria
Ann Hematol (2014) 93:1629–1636DOI 10.1007/s00277-014-2141-x

Organ dysfunctions in cancer patients may arise from com-plications of the malignant disease itself as well as from toxictherapy-related effects or ensuing infections [14]. Thus, inten-sive care management of these patients requires specificknowledge and close cooperation between intensivists, hema-tologists, and oncologists [15]. Particular considerations arisewhen clinicians have to evaluate whether indicated chemo-therapy (CT) should be administered to patients with acuteorgan dysfunctions. In fact, such decisions have to be takenregularly and may, in specialized centers, arise during treat-ment of every fourth hematologic intensive care unit (ICU)patient [1]. However, as of today, surprisingly, only threereports on moderately sized cohorts have been dedicated tothe detailed description of such patients [16–18].
We report a single-center experience with critically ill ICUcancer patients and urgent indication of chemotherapy.
Materials and methods
We retrospectively studied the clinical courses of all adult ICUpatients (≥18 years of age) who received anti-cancer therapy atthe Medical University of Vienna, General Hospital betweenOctober 2006 and November 2013. This study was conductedin accordance with Good Clinical Practice guidelines and theamended Declaration of Helsinki. The Institutional EthicalReview Board of the Medical University of Vienna approvedthe protocol and waved the need for informed consent due tothe non-interventional retrospective design of theinvestigation.
In our center, medical admissions to the ICU are granted toall cancer patients with one or more organ dysfunctions andlife-extending therapeutic options on the discretion of thetreating hemato-oncologist and the intensivist in charge.Decisions to admit a patient to the ICU are based onevidence-derived recommendations [14, 19]. Decisions onthe administration of CT are made by the treating hemato-oncologis t in coopera t ion wi th the in tens ivis t .Interdisciplinary rounds are granted at least once a day.
By analyzing the charts of the patients, we recorded theage, gender, characteristics of the underlying malignancy—including type and stage of the respective malignancy—timeof diagnosis, type and timing of previous cancer specifictreatments, and performance status (PS) 1 week prior to theactual hospitalization as described by the Eastern CooperativeOncology Group scale [20], Charlson Comorbidity Index(CCI) [21], and Simplified Acute Physiology Score II(SAPS II) [22, 23] to quantify the severity of illness at ICUadmission, the primary reason for ICU admission, presenceand source of any documented infection, type of CT adminis-tered during the ICU stay, and intention of CT (curative vs.palliative) together with laboratory parameters (blood cellcount, serum chemistry, and coagulation). Furthermore, the
need for invasive mechanical ventilation, vasopressors, renalreplacement therapy (RRT), and extracorporeal life support(ECLS) were recorded as well as the occurrence of dissemi-nated intravascular coagulation (DIC) by the definition of theInternational Society of Thrombosis and Hemostasis (ISTH)DIC score [24], risk for [25, 26] tumor lysis syndrome (TLS)as assessed by the stratification of Cairo et al. [26] and the TLSrisk score of Darmon et al. [25], and the development oflaboratory or clinically manifested TLS [26], use of bloodproducts and coagulation factors, and medication for hyper-uricemia (i.e., allopurinol and rasburicase). As follow-up, ICUand hospital survival, course of the malignancy (remissionstatus), death date (if applicable), and date of the last visitwere assessed.
Continuous data are presented as median and inter-quartile ranges (25–75 %) unless otherwise indicated.Dichotomous data are presented as number and percent-age. Data were compared between survivors and non-survivors by Fisher’s exact test for dichotomous vari-ables and the Mann–Whitney U test for continuousvariables, respectively. Differences were considered tobe statistically significant when p was <0.05. The prod-uct limit method of Kaplan and Meier was used toanalyze the probability of overall survival. Sensitivityand specificity to predict TLS during the ICU stay werecalculated using each individual’s TLS risk score [25]as a cutoff value. Sensitivity in this setting is thelikelihood that the TLS risk score of a patient notdeveloping TLS exceeds a particular cutoff (=“positivetest”). Specificity is the likelihood that the TLS score ofa patient developing TLS is below this particular cutoff(=“negative test”). A receiver-operating characteristic(ROC) curve for the prediction of TLS by means ofthe TLS risk score was constructed [27].
Results
Fifty-six consecutive patients with a male/female ratio of33:23, age 47 (32 to 62)years, CCI 3 (2 to 5), and SAPS II50 (39 to 61) were identified. During the observational period,437 patients with malignancies were admitted to our ICU.Thus, the proportion of cancer patients receiving CT therapywas 12.8 %. The performance status was 0–1 in 41 patients(73 %), 2–3 in 9 patients (16 %), 4 in one patient (2 %), andunknown in 5 patients (9 %). Patients were mainly admitteddue to acute respiratory failure (n=25), acute kidney failure(n=9), and septic shock (n=7). Invasive mechanical ventila-tion and vasopressor therapy were applied in 34 patients(61 %) each, hemofiltration in 22 (39 %), and extracorporeallife support in 7 patients (13 %), consisting of interventionallung assist (n=1), veno-venous extracorporeal membraneoxygenation (ECMO; n=3), and veno-arterial ECMO (n=3)
1630 Ann Hematol (2014) 93:1629–1636
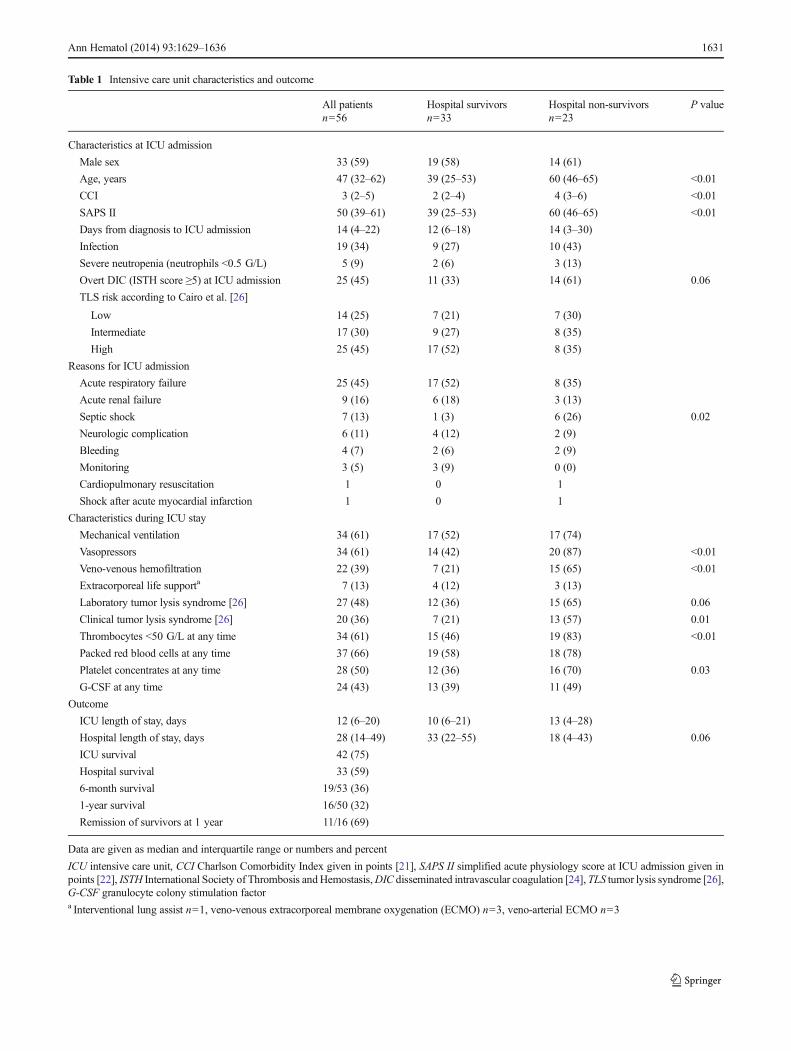
Table 1 Intensive care unit characteristics and outcome
All patientsn=56
Hospital survivorsn=33
Hospital non-survivorsn=23
P value
Characteristics at ICU admission
Male sex 33 (59) 19 (58) 14 (61)
Age, years 47 (32–62) 39 (25–53) 60 (46–65) <0.01
CCI 3 (2–5) 2 (2–4) 4 (3–6) <0.01
SAPS II 50 (39–61) 39 (25–53) 60 (46–65) <0.01
Days from diagnosis to ICU admission 14 (4–22) 12 (6–18) 14 (3–30)
Infection 19 (34) 9 (27) 10 (43)
Severe neutropenia (neutrophils <0.5 G/L) 5 (9) 2 (6) 3 (13)
Overt DIC (ISTH score ≥5) at ICU admission 25 (45) 11 (33) 14 (61) 0.06
TLS risk according to Cairo et al. [26]
Low 14 (25) 7 (21) 7 (30)
Intermediate 17 (30) 9 (27) 8 (35)
High 25 (45) 17 (52) 8 (35)
Reasons for ICU admission
Acute respiratory failure 25 (45) 17 (52) 8 (35)
Acute renal failure 9 (16) 6 (18) 3 (13)
Septic shock 7 (13) 1 (3) 6 (26) 0.02
Neurologic complication 6 (11) 4 (12) 2 (9)
Bleeding 4 (7) 2 (6) 2 (9)
Monitoring 3 (5) 3 (9) 0 (0)
Cardiopulmonary resuscitation 1 0 1
Shock after acute myocardial infarction 1 0 1
Characteristics during ICU stay
Mechanical ventilation 34 (61) 17 (52) 17 (74)
Vasopressors 34 (61) 14 (42) 20 (87) <0.01
Veno-venous hemofiltration 22 (39) 7 (21) 15 (65) <0.01
Extracorporeal life supporta 7 (13) 4 (12) 3 (13)
Laboratory tumor lysis syndrome [26] 27 (48) 12 (36) 15 (65) 0.06
Clinical tumor lysis syndrome [26] 20 (36) 7 (21) 13 (57) 0.01
Thrombocytes <50 G/L at any time 34 (61) 15 (46) 19 (83) <0.01
Packed red blood cells at any time 37 (66) 19 (58) 18 (78)
Platelet concentrates at any time 28 (50) 12 (36) 16 (70) 0.03
G-CSF at any time 24 (43) 13 (39) 11 (49)
Outcome
ICU length of stay, days 12 (6–20) 10 (6–21) 13 (4–28)
Hospital length of stay, days 28 (14–49) 33 (22–55) 18 (4–43) 0.06
ICU survival 42 (75)
Hospital survival 33 (59)
6-month survival 19/53 (36)
1-year survival 16/50 (32)
Remission of survivors at 1 year 11/16 (69)
Data are given as median and interquartile range or numbers and percent
ICU intensive care unit, CCI Charlson Comorbidity Index given in points [21], SAPS II simplified acute physiology score at ICU admission given inpoints [22], ISTH International Society of Thrombosis andHemostasis,DIC disseminated intravascular coagulation [24], TLS tumor lysis syndrome [26],G-CSF granulocyte colony stimulation factora Interventional lung assist n=1, veno-venous extracorporeal membrane oxygenation (ECMO) n=3, veno-arterial ECMO n=3
Ann Hematol (2014) 93:1629–1636 1631
respectively [28]. Table 1 summarizes patients’ characteristicsand clinical data.
Cancer characteristics and therapies
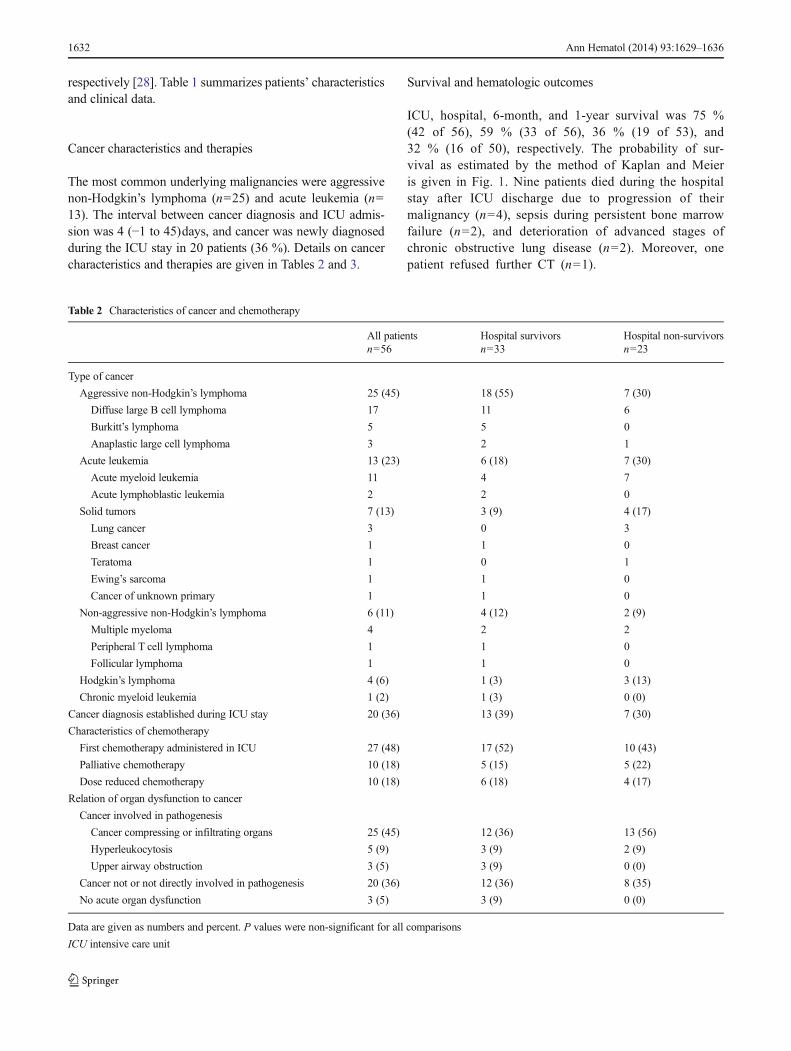
The most common underlying malignancies were aggressivenon-Hodgkin’s lymphoma (n=25) and acute leukemia (n=13). The interval between cancer diagnosis and ICU admis-sion was 4 (−1 to 45)days, and cancer was newly diagnosedduring the ICU stay in 20 patients (36 %). Details on cancercharacteristics and therapies are given in Tables 2 and 3.
Survival and hematologic outcomes
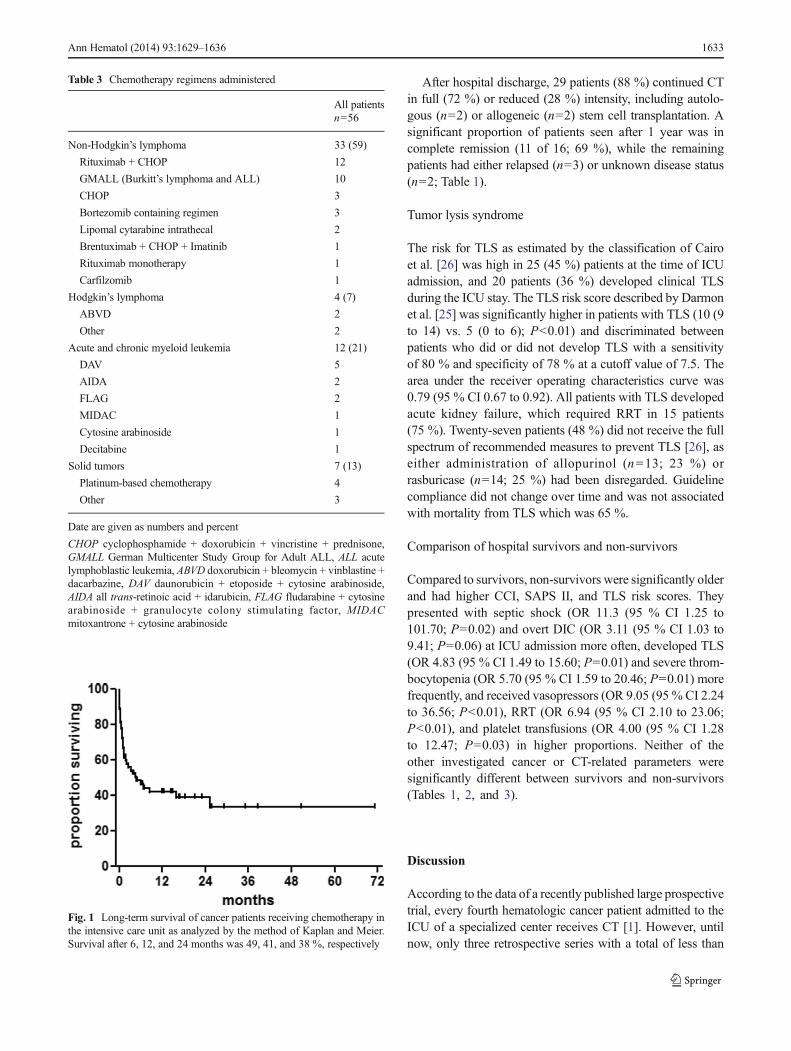
ICU, hospital, 6-month, and 1-year survival was 75 %(42 of 56), 59 % (33 of 56), 36 % (19 of 53), and32 % (16 of 50), respectively. The probability of sur-vival as estimated by the method of Kaplan and Meieris given in Fig. 1. Nine patients died during the hospitalstay after ICU discharge due to progression of theirmalignancy (n=4), sepsis during persistent bone marrowfailure (n=2), and deterioration of advanced stages ofchronic obstructive lung disease (n=2). Moreover, onepatient refused further CT (n=1).
Table 2 Characteristics of cancer and chemotherapy
All patientsn=56
Hospital survivorsn=33
Hospital non-survivorsn=23
Type of cancer
Aggressive non-Hodgkin’s lymphoma 25 (45) 18 (55) 7 (30)
Diffuse large B cell lymphoma 17 11 6
Burkitt’s lymphoma 5 5 0
Anaplastic large cell lymphoma 3 2 1
Acute leukemia 13 (23) 6 (18) 7 (30)
Acute myeloid leukemia 11 4 7
Acute lymphoblastic leukemia 2 2 0
Solid tumors 7 (13) 3 (9) 4 (17)
Lung cancer 3 0 3
Breast cancer 1 1 0
Teratoma 1 0 1
Ewing’s sarcoma 1 1 0
Cancer of unknown primary 1 1 0
Non-aggressive non-Hodgkin’s lymphoma 6 (11) 4 (12) 2 (9)
Multiple myeloma 4 2 2
Peripheral T cell lymphoma 1 1 0
Follicular lymphoma 1 1 0
Hodgkin’s lymphoma 4 (6) 1 (3) 3 (13)
Chronic myeloid leukemia 1 (2) 1 (3) 0 (0)
Cancer diagnosis established during ICU stay 20 (36) 13 (39) 7 (30)
Characteristics of chemotherapy
First chemotherapy administered in ICU 27 (48) 17 (52) 10 (43)
Palliative chemotherapy 10 (18) 5 (15) 5 (22)
Dose reduced chemotherapy 10 (18) 6 (18) 4 (17)
Relation of organ dysfunction to cancer
Cancer involved in pathogenesis
Cancer compressing or infiltrating organs 25 (45) 12 (36) 13 (56)
Hyperleukocytosis 5 (9) 3 (9) 2 (9)
Upper airway obstruction 3 (5) 3 (9) 0 (0)
Cancer not or not directly involved in pathogenesis 20 (36) 12 (36) 8 (35)
No acute organ dysfunction 3 (5) 3 (9) 0 (0)
Data are given as numbers and percent. P values were non-significant for all comparisons
ICU intensive care unit
1632 Ann Hematol (2014) 93:1629–1636
After hospital discharge, 29 patients (88 %) continued CTin full (72 %) or reduced (28 %) intensity, including autolo-gous (n=2) or allogeneic (n=2) stem cell transplantation. Asignificant proportion of patients seen after 1 year was incomplete remission (11 of 16; 69 %), while the remainingpatients had either relapsed (n=3) or unknown disease status(n=2; Table 1).
Tumor lysis syndrome
The risk for TLS as estimated by the classification of Cairoet al. [26] was high in 25 (45 %) patients at the time of ICUadmission, and 20 patients (36 %) developed clinical TLSduring the ICU stay. The TLS risk score described by Darmonet al. [25] was significantly higher in patients with TLS (10 (9to 14) vs. 5 (0 to 6); P<0.01) and discriminated betweenpatients who did or did not develop TLS with a sensitivityof 80 % and specificity of 78 % at a cutoff value of 7.5. Thearea under the receiver operating characteristics curve was0.79 (95 % CI 0.67 to 0.92). All patients with TLS developedacute kidney failure, which required RRT in 15 patients(75 %). Twenty-seven patients (48 %) did not receive the fullspectrum of recommended measures to prevent TLS [26], aseither administration of allopurinol (n=13; 23 %) orrasburicase (n=14; 25 %) had been disregarded. Guidelinecompliance did not change over time and was not associatedwith mortality from TLS which was 65 %.
Comparison of hospital survivors and non-survivors
Compared to survivors, non-survivors were significantly olderand had higher CCI, SAPS II, and TLS risk scores. Theypresented with septic shock (OR 11.3 (95 % CI 1.25 to101.70; P=0.02) and overt DIC (OR 3.11 (95 % CI 1.03 to9.41; P=0.06) at ICU admission more often, developed TLS(OR 4.83 (95 % CI 1.49 to 15.60; P=0.01) and severe throm-bocytopenia (OR 5.70 (95 % CI 1.59 to 20.46; P=0.01) morefrequently, and received vasopressors (OR 9.05 (95 % CI 2.24to 36.56; P<0.01), RRT (OR 6.94 (95 % CI 2.10 to 23.06;P<0.01), and platelet transfusions (OR 4.00 (95 % CI 1.28to 12.47; P=0.03) in higher proportions. Neither of theother investigated cancer or CT-related parameters weresignificantly different between survivors and non-survivors(Tables 1, 2, and 3).
Discussion
According to the data of a recently published large prospectivetrial, every fourth hematologic cancer patient admitted to theICU of a specialized center receives CT [1]. However, untilnow, only three retrospective series with a total of less than
Table 3 Chemotherapy regimens administered
All patientsn=56
Non-Hodgkin’s lymphoma 33 (59)
Rituximab + CHOP 12
GMALL (Burkitt’s lymphoma and ALL) 10
CHOP 3
Bortezomib containing regimen 3
Lipomal cytarabine intrathecal 2
Brentuximab + CHOP + Imatinib 1
Rituximab monotherapy 1
Carfilzomib 1
Hodgkin’s lymphoma 4 (7)
ABVD 2
Other 2
Acute and chronic myeloid leukemia 12 (21)
DAV 5
AIDA 2
FLAG 2
MIDAC 1
Cytosine arabinoside 1
Decitabine 1
Solid tumors 7 (13)
Platinum-based chemotherapy 4
Other 3
Date are given as numbers and percent
CHOP cyclophosphamide + doxorubicin + vincristine + prednisone,GMALL German Multicenter Study Group for Adult ALL, ALL acutelymphoblastic leukemia, ABVD doxorubicin + bleomycin + vinblastine +dacarbazine, DAV daunorubicin + etoposide + cytosine arabinoside,AIDA all trans-retinoic acid + idarubicin, FLAG fludarabine + cytosinearabinoside + granulocyte colony stimulating factor, MIDACmitoxantrone + cytosine arabinoside
Fig. 1 Long-term survival of cancer patients receiving chemotherapy inthe intensive care unit as analyzed by the method of Kaplan and Meier.Survival after 6, 12, and 24 months was 49, 41, and 38 %, respectively
Ann Hematol (2014) 93:1629–1636 1633

200 patients have been dedicated to the detailed analysis ofsuch cases [16–18]. Our descriptive analysis of 56 cancerpatients is confirmative of earlier findings concerning thegeneral feasibility of CTadministration to selected ICU cancerpatients. Moreover, it adds significant information to the liter-ature by firstly reporting on long-term data regarding survivaland remission status. Furthermore, we found so far unreportedhigh rates of the TLS, which allowed for assessing the perfor-mance of a new clinical prediction risk instrument.
Patients in our cohort presented with predominantly hema-tologic malignancies, were admitted mostly due to acute re-spiratory failure, had infections, were ventilated to a consid-erably large proportion, and suffered from severe acute illness.These findings are in line with the previously published data[16–18]. However, use of vasopressors and RRTwas higher inour cohort, and the use of ECLS in this particular setting hasnot been reported so far by other centers. Despite the presenceof severe organ failure in a high proportion of our patients,ICU and hospital survival was remarkably high. In line withprevious findings [1–4, 10, 12, 14, 19, 29], cancer- andchemotherapy-associated characteristics including the inten-tion of chemotherapy (i.e., palliative vs. curative) were notassociated with hospital survival. Survival was mainly corre-lated with age, comorbidity, severity of acute illness as indi-cated by SAPS II scores, septic shock, vasopressor use, andRRT respectively. Interestingly, the need for mechanical ven-tilation was not associated with survival. As this finding is incontrast to data on large cohorts of critically ill cancer patients[1–4, 10, 12, 14, 19, 29, 30], it may be misleading due to therelatively small number of patients analyzed. However, re-garding the notably high survival rates of 50 % in mechani-cally ventilated cancer patients who additionally receivedvasopressors, RRT, and ECLS in 88, 53, and 21 %, respec-tively, it might also reflect a gradually improving care ofseverely ill cancer patients.
The estimated 1- and 2-year survival rates were 41 and38 %, meaning that approximately two out of three hospitalsurvivors can expect long-term survival. Similar to the find-ings of Azoulay et al. [1], critical illness and ICU admissiondid not alter treatment plans in general, as most of the patients(88 %) continued with CT. Although treatment intensity wasreduced in one out of three patients (28 %), two thirds ofpatients (69%) seen after 1 year were in complete remission oftheir malignancy.
Every third patient of our cohort developed clinically man-ifested TLS, which required RRT in most cases and wasassociated with higher hospital mortality. Since administrationof rasburicase is widely recommended in patients with highrisk for TLS [31, 32, 26], adequate risk stratification is imper-ative. Applying the established TLS risk stratification pro-posed by Cairo et al. [26], 45 % of our patients fulfilled thehigh-risk criteria. In contrast, Darmon et al. recently analyzeda group of patients who all fulfilled high-risk criteria and
found a TLS rate of only 20 %, which was much lower thanthe rate in our study (36 %) [25]. As their cohort consisted ofprimarily non-ICU patients, these findings could imply thatthe risk stratification proposed by Cairo et al. [26] isunderestimating TLS risk in patients with acute(multi-)organ dysfunction. In fact, sicker patients had higherTLS rates in our cohort, as SAPS II scores were significantlyhigher in TLS patients when compared to non-TLS patients(data not shown). In the abovementioned study of Darmonet al., the authors developed a TLS risk score, which includeslactate dehydrogenase, serum phosphate levels, and DIC [25].Employing this particular score in our patients, we were ableto predict TLS with a sufficiently high sensitivity and speci-ficity. Thus, incorporating the new Darmon score into TLSrisk assessment in critically ill patients undergoing CT seemsadvisable. As guideline compliance concerning the adminis-tration of allopurinol and rasburicase was found to be as lowas 50 %, adoption of institutional standard operating proce-dures in the context of TLS management is recommended.
Administering CT to ICU patients calls for appropriatestaff expertise and organizational requirements [15], consid-ering that every third cancer diagnosis in our cohort wasestablished in the ICU, half of patients received CT for thefirst time, and aggressive CTs with curative intention wereavailable for the majority of patients. These findings furtherunderline the need for close collaboration betweenintensivists, hematologists, and oncologists which will mostlikely be at the best achieved in specialized cancer centers.Our data confirm the general feasibility of CT administrationto critically ill ICU cancer patients. However, a series ofimportant questions are still to be answered: What is theoptimal timing of CTadministration concerning present organdysfunctions and/or infectious complications? How can wesafely establish the optimal CT dose in patients with organdysfunctions, which allows for minimal toxicity and maximalanti-cancer effect? What is the prognostic relevance of pre-emptive ICU admissions for “safer CT administration” inpatients at high risk for complications and what would bethe criteria to admit such patients [1]? To what extent shouldwe decrease peripheral tumor load, e.g., by means ofleukapheresis or hydroxyurea before initiating full CT inhighly aggressive and/or leukemic malignancies? Close sci-entific cooperation of dedicated cancer centers will be neededto generate answers to these questions.
Our report has several limitations. First of all, our findingsmay not be generalized since they reflect the experience of asingle cancer referral center. We present a cohort of highlyselected patients, as we follow the recommended ICU admis-sion criteria for critically ill cancer patients, which excludepatients with low performance status, e.g., bedridden patients,patients with prohibitive limitations, and those without thera-peutic options [14, 19]. On the contrary, all patients in remis-sion of their malignant disease, those with newly diagnosed
1634 Ann Hematol (2014) 93:1629–1636

cancer, patients with TLS, and patients with good life expec-tancy receive a full code ICU management without limita-tions. Second, the number of patients is limited and did notmake the utilization of advanced statistical methods advisable.Nevertheless, since the total published number of patientsreceiving CT in the ICU is still small, we believe that ourreport can add relevant information to the body of literature.Finally, we cannot report on quality of life, which is anincreasingly studied outcome variable of chief importance incritically ill cancer patients [1, 2, 13].
Conclusions
In conclusion, the administration of urgently indicated CT inselected ICU cancer patients with acute organ failure is feasi-ble and can be associated with considerable long-term surviv-al, as well as long-term disease-free survival. Short-term sur-vival mainly depends on the acute severity of illness, whileseveral cancer characteristics including palliative status maynot have an impact. We found high rates of TLS, which was ofprognostic relevance and warrants for optimal management aswell as further investigations.
Conflict of interest The authors declare that they have no conflict ofinterest.
References
1. Azoulay E, Mokart D, Pene F, Lambert J, Kouatchet A, Mayaux J,Vincent F, Nyunga M, Bruneel F, Laisne LM, Rabbat A, Lebert C,Perez P, Chaize M, Renault A, Meert AP, Benoit D, Hamidfar R,Jourdain M, DarmonM, Schlemmer B, Chevret S, Lemiale V (2013)Outcomes of critically ill patients with hematologic malignancies:prospective multicenter data from France and Belgium—a groupe derecherche respiratoire en reanimation onco-hematologique study. JClin Oncol 31(22):2810–2818. doi:10.1200/JCO.2012.47.2365
2. Oeyen SG, Benoit DD, Annemans L, Depuydt PO, Van Belle SJ,Troisi RI, Noens LA, Pattyn P, Decruyenaere JM (2013) Long-termoutcomes and quality of life in critically ill patients with hematolog-ical or solid malignancies: a single center study. Intensive Care Med39(5):889–898. doi:10.1007/s00134-012-2791-x
3. Soares M, Caruso P, Silva E, Teles JM, Lobo SM, Friedman G, DalPizzol F, Mello PV, Bozza FA, Silva UV, Torelly AP, Knibel MF,Rezende E, Netto JJ, Piras C, Castro A, Ferreira BS, Rea-Neto A,Olmedo PB, Salluh JI (2010) Characteristics and outcomes of pa-tients with cancer requiring admission to intensive care units: aprospective multicenter study. Crit Care Med 38(1):9–15. doi:10.1097/CCM.0b013e3181c0349e
4. Staudinger T, Stoiser B,Mullner M, Locker GJ, Laczika K, Knapp S,Burgmann H, Wilfing A, Kofler J, Thalhammer F, Frass M (2000)Outcome and prognostic factors in critically ill cancer patients ad-mitted to the intensive care unit. Crit Care Med 28(5):1322–1328
5. Gristina GR, Antonelli M, Conti G, Ciarlone A, Rogante S, Rossi C,Bertolini G (2011) Noninvasive versus invasive ventilation for acuterespiratory failure in patients with hematologic malignancies: a 5-
year multicenter observational survey. Crit Care Med 39(10):2232–2239. doi:10.1097/CCM.0b013e3182227a27
6. Azoulay E,Mokart D, Lambert J, Lemiale V, Rabbat A, Kouatchet A,Vincent F, Gruson D, Bruneel F, Epinette-Branche G, Lafabrie A,Hamidfar-Roy R, Cracco C, Renard B, Tonnelier JM, Blot F, ChevretS, Schlemmer B (2010) Diagnostic strategy for hematology andoncology patients with acute respiratory failure: randomized con-trolled trial. Am J Respir Crit Care Med 182(8):1038–1046. doi:10.1164/rccm.201001-0018OC
7. Schnell D, Mayaux J, Lambert J, Roux A, Moreau AS, Zafrani L,Canet E, Lemiale V, Darmon M, Azoulay E (2013) Clinical assess-ment for identifying causes of acute respiratory failure in cancerpatients. Eur Respir J 42(2):435–443. doi:10.1183/09031936.00122512
8. Benoit DD, Hoste EA, Depuydt PO, Offner FC, Lameire NH,Vandewoude KH, Dhondt AW, Noens LA, Decruyenaere JM(2005) Outcome in critically ill medical patients treated with renalreplacement therapy for acute renal failure: comparison betweenpatients with and those without haematological malignancies.Nephrol Dial Transplant 20(3):552–558. doi:10.1093/ndt/gfh637
9. Canet E, Zafrani L, Lambert J, Thieblemont C, Galicier L, Schnell D,Raffoux E, Lengline E, Chevret S, Darmon M, Azoulay E (2013)Acute kidney injury in patients with newly diagnosed high-gradehematological malignancies: impact on remission and survival. PLoSOne 8(2):e55870. doi:10.1371/journal.pone.0055870
10. Pene F, Percheron S, Lemiale V, Viallon V, Claessens YE, Marque S,Charpentier J, Angus DC, Cariou A, Chiche JD, Mira JP (2008)Temporal changes in management and outcome of septic shock inpatients with malignancies in the intensive care unit. Crit Care Med36(3):690–696. doi:10.1097/CCM.0B013E318165314B
11. Zuber B, Tran TC, Aegerter P, Grimaldi D, Charpentier J, Guidet B,Mira JP, Pene F (2012) Impact of case volume on survival of septicshock in patients with malignancies. Crit Care Med 40(1):55–62. doi:10.1097/CCM.0b013e31822d74ba
12. Legrand M, Max A, Peigne V, Mariotte E, Canet E, Debrumetz A,Lemiale V, Seguin A, Darmon M, Schlemmer B, Azoulay E (2012)Survival in neutropenic patients with severe sepsis or septic shock.Crit Care Med 40(1):43–49. doi:10.1097/CCM.0b013e31822b50c2
13. van Vliet M, van den Boogaard M, Donnelly JP, Evers AW,Blijlevens NM, Pickkers P (2014) Long-term health related qualityof life following intensive care during treatment for haematologicalmalignancies. PLoS One 9(1):e87779. doi:10.1371/journal.pone.0087779
14. Azoulay E, Soares M, Darmon M, Benoit D, Pastores S, Afessa B(2011) Intensive care of the cancer patient: recent achievements andremaining challenges. Ann Intensiv Care 1(1):5. doi:10.1186/2110-5820-1-5
15. von Bergwelt-Baildon M, Hallek MJ, Shimabukuro-Vornhagen AA,Kochanek M (2010) CCC meets ICU: redefining the role of criticalcare of cancer patients. BMC Cancer 10:612. doi:10.1186/1471-2407-10-612
16. Darmon M, Thiery G, Ciroldi M, de Miranda S, Galicier L, RaffouxE, Le Gall JR, Schlemmer B, Azoulay E (2005) Intensive care inpatients with newly diagnosed malignancies and a need for cancerchemotherapy. Crit Care Med 33(11):2488–2493
17. Benoit DD, Depuydt PO, Vandewoude KH, Offner FC,Boterberg T, De Cock CA, Noens LA, Janssens AM,Decruyenaere JM (2006) Outcome in severely ill patients withhematological malignancies who received intravenous chemo-therapy in the intensive care unit. Intensive Care Med 32(1):93–99. doi:10.1007/s00134-005-2836-5
18. Song JU, Suh GY, Chung MP, Kim H, Kwon OJ, Jung CW, KangWK, Park K, Jeon K (2011) Risk factors to predict outcome incritically ill cancer patients receiving chemotherapy in the intensivecare unit. Support Care Cancer 19(4):491–495. doi:10.1007/s00520-010-0841-x
Ann Hematol (2014) 93:1629–1636 1635

19. Lecuyer L, Chevret S, Thiery G, Darmon M, Schlemmer B, AzoulayE (2007) The ICU trial: a new admission policy for cancer patientsrequiring mechanical ventilation. Crit Care Med 35(3):808–814. doi:10.1097/01.CCM.0000256846.27192.7A
20. OkenMM, Creech RH, Tormey DC, Horton J, Davis TE, McFaddenET, Carbone PP (1982) Toxicity and response criteria of the EasternCooperative Oncology Group. Am J Clin Oncol 5(6):649–655
21. Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A newmethod of classifying prognostic comorbidity in longitudinal studies:development and validation. J Chronic Dis 40(5):373–383
22. Le Gall JR, Lemeshow S, Saulnier F (1993) A new Simplified AcutePhysiology Score (SAPS II) based on a European/North Americanmulticenter study. JAMA 270(24):2957–2963
23. Schellongowski P, Benesch M, Lang T, Traunmuller F, Zauner C,Laczika K, Locker GJ, Frass M, Staudinger T (2004) Comparison ofthree severity scores for critically ill cancer patients. Intensive CareMed 30(3):430–436. doi:10.1007/s00134-003-2043-1
24. Taylor FB Jr, Toh CH, Hoots WK, Wada H, Levi M (2001) Towardsdefinition, clinical and laboratory criteria, and a scoring system fordisseminated intravascular coagulation. Thromb Haemost 86(5):1327–1330
25. Darmon M, Vincent F, Camous L, Canet E, Bonmati C, Braun T,Caillot D, Cornillon J, Dimicoli S, Etienne A, Galicier L, Garnier A,Girault S, Hunault-Berger M, Marolleau JP, Moreau P, Raffoux E,Recher C, Thiebaud A, Thieblemont C, Azoulay E (2013) Tumourlysis syndrome and acute kidney injury in high-risk haematologypatients in the rasburicase era. A prospective multicentre study fromthe Groupe de Recherche en Reanimation Respiratoire et Onco-Hematologique. Br J Haematol 162(4):489–497. doi:10.1111/bjh.12415
26. Cairo MS, Coiffier B, Reiter A, Younes A (2010) Recommendationsfor the evaluation of risk and prophylaxis of tumour lysis syndrome
(TLS) in adults and children with malignant diseases: an expert TLSpanel consensus. Br J Haematol 149(4):578–586. doi:10.1111/j.1365-2141.2010.08143.x
27. Zweig MH, Campbell G (1993) Receiver-operating characteristic(ROC) plots: a fundamental evaluation tool in clinical medicine.Clin Chem 39(4):561–577
28. Wohlfarth P, Ullrich R, Staudinger T, Bojic A, Robak O, Hermann A,Lubsczyk B, Worel N, Fuhrmann V, Schoder M, Funovics M,Rabitsch W, Knoebl P, Laczika K, Locker GJ, Sperr WR,Schellongowski P (2014) Extracorporeal membrane oxygenation inadult patients with hematologic malignancies and severe acute respi-ratory failure. Crit Care 18(1):R20. doi:10.1186/cc13701
29. Schellongowski P, Staudinger T, Kundi M, Laczika K, Locker GJ,Bojic A, Robak O, Fuhrmann V, Jager U, Valent P, Sperr WR (2011)Prognostic factors for intensive care unit admission, intensive careoutcome, and post-intensive care survival in patients with de novoacute myeloid leukemia: a single center experience. Haematologica96(2):231–237. doi:10.3324/haematol.2010.031583
30. Mokart D, Lambert J, Schnell D, Fouche L, Rabbat A, Kouatchet A,Lemiale V, Vincent F, Lengline E, Bruneel F, Pene F, Chevret S,Azoulay E (2013) Delayed intensive care unit admission is associatedwith increasedmortality in patients with cancer with acute respiratoryfailure. Leuk Lymphoma 54(8):1724–1729. doi:10.3109/10428194.2012.753446
31. Coiffier B, Altman A, Pui CH, Younes A, Cairo MS (2008)Guidelines for the management of pediatric and adult tumor lysissyndrome: an evidence-based review. J Clin Oncol 26(16):2767–2778. doi:10.1200/JCO.2007.15.0177
32. Lopez-Olivo MA, Pratt G, Palla SL, Salahudeen A (2013)Rasburicase in tumor lysis syndrome of the adult: a systematicreview and meta-analysis. Am J Kidney Dis 62(3):481–492. doi:10.1053/j.ajkd.2013.02.378
1636 Ann Hematol (2014) 93:1629–1636