Embed Size (px)
Citation preview
Program Project IV:
The Biology of Chronic
Disease Emergence
• Add Health Program Project IV:
The Biology of Chronic Disease Emergence
– context for project inception
– motivation for its development
– knowledge gaps
– introduction to the study intent on filling them
– aims
– cohort surveillance initiative
– preliminary findings
– summary
Overview
• As of 2013, cardiovascular disease (CVD) mortality in
the U.S. had been slowly declining
Circulation 2016;133:e38-e360.
Context
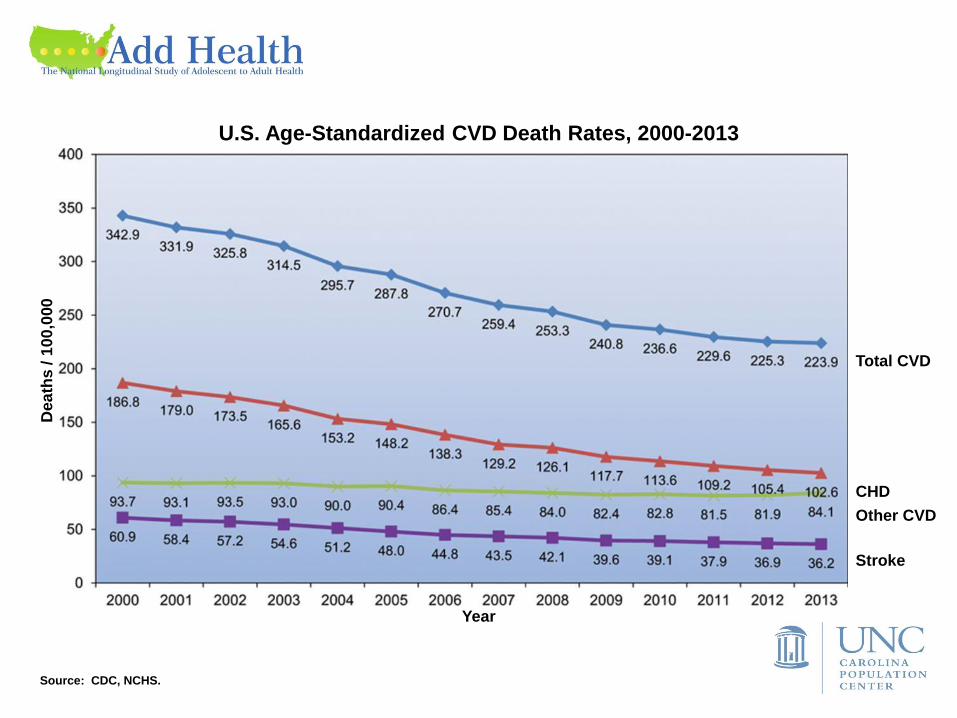
Year
CHD
Stroke
Other CVD
Total CVD
Dea
ths
/ 1
00
,000
U.S. Age-Standardized CVD Death Rates, 2000-2013
Source: CDC, NCHS.
Circulation 2016;133:e38-e360.
• However, at that time in the U.S., CVD events were still
– occurring every 34-40 seconds
– accounting for ~ 610-660k new cases / year
– costing us ~ $317 billion / year
• So the national burden of CVD remained quite high…
Context
Age (years)
% o
f P
op
ula
tio
n
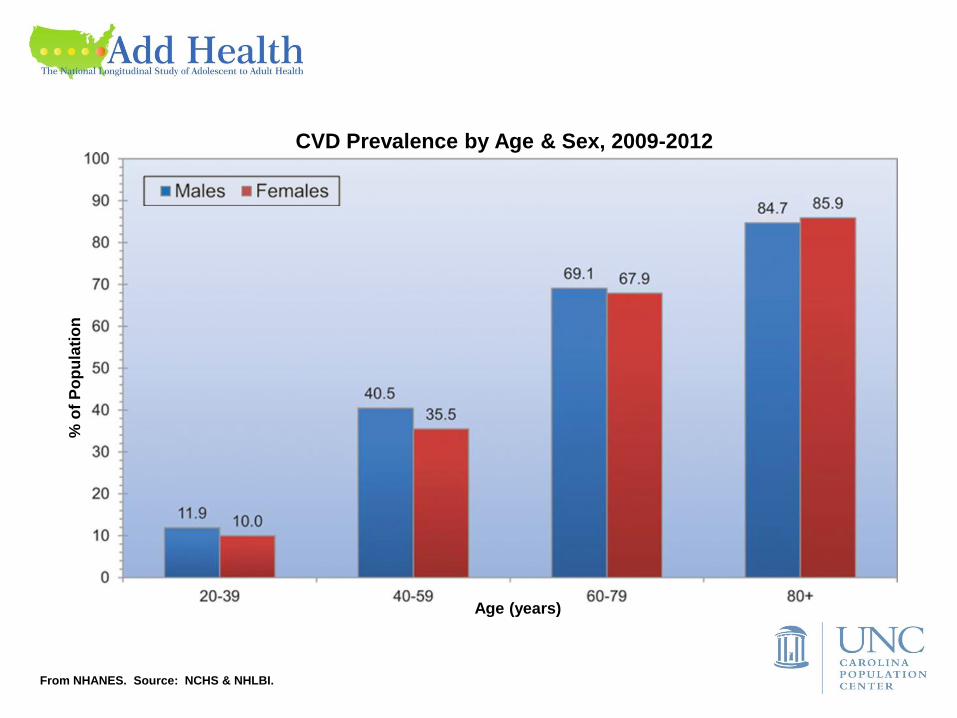
CVD Prevalence by Age & Sex, 2009-2012
From NHANES. Source: NCHS & NHLBI.
Dea
ths
in
Th
ou
sa
nd
s
Can
ce
r
Ac
cid
en
ts
CL
RD
DM
AD
Can
ce
r
Ac
cid
en
ts
CL
RD
DM
AD
CV
D
CV
D
Cause
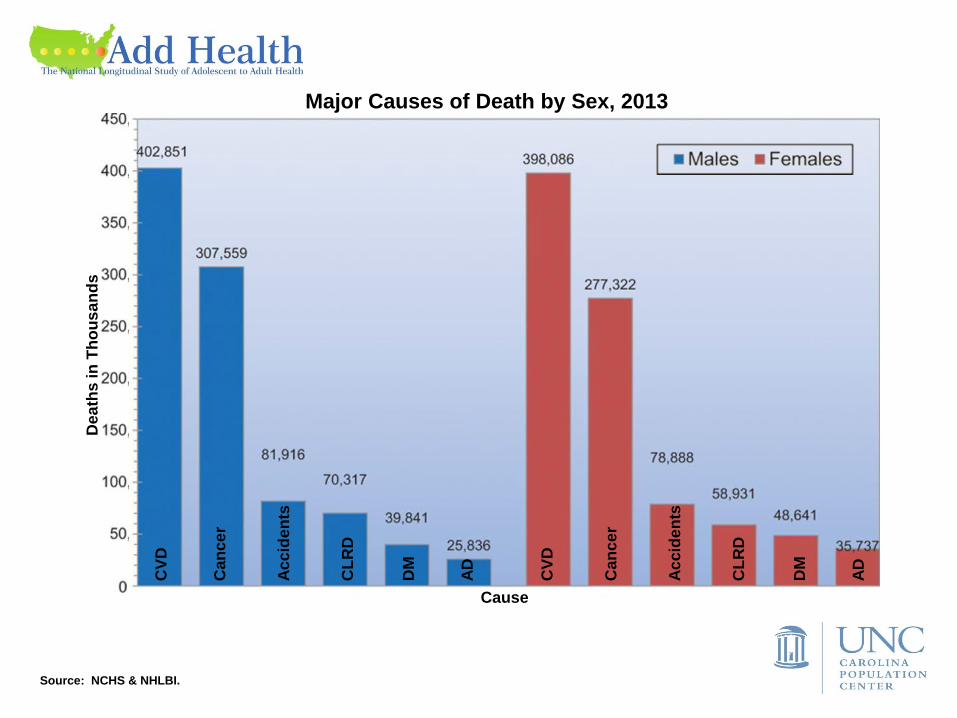
Major Causes of Death by Sex, 2013
Source: NCHS & NHLBI.
Source: NCHS.
Dea
ths
in
Th
ou
sa
nd
s
Age (years)
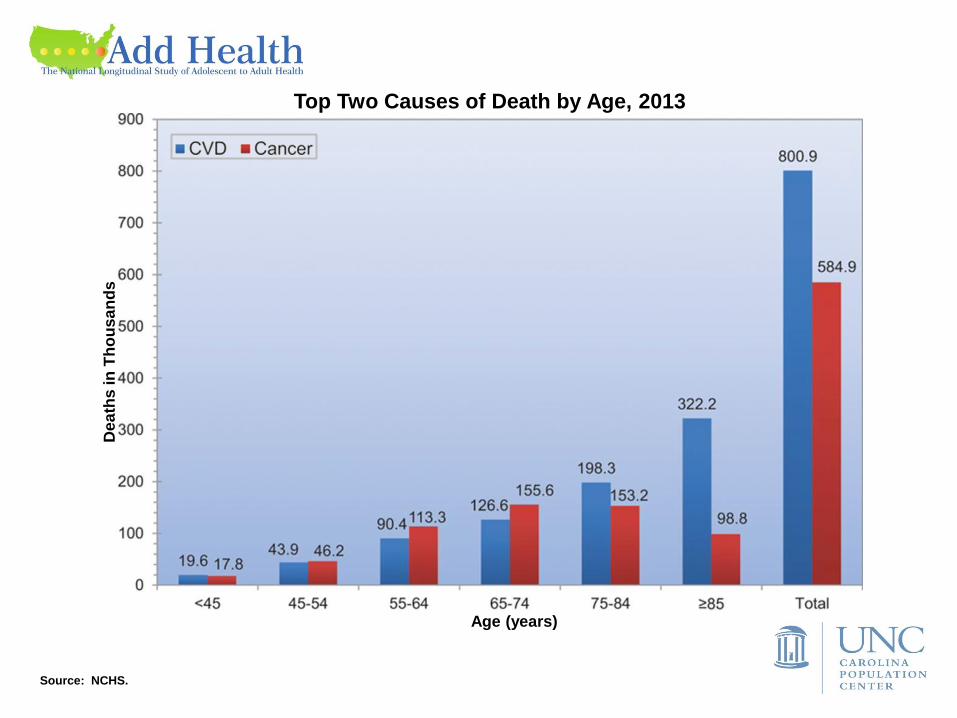
Top Two Causes of Death by Age, 2013
Circulation 2016;133:e38-e360.
Motivation • Although ~ 70% of CVD can be averted or delayed via
prevention, screening & intervention
– CVD risk reduction in U.S. adults is challenging
• 69% overweight/obese
• 33% hypertensive
• 17% currently smoking
• 13% hypercholesterolemic
• 12% diabetic
– temporal evolution of CVD burden was anticipated
• Although young adults can be mischaracterized as
unburdened by CVD & other chronic diseases
– the challenge of CVD risk reduction isn’t peculiar to
older U.S. adults
– Add Health Wave IV illustrated this…
Motivation
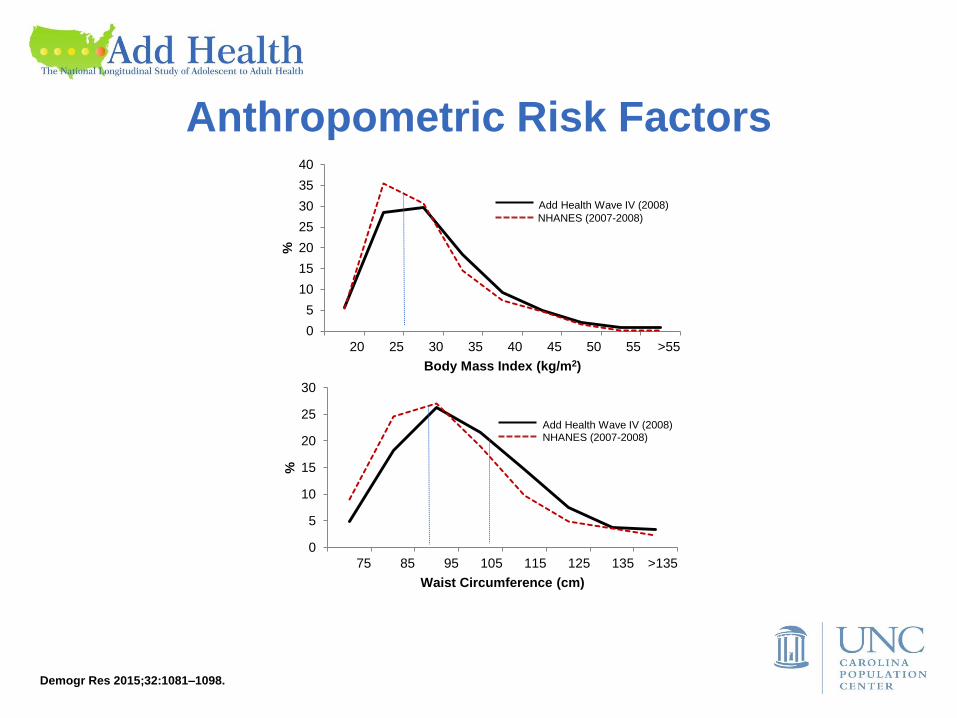
Demogr Res 2015;32:1081–1098.
0
5
10
15
20
25
30
75 85 95 105 115 125 135 >135
%
Waist Circumference (cm)
Add Health Wave IV (2008) NHANES (2007-2008)
0
5
10
15
20
25
30
35
40
20 25 30 35 40 45 50 55 >55
%
Body Mass Index (kg/m2)
Add Health Wave IV (2008)
NHANES (2007-2008)
Anthropometric Risk Factors
0
.01
.0
2
.03
.0
4
Density
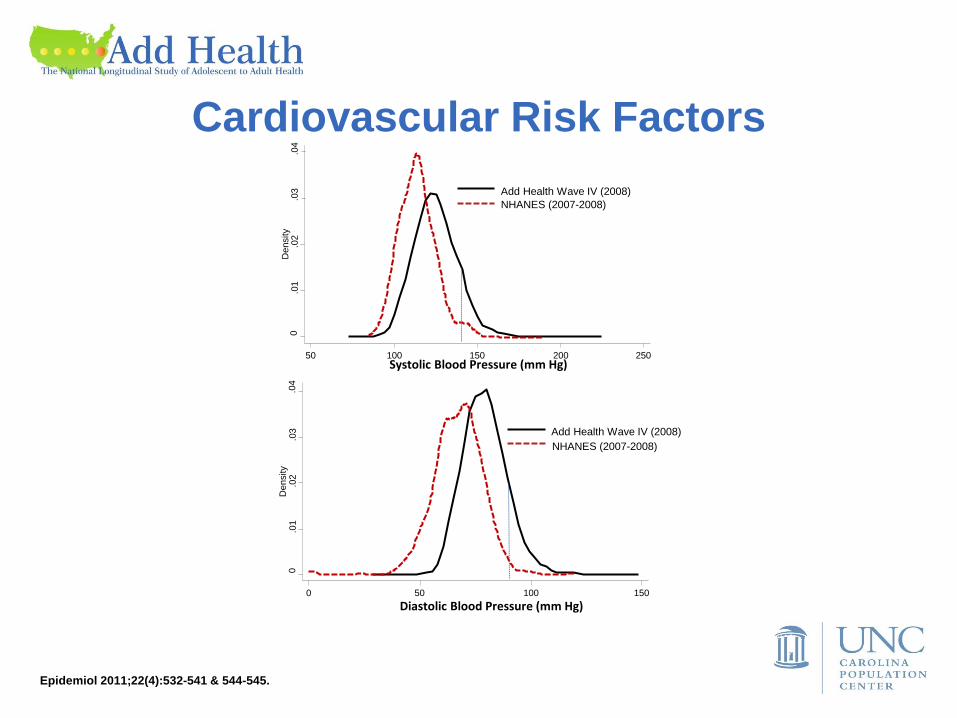
50 100 150 200 250
Add Health Wave IV (2008)
NHANES (2007-2008)
Systolic Blood Pressure (mm Hg)
0
.01
.0
2
.03
.0
4
Density
0 50 100 150
Diastolic Blood Pressure (mm Hg)
Add Health Wave IV (2008)
NHANES (2007-2008)
Epidemiol 2011;22(4):532-541 & 544-545.
Cardiovascular Risk Factors
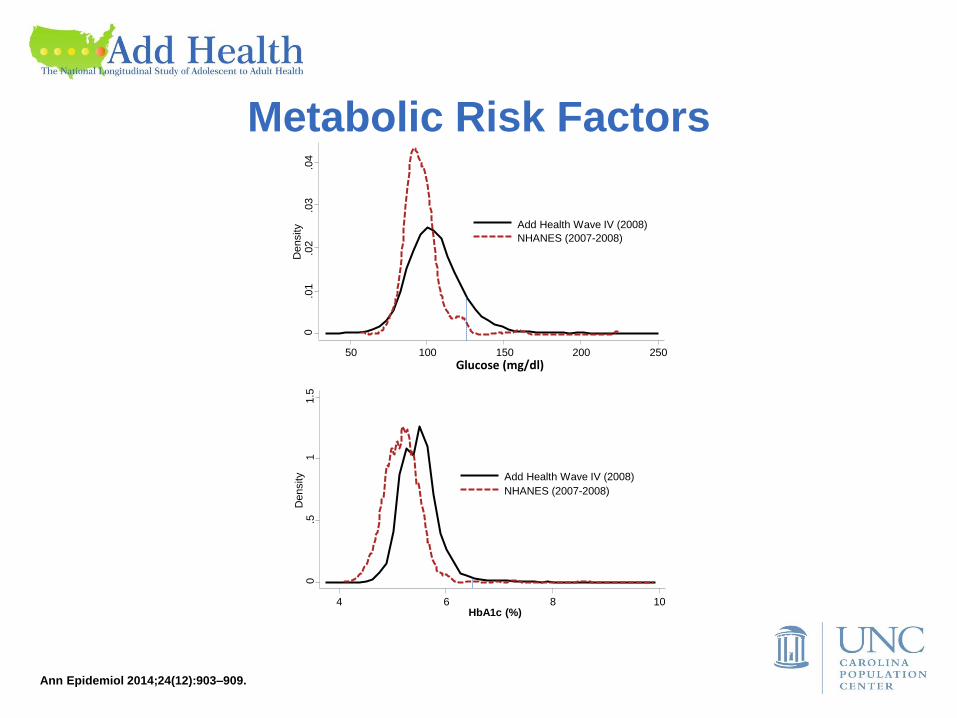
0
.01
.0
2
.03
.0
4
Density
50 100 150 200 250
Glucose (mg/dl)
Add Health Wave IV (2008)
NHANES (2007-2008)
0
.5
1
1.5
D
ensity
4 6 8 10 HbA1c (%)
Add Health Wave IV (2008)
NHANES (2007-2008)
Ann Epidemiol 2014;24(12):903–909.
Metabolic Risk Factors
• These & other factors ↑ risk of subclinical atherosclerosis
or hemorrhage of the arteries supplying e.g.
– brain
– heart
– abdomen
– kidneys
– lower extremities
• The risk often culminates in later life as overt CVD with
obvious implications for public health
– carotid artery disease, TIA, stroke
– CHD, MI, HF
– AAA, dissection, ischemic bowel
– renal artery stenosis, CKD, ESRD
– PAD, critical limb ischemia
Motivation
• Generally, to study emergence of CVD & other chronic
diseases in U.S. adults at risk
• Specifically, to study emergence of CVD & other chronic
diseases in the Add Health cohort through Wave V,
despite its current focus on younger adults
Motivation
• CVD & other chronic disease risk factors had not been
thoroughly examined in a contemporary or nationally
representative study capable of documenting changes in
& manifestations of those risks from adolescence
through 4th decade of life, after which virtually no one
has ideal CV health
• Their examination awaited greater availability, diversity &
generalizability of longitudinal data capable of supporting
epidemiologic inferences about chronic disease risk to
the larger population of young adults
Knowledge Gaps
• Enter
Add Health Program Project IV:
The Biology of Chronic Disease Emergence
• http://www.cpc.unc.edu/projects/addhealth
• https://projectreporter.nih.gov/ (subproject ID: 5096)
Introduction
• (1) Design protocols for collecting bio data / specimens
• (2) Monitor & control field / lab operations so as to
ensure high quality bio data & specimens
• (3) Estimate prevalence / incidence of societally
burdensome chronic diseases & disparities in their
distributions
• (4) Serve as the bio data resource to the program & the
entire scientific community
• (5) Implement a scalable surveillance system for chronic
disease events
Aims
• (1) Design protocols for collecting bio data / specimens
• (2) Monitor & control field / lab operations so as to
ensure high quality bio data & specimens
• (3) Estimate prevalence / incidence of societally
burdensome chronic diseases & disparities in their
distributions
• (4) Serve as the bio data resource to the program & the
entire scientific community
• (5) Implement a scalable surveillance system for chronic
disease events
Aims
• Implement a scalable surveillance system for chronic
disease events
– ascertainment
– review
– adjudication
– classification
• Begin w/ participant deaths due to e.g.
– accidents
– CVD
– cancer
• Thereby position the study for
– ongoing surveillance of mortality
– potential expansion to morbidity
Surveillance
• How do you do that?
– assemble experienced team
Surveillance
Surveillance Team

CSI: Add Health
Surveillance Team
CSI: Add Health
Eric
Whitsel
Laura
Loehr
Bob
Hummer Elyssa
Trani Carol
Murphy
Surveillance Team
• How do you do that?
– assemble experienced team
– develop standardized protocol
Surveillance
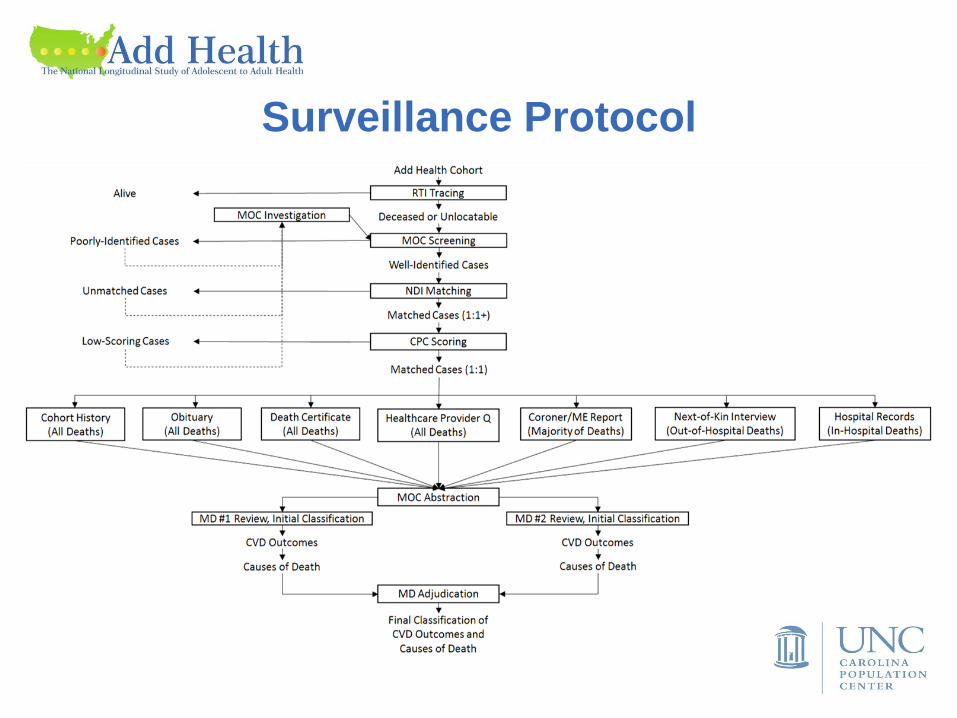
Surveillance Protocol
• How do you do that?
– assemble experienced team
– develop standardized protocol
• NDI matching
• CPC scoring
• MOC investigation
• MD review, classification & adjudication
Surveillance
• NDI matching
Determine if Add Health & NDI agree re ≥ 1 of:
– SSN
– month & ±1 year of birth, 1st & last name
– month & ± 1 year of birth, 1st & mid initial, last name
– month & day of birth, 1st & last name
– month & day of birth, 1st & mid initials, last name
Surveillance
• CPC scoring*
Assign points based on match of: – 1st name or initial (0;1) – SSN (0-9)
– middle initial (0;1) – birth day (0;2)
– last name (0;2) – birth month (0;2)
– sex (0;1) – birth year (0;2)
– state of residence (0;1) Sum & group scores, as follows:
Total Group
0-11 non-match
12-19 potential match, investigate
20-21 match
Surveillance
*Based on Atherosclerosis Risk in Communities (ARIC) algorithm.
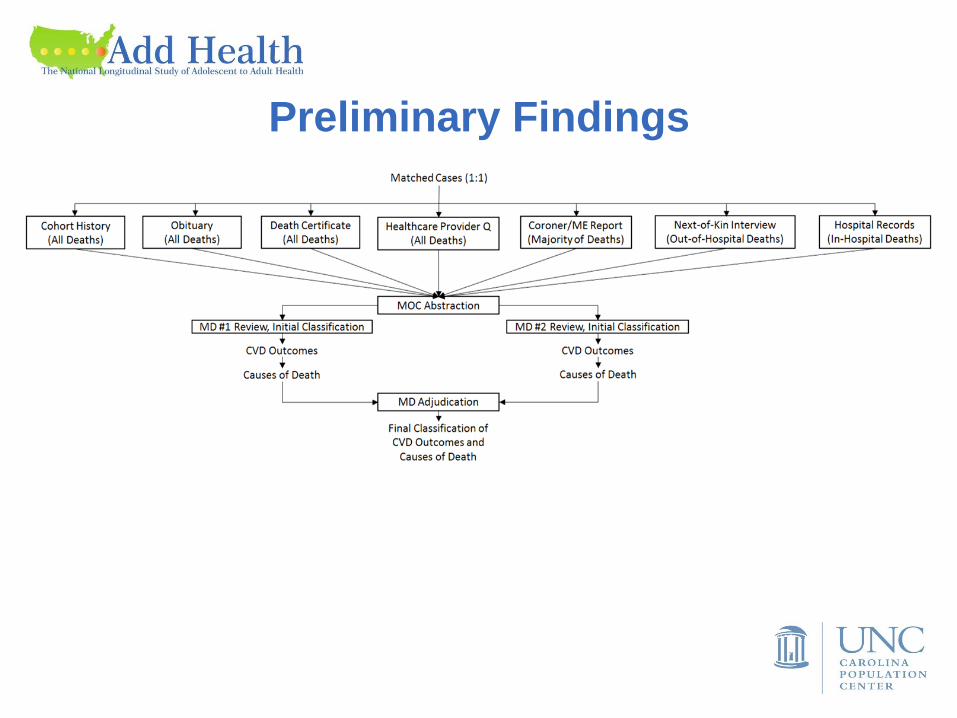
• MOC investigation
Assemble, abstract & enter into DES – cohort history (automatic)
– obituary
– death certificate
– health provider Q
– ME/coroner report
– next-of-kin interview
– hospital records
• MD review, classification
& adjudication
Surveillance
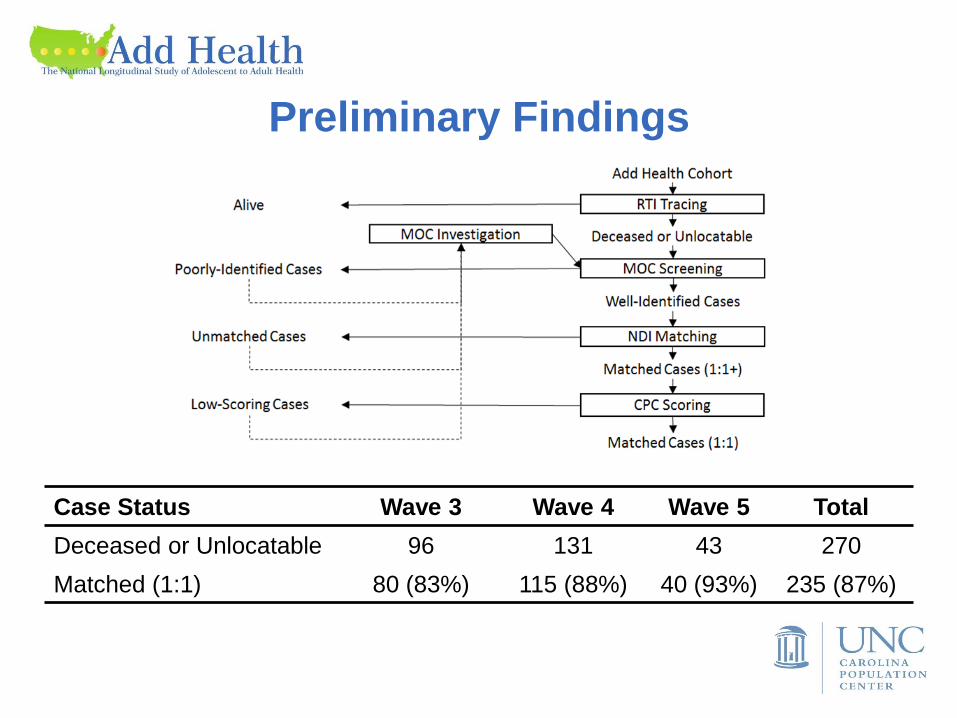
Preliminary Findings
Case Status Wave 3 Wave 4 Wave 5 Total
Deceased or Unlocatable 96 131 43 270
Matched (1:1) 80 (83%) 115 (88%) 40 (93%) 235 (87%)
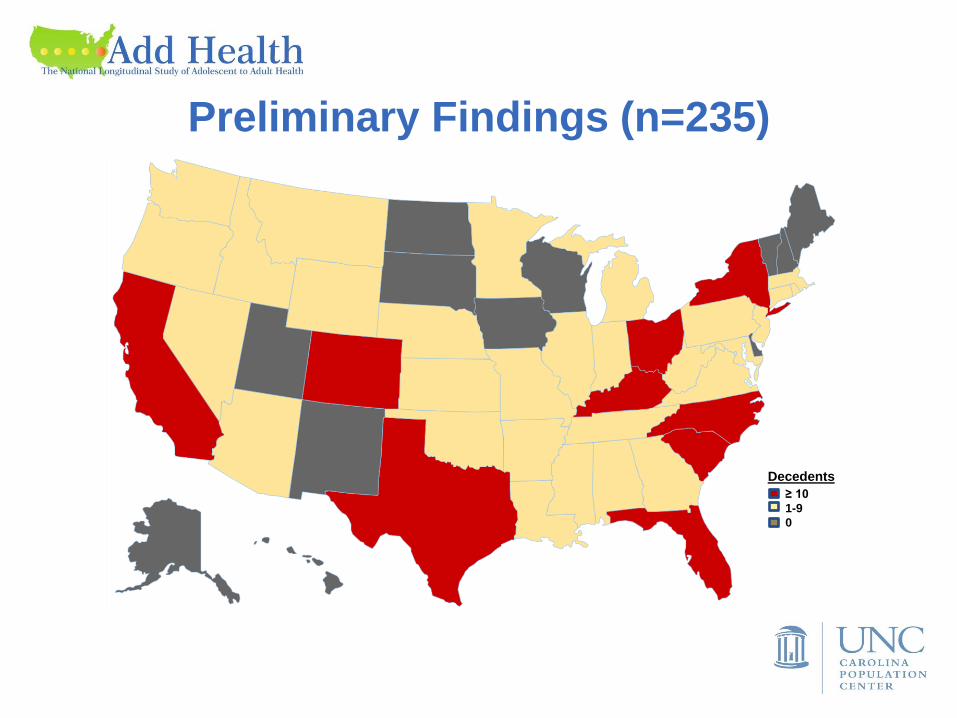
Preliminary Findings (n=235)
≥ 10
1-9
0
Decedents
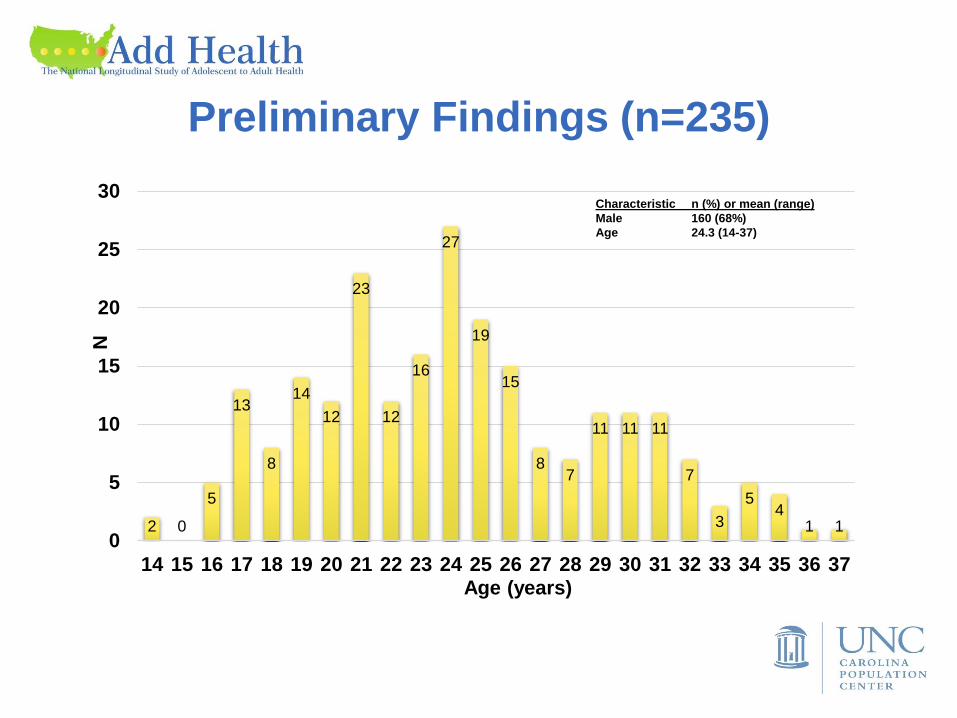
Preliminary Findings (n=235)
2 0
5
13
8
14
12
23
12
16
27
19
15
8 7
11 11 11
7
3
5 4
1 1 0
5
10
15
20
25
30
14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37
N
Age (years)
Characteristic n (%) or mean (range)
Male 160 (68%)
Age 24.3 (14-37)
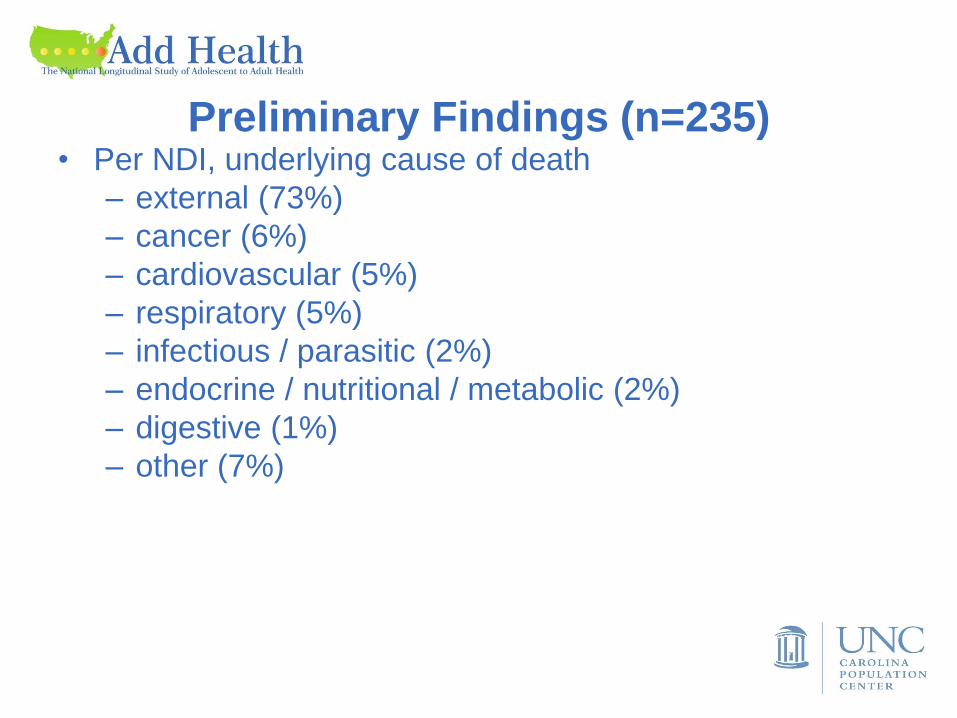
Preliminary Findings (n=235) • Per NDI, underlying cause of death
– external (73%)
– cancer (6%)
– cardiovascular (5%)
– respiratory (5%)
– infectious / parasitic (2%)
– endocrine / nutritional / metabolic (2%)
– digestive (1%)
– other (7%)
Preliminary Findings
Summary • Add Health Program Project IV:
The Biology of Chronic Disease Emergence
• Scalable surveillance system for chronic disease events
• Our hope is that the data it generates will help
– support your research
– generate actionable, timely knowledge for public
health professionals at the local, state, regional &
national levels
– assess the latest DHHS & AHA prevention efforts
• by 2016, to thwart 1 million MIs & strokes
• by 2020, to ↑ CV health of the US population
to ↓ CVD deaths by 20%





























