Embed Size (px)
Citation preview

Research Article
Prospective evaluation of the prognostic scores for cirrhoticpatients admitted to an Intensive Care Unit
Eric Levesque1, Emir Hoti1, Daniel Azoulay1,2,3, Philippe Ichaï1,2,4, Houssam Habouchi1,Denis Castaing1,2,4, Didier Samuel1,2,4, Faouzi Saliba1,2,4,⇑
1AP-HP Hôpital Paul Brousse, Centre Hépato-Biliaire, Villejuif, France; 2Univ Paris-Sud, UMR-S 785, Villejuif, France;3Inserm, Unité 1004, 94800 Villejuif, France; 4Inserm, Unité 785, 94800 Villejuif, France
Background & Aims: Cirrhotic patients admitted to an Intensive Conclusions: For cirrhotic patients admitted to the ICU, SAPS II,
Care Unit (ICU) have a poor prognosis. Identifying patients inwhom ICU care will be useful can be challenging. The aim of thisstudy was to assess the predictive value of prognostic scores withrespect to mortality and to identify mortality risk factors.Methods: Three hundred and seventy-seven cirrhotic patientsadmitted to a Liver ICU between May 2005 and March 2009 wereenrolled in this study. Their average age was 55.5 ± 11.4 years.The etiology of cirrhosis was alcohol (68%), virus hepatitis(18%), or mixed (5.5%). The main causes of hospitalization weregastrointestinal hemorrhage (43%), sepsis (19%), and hepaticencephalopathy (12%).Results: ICU and in-hospital mortality rates were 34.7% and43.0%, respectively. Infection was the major cause of death(81.6%). ROC curve analysis demonstrated that SOFA (0.92) andSAPS II (0.89) scores calculated within 24 h of admission pre-dicted ICU mortality better than the Child–Pugh score (0.79) orMELD scores with (0.79–0.82) or without the incorporation ofserum sodium levels (0.82). Statistical analysis showed that theprognostic severity scores, organ replacement therapy, and infec-tion were accurate predictors of mortality. On multivariate anal-ysis, mechanical ventilation, vasopressor therapy, bilirubin levelat admission, and infection were independently associated withICU mortality.Journal of Hepatology 20
Keywords: Cirrhosis; Prognostic scores; Intensive Care Unit; Outcome; Mortality;Model for End-Stage Liver Disease.Received 1 February 2011; received in revised form 24 May 2011; accepted 17 June2011; available online 9 August 2011⇑ Corresponding author. Address: Réanimation, Centre Hépato-Biliaire, HôpitalPaul Brousse, 12 avenue Paul-Vaillant-Couturier, 94804 Villejuif, France. Tel.: +331 45 59 64 12; fax: +33 1 45 59 38 57.E-mail address: [email protected] (F. Saliba).Abbreviations: ICU, Intensive Care Unit; SOFA, Sequential Organ Failure Assess-ment; APACHE, Acute Physiology and Chronic Health Evaluation; MELD, Modelfor End-Stage Liver Disease; TIPS, Transjugular Intrahepatic Portosystemic Shunt;UNOS, United Network for Organ Sharing; MELD-Na, Model for End-Stage LiverDisease with incorporation of serum sodium; iMELD, Integrated Model for End-Stage Liver Disease; MESO, Model for End-Stage Liver Disease to Sodium index;SAPS II, Simplified Acute Physiology Score; ROC, Receiver Operating Character-istic; MARS, Molecular Adsorbent Recirculating System; RRT, Renal ReplacementTherapy; AUROC, Area Under Receiver Operating Characteristic; SIRS, SystemicInflammatory Response Syndrome; CFU, Colony Forming Units; CPIS, ClinicalPulmonary Infection Score.
and SOFA scores predicted ICU mortality better than liver-specificscores. Mechanical ventilation or vasopressor therapy, bilirubinlevels at admission and infection in patients with advanced cir-rhosis were associated with a poor outcome.� 2011 European Association for the Study of the Liver. Publishedby Elsevier B.V. All rights reserved.
Introduction
Cirrhotic patients admitted to an Intensive Care Unit (ICU) have apoor prognosis, with mortality rates ranging from 36% to 86%[1–4]. In addition, management of these patients requires that asignificant percentage of the total ICU care budget is devoted toa subgroup of cirrhotic patients who will eventually not survive[5,6].
To identify patients in whom aggressive treatment may offerrecovery, or those who may benefit from a transfer to an ICU orfrom liver transplantation, has always been a challenge forintensivists and hepatologists. To this end, several prognosticscores [7,8] have been proposed, including the Child–Pugh, whichuntil now has been the most widely utilized liver-specific score[9,10]. However, the discriminatory power of this score relativeto mortality in cirrhotic patients admitted to the ICU is inferiorto that of general ICU scores (SOFA or APACHE) [11]. This mightbe due, at least in part, to the fact that the Child–Pugh score doesnot include any markers of renal function.
Recently, the Model for End-Stage Liver Disease (MELD) score,initially developed for cirrhotic patients treated with Transjugu-lar Intrahepatic Portosystemic Shunt (TIPS) [12], has been appliedwidely to predict mortality across a broad spectrum of liver dis-eases. Thus, the MELD score was implemented in 2002 by theUnited Network for Organ Sharing (UNOS) as a tool to estimatethe severity of liver disease, the mortality of patients on waitinglists for liver transplantation and subsequently for the allocationof liver grafts. The MELD score has been associated with 3-monthmortality in patients on the waiting list. Despite its potential ben-efits, relatively few studies have analyzed the predictive value ofthe MELD score in cirrhotic patients admitted to an IntensiveCare Unit [13–15]. Moreover, hyponatremia, as a surrogate ofportal hypertension, has now been recognized as an important
12 vol. 56 j 95–102

Research Article
prognostic factor in patients with liver cirrhosis [16]. SeveralMELD models incorporating serum sodium (Na+) levels (theMELD-Na [16], iMELD [17], and MESO [18]) have been shownto improve prognostic accuracy in cirrhotic patients awaitingliver transplantation [19,20]. However, only one study has evalu-ated these modified versions (MELD combined with serumsodium) in cirrhotic patients admitted to an ICU and observed asimilar discrimination ability of MELD-Na and MELD to predictin-hospital mortality [15].To evaluate the performance of these scores as predictivetools of mortality in patients with cirrhosis in an ICU, we com-pared the Child–Pugh classification, liver-specific prognosticmodels (MELD and MELD combined with serum sodium) andtwo ICU prognostic scores [the Simplified Acute Physiology Score(SAPS II) [21] and Sequential Organ Failure Assessment (SOFA)][22]. In addition, we looked for specific factors that might predictmortality in patients with cirrhosis admitted to an ICU.
Patients and methods
Patients
This prospective cohort study was performed in the Liver Intensive Care Unit (15beds) at Paul Brousse University Hospital. This is a tertiary referral unit that hasbeen highly specialized in liver diseases since 1970. The unit is run by hepatolo-gists, intensivists, and liver surgeons. Between May 2005 and March 2009, 377consecutive cirrhotic patients requiring intensive monitoring and/or treatmentthat could not be provided outside an ICU were enrolled. All patients wereP18 years of age and had histologically-proven or clinically diagnosed cirrhosis(e.g. portal hypertension with ascites, esophageal varices, or encephalopathy). Cir-rhotic patients admitted to the Liver ICU before or following any type of surgerywere excluded from this study.
Data
The following clinical and demographic data were collected: age, gender, etiologyof cirrhosis, and primary diagnosis at ICU admission including variceal bleeding,encephalopathy, sepsis, and hepatorenal syndrome. The SAPS II [21] and initialSequential Organ Failure Assessment (SOFA) [22] were determined within 24 hof admission to determine the severity of the acute illness. These scores have beenvalidated to predict survival in general ICU populations. The SAPS II system is basedon age, chronic health status, admission status, and an acute physiological scoreincluding systolic blood pressure, heart rate, body temperature, Glasgow comascore, urine output, serum sodium, serum potassium, serum urea, serum bicarbon-ate, serum bilirubin, white blood cell count, and arterial oxygen tension or alveo-lar–arterial oxygen tension gradient. The SOFA comprises scores for six organsystems (respiratory, cardiovascular, hepatic, renal, coagulation, and neurological)graded from 0 to 4 according to normal function or the degree of dysfunction.
The severity of liver disease at ICU admission was graded using the Child–Pugh classification [20]. All other prognostic models (MELD, MELD-Na, iMELD,and MESO index) were calculated based on the laboratory results obtained onthe day of admission.
The following equations were used to calculate the severity scores:
– MELD: 9.6 � log[creatinine (mg/dl)] + 3.8 � log[bilirubin (mg/dl)] + 11.2 �log(INR) + 6.43 [23]The MELD score ranges from 6 to 40, with higher values indicating moresevere disease.
– MELD-Na: MELD + 1.59 � (135 � Na) (with Na between 135 and120 mmol/L) [16].
– iMELD: MELD + (0.3 � age) � (0.7 + Na) + 100 [17].– MESO index: [MELD/Na (mmol/L)] � 10 [18].
During our study, organ failure was defined as a SOFA score of 3 or 4 for theorgan concerned [22] (Cardiovascular: need for epinephrine or norepinephrine ordopamine >5 lg/kg/min; Respiratory: PaO2/FiO2 <200 mmHg with respiratory
96 Journal of Hepatology 20
support; Renal: creatinine >300 lmol/L or urine output <500 ml/day; Hematol-ogy: platelet count <50 � 103/mm3; Hepatic: bilirubin >102 mmol/L; Central Ner-vous system: Glasgow coma score <9).
At admission and during follow-up in the ICU, systematic screening for infec-tion included chest X-rays, biological parameters (leukocytes, C-reactive protein),clinical features (temperature, signs of shock), and cultures of blood, sputum,urine, and ascites. Infection at admission was defined as an infection occurringwithin the first 48 h following admission to the ICU. A diagnosis of infectionwas based on the following criteria: (1) spontaneous bacterial peritonitis wasdefined when the ascitic fluid neutrophil count was >250/mm3, (2) positive urineculture for urinary tract infection, (3) positive blood cultures (two blood culturesfor Staphylococcus epidermidis) for bacteremia, (4) a suspicion of pneumonia wasbased on combined criteria including elevated leukocytes (>12,000/mm3), ele-vated C-reactive protein (>50 mg/L), fever or hypothermia (<36.5 �C or>38.5 �C), tracheal secretions, a need for oxygen supply or mechanical ventilation,lung infiltrates or opacities on a chest X-ray. For all prospectively identified epi-sode of pneumonia, modified Clinical Pulmonary Infection Score (mCPIS) was cal-culated retrospectively [24,25]. Pneumonia was confirmed by a positive microbialdiagnosis (with a threshold of 104 Colony Forming Units/ml (CFU/ml) for bron-choalveolar lavage cultures or 106 CFU/ml in the case of tracheal aspiration[26]) when available or a mCPIS P5.
Statistical analysis
Data are expressed as mean ± SD. The Mann–Whitney U-test was used to comparecontinuous variables and Chi-square for categorical variables. Univariate andmultivariate Cox regression hazard analysis models were used to determine inde-pendent, significant, predictive factors of ICU mortality. Survival rates were calcu-lated using the Kaplan–Meier method on day 60 after ICU admission and groupswere compared with the log-rank test. None of the patient was lost. Median fol-low-up was 8 months (2–36 months). Statistical analyses were performed usingStatview 5.0 for Macintosh (SAS Institute Inc., Cary, NC, USA).
A ROC curve analysis software (MedCalc version 10.2.0.0, for windows) wasused to determine the Receiver Operating Characteristic (ROC) curve. To identifywhich score had the best discrimination capacity to predict ICU mortality, AreasUnder Receiver Operating Characteristics curve (AUROC) were compared [27].Sensitivity, specificity, and positive and negative predictive values were deter-mined for MELD, SOFA, and SAPS II. Cut-off values were identified using the high-est Youden index (sensitivity + specificity �1) [28]. A p value of less than 0.05 wasconsidered to be statistically significant.
Results
Patients
Between May 2005 and March 2009, 377 consecutive cirrhoticpatients admitted to our ICU were enrolled in this study. Thecharacteristics of these patients are shown in Table 1. The medianage was 55.5 ± 11.4 years; 73% were men and the liver diseaseconcerned was most frequently alcohol-related (68%). The mostcommon primary diagnoses at ICU admission were: acute vari-ceal bleeding (43%), severe infection (19%), or hepatic encepha-lopathy (13%). Among the patients with alcoholic cirrhosis, 39patients (14%) had a histologically proven severe acute alcoholichepatitis. Follow-up to 60 days or time of death was completedfor the whole cohort. In this series, none of the patient was lost.Five patients were transferred to another hospital (ICU dis-charge). Three died within 60 days and considering living inICU and died in hospital.
The cumulative incidence of mortality was 34.7% (131 out of377 patients) in the Liver ICU and 43% (162 out of 377 patients)in the hospital. The results of the univariate analysis performedon all 377 cirrhotic patients admitted, in order to the ICU todetermine predictive factors of ICU mortality, are presented inTable 2. There were no significant differences in age and genderbetween the survivor and non-survivor groups. The primary diag-nosis at admission to the ICU differed significantly between the
12 vol. 56 j 95–102

Table 1. Clinical characteristics of 377 cirrhosis patients admitted to an ICU.Data are expressed as mean ± S.D.
Variable Patients(n = 377)
Age (years, mean ± SD) 55.5 ± 11.4Gender (M/F) 277/100Length of ICU stay (days, mean ± SD) 9.7 ± 11.3Length of hospital stay (days, mean ± SD) 23.0 ± 26.4Cause of cirrhosis
Alcoholic 258 (68%)Hepatitis B 15 (4%)Hepatitis C 52 (14%)Alcoholic + Hepatitis 21 (6%)Others 31 (8%)
Primary ICU admissionAcute variceal bleeding 162 (43%)Severe infection 72 (19%)Hepatic encephalopathy 47 (13%)Hepatorenal syndrome type I 19 (5%)Other 77 (20%)
Prognostic scores at ICU admission (mean ± SD)
SAPS II 45.6 ± 21.2SOFA 9.4 ± 4.9Child Pugh 10.5 ± 2.3Child Pugh category (A/B/C) 25/89/263MELD 24.9 ± 10.8MELD Na 29.7 ± 13.8MESO 1.9 ± 0.8iMELD 48.1 ± 13.2
Biological parameters at admissionSerum sodium (mmol/L) 133.9 ± 6.8Serum creatinine (µmol/L) 155.6 ± 138.8Bilirubin T (µmol/L) 169.7 ± 193.9INR 3.02 ± 2.39
Mortality ICU 131 (34.7%)Hospital 162 (42.9%)
SAPS, Simplified Acute Physiology Score; SOFA, Sequential Organ Failure Assess-ment; MELD, Model for End-Stage Liver Disease; MESO, the MELD to sodiumindex; iMELD, the integrated MELD; MELD-Na, the MELD with the incorporationof serum sodium; ICU, Intensive Care Unit.
JOURNAL OF HEPATOLOGY
two groups (p <0.001). Patients admitted with acute varicealbleeding and hepatic encephalopathy had better prognosis forsurvival, respectively 76.5% and 74.5%, whereas patients admit-ted for infection had a cumulative survival in the ICU of 36.2%.In the subgroup of patients with severe acute histologically pro-ven alcoholic hepatitis, the ICU and hospital mortality rate were61% and 74%, respectively. Among the surviving patients, fivepatients underwent liver transplantation within 5–356 days afterICU admission.
Journal of Hepatology 20
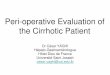
Patients with cirrhosis who died during their ICU stay dis-played significantly higher values on all prognostic scores atadmission when compared to those who survived (Table 2). Recei-ver Operating Characteristic curves were used to evaluate thepower of the scores (Fig. 1A and B). SOFA and SAPS II scores calcu-lated 24 h after ICU admission were found to be the most reliablesystems relative to survival, with AUROC values of 0.92 (SE 0.01,95% CI 0.89–0.95) and 0.89 (SE 0.2, 95% CI 0.86–0.93), respectively.The AUROC of SOFA score was not statistically different from theAUROC of SAPS II score (p = 0.1). General prognostic scores had thehighest AUROC values when compared to liver-specific prognosticmodels (p <0.01 with each of these scores). No differences wereseen between the MELD and the different models incorporatingserum sodium (p >0.05). The Child–Pugh score had the lowestAUROC (0.79, SE 0.02, 95% CI 0.74–0.84).
Using the highest Youden Index [28], we determined the mostdiscriminative cut-off point (for each prognostic score) from thedifferent ROC curves. Different datasets were calculated basedon the cut-off values for the SAPS II, SOFA, and MELD scores,which were 47.5, 10.5, and 28.5, respectively (Table 3).Fig. 2(A–C) shows the cumulative survival rates for the studypopulation dichotomized by the cut-off point which discernedpatients who would die in the ICU with a p <0.001. We alsoobserved a significant difference in cumulative survival at60 days between the three Child–Pugh categories (A–C) (Fig. 2D).
At admission to the ICU, 71% (270/377) of patients presentedwith failure of one or more organs. The number of organ failuresat admission (as defined by the SOFA score) was significantlyrelated to ICU mortality, with a rate ranging from 2.8% in patientswithout organ failure to 90.6% in patients with three or moreorgan failures. At admission, 30.5% (n = 115) of the patientsneeded an organ support. Eighty eight patients (23.3%) were trea-ted with vasopressors (e.g. epinephrine, norepinephrine, dobuta-mine, or dopamine >5 lg/kg/min). Eighty seven patients (23.1%)required mechanical ventilation. The main reasons for endotra-cheal intubation and mechanical ventilation at admission were:respiratory insufficiency secondary to infection in 38 cases(including 16 patients with pneumonia), hemorrhagic shock in19 cases, airway protection (endoscopy) in 10 cases, and hepaticencephalopathy in eight cases.
ICU stay
During their stay in the ICU, a total of 172 patients (45.6%)required intubation and mechanical ventilation. In addition tothe patient who required mechanical ventilation at admission,85 other patients were intubated during their ICU stay including69 patients for respiratory insufficiency due to an infection(mainly pneumonia, n = 59) and hepatic encephalopathy(n = 10). There was no difference in ICU mortality between thepatients who were intubated for airway protection (includingencephalopathy) and those who were intubated for respiratoryfailure.
One hundred and fifty four patients (40.8%) needed vasopres-sor therapy (epinephrine, norepinephrine, dobutamine, or dopa-mine >5 lg/kg/min) for septic or hemorrhagic shock. Thirtynine patients required Renal Replacement Therapy (RRT) duringtheir ICU stay. The Molecular Adsorbent Recirculating System(MARS�) was used in 36 patients (9.5%) with severe progressivejaundice, hepatic encephalopathy, hepatorenal syndrome, orany combination of these syndromes. The number of organ sup-
12 vol. 56 j 95–102 97

Table 2. Predictive factors of ICU mortality determined by univariate analysis in 377 cirrhosis patients admitted to an ICU. The Area Under the Receiver OperatingCharacteristic Curve (AUROC) value of prognostic scores at ICU admission were: SOFA, 0.92; SAPS II, 0.89; MELD, 0.82; MESO, 0.82; iMELD, 0.81; MELD-Na, 0.79; Child–Pugh, 0.79. Data are expressed as mean ± S.D.
Variable Survivors(n = 246)
Non-Survivors(n = 131)
p value
Age (years, mean ± SD) 55.2 ± 11.9 56.1 ± 10.2 0.49Gender (M/F) 179/67 98/33 0.67Cause of cirrhosis n (%) 0.64
Alcoholic 163 (66) 95 (73)Hepatitis B 10 (4) 5 (4)Hepatitis C 37 (15) 15 (11)Alcoholic + Hepatitis 13 (5) 8 (6)Others 23 (10) 8 (6)
Primary diagnosis ICU admission n (%) <0.0001Acute variceal bleeding 124 (51) 38 (29)Severe infection 26 (10) 46 (35)Hepatic encephalopathy 35 (14) 12 (9)Hepatorenal syndrome type I 11 (5) 8 (6)Other 50 (20) 27 (21)
Laboratory dataSerum sodium (mmol/L) 134.4 ± 6.1 133.2 ± 7.9 0.02Serum creatinine (µmol/L) 126.9 ± 131.4 209.3 ± 136.9 <0.001Serum bilirubin (mmol/L) 124.8 ± 157.9 253.9 ± 224.8 <0.001INR 2.34 ± 1.26 4.29 ± 3.30 <0.001
Organ support at admissionMechanical ventilation 18 (7) 69 (52) <0.001Vasopressor therapy* 18 (7) 70 (53) <0.001
Prognostic scores at ICU admissionSAPS II 35.4 ± 13.7 64.9 ± 19.3 <0.0001SOFA 6.8 ± 3.1 14.2 ± 4.0 <0.0001Child Pugh 9.7 ± 2.2 12.0 ± 1.8 <0.0001Child Pugh category (A/B/C) 24/81/141 1/8/122 <0.0001MELD 20.7 ± 9.5 32.8 ± 8.2 <0.0001MELD Na 24.8 ± 12.4 38.7 ± 11.6 <0.0001MESO 1.6 ± 0.7 2.48 ± 0.6 <0.0001iMELD 43.2 ± 11.4 57.3 ± 11.4 <0.0001
Clinical feature during ICU n (%)Mechanical ventilation 45 (18) 127 (97) <0.0001Vasopressor therapy* 30 (12) 124 (95) <0.0001Renal replacement therapy 4 (2) 35 (27) <0.0001Molecular adsorbent recirculating system 18 (7) 18 (14) 0.04
SAPS, Simplified Acute Physiology Score; SOFA, Sequential Organ Failure Assessment; MELD, Model for End-Stage Liver Disease; MESO, the MELD to sodium index; iMELD,the integrated MELD; MELD-Na, the MELD with the incorporation of serum sodium; ICU, Intensive Care Unit.⁄Vasopressors: epinephrine, norepinephrine, dobutamine, or dopamine >5 lg/kg/min.
Research Article
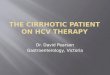
ports (mechanical ventilation, vasopressor therapy, RRT, andMARS�) during the ICU stay was significantly related to ICU mor-tality, which ranged from 2.2% (patients not requiring organ sup-port) to 96.1% in patients requiring the support of three or moreorgans (Fig. 3).
The length of ICU stay in survivor patients was statisticallysignificantly shorter than in non-survivor patients (7.5 ± 7.8 daysvs. 13.8 ± 15.1 days, p <0.0001).
98 Journal of Hepatology 20
Infections
One hundred and sixty-nine patients (44.8% of the totalstudy population) had obvious infection as alreadydefined. Infection was present in 72 patients at their admis-sion to the Liver ICU, related to pneumonia in 51% of cases(n = 37) or spontaneous bacterial peritonitis in 21% of cases(n = 14).
12 vol. 56 j 95–102

1.0
0.8
0.6
0.4
0.2
0.0
Sens
itivi
ty
0.0 0.4 0.60.2 0.8 1.0
A B
SAPSIISOFAMELDCP
iMELDMELDNaMELDMESO
1.0
0.8
0.6
0.4
0.2
0.0Se
nsiti
vity
0.0 0.4 0.60.2 0.8 1.01-Specificity1-Specificity
Fig. 1. Receiver Operating Characteristic (ROC) curves for (A) SAPS II, SOFA,MELD, Child–Pugh and for (B) MELD, MELD-Na, MESO, iMELD in 377 cirrhoticpatients admitted to an ICU.
T
Sn
JOURNAL OF HEPATOLOGY
Among the organisms identified in the 37 community-acquired pneumonia, gram negative bacilli were the most fre-quent (10 out of the 21 isolates, mainly Escherichia coli) and grampositive cocci in 9 out of the 21 isolates (Streptococcus pneumo-niae and Staphylococcus aureus). The most frequent organism iso-late in spontaneous bacterial peritonitis were E. coli (n = 5),Enterobacter spp. (n = 3) and streptococcus (n = 3).
Ninety-seven patients developed a hospital-acquired infectionat the following sites: respiratory infections (n = 55, 56%); bacter-emia (n = 26; 26.8%) and others including spontaneous bacterialperitonitis and urinary tract infections (n = 16; 16.5%). The mostfrequent organism causing acquired pneumonia were E. coli andEnterobacter spp. (n = 21; 38%), Pseudomonas (n = 8; 14.5%), andStaphylococcus (n = 8; 14.5%). Staphylococcus was the main organ-ism identified in the hospital acquired bacteremia.
In this cohort, the fungal infections impacted on ICU mortal-ity. Among the 20 patients with a fungal positive sample, 18 diedduring their ICU stay (90%) and one patient within 2 months fol-lowing ICU discharge. The distribution of fungal infections associ-ated Pneumocystis Juroveci pneumonia in two patients,candidemia in four patients, pulmonary aspergillosis in sixpatients, and positive tracheal aspirate samples for candida colo-nization (n = 9).
The presence of infection was strongly associated with poorsurvival at 2 months (Fig. 4A). In the subgroup of patients withinfection, we observed a similar cumulative survival betweenpatients with an infection at admission and patients with hospi-tal-acquired infection (Fig. 4B).
In addition, in 107 patients (81.6%), the infection (pneumonia,spontaneous bacterial peritonitis, or septicemia) is the cause ofdeath. Of these, 46 patients (43%) presented with sepsis at admis-sion to the ICU. In the other 61 patients, mortality was secondaryto hospital-acquired infection.
able 3. Prediction of subsequent ICU mortality in 377 cirrhotic patients after the firs
Scoring system Cut-off point Youden Index Sensitivi
SOFA 10.5 0.67 79MELD 28.5 0.50 72SAPS II 47.5 0.65 83
APS, Simplified Acute Physiology Score; SOFA, Sequential Organ Failure Assessment; Megative predictive value.
Journal of Hepatology 20
Factors associated with mortality: multivariate logistic regressionanalyses
A logistic regression analysis with mortality as the end-point wasperformed using categorical and/or continuous variables. Prog-nostic scores at admission were excluded from this analysis toprevent any risk of colinearity. Table 4 shows that bilirubin atadmission, infection at admission or acquired during the ICU stay,mechanical ventilation and vasopressor therapy were indepen-dently related to ICU mortality.
Discussion
The main result of this study is that the SAPS II and SOFA scoresperformed better than standard MELD, MELD incorporatingsodium levels and the Child–Pugh score to predict ICU mortalityin cirrhotic patients admitted to an ICU.
Our findings agree with those of Cholongitas et al. [11]. Intheir meta-analysis grouping 21 cohorts from studies publishedduring the past 20 years, these authors observed that liver func-tion was not the main determinant of outcome in cirrhoticpatients with multi-organ failure, so that an organ failure scoresuch as SOFA could be more useful in predicting outcome [11].Nevertheless, for several decades, Child–Pugh remained the mostwidely-used score despite its major limitation i.e. it does notinclude other organ dysfunctions known to highly contribute tomortality rates in critically ill cirrhotic patients [29].
Recognizing the problems inherent in the Child–Pugh score,two recent studies evaluated the performance of the MELD score(a liver prognostic score that includes renal function) in cirrhoticpatients admitted to an ICU [13,14]. Both studies reported thatthe MELD is a reliable scoring system to predict mortality inpatients with decompensated cirrhosis. In addition, the MELDand SOFA scores had similar discriminatory power (AUROC = 0.81and 0.83, respectively) [13]. Although we found a discriminatorypower for the MELD (AUROC = 0.83) that was similar to thosereported by these two studies, we observed that the SOFA scorewas more effective in predicting ICU mortality (AUROC = 0.92),which was in line with the findings of other studies [4,6,30].
The MELD model does not include any surrogate of portalhypertension, the complications of which are a frequent causeof admission to an ICU. To make up for this deficiency, Na valueshave now been added to the MELD score [16]. Indeed, in patientswith liver cirrhosis, hyponatremia is a common event that corre-lates with the severity of portal hypertension [16,31–33]. To date,this concept has only been evaluated by one study in decompen-sated cirrhotic patients [34], which reported that the three vari-ants of MELD scores incorporating Na levels improved the
t day of ICU admission.
ty (%) Specificity (%) PPV (%) NPV (%)
87 78 8878 63 8481 70 91
ELD, Model for End-Stage Liver Disease; PPV, positive predictive value; NPV,
12 vol. 56 j 95–102 99

100
80
60
40
20
0Cum
ulat
ive
surv
ival
rate
(%)
0
223104
21288
20166
19050
18942
18750
18438
10 20 30From admission to ICU (Days)
40 50 60No. of patients at risk:
<47.5≥47.5
A
p <0.001
82.5%
24.7%SAPS II <47.5SAPS II ≥47.5
100
80
60
40
20
0Cum
ulat
ive
surv
ival
rate
(%)
0
243134
22773
21453
20436
20229
20027
19626
10 20 30From admission to ICU (Days)
40 50 60No. of patients at risk:
<10.5≥10.5
B
p <0.001
80.7%
19.4%SOFA <10.5SOFA ≥10.5
100
80
60
40
20
0Cum
ulat
ive
surv
ival
rate
(%)
0
228149
20694
19869
18951
18546
18344
18042
10 20 30From admission to ICU (Days)
40 50 60No. of patients at risk:
<28.5≥28.5
C
p <0.001
78.9%
28.2%
MELD <28.5MELD ≥28.5
100
80
60
40
20
0Cum
ulat
ive
surv
ival
rate
(%)
0
2489255
2385189
2379163
2378137
2378129
2377126
2375123
10 20 30From admission to ICU (Days)
40 50 60No. of patients at risk:
Child AChild BChild C
D
p <0.001
96.0%84.3%
48.2% Child A Child B Child C
Fig. 2. Cumulative survival in 377 cirrhotic patients admitted to an ICUaccording to (A) SAPS II (solid curve, SAPS II >47.5 and dashed curve SAPS II<47.5), (B) SOFA (solid curve, SOFA >10.5 and dashed curve SOFA <10.5), (C)MELD score (solid curve, MELD >28.5 and dashed curve MELD <28.5), and (D)category of Child–Pugh (A, B or C) after the first day of ICU admission.
100
80
60
40
20
0Perc
enta
ge o
f mor
talit
y (%
)
0 (n = 178)
2 (n = 95)
3 or more (n = 52)
1 (n = 52)
2.2
77.9
96.1
5.8
Number of organ support during ICU stay
Fig. 3. Correlation between the number of organ supports required (duringthe ICU stay) and ICU mortality in 377 cirrhotic patients (p <0.005).
Research Article
prognostic value of MELD at 3, 6, and 12 months. The presentstudy is the first to show that models incorporating Na levelsdo not predict ICU mortality better than MELD alone in such
100 Journal of Hepatology 20
patients. Recently, using only the MELD-Na model and studyinga smaller cohort, Das et al. reported results similar to ours [15].The higher MELD values obtained in our cohort (when comparedto those found by Jiang et al. [34]) might explain this difference.
As mentioned above, the performance of scores to predict ICUmortality can partly be explained by the inclusion in these mod-els of surrogate variables related to organ dysfunction and notjust the variable related to liver severity (Na+, bilirubin, or INR).During our study, cirrhotic patients admitted to an ICU had amortality rate approaching 90% if they experienced the failureof more than three organs or if they required more than twotypes of organ support or replacement therapy (mechanical ven-tilation, vasopressor therapy, RRT, or MARS). Based on our logisticregression models, organ support (mechanical ventilation andvasopressor therapy) was an independent predictor of mortalityin our population.
Like other authors, we also observed that infection in cirrhoticpatients was an independent predictor of mortality [35–37].Infection has also been associated with significantly more inten-sive support [36]. This concept is consistent with similar studiesshowing a close relationship between mortality and SIRS, consid-ering that 46–60% of infected patients with cirrhosis will developSIRS [38–40].
The cause of ICU admission is associated with the prognosis ofpatients. In our experience, patients admitted in ICU for acutevariceal bleeding or hepatic encephalopathy had a markedlyimproved ICU survival of 76.5% vs. 36.2% for patients admittedfor infection indication. However, in comparison with recentstudies, in our work, the ICU mortality rate for the subgroup ofpatients with acute variceal bleeding is high [41,42]. However,our situation of tertiary university intensive care unit may causea selection bias in the patient recruitment, including morepatients with failure to control variceal bleeding, rebleeding,hemorrhagic shock, and patients transferred for salvage TIPS.
In an era of advanced organ-targeted therapies in critical care,we believe that the key issue is to ensure a more aggressive man-agement of cirrhotic patients before the onset of organ dysfunc-tion. In this situation, admission to the ICU of cirrhotic patientsis not futile and can result in survival rates as high as 65%. Inaddition, because prognostic models can predict a better outcomein cirrhotic patients when assessed 48 h after admission [43], webelieve that all cirrhotic patients should be admitted to an ICUand then rapidly reassessed. However, the criteria for this reas-sessment need to be defined, but they should include prognosticscores (to evaluate organ failure) and additional factors (primaryICU diagnosis, sepsis, organ support). In this regard, Gildea et al.
12 vol. 56 j 95–102

100
80
60
40
20
0Cum
ulat
ive
surv
ival
rate
(%)
0
208169
182118
17592
17268
17160
16957
16854
10 20 30Days
40 50 60No. of patients at risk:
Infection groupNo-infection group
100
80
60
40
20
0Cum
ulat
ive
surv
ival
rate
(%)
0
7297
4177
3458
2939
2634
2532
2331
10 20 30Days
40 50 60No. of patients at risk:
At admission groupHospital aquired group
A
B
p <0.001
80.8%
32.0%
p = 0.32
31.9%
32.0%
Infection at admissionHospital acquired infection
Infection No-infection
Fig. 4. Cumulative survival in 377 cirrhotic patients admitted to an ICUaccording to the development of infection during the ICU stay. Day 0 is the dayof admission to the ICU.
Table 4. Factors independently associated with ICU mortality in 377 cirrhoticpatients admitted in an ICU.
Odds ratio
95% CI p
Mechanical ventilation 50.3 8.99-281 <0.001Vasopressor therapy 11.9 3.77-37.03 <0.001Infection 3.51 1.35-9.15 0.01Bilirubin 1.006 1.003-1.01 0.0005
JOURNAL OF HEPATOLOGY
whose study included 420 cirrhotic patients admitted to a med-ical ICU, showed that those with three risk factors had a 1 monthmortality rate of 92%, compared to 11% for patients with no riskfactors [7]. The risk factors applied during the present study werea prognostic score (APACHE III score) of >90, organ support(requirement for vasopressors), and biological parameters whichincreased during sepsis (severity of jaundice).
In conclusion, our data show that the prognosis for cirrhoticpatients admitted to an ICU depends on both the severity ofhepatic and extra-hepatic organ dysfunctions and the primarydiagnosis at admission. With a positive predictive value of only78%, we believe that the influence of prognostic scores on deci-sions to admit (or not to admit) patients with cirrhosis to anICU should be minimal, and that these scores should not consti-tute a preadmission screening tool. It is difficult to predict out-come in cirrhotic ICU patients, and a combination of prognosticscores such as SOFA (developed in large and heterogeneous ICUpopulations) and MELD (developed to predict the short-term
Journal of Hepatology 20
prognosis for non-critically ill cirrhotic patients with additionalfactors such as infection, organ failure or organ support) couldbe applied during the decision-making process on whether towithdraw or pursue care for cirrhotic patients in an ICU.
Conflict of interest
The authors who have taken part in this study do not have anyrelationship with the manufacturers of the drugs involved eitherin the past or present and did not receive any funding from themanufacturer to carry out this research.
References
[1] Shellman RG, Fulkerson WJ, DeLong E, Piantadosi CA. Prognosis of patientswith cirrhosis and chronic liver disease admitted to the medical intensivecare unit. Crit Care Med 1988;16:671–678.
[2] Singh N, Gayowski T, Wagener MM, Marino IR. Outcome of patients withcirrhosis requiring intensive care unit support: prospective assessment ofpredictors of mortality. J Gastroenterol 1998;33:73–79.
[3] Aggarwal A, Ong JP, Younossi ZM, Nelson DR, Hoffman-Hogg L, Arroliga AC.Predictors of mortality and resource utilization in cirrhotic patients admittedto the medical ICU. Chest 2001;119:1489–1497.
[4] Chen YC, Tsai MH, Ho YP, Hsu CW, Lin HH, Fang JT, et al. Comparison of theseverity of illness scoring systems for critically ill cirrhotic patients withrenal failure. Clin Nephrol 2004;61:111–118.
[5] Wong LL, McFall P, Wong LM. The cost of dying of end-stage liver disease.Arch Intern Med 1997;157:1429–1432.
[6] Wehler M, Kokoska J, Reulbach U, Hahn EG, Strauss R. Short-term prognosisin critically ill patients with cirrhosis assessed by prognostic scoringsystems. Hepatology 2001;34:255–261.
[7] Gildea TR, Cook WC, Nelson DR, Aggarwal A, Carey W, Younossi ZM, et al.Predictors of long-term mortality in patients with cirrhosis of the liveradmitted to a medical ICU. Chest 2004;126:1598–1603.
[8] Rabe C, Schmitz V, Paashaus M, Musch A, Zickermann H, Dumoulin FL, et al.Does intubation really equal death in cirrhotic patients? Factors influencingoutcome in patients with liver cirrhosis requiring mechanical ventilation.Intensive Care Med 2004;30:1564–1571.
[9] Child C, Turcotte J. The liver and portal hypertension. In: Child CI, editor.Surgery and portal hypertension. Philadelphia, PA: Saunders; 1964. p. 50–58.
[10] Pugh RN, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transectionof the oesophagus for bleeding oesophageal varices. Br J Surg1973;60:646–649.
[11] Cholongitas E, Senzolo M, Patch D, Shaw S, Hui C, Burroughs AK. Reviewarticle: scoring systems for assessing prognosis in critically ill adultCirrhotics. Aliment Pharmacol Ther 2006;24:453–464.
[12] Malinchoc M, Kamath PS, Gordon FD, Peine CJ, Rank J, ter Borg PC. A model topredict poor survival in patients undergoing transjugular intrahepaticportosystemic shunts. Hepatology 2000;31:864–871.
[13] Cholongitas E, Senzolo M, Patch D, Kwong K, Nikolopoulou V, Leandro G,et al. Risk factors, sequential organ failure assessment and model for end-stage liver disease scores for predicting short term mortality in cirrhoticpatients admitted to intensive care unit. Aliment Pharmacol Ther2006;23:883–893.
[14] Yu JW, Wang GQ, Li SC. Prediction of the prognosis in patients with acute-on-chronic hepatitis using the MELD scoring system. Gastroenterol Hepatol2006;21:1519–1524.
[15] Das V, Boelle PY, Galbois A, Guidet B, Maury E, Carbonell N, et al. Cirrhoticpatients in the medical intensive care unit: early prognosis and long-termsurvival. Crit Care Med 2010;38:2108–2116.
[16] Kim WR, Biggins SW, Kremers WK, Wiesner RH, Kamath PS, Benson JT, et al.Hyponatremia and mortality among patients on the liver-transplant waitinglist. N Engl J Med 2008;359:1018–1026.
[17] Biggins SW, Rodriguez HJ, Bacchetti P, Bass NM, Roberts JP, Terrault NA.Serum sodium predicts mortality in patients listed for liver transplantation.Hepatology 2005;41:32–39.
[18] Biggins SW, Kim WR, Terrault NA, Saab S, Balan V, Schiano T, et al. Evidence-based incorporation of serum sodium concentration into MELD. Gastroen-terology 2006;130:1652–1660.
[19] Luca A, Angermayr B, Bertolini G, Koenig F, Vizzini G, Ploner M, et al. Anintegrated MELD model including serum sodium and age improves the
12 vol. 56 j 95–102 101

Research Article
prediction of early mortality in patients with cirrhosis. Liver Transpl2007;13:1174–1180.[20] Huo TI, Wang YW, Yang YY, Lin HC, Lee PC, Hou MC, et al. Model for end-stage liver disease score to serum sodium ratio index as a prognosticpredictor and its correlation with portal pressure in patients with livercirrhosis. Liver Int 2007;27:498–506.
[21] Le Gall JR, Lemeshow S, Saulnier F. A new Simplified Acute Physiology Score(SAPS II) based on a European/North American multicenter study. JAMA1993;270:2957–2963.
[22] Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, et al.The SOFA (Sepsis-related Organ Failure Assessment) score to describe organdysfunction/failure. On behalf of the Working Group on Sepsis-RelatedProblems of the European Society of Intensive Care Medicine. Intensive CareMed 1996;22:707–710.
[23] Wiesner R, Edwards E, Freeman R, Harper A, Kim R, Kamath P, et al. UnitedNetwork for Organ Sharing Liver Disease Severity Score Committee. Modelfor end-stage liver disease (MELD) and allocation of donor livers. Gastro-enterology 2003;124:91–96.
[24] Luna CM, Blanzaco D, Niederman MS, et al. Resolution of ventilator-associated pneumonia: prospective evaluation of the clinical pulmonaryinfection score as an early clinical predictor of outcome. Crit Care Med2003;31:676–682.
[25] Pugin J, Auckenthaler R, Mili N, et al. Diagnosis of ventilator-associatedpneumonia by bacteriologic analysis of bronchoscopic and nonbroncho-scopic ‘‘blind’’ bronchoalveolar lavage fluid. Am Rev Respir Dis1991;143:1121–1129.
[26] Meduri GU, Chastre J. The standardization of bronchoscopic techniques forventilator-associated pneumonia. Chest 1992;102:557S–564S.
[27] DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under twoor more correlated receiver operating characteristic curves: a nonparametricapproach. Biometrics 1988;44:837–845.
[28] Youden WJ. Index for rating diagnostic tests. Cancer 1950;3:32–35.[29] Du Cheyron D, Bouchet B, Parient JJ, Ramakers M, Charbonneau P. The
attributable mortality of acute renal failure in critically ill patients with livercirrhosis. Intensive Care Med 2005;31:1693–1699.
[30] Tsai MH, Peng YS, Lien JM, Weng HH, Ho YP, Yang C, et al. Multiple organsystem failure in critically ill cirrhotic patients. A comparison of twomultiple organ dysfunction/failure scoring systems. Digestion2004;69:190–200.
[31] Samuel D. MELD-Na as a prognostic score for cirrhotic patients: hyponatre-mia and ascites are back in the game. J Hepatol 2009;50:836–841.
102 Journal of Hepatology 20
[32] Ginès A, Escorsell A, Ginès P, Saló J, Jiménez W, Inglada L, et al. Incidence,predictive factors, and prognosis of the hepatorenal syndrome in cirrhosiswith ascites. Gastroenterology 1993;105:229–236.
[33] Arroyo V, Rodés J, Gutiérrez-Lizárraga MA, Revert L. Prognostic value ofspontaneous hyponatremia in cirrhosis with ascites. Am J Dig Dis1976;21:249–256.
[34] Jiang M, Liu F, Xiong WJ, Zhong L, Chen XM. Comparison of four models forend-stage liver disease in evaluating the prognosis of cirrhosis. World JGastroenterol 2008;14:6546–6550.
[35] Moreau R, Hadengue A, Soupison T, Kirstetter P, Mamzer MF, Vanjak D, et al.Septic shock in patients with cirrhosis: hemodynamic and metaboliccharacteristics and intensive care unit outcome. Crit Care Med1992;20:746–750.
[36] Karvellas CJ, Pink F, McPhail M, Austin M, Auzinger G, Bernal W, et al.Bacteremia, acute physiology and chronic health evaluation II and modifiedend stage disease are independent predictors of mortality in critically illnontransplanted patients with acute on chronic liver failure. Crit Care Med2010;38:121–126.
[37] Cho JH, Park KH, Kim SH, Bang JH, Park WB, Kim HB, et al. Bacteremia is aprognostic factor for poor outcome in spontaneous bacterial peritonitis.Scand J Infect Dis 2007;39:697–702.
[38] Cazzaniga M, Dionigi E, Gobbo G, Fioretti A, Monti V, Salerno F. The systemicinflammatory response syndrome in cirrhotic patients: relationship withtheir in-hospital outcome. J Hepatol 2009;51:475–482.
[39] Thabut D, Massard J, Gangloff A, Carbonell N, Francoz C, Nguyen-Khac E,et al. Model for end-stage liver disease score and systemic inflammatoryresponse are major prognostic factors in patients with cirrhosis and acutefunctional renal failure. Hepatology 2007;46:1872–1882.
[40] Plessier A, Denninger MH, Consigny Y, Pessione F, Francoz C, Durand F, et al.Coagulation disorders in patients with cirrhosis and severe sepsis. Liver Int2003;23:440–448.
[41] Carbonell N, Pauwels A, Serfaty L, Fourdan O, Levy VG, Poupon R. Improvedsurvival after variceal bleeding in patients with cirrhosis over the past twodecades. Hepatology 2004;40:652–659.
[42] Bittencourt PL, Farias AQ, Strauss E, Mattos AA, et al. Variceal bleeding:consensus meeting report from the Brazilian Society of Hepatology. ArqGastroenterol 2010;47:202–216.
[43] Cholongitas E, Betrosian A, Senzolo M, Shaw S, Patch D, Mamousou P, et al.Prognostic models in cirrhotics admitted to intensive care units betterpredict outcome when assessed at 48 h after admission. J GastroenterolHepatol 2008;23:1223–1227.
12 vol. 56 j 95–102