Embed Size (px)
Citation preview

Psychotherapy Volume 33/Fall 1996/Number 3
SIMILARITIES IN RESPONSES TO EXTREME ANDUNREMITTING STRESS: CULTURES OF COMMUNITIES
UNDER SIEGE1
A. STEVEN FRANKEL2 TODD C. O'HEARNUniversity of Southern California
National Treatment Center for Traumatic and Dissociative Disorders
During World War II, eastern Europeanghettos served to contain and oppressghetto residents. The organizationalstructures and processes that emergedwithin the ghetto are directly analogousto those in patients with DissociativeIdentity Disorder (DID, formerly MPD).This article explores the analoguesbetween ghetto organization and theinternal worlds of DID patients. ComplexDID patients, like ghetto residentssubjected to extreme and unremittingstress, develop homeostatic systemscharacterized by competing forces thatserve agendas of help-seeking,communication to outsiders aboutatrocities and utilitarian efforts toprevent destabilization. The ghettoanalogue to DID is offered as adescriptive teaching device for bothclinicians and patients.
1 The authors ate indebted to the following individuals andagencies for their assistance at various stages in preparationof this article: Aaron Breitbart, Kevin Connors, Rabbi GilKollin, Walter Young, the Simon Wiesenthal Center for Holo-caust Studies and the U.S. Holocaust Museum.
Correspondence regarding this article should be addressedto A. Steven Frankel, 2537D Pacific Coast Highway, Suite389, Torrance, CA 90505.
2 This article is based on presentations by the first authorto the 11th International Conference on Dissociative States,Chicago, 11/4/94 and to the 102nd Annual Convention of theAmerican Psychological Association, Los Angeles, 8/15/94.
This is the first of two articles which presenta metaphoric view of the internal world of patientswith Dissociative Identity Disorder (DID, for-merly MPD).3 DID is generally believed to de-velop primarily in children who are both high inhypnotic capacity and exposed to extreme andon-going abuse (see Putnam, 1989; Ross, 1989).These children are seen has developing alternatepersonalities in order to contain the physical andemotional pain as well as the memory of abuseexperiences.
This article describes the development and de-scriptive value of the metaphor, while the secondis concerned with treatment of the disorder. Theapproach taken here developed out of discussionsthe first author had with professional peers duringstudy groups devoted to treatment issues with thishighly complex population. It is based on thecultural mix found in Eastern European ghettosfrom 1939-1943, particularly those of Warsaw,Lodz, and Vilna. The cultural mix that developedin the non-clinical populations of these ghettosdirectly parallels the cultural mix of alter typesfound in the internal worlds of many patients withDID. This comparison holds implications for the-ory, research, and practice. It offers accessibility,understanding, and a demystification of the inter-nal world to clinicians and patients workingwith DID.
Alters have been conceptualized as "highly dis-crete states of consciousness organized around aprevailing affect, sense of self (including the bodyimage), with a limited repertoire of behaviors andstate-dependent memories" (Putnam, 1989, p.
3 In recent years, attention to the understanding and treat-ment of DID has increased dramatically. That material isbeyond the scope if this article. Interested readers are referredto works by Putnam (1989) and Ross (1989).
485

A. S. Frankel & T. C. O'Hearn
103). Amnestic barriers between alters are quitecommon, such that any given alter may or maynot know of the existence of other(s).
The strength of the ghetto comparison lies inits clarification of internal dynamics, fine-tuningof alter types, and direct relationships to clinicalstrategy. It is offered as a teaching model for bothclinicians and patients. It is an alternative to thelisting of alter types found in textbooks on thesubject of DID (Putnam, 1989) in that its focusis both within patients and between patient andclinician. It is not a substitute for alter systemmapping (Ross, 1989), which is concerned withwithin-patient issues. The interface betweenghetto metaphor and system mapping allows cli-nicians to understand patient dynamics morecomprehensively and more clearly, offering aschematic structure not only of how inner forcesmay be grouped together, but also how they coex-ist, interact, and function with respect to out-side influences.
The comparison involves an elaboration of thecommon tetrad of alter groups (persecutors, trau-matized alters, and protectors, behind a host) de-scribed by Kluft (1987). It clarifies the commontetrad labels by emphasizing that all alter typesare essentially protective. It also appreciates thecomplexity and heterogeneity of persecutory altertypes. Finally, while traditional categories suchas the common tetrad have focused primarily oninterrelationships between alter types of theghetto analogue extends this analysis of internalcharacteristics by exploring how the internal bal-ance is affected by the external force introducedby a clinician in the treatment of DID. In manyways those familiar with the Fairbairnian ap-proach to object relations theory will find the typeof thinking involved with the ghetto comparisonto be familiar. However, a more complete elabo-ration of the similarities is beyond the scope ofthis article. The interested reader is referred toworks by Fairbairn (1954) and Bacal and New-man (1990).
Several caveats should be mentioned beforeproceeding: First, the authors are not aware ofliterature that supports any necessary connec-tions between the organization of social groupsand intrapersonal processes. The views ex-pressed here are indeed metaphoric, and shouldbe seen in that light. Further, readers shouldtry to avoid the tendency to reify metaphoricconcepts (e.g., it would probably be unhelpfulfor clinicians to ask—either themselves or al-
ters with whom they interact—if a given alterrepresents a "bonding force," a "pro-bondingforce," an "anti-bonding force," or an "indepen-dent force.") Rather, clinicians are well-ad-vised to understand that such forces are oftenactive in a DID system, such that interventionsmust be planned accordingly.
Third, clinical experience suggests that theghetto analogue is not a universal for DID pa-tients. In particular, it may be inapplicable tothose DID patients who tend to be seen as highfunctioners (see Kluft, 1986). Its applicability islikely to be greatest with patients Kluft (1988)has termed "extremely complex."
Fourth, clinical experience suggests that somepatients who present with memories of particularabusive experiences, but who later recant, sayingthat their "memories" were confabulated ratherman corroborated, may nonetheless represent mattheir internal worlds are highly analogous to thosefound in ghettos. Whether or not such presenta-tions reflect social contagion, and regardless ofwhether the recanting is motivated by clarity (the"memories" weren't "real") or fear (the patientrecants in order to re-establish relationships withthose who have been abusive), the nature of thecaveat is that the relationship between abuse-related DID and an internal organization consist-ent with ghettos is correlative rather than caus-ative. It would thus be unhelpful for clinicians toconclude that patients must have had a particulartype of abuse history (or any abuse history at all),given presentations with apparent DID and ghettotypes of internal organizations.
With the above caveats in mind, we turn to theghetto analog and its development. The relevanceof the ghetto as a metaphor for DID became ap-parent through a literature review of scholarlyworks on the subject of Eastern European ghettosthat existed in the early 1940's. That review sug-gested that as a result of extreme and unremittingstress, the organization of ghetto residents in-volved particular components which developed inpart due to captors' instructions and in part byspontaneous response to siege. Both the constitu-ent components and the modes of interaction be-tween those components are analogous to alterorganization and interaction in DID.
I. Development of the Eastern EuropeanGhetto
During the years 1939-1943, the Nazis orches-trated a plan to exterminate certain groups of peo-
486

Stress Reactions in Ghettos and DID
pie. The first step of this plan was containment,which would provide management and control ofthe target groups. Contained areas, which laterbecame known as ghettos, were created and po-liced. Depending on the relationships betweenghetto residents and the broader community priorto ghettoization, the permeability of ghetto wallsvaried considerably. At one extreme was the War-saw ghetto, where residents had already estab-lished valuable and productive relationships withthe community. Here a great deal of transit tookplace under and through ghetto walls. At the otherend of the continuum was Lodz, where relation-ships were poor, resulting in a ghetto that was"truly hermetically sealed, cut off from otherJews and non-Jews alike" (Dobroszycki, 1984,p. xxiii). (Permeability may have played a sig-nificant role in the course of ghetto responses toconfinement, in that the Warsaw ghetto uprisingstood in stark contrast to the apparent acquies-cence of the residents of the Lodz ghetto. How-ever, there were so many differences betweenWarsaw and other ghettos that it is impossible tohave confidence in the relative importance of thepermeability variable.)
The ghettos amounted to tiny pockets of landwith astounding population density. For example,in the" Warsaw ghetto (1.6 square miles) therewere over 200,000 people per square mile andover nine people per room of living space (Gut-man, 1989). This small area was encased by a10-foot wall topped by barbed wire. The physicalenvironment alone was an immediate and chronicsource of stress in the ghetto community. Thestarvation and disease which resulted as a functionof such gross overcrowding was widespread,deadly, and unremitting.
There has been some disagreement in the schol-arly community as to whether the Nazi strategistspurposely planned to use the ghettos as part ofthe process of rendering their victims docile andthus easier to exterminate. This type of tactic ismirrored in contemporary criminal justice wherethe environments created for death row inmatesare designed to produce maximal compliance withprison procedures, with minimization of combat-ive events at the time of execution. Some histori-ans suggest that the use of the ghetto as a meansof pacification for those about to be killed devel-oped as a post-hoc implication rather than as ana priori intention (see Gutman, 1989; Hilberg,198S). In either case, the dynamic that emergedin the ghettos was one of a society under siege
where interests were divided along individual,family, and community lines. These conflictinginterests led to the need for a delicate dynamicbalance between a stabilizing utilitarian force thatsought the greatest good for the greatest numberand a destabilizing opposition that struggled totell the world of the horrors taking place, even atthe cost of self-destruction.
II. Cultural Components of the Ghetto
A. Group I
Since any opposition to Nazi rule, ranging frommild protest to overt rebellion, could result inimmediate extermination of the entire ghetto, thefirst force represented in the ghetto culture wasconcerned with the minimization of such disrup-tion. The dilemma faced by this first group wasto find a set of strategies, both in principle andin practice, for avoiding immediate annihilationand for facilitating long term survival. Since theNazis wanted to keep the ghetto environment self-sustaining if not self-destructive, ghetto leaderswere forced to generate belief systems and imple-ment policies that were at once imperative andimpossible to maintain.
1. The co-opted government: The Judenra-ten. The Nazis initiated their overarching con-trol of the ghettos via indigenous members ofthe target communities. They installed a co-optedgovernment—a body of leaders chosen from thecommunity and assigned the task of overseeingghetto members and enforcing Nazi directives.These councils, known as the Judenraten, werecomposed of Jewish men who were obligated torespond to the unreasonable and inhumane de-mands and threats of the Nazis. These demandsput Jewish leaders in a very difficult position, asthey were required to forward large amounts oftax dollars to the Nazis, select members of theirown community for forced labor, and even desig-nate individuals for deportation and certain death(see Gutman, 1989).
The Judenraten were thus faced with an impos-sible paradox. Their adherence to a utilitarianmodel, seeking the greatest good for the greatestnumber, left them inevitably unable to satisfyboth the Nazis and their own ghetto constituency.In Warsaw, the activities of the Judenrat "contrib-uted to the alienation of the Jewish masses fromits official leadership and a crisis of confidencein the council's representatives" (Gutman, 1989,p. 24). The hubris stemmed from the notion that
487

A. S. Frankel & T. C. O'Hearn
these Jewish leaders believed that they had thebest interests of their respective ghettos at heart.In most instances they were simply responding toNazi demands in order to avoid deportation andtotal destruction. However, members of theghetto were hardly sympathetic to this group ofleaders who took their money, offered them upas slaves, sacrificed them, and essentially ap-peared to betray them at every turn. Since thepublic had no direct contact with the Nazis, theywere left with no recourse but to "direct theirrage against their own representatives" (Gutman,1989, p. 39).
In many ways the actions of the Judenraten inWarsaw, Vilna, and Lodz, can be seen as verynormal responses to extraordinary circumstances.They performed a daily balancing act not onlybetween groups, but also within themselves. Theinternal sense of morality of these leaders vacil-lated from "good" to "evil" in the space of min-utes, leaving their identities shattered. The tragicnature of this scenario is most acutely exemplifiedby the plight of Adam Czerniakow, the leader ofthe Judenrat in the Warsaw ghetto, who "keptready a potassium cyanide tablet which he in-tended to use, should he ever receive an order thatwent against his conscience" (Hilberg, Staron, &Kermisz, 1982, p. 23).
The circumstances in which Czerniakow foundhimself forced him to redefine orders that wentagainst his conscience. To do this he employedthe familiar psychological mechanisms of denial,suppression, and rationalization. When thesefailed, the unspeakable evil Czerniakow had toauthorize left him a patriarch one moment and apotential suicide victim the next. In fact he didcommit suicide, providing a testament to the im-possible load he had to bear. It is here that notjust historians, but all of us find sympathy for anindividual who was ultimately powerless in theparadoxical power he was accorded.
In a manner tragically similar to the Scare-crow's song from The Wiz: "You can't win, youcan't break even, and you can't get out of thegame" (Smalls, 197S), the Judenraten had to finda mechanism to implement policies that wouldserve the utilitarian interest. This policy imple-mentation revolved around compliance and hadtwo components, one behavioral and the othercognitive.
2. The Judenpolizei (ghetto police). The taskof ensuring behavioral compliance fell to the Ju-denpolizei. They had to make certain that the
daily movements of inhabitants did not violateNazi directives, including such prohibitions as"nobody leaves the premises," "nobody calls forhelp," and "nobody smuggles food in or out." Asenforcers, the Judenpolizei were caught in aplight similar to that of the Judenrat itself. Giventhe thankless job of seizing their own people, "thebehavior of the Jewish police at the gate—thesearches and the beatings—made mem and theircommander the most hated group among the Jewsof the [Vilna] ghetto" (Arad, 1982, p. 305).
The role of the police became so defined thatthey broke off and "evolved as an independentforce in which the police chief and officers setthe tone" (Gutman, 1989, p. 88). The Lodz policewere described as "brutal and Gestapo-like," ex-isting as a "class apart" (Dobroszycki, 1984, p.xxix). The sense of independence the police feltseemed to be validated by the immunity they werepromised by Nazis as the inevitable deportationdrew nigh. This resolved as a tragic delusionwhen the police were forced to reckon with theirown vulnerable position in the ghetto as the goalsof the Nazi authorities became clear (see Gut-man, 1989).
3. Loyalists: Self-blamers, and deniers. Thecognitive component of compliance fell to a thirdsubgroup. Even in the ghettos there were groupsmat appeared to be loyal to the Nazis. Loyalistsoften took the form of spies who would gatherinformation for the Nazis regarding destabilizingactivities in the ghetto. These informants wouldcurry favor with the Nazis, believing that theywould receive immunity in return for the informa-tion they conveyed. For example, after receiving"information from agents planted in the ghetto"(Gutman, 1989, p. 178) pertaining to resistanceactivities in Warsaw, the Nazis murdered 52 in-habitants in a massacre that became known as the"Night of Blood."
There were also a large number of inhabitantswho denied the severity of Nazi intentions. Thevery existence of a leadership made up of indige-nous members of the community also served toreinforce illusions that nothing extraordinarywould happen. For example, in Vilna "the recon-stitution of an official Jewish representation, rec-ognized by the authorities, added to the illusionof stability and security which the Jews felt uponentering the ghetto" (Arad, 1982, pp. 123-124).This denial was intensified by the outbreaks oftyphus and other contagious diseases which oc-curred in the ghettos, notably in Warsaw. These
488

Stress Reactions in Ghettos and DID
epidemic conditions led to self-blame and re-inforced Jewish illusions that they were simplybeing quarantined in a safely contained location.Denial was also expressed in response to the be-lief that the "Nazis intended to uproot only partof the ghetto population—primarily refugees andthose without a stable means of support" (Gut-man, 1989, p. 227).
Even when news regarding realities on the out-side did seep into the ghettos, psychological de-fenses were mobilized to contain and reframesuch information. In response to the atrocities atTreblinka, Warsaw deemed it "simply not possi-ble" and referred to it as a "bad dream, a night-mare that was destined to end" (Gutman, 1989,p. 226). These reactions have been conceptual-ized as a "Jewish repressive mechanism that waslargely self-administered and automatic" (Hil-berg, 1985, p. 303). In addition to being deceivedby the Nazis, the ghetto residents "deceived them-selves" (Hilberg, 1985, p. 301) and engaged in"automatic compliance" (Hilberg, 1985, p. 298).In its automaticity, this denial was largely a nor-mal and expected response to events too terribleto acknowledge. As such, it characterized a sub-stantial number of ghetto inhabitants. This prece-dent in turn worked in favor of the Nazis, asdeniers were not prone to resist. Further, denialmade it more difficult for those who did recognizethe truth to gain support.
Denial existed at all levels of the ghetto struc-ture. As Gutman (1989, p. 226) observes: "Thesepsychological blocks and emotional defensemechanisms were as characteristic of public fig-ures as of the average man in the street." EvenCzerniakow repeatedly denied the intractabilityand futility of his position and the inevitable fateof the Jews. In the hours before his own deathCzerniakow was "still deluding himself that therewas some misunderstanding and that some possi-bility remained of averting the threatened evil"(Hilberg, Staron, & Kermisz, 1982). This kindof denial persisted and evolved into self-blame atthe level of the Jewish leaders, as people likeCzerniakow could no longer live with themselvesand the decisions they had to make. Denial alsoserved to increase the misery of the next groupto be considered: the victims.
B. Group IIThe second major group of people living in
the ghettos were the victims. This group was bydesign the largest of the ghetto divisions and in-
cluded laborers, artisans, and the many who weretortured and killed. In addition to victimizationoccurring immediately and relentlessly as a func-tion of the physical surround, inhabitants werepulled from their professions and their homes toengage in forced labor. The situation in Warsawexemplifies the horrible nature of this condition:
"Working conditions were abominable. Most Jews were notaccustomed to strenuous physical labor, and they also sufferedfrom malnutrition and lack of proper clothing. Many of theyoung Nazi soldiers were not satisfied with merely humiliatingthe Jews. In some instances they forced Jews to remove then-gloves and carry freezing lead pipes. . . ." (Gutman, 1989,p. 23)
Victims also included those craftsmen whowere directly exploited in their existing vocations.They essentially assumed the role of working forthe survival of the ghetto as a whole. The Juden-raten sought to expand the efforts of these crafts-men, as this was "the only way to pay for thefood and goods apportioned to the ghetto by theNazi authorities" (Gutman, 1989, p. 74).
Besides being economically bound to thewhims of the Nazis, the ghettos were forced toremain silent about the extent of their victimiza-tion. In Vilna, the massacre of hundreds at Ponar,which was supposedly a labor camp, was knownonly to a few doctors who "listened to their tale[and] kept it a secret" (Arad, 1982, p. 175). Oneindividual who had witnessed the real events atPonar was coerced by the ghetto police into keep-ing silent. The police admonished hen "Thendon't say a word of what you saw. I'll help youget work, but just keep quiet. You saw and heardnothing" (Arad, 1982, p. 177). Even the Judenratof Vilna adopted a "policy of silence" and "suc-ceeded in concealing news of the Ponar massa-cres" (Arad, 1982, p. 182). In fact the Judenratheld the general belief that anyone who "carriedinformation to the Nazi administration regardingillegal activities in the ghetto" would surely"bring disaster upon it" (Arad, 1982, p. 293).
Given the prohibitions against and conse-quences of breaking the silence, victims wereforced to accept and cope with their horrible con-ditions. Many scholarly descriptions offer a wayof capturing the general picture of ghetto life forthese victims and laborers. A commonality acrossthese horrible portraits is the presence of chronicand unremitting stressful conditions. Gutman(1989, p. 115) observes that ghetto conditions:". . . left the public in a continuous state of anxi-ety, which left not time or strength to concentrate
489

A. S. Frankel & T. C. O'Hearn
on or analyze affairs from a broad and forward-looking perspective."
The ghetto inhabitants became hyperarousedand hypervigilant, as the Nazis kept them in "astate of suspense about their fate, thereby wearingon their nerves" (Gutman, 1989, p. 214). Withthis kind of chronic stress, there were frequent"outbursts" of impulsivity. For example, in War-saw individuals known as "snatehers/' usually"young people dressed in rags," would "ambushwomen leaving stores with baskets of food in theirhands" (Gutman, 1989, p. 109). These snatchersactually fall into a fourth group and are describedbelow in more detail.
As members of the ghetto became accustomedto atrocity, a numbing of emotional reactions de-veloped. This contributed to the withdrawal andthe scarcity of resistance that characterized thevictims. Gutman (1989, p. 227) notes that "thesteadily deteriorating circumstances paralyzed thewill to live and the ability to resist." Hilberg(1985, p. 298) interprets a similar kind of "victimparalysis" when, during ghetto clearing opera-tions, "many Jewish families were unable to fight,unable to petition, unable to flee, and also unableto move to the concentration point to get it overwith. They waited for the raiding parties in theirhomes, frozen and helpless." This type of re-sponse to overwhelming trauma has been likenedto animal responses to inescapable shock (vander Kolk & Greenberg, 1987)—responses thatSeligman (197S) termed "learned helplessness."It is characterized by massive outputs of norepi-nephrine which results in corresponding alter-ations in neurochemical makeup, with suchchanges assumed to be responsible for the behav-ioral withdrawal that is observed (Bremner,Davis, Southwick, Krystal, & Charney, 1994).
Faced with unremitting tragedy and unable toget out of mis horrible "game," a third force nec-essary to maintain the delicate balance of ghettolife had to develop. This force was one of hopeand carried with it two concerns. The first was ahope for survival and the second a hope for asense of purpose and meaning in the event ofdefeat (see Frankl, 1962, 1978).
C. Group IIIThe third group of ghetto members consisted
primarily of the underground/resistance and so-cial relief efforts that arose in response to thesiege. This group included welfare workers whoaddressed the basic survival needs of the ghetto,
political activists who strived to give a voice toand defend ghetto concerns, and archivists whokept a running record of the events that tookplace.
1. Social aid. To meet the basic survivalneeds of ghetto inhabitants, a nurturing force wasneeded that might balance the siege of the perpe-trators. This force took the form of social serviceproviders and childcare workers who dealt withinstances of disease, starvation, and physical tor-ture that plagued the ghettos. They sought waysto shelter, clothe, feed, and medically care forthose most in need, especially children. In Vilna,social aid and welfare assumed distinctly restor-ative functions:
"The Social Aid Department of the Judenrat and the PublicCommittee for Social Welfare were in charge of granting freemeals at the public canteens and directing financial support,free medical treatment, and part or full ex-emption from pay-ing rent for housing." (Arad, 1982, p. 312)
The social aid agencies were so instrumentalduring one year in Vilna that "there were no casesof death due to hunger or as a direct result ofexposure to the cold in the ghetto" (Arad, 1982,p. 315).
Social assistance often took the form of reliefspecifically for children in need, primarily or-phans (see Arad, 1982; Gutman, 1989). Beyondmeeting the basic needs of survival for ghettoinhabitants, the social service providers alsosought to improve the general quality of life in theghettos. Efforts were directed towards salvagingsome kind of continuing education for childrenamid the plight. Others attempted to sustain theghettos by adding cultural vitality through spon-sorship of library, theatrical, and musical enter-prises (see Arad, 1982). Thus, the social aid ef-forts provided a source of hope that balanced thecompliance and withdrawal of the victims.
2. The Underground/Resistance. In additionto practical and survival considerations, anotherforce of political resistance also developed. Thisnetwork, known as the "underground," held fre-quent assemblies for the broadcasting of informa-tion and the dissemination of various propaganda.This type of activity was directly contradictoryto, and thus balanced, the prohibitions placed onvictims concerning the disclosure of secrets. InWarsaw one underground faction, theHa-Shomeractivists, "telephoned secret contacts outside theghetto, stamped forged documents, and obtainedhelpful information on the planned course of the[deportation]" (Gutman, 1989, p. 234).
490

Stress Reactions in Ghettos and DID
Subtle resistance was not only fostered againstthe Nazis, but perhaps even more readily againstthe Judenraten. The underground eventually de-veloped a sense of disdain for the Judenraten,"and dissociation from and denunciation of theJudenrat were common to all factions in the [po-litical] underground" (Gutman, 1989, p. 128).This opposition, however, never translated intoany concrete action, and the extent of such oppo-sition was protest demonstrations held by the hun-gry in Lodz (see Gutman, 1989).
Members of the underground were more mili-tant and in some cases separated themselves frommore formal social relief efforts. For example, inWarsaw "the members of the youth movementstook the personally painful step of detachingthemselves from the familial framework" (Gutman,1989, p. 235) of the larger underground operations.Groups like these were "dedicated to the cause ofimnvHiafp armed resistance" (Gutman, 1989, p.235). Despite the existence of such factions, theywere generally too compartmentalized and disorga-nized to initiate a full-fledged resistance.
The Nazi authorities were essentially "indiffer-ent" (Gutman, 1989, p. 178) to the undergroundand they "never related seriously to them andtheir potential" (Gutman, 1989, p. 131). Somescholars interpret this indifference as apathy andothers attribute it to a lack of knowledge andawareness of the underground (see Arad, 1982;Gutman, 1989). In either case, they were neverable to "discern the secret organizational activitiesin the ghetto, preparations for uprising, and thecrystallization of the resistance forces" (Gutman,1989, p. 131). At times the Nazis did learn ofthe destabilizing activities of the underground anddemonstrated their disapproval of the resistancesymbolized by this group. For example, the"Night of Blood," discussed above, was interpre-ted by most in the ghetto as "punishment becauseof the relative few who were operating in theunderground" (Gutman, 1989, p. 178).
Although the underground's illicit activities,when exposed, were often objectionable to ghettomembers, many of those in the ghetto were unawareof the underground's existence, in a manner analo-gous to the amnestic barriers between alters in DID.hi Warsaw, "many did not even know that an under-ground existed [until] they saw proof of its deeds."On the occasion that they did learn of this "orga-nized force" that was an "alternative to the Juden-rat, hope revived in the hearts of the doomed"(Gutman, 1989, p. 319). Thus, the underground
was at once a source of hope and of dismay andliability. While the actions of the undergroundplaced the ghetto in a state of fear and vulnerabilityfrom time to time, the spirit of hope they fosteredbalanced the force of the perpetrators. The under-ground also balanced the action of the deniers byrevealing the truth through the activities of the nextsubgroup: the archivists.
3. The Archivists. The underground soughtto keep people outside the ghetto apprised of whatwas transpiring, with an emphasis on correctingmyths about Nazi restraint. This type ofinformation-seeking and distribution was oftenachieved through the "clandestine publication ofnewspapers" (Gutman, 1989, p. 125). There wereother publication sources, such as the Oneg Shab-bat Archive in Warsaw, which recorded eventsthat transpired in the hopes that ghetto atrocitiescould eventually be revealed. The Oneg ShabbatArchive "adopted the aim of giving as much cov-erage as possible to the changes that had takenplace during the period of occupation and theghetto in Warsaw" (Gutman, 1989, pp. 144-145).Typical topics for archival sources included "shoot-ings near the barbed wire fence surrounding theghetto, suicides, arrival of food supplies and theirrationing to inhabitants of the ghetto, prices on theblack market and incidences of smuggling into theghetto, matters of public health. . ." (Dobroszycki,1984, p. xvi). Thus, these reporters made observa-tions of all the cultural components and phenomenathat existed in the ghetto.
The broader goal of the archivists involved asense of purpose surrounding the plight of ghettovictims (see Frankl, 1962, 1978), as they hada "desire to transmit testimony from the age ofextermination to posterity" (Dobroszycki, 1984,pp. xvi-xvii). This kind of record keeping was"done in secret and would have been dangerousto the author [archivist] and those around himif exposed," a circumstance which "indicates aconscious choice and a stance by the writer [archi-vist] toward the forces and events at work in hisworld" (Dobroszycki, 1984, p. xvii). This impli-cation translated into a caveat against writing spe-cifically about the Nazis as criminals: "The chron-iclers seem to have adopted the followingprinciple—since it is not possible to write aboutthose who commit the crimes, we will speak oftheir victims, and in some detail" (Dobroszycki,1984, p. xviii).
In reporting on the experiences of the victims,the archivists maintained a detached and emotion-
491

A. S. Frankel & T. C. O'Hearn
less style of data recording. In Lodz, the chroni-clers "never reported what the victims think andfeel about those who caused their tragedy, evenwhen they are being sent to their deaths. Thereare only facts and the descriptions of events: howthings really were, how the Jews lived and diedin the ghettos" (Dobroszycki, 1984, p. xviii).
In Warsaw, the founder and guiding spirit ofthe archives, Ringlebaum, stressed a "sense ofunity in the face of challenges of the day" (Gut-man, 1989, p. 128). However, even the differentarchival sources varied in their manner of cover-age and presentation, which worked to "dull theperceptions of the impending dangers and re-tarded somewhat the general organization ofarmed resistance" (Gutman, 1989, p. 128). Thiskind of disorganization was typical of the nextgroup to be considered: the anarchists.
D. Group IVThe final group in the ghetto consisted of anar-
chists who did not side with any faction and func-tioned only for themselves. Included in this groupwere observers, thieves, food smugglers, and un-organized forms of resistance. Although therewere spies and informants working for the under-ground, the Judenraten, and the Nazis, there werealso those who functioned independently. Theyoften reported ghetto transgressions to the policeand Nazi authorities in exchange for food ormoney. However, observers of the anarchistgroup were not loyalists of any kind and operatedonly for their own personal gain.
Theft occurred on various scales, small andlarge. Most commonly it involved the impulsiveacts of starving individuals, especially teenagers.Those who stole bread from people on the streetbecame known as "snatchers." Stealing of cloth-ing also occurred and usually involved needy indi-viduals who were acting for their own survival.This kind of thievery was an alternative to thesocial aid efforts which were organized and di-rected at those most in need. As such, theft grewbom out of the inadequacy of the social reliefand from the impulsive reactions of individualsin extreme distress.
Food smugglers were more prevalent in War-saw and Vilna, as the walls of Lodz were muchless permeable. In Vilna, "there were times whenfood could be brought through the gate withoutdifficulty, but at other times those caught wereseverely punished" (Arad, 1982, p. 304). In fact,the "murder of Jews for buying and smuggling
food continued throughout the existence of theghetto" (Arad, 1982, p. 306). Smuggling prolifer-ated when food or supply lines were cut off tothe ghetto. Although food smuggling may haveoccurred for altruistic or community goals, itoften involved independent entrepreneurs whonetworked with many groups in the ghetto fortheir own gain:". . . people engaged in food traf-ficking on a much larger scale for their own profit.These contrabandists had connections with thegate police, who, against due payment, helpedthem bring whole cartloads of commoditiesthrough the gate. Secret routes were sometimesused by the smugglers, including attics, cellars,and walls of houses adjoining the Aryan area andleading into the ghetto area" (Arad, 1982, p.307). These smugglers were rewarded for theirefforts, although they performed their activitieswith considerable risk and consequence.
In addition to food smuggling, other indepen-dent forces developed and functioned much likeanarchists, loyal to no group or cause. Their exer-cises of resistance were not affiliated with theactivities of the underground: "wildcat bands alsobegan to make their appearance in the ghetto.These were armed groups that operated under theguise of being underground organizations pre-paring for an armed struggle, while the combatorganizations maintained their secret character"(Gutman, 1989, p. 350).
Disdain for anarchists of all kinds developedas the ghetto community recognized how suchgroups placed the entire community in jeopardy.Ghetto residents "were hardly sympathetic tothose who were playing around with outlawedpolitics and thereby invited further persecutionand risks" (Gutman, 1989, p. 178).
The four groups discussed above coexisted tomaintain a delicate balance in daily ghetto life:the Judenraten would solicit aid and the laborerswould produce; the underground would propa-gandize and be chastised by the Judenraten; theanarchists would impulsively act on a whim andthe rest of the ghetto would shudder in anticipa-tion of the consequences; the archivists wouldrecord facts while the deniers would distort andreframe them. This interplay occurred almost au-tomatically, with the ghetto constantly striving toachieve some approximation of homeostasis.
The homeostasis that the ghetto struggled tomaintain was a direct result of competition thatexisted between the various subcultures. Theghetto became inward-focused, with its delicate
492

Stress Reactions in Ghettos and DID
internal balance subject to mistrust and competi-tion across the various groups inside the ghettowalls. Instead of reacting only outwards againstthe Nazis, the ghetto groups competed with oneanother and often saw each other as the "evil"force to be resisted. Each group reacted in acharacteristic way to the victimization processand did not trust those who responded differ-ently. Even within the same group there wasfurther variation and dissent regarding the bestcourse of action.
The mistrust between groups in the ghetto be-came salient when the Nazis initiated some courseof action that effected only some of the ghettoinhabitants. For example, the Nazis would selectpeople for deportation in a fairly arbitrary way.However, ghetto inhabitants attached meaningand significance to these acts according to thesubgroup with which they primarily identified.Those in denial analyzed this arbitrary selectionprocess in a way that supported their denial, whilethose who recognized the atrocities, like the un-derground, interpreted things in a way that sup-ported their suspicions. These groups resentedeach other for their differing construction of real-ity, leading to a constant state of suspense andmistrust (see Gutman, 1989).
Nazi victimization thus had primary and sec-ondary effects. The primary effects included star-vation, exploitation, and torture that resulted fromthe Nazi imperative of containment. The second-ary fallout resulted as ghetto inhabitants orga-nized spontaneously in the face of unremittingstress. The individuating and separating nature ofmis spontaneous organization led to internal strug-gle, discord, and competition. The cultural mixfound in the ghettos represented a diverse range ofpossible reactions to mis unremitting stress. Thedispersal of these reactions across groups in theghetto was an automatic survival strategy.
However, for DID patients the implications ofthese survival strategies for long term functioningbecome critical and problematic as internal fac-tions compete and resist each other. Thus, thereactive solution of fragmentation and specializa-tion as an adaptation to unremitting stress be-comes itself the problem both for the DID patientand the clinician after the traumatic period hasended (see Watzlawick, 1967).
Comparison of the Ghetto with DIDFractionated internal organizations in the face
of unremitting stress are common to both ghetto
cultures and the internal cultures of DID patients.As in the ghettos, the typical alter groups seen inDID struggle for position in and control of thebody, dictating the necessity for maintenance ofa delicate internal balance. The characteristicswithin these groups, the interrelationships be-tween them, and their dynamics with respect toexternal influences are similar to those notedabove in the Eastern European ghettos.
To facilitate the comparative transition to thetreatment of DID, it might be helpful to considerthe following hypothetical scenario:
With the war having come to an end before liquidation of theghettos, an Allied soldier parachutes into the ghetto. Thepeople in (he ghetto are oblivious to the fact that the war hasended because of the tight seal formed by the ghetto walls.Knowing nothing of the coalitions and interrelationships inthe ghetto, but knowing that the inhabitants needed help, thesoldier asks the first person s/he sees: "Who do I talk to aboutliberation around here?'
This kind of encounter would probably meetwith a range of reactions from the various subcul-tures, with fear and suspicion being the over-whelming sentiment. The ghetto residents maynot know or believe that the Nazis were gone.The literature has described a long term fear oftrauma victims that the perpetrator(s) will inevita-bly return, resulting in pervasive suspicion andhypervigilance (see Herman, 1992).
Ghetto inhabitants might interpret this outsideagent in a number of characteristic ways de-pending on the subculture with which they pri-marily identified. The victims would be the mostdesperate and perhaps the first to approach theagent, in such dire need of help that any suspicionwould be displaced. The social service workerswould be hopeful for the victims, keeping themunder their own watchful eyes as the victims ap-proached the helper. The underground may regardthe new element as a threat insofar as the individ-ual might be a Nazi spy or an anarchist of somekind. The Judenrat would also be suspicious,thinking any kind of association with this outsideagent preaching freedom would be dangerous anddestabilizing, possibly invoking a Nazi backlash.
The impact made by the soldier inquiring aboutliberation is directly analogous to the clinicianwho seeks to help a DID patient. This kind of anaddition to a balanced system has been discussedin the domain of family systems theory (see Mi-nuchin, 1974, 1981). The resulting dynamic istenuous at best when a helper enters the internalworld of a DID patient and evokes a powerful
493

A. S. Frankel & T. C. O'Hearn
response. Just as each dyad, triad, and so on,reacts to the introduction of a new element infamily therapy, so there will be a reaction amongevery permutation and combination of the forcesin the internal world of a DID patient. One impli-cation of this family systems analysis is that con-cepts that go beyond a description of the culturalcomponents in relation to each other are needed;concepts that describe both those interrelation-ships and the new set of relationships that evolveas a result of a helping agent's introduction tothe system. A more complete development of thecomparison between the ghetto formulation andfamily systems thinking can be found in worksof Guerin and Chabot (1993) and Shoham, Ror-baugh, and Patterson (199S).
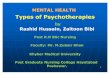
In order for the ghetto metaphor to providedescriptors both for how the internal elementsrelate to each other and to the clinician, the cat-egory labels of the common tetrad might be re-vised. One set of possibilities is offered in Figure1, where the traumatized alters are viewed in
terms of a bonding force, because they are seek-ing to offload pain and to find someone to improvetheir lives; the protectors are seen in the contextof a pro-bonding force, because their mission isto give hope and comfort and to disclose secretsof the trauma. The persecutory alters are viewedas part of an anti-bonding force because they arethere to disrupt any bonding with the outsideworld (for fear of retaliation), and are themselvesbonded to the perpetrators (see Graham, 1994).These categories in turn have direct analogs inthe ghetto subculture, as indicated in Table 1.
The common tetrad also includes the "host"category. Relatively little has been said about thehost in the ghetto culture because its function wasnot as crucial or articulated as it is in DID. It wasa rare event that those who might disapprove ofghettoization would actually visit the ghettos, andthus a robust analog of the host was not a consist-ent necessity. A quick feeding and clothing ofselect ghetto inhabitants for meetings with suchgroups as the Red Cross could be executed on an
Figure 1. Modification of common tetrad, reflecting internal relationships between alters as well as potentials for relationshipswith clinicians and others.
494

Stress Reactions in Ghettos and DID
TABLE 1. Comparison of Constituents of Eastern European Ghettos, the Common Tetrad and the Ghetto Metaphor of DID.
Banding Force Anti-Banding Force Flo-Banding Force Independent Force Host
I. WWII GhettoConstituents
n. Common Tetrad
m. Ghetto MetaphorConstituents
Victims; Laborers; Artisans;Children
Traumatized Anas
Victims; Adaptive Role-Players; MaladaptiveAltos
Judennl; Jndenpolizei andtheir supporters
Persecutor? Alters
Internal Ljeaders; Enforcers;Deiuers; Self-Blamers;Approval-Scckcis
Social Service; Child-Can;Workers; Archivists;Underground
Protectors
Care-Takers; Disclosers;Archivists
Anarchists
None
Observers; Guides("ISHesT
None
Host
Host
as-needed basis. With DID, however, there is aconsistent and recurrent need for such an alter(s)to interact with others in social, occupational, andfamily domains. As such, the host's role is well-developed and instrumental for the internal bal-ance and genera] functioning of the DID patient.
The host is often (but not invariably—the hostmay present with a broad variety of complaints,and some DID patients have no consistent host)the depleted, depressed, anxious, and masochisticindividual who presents for treatment and be-comes identified as the "patient" prior to the diag-nosis of DID (see Putnam, 1989). Although thehost may know of the existence of other alters,s/he more commonly denies evidence of othersin the system.
While the host may present for therapy withboth psychological and somatic symptoms, it isthe appearance of other alters which suggests thepresence of DID. Anecdotal reports from someclinicians indicate that victim children are oftenthe first alters to appear as DID patients begin toreveal themselves. They would probably be themost needy and anxious to receive help, seekingto make first contact with the clinician. Thus, thepatient's neediness provides the pivot point forthe major tension in the system: pro-bonding vs.anti-bonding forces.
The relationship with the clinician would besubject to the close scrutiny of pro-bonding alters.Their attitude toward the clinician is likely toreflect skeptical hopefulness (social service).These alters would thus be reacting to the internalneeds to bond, seeking support and comfort forthose in pain. They would also be concerned withreporting the injustices and victimization that oc-curred (underground).
The anti-bonding forces would be the most re-sistant to the establishment of any relationshipto the clinician on the basis that it threatens theutilitarian interest of the entire system. They
would react to any efforts at outside contact andany inclination to publicize the atrocities, seekingto balance and counteract these imperatives withtheir own agenda. DID patients, like ghettogroups that ultimately reacted more to othergroups inside the walls man to external factors,show the same kind of inward focus and competi-tion that gave the ghetto its fragmented and self-destructive characteristics.
While there are many specific pitfalls that areworrisome for clinicians entering the world ofDID, the primary concern, as emphasized by theghetto metaphor, is that all constituents of theculture are there and have been necessary for abalance. The clinician should keep in mind thatall alter types are fundamentally protective, mak-ing it necessary to appreciate anti-bonding forces.Although the bonding alters may be the most ap-parently in need of help and the most amenableto aid, the clinician must consider the reactionsof the other alter groups, which range from apathyto mild skepticism to direct opposition. Stabiliza-tion is increased by working with all groups.
IV. Implications of the Ghetto Metaphor forDID Alter Groups
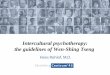
The following outline traces the characteristicsof the four alter groups, drawing on implicit andexplicit comparisons with the Eastern Europeanghettos. The analysis is offered specifically withrespect to how each group might react to a clini-cian's attempts to help, and is represented graphi-cally in Figure 2.
A. The Anti-bonding Forces
The new category labels expand most signifi-cantly on the common tetrad's "persecutory"heading by placing this subgroup within the moregeneral anti-bonding category, which includes acomplex and heterogeneous group. Since thereare many ways in which the requirement for cul-
495

A. S. Frankel & T. C. O'Hearn
Figure 2. Complex alter system, with direct comparison to the cultural components of the typical eastern European ghetto, circa1939-43.
tural stability can be implemented, persecutoryalters4 are just one of a larger group of anti-bonding alters, all with the same general purposeof stabilizing the culture, consonant with the de-mands of the perpetrators. The means by whicheach subgroup seeks to achieve compliance dif-fers from others in the anti-bonding contingent.
Since utilitarianism is the guiding principle ofthe anti-bonding forces, these alters, as a group,disrupt any bonding with outside agents by bothdirect and indirect means. Indirect attempts todisrupt the clinician may be exhibited by inflictingpain on bonding alters and the host, seen as theclassic symptoms of Post-traumatic Stress Disor-der (PTSD): 1) hyperarousal and reactivity;2) flashbacks and intrusions; and 3) numbing,
4 Our clinical observations indicate that patients dislike thelabel'persecutory" and feel that "anti-bonding altei''is a moresuitable and representative heading.
appearing as anesthesia, and ultimately dissocia-tion (see Herman, 1992; Pynoos, 1994; van derKolk & Greenberg, 1987). In addition, the classicPTSD tendency to avoid discussing the trauma isseen as distraction and denial, overt characteris-tics which can also be orchestrated by the anti-bonding alters. This kind of purposeful disruptionin functioning works to distract, discourage, anddisrupt progress in treatment. Direct attempts tothwart the helper may include forewarning clini-cians that they are intruding where they are notwelcome, with threats of dire consequences forpersistence.
The first anti-bonding subgroup is analogousto the co-opted leadership of the ghetto. As inthe ghetto, these leaders generally set policy pre-venting the divulging of secrets and the cultiva-tion of relationships and activities that will bringdisaster on the entirety of the system. Thus, theywill discourage the transfer of information to thehelper, or distort it in some fashion. As in the
496

Stress Reactions in Ghettos and DID
ghetto, this involves principle and practice aimedat maintaining stability in the internal world.
1. Internal Leaders. The internal leaders(Boon & van der Hart, 1995) are the dominantanti-bonding sub-group, and perhaps the mostdominant group in the system. In ways analogousto the function of the Judenraten in the ghettos,this oversight committee will discourage a bondwith the clinician on the basis that it will put thewhole internal community in grave danger for theviolation of various prohibitions: nobody talks,nobody seeks help, nobody misbehaves, and soon. "Strength" is defined as the capacity to toler-ate great pain without complaint (leaders are quiteoften anesthetic to pain themselves). This trans-lates into a concerted effort to extrude the destabi-lizing force embodied by the clinician.
As in the ghetto, there is great distortion and, refraining of information and experience. Instead
of seeing the misery of bonding forces as painthat needs to be remediated, the leaders come tosee it as a sign of weakness and demand thatthose in apparent pain become more resilient andhearty. This kind of refraining has a family sys-tems analogue: a rigid and demanding parentviews anything other than dogmatic "party-line"behavior on the part of their child as weak. Inturn, the rigid parent regards the other parent,who may have initiated psychotherapy, as alsosoft, weak, and ineffectual. This dynamic resultsin great resistance to and subversion of therapyby the rigid parent, as therapy validates the painand suffering of victims rather than dismissing it.In DID, the leaders assume the role of the rigidand demanding parent who refuses to recognizethe true pain and suffering of real victims.
A second form of distortion concerns the pas-sage of time. Because this is a short term solutionapplied over a long term, the psychological mech-anisms operative among the leaders result in aloss of the capacity to recognize that time haspassed since the abuse period ended. Many anti-bonding alters still believe they are living in the"bad time."
A third example of distortion concerns issuesof "good" and "evil." Many leaders resolve thisdilemma through a combination of denial andwholesale adoption of the belief system of theperpetrators, as was seen in the ghetto leaders.The identities of the leaders are distorted to theextent that, by adopting the belief system of theperpetrators, their perceptions of themselves be-
come consistent with the notion that they are, orwere sent by, perpetrators. Seeing themselves thisway provides a means for them to tolerate (andoften forget) the greatest shame in an alter system,much like Czerniakow's position in the Warsawghetto. It is thus not uncommon to find mem ortheir agents looking, acting, and talking like theperpetrators, discussed by Bettelheim (1943),Mahl (1971) and Schmolling (1984) as the phe-nomenon of "identification with the aggressor."Because they are forced to perpetrate, the leaderscarry the greatest guilt and shame in the system.The work of healing that dissociative patientsmust go through applies most dramatically to thisgroup. The leaders, along with the rest of theiranti-bonding contingent, thus have the farthest togo in psychotherapy between their self-views atthe beginning and end of treatment.
Given their role, the internal leaders would notbe likely to make or encourage a warm welcometo a clinician who arrives on the scene. Theymight instead react to a "victim's" (see below)initial contact with the helper by forbidding thecultivation of a bond. It is this stance that dictatesthe need for any agent of change to obtain permis-sion to be helpful. Thus, it is important that theclinician recognize the determinative role of theleaders and secure their consent prior to treat-ment interventions.
In addition to their negative reactions to contactbetween an alter(s) and a clinician, the leadersalso prepare victims prior to contacts with clini-cians. This may take the form of such preventa-tive measures as stipulating rules, instilling de-nial, or ordering anticipatory punishment. Toimplement their utilitarian policies, these leadersneed vehicles of both behavioral and cognitivecompliance.
2. Enforcers. Enforcers, a group traditionallyconceptualized as persecutory alters, assist in thebehavioral component of compliance for the anti-bonding force. Like the leaders, enforcers tendto be anesthetic to pain and amnestic for the cir-cumstances surrounding their original emergenceinto the system. They also hold the belief systemthat "it is good to be bad" and they behave ac-cording to hostile tendencies that are modeledafter the perpetrators. Their acts are likely to bedirectly observable as behavioral disruptions inthe DID patient.
Also like leaders, enforcers often appear asintrojects of the original perpetrators) (see Put-
497

A. S. Frankel & T. C. O'Hearn
nam, 1989). However, they are more visible andactive than the leaders, who remain hidden anddictate policy behind the scenes while enforcersintimidate and punish. Evidence of their activitiesis found in incidents of self-harm, hostility to-wards various alters, and re-experiencing of trau-matic events via flashbacks. The enforcers oper-ate at Kohlberg's (1984) second stage of moraldevelopment, whereby they punish those that are"caught," regardless of whether or not they de-serve it.
In following the various injunctions of the lead-ers, the enforcers seek to control the system byforce. In one of the most tragic examples of theparadox of faulty imitation learning, the enforcersoperate with the perpetrator's belief that anticipa-tory punishment will be effective in eliminatingundesirable behavior. Thus, they will punish al-ters as a way of preventing them from even con-sidering prohibited behavior. While the enforcershave the intent of illustrating negative conse-quences for transgressions through anticipatorypunishment, the eventual impact of this tacticbackfires. When anticipatory punishment is ad-ministered, it sends shock waves throughout thesystem: bonding forces react with pain and pro-bonding forces protect. The synergy of these threeforces results in rapid escalation. Such escalationscomprise many of the acute emergencies that areseen with DID patients. Therefore, anticipatorypunishment is one of the primary targets for treat-ment intervention.
Although enforcers are resistant and even hos-tile to an entering clinician, their assistance canand must be enlisted for treatment. Like the Juden-polizei—the ghetto police—they can be arro-gant, challenging, and hurtful. However, giventheir power in the system from a practical day-to-day standpoint, it is crucial that clinicians activelyavoid alienating them. Respecting them and rec-ognizing their fundamentally protective role is agood first step towards constructive interaction.The enforcers can be influenced in useful direc-tions, although any attempts to work with themmust be executed slowly and carefully.
It is often helpful, if not imperative, for clini-cians to gain permission from the leaders to workwith enforcers, as leaders supervise enforcers ina far more demanding way than pro-bonding al-ters are watchful over bonding alters. At times,changes in enforcers can be achieved relativelyeasily, but this can result in heightened subversionand resistance by the clandestine leaders, much
like the rigid parent who is not present in sessionsof family psychotherapy for his/her spouse andchildren and denies the need for it, but counteractstreatment effects elusively from afar.
3. Deniers, self-blamers and approval-seekers.The third anti-bonding subgroup implements thecognitive/attitudinal component of compliance. Ifa given alter does make contact with a clinician,anti-bonding forces may engage in fall back plansdesigned to mislead and divert the clinician. De-niers and self-blamers often sew doubts about thediagnosis of DID, increasing apparent resistanceto treatment. They frequently appear at timeswhen traumatic material may be emerging intoconsciousness, seeking to discourage or distortits disclosure. Thus, deniers can signal a clinicianthat important material is surfacing. (For patientswho later recant their "memories," deniers mayactually be a reality-testing resource.)
For those DID patients who maintain relation-ships with perpetrator(s), deniers are often in-volved in the ongoing contact. Approval seekerscarry guilt, finding it difficult to hurt perpetrators'feelings or to resist perpetrators' urgings forinvolvement. They seek the approval of perpetra-tor(s) through continued interaction, hoping tosoften and appease with the cultivation of a bond.This is an example of the "Stockholm syndrome,"whereby victims become bonded to their captorsand the actions of the latter become softened (Gra-ham, 1994). Bonding between captors and cap-tives has been seen in events including the IranHostage Crisis and hi the movie The CryingGame. It is normal, predictable, and expectablein the context of sustained trauma, as it maxi-mizes survival.
The group of alters instills denial both insidethe system, and between the DID patient and theclinician. Internally, denial and self-blame serveto keep the bonding process off-balance becausethe ongoing doubt prevents the patient from tak-ing a stand and saying "this is the truth." Bondingand pro-bonding forces are left in a fearful, debili-tated state of constantly questioning reality. Denialwith respect to the clinician is often seen in thegeneral difficulty of diagnosing DID. Patients oftengo undiagnosed for years as their social and occupa-tional lives dictate the hiding of those in pain andthose in need. The presenting alter may say "every-thing is fine, nothing's wrong," and so on.
Self-blame takes the form of making variousalters among the bonders culpable for: 1) thetrauma endured; 2) current functioning; and
498

Stress Reactions in Ghettos and DID
3) the clinician's presence. Culpability is interpre-ted by self-blamers through the lens of Kohlberg'sfirst stage of moral development. This stage re-gards people who have negative experiences asdeserving of them (Kohlberg, 1984). Deniers in-still this kind of self-blame in the bonders, whoare acutely susceptible to it, given the childhoodstage in which they are often frozen.
B. The Bonding ForceAs noted above, victim children are often
among the first alters to appear on therapy. Thesetraumatized alters often present as children or in-fants who have been frozen in time and containmemories and affects associated with the originaltrauma (see Putnam, 1989). Among these altersare victims in pain, alters who carry the burdenof daily living, and alters who are behaving mal-adaptively and self-destructively.1. Victims. The first subgroup is the most fre-quently cited in the literature and is often concep-tualized as "traumatized alters" (see Putnam,1989). Similar to the ghetto inhabitants, the vic-tims experience the classic symptoms of PTSD:hyperarousal, intrusions, and numbing. Thesesymptoms correspond to physiologically basedchanges that result from chronic and unremittingstress. Affectively laden traumatic memories areneurologically stored in deviant ways, resultingin re-experiencing of events. Physiological reac-tivity increases as the physical readiness to re-spond to danger is continually facilitated. Someresearchers have posed a diagnostic entity in andof itself that involves these characteristics and hasbeen termed "physioneurosis" (see van der Kolk& Greenberg, 1987) and "disorder of extremestress not otherwise specified" or DESNOS (seevan der Kolk, 1994).
Hyperarousal is seen in bonding alters as reac-tive and fearful behavior in response to benignstimuli. For example, the sound of a door shuttingin a therapy session can evoke an acute avoidanceresponse, or "startle" reflex. Similarly, quick mo-tion of any kind can be perceived as potentiallythreatening, producing a startle. The startle reflexseems to have both a neurophysiological and apsychological component. The former has beenlinked to physiologially based changes associatedwith repeated trauma (see van der Kolk &Greenberg, 1987), while the latter may be dueto the fact that the perpetrator's presence is stillperceived, even after liberation (Herman, 1992).The frequent state of hyperarousal that develops
to compensate for such fears can often result inimpulsive and harmful behavior. During abreacti-ons child alters have been observed to writhe onthe floor, re-enacting the experience, and throw-ing themselves into walls (see Putnam, 1989).Substance abusers and promiscuous personalities(see Putnam, 1989) are other examples of post-traumatic impulsivity mat can often result in co-morbid diagnoses for DID patients.
In addition to hyperarousal, victim alters alsopresent with an overwhelming sense of help-lessness from being exposed to trauma mat wasrepeated and inescapable (see Bremner, Davis,Southwick, Krystal, & Charney, 1994; Herman,1992; Seligman, 197S; van der Kolk & Green-berg, 1987). They report feelings of intense sad-ness and distress. These conditions often appearas anxiety and depressive disorders seen so fre-quently in DID patients.
Re-experiencing the trauma in the form offlashbacks, nightmares, and intrusions is also afrequent symptom seen among victims. Such ex-periences may be triggered by stress, and areoften seen during sleep states. Evidence indicatesthat autonomic arousal may activate and potenti-ate certain susceptible noradrenergic pathways,leading to automatic retrieval and heightenedawareness of memories (see van der Kolk &Greenberg, 1987).
2. Adaptive role-players. Alters who carrythe burden of the symptoms include both thosewho are functioning somewhat normally andthose who are behaving maladaptively. Like thelaborers and artisans of the ghetto, certain altersengage in the challenges and routines of dailylife. There may be some who assume a distinctlyoccupational role, performing work functions ad-equately enough to hide signs of the disorder.Others serve their primary roles in social and fam-ily settings. Thus, these role-playing alters ad-dress daily tasks, which helps maintain function-ing but may simultaneously mask the presence ofDID. Frequently, the bulk of such adaptive rolesis expressed through the role of the "host."
3. Maladaptive alters. The flip side of these"normal" personalities consists of the wide rangeof psychological disorders which characterize theother victims. Like the sick, starving, and tor-tured victims of the ghetto, these alters includesubstance abusers, promiscuous personalities,and suicidal personalities (see Putnam, 1989).This group of presentations essentially spans theDiagnostic and Statistical Manual of Mental Dis-
499

A. S. Frankel & T. C. O'Hearn
orders (American Psychiatric Association, 1994)with their broad range of symptoms, includingpsychotic, characterological, obsessional, anx-ious, and depressive. This variability can makethe diagnosis of DID difficult and delayed, andcan lead to misdiagnosis.
The desperate neediness represented by thebonding force is balanced by the sustaining influ-ence of the next DID subgroup to be considered.
C. The Pro-bonding ForceAs the name of this force implies, these alters
provide hope and comfort for those in distress.They have been conceptualized in some texts asprotector personalities (see Putnam, 1989). In ad-dition to their purpose of getting safe help, theymay also have an overarching goal of disclosingthe abuse history. They have an impetus to tellthe world of the horrors that took place, therebyinitiating justice against the perpetrators and "val-idating" the victims. This kind of secondaryagenda directly contradicts the anti-bonding mis-sion and provides one of the catalytic ingredientsfor the fundamental tension that exists in the sys-tem. Pro- and anti-bonding forces are in intenseconflict, producing the fierce state of internalcompetition that characterizes the system.
1. Caretakers. The first pro-bonding sub-group is concerned with the basic needs repre-sented by the bonding force, including economicsecurity, sustenance, warmth, and ultimately,hope for a better life. One example of this care-taking capacity comes from our clinical obser-vation:In one patient, the host was a depleted, lost child who had acaretalting alter that was in the image of her "good mother."When the system needed money, the caretaker would driveto a carwash. When it came time to pay for me carwash, shewould burst into tears and exclaim that someone had stolenher purse. Everyone would then give her money, allowingher to pay for the carwash and still have money left over.The host would then reassume executive control of the bodyon the drive home, with a clean car and money in her wallet.
Caretaking also takes the form of nurturing andparenting those child alters who are most in painand most vulnerable. Some do this very well, butothers get caught up in caretaking to their owndetriment as they become increasingly self-sacrificing. This can lead to co-dependency asthey carry a limitless allegiance to those in need.In addition to fostering their own co-dependencyinside the system, caretakers will also engage insimilar relationships with outside people. Theymay get involved in relationships where they give
and give, receiving nothing in return. They de-velop a tendency to want to help everyone, re-sulting in unfortunate oversights to their ownneeds.
2. The Disclosers: the DID underground.Within the pro-bonding force is a group of alterswho have the desire to release details of the abusehistory in the hopes that justice will be servedagainst the perpetrators. These alters functionmuch like the underground in the ghetto. In seek-ing righteous purpose, they may put themselvesin grave danger. Their efforts are continuallycounteracted by anti-bonding alters, often in vio-lent ways. A transcendental hope of passing onthe truth for posterity may alleviate concern fortheir own demise.
Similar to the underground in the ghetto, theunderground in DID subverts the efforts of boththe anti-bonding forces and perpetrators. In theirwillingness to "go down fighting," the under-ground alters engage in extremely risky behavior.For example, they may arrange things so that achild cannot comply with a perpetrator's wishes,thereby thwarting the perpetrator. This mobilizesanti-bonding forces to retaliate by punishing thechild, resulting in possible escalation and behav-ioral disruption. The DID underground may im-plement its mission more directly and overtly bycutting the body or initiating an array of symp-toms in order to get attention from the outsideworld.
3. The Archivists. The analogue to theghetto's archivists, termed the "memory tracepersonality" by some (see Putnam, 1989), maycontain and articulate the complete abuse history.Because mere is such great danger in holding thiskind of information, these alters are often noteasily or directly accessible. Sometimes, otheralters, such as those of the underground, serve asenvoys for the archivists and relate informationto the outside world at considerable risk. As in theghetto, the archivists may assume an emotionlessstyle of data recording, logging events in a de-tached and automatic manner. The archivists canbe very helpful because of their continuous mem-ory of the traumatic history.
D. The Independent ForceThe independents represent a force that trusts
no one—inside or outside. While anti-bondingforces are loyal to outside perpetrators and pro-bonding forces are loyal to outside protectors,independents show no loyalty to any group or role
500

Stress Reactions in Ghettos and DID
model. Anecdotal reports from some cliniciansindicate that independents may present as adoles-cents who claim that they have been hurt to sucha degree that they trust no one. They may tend toview an entering clinician as just another potentialtarget to play with in the midst of their self-serving activities.
Independents have a broader overview of thesystem. With their wide angle perspective, theytend to have a special dispensation to move aboutthe system with a kind of limited immunity. Attimes they disrupt, as when they report an inci-dence of bonding to anti-bonding alters. Some-times they stabilize, as when they communicate topro-bonding alters that an anniversary of a painfulevent is coming and that preparations should bemade for the accompanying disruption. At times,the movement of the independents is tied to theoverall survival of the system, as when they inter-face with outside people to benefit the system.
A subgroup of independents may relay infor-mation to others, pretending to have allegianceto various groups and individuals, including theclinician. However, they are totally self-servingand do not trust any of the sources to whom theyreport. The negative rippling effects of such be-havior take the form of system imbalances andexacerbations of the already heated competition.In working intermittently for nearly every forcein the system, they equalize the conflict betweenanti- and pro-bonding forces, thereby securingtheir own "employment and livelihood."
Independents may also disrupt the system byadding confusion through the impersonation ofalters from other groups, creating havoc and dis-cord upon provoking a clinician's response totheir portrayal. They thus continue their internaldisruption as they always have in addition to ex-panding their playing field to include theclinician.
The observational prowess of independentsalso represents a positive potential force, how-ever. Their relative perspective on the entire sys-tem and the immunity that characterizes their sta-tus may outfit them for a role of therapeutic utility.For example, they may be excellent observers oftherapeutic contracts clinicians try to forge be-tween conflicting forces. Since the making andkeeping of contracts becomes an integral part ofstabilizing the system for treatment intervention,the role of independents as observers of difficult-ies in contract maintenance may be indispensibleto the clinician. They will likely have no qualms
about reporting these kinds of events because theyare not loyal to any one group, and do not careif they evoke anger from a given group.
Beyond the specific capacity of observing con-tracts between groups, independents may func-tion as keys to the internal world of DID in gen-eral. They often allege to know the needs andpotential difficulties of all alters in the system.They may warn of impending problems, therebyhelping those in the system in addition to servingas a guide for the clinician. When operating inthis capacity they have been referred to as internalself-helpers or ISHs (see Allison, 1974; Putnam,1989). These guides often possess a more contin-uous memory and can provide clues to internalactivity and dynamics, potentially helping a clini-cian move about the system. While independentscan act as guides or self-helpers, they may notengage in this type of activity until a sufficientlytrusting relationship has developed with the clini-cian. Given die tendency of independents to beuntrustworthy by nature, the self-help functionmay not appear until later in psychotherapy.
V. Conclusion
We believe that the structure and function of theeastern European ghettos provides a very helpfulteaching tool with DID patients, as the forces matdeveloped and operated within ghettos very muchparallel the forces found in the inner landscape ofDID. Complex DID patients, like ghetto residentssubjected to extreme and unremitting stress, de-velop homeostatic systems characterized by com-peting forces that serve agendas of help-seeing(bonding forces), communication to outsidersabout atrocities (pro-bonding forces) and utilitar-ian efforts to prevent destabilization (anti-bondingforces). The presence of a clinician serves to de-stabilize DID systems. Our hope is that by view-ing DID systems as analogues to ghettos, clini-cians can better understand destabilization risksand avoid some of the untoward consequences offailing to ally with all internal subgroups.
ReferencesALLISON, R. (1974). A new treatment approach for multiple
personalities. American Journal of Clinical Hypnosis, 17,15-32.
American Psychiatric Association. (1994). Diagnostic andStatistical Manual IV. Washington, DC: American Psychi-atric Association.
ARAD, Y. (1982). Ghetto inflames: The struggle and destruc-tion of the Jews in Vilna in the Holocaust. New York:Holocaust Library.
501

A. 5. Frankel & T. C. O'Hearn
BACAL, H. &. NEWMAN, K. (1990). Theories of object rela-tions: Bridges to self-psychology. New York: ColumbiaUniversity Press.
BETTELHEIM, B. (1943). Individual and mass behavior in ex-treme situations. Journal of Abnormal and Social Psychol-ogy, 38, 417-452.
BOON, S. & VAN DER HART, O. (1995). Supportive therapyfor MPD patients. Presented at the 11th International Con-ference on Dissociative States, Chicago.
BREMNER, J., DAVIS, M., SOUTHWICK, S., KRYSTAL, J., &
CHANEY, D. (1994). Neurobiology of post-traumatic stressdisorder. In R. Pynoos (Ed.), Post-traumatic Stress Disor-der: A Clinical Review (pp. 43-53). New York.
DOBROSZYCKI, L. (1984). The chronicle of the Lodz ghetto,1941-1944. New Haven: Yale University Press.
FAKBAIRN, W. R. D. (1954). An object relations theory ofpersonality: Psychoanalytic studies of personality. NewYork: Basic.
FRANKL, V. (1962). Man's search for meaning: An introduc-tion to logotherapy. Beacon Press: Boston.
FRANKL, V. (1978). Unheard cry for meaning. New York:Simon & Schuster.
GRAHAM, D. (1994). Loving to survive: Sexual terror, men'sviolence and women's lives. New York: New York Univer-sity Books.
GUERIN, P. J. & CHABOT, D. R. (1993). Development offamily systems theory. In D. K. Freedheim (Ed.), Historyof psychology: A century of change (pp. 225-260). Wash-ington, DC: American Psychological Association Press.
GUTMAN, Y. (1989). The Jews of Warsaw: 1939-1943.Bloomington: Indiana University Press.
HERMAN, J. L. (1992). Trauma and recovery. New York:Basic.
HILBERG, R. (1985). The destruction of the European Jews.New York: Holmes & Meier.
HILBERG, R., STARON, S., & KERMISZ, J. (1982). The Warsaw
diary of Adam Czerniakow. New York: ScarboroughHouse.
KOHLBERG, L. (1984). Essays on moral development, Vol.2. The psychology of moral development: The nature andvalidity of moral stages. San Francisco: Harper & Row.
KLUFT, R. (1986). High-functioning multiple personality pa-tients: three cases. The Journal of Nervous and MentalDisease, 174(12), 722-726.
KLUFT, R. (1987). The simulation and dissimulation of Multi-ple Personality Disorder. American Journal of ClinicalHypnosis, 30, 104-116.
KLUFT, R. (1988). The phenomenology and treatment of ex-tremely complex multiple personality disorder. Dissocia-tion, 1(4), 47-58.
MAHL, G. F.. (1971). Psychological conflict and defense.New York: Harcourt, Brace, Jovanovich.
MmucmN, S. (1974). Families and family therapy. Cam-bridge: Harvard University Press.
MINUCHIN, S. (1981). Family therapy techniques. Cambridge:Harvard University Press.
PUTNAM, F. (1989). Diagnosis and treatment of Multiple Per-sonality Disorder. New York: Guilford.
PYNOOS, R. S. (1994). Post-traumatic stress disorder: A clini-cal review. Lutherville, MD: Sidran Press.
Ross, C. (1989). Multiple Personality Disorder: Diagnosis,clinical features and treatment. New York: John Wiley.
SCHMOLUNG, D. (1984). Human reactions to the Nazi concen-tration camps. Journal of Human Stress, 10, 108-120.
SEUGMAN, M. (1975). Helplessness: On depression, develop-ment and death. San Francisco: Freeman.
SHOHAM, V., RORBAUGH, M., & PATTERSON, I. (1995). Prob-lem and solution focused couple therapies: The MRI andMilwaukee models. In N. S. Jacobson and A. S. Gurman(Eds.), Clinical handbook of couple therapy (pp. 142-163).New York: Guilford.
SMALLS, C. (1975). The Wiz: The super soul musical Wonder-ful Wizard qfOz, Sound Recording (Music & lyrics CharlieSmalls), Atlantic Records.
VANDERKOLK, B. (1994). InR. Pynoos (Ed.), Post-traumaticStress Disorder: A clinical review (pp. 43-53). New York.
VAN DER KOLK, B. & GREENBERG, M. S. (1987). Psychologyof the trauma response: Hyperarousal, constriction, andaddiction to trauma reexposure. In van der Kolk (Ed.),Psychological trauma. Washington: American PsychiatricPress.
WATZLAWICK, P. (1967). Pragmatics of human communica-tion: A study of interactional patterns, pathologies, andparadoxes. New York: Norton.
502