Embed Size (px)
Citation preview
www.elsevier.com/locate/ajem
American Journal of Emergency Medicine (2013) 31, 185–189
Original Contribution
Prospective evaluation of the use of the thrombolysis inmyocardial infarction score as a risk stratification tool forchest pain patients admitted to an ED observation unit☆
Jessica Holly MD, Matthew Fuller MD⁎, David Hamilton BS, Michael Mallin MD,Kathryn Black BS, Riann Robbins BS, Virgil Davis MD, Troy Madsen MD
University of Utah School of Medicine, Department of Surgery, Division of Emergency Medicine, Salt Lake City,UT 84132, USA
Received 13 April 2012; revised 4 July 2012; accepted 7 July 2012
AbstractBackground: The Thrombolysis in Myocardial Infarction (TIMI) score has shown use in predicting 30-day and 1-year outcomes in emergency department (ED) patients with potential acute coronarysyndrome. Few studies have evaluated the TIMI score in risk stratifying patients selected for the EDobservation Unit (EDOU). Risk stratification of patients in this group could identify those at risk forsignificant cardiac events. Our goal was to evaluate TIMI use for risk stratification in this population andcompare outcomes among differing scores.Methods: A prospective observational study with 30-day telephone follow-up for a 12 month period.Baseline data, outcomes related to EDOU stay, admission, and 30-day outcomes were recorded. TIMIscores were calculated for each patient placed in EDOU. TIMI score was not utilized in the decision toplace patients in observation.Results: N = 552. Composite outcomes recorded were myocardial infarction, revascularization, ordeath either during the EDOU stay, inpatient admission, or the 30-day follow-up. Eighteencomposite outcomes were recorded: stent (12 patients), coronary artery bypass graft (3 patients),myocardial infarction and stent (2 patients), and myocardial infarction, and coronary artery bypassgraft (1 patient). Distribution by TIMI score was: 0 (102 patients), 1 (196), 2 (142), 3 (72), 4 (27),and 5 (5). Risk of composite outcome increased by score: 0 (1%), 1 (2.6%), 2 (2.1%), 3 (6.9%), 4(11.1%), and 5 (20%). Those with an intermediate risk score (3-5) were also more likely to requireadmission (15.4% vs 9.8%, P = .048).Conclusion: The TIMI risk score may serve as an effective risk stratification tool among chest painpatients selected for EDOU placement. Patients with intermediate-risk by TIMI may be consideredfor inpatient admission and/or more aggressive evaluation and therapy.© 2013 Elsevier Inc. All rights reserved.
☆ Funding Sources: University of Utah Medical Group QualityAssessment Grant.
⁎ Corresponding author. Tel.: +1 801 581 2272; fax: +1 801 585 0603.E-mail address: [email protected] (M. Fuller).
0735-6757/$ – see front matter © 2013 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.ajem.2012.07.006
1. Introduction
Chest pain is a common presenting complaint amongemergency department (ED) patients. Accurate and timelyrisk stratification is necessary to initiate appropriate

186 J. Holly et al.
treatment and patient disposition. Electrocardiograms(ECG) and cardiac biomarkers can be helpful; however,risk stratification of non–ST-segment elevation (NSTE)acute coronary syndrome (ACS) remains a challenge.Among chest pain patients with nondiagnostic ECGs andnormal cardiac biomarkers, 2% to 4% of patients withacute myocardial infarction (MI) are inadvertently dis-charged home from the emergency department [1-3].
Several scoring systems have been developed to aid inthe risk stratification of patients with unstable angina andNSTE MI. The Thrombolysis In Myocardial Infarction(TIMI) score is a widely validated tool initially developed topredict the patient's risk of death or cardiac ischemic eventsat 14 days [4]. The TIMI score is a simple summation of 7variables that can be easily calculated in an emergencydepartment setting (Table 1). Multiple studies havedemonstrated the utility of the TIMI score in predictingboth 30-day and 1-year outcomes among emergencydepartment patients with potential ACS. [5-12]; however,few studies have evaluated the utility of the TIMI score as arisk stratification tool among patients selected for placementin an emergency department observation unit (EDOU) [13].Conti and colleagues [13] demonstrated that EDOUs wereequally as safe and more cost effective than conventionalinpatient units for care of intermediate- (TIMI 3-4) to high-risk (TIMI N4) chest pain patients. This cost effectiveadvantage, however, was lost in patients with TIMI scoreN4, suggesting these patients should be admitted totraditional inpatient units.
Accurate risk stratification in this group could potentiallyidentify patients at higher risk for significant cardiac eventswho may be more appropriate for inpatient admission, ratherthan EDOU admission. Our goal was to evaluate the use ofthe TIMI score as a risk stratification tool for chest painpatients admitted to an EDOU and to compare outcomesand inpatient admission rates for patients stratified by theTIMI score.
Table 1 The TIMI risk score for unstable angina andNSTEMI
Historical Points
Age N65 13 or more CAD risk factors (FHx, HTN,hyperlipidemia, DM, smoker)
1
Known CAD (stenosis N50%) 1Aspirin use in past 7 days 1
PRESENTATION2 or more angina events in the past 24 hours 1ST-elevation or depression N1 mm 1Elevated cardiac biomarkers 1RISK SCORE = total points (0-7)
2. Methods
The study design was a prospective observational studyof all chest pain patients admitted to our observation unitwith 30-day follow up. The University of Utah EmergencyDepartment is an urban emergency department with 39000patient visits per year. The observation unit is a 10-bedunit, which opened in April 2006. The observation unit isunder the direction of ED physicians and physicianassistants and cares for over 2500 patients per year. Theunit is designed to care for a variety of patients who areadmitted under different treatment protocols. Each protocolhas specific inclusion and exclusion criteria for theobservation unit and protocolized order sets for thesepatients. The University of Utah EDOU has 21 differenttreatment protocols for patient care, including chest pain,abdominal pain, transient ischemic attack, and pulmonaryembolism, among others, with the chest pain protocol beingthe most frequently used.
The chest pain protocol allows physicians to admit chestpain patients to the observation unit if they have a non-diagnostic ECG, normal or indeterminate troponin I on initialED testing, are hemodynamically stable, and are chest painfree. Patients requiring escalation of care for continued chestpain require inpatient subsequent admission. Additionalexclusion criteria include age greater than 80 and significantcomorbidities such as cancer, liver disease, congestive heartfailure, or renal disease. These were not included as theyhave not been demonstrated as risk factors for heart disease,given our primary outcomes identified. A history of coronaryartery disease is not an exclusion criterion and patients couldbe admitted to the observation unit if the emergencyphysician felt that the individual episode of chest pain hadlow-risk features.
All chest pain patients admitted to the EDOU receiveserial troponin I measurements every six hours for a total ofthree, and ECGs as needed for recurrent chest pain or asdeemed necessary by the EDOU midlevel provider.Cardiology attending physicians evaluate chest pain patientsin the morning, if requested by the ED attending/midlevelprovider after their observation unit admission and makefurther decisions on mode of evaluation (nuclear vstreadmill stress test vs coronary computed tomographyangiography), cardiac catheterization, and inpatient admis-sion. Cardiology consultations were available in the EDOUseven days a week and on holidays. Stress testing isavailable every day except Sunday before noon. Patientsdischarged Sunday morning who were unable to completetesting had prompt next day testing arranged. Patients placedin the ECU in the early afternoon were kept overnight for aperiod of up to 23 hours for additional testing andcardiology consultation.
The ultimate decision to admit the patient to an inpatientunit from the EDOU is made by the consulting cardiologistin cooperation with the EDOU midlevel provider and theattending emergency physician, as needed. Admission

Table 2 Baseline characteristics
Total 552Age(y) 54.1 (19-80)Male 46% (254)Smoker 19.6% (108)Diabetic 19.9% (110)Fam Hx CAD 37.1% (205)Hyperlipidemia 36.6% (204)Prior CAD 18.1% (100)
187TIMI as risk stratification tool for chest pain patients
decisions are based on results of the patient's testing in theEDOU, determination for further inpatient evaluation basedon the patient's history and presentation, or additionaldiagnoses or conditions which may have been identifiedduring the EDOU stay.
We performed a prospective evaluation of all patientsadmitted to the observation unit under the chest painprotocols for the 12-month period from June 1, 2009, toMay 31, 2010. The study received approval from thehospital's institutional review board in October 2007, and allparticipants provided informed written consent for partici-pation and contact via phone at 30 days. Trained researchassociates staffed the observation unit seven days a week toobtain baseline data on all patients placed in the observationunit under the chest pain protocols. Baseline data wererecorded at the time of the patient's observation unitadmission. TIMI scores were calculated based on baselinerisk factors and clinical characteristics as well as providerinterpretation of ECG. ECG interpretation for all patientswas reviewed by the principal investigator (TM). Anydiscrepancies in ECG interpretation were clarified byanother investigator (JH). TIMI score was not utilized inthe decision to admit to the ECU and was calculated withblinding to the patient outcomes. Electronic medical recordswere reviewed for patient outcomes related to the EDOUstay, including positive troponin, provocative testing,cardiac catheterization, stent placement, coronary arterybypass graft (CABG) surgery, and inpatient admission fromthe observation unit. Adverse events during observation unitadmission were recorded, including bleeding, clinicallysignificant arrhythmia requiring medical intervention, un-stable vital signs, and death. A positive troponin was definedas a Troponin I greater than or equal to 0.50 ng/mL (ARUPMill, CPT code 84484), consistent with myocardialischemic injury.
Patient outcomes during 30-day follow-up were deter-mined through telephone contact with patients and review ofthe electronic medical record (EMR) at least 30 days after theEDOU admission. We were able to contact 79.2% of patientsby phone, with follow up performed by EMR review for theremaining 20.8% not contacted by phone. All patients wereincluded in the final database. Outcomes measured at 30-dayfollow up included myocardial infarction, stent placement,CABG or other unplanned events including death. Weconsidered any patient to have experienced an unanticipatedadverse event during the 30-day follow up period if theyexperienced MI or death, or if stent placement or CABG wasperformed and was not part of their arranged outpatientfollow-up from the EDOU.
The principal investigator (TM) reviewed 20% of thecharts, selected randomly, as quality assessment of dataobtained from electronic medical record (κ = .96). Inaddition, the principal investigator reviewed the records ofall patients who had myocardial infarction, inpatientadmission, cardiac catheterization, positive stress test,stent, or CABG to assure the accuracy of the chart review
and to confirm details as reported by patients in telephonefollow-up.
Data were entered into Research Electronic Data Capturedatabase and imported into a Microsoft Excel database for χ2
statistical analysis (SPSS v 17.0). Categorical data arepresented as the percentage frequency occurrence. Therelationship between TIMI risk score and the compositeoutcome was presented as percentage frequency occurrence.
3. Results
During the 12-month study period, a total of 552 patientswere admitted to the observation unit under the chest painprotocol, 46% of whom were male with a mean age of 54.1years (Table 2). Other gathered demographic data indicatedthat approximately 20% were smokers, 20% were diabetic,37% had family history of cardiac disease, 18% had priorcoronary artery disease, and another 36.6% had 3 or morecardiac risk factors.
Of the 552 patients admitted for chest pain, 269 (48.7%)patients had stress echocardiogram and 16 (2.9%) hadmyocardial perfusion stress testing performed. Of the 275patients who had stress testing performed, 7.4% had resultssuggestive of ischemia.
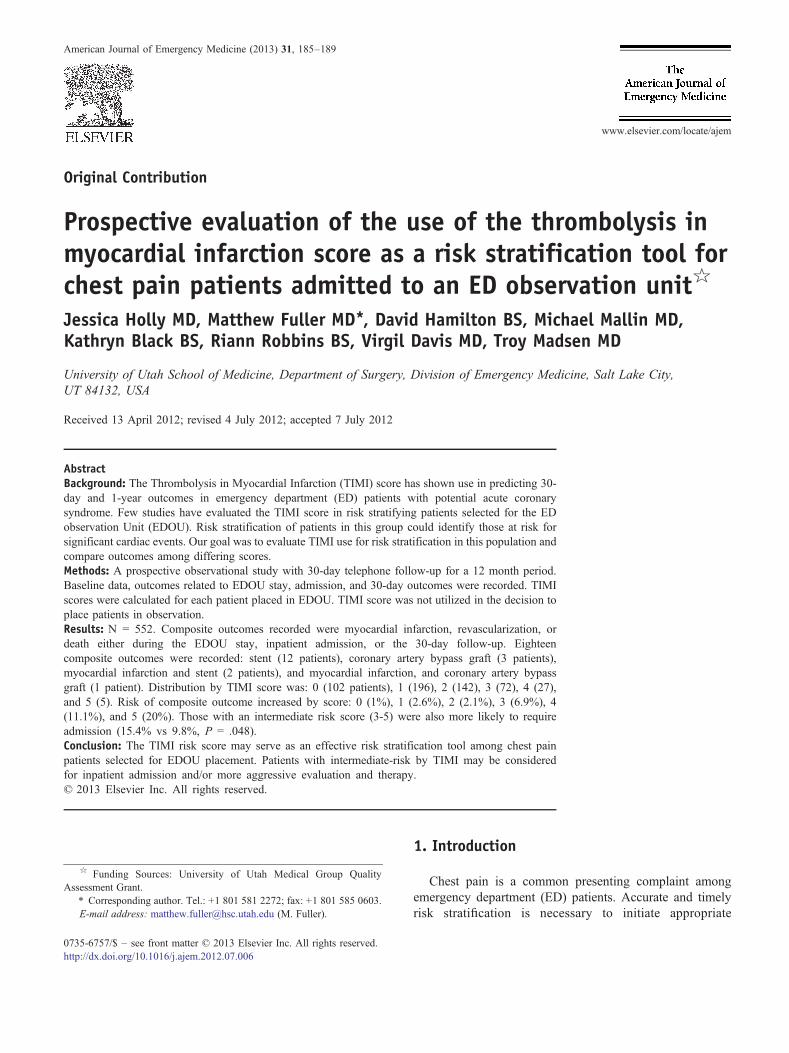
Primary composite study outcomes included myocardialinfarction, revascularization (stent/CABG), or death eitherduring the EDOU stay, inpatient admission, or the 30-dayfollow-up period were evaluated. Eighteen (3.2%) patientsexperienced the composite outcome; 12 patients underwentstent, 3 patients underwent CABG, 2 patients experiencedMI and stent, and 1 patient experienced MI and CABG. Riskof the composite outcome generally increased by TIMIscore: 0 (1%), 1 (2.6%), 2 (2.1%), 3 (6.9%), 4 (11.1%), and 5(20%) (Table 3).
Based on the rates of composite outcome, we establisheda threshold score of 3 or higher as a potential predictor ofintermediate-risk EDOU chest pain patients; 104 (18.8%)patients were intermediate-risk (TIMI score 3-5) vs 448(81%) low-risk patients (TIMI score 0-2). Those who wereintermediate-risk were significantly more likely to experi-ence MI, stent, or CABG than the low-risk group (8.7% vs2%, P = .002) (Fig.). Those intermediate-risk by TIMI score
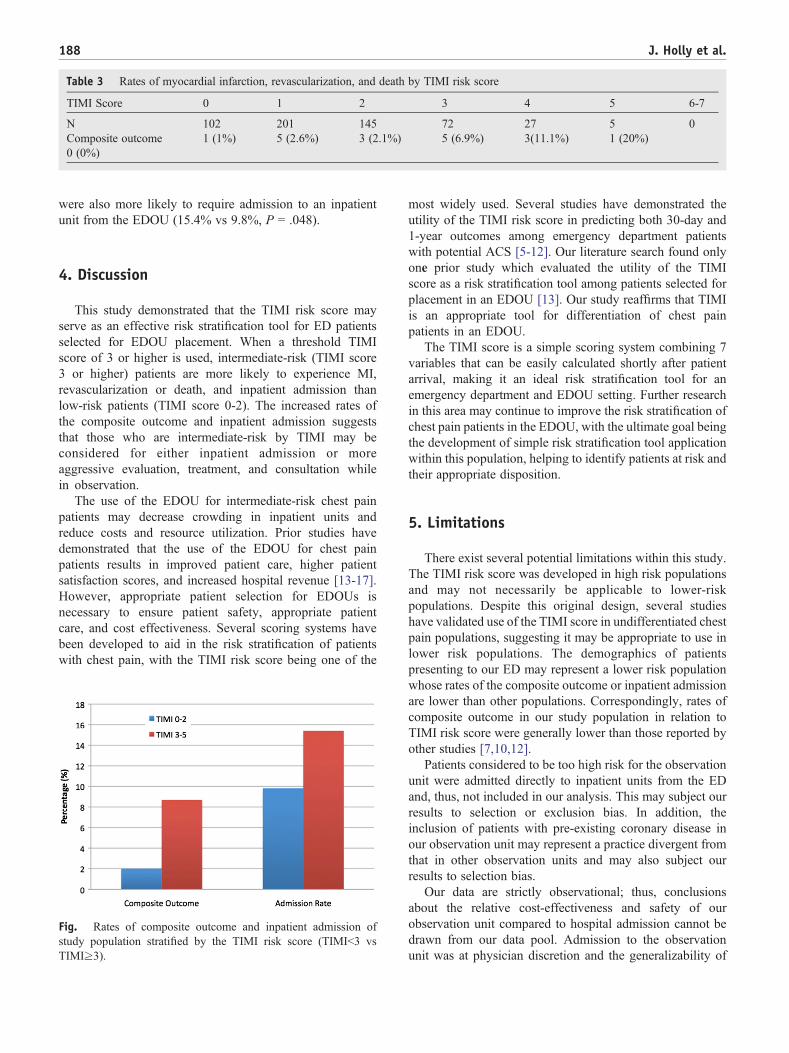
Table 3 Rates of myocardial infarction, revascularization, and death by TIMI risk score
TIMI Score 0 1 2 3 4 5 6-7
N 102 201 145 72 27 5 0Composite outcome 1 (1%) 5 (2.6%) 3 (2.1%) 5 (6.9%) 3(11.1%) 1 (20%)0 (0%)
188 J. Holly et al.
were also more likely to require admission to an inpatientunit from the EDOU (15.4% vs 9.8%, P = .048).
4. Discussion
This study demonstrated that the TIMI risk score mayserve as an effective risk stratification tool for ED patientsselected for EDOU placement. When a threshold TIMIscore of 3 or higher is used, intermediate-risk (TIMI score3 or higher) patients are more likely to experience MI,revascularization or death, and inpatient admission thanlow-risk patients (TIMI score 0-2). The increased rates ofthe composite outcome and inpatient admission suggeststhat those who are intermediate-risk by TIMI may beconsidered for either inpatient admission or moreaggressive evaluation, treatment, and consultation whilein observation.
The use of the EDOU for intermediate-risk chest painpatients may decrease crowding in inpatient units andreduce costs and resource utilization. Prior studies havedemonstrated that the use of the EDOU for chest painpatients results in improved patient care, higher patientsatisfaction scores, and increased hospital revenue [13-17].However, appropriate patient selection for EDOUs isnecessary to ensure patient safety, appropriate patientcare, and cost effectiveness. Several scoring systems havebeen developed to aid in the risk stratification of patientswith chest pain, with the TIMI risk score being one of the
Fig. Rates of composite outcome and inpatient admission ofstudy population stratified by the TIMI risk score (TIMIb3 vsTIMI≥3).
most widely used. Several studies have demonstrated theutility of the TIMI risk score in predicting both 30-day and1-year outcomes among emergency department patientswith potential ACS [5-12]. Our literature search found onlyone prior study which evaluated the utility of the TIMIscore as a risk stratification tool among patients selected forplacement in an EDOU [13]. Our study reaffirms that TIMIis an appropriate tool for differentiation of chest painpatients in an EDOU.
The TIMI score is a simple scoring system combining 7variables that can be easily calculated shortly after patientarrival, making it an ideal risk stratification tool for anemergency department and EDOU setting. Further researchin this area may continue to improve the risk stratification ofchest pain patients in the EDOU, with the ultimate goal beingthe development of simple risk stratification tool applicationwithin this population, helping to identify patients at risk andtheir appropriate disposition.
5. Limitations
There exist several potential limitations within this study.The TIMI risk score was developed in high risk populationsand may not necessarily be applicable to lower-riskpopulations. Despite this original design, several studieshave validated use of the TIMI score in undifferentiated chestpain populations, suggesting it may be appropriate to use inlower risk populations. The demographics of patientspresenting to our ED may represent a lower risk populationwhose rates of the composite outcome or inpatient admissionare lower than other populations. Correspondingly, rates ofcomposite outcome in our study population in relation toTIMI risk score were generally lower than those reported byother studies [7,10,12].
Patients considered to be too high risk for the observationunit were admitted directly to inpatient units from the EDand, thus, not included in our analysis. This may subject ourresults to selection or exclusion bias. In addition, theinclusion of patients with pre-existing coronary disease inour observation unit may represent a practice divergent fromthat in other observation units and may also subject ourresults to selection bias.
Our data are strictly observational; thus, conclusionsabout the relative cost-effectiveness and safety of ourobservation unit compared to hospital admission cannot bedrawn from our data pool. Admission to the observationunit was at physician discretion and the generalizability of

189TIMI as risk stratification tool for chest pain patients
this patient group to other settings and practice patternscannot be predicted.
We utilized telephone follow-up and EMR chart reviewfor outcomes related to the EDOU stay and inpatientadmission, as well as the 30-day follow-up evaluation. Theuse of EMR chart review exposes us to inherent limitationsassociated with chart reviews, and the use of telephonefollow up limits us by patient memory and recall of events. Inan effort to address these stated limitations, EMR data wascompared with telephone follow-up data and confirmed thatall events which patients reported by phone were alsodocumented in the EMR.
Finally, not all observation patients underwent stresstesting, as this practice was at the discretion of the EDattending and the consulting cardiologist. This may introducea bias as to which patients were diagnosed with ACS duringtheir ED stay and may have eventually required stentplacement. Our study design aimed to utilize the 30-dayfollow-up evaluation to capture any diagnoses or outcomeswhich may have been missed due to possible selection andtesting bias. However, this potential for bias remains.
6. Conclusion
The data from our study would suggest that TIMI score isnot only applicable in an ED setting, but also in an EDOUpopulation. The risk stratification of chest pain patients in anED/EDOU setting continues to be an important and pressingissue, both in terms of allocating appropriate care, but also interms of controlling cost. As such, use of the TIMI score inpatients admitted to an EDOU may serve as a simple andeffective evaluation strategy. Our study data suggestsintermediate-risk (TIMI score 3 or higher) patients weremore likely to experience MI, revascularization or death, andinpatient admission than low-risk patients (TIMI score 0-2).The use of this tool helps facilitate further delineationbetween low and intermediate risk chest pain patientsadmitted to the EDOU, with the end result being identifica-tion of those patients who would benefit from a moreaggressive work up and intervention.
Acknowledgments
REDCap (Research Electronic Data Capture).
References
[1] Lee TH, et al. Clinical characteristics and natural history of patientswith acute myocardial infarction sent home from the emergency room.Am J Cardiol 1987;60(4):219-24.
[2] McCarthy BD, et al. Missed diagnoses of acute myocardial infarctionin the emergency department: results from a multicenter study. AnnEmerg Med 1993;22(3):579-82.
[3] Rouan GW, et al. A chest pain clinic to improve the follow-up ofpatients released from an urban university teaching hospital emergencydepartment. Ann Emerg Med 1987;16(10):1145-50.
[4] Antman EM, et al. The TIMI risk score for unstable angina/non-STelevation MI: a method for prognostication and therapeutic decisionmaking. JAMA 2000;284(7):835-42.
[5] Conway Morris A, et al. TIMI risk score accurately risk stratifiespatients with undifferentiated chest pain presenting to an emergencydepartment. Heart 2006;92(9):1333-4.
[6] Bartholomew BA, et al. A population-based evaluation of thethrombolysis in myocardial infarction risk score for unstable anginaand non-ST elevation myocardial infarction. Clin Cardiol 2004;27(2):74-8.
[7] Hess EP, et al. Prospective validation of a modified thrombolysis inmyocardial infarction risk score in emergency department patients withchest pain and possible acute coronary syndrome. Acad Emerg Med2010;17(4):368-75.
[8] Pollack Jr CV, et al. Application of the TIMI risk score for unstableangina and non-ST elevation acute coronary syndrome to anunselected emergency department chest pain population. AcadEmerg Med 2006;13(1):13-8.
[9] Karounos M, et al. TIMI risk score: does it work equally well in bothmales and females? Emerg Med J 2007;24(7):471-4.
[10] Chase M, et al. Prospective validation of the Thrombolysis inMyocardial Infarction Risk Score in the emergency department chestpain population. Ann Emerg Med 2006;48(3):252-9.
[11] Campbell CF, et al. Combining Thrombolysis in Myocardial Infarctionrisk score and clear-cut alternative diagnosis for chest pain riskstratification. Am J Emerg Med 2009;27(1):37-42.
[12] Weisenthal BM, et al. Relation between thrombolysis in myocardialinfarction risk score and one-year outcomes for patients presenting atthe emergency department with potential acute coronary syndrome.Am J Cardiol 2010;105(4):441-4.
[13] Conti A, et al. Updated management of non-st-segment elevation acutecoronary syndromes: selection of patients for low-cost care: ananalysis of outcome and cost effectiveness. Med Sci Monit 2005;11(3):CR100-8.
[14] Cross E, How S, Goodacre S. Development of acute chest painservices in the UK. Emerg Med J 2007;24(2):100-2.
[15] Goodacre SW. Should we establish chest pain observation units in theUK? A systematic review and critical appraisal of the literature. JAccid Emerg Med 2000;17(1):1-6.
[16] Farkouh ME, et al. A clinical trial of a chest-pain observation unit forpatients with unstable angina. Chest Pain Evaluation in the EmergencyRoom (CHEER) Investigators. N Engl J Med 1998;339(26):1882-8.
[17] Wilkinson K, Severance H. Identification of chest pain patientsappropriate for an emergency department observation unit. Emerg MedClin North Am 2001;19(1):35-66.









![Review Interventional Cardiology · or Thrombolysis In Myocardial Infarction (TIMI) risk models in patients with suspected acute coronary syndrome (Class IIaB) [14]. The European](https://img.pdfslide.net/doc/110x75/5f22ebfe2e6de736c9603dd5/review-interventional-cardiology-or-thrombolysis-in-myocardial-infarction-timi.jpg)

![Role of ticagrelor in the treatment of coronary artery disease · Prasugrel–Thrombolysis in Myocardial Infarction 38 (TRITON–TIMI 38) study [10]. However, the higher level of](https://img.pdfslide.net/doc/110x75/5f8e3e6f18496b37da0ba95a/role-of-ticagrelor-in-the-treatment-of-coronary-artery-disease-prasugrelathrombolysis.jpg)


![ΠΤΡΟ Ν. ΠΑΠΑΪΩΑΝΝΟΤ MD. PHD. FESC · safety end point (Thrombolysis in Myocardial Infarction [TIMI] major bleeding not related to coronary-artery bypass grafting)](https://img.pdfslide.net/doc/110x75/5f765ace2664f83f9d7549d0/-md-phd-fesc-safety-end-point-thrombolysis.jpg)