Embed Size (px)
Citation preview

Protozoan Parasites:
Lecture 21 – Apicomplexans 3 Heteroxenous Coccidia - Part 1
Pages 37-49

“Tissue cyst”-forming Coccidia
• General Taxonomy – Apicomplexa
• Heteroxenous
– Two host life cycles
• Asexual & sexual reproduction
– Intestinal epithelium or sub- epithelium of a carnivore definitive host
• Asexual development also takes place in extra-intestinal tissues of the intermediate host
– “Tissue cysts”- forming coccidia

General Morphology
• Intestinal stages
• Same as for other coccidia merozoites, microgamonts, macrogamonts

General Morphology
• Extra-Intestinal stages
– General coccidian ‘zoite’ morphology
• Tachyzoites
– Crescent shaped, ~6 µm
• Proliferate rapidly forming colonies
• Bradyzoites
– Crescent shaped, ~7 µm
• Multiply slowly within tissue cysts
Bradyzoite within tissue cyst
Tachyzoite on blood smear

General Morphology
• Extra-Intestinal stages
• Tissue cysts
– Contain bradyzoites which divide slowly resulting in increasing sizes of tissue cysts
– Young tissue cysts 5 µm
– Older tissue cysts grow to 50 µm

Toxoplasmosis
• Toxoplasma gondii
– World wide distribution
• Definitive host
– Cats & other felids
• Intermediate host
– Indiscriminate
– Any warm blooded animal
• mammals or birds

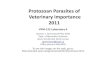
Toxoplasma gondii: Life Cycle
1-5 days to mature = sporulate
Cats Ingesting bradyzoites produce millions of oocysts = most important mode of transmission to definitive host
Few oocysts Produced from ingesting tachyzoites
20% of cats ingesting oocysts develop a patent infection - few oocysts
Dubey 1998

Jones et al. 2003

Prevalence
• Cats: – North America ~ 30%
– Spain ~ 45%
– Japan ~ 6%
• Humans: – North America - 15-23%
– Veterinary staff (Ontario 2002) - 14.2%
– U.K. - 30%
– France - 80%
– New Zealand - 60%
– BUT all are dropping…
• Other animals: – Variable seroprevalences

Pathogenesis & Clinical signs
Cats - definitive host
• Intestinal phase – Young cats
• Shed oocysts - intense & brief
• No pathology, no clinical signs
• Extra-intestinal phase – Kittens (< 3 months)
– Rarely in older cats
– Common clinical signs - Anorexia, depression, lethargy, icterus, vomiting
– Less common signs – pneumonia, encephalitis & chorioretinitis
– Death in severe cases (rare)

Pathogenesis & Clinical signs
Intermediate hosts
• Two types of disease:
– Acquired Toxoplasmosis
– Congenital Toxoplasmosis

Acquired Toxoplasmosis
Domestic animals • Sheep & Goats
– Mild febrile response
• Cattle & Horses – Clinical signs rare
• Swine – Clinical signs rare
• Dogs – Clinical signs rare – BUT when occur
• Young dogs <1 year old • Myositis & muscle atrophy • CNS signs - ataxia, tremors, uveitis

Acquired Toxoplasmosis
Humans – Zoonosis
• Healthy people:
– Most have no clinical signs
• Mild clinical signs – Flu-like symptoms
– Transient headache, muscle & joint pain, fatigue, swollen lymph nodes
• “Once infected forever protected” – But this may not be true anymore…

Acquired Toxoplasmosis
Humans – Zoonosis
• Immunodeficient people:
– Severe disease
• Pneumonia, myocarditis, encephalitis, chorioretinitis, fatigue, swollen lymph nodes
• Reactivated latent infection...

Congenital Toxoplasmosis
• Most serious form of disease
• Major concern
– Humans
– Sheep > goats
• Primary maternal infection acquired during pregnancy for transmission to placenta / fetus

Congenital Toxoplasmosis
Sheep > Goats
• Major cause of abortion
– Fetus may be mummified, macerated, autolyzed or resorbed
– Fetal lesions in heart, brain & liver

Congenital Toxoplasmosis
Sheep > goats
• Focal inflammation & necrosis within the placenta
– Small (~2 mm) white chalky lesion
– Tachyzoites & tissue cysts
• Subsequent pregnancy
– Abortions are rare
– Ewe develops immunity • Normal pregnancy

Congenital Toxoplasmosis
Humans – Zoonosis • Abortion rare
• Premature birth common
– At birth: “Classic triad”
• Chorioretinitis, hydrocephalus, intracranial calcification
• Later in life
– Mental illness, blindness, epilepsy ...
• Asymptomatic
– No clinical signs
– Reactivated latent infections...

Diagnosis
• Definitive host: Cats
• Centrifugal Fecal flotation
– Cats shed oocysts
• sporadic & inconsistent
• confounders Hammondia & Besnoitia sp.
• Toxoplasma Reference Lab
– ELISA & PCR

Diagnosis • Serology • Valuable in Humans > Sheep but less value in cats… • Cats Acute infection
– Elevated IgM titres with low/normal IgG – Greatest risk to shed oocysts
• Chronic/Previous infection – Low IgM titres & higher IgG – Less likely to shed oocysts
• Assessing human health risk • Seronegative cat: not likely currently shedding but will shed if exposed.
– This cat is the greatest risk to human health. • Seropositive cat: probably not shedding oocysts (see above acute vs.
chronic) & is less likely to shed oocysts if re-exposed or immunosuppressed. – Still recommended that potential exposure to oocysts (infected
intermediate hosts) be minimized.

Toxoplasmosis Treatment
Humans – Congenital
• Mother & child
– Acquired / Reactivated • Immunodeficient
– Pyrimethamine & sulphadiazine &/or spiramycin with folinic acid
Animals – Rare to treat livestock – Common to treat companion animals – Pyrimethamine & sulphadiazine,
clindamycin, azithromycin

Prevention & Control
Cats : – Prevent hunting & scavenging – Keep cats indoors – Do not feed raw or undercooked meat
&/or unpasteurized dairy – Seronegative cat is a risk to humans if
infected – Seropositive cat less risk to humans
• Unless shedding now = risk • If not shedding = less risk
Domestic Animals: – Prevent cats defecating in feed & water – Control cat population on farm – Toxovax® in sheep / goats
• One dose = lifetime protection (New Zealand & UK)

Prevention & Control Humans – Zoonosis • What can you do?
– Do not eat meat • Uncooked or rare
– Pasteurized dairy products only – Empty litter box daily - gloves, spouse? – Gardening - wear gloves – Wash vegetables & fruit – Proper hygiene – hand washing – Starting a family?
• Contact you health professional and have a conversation…
• Remember Dogma of – “Once infected forever protected” may not be
true anymore…

?

Neosporosis
• Neospora caninum
• Fatal neuromuscular disease of dogs
• Major cause of reproductive failure & abortion in cattle

Morphology
• All stages identical to Toxoplasma except the tissue cysts – Neospora tissue cysts are
found only in the CNS, peripheral nerves & retina
– Toxoplasma tissue cysts thin walls (< 1 µm)
– Neospora tissue cysts thick walls (>1 µm & up to 4 µm)

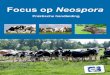
Neospora life cycle
#’s correspond to clinical signs, please see later slides 41-43
1
2 & 3
4

Epidemiology
Transmission
• Percentage of dogs/canids shedding oocysts is unknown
• Congenital transmission occurs in dogs, cattle, sheep, goats, pigs, horses cats, mice, monkeys...birds too!
– No evidence of zoonosis
• Repeated congenital transmission may occur & can occur over several generations

Epidemiology
Prevalence – Common cause of
abortion in beef & dairy cattle worldwide
– Serologic surveys – cattle • Up to 100% of cattle
have been exposed in some herds
• Maritime dairies - 73% of herds & 19% of cows found to be positive
• UK ~ 35% of abortions

Epidemiology
Prevalence
– Seroprevalence in dogs
• Variable
• Higher rates in dogs on dairy farms vs. dogs from urban areas
• Most clinical cases occur in congenitally infected young dogs

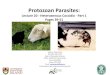
Pathogenesis
• Similar to toxoplasmosis
– Destruction of host cells by tachyzoites resulting in focal areas of necrosis
– Focal encephalitis, encephalomyelitis, myositis & myocarditis characterized by necrosis & non-suppurative inflammation
http://www.visionveterinaria.com/rivep/art/09jun43.htm

Clinical signs
Cattle – Abortion is major clinical
sign (2) • Cows of any age can abort
between 3 months gestation & term
• Most abortions around 5-6 months
• Fetus may die in utero, be resorbed, mummified, autolyzed or stillborn

Clinical signs
Cattle
– Infected calves born alive (3)
• Neurological signs – Ataxia, decreased patellar reflexes
& exophthalmia
• Underweight, downer, hind limbs &/or forelimbs flexed or hyper extended

Clinical signs
Cattle
– Calves may also be born infected without clinical signs (1)
• Persistent infection
– Risk to next generation
– Calves may also be born free of infection (4)
• Cycle is broken

Clinical signs
Neosporosis in Dogs – Subclinical infection is common – Clinical disease
• Young dogs 3 weeks to < 6 months • Rigid hyper-extended limbs & hind limb
paresis - paralysis • Paralysis of the jaw with difficulty swallowing • Muscle flaccidity, muscle atrophy, heart
failure • Severe dermatitis • Worst case - all above + cervical weakness,
dysphagia, megaesophagus...death
– Litter mates are often infected – Older dogs less common

Diagnosis
Cattle • Fetal tissues - brain, heart, liver,
lungs – Tissue cysts – Lesions
• Focal areas of necrosis • Non-suppurative inflammation
– Immunohistochemistry – IHC • Neospora vs. Toxoplasma tachyzoites
– Fetal fluids & serum of cows • Antibody titre - IFAT, ELISA, DAT http://www.visionveterinaria.com/
rivep/art/09jun43.htm

Diagnosis
Dogs • Antibodies - serum or CSF • Litter mates with clinical signs
– Congenital neosporosis
• Gross lesions – Ulcerative dermatitis – Necrosis of CNS – Yellowish-white streaks in muscles
• IHC, ELISA...? • Centrifugal Fecal flotation
– Sporadic & inconsistent shedding – confounder species
• Hammondia &Toxoplasma

Treatment & Control
Cattle • Protect feed & water sources
from contamination
• Do not let dogs eat fetal membranes, fetuses or dead calves
• Cow that aborts once may abort again (persistent infection) & may have to be culled
• No treatment for livestock
• Vaccine but no efficacy data?

Treatment & Control
Dogs • Prevent canids from eating fetal membranes, fetuses or dead
calves by proper disposal
• Treatment may be attempted with sulfonamides, pyremethamine & clindamycin
• Treat all littermates
• No therapy to Tx “doggie mothers” to prevent transmission

VPM-122 Midterm Exam # 3
• Thursday, March 23, 2017
• Lecture 286A N/286B N/286C N/287N
• 0830-0920H
• Covers my lectures (#17-22)
• Lecture 23 is a review (20/03/2017)
• Protozoan Parasites lecture notes pages, 1-54.
• Format – Multiple choice, short answer & essay
– Point form is okay for answers...including the essay!!!!!
– Say no to drugs & no drug names on exam either!
– No prevalence numbers