Embed Size (px)
Citation preview

11/2/11
1
Catheter Ablation of Atrial Fibrillation Has Become the Prime Therapy for Most Patients
with Atrial Fibrillation
♥ Proponent: Roger A. Winkle
♥ Disclosures • Investigator for Cardiorobotics • Investigator for CABANA trial • Investigator Medtronic • MelScheinerone is not FDA approved • I have no financial interest in MelScheinerone
Questions
1. I believe in Afib ablation and it is my treatment of choice for symptomatic patients
2. I like the idea of Afib ablation but there are too many complications
3. I like the idea of Afib ablation but it does not cure enough patients to make it worthwhile
4. I like the idea of Afib ablation but there are too many complications and it does not cure enough patients
5. I don’t like the idea of Afib ablation
11/2/11
2
Future Afib Ablator
Atrial Fibrillation is Bad!
♥ Symptoms are present in almost all patients
♥ Worsens most patient’s QOL ♥ Increases stroke risk substantially ♥ Results in multiple hospitalizations and
medical encounters ♥ Increases mortality ♥ Makes “patients fatter and wears out their
hearts”
11/2/11
3
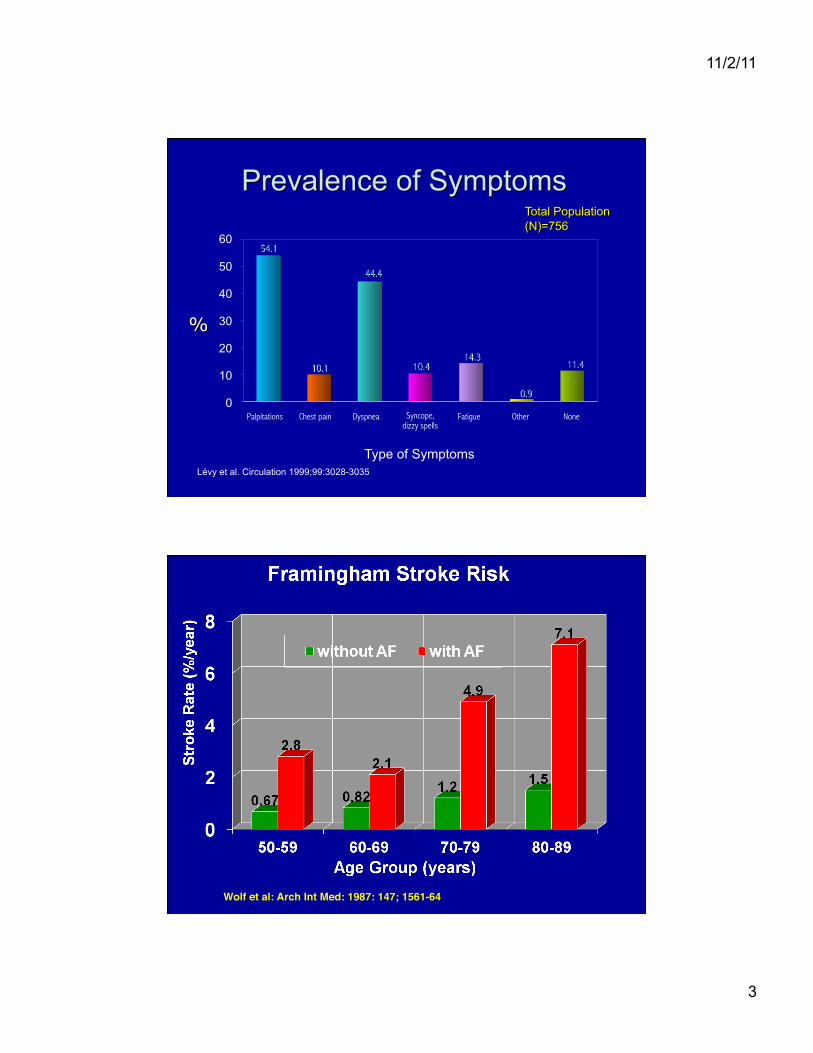
Lévy et al. Circulation 1999;99:3028-3035.
Type of Symptoms
Palpitations Chest pain Dyspnea Syncope, dizzy spells
Fatigue Other None
54.1
44.4
10.1 10.4 14.3
0.9
11.4
60
50
40
30
20
10
0
Wolf et al: Arch Int Med: 1987: 147; 1561-64"
11/2/11
4
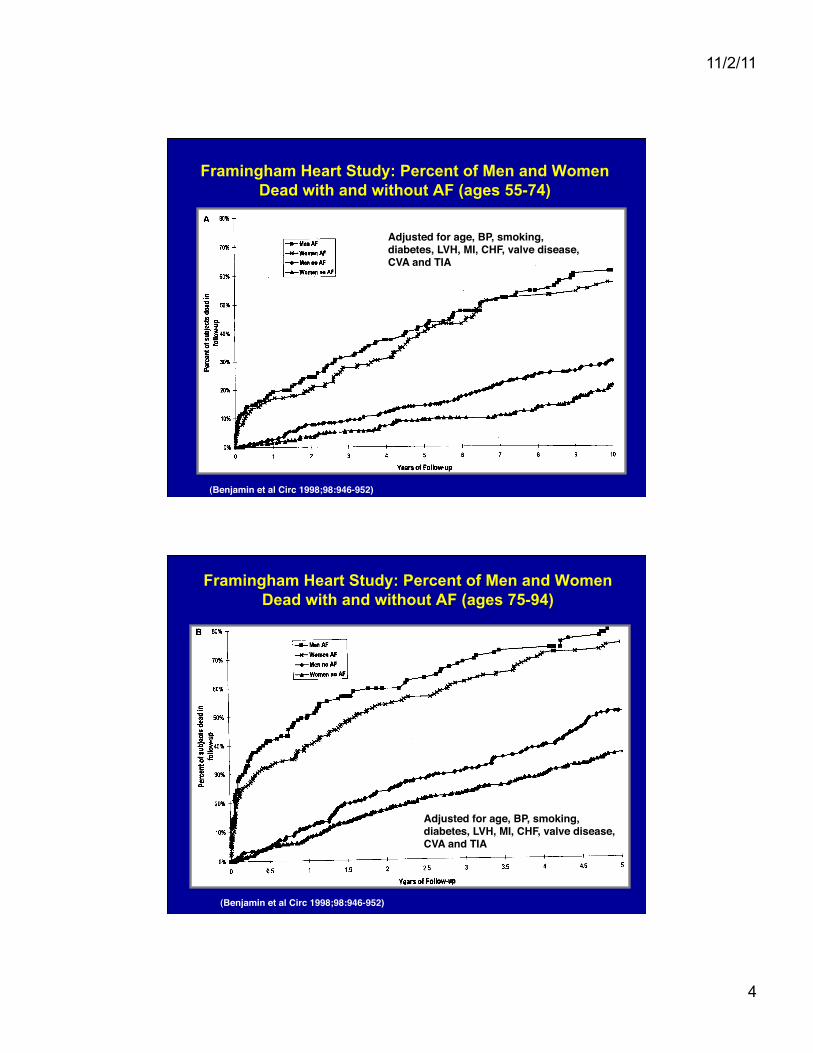
Framingham Heart Study: Percent of Men and Women Dead with and without AF (ages 55-74)
(Benjamin et al Circ 1998;98:946-952)"
Adjusted for age, BP, smoking,"diabetes, LVH, MI, CHF, valve disease, "CVA and TIA"
Framingham Heart Study: Percent of Men and Women Dead with and without AF (ages 75-94)
(Benjamin et al Circ 1998;98:946-952)"
Adjusted for age, BP, smoking,"diabetes, LVH, MI, CHF, valve disease, "CVA and TIA"

11/2/11
5
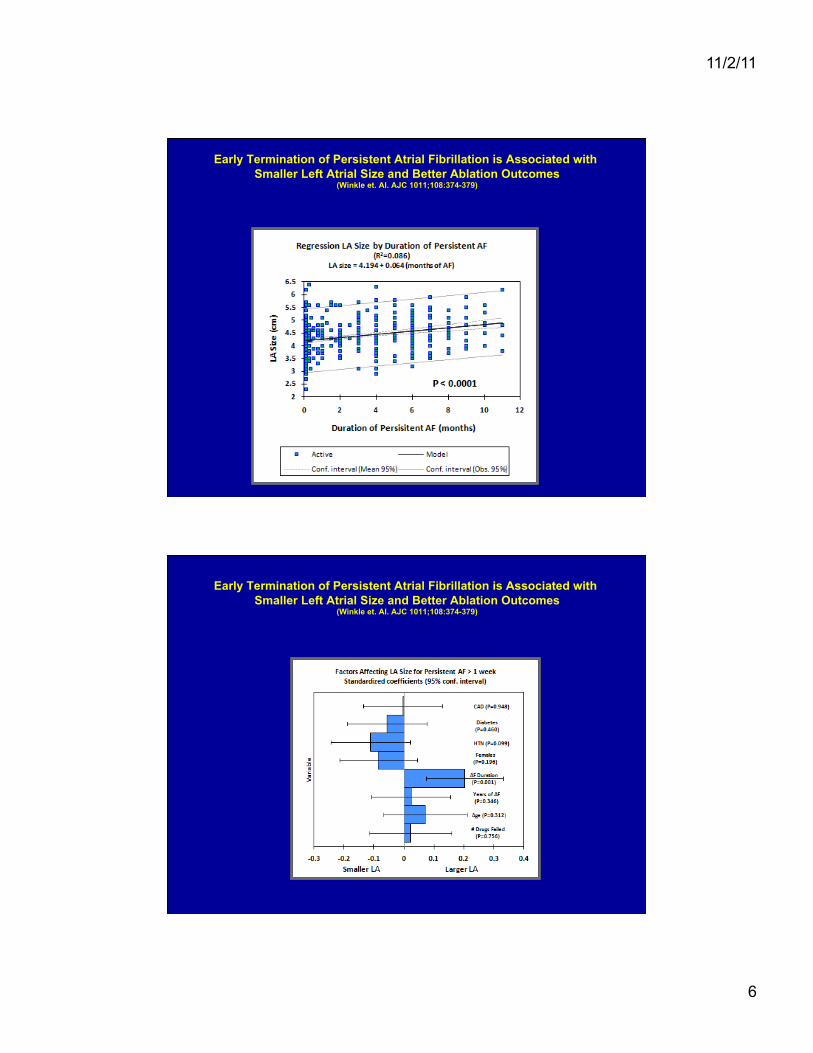
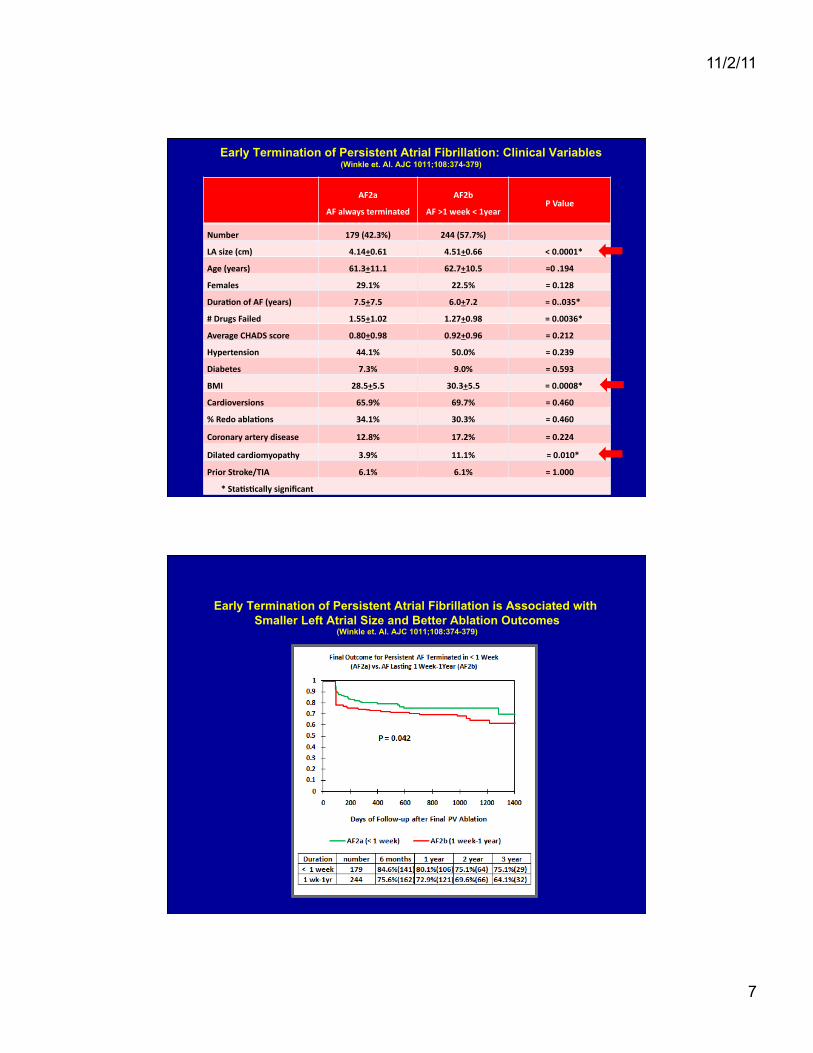
Early Termination of Persistent AF and Ablation Outcomes
(Winkle et. Al. AJC 1011;108:374-379)
Persistent AF (AF2)
♥ AF2a: 179 patients whose physicians always terminated persistent AF by drugs or CV in < 1 week
♥ AF2b: 244 patients left in persistent AF for > 1 week up to 1 year
Compared to
11/2/11
6
Early Termination of Persistent Atrial Fibrillation is Associated with Smaller Left Atrial Size and Better Ablation Outcomes
(Winkle et. Al. AJC 1011;108:374-379)
Early Termination of Persistent Atrial Fibrillation is Associated with Smaller Left Atrial Size and Better Ablation Outcomes
(Winkle et. Al. AJC 1011;108:374-379)
11/2/11
7
AF2a
AF always terminated
AF2b
AF >1 week < 1year P Value
Number 179 (42.3%) 244 (57.7%)
LA size (cm) 4.14+0.61 4.51+0.66 < 0.0001*
Age (years) 61.3+11.1 62.7+10.5 =0 .194
Females 29.1% 22.5% = 0.128
DuraNon of AF (years) 7.5+7.5 6.0+7.2 = 0..035*
# Drugs Failed 1.55+1.02 1.27+0.98 = 0.0036*
Average CHADS score 0.80+0.98 0.92+0.96 = 0.212
Hypertension 44.1% 50.0% = 0.239
Diabetes 7.3% 9.0% = 0.593
BMI 28.5+5.5 30.3+5.5 = 0.0008*
Cardioversions 65.9% 69.7% = 0.460
% Redo ablaNons 34.1% 30.3% = 0.460
Coronary artery disease 12.8% 17.2% = 0.224
Dilated cardiomyopathy 3.9% 11.1% = 0.010*
Prior Stroke/TIA 6.1% 6.1% = 1.000
* StaNsNcally significant
Early Termination of Persistent Atrial Fibrillation: Clinical Variables (Winkle et. Al. AJC 1011;108:374-379)
Early Termination of Persistent Atrial Fibrillation is Associated with Smaller Left Atrial Size and Better Ablation Outcomes
(Winkle et. Al. AJC 1011;108:374-379)

11/2/11
8
Rate control is not the answer!
♥ Multiple studies compare rate control to rhythm control using AADs
♥ Rate control does nothing to reduce the stroke risk
♥ The drugs for rate control cause side effects and even death (digoxin)
♥ Due to poor AAD efficacy and crossovers the studies may not really show what they claim
♥ AADs may be so toxic that they “wipe out” any benefit of NSR
Atrial Fibrillation Follow-Up Investigation of Rhythm Management-The AFFIRM Study Design
(AFFIRM Investigators. NEJM 2002;347:1825-1833)
♥ Enrolled 4060 patients ♥ Patients with atrial fibrillation and high risk of
stroke ♥ All patients on anticoagulation with target INR =
2.5 (range 2.0-3.0) ♥ Randomized to initial strategy of rate control or
attempts to maintain NSR ♥ Primary endpoint: Total Mortality ♥ Intention to treat analysis
11/2/11
9
Atrial Fibrillation Follow-Up Investigation of Rhythm Management-The AFFIRM Study Design
(AFFIRM Investigators. NEJM 2002;347:1825-1833)
♥ Hypothesis: Antiarrhythmic therapy to maintain NSR has no effect on total mortality compared with therapy that controls the heart rate
♥ Enrolled 4060 patients ♥ Primary endpoint: Total Mortality ♥ Secondary endpoints
• mortality + CVA’s • mortality + CVA’s + cardiac arrest • cost • quality of life
♥ Intention to treat analysis
Atrial Fibrillation Follow-Up Investigation of Rhythm Management-The AFFIRM Study Design
(AFFIRM Investigators. NEJM 2002;347:1825-1833)
♥ Patients with atrial fibrillation and high risk of stroke • > 65 years old • < 65 years old and > 1 other risk factor
• (hypertension, diabetes, CHF, TIA, prior CVA, LA > 50mm, fractional shortening < 25%, LVEF< 40%)
♥ All patients on anticoagulation with target INR = 2.5 (range 2.0-3.0)
♥ All patients may have one initial successful cardioversion
♥ Randomized to initial strategy of rate control or attempts to maintain NSR
11/2/11
10
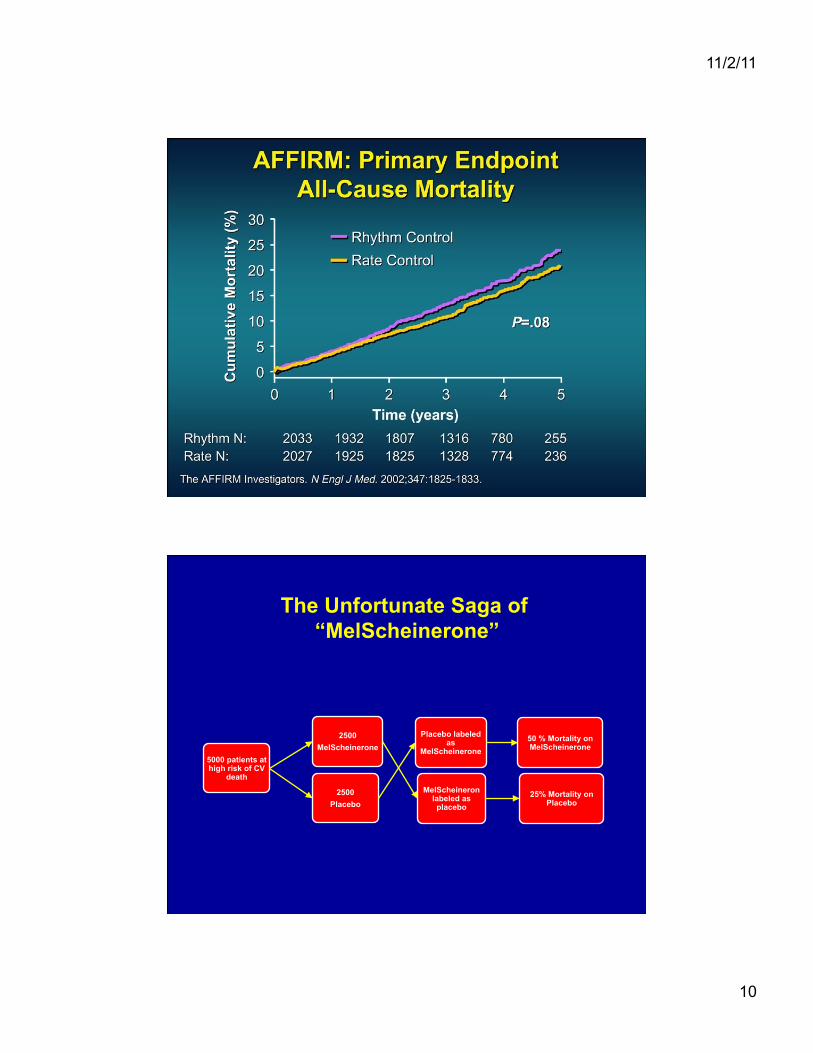
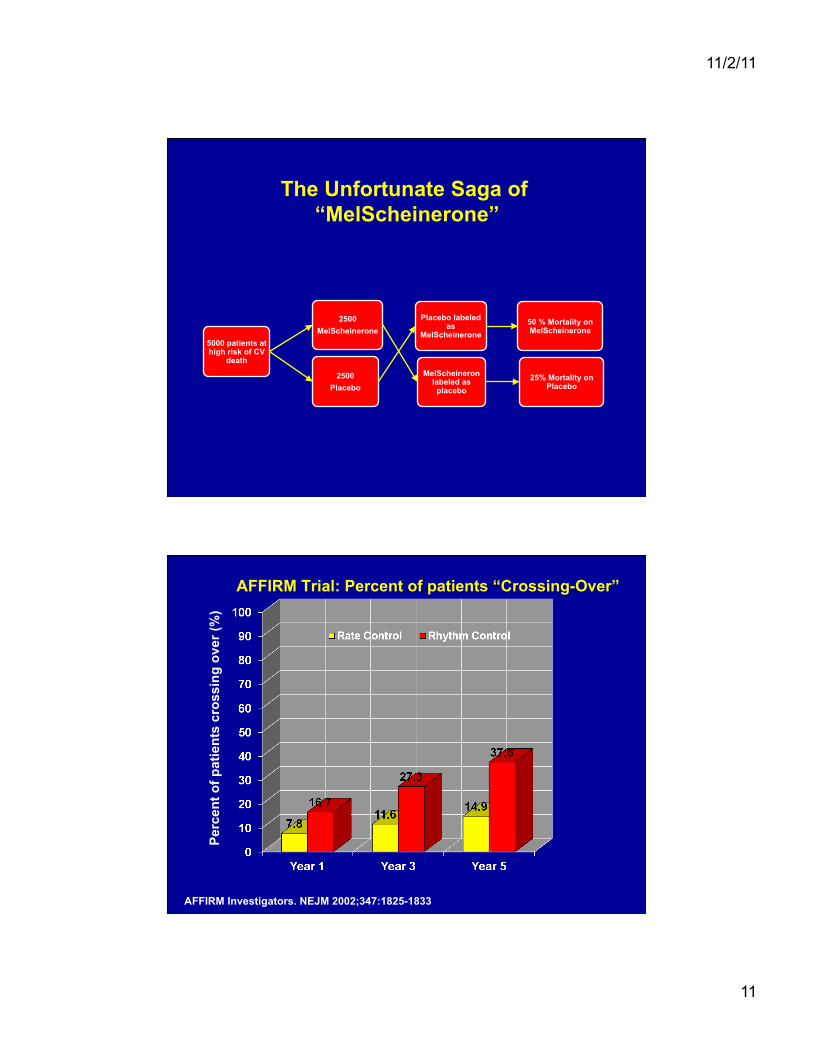
The Unfortunate Saga of “MelScheinerone”
5000 patients at high risk of CV
death
2500 MelScheinerone
MelScheineron labeled as placebo
25% Mortality on Placebo
2500 Placebo
Placebo labeled as
MelScheinerone 50 % Mortality on MelScheinerone
11/2/11
11
The Unfortunate Saga of “MelScheinerone”
5000 patients at high risk of CV
death
2500 MelScheinerone
MelScheineron labeled as placebo
25% Mortality on Placebo
2500 Placebo
Placebo labeled as
MelScheinerone 50 % Mortality on MelScheinerone
AFFIRM Trial: Percent of patients “Crossing-Over”
AFFIRM Investigators. NEJM 2002;347:1825-1833
Perc
ent o
f pat
ient
s cr
ossi
ng o
ver (
%)
11/2/11
12
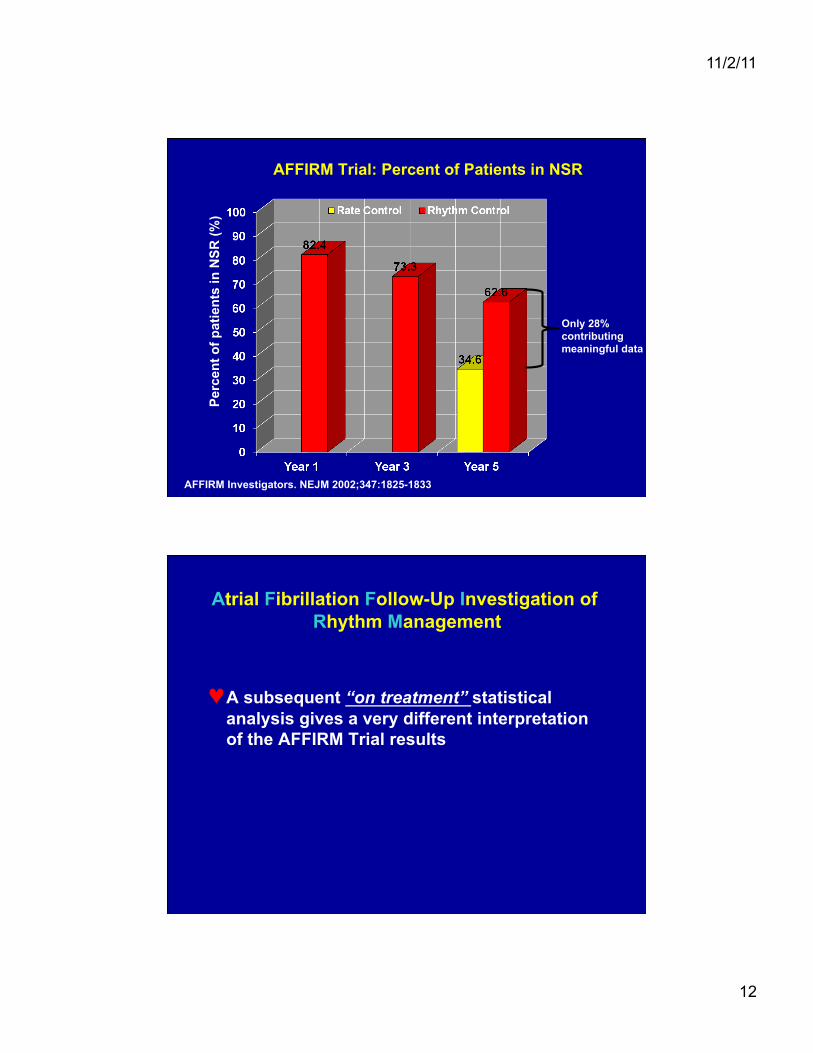
AFFIRM Trial: Percent of Patients in NSR
AFFIRM Investigators. NEJM 2002;347:1825-1833
Perc
ent o
f pat
ient
s in
NSR
(%)
Only 28% contributing meaningful data
Atrial Fibrillation Follow-Up Investigation of Rhythm Management
♥ A subsequent “on treatment” statistical analysis gives a very different interpretation of the AFFIRM Trial results
11/2/11
13
Atrial Fibrillation Follow-Up Investigation of Rhythm Management
♥ Due to the large number of cross-overs, the poor efficacy of AADs with many rhythm control patients in AF and the fact that many “rate control” patients were actually in NSR, Intention to treat analysis may be misleading
♥ A subsequent “on treatment” statistical analysis gives a very different interpretation of the AFFIRM Trial results
AFFIRM Trial: Importance of NSR (Circ 2004; 109:15009-1513)
11/2/11
14
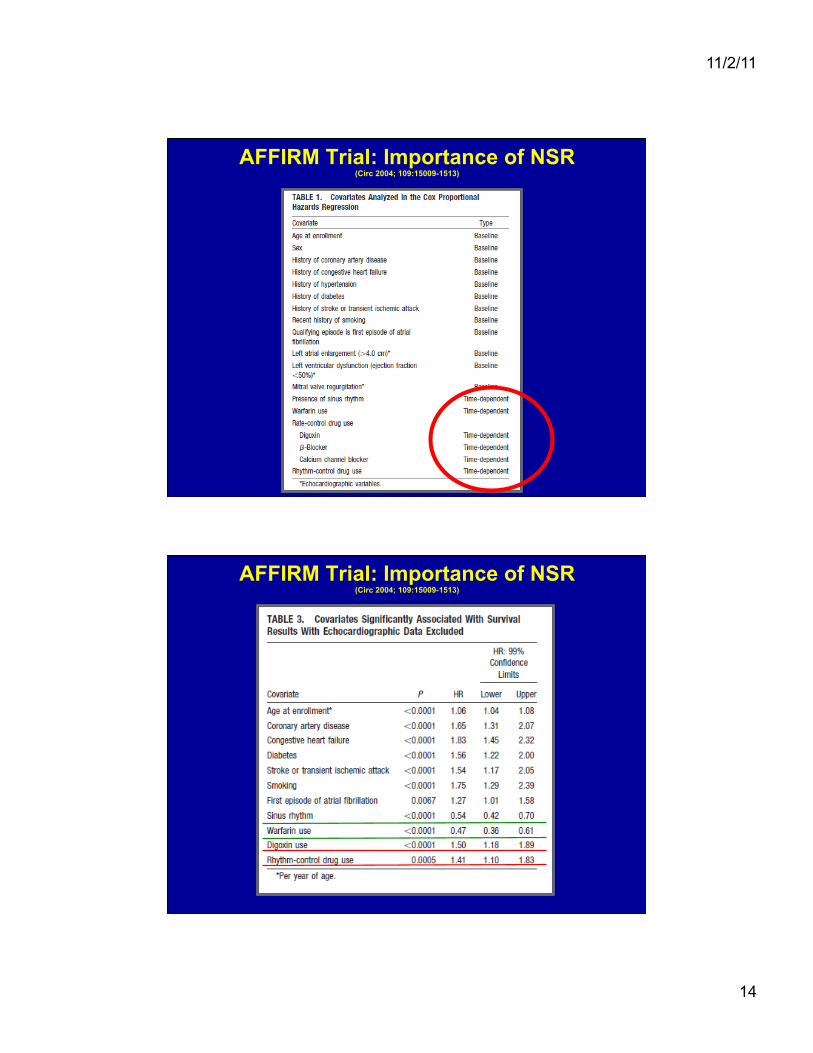
AFFIRM Trial: Importance of NSR (Circ 2004; 109:15009-1513)
AFFIRM Trial: Importance of NSR (Circ 2004; 109:15009-1513)

11/2/11
15
AFFIRM Trial: Importance of NSR (Circ 2004; 109:15009-1513)
Danish Investigators of Arrhythmia and Mortality on Dofetitlde in CHF (DIAMOND-CHF)
(NEJM 1999;341:857-865)
♥ 1518 patients with symptomatic CHF and LV dysfunction
♥ Double-blind, placebo controlled at 34 Danish centers
♥ Inclusion criteria • hospitalized patients with new or worsening CHF and • at least one episode of SOB on minimal exertion or at rest or
PND • ECHO with wall motion score of 1.2 or less (EF approx. 35%)
♥ Exclusion criteria acute MI within 7 days K+ < 3.6 or > 5.5 heart rate < 50 creatinine clearance < 20 cc/min SA or AV block without a pacer recent Class I or III antiarrhythmics history of proarrhythmia planned or recent PTCA/CABG QTc >460msec (>500 if bundle branch block) Aortic stenosis BP > 115 diastolic or < 80 systolic ICD

11/2/11
16
Dofetilide in patients with CHF and LV dysfunction (DIAMOND-CHF) (NEJM 1999;341:857-865)
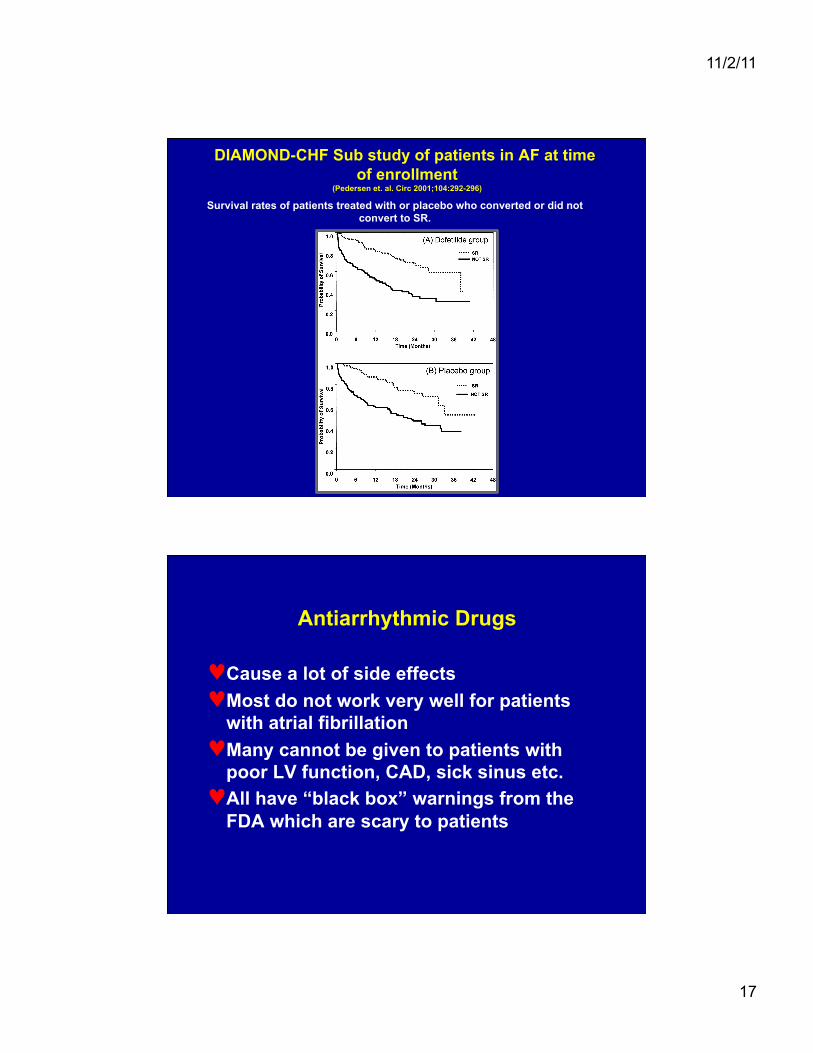
DIAMOND-CHF Sub study of patients in AF at time of enrollment
(Pedersen et. al. Circ 2001;104:292-296)
Probability of survival during treatment and follow-up periods in 506 patients with LV dysfunction and AF-AFl at baseline treated with dofetilide or placebo.
11/2/11
17
DIAMOND-CHF Sub study of patients in AF at time of enrollment
(Pedersen et. al. Circ 2001;104:292-296)
Survival rates of patients treated with or placebo who converted or did not convert to SR.
Antiarrhythmic Drugs
♥ Cause a lot of side effects ♥ Most do not work very well for patients
with atrial fibrillation ♥ Many cannot be given to patients with
poor LV function, CAD, sick sinus etc. ♥ All have “black box” warnings from the
FDA which are scary to patients
11/2/11
18
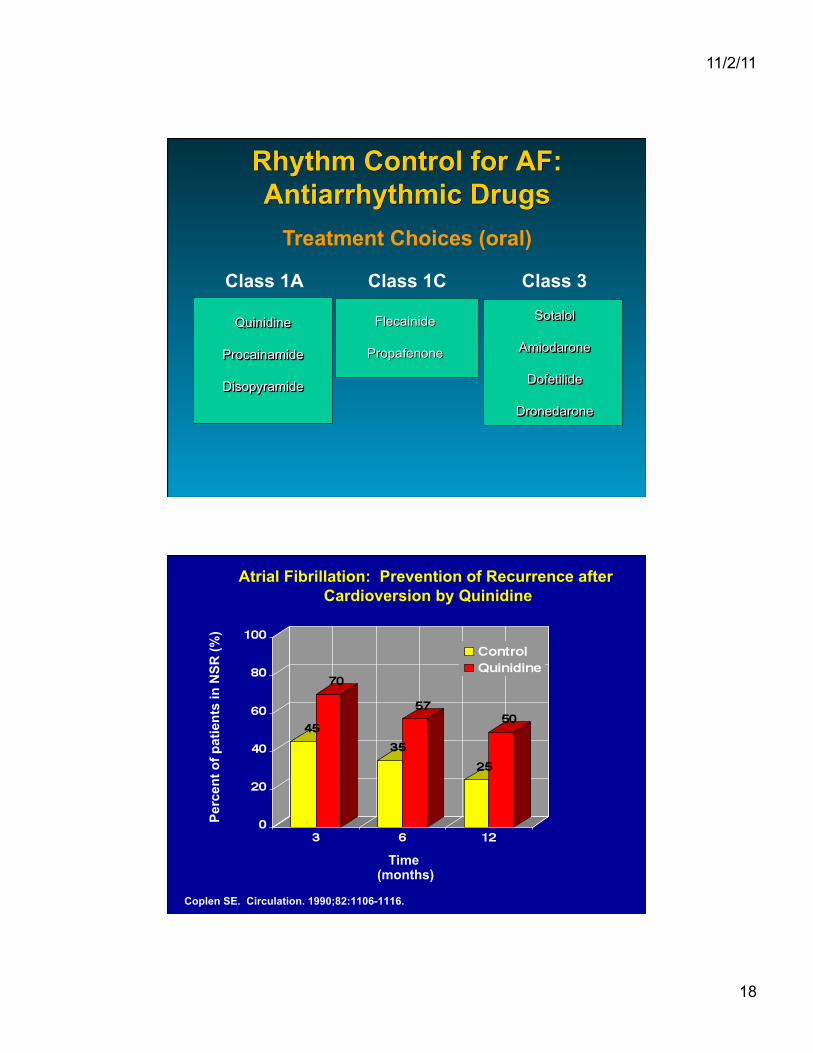
Rhythm Control for AF: Antiarrhythmic Drugs
Flecainide
Propafenone
Class 1A Class 1C Class 3
Treatment Choices (oral)
Atrial Fibrillation: Prevention of Recurrence after Cardioversion by Quinidine
Coplen SE. Circulation. 1990;82:1106-1116.
Perc
ent o
f pat
ient
s in
NSR
(%)
Time (months)
11/2/11
19
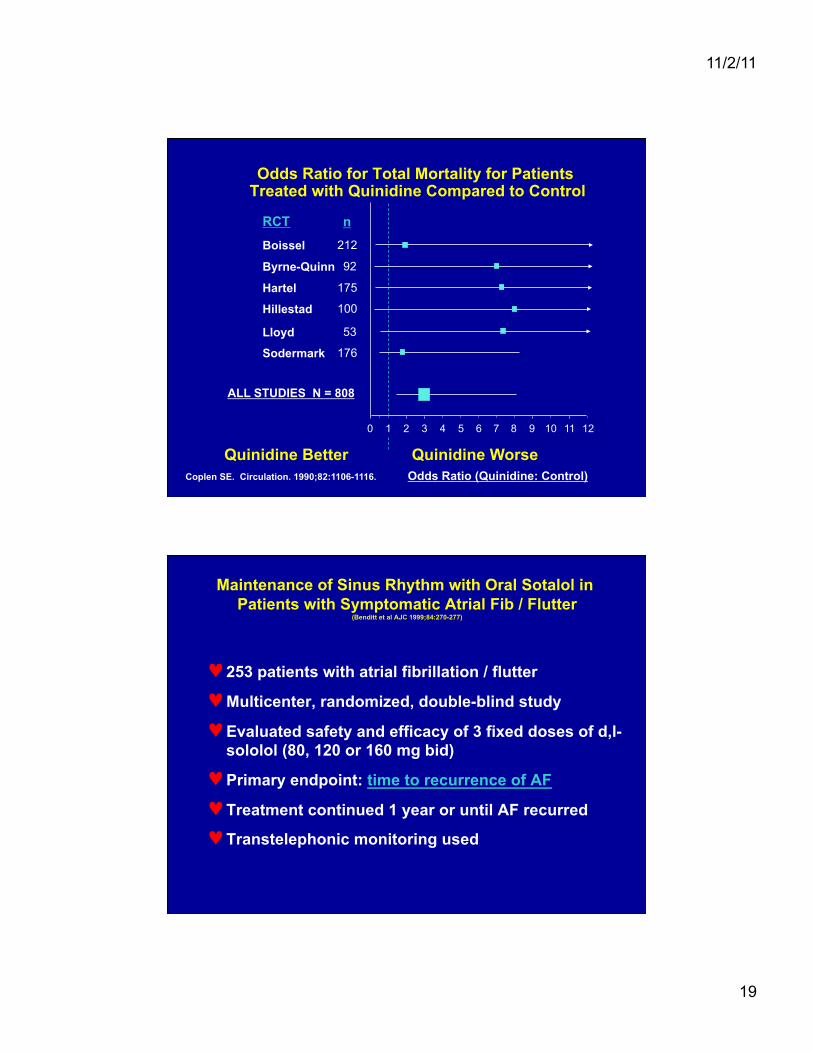
Odds Ratio for Total Mortality for Patients Treated with Quinidine Compared to Control
Coplen SE. Circulation. 1990;82:1106-1116.
RCT
Boissel
Byrne-Quinn
Hartel
Hillestad
Lloyd
Sodermark
ALL STUDIES N = 808
0 1 2 3 4 5 6 7 8 9 10 11 12
Odds Ratio (Quinidine: Control) Quinidine Better Quinidine Worse
212
92
175
100
53
176
n
Maintenance of Sinus Rhythm with Oral Sotalol in Patients with Symptomatic Atrial Fib / Flutter
(Benditt et al AJC 1999;84:270-277)
♥ 253 patients with atrial fibrillation / flutter
♥ Multicenter, randomized, double-blind study
♥ Evaluated safety and efficacy of 3 fixed doses of d,l-sololol (80, 120 or 160 mg bid)
♥ Primary endpoint: time to recurrence of AF
♥ Treatment continued 1 year or until AF recurred
♥ Transtelephonic monitoring used
11/2/11
20
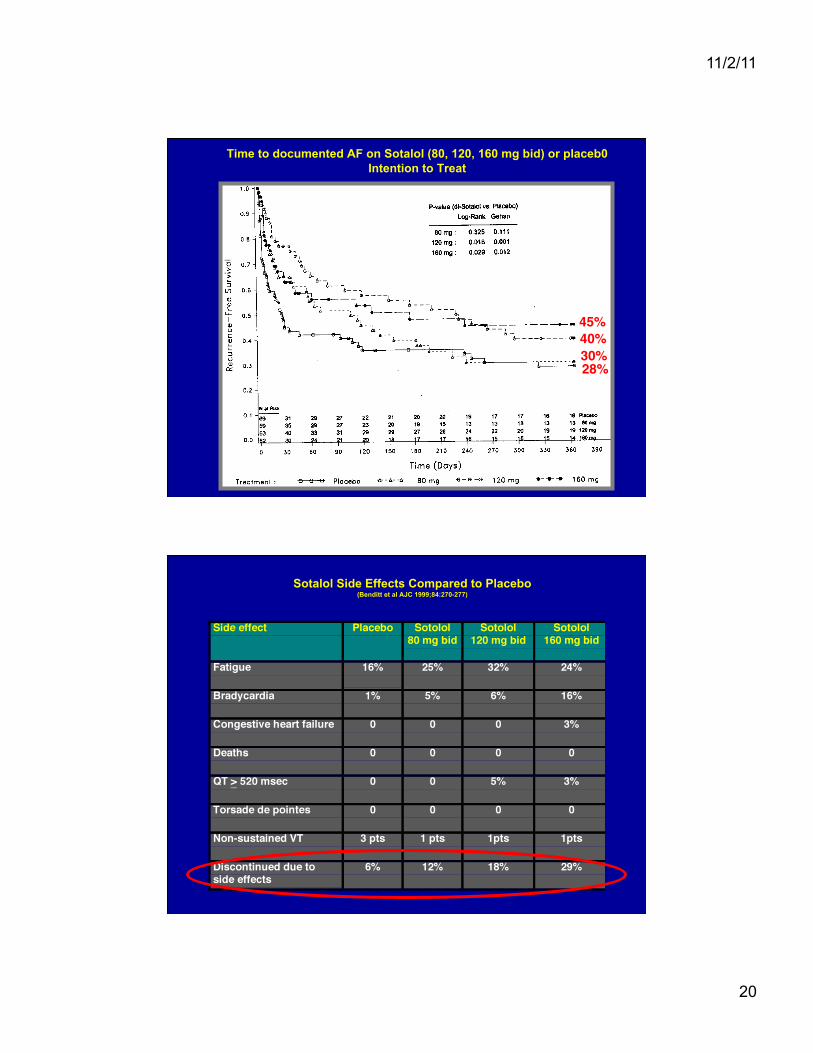
Time to documented AF on Sotalol (80, 120, 160 mg bid) or placeb0 Intention to Treat
30%"40%"45%"
28%"
Sotalol Side Effects Compared to Placebo (Benditt et al AJC 1999;84:270-277)
11/2/11
21
11/2/11
22
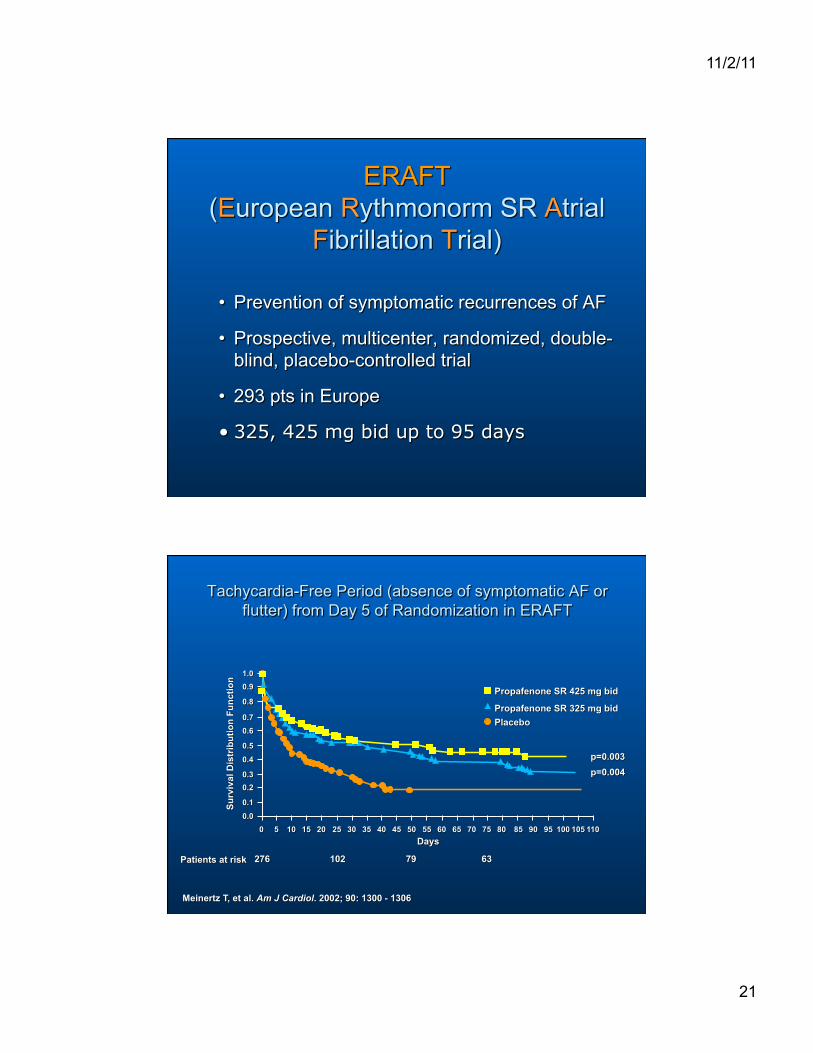
Dronedarone: Amiodarone Without Side Effects or Just a Different Poison?
EURIDIS AND ADONIS (Singh B et al. N Engl J Med 2007;357:987-999)
♥ Age >21 years ♥ One episode of Afib in prior 3 months ♥ In NSR for one hour before randomization ♥ Randomized 2:1 Dronedarone 400mg bid
or placebo ♥ Endpoint: Time to first documented AF
lasting 10 minutes ♥ Secondary endpoints
• Symptoms related to AF • Mean Ventricular Rate during first AF
recurrence
11/2/11
23
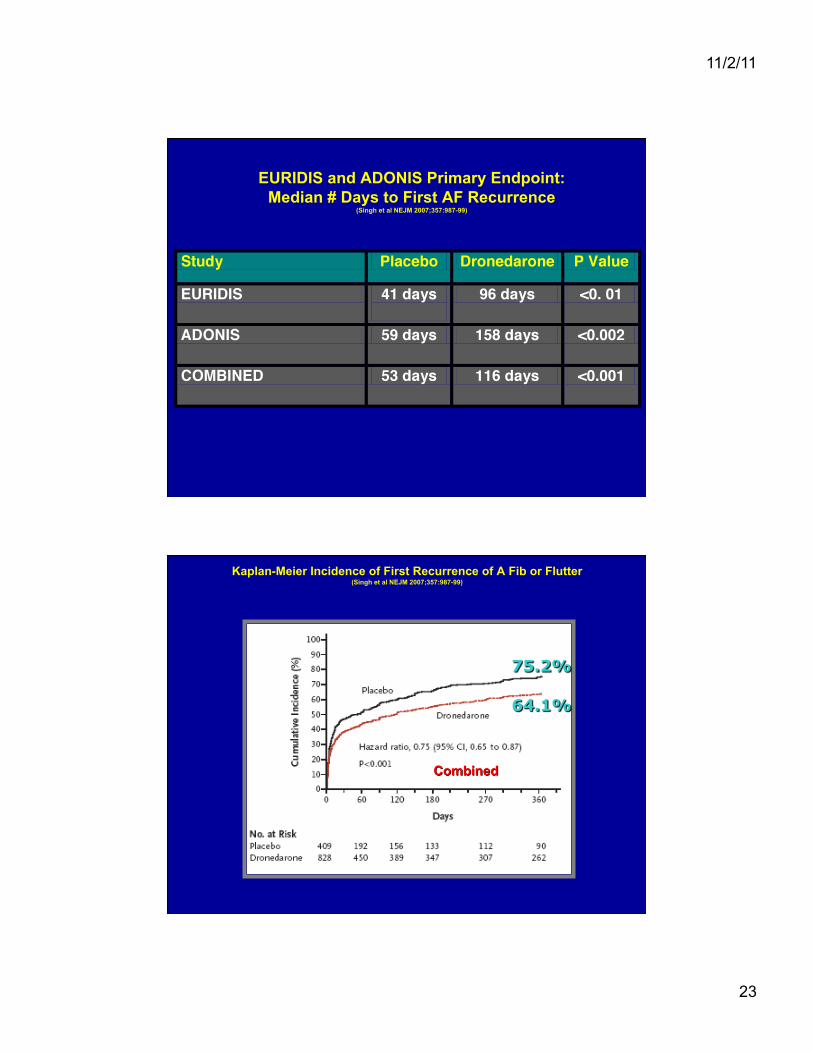
EURIDIS and ADONIS Primary Endpoint: Median # Days to First AF Recurrence
(Singh et al NEJM 2007;357:987-99)
Kaplan-Meier Incidence of First Recurrence of A Fib or Flutter (Singh et al NEJM 2007;357:987-99)
11/2/11
24
“ANDROMEDA” Antiarrhythmic Trial with Dronedarone in
Moderate-to-Severe CHF Evaluating Morbidity Decrease
Stopped by DSMB January,2003 after 627 patients enrolled due to increased mortality in Dronedarone group
PALLUS Trial
♥ Age > 65 years with at least one of the following major risk factors • systemic arterial embolism • myocardial infarction • documented coronary artery disease • prior stroke • symptomatic heart failure
♥ Age > 75 years + hypertension and diabetes mellitus. ♥ Exclusions: NYHA Class IV or unstable Class III CHF ♥ Endpoints
• Major cardiovascular events (stroke, systemic arterial embolism, myocardial infarction or cardiovascular death)
• Cardiovascular hospitalization or death from any cause
♥ 10,800 patients enrolled in 43 countries at 700 sites ♥ Randomized to dronederone 400 mg bid or placebo
11/2/11
25
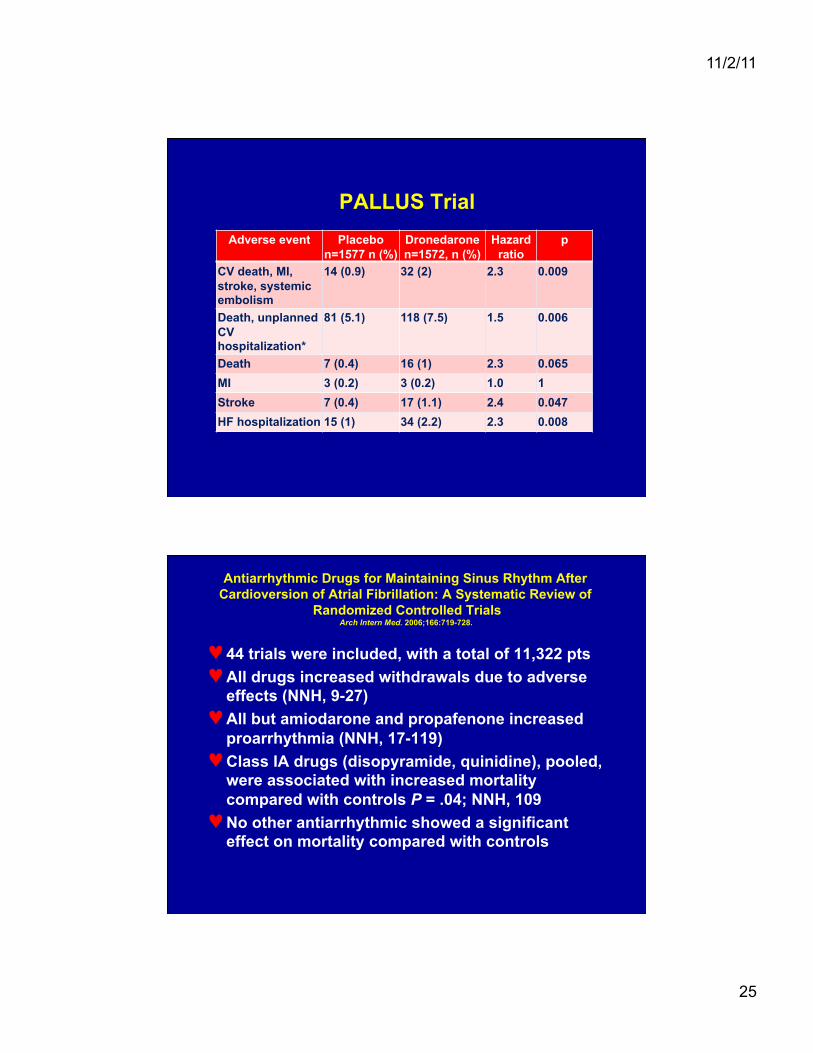
PALLUS Trial Adverse event Placebo
n=1577 n (%) Dronedarone n=1572, n (%)
Hazard ratio
p
CV death, MI, stroke, systemic embolism
14 (0.9) 32 (2) 2.3 0.009
Death, unplanned CV hospitalization*
81 (5.1) 118 (7.5) 1.5 0.006
Death 7 (0.4) 16 (1) 2.3 0.065 MI 3 (0.2) 3 (0.2) 1.0 1 Stroke 7 (0.4) 17 (1.1) 2.4 0.047 HF hospitalization 15 (1) 34 (2.2) 2.3 0.008
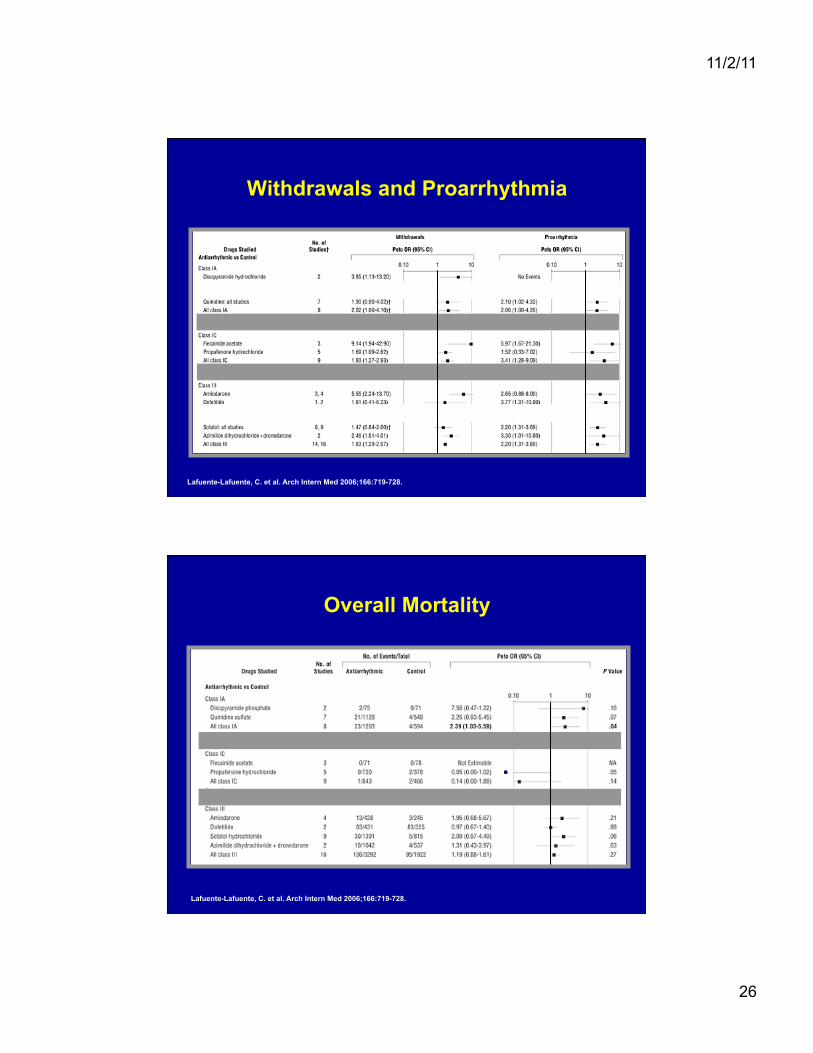
Antiarrhythmic Drugs for Maintaining Sinus Rhythm After Cardioversion of Atrial Fibrillation: A Systematic Review of
Randomized Controlled Trials Arch Intern Med. 2006;166:719-728.
♥ 44 trials were included, with a total of 11,322 pts ♥ All drugs increased withdrawals due to adverse
effects (NNH, 9-27) ♥ All but amiodarone and propafenone increased
proarrhythmia (NNH, 17-119) ♥ Class IA drugs (disopyramide, quinidine), pooled,
were associated with increased mortality compared with controls P = .04; NNH, 109
♥ No other antiarrhythmic showed a significant effect on mortality compared with controls
11/2/11
26
Withdrawals and Proarrhythmia
Lafuente-Lafuente, C. et al. Arch Intern Med 2006;166:719-728.
Overall Mortality
Lafuente-Lafuente, C. et al. Arch Intern Med 2006;166:719-728.
11/2/11
27
Death by Treadmill!
♥ 59 year old recently retired lawyer ♥ No cardiac or non-cardiac diseases ♥ Spring 2007 first Afib while visiting NYC
• Hospitalized 4 days, spontaneous conversion, echo normal and DC on warfarin and metoprolol
♥ California cardiologist changed to ASA ♥ Afib got worse, occurring anytime ♥ Treated with propafenone but had side effects ♥ Flecainide started 100 mg bid, increased to 150 mg
bid, still had Afib ♥ October, 2007 was at movie and felt lightheaded ♥ Went to urgent care where sinus rate in 30s and
metoprolol decrease to 25 mg a day ♥ Referred for a treadmill
11/2/11
28
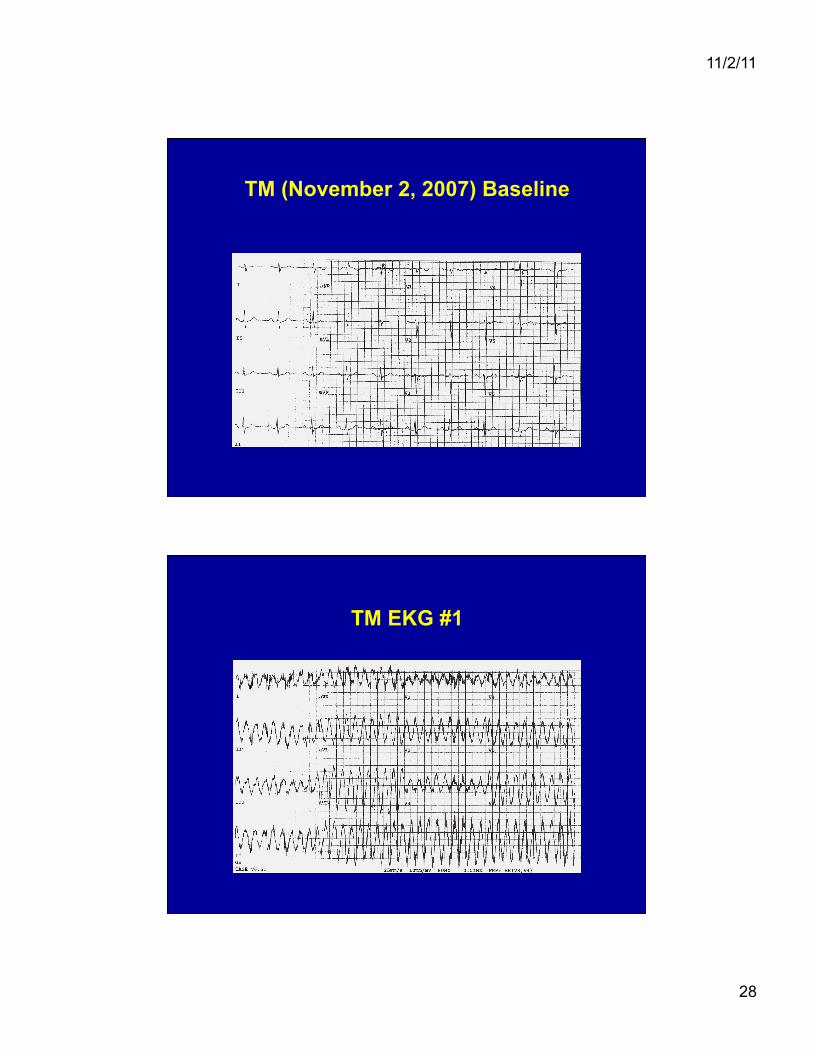
TM (November 2, 2007) Baseline
TM EKG #1
11/2/11
29
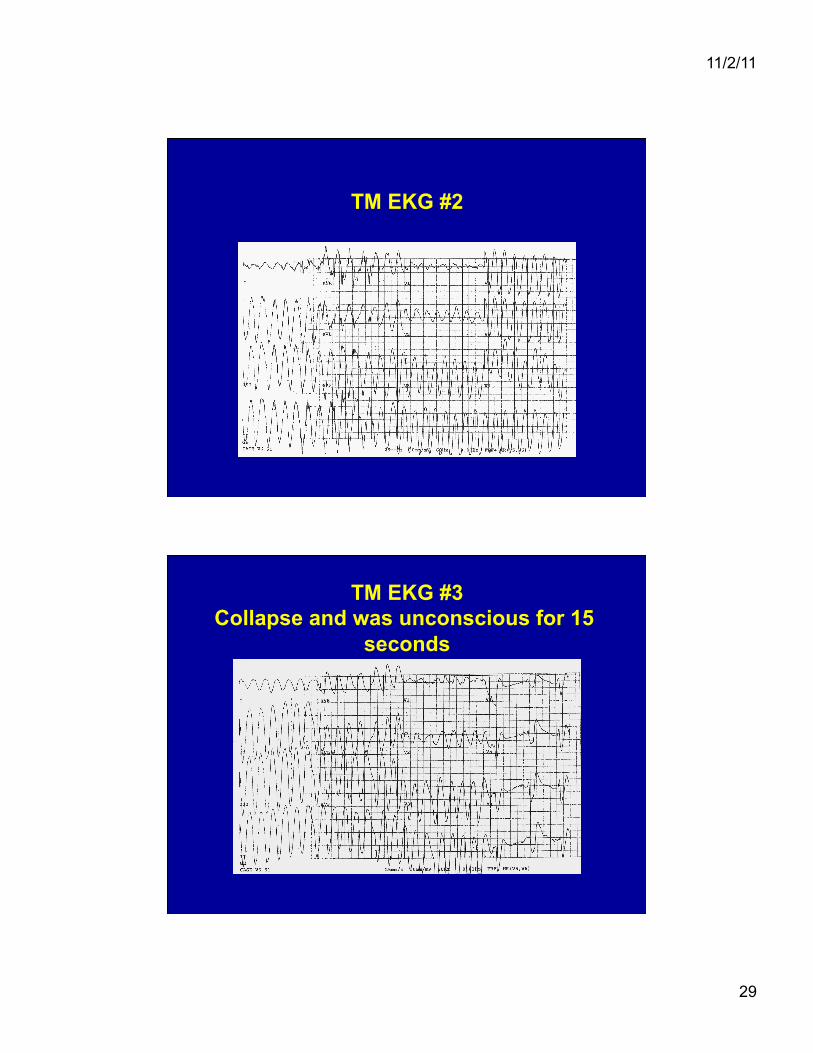
TM EKG #2
TM EKG #3 Collapse and was unconscious for 15
seconds
11/2/11
30
Saw Dr. Winkle on November 15, 2007
♥ Patient declined further antiarrhythmic drugs ♥ Metoprolol 25 mg a day (very fatigued on
higher doses changed to diltiazem with gradual dose escalation to 240 mg AM and 120 mg PM
♥ Still with several episodes of Afib a week lasting for hours at a time during which he could not do much
♥ Underwent successful Afib ablation March 21, 2008. AF free ever since.
Ablation to treat AF: Frequent Negative Comments
♥ It takes all day to do ♥ It does not work ♥ Repeat ablations do not work ♥ There are too many complications ♥ It works, but almost all patients eventually
have a recurrence ♥ Most patients still have to stay on
anticoagulation even if they are not having AF
None of these are true in 2011
11/2/11
31
Sequoia Hospital AF Ablation Results
♥ 1504 AF ablations in 1125 patients as of Dec, 31, 2010
♥ All patients symptomatic and most have failed rate control and rhythm control
♥ Includes both paroxysmal and persistent AF with and without heart disease
270 (30.9%) AF1 (paroxysmal)
423 (52.8%) AF2 (persistent) 150 (16.3%) AF3 (long-standing persistent)
Sequoia Hospital AF Ablation Results
♥ Success = no AF off of all drugs
♥ Partial success = no AF on AAD • Most partial successes and failures offered redo
ablation
♥ Failure = AF on AAD 3 months after final procedure
Both Single Procedure Success rates and final status reported
11/2/11
32
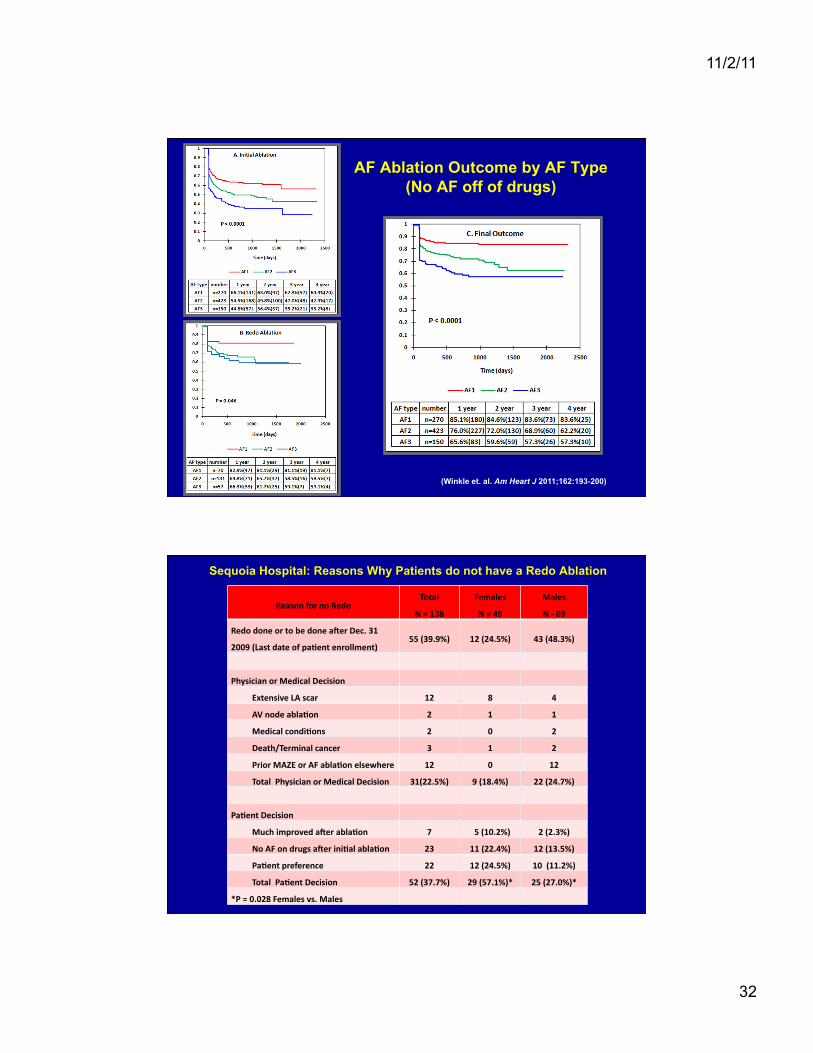
AF Ablation Outcome by AF Type (No AF off of drugs)
(Winkle et. al. Am Heart J 2011;162:193-200)
Sequoia Hospital: Reasons Why Patients do not have a Redo Ablation
Reason for no Redo Total
N = 138
Females
N = 49
Males
N -‐ 89
Redo done or to be done a`er Dec. 31
2009 (Last date of paNent enrollment) 55 (39.9%) 12 (24.5%) 43 (48.3%)
Physician or Medical Decision
Extensive LA scar 12 8 4
AV node ablaNon 2 1 1
Medical condiNons 2 0 2
Death/Terminal cancer 3 1 2
Prior MAZE or AF ablaNon elsewhere 12 0 12
Total Physician or Medical Decision 31(22.5%) 9 (18.4%) 22 (24.7%)
PaNent Decision
Much improved a`er ablaNon 7 5 (10.2%) 2 (2.3%)
No AF on drugs a`er iniNal ablaNon 23 11 (22.4%) 12 (13.5%)
PaNent preference 22 12 (24.5%) 10 (11.2%)
Total PaNent Decision 52 (37.7%) 29 (57.1%)* 25 (27.0%)*
*P = 0.028 Females vs. Males
11/2/11
33
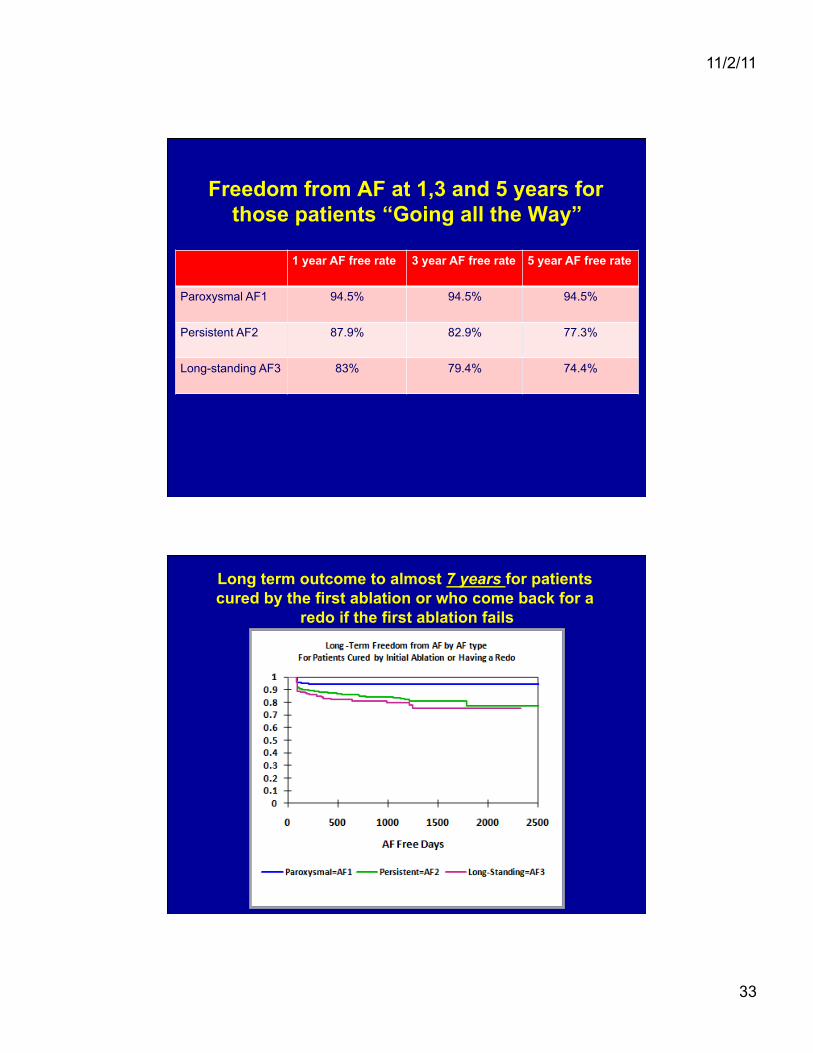
Freedom from AF at 1,3 and 5 years for those patients “Going all the Way”
1 year AF free rate 3 year AF free rate 5 year AF free rate
Paroxysmal AF1 94.5% 94.5% 94.5%
Persistent AF2 87.9% 82.9% 77.3%
Long-standing AF3 83% 79.4% 74.4%
Long term outcome to almost 7 years for patients cured by the first ablation or who come back for a
redo if the first ablation fails
11/2/11
34
How to do a faster and safer AF ablation
♥ Use only one groin ♥ Do only one transseptal puncture (you can put 2
catheters thru the single stick) ♥ Use an RF needle for the transseptal ♥ No Foley catheter ♥ Have dedicated echo machine in EP lab ♥ Use general anesthesia ♥ Use the open irrigated tip catheter at 50W ♥ Mark the location of the esophagus ♥ Keep the ACT at 225 and infuse heparin thru the
transseptal sheath ♥ Reverse heparin and pull sheaths in the EP lab ♥ Avoid “gadgets”: Stereotaxis, Cyroballoons, Robots
Zero Gravity: A cheaper way to reduce operator radiation than $2M magnets!

11/2/11
35
Comparison of Cryoballoon to RF ablation Cryoballoon
Medronic FDA data
(n = 163 patients)
Radiofrequency at
Sequoia Hospital
(n = >1800 ablations)
Superior
outcome Cryo
or RF
Death 0.6% 0.0% RF Superior
Stroke/TIA 4.3% 0.26% RF Superior
Heart Attack 1.2% 0.0% RF Superior
Pulmonary Vein Stenosis 3.1% 0.07% RF Superior
Bleeding Needing
Transfusion 1.8% 0.13% RF Superior
AV fistula/
Pseudoaneurysms 1.8% 0.93% RF Superior
Phrenic Nerve Paralysis 16% 0.0% RF Superior
Procedure Time 6 hours 11 minutes 2 hours RF Superior
Flouroscopy Time 62.8 minutes 60.2 minutes RF Superior
1Year Cure Rate 69.9% 86.2% RF Superior
With OITC Ablate at 50W and Keep the Catheter Moving (Winkle et. al. PACE 2011;34 :531-539)
11/2/11
36
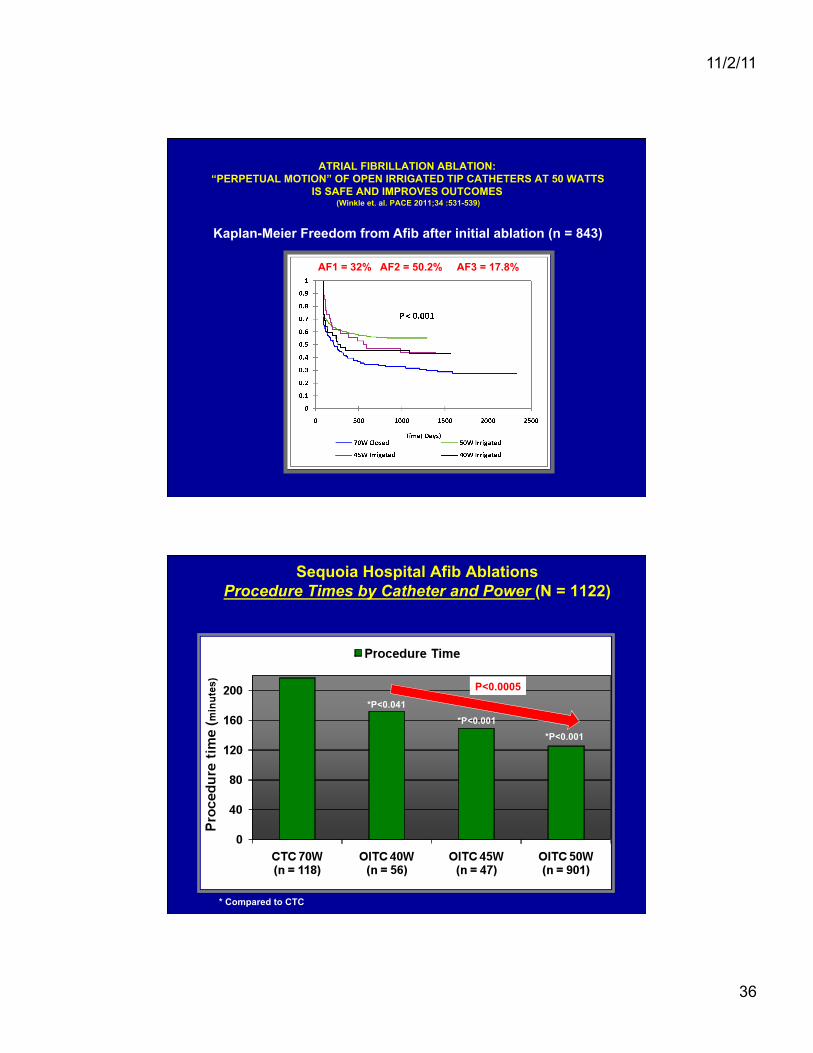
ATRIAL FIBRILLATION ABLATION: “PERPETUAL MOTION” OF OPEN IRRIGATED TIP CATHETERS AT 50 WATTS
IS SAFE AND IMPROVES OUTCOMES (Winkle et. al. PACE 2011;34 :531-539)
Kaplan-Meier Freedom from Afib after initial ablation (n = 843)
AF1 = 32% AF2 = 50.2% AF3 = 17.8%
Sequoia Hospital Afib Ablations Procedure Times by Catheter and Power (N = 1122)
*P<0.041 *P<0.001
*P<0.001
* Compared to CTC
P<0.0005
11/2/11
37
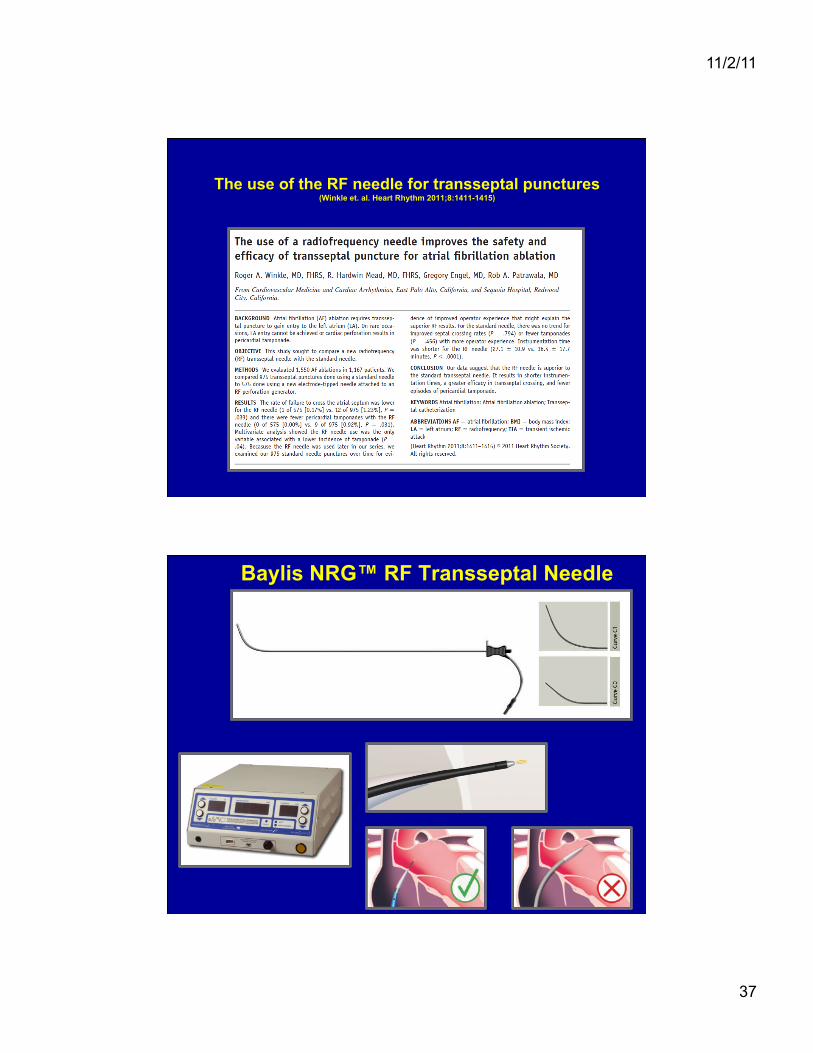
The use of the RF needle for transseptal punctures (Winkle et. al. Heart Rhythm 2011;8:1411-1415)
Baylis NRG™ RF Transseptal Needle
11/2/11
38
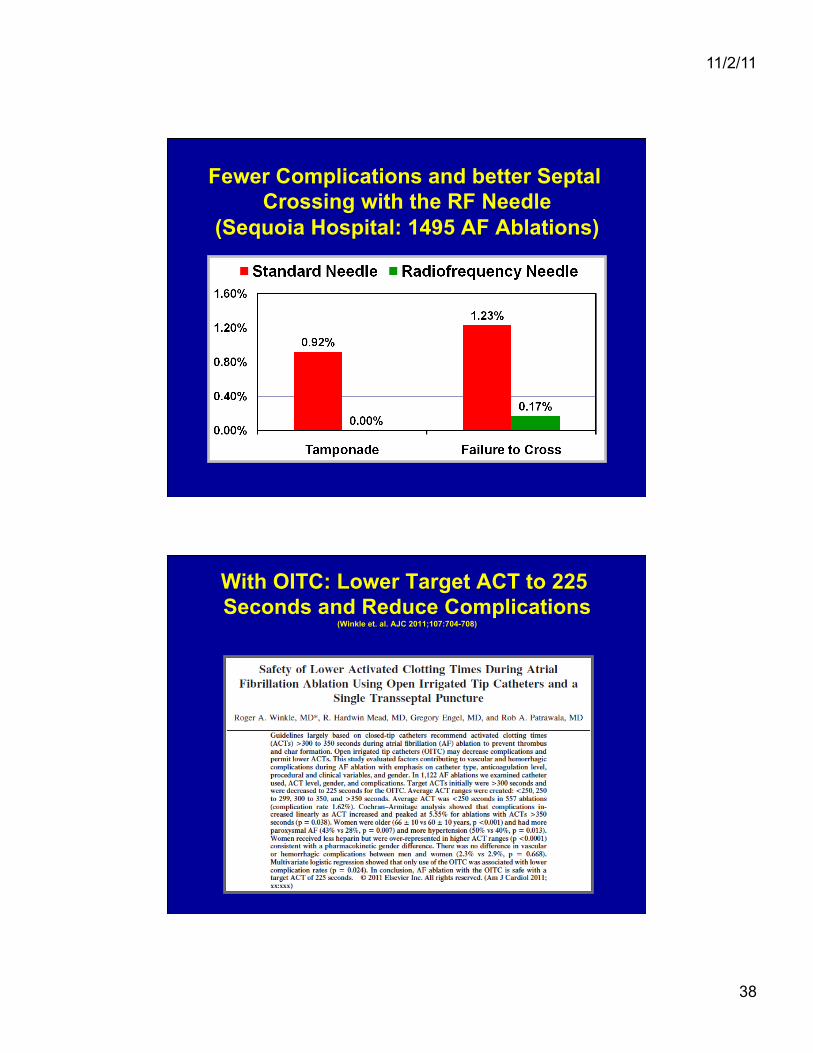
Fewer Complications and better Septal Crossing with the RF Needle
(Sequoia Hospital: 1495 AF Ablations)
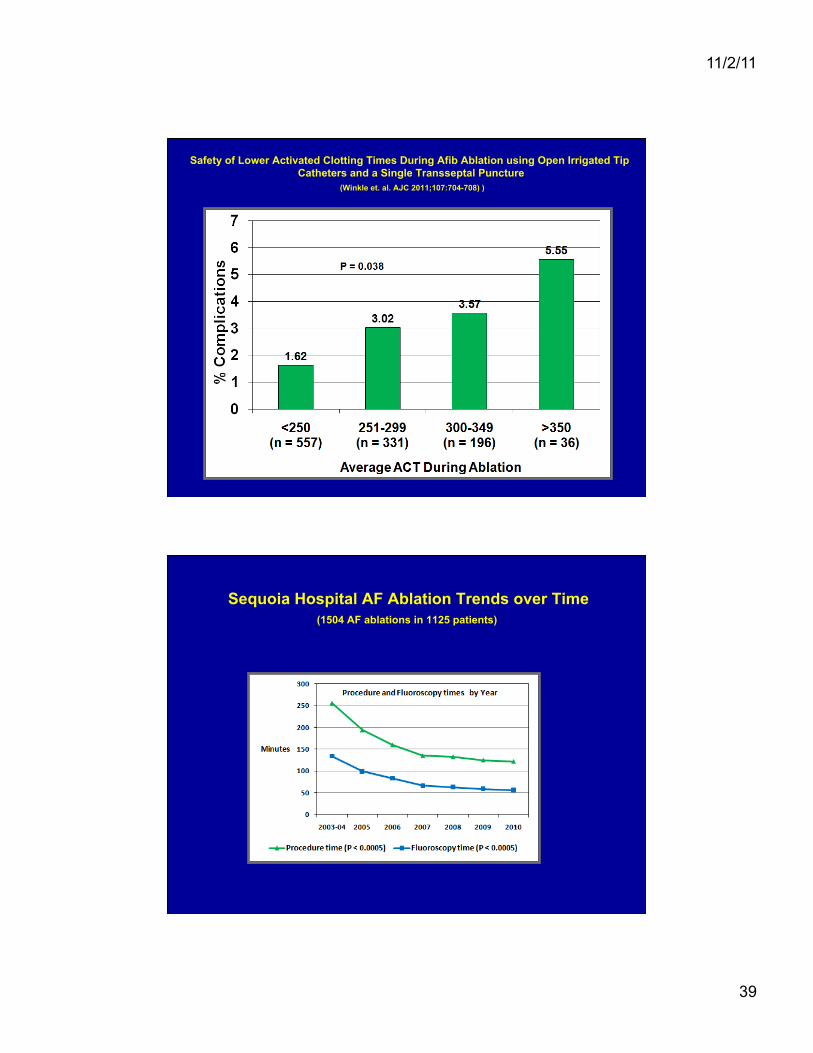
With OITC: Lower Target ACT to 225 Seconds and Reduce Complications
(Winkle et. al. AJC 2011;107:704-708)
11/2/11
39
Safety of Lower Activated Clotting Times During Afib Ablation using Open Irrigated Tip Catheters and a Single Transseptal Puncture
(Winkle et. al. AJC 2011;107:704-708) )
Sequoia Hospital AF Ablation Trends over Time (1504 AF ablations in 1125 patients)
11/2/11
40
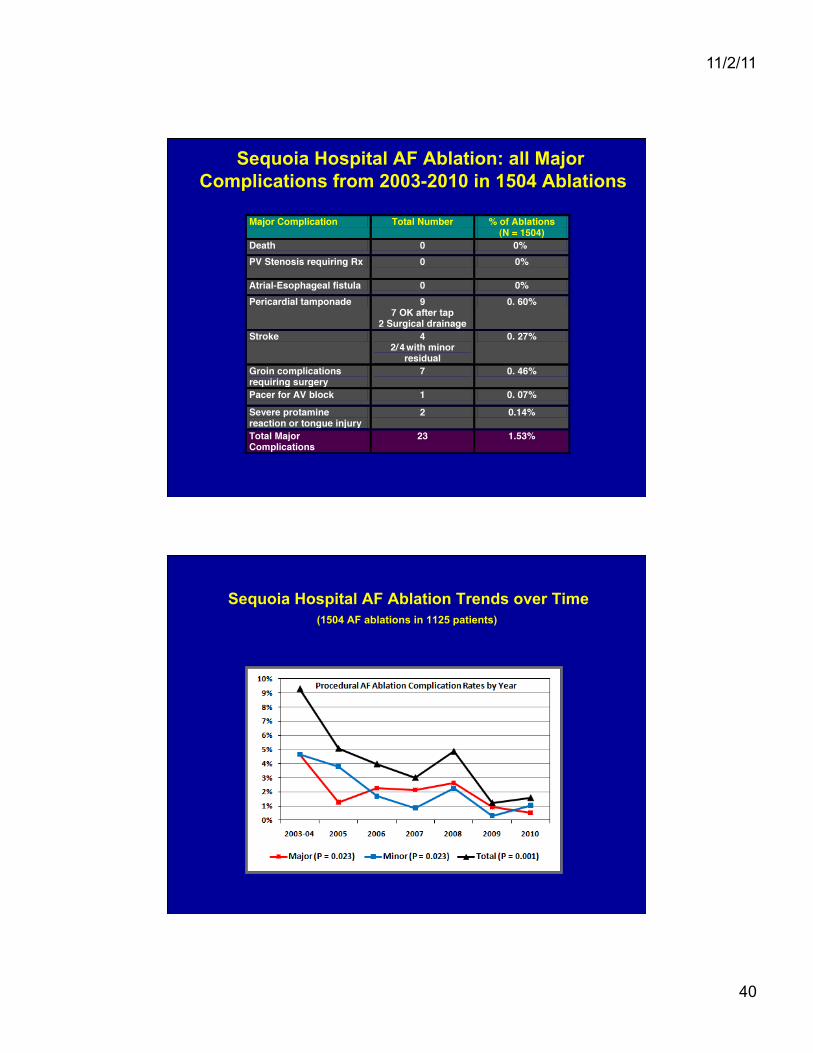
Sequoia Hospital AF Ablation: all Major Complications from 2003-2010 in 1504 Ablations
Sequoia Hospital AF Ablation Trends over Time (1504 AF ablations in 1125 patients)
11/2/11
41
Why Patients Should Skip AADs and Go Directly to Ablation
♥ The risk of permanent side effect from ablation is about 1:400 which is the risk of stroke every 2-3 months for the lowest risk AF groups
♥ Every drug a patient fails lowers their chance of a successful ablation
♥ Every randomized trial of Ablation vs. AAD strongly favors Ablation
Sequoia Hospital AF Ablation: Impact of number of AADs failed pre-ablation
(Europace in press)
♥ 942 patients with paroxysmal AF (n = 348) and persistent AF (n = 594) • We examined the impact of number of AADs
failed on clinical characteristics and ablation outcomes
11/2/11
42
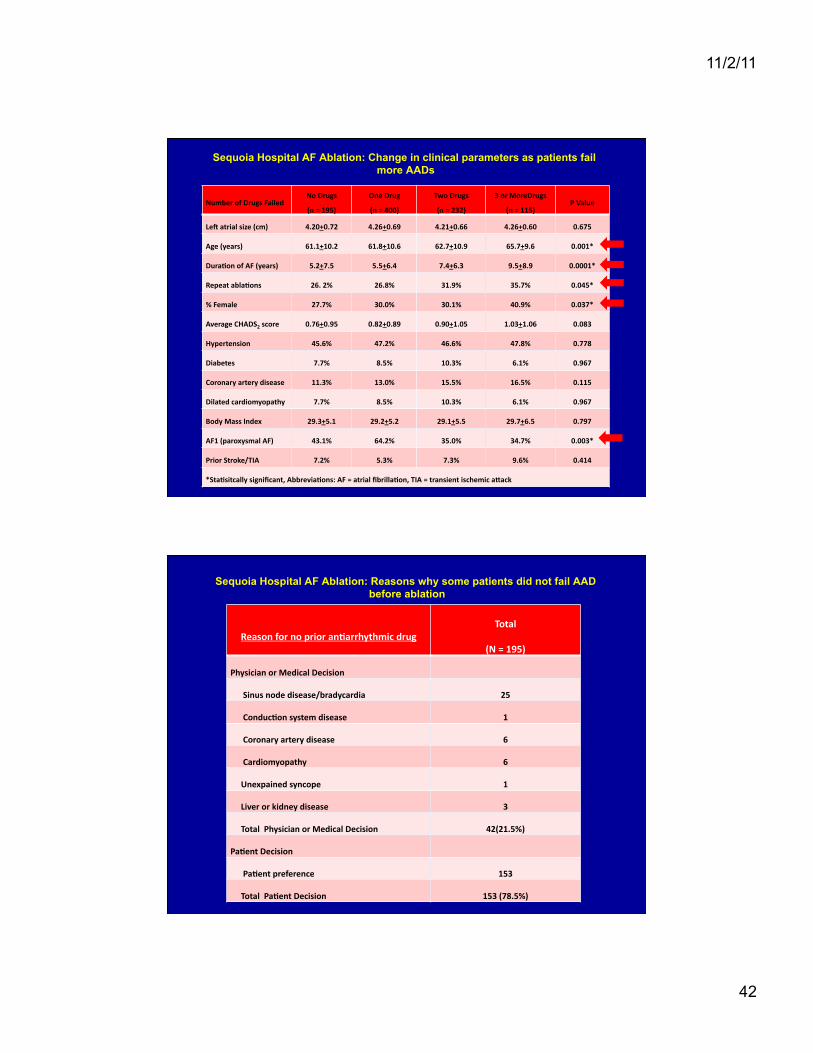
Sequoia Hospital AF Ablation: Change in clinical parameters as patients fail more AADs
Number of Drugs Failed No Drugs
(n = 195)
One Drug
(n = 400)
Two Drugs
(n = 232)
3 or MoreDrugs
(n = 115) P Value
Le` atrial size (cm) 4.20+0.72 4.26+0.69 4.21+0.66 4.26+0.60 0.675
Age (years) 61.1+10.2 61.8+10.6 62.7+10.9 65.7+9.6 0.001*
DuraNon of AF (years) 5.2+7.5 5.5+6.4 7.4+6.3 9.5+8.9 0.0001*
Repeat ablaNons 26. 2% 26.8% 31.9% 35.7% 0.045*
% Female 27.7% 30.0% 30.1% 40.9% 0.037*
Average CHADS2 score 0.76+0.95 0.82+0.89 0.90+1.05 1.03+1.06 0.083
Hypertension 45.6% 47.2% 46.6% 47.8% 0.778
Diabetes 7.7% 8.5% 10.3% 6.1% 0.967
Coronary artery disease 11.3% 13.0% 15.5% 16.5% 0.115
Dilated cardiomyopathy 7.7% 8.5% 10.3% 6.1% 0.967
Body Mass Index 29.3+5.1 29.2+5.2 29.1+5.5 29.7+6.5 0.797
AF1 (paroxysmal AF) 43.1% 64.2% 35.0% 34.7% 0.003*
Prior Stroke/TIA 7.2% 5.3% 7.3% 9.6% 0.414
*StaNsitcally significant, AbbreviaNons: AF = atrial fibrillaNon, TIA = transient ischemic agack
Sequoia Hospital AF Ablation: Reasons why some patients did not fail AAD before ablation
Reason for no prior anNarrhythmic drug Total
(N = 195)
Physician or Medical Decision
Sinus node disease/bradycardia 25
ConducNon system disease 1
Coronary artery disease 6
Cardiomyopathy 6
Unexpained syncope 1
Liver or kidney disease 3
Total Physician or Medical Decision 42(21.5%)
PaNent Decision
PaNent preference 153
Total PaNent Decision 153 (78.5%)
11/2/11
43
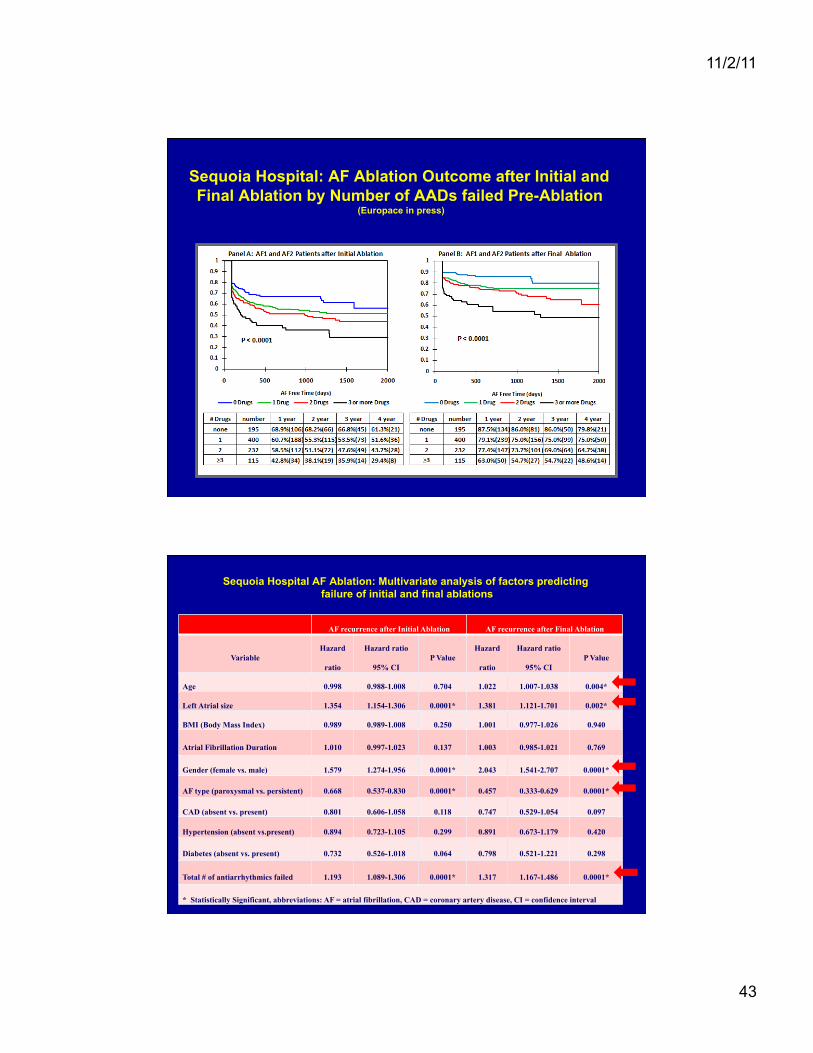
Sequoia Hospital: AF Ablation Outcome after Initial and Final Ablation by Number of AADs failed Pre-Ablation
(Europace in press)
Sequoia Hospital AF Ablation: Multivariate analysis of factors predicting failure of initial and final ablations
AF recurrence after Initial Ablation AF recurrence after Final Ablation
Variable Hazard
ratio
Hazard ratio
95% CI P Value
Hazard
ratio
Hazard ratio
95% CI P Value
Age 0.998 0.988-1.008 0.704 1.022 1.007-1.038 0.004*
Left Atrial size 1.354 1.154-1.306 0.0001* 1.381 1.121-1.701 0.002*
BMI (Body Mass Index) 0.989 0.989-1.008 0.250 1.001 0.977-1.026 0.940
Atrial Fibrillation Duration 1.010 0.997-1.023 0.137 1.003 0.985-1.021 0.769
Gender (female vs. male) 1.579 1.274-1.956 0.0001* 2.043 1.541-2.707 0.0001*
AF type (paroxysmal vs. persistent) 0.668 0.537-0.830 0.0001* 0.457 0.333-0.629 0.0001*
CAD (absent vs. present) 0.801 0.606-1.058 0.118 0.747 0.529-1.054 0.097
Hypertension (absent vs.present) 0.894 0.723-1.105 0.299 0.891 0.673-1.179 0.420
Diabetes (absent vs. present) 0.732 0.526-1.018 0.064 0.798 0.521-1.221 0.298
Total # of antiarrhythmics failed 1.193 1.089-1.306 0.0001* 1.317 1.167-1.486 0.0001*
* Statistically Significant, abbreviations: AF = atrial fibrillation, CAD = coronary artery disease, CI = confidence interval
11/2/11
44
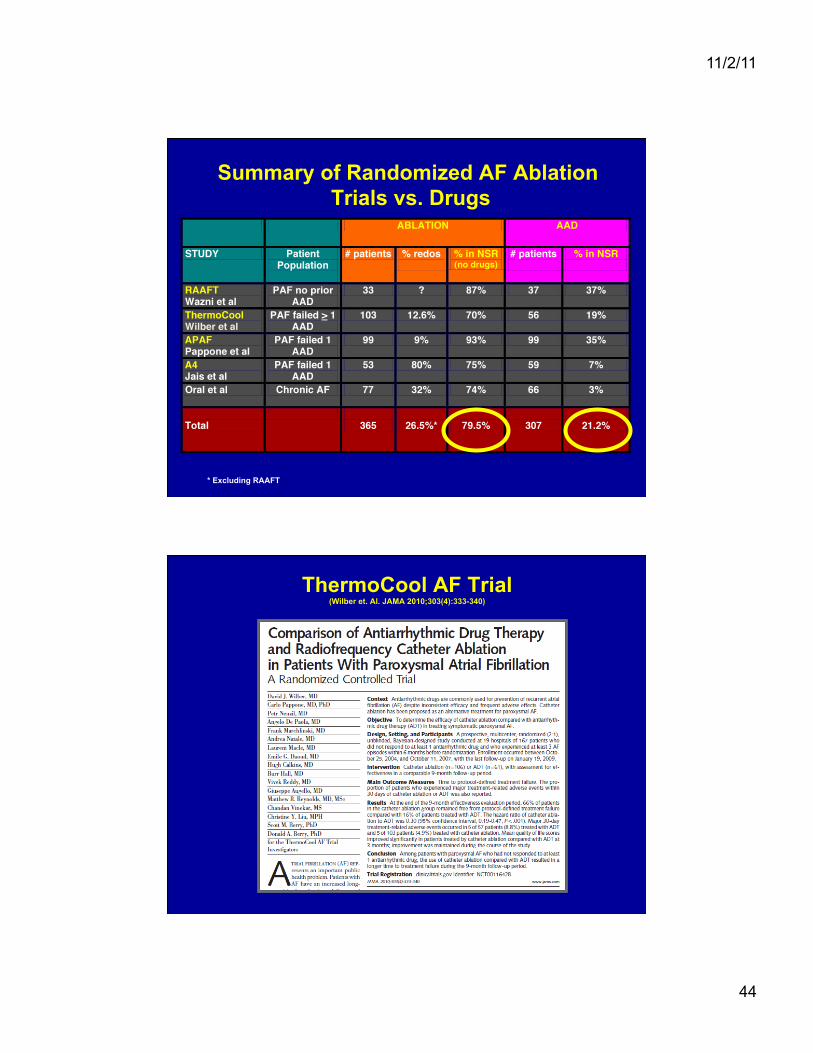
Summary of Randomized AF Ablation Trials vs. Drugs
* Excluding RAAFT
ThermoCool AF Trial (Wilber et. Al. JAMA 2010;303(4):333-340)

11/2/11
45
ThermoCool AF Trial (Wilber et. Al. JAMA 2010;303(4):333-340)
Kaplan-Meier Curves of Time to Protocol-Defined Treatment Failure, Recurrence of Symptomatic Atrial Arrhythmia, and Recurrence of Any Atrial Arrhythmia by Treatment
Group
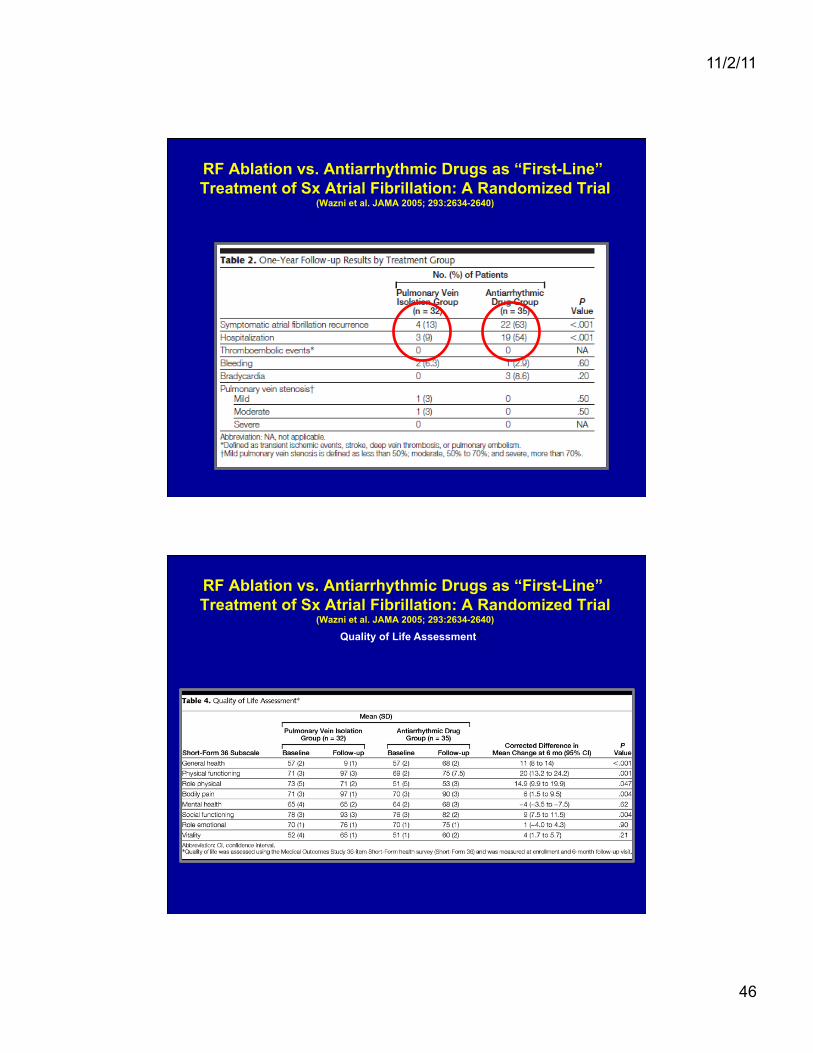
RF Ablation vs. Antiarrhythmic Drugs as “First-Line” Treatment of Sx Atrial Fibrillation: A Randomized Trial
(Wazni et al. JAMA 2005; 293:2634-2640)
11/2/11
46
RF Ablation vs. Antiarrhythmic Drugs as “First-Line” Treatment of Sx Atrial Fibrillation: A Randomized Trial
(Wazni et al. JAMA 2005; 293:2634-2640)
RF Ablation vs. Antiarrhythmic Drugs as “First-Line” Treatment of Sx Atrial Fibrillation: A Randomized Trial
(Wazni et al. JAMA 2005; 293:2634-2640)
Quality of Life Assessment*.
11/2/11
47
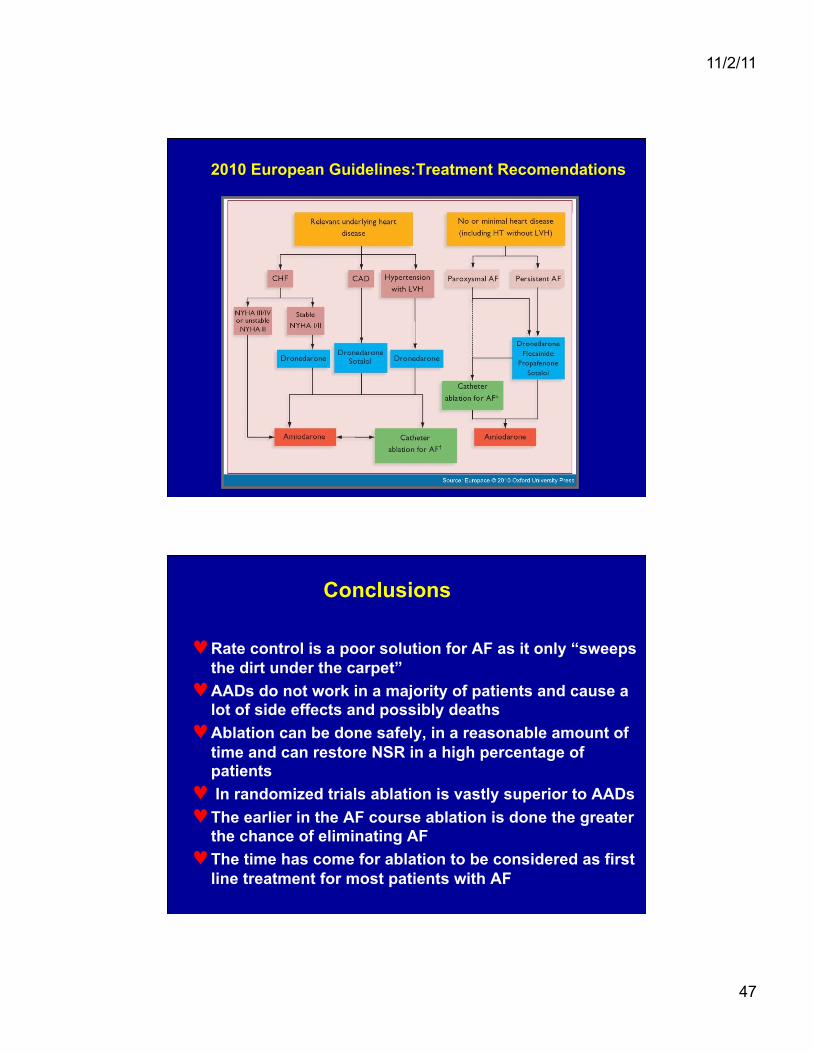
2010 European Guidelines:Treatment Recomendations
Conclusions
♥ Rate control is a poor solution for AF as it only “sweeps the dirt under the carpet”
♥ AADs do not work in a majority of patients and cause a lot of side effects and possibly deaths
♥ Ablation can be done safely, in a reasonable amount of time and can restore NSR in a high percentage of patients
♥ In randomized trials ablation is vastly superior to AADs ♥ The earlier in the AF course ablation is done the greater
the chance of eliminating AF ♥ The time has come for ablation to be considered as first
line treatment for most patients with AF

11/2/11
48
Dr. Moss Thank you for all you have done over
so many years to help our patients live longer and better quality lives!



![wildcard72.files.wordpress.com · Web view[ ] [ ] [🙏] [♫] [🌿] [*] [ : ] [♥♥♥] ] [ [:))] [🙏] [♫] [🌿] [*] [ : ] [♥♥♥] ] [ [:))] [🙏] [♫] [🌿] [*]](https://img.pdfslide.net/doc/110x75/602ccf4eada9400256693c63/web-view-a-oe-aaa-a.jpg)

























