Embed Size (px)
Citation preview
Pseudomonas and related organisms
Aerobic gram-negative nonfermentative rods
Pseudomonas aeruginosa: opportunistic infections of multiple sites
Burkholderia cepacia: RT infection in cystic fibrosis patients, UTI, opportunistic infections
Burkholderia pseudomallei: opportunistic pulmonary infections or sepsis
Stenotrophomonas maltophilia: opportunistic infections
Acinetobacter baumannii: opportunistic infections of RT
Moraxella catarrhalis: opportunistic RT infections
Pseudomonas
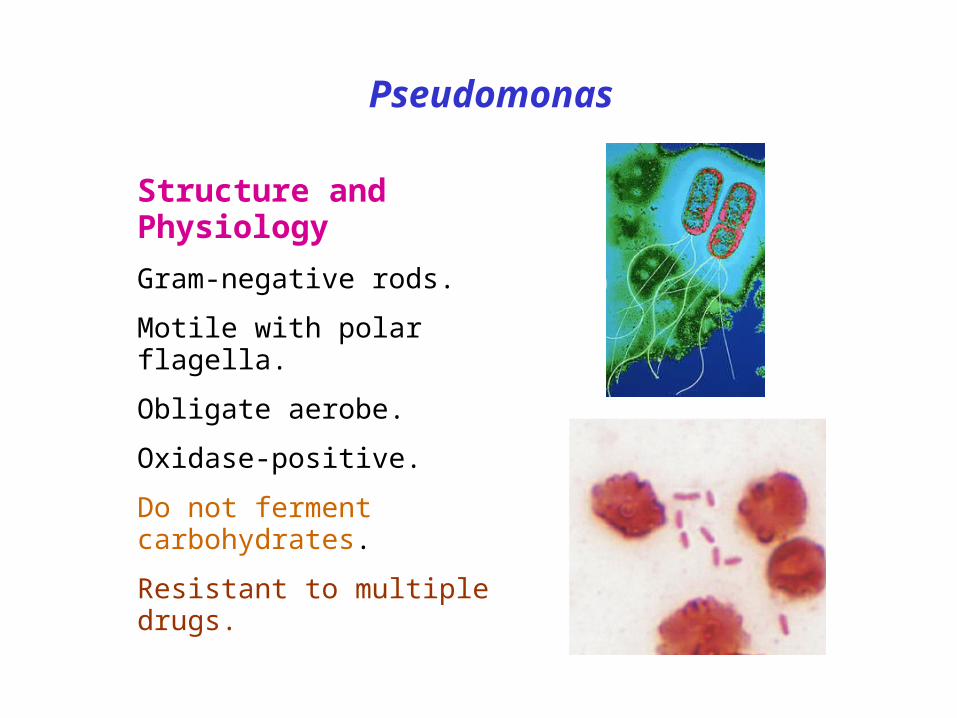
Structure and Physiology
Gram-negative rods.
Motile with polar flagella.
Obligate aerobe.
Oxidase-positive.
Do not ferment carbohydrates.
Resistant to multiple drugs.
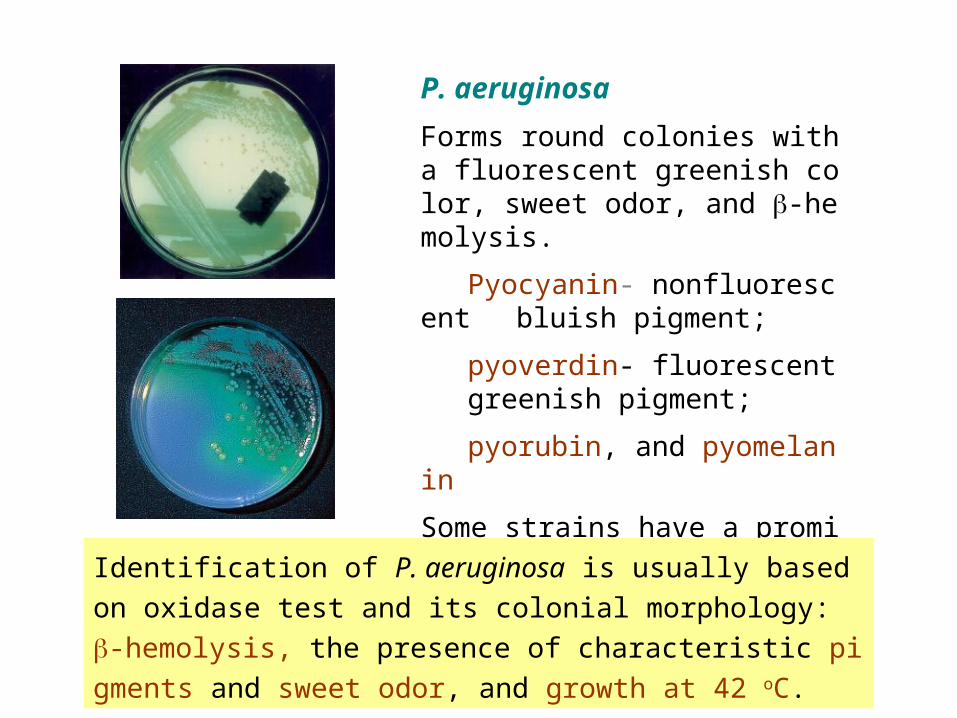
P. aeruginosa
Forms round colonies with a fluorescent greenish color, sweet odor, and -hemolysis.
Pyocyanin- nonfluorescent bluish pigment;
pyoverdin- fluorescent greenish pigment;
pyorubin, and pyomelanin
Some strains have a prominent capsule (alginate).
Identification of P. aeruginosa is usually based on oxidase test
and its colonial morphology: -hemolysis, the presence of cha
racteristic pigments and sweet odor, and growth at 42 oC.
P. aeruginosaPathogenesis and Immunity
This organism is widely distributed in nature and is commonly present in moist environments in hospitals. It is pathogenic only when introduced into areas devoid of normal defenses, e.g.,
1. Disruption of mucous membrane and skin.
2. Usage of intravenous or urinary catheters.
3. Neutropenia (as in cancer therapy).
P. aeruginosa can infect almost any external site or organ.
P. aeruginosa is invasive and toxigenic. It attaches to and colonizes the mucous membrane or skin, invade locally, and produces systemic diseases and septicemia.
P. aeruginosa is resistant to many antibiotics. It becomes dominant when more susceptible bacteria of the normal flora are suppressed.
P. aeruginosa
Antigenic structure, enzymes, and toxins
Pili and nonpilus adhesins.
Capsule (alginate, glycocalyx): seen in cultures from patients with cystic fibrosis.
LPS- endotoxin, multiple immunotypes.
Pyocyanin: catalyzes production of toxic forms of oxygen that cause tissue damage. It also induces IL-8 production. Pyoverdin: a siderophore.
Proteases
Serine protease, metallopr
otease andalkaline proteasecause tissue damage and help
bacteria spreadPhospholipase C: a hemolysin
Exotoxin A: causes tissue necrosis and is lethal for animals (disrupts protein synthesis); immunosuppressive.
Exoenzyme S and T: cytotoxic to host cells.
Pathogenesis
P. aeruginosa
Infection of wounds and burns (blue-green pus). Patients with severe burns may develop into bacteremia.
Skin and nail infections
Meningitis (when introduced by lumbar puncture).
Pulmonary infection
Tracheobronchitis
Necrotizing pneumonia in CF patients: diffuse, bilateral bronchopneumonia with microabscess and necrosis.
Eye infections: corneal ulcer.
Ear infections
Otitis externa: mild in swimmers; malignant (invasive) in diabetic patients.
Chronic otitis media
Osteochondritis of the foot.
Urinary tract infection
Sepsis: most cases originate from infections of lower RT, UT, and skin and soft tissue. Ecthyma gangrenosum (hemorrhagic
necrosis of skinmay be seen in some patients.
Clinical Diseases
Laboratory Diagnosis
Specimen: skin lesions, pus, urine, blood, spinal fluid, sputum.
Culture: blood agar plate and differential media. Identification of P. aeruginosa is described above.
Several subtyping methods, including phage typing and molecular typing, are available for epidemiologic purposes.
Treatment
Combined antibiotic therapy is generally required to avoid resistance that develops rapidly when single drugs are employed. Avoid using inappropriate broad-spectrum antibiotics, which can suppress the normal flora and permit overgrowth of resistant pseudomonads.
P. aeruginosa
P. aeruginosaPrevention and Control
Pseudomonas spp. normally inhabit soil, water, and vegetation and can be isolated from the skin, throat, and stool of healthy persons.
Spread is mainly via contaminated sterile equipments and cross-contamination of patients by medical personnel.
High risk population: patients receiving broad-spectrum antibiotics, with leukemia, burns, cystic fibrosis, and immunosu
ppression.
Methods for control of infection are similar to those for other nosocomial pathogens. Special attention should be paid to sinks, water baths, showers, hot tubs, and other wet areas.
P. aeruginosa
Prevention and Control
Control:
1. Patients at high risk should not be admitted to a ward
where cases of pseudomonas infection are present.
2. Patients infected with P. aeruginosa should be
isolated.
3. Sterilize
all instruments, apparatus, and dressing;
antimicrobial and other therapeutic substances.
4. Monitor clinically relevant isolates of P. aeruginosa by
a suitable typing system to identify epidemic strains.
Stenotrophomonas maltophiliaA common nonfermentative, gram-negative isolate.
It infects debilitated or immunocompromised persons,
and causes a wide spectrum of diseases, including wo
und infections, UT infections, pneumonia, sepsis, men
ingitis, etc.
It is resistant to many commonly used antibiotics, and
patients receiving long-term antibiotic therapy are parti
cularly at risk for acquiring infections.
Infections may be acquired from iv catheters, contami
nated disinfectants, respiratory therapy and monitoring
equipment, and ice machines.
BurkholderiaThey colonize the moist environmental surfaces and are commonl
y associated with nosocomial infections.
B. cepacia complex (of 9 species), B. gladioli and B. pseudomallei
are important pathogens.
B. cepacia complex causes RT infections particularly in cystic fibr
osis patients, UT infections and septicemia. Usually non-fatal exc
ept for RT infections in CF patients.
B. pseudomallei usually causes opportunistic infections (called m
elioidosis, but may sometimes infect previously healthy persons.
Infection by this organism may result in asymptomatic infection, a
cute suppurative cutaneous infection, and chronic pulmonary infe
ction ranging in severity from mild bronchitis to necrotizing pneum
onia. All may progress to sepsis.
2005/7/30 台南高雄疑似發生類鼻疽疫情,疾病管制局提醒民眾,皮膚如有傷口,請勿接觸污染的土壤或水源
疾病管制局今天公佈今年自七月 11 日至 29 日以來,類鼻疽累計通報 16 例,其中高雄縣 9 例、台南市 4 例、高雄市 2 例、台南縣 1 例。其中 6 例死亡, 3 例在加護病房,另 7 例住普通病房。類鼻疽係由類鼻疽伯克氏菌 Burkholderia pseudomallei 所造成的臨床感染症,屬假單孢菌屬革蘭氏陰性桿菌,此菌在土壤、水池及積水環境中存在,會感染馬、羊、豬等動物以及人類。其流行地域為東南亞地區及澳洲北部的熱帶地域。該局自 89 年即將此病納入監測。 89 年通報病例 1例、 90 年 15 例、 91 年 9例、92 年 5例、 93 年 13 例。本次疫情發生原因,疾病管制局初步調查研判可能係因日前南部豪大雨,將土壤中之病菌沖刷出來,所造成的民眾感染事件,病例多發生在二仁溪流域。該局鄭重呼籲在二仁溪流域附近居民,若有發燒等症狀者,務必迅速就醫。並告訴醫師居住地區,疾病管制局呼籲,醫師對於上述地區發燒病患,應先排除感染此病的可能性,若有懷疑應立即以抗生素治療,並採檢送驗。
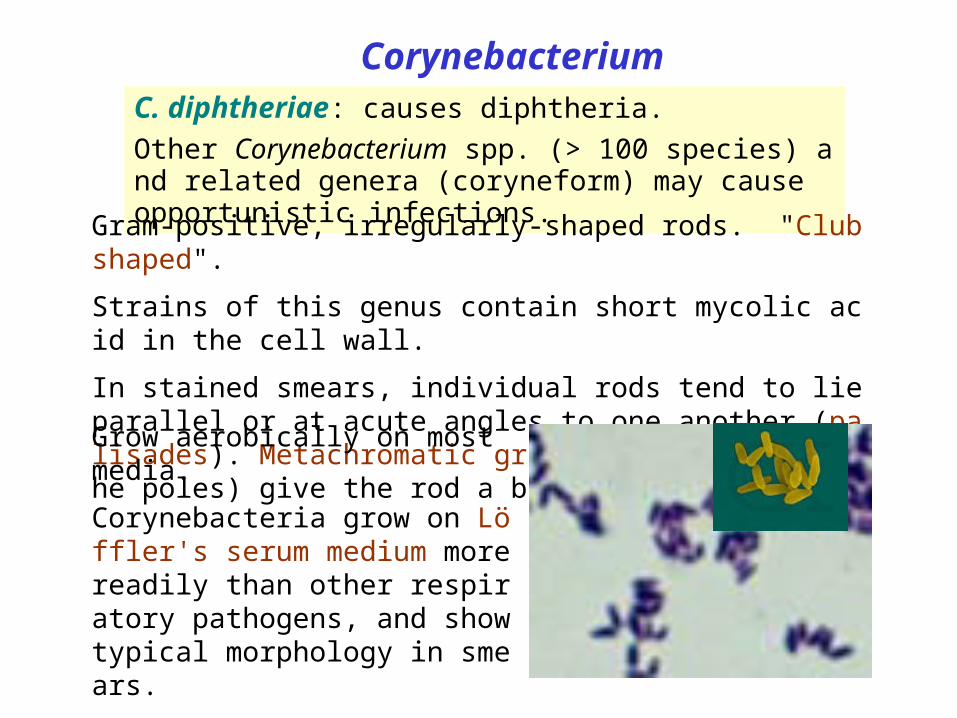
CorynebacteriumC. diphtheriae: causes diphtheria.
Other Corynebacterium spp. (> 100 species) and related genera (coryneform) may cause opportunistic infections.
Gram-positive, irregularly-shaped rods. "Club shaped".
Strains of this genus contain short mycolic acid in the cell wall.
In stained smears, individual rods tend to lie parallel or at acute angles to one another (palisades). Metachromatic granules (often near the poles) give the rod a beaded appearance.
Grow aerobically on most media.
Corynebacteria grow on Löffler's serum medium more readily than other respiratory pathogens, and show typical morphology in smears.
Non-motile; noncapsulate.
C. diphtheriaePathogenesis and Immunity
C. diphtheriae occurs in the respiratory tract, in wounds, or on the skin of infected persons or normal carriers. It is spread by droplets or skin contact.
Portal of entry: respiratory tract or skin abrasions.
Diphtheria bacilli colonize and grow on mucous membranes, and start to produce toxin, which is then absorbed into the mucous membranes, and even spread by the bloodstream.
Local toxigenic effects: elicit inflammatory response and necrosis of the faucial mucosa cells-- formation of "pseudo-membrane“ (composed of bacteria, lymphocytes, plasma cells, fibrin, and dead cells), causing respiratory obstruction.
Systemic toxigenic effects: necrosis in heart muscle, liver, kidneys and adrenals. Also produces neural damage.
C. diphtheriaeClinical Diseases
Respiratory diphtheria
Incubation period: 2-4 days.
Inflammation begins in the respiratory tract, causing sore throat, exudative pharyngitis that develops into pseudomembrane, and low grade fever. Prostration and dyspnea soon follow, which may lead to suffocation if not promptly relieved by intubation or tracheotomy.
Myocarditis causing cardiac arrhythmias develops in many patients.
Visual disturbance, difficulty in swallowing and paralysis of the arms and legs also occur but usually resolve spontaneously.
Death may be due to asphyxia or heart failure.
Cutaneous diphtheria: mild (papule ulcer with grayish membrane) with little toxigenic effects. Stimulates antitoxin production.
C. diphtheriaeLaboratory DiagnosisSpecific treatment should be given before the lab reports if the clinical picture strongly suggests diphtheria.
Specimens: swabs from the nose, throat or suspected lesions.
Gram's stain: beaded rods in typical arrangement (unreliable).
Culture: inoculate specimen onto a blood plate, and a selective medium like cysteine-tellurite blood plate. Identification: biochemical tests.
Toxigenicity test:
1. Tissue culture neutralization assay.
2. in vitro test: immunodiffusion assay (Elek test ).
3. Detection of toxin gene by PCR.
C. diphtheriae
Treatment
Treatment of diphtheria rests on prompt ad
ministration of antibiotics (penicillin or eryth
romycin) and diphtheria antitoxin.
Maintenance of an open airway.
Vaccination of recovered patients with toxoi
d is required because most patients fail to
develop antitoxin antibodies.
C. diphtheriae
Prevention and Control
Humans are the only known reservoir of C. diphtheriae.
Diphtheria was mainly a disease of small children.
This organism is maintained in the oroparynx or skin of as
ymptomatic carriers.
The bacteria are spread directly from person to person.
To limit contact with diphtheria bacilli to a minimum, patien
ts with diphtheria should be isolated.
Prophylactic antibiotic treatment to unimmunized contacts.
Active immunization in childhood with diphtheria toxoid (fromalin-i
nactivated toxin) yields antitoxin levels adequate until adulthood.
All children must receive an initial course (2, 4, and 6 months) of i
mmunizations and boosters (18 months and 6 years).
Regular booster with Td (tetanus and diphtheria) toxoids are parti
cularly important for adults who travel to developing countries.
Vero cell neutralization test can be used to measure antitoxin anti
bodies in serum.
C. diphtheriaePrevention and Control
Toxoids for delayed absorption: Fluid toxoid absorbed onto aluminum hydroxide or aluminum phosphate. Usually combined with tetanus toxoid and pertussis vaccine (DPT vaccine).
Other Corynebacterium Species
They are ubiquitous in plants and animals. Many are found as part of human normal flora on the skin and mucosal surfaces, and may cause opportunistic infections in hospitalized or immunocompromised patients.
C. jeikeium and C. amycolatum: sepsis, endocarditis, wound infections, foreign body infections, pneumonia, and UT infections.
C. urealyticum causes UT infections. It is a strong urease producer, infection of UT may lead to formation of stones.
Some strains of C. ulcerans and C. pseudotuberculosis may produce diphtheria toxin and cause diphtheria.
Resistant to many antibiotics. Treatment of bacteremia or endocarditis must be guided by antibiotic susceptibility tests.
Listeria and Erysipelothrix
Structure and Physiology of Listeria
Small gram-positive coccobacilli; facultative anaerobe.
Motile at room temperature but less so at 37 oC.
-hemolytic (weak)
Grow on most conventional media in a wide pH and
temperature range (1 oC to 45 oC).
L. monocytogenes: meningitis and bacteremia
E. rhusiopathiae: erysipeloid (a zoonotic disease)
L. monocytogenesPathogenesis and Immunity
Widely distributed in nature (soil, water, vegetation, and the intestines of a variety of animals). Fecal carriage in healthy people: 1%-5%.
Human disease is rare and is restricted to neonates and the elderly, pregnant women, and immunocompromised patients (particularly those with defective cell-mediated immunity, such as AIDS patients).
Infection is initiated in the intestine.
Facultative intracellular pathogen. The intracellular survival and spread of the bacteria are critically important in pathogenesis and, therefore, cellular immunity is more important than humoral immunity in host defense against this organism.
Neonates
Early onset disease (acquired tr
ansplacentally in utero): granulo
matosis infantiseptica, with diss
eminated abscesses and granul
omas in multiple organs.
Late onset disease (acquired at
or soon after birth): meningitis or
meningoencephalitis with septic
emia, similar to that caused by g
roup B streptococci.
Adults
Infection in healthy adults: asymptomatic or mild influenza-like illness; gastrointestinal symptoms in some patients.
Meningitis; primary bacteremia with chills and fever; high fever and hypotension in severe cases. Maybe fatal. (High risk: organ transplant patients, cancer patients, pregnant women)
Clinical Diseases
L. monocytogenes
Laboratory Diagnosis
Specimen: CSF and blood.
Gram stain: CSF typically show no Listeria because of the low bacterial concentration.
Culture
Listeria grows on most conventional media.
Selective media and cold enrichment are used for specimens contaminated with rapidly growing bacteria.
Hemolysis (CAMP-positive) and motility in liquid or semisolid medium are useful for preliminary
identification.
Identification
Biochemical and serological tests (13 serotypes).
L. monocytogenes
Treatment, Prevention, and Control
L. monocytogenes is resistant to multiple antibiotics (e.g., cepha
losporin and tetracycline). Currently, gentamicinwith eitherpenicillin or ampicillin is the treatment of choice.
Outbreaks have been associated with the consumption of contaminated milk, soft cheese, undercooked meat, unwashed raw vegetables, and cabbage. Refrigeration of contaminated food products permits the slow multiplication of the organisms to an infectious dose.
Because Listeria organisms are ubiquitous and most infections are sporadic, prevention and control are difficult. High risk people should avoid eating raw or partially cooked foods.
L. monocytogenes
Erysipelothrix (Hair of red disease)E. rhusiopathiae
Slender gram-positive, microaerophilic, with a tendency to form filaments. Form small, grayish -hemolytic colonies after 2 to 3 days incubation.
Widely distributed in wild and domestic animals. Animal disease (particularly in swine) is widely recognized, but human disease is uncommon.
Causes zoonotic infections through an abrasion or wound:
Localized skin infection (erysipeloid): 1-4 day incubation; painful and pruritic, slowly spreading inflammatory skin lesions on the fingers or hands, violaceous with raised edge. Suppuration is uncommon.
Diffuse cutaneous infection: rare and often associated with systemic manifestation.
Septicemia: uncommon and frequently associated with endocarditis.
Erysipelothrix
Penicillin is the antibiotic of choice.
Specimen: full-thickness biopsy specimens or deep aspirates (because the bacteria locate only on deep tissues).
Culture: grow on most conventional media in the presence of 5%-10% CO2.
Identification
Motility- and catalase-negative.
Biochemical tests.
People at occupational risk (butchers, meat processors, farmers, poultry workers, fish handlers, and veterinarians) are prevented by use of gloves and other coverings on exposed skin.
Vaccination is used to control disease in swine.
Bacillus
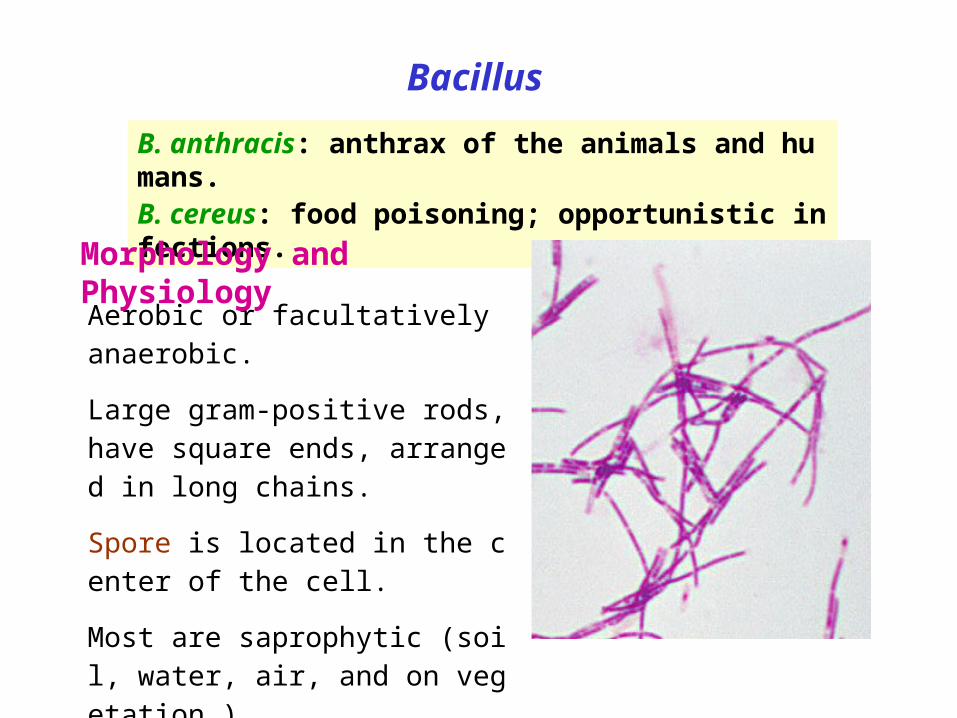
B. anthracis: anthrax of the animals and humans.B. cereus: food poisoning; opportunistic infections.
Aerobic or facultatively anaerobic.
Large gram-positive rods, have square ends, arranged in long chains.
Spore is located in the center of the cell.
Most are saprophytic (soil, water, air, and on vegetation.)
Morphology and Physiology
B. anthracis
B. anthracis is encapsulated and non-motile.
The capsule consists of polypeptide (poly-D-glutamic
acid) and is an important virulence factor.
The spores can withstand dry heat and certain disinfec
tants for moderate periods, and persist for years in dry
earth. Animal products contaminated with anthrax spo
res can be sterilized only by autoclaving.
Physiology and Structure
B. anthracis
Primarily a disease of herbivores (sheep, cattle, horses);
humans are rarely affected.
Being used by the terrorists as a biological warfare.
In animals, portal of entry is mouth and GI tract. In humans, scra
tches in the skin (95% of infection), ingestion or inhalation lead t
o infection. Inhalation is the most likely route for infection with bi
ological warfare (LD50: 2,500-55,000).
The spores germinate in the tissue at the site of entry, and grow
th of the vegetative forms results in gelatinous edema and cong
estion. Bacillus spread via lymphatics to the blood and other tis
sues.
Pathogenesis and Immunity
B. anthracis
Virulence factors
Capsule (encoded from a plasmid)
Exotoxins (A-B toxins encoded from another plasmid)
Edema toxin is composed of protective antigen (B-subunit) and edema factor (EF; an adenylate cyclase). This toxin complex increases vascular permeability which leads to shock.
Lethal toxin is composed of protective antigen and lethal factor (LF; a metalloprotease). This toxin causes cell death and stimulates macrophages to release proinflammatory cytokines.
Pathogenesis and Immunity
B. anthracis
Cutaneous anthrax (malignant pustule): develops in 12-36 hours. The papule rapidly changes into a vesicle, then a pustule, and finally a necrotic eschar. The infection may disseminate, giving rise to septicemia.
Inhalation anthrax (wool-sorters’ disease): long incubation time (2 months or more). Mediastinitis (enlargement of mediastinal lymph nodes), sepsis, and meningitis (50% patients). Pulmonary disease rarely develops.
Gastrointestinal anthrax (very rare): symptoms vary depending on the sites of infection. Can result in ulcers in the mouth and esophagus, or abdominal pain, vomiting and bloody diarrhea. Both rapidly progress to septicemia with a mortality that can be 100%.
Clinical Diseases
B. anthracis
Specimens: fluid or pus from local lesion, blood, or sputum.
Smears: long chains (a characteristic of B. anthracis) of large gram-positive rods without spores can be seen. Immuno-fluorescence stain can be used for dried smears.
Culture: nonhemolytic gray colonies with dry “ground glass” surface on blood agar plates (“Medusa head” morphology: irregular edges with projections).
Identification: made in a reference lab by direct fluorescent Ab test against capsular polypeptide or PCR test.
Serological tests: detection of antibodies to lethal toxin and edema toxin.
Laboratory Diagnosis
B. anthracis
Sensitive to penicillin but resistant to sulfonamides and cephalosporins. Combined antibiotic treatment is used for penicillin- and doxycycline-resistant strains.
Treatment
Control
Proper disposal of animal carcasses (burning or deep burial in lime pit).
Autoclaving of animal products.
Protective clothing and gloves for handling infected animals.
Vaccination of domestic animals.
Immunization of persons at high risk with a cell-free vaccine based on the protective antigen is under investigation.
B. cereus and other bacillus speciesUbiquitous organisms; primarily opportunistic pathogens.
B. cereus: the most important among them.
Noncapsulated and motile, causing
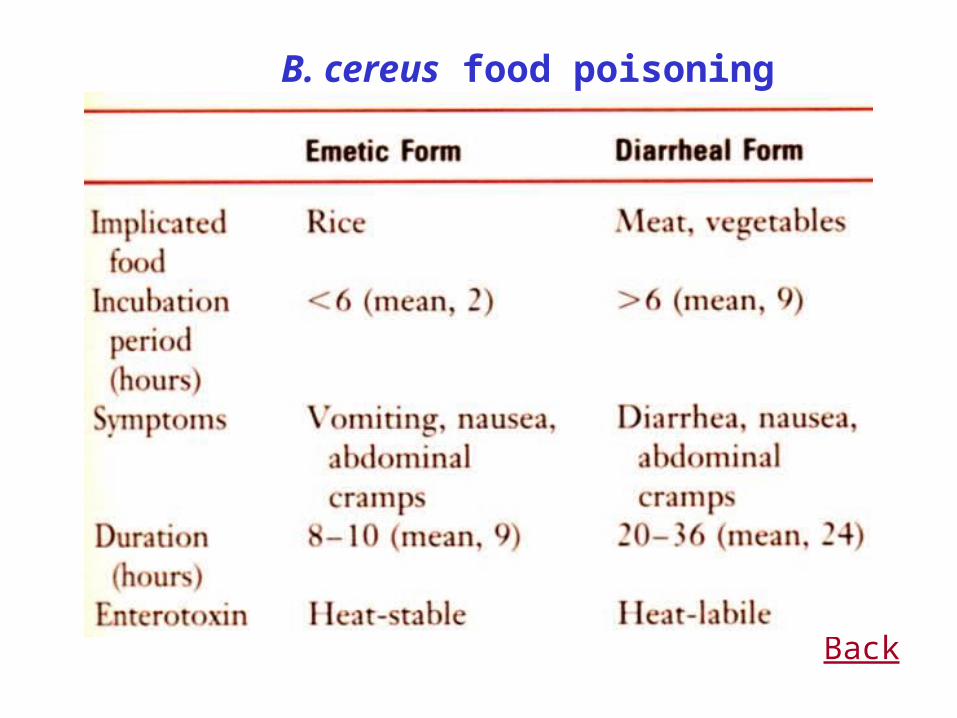
gastroenteritis: emetic form and diarrheal form.
ocular infections: acute panophthalmitis occurs after traumatic, penetrating injuries of the eye with a soil-contaminated object. A variety of toxins are involved.
intravenous catheter-related sepsis.
Other infections: endocarditis, pneumonitis, sepsis, meningitis, etc. in immunosuppressed patients.
Symptomatic treatment is adequate for B. cereus gastroenteritis. The treatment of other Bacillus is complicated because the course is rapid and progressive and they are resistant to multiple drugs.
Food poisoning can be prevented by quick consumption and proper storage of food.


Back
B. cereus food poisoning
Back
Diphtheria toxin is an A-B toxin expressed from a te
mperate phage (-phage) in the presence of low iron c
oncentrations.
This toxin binds to a receptor (heparin-binding epider
mal growth factor) on the surface of many eukaryotic c
ells, particularly heart and nerve cells, and results in in
hibition of polypeptide chain elongation by ribosylation
of the elongation factor EF-2.
It can induce protective antibodies (antitoxin).
Back
Back
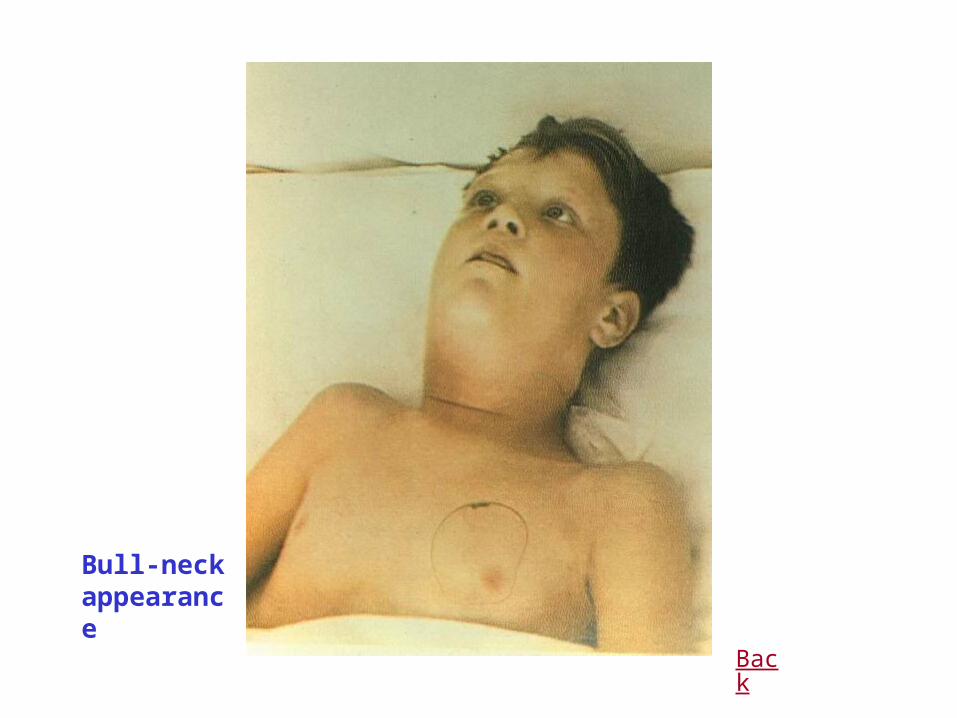
Bull-neck appearance

Back
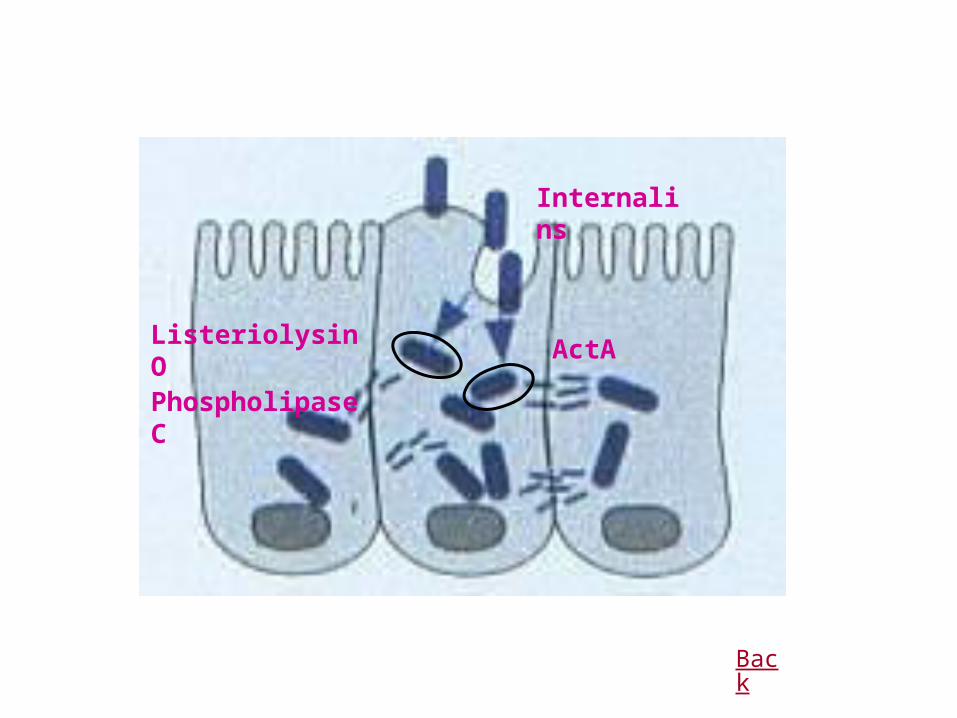
Listeriolysin OPhospholipase C
Internalins
ActA
Back
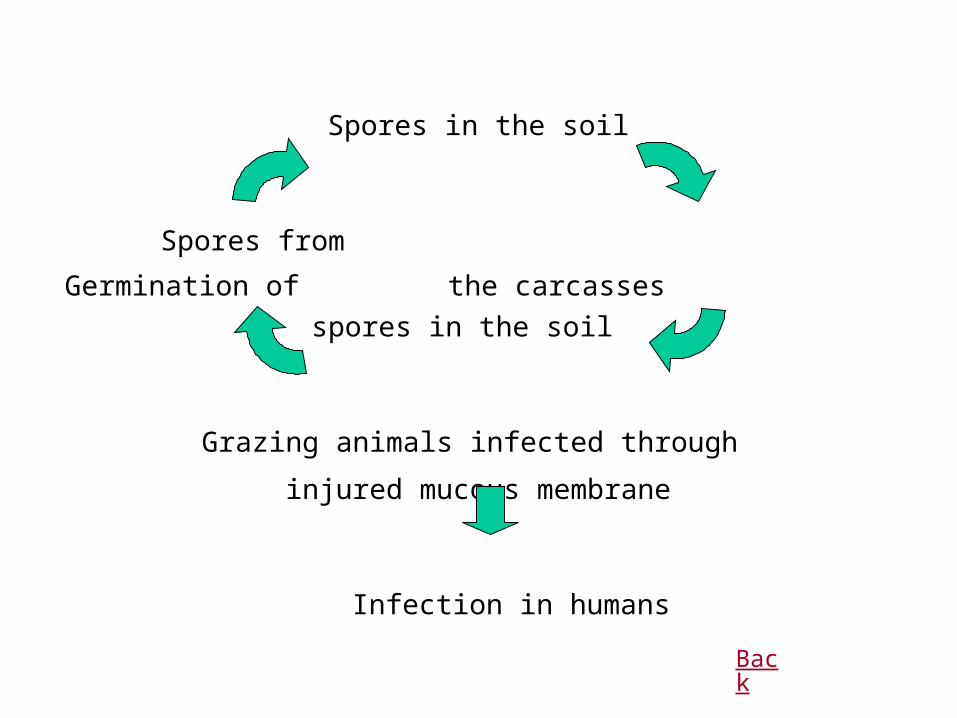
Spores in the soil
Spores from Germination of
the carcasses spores in the soil
Grazing animals infected through
injured mucous membrane
Infection in humans
Back





























