Embed Size (px)
Citation preview

[CANCER RESEARCH 46, 2600-2605, May 1986]
Pulmonary Carcinoid Tumors: Enzymic Discriminants, Growth Rate, and Early Ageof Inception1
Olga Greengard,2 Jonathan F. Head, Steven L. Goldberg, and Paul A. Kirschner
Departments of Pediatrics, [O. G. and J. F. H.J, Pharmacology fO. G.J, and Surgery [P. A. K.J, Mount Sinai Medical Center, New York, New York 10029, andDepartment of Pathology [S. L. G.], Overlook Hospital, Summit, New Jersey 07901
ABSTRACT
Analyses of enzymes from various metabolic pathways in pulmonarycarcinoid tumors and radiological measurements of their volume increasewere compared with those for lung carcinomas of various cell types. Theresults describe new biochemical features in carcinoid tumors, presentthe first quantitative evidence for their slow growth rate (i.e., longdoubling time) in vivo, and show that measurement of 2 or 3 appropriateenzymes in biopsy samples can guard against instances in which carci-noids and adeno- or oat cell carcinomas are mistaken for one another onhistológica!examination.
The uridine kinase to thymidine kinase ratio as well as the /î-galacto-sidase concentration of carcinoid tumors were 5 times higher than ofcarcinomas, and their -y-glutamyl transpeptidase was below that of all 35adeno- and the 11 squamous cell carcinomas. Thymidine kinase, whichbears a quantitative inverse correlation to volume doubling time (irrespective of cell type), had much lower titers in the 9 carcinoids than inthe 6 oat cell carcinomas and reflects most clearly their very different(despite common histogenesis) clinical malignancy.
Owing to their long doubling time, carcinoid tumors on the averagerequired a much longer period (40.5 years) to attain final volume thandid carcinomas (17.8 years). The calculated mean age of the subjectswhen growth began, —0.5years (as opposed to 51 years for carcinomas),suggests a prenatal or early childhood inception for pulmonary carcinoidtumors.
INTRODUCTION
Among carcinoid tumors, those of the lung are unusual inthat very few of them (perhaps 1%) (1, 2) evoke the carcinoidsyndrome, the endocrine abnormalities frequently associatedwith gastrointestinal carcinoids. Histopathological examination of biopsy samples is, thus, the routine method of identifyingpulmonary carcinoids and, since diagnosis is often uncertain,electron microscopic confirmation is considered to be desirable.
Previous biochemical studies on carcinoid tumors were restricted to assay of hormones, neurotransmitters and associatedenzymes which are usually also present in oat cell carcinomasand which are thought to coniimi the postulated common celltype of origin of these two kinds of neoplasms (3-5). Thepresent investigations, on the other hand, focus mainly oncharacteristics of carcinoid tumors (sluggish growth rate andlow clinical malignancy) which contrast them more strikinglyfrom oat cell than from other carcinomas. In the course ofexaming biochemical features underlying the low growth potential of carcinoids we also identified, however, enzymic parameters which appear to distinguish carcinoids from lung carcinomas of any cell type and which are useful aids to differentialdiagnosis.
MATERIALS AND METHODS
Subjects and Pathological Characterization of Tumors. Ten subjectswith tumors diagnosed as carcinoids were studied. Nine of these pro-
Received 7/19/85; revised 1/9/86; accepted 1/31/86.The costs of publication of this article were defrayed in part by the payment
of page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
1Supported by USPHS Grant CA-25005 from the National Cancer Institute.1To whom requests for reprints should be addressed.
vided surgical biopsy samples for biochemical analyses. Re-examinationof their h¡siologica Icharacteristics in portions of each sample preservedfor this purpose confirmed the routine diagnosis. They were all welldifferentiated and exhibited ribbon-like, trabecular, glandular, or mixedarrangement of monomorphic cells typical for carcinoid tumors. Theargyrophilic reaction (not tested in one case) was always positive, andthere was no argentaffin reaction in the seven cases tested. Detectablemitotic frequency (2.3 and 1.4 per 10 high power fields) was found inonly two cases: the latter was the only one showing some (mull¡local)necrosis. None of the tumors showed more than minimal pleomorph-ism, nor was an abnormal nuclear/cytoplasmic ratio or disorganizedcellular architecture seen in any of the carcinoid tumors. The subjectsof these tumors received no cancer therapy other than the surgery whichyielded the samples for the present analyses.
In the histopathological examination of the carcinoma biopsy samples, cell type was assessed in the conventional manner, and they wereclassified according to the criteria of the WHO system, with thepresence of intracytoplasmic vacuoles of mucin being sufficient toclassify them as adenocarcinoma rather than large cell carcinoma.
Radiological Studies. As in our recent studies on human cancers (6),previously established methods (7-9) were used to determine tumorvolume (V) and volume DT.3 Volume is given by the formula V = 1/6
ir (di x d2 x d3). Diameters d, and d2 were the length and perpendicularwidth of the ellipsoid or circular shadow, measured with a mm ruler onstandard 72-inch target-film distance posterior-anterior roentgeno-grams. When a lateral roentgenogram was not available, the thirddiameter (d3) was taken as the average of d, and d:.
To obtain DT, log V (determined in sequential roentgenograms) wasplotted against time. In the case of carcinomas, these determinationswere restricted to cases in which presurgery chest X-rays were taken onthree or more occasions. Three of the carcinoid cases conformed tothese criteria. At the last measurement, the mean tumor volume of thecarcinoids and carcinomas was 22.4 ±13.2 (n = 10) and 70.1 ±23.4(n = 19) cm3, respectively.
As described previously (10-12), the duration of each tumor isobtained by multiplying DT (which is assumed to be constant throughout the existence of the tumor) with the number of doublings thatoccurred to grow from one cell (with an average volume of 10"' cm3)
to the volume (V,) at the time of the last measurement. The formulathus is: duration = DT x In (V,/10-9)/0.693.
Biochemical Methods. Previously described methods were used forthe assay (in extracts of fresh biopsy samples) of thymidine kinase (13),uridine kinase (14), hexokinase (15), aldolase (16), adenylate kinase(14), 7-glutamyl transpeptidase (17), /3-galactosidase (17), cathepsin c(17), protein (18), and DNA (19). The enzyme assays used systems,optimally fortified with substrates and cofactors, in which reaction rateremained constant during the measurements and was proportional tothe concentration of the enzyme. The results are presented as enzymeunits per g wet weight; units were nmol/min for thymidine kinase anduridine kinase, and umol/min for the other enzymes. Expression of theenzyme units per mg protein or DNA led to the same conclusions,because the protein and DNA concentration of the biopsy samples perg (which were routinely determined) varied over a relatively narrowrange and showed no appreciable, consistent differences between classesof neoplasms.
RESULTS
One group of enzymes quantified in this study are previouslyidentified indicators of pulmonary neoplasia: in biopsy samples
'The abbreviations used are: DT, doubling time; UK, uridine kinase; TK,thymidine kinase.
2600
on June 27, 2020. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

ENZYME PATHOLOGY OF PULMONARY CARCINOIDS
Table 1 Eniymic comparison of carcinoids, carcinomas, and non-neoplastic lung biopsy samples
In the first part of the table, the values are means or refer to single individuals. These means, divided by (see asterisks) means for the same enzyme in column 3("all cell types"), are listed in the lower part of the table.
CarcinomaEnzymesTKUKPSP*HKALDAKTK/TK«UK/UK*PSP/PSP*HK/HK«ALD/ALD*AK/AK«Normal
lung0.30±0.02°(73)*5.58
±0.35(68)46±2(70)0.56±0.04(42)0.56±0.04(27)20.6±1.5(36)Carcinoid0.62
±0.14(9)48.2±5.8(10)135±29(7)2.21
±0.49(3)2.02±0.28(4)23.7,22.00.21.60.51.00.8All
celltypes*3.32
±0.45(82)c29.2
±2.5(76)269±21(76)2.14±0.17(61)2.66±0.17(50)12.1±0.76(49).0.0.0.0.01.0Adenocarcinoma2.53
±0.37(50)24.0±2.6(48)234±26(47)1.67±0.14(36)2.66±0.25(29)12.6±1.0(31)0.80.80.90.81.01.0Squamous3.30
±0.09(20)35.6±5.4(20)300±43(20)2.96±0.41(17)2.75±0.33(14)13.1±1.4(11).0.2.1.4.0.1Oat
cell3.98
±0.64(6)66.9±9.5(6)396±55(6)2.56,
2.072.26,1.5410.61.22.31.5
•Mean ±SE.* Numbers in parentheses, number of subjects.' The 82 cases include large cell and mixed cell type carcinomas, as well as those in the last three columns."*PSP. phosphoserine phosphatase, HK, hexokinase, ALD, aldolase; AK, adenylate kinase.
of human lung carcinomas of any cell type, the concentrationsof the first 5 enzymes in Table 1 were higher and that of thelast one was lower than in normal lung samples (14, 20). Thepresent results showed that carcinoid tumors can also be recognized as "neoplastic" by measurements of some of these
enzymes (compare uridine kinase, phosphoserine phosphatase,hexokinase, and aldolase in the first and second column offigures).
Previous comparison of the same parameters in a variedspectrum of pulmonary carcinomas showed that they constitutea coordinated group, in that the distribution among individualtumors of the different enzymes correlated with one another(14, 20). The same was true for the larger number of casesstudied by now; however, carcinoid tumors did not fit the samerelationships. This is apparent, for example, from the meanvalues for the first 3 enzymes in Table 1; the concerted gradationthey undergo from adeno- through squamous cell to oat cellcarcinomas clearly does not extend to carcinoid tumors, in thatthymidine kinase or phosphoserine phosphatase would rankthem below adenocarcinomas, while uridine kinase would rankthem above squamous cell carcinomas. From the lower part ofTable 1, which is unencumbered by the absolute activities forthe different enzymes (see legend), the overall pattern is evidentat a glance; these standardized values for the different enzymesare similar to one another in adenocarcinomas (0.8 to 1.0) orin squamous cell carcinomas (1.0 to 1.4), whereas in carcinoidtumors they encompass an over 8-fold range (0.2 to 1.6), forthey are relatively rich, for example, in glycolytic enzymes orUK but poor in TK. As seen from the data for individualneoplasms in Fig. 1, a high UK/TK ratio is a striking characteristic of carcinoid tumors; only 2 overlapped with the rangefor carcinomas.
High /3-galactosidase combined with low 7-glutamyl trans-peptidase and cathepsin c activities are additional unusual characteristics of carcinoid tumors (Fig. 2). It may be seen that the7-glutamyl transpeptidase of the eight carcinoid tumors wasbelow that of the 35 adenocarcinomas or 14 squamous cellcarcinomas, and it was also below that of normal lung (Fig.2b). Similarly, in the 5 carcinoids measured, cathepsin c was atlower levels than in all but one of the 42 carcinomas (Fig. 2c).Among carcinomas, the oat cell type had the lowest values inFig. 2, b and c; it is possible, therefore, that these two enzymesreflect the common histogenesis of carcinoid tumors and oatcell carcinomas. This does not apply to /3-galactosidase (Fig.2a) or to the UK/TK ratios (Fig. 1), since the values for both
2601
300
260-
140
120
100
80
60
40
20
jt_ï_N O C
Fig. 1. Contrasting uridine kinase/thymidine kinase ratio of pulmonary carcinoids and carcinomas. Each solid circle refers to a biopsy sample from acarcinoid tumor (C) or a carcinoma of the adeno- (lì.squamous cell (5), or oatcell (O) types; line indicates mean. The open circle above W is a mean for non-neoplastic lung samples from 79 individuals. Bars, SE.
£¿UU200018001600140012001000800600400200n.
a-.-i•-•
'•
l\•
i;"
i Sb.1;..ÃŒM
—v
-v
:¡c.-_-•---:
:'A
T-À>•*tt
- . A
Fig. 2. Enzymic discriminants of pulmonary carcinoid tumors. Each value for/3-galactosidase (a). 7-glutamyl transpeptidase (b), and cathepsin c (c) refers to apulmonary carcinoid or to a carcinoma of the indicated cell type (see Fig. 1,legend). Lines indicate mean. Open circles refer to mean values for normal samplesfrom 66 (a), 61 (b), or 32 (c) lungs. Bars, SE. The absolute units on the ordinateof c are one-half of those on the ordinates of a and b.
on June 27, 2020. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

ENZYME PATHOLOGY OF PULMONARY CARCINOIDS
of these parameters in oat cell carcinomas were in the middleof the range for all carcinomas and below that in each of thecarcinoid tumors.
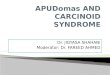
Sequential roentgenograms permitting tumor diameter measurements were traced for 3 of the pulmonary carcinoid cases.The results in Fig. 3 (which include two carcinomas for comparison) show that the volume doubling time (DT) of thecarcinoids were 495, 515, and 717 days. They were thus aboveor in the extreme upper range (20 to 500 days) (12, 21, 22) ofDTs measured previously in a large and varied population oflung cancers which did not include carcinoid tumors. In thatvaried population, the DT of any given tumor was found to beconstant; i.e., log volume increased linearly with time (see"Discussion"). The results in Fig. 3 indicate that this is also
true for carcinoid tumors. As in the case of carcinomas (illustrated with two examples in Fig. 3) the points fell close to thestraight lines; the carcinoid for which sequential chest X-rayson 5 different occasions were available in the course of 6 yearsmay attest most reliably to an unchanging, exponential growthrate.
Lower TK content (Table 2) may be looked upon as furtherevidence for the long DT of pulmonary carcinoids, for in recentstudies log TK concentration was shown to bear a significantinverse correlation to the log of the DT (measured radiologi-cally) of human lung neoplasms (6). Carcinoid tumors (Fig. 4)also appear to fit this linear relationship. The regression line inFig. 4 was, therefore, used to read off the DT of the carcinoidtumors (as well as of oat cell carcinomas) for which no appropriate roentgenograms were available. The results, togetherwith the DTs of all human lung neoplasms that we studied sofar, are listed in Table 2. It may be seen that the DT of the first6 carcinoids is uniformly long (over 495 days), while that of the4 others was appreciably shorter. These differences cannot beexplained on histological grounds, since all 10 carcinoids hadsimilar microscopic and staining characteristics (see "Materialsand Methods"). One of the two carcinoids with detectable but
°°0 300 600 900 1200 1500 1800 2100
DAYS
Fig. 3. Size of pulmonary carcinoids in sequential roentgenograms. Solidsymbols refer to three carcinoid subjects with chest X-rays on at least 3 differentoccasions. For comparison, examples of two carcinomas (open symbols) areincluded. Volume (ordinale) was calculated (see "Materials and Methods") from
diameters in roentgenograms taken at intervals indicated by the abscissa, where0 is the time of the first measurement.
Table 2 Tumor doubling time and duration of various lung neoplasms inindividual subjects
The list includes all carcinoid tumors and oat cell carcinomas studied; of thelarger number of non-oat cell carcinomas subjected to biochemical analyses, thelist includes only those for which both TK and radiological data were available.For the sake of uniformity, all DTs (except in case 1) are based on TK (i.e., usingthe regression line in Fig. 4). The calculation of duration, by multiplying DT withthe number of doublings required to attain final volume, was as describedpreviously (Refs. 10-12; see also "Materials and Methods"). "Age of inception"is obtained by subtracting duration from "age of surgery." BA, S, and A refer to
bronchioloalveolar cell, squamous cell, and adenocarcinoma, respectively.
SubjectNeoplasmPulmonaryneoplasmsCarcinoid
tumorTK(units/g)0.300.300.320.320.340.660.711.081.54DT(days)(495)566566544544518302285202152Numberofdoub
lings28.532.035.428.632.634.332.532.437.029.0Duration(yr)39505543494927252012Age
atsur
gery(yr)47693169332452223221Age
atincep-ofneo
plasm(yr)819-2426-16-2525-3129Non-oat
cellcarcinomaBAASSASASAASAASA0.500.530.560.830.860.981.571.841.872.923.353.455.65Oat
cell carcinoma2.24IQO8.06.0f
4.0*CIDw
2.0to¡
1.0LJ8*
6
I4X.22.823.474.044.606.70'
0'•\«0----1
13793613482512452201501321309081795311293797063461
'1s.\A..AS
\,
132.131.733.333.531.434.336.030.735.236.436.936.034.337.335.437.238.635.034.3•A•S•AVAS\
«sS*A\S'A\,
,34313223212115111298851198764'
'1ABA
\ •\i
i 151638175747563806176796661595265666866-------1732495253544869496771585648435759626210 20 40 60 100 200 400 600 1000
VOLUME DOUBLING TIME (days)
Fig. 4. Quantitative relationship of thymidine kinase to volume DT. Thetriangle and square refer to carcinoid tumors (see same symbols in Fig. 3); eachof the other points refers to a carcinoma of the bronchioloalveolar (lìI), squamouscell (S), adenocarcinoma (A), or oat cell (O) type. The calculated regression isbased on all 17 points.
very low mitotic frequency is the 8th on the list; however, theother (which, exhibiting signs of necrosis, might be considered"atypical") had a long (544 days) DT.
It should be noted that the radiological measurement of avery long DT (i.e., of very small volume changes between two
2602
on June 27, 2020. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

ENZYME PATHOLOGY OF PULMONARY CARCINOIDS
chest X-rays) tends to be less accurate, so that differences inDT among carcinoids or slowly growing carcinomas cannot beestablished as reliably as among relatively fast growing neoplasms. To some extent, this also applies to the-biochemical
method in that the assay of tumors with TK activities close tothe very low values in normal lung is relatively inprecise.However, under- and overestimation should be equally likely.For this reason, and also because the present values (whetherbased on TK or on roentgenograms) for the adeno-, squamouscell, and oat cell carcinomas are in agreement with previousstudies (7, 22, 23), it is safe to conclude that the DT of thecarcinoid tumors is above or in the upper range of that forcarcinomas. Consequently, duration (i.e., time to attain finalsize) was above two decades for all but one of the carcinoids(Table 2). The generally lower but variable duration of carcinomas is in agreement with previous radiological studies showing that most of these begin to grow in adulthood, while someof them (represented here by the bronchioloalveolar cell type)trace back to the late teens or early 20s. The error in theseresults may amount to a few years for most carcinomas but canbe much greater for slowly growing tumors, because the abovementioned inaccuracies in their DT measurement are multipliedwhen calculating duration (see "Materials and Methods"). The
much longer duration of the third, fifth, and sixth carcinoidthan the age of subject is patently impossible. The second,fourth, and seventh carcinoid in Table 2, on the other hand,might have begun to grow much earlier than indicated (lastcolumn), since underestimation of duration (which never yieldsobviously impossible results) is as likely as overestimation.Because of this symmetry in the error, the results were averagedfor groups of tumors. It may be seen from Table 3 that themean DT of the carcinoid tumors was not only strikingly longerthan of oat cell carcinomas but also showed a statisticallysignificant difference from that of the non-oat cell carcinomas.Since the number of doublings was similar, the mean durationof the carcinoid tumors was also significantly longer (40.5 years)than of the non-oat cell (18.4 years) as well as of the oat cell(6.5 years) carcinomas. The consequent difference with respectto age of inception, being magnified by the younger age of thecarcinoid than of the carcinoma subjects, is even more striking;—0.5years (i.e., midgestation) and about 50 years are therespective calculated mean ages when the growth of the carcinoids and of the various carcinomas began.
DISCUSSION
The biochemical constituents in Table 1, as demonstrated byanalysis of surgical samples from 39 patients (20), show an
intercorrelating distribution among individual human lung carcinomas; tumor to tumor elevations (above normal lung) inenzymes involved in nucleic acid (TK and UK) and non-essential amino acid synthesis (phosphoserine phosphatase) werecoordinated with one another and were matched by commensurate variations of enzymes (hexokinase, aldolase, and adenyl-ate kinase) involved in the production of energy necessary forthese synthetic processes. This coordination does not quiteextend to pulmonary carcinoid tumors. Their high capacity forthe utilization of uridine and cytidine and for glycolysis (asindicated by relatively high uridine kinase, hexokinase, andaldolase concentrations) is "wasted" in that thymidine kinase,
catalyzing the formation of another essential nucleotide, is atdisproportionately low levels (Table 1, Fig. 1). It is likely,therefore, that the concentration of thymidine kinase limitsnucleic acid synthesis and thus the growth rate of pulmonarycarcinoid tumors.
The quantitative evidence obtained here for the much longervolume DT in vivo of pulmonary carcinoid tumors than of oatcell carcinomas is in accord with their contrasting clinicalmalignancy. Common histogenesis, which precludes the use ofneuroendocrine markers as discriminants, is probably the reason why pulmonary carcinoids and oat cell carcinomas have insome instances been mistaken for one another upon routinehistological examination (2, 24). This prognostic error couldclearly be avoided by radiological measurement of DTs. Theproblem, that sequential chest X-rays over a long enough period(of well outlined tumors with regular, ellipsoid shape) are veryrarely available, can also be overcome. As indicated by the non-overlapping thymidine kinase values in Table 2, measurementof this enzyme (in routinely available biopsy samples) shouldprovide an unequivocal distinction of pulmonary carcinoidsfrom oat cell carcinomas.
Some non-oat cell carcinomas, however, may have equallyslow growth rates (Table 2), so that instances in which carcinoids and adeno- or squamous cell carcinomas are mistaken forone another on histopathological examination (25) would notnecessarily be avoided by direct DT or thymidine kinase measurements. Nor would qualitative tests for neuroendocrinemarkers be necessarily conclusive, since they are also positivein some adeno- or large cell carcinomas (26). There is, however,a set of quantitative biochemical characteristics (low 7-glutamyltranspeptidase and cathepsin c coupled with high /3-galactosid-ase and UK/TK ratio; see Figs. 1 and 2) which must beassociated with histogenesis rather than the slow growth ofcarcinoid tumors, since 7-glutamyl transpeptidase, cathepsin c,0-galactosidase, or UK/TK do not show any quantitative correlation to the neoplasms' doubling time or mitotic frequency.
Table 3 Age of inception of pulmonary carcinoid tumors and carcinomasThe age of the subjects and the number of doublings used to calculate duration in Table 2 are shown. To be more comparable with previous publications, the mean
DT and thus the mean duration are based on the radiological measurements (see Figs. 2 and 3) whenever possible; however, the data based on TK only as a measureof DT (see Table 2) are shown in parentheses.
PulmonaryneoplasmsCarcinoids
Non-oat cell carcinomas
Oat cell carcinomasDT(days)0459±58*(10)c
(409 ±57)(9)200
±27(13)°
(194 ±32)(13)65
±15(6)"
(77 ±9) (6)No.
of doublingsto linaivolume32.2
±0.9 (10)
34.0 ±0.6(13)
36.3 ±0.7 (6)Duration
(yif40.5
±5.3 (10)(36.5 ±5.1)(9)18.4
±2.4 (13)°
(17.7 ±2.8)(13)6.5
±1.5(6)°
(7.7 ±1.0) (6)Age
ofsubject(yr)40.0
±5.8 (10)
69.6 ±2.6(13)62.7
±2.5 (6)Age
ofinception(yif0.5
±7.6(10)(2.6 ±6.8)(9)51.2
±4.2 (13)°
(51.9 ±4.1)(13)56.3
±3.6 (6)"
(55.2 ±3.2) (6)" Values for carcinoid tumors were significantly different (P < 0.001 by Student's Mest, 2-tail) from those for non-oat cell or oat cell carcinomas.* Mean ±SE.c Numbers in parentheses, number of subjects.
2603
on June 27, 2020. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

ENZYME PATHOLOGY OF PULMONARY CARCINOIDS
The reason why these particular enzymic parameters appear toreflect the unusual cell type, or perhaps the unusually early ageof inception (Table 3), of the pulmonary carcinoid tumorsremains to be investigated. In the meantime, the results areonly of pragmatic significance: they show that by quantifying 3enzymes, e.g., 7-glutamyl transpeptidase (or cathepsin c) anduridine kinase (or /3-galactosidase), as well as thymidine kinase,one can differentiate pulmonary carcinoids from both non-oatcell and oat cell carcinomas (Figs. 1 and 2, Table 2) and obtainat the same time an estimate of volume DT in vivo (Fig. 4).When cell type is equivocal, electron microscopy can yield asconclusive an identification, but not in time to influence thesurgeon's decision as to the extent or advisability of resection.
The rapidity of the assay procedures is thus a practical advantage of the above enzymic discriminants.
Thymidine kinase (TK) and other enzymes with direct orindirect involvement in nucleic acid synthesis have long beenknown to correlate quantitatively with the growth rate of s.c.rat tumors of a variety of histogenesis (13, 27, 28). In humanlung tumors too, the significant inverse correlation between logTK and log volume DT extended over tumors of a variety ofcell types (6; Fig. 4). Indications of such a relationship couldbe obtained even without volume measurements, in that in 37lung tumors with diverse histogenesis (20) and in the 88 studiedby now, there was a highly significant correlation (r = 0.322, P= 0.002) between log mitotic frequency and TK concentration.Thus, not only the direct measurements of DT but also thosebased on TK content (i.e., read off the straight line in Fig. 4)provide reliable indication of the very slow growth rate (i.e.,long DT) of the pulmonary carcinoids. The linear increase oflog volume with time in the few with three or more sequentialchest roentgenograms (Fig. 3), as well as the similarly low TKof the seven, irrespective of whether tumor size happened to besmall or large at the time of sampling, was in accord with theprinciple [established for a variety of lung cancers (7, 29-32)]that the DT of any given human tumor remains constant duringthe clinical course of the disease. The present validation of thisprinciple for carcinoid tumors re-emphasizes the obvious butnoteworthy conclusion first drawn by Collins et al. (32) in 1956,namely, that unchanging long DT, rather than unpredictableperiods of dormancy, explains the very slow progression ofsome human cancers.
As shown in early studies by Mottram (33) on mice, the timethat experimentally induced tumors require to attain palpablesize is directly related to the growth rate they exhibit afterattaining this size. This growth rate was, therefore, used byCollins et al. (32) to extrapolate back to the time of inceptionof human neoplasms, i.e., to the first appearance of the cancerous cell which (in accord with clonal origin) gave rise to thattumor. They assumed an average cell volume of IO"9 cm3 sothat growth to 1 cm3 (the usual minimal volume at diagnosis)
involves 30 doublings and a period of 30 times the days requiredfor each doubling. Massive evidence (7, 29-32, 34) has been
gathered since then that the constancy of DT of any individualhuman tumor (seen up to a diameter of 10 cm) begins by atleast the 0.5-1.0-cm stage; only before this stage is the constancy of DT an assumption rather than a demonstrated fact.
For the carcinomas now studied, duration (Table 2 and 3)was in agreement with the previously reported ranges andmeans (e.g., 18.6 years) ( 12), even though there are complicatingfactors which (e.g., tumor heterogeneity, necrosis, or medicalhistory) may introduce inaccuracies in the calculation appliedin such studies. It may also be noted that (as discussed under"Results") in the case of slowly as opposed to quickly growing
tumors the error in DT determination is considerable, thoughwith an equal likelihood of over- and underestimation. Thus,while the calculated duration of some individual pulmonarycarcinoids was patently impossible, the mean value of 40.5years was reasonable in that it was similar to some slowlygrowing carcinomas (10, 12; see also Table 2) and, despite thelarge standard error, significantly different from the mean forall non-oat (as well as oat) cell carcinomas (Table 3). Thesubjects' age at the time when their carcinoids began to growthus averages to -0.5 years (Table 3), suggesting the prenatal
origin of several of these carcinoids.In view of the above mentioned errors in the measurements,
it should be noted that several lines of evidence independentfrom such measurements have pointed to the longer DT, andthus duration, of pulmonary carcinoid tumors. Minimal mitoticfrequency is, of course, one of these. Clinical observationsprovide extensive documentation of the very slow growth rateof this carcinoid (5, 35). The associated statistical evidence fora generally favorable prognosis (36, 37) is equally important;the 91% 10-year (1) and 66% 25-year (38) survival is in clearcontrast to even adenocarcinomas, the least rapidly lethal groupamong carcinomas. Pulmonary carcinoids are not free of met-astatic potential (1, 39), but in follow up studies the majorityof individuals were found to be disease free 20 years after theresection of a pulmonary carcinoid (25, 37). This, and the casein which a metastasis of a pulmonary carcinoid became detectable 32 years after resection of the primary (35), is also inaccord with the present results. For, if DT is 400-500 days,then regrowth from a cell left behind at surgical resection wouldnot attain clinically detectable size until about 30 years later.
Some carcinomas have been growing for 20-30 years, i.e.,from the time the subjects were in their 20s (10, 12). The muchyounger average age [38.9 (1) or 40 (40) years] of pulmonarycarcinoid subjects would suggest that their tumors began togrow in their teens (or before), but their clinically evidencedunusually slow growth rate (see above) makes an even earlier,perinatal inception plausible. Thus, the present hypothesiscould have been posed before the results reported here andwithout the perhaps questionable assumptions necessary for thecalculation of duration. However, one has tended to associateearly inception with quickly growing pediatrie tumors. Thismay have obscured the principle that slower growing tumorsoriginating at the same early time would not be "pediatrie"
(because they would not become detectable in childhood) andthat slow growth rate (i.e., long DT) is, in fact, what shouldlead one to suspect the developmental origin of an "adult"
tumor. In the case of pulmonary carcinoids there is an additional reason for this suspicion, one independent from slowgrowth rate. The provenance of carcinoids from the argyrophilicKulchinsky cells (3, 4) found in the bronchial lining of humans,especially infants (41), is consistent with developmental origin.For, the large number of these Kulchinsky cells in the fetalhuman lung (42), and their extreme rarity in the bronchi ofinfants beyond the age of 1 year (43), suggests that neoplastictransformation leading to pulmonary carcinoid tumors may bea more probable event in perinatal life than later on.
REFERENCES
1. Markel, S. F., Abell, M. R., Haight, C., and French, A. J. Neoplasms ofbronchus commonly designated as adenomas. Cancer (Phila.), 17: 590-608,1964.
2. Smith, R. A. Bronchial carcinoid tumours. Thorax, 24: 43-50, 1969.3. Bensch, K. G., Corrin, B., Pariente, P. R., Spencer, H., and Path, F. C. Oat-
cell carcinoma of the lung: its origin and relationship to bronchial carcinoid.Cancer (Phila.), 22:1163-1172, 1968.
2604
on June 27, 2020. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

ENZYME PATHOLOGY OF PULMONARY CARCINOIDS
4. Bensch, K. G., Gordon, G. B., and Miller, L. R. Electron microscopic andbiochemical studies on the bronchial carcinoid tumor. Cancer (Phila.), 18:592-602, 1965.
5. Godwin, J. D. Carcinoid tumors: an analysis of 2,837 cases. Cancer (Phila.),36: 560-569, 1975.
6. Greengard, O., Head, J. F., Goldberg, S. L., and Kirschner. P. A. Biochemicalmeasure of the volume doubling time (DT) of human pulmonary neoplasms.Cancer (Phila.), 55: 1530-1535, 1985.
7. Meyer, J. A. Collective review: growth rates in pulmonary tumors. Ann.Thorac. Surg., 14:309-322, 1972.
8. Chahinian. P. and Israel, L. Rates and patterns of growth of lung cancer. In:L. Israel and P. Chahinian (eds.). Lung Cancer: Natural History. Prognosis,and Therapy, pp. 63-79. New York: Academic Press, Inc., 1976.
9. Weiss, W. The Philadelphia pulmonary neoplasm research project. Appi.Radio!.,«: 50-141. 1979.
10. Collins, V. P. Time of occurrence of pulmonary metastasis from carcinomaof colon and rectum. Cancer (Phila.). 15: 387-395, 1962.
11. Spratt, J. S., Spjut, H. J., and Roper. C. L. The frequency distribution of therates of growth and the estimated duration of primary pulmonary carcinomas.Cancer (Phila.), 16: 687-693, 1963.
12. Garland. L. H., Coulson. W., and Wollin, E. The rate of growth and apparentduration of untreated primary' bronchial carcinoma. Cancer (Phila.), 16:694-707, 1963.
13. Machovich, R. and Greengard, O. Thymidine kinase in rat tissues duringgrowth and differentiation. Biochim. Biophys. Acta, 290: 375-381. 1972.
14. Greengard. O., Head. J. F.. and Goldberg, S. L. Uridine kinase, adenylatekinase. and guanase in human lung tumors. Cancer Res., 40: 2295-2299,1980.
15. Jamdar. S. C. and Greengard, O. Premature formation of glucokinase indeveloping rat liver. J. Biol. Chem., 245: 2779-2783, 1970.
16. Schapira. F., Dreyfus, J. C.. and Schapira, G. Anomaly of aldolase in primaryliver cancer. Nature (Lond.), 200: 995-997, 1963.
17. Seymour, C. A. and Peters, T. J. Enzyme activities in human liver biopsies:assay methods and activities of some lysosomal and membrane-bound enzymes in control tissue and serum. Clin. Sci. Mol. Med., 52: 229-239, 1977.
18. Lowry. O. H.. Rosebrough, N. J.. Fair, A. L., and Randall, R. J. Proteinmeasurement with the Folin phenol reagent. J. Biol. Chem., ¡93:265-275,1951.
19. Hinegardener. R. T. An improved fluorometric assay for DNA. Anal.Biochem., 39: 197-201, 1971.
20. Greengard, O., Head, J. F., Goldberg. S. L., and Kirschner, P. A. Enzymepathology and the histological categorization of human lung tumors: thecontinuum of quantitative biochemical indices of neoplasticity. Cancer(Phila.), 49: 460-467, 1982.
21. Spratt, J. S. and Spratt, 1. L. Rate of growth of pulmonary métastasesandhost survival. Ann. Surg., 159: 161-171, 1964.
22. Weiss, W., Boucot, K. R., and Cooper, D. A. Growth rate in the detectionand prognosis of bronchogeneic carcinoma. J. Am. Med. Assoc.. 198: 1246-1252, 1966.
23. Strauss, M. J., Janis, M. G., and Moran, R. E. Tumor biology of lung cancer.In: C. C. Harris (ed.), Pathogenesis and Therapy of Lung Cancer, Vol. 10,
pp. 611-651. New York: Marcel Dekker, 1978.24. Fisher, E. R., Palekar. A., and Paulson. J. D. Comparative histopathologic.
histochemical, electron microscopic and tissue culture studies of bronchialcarcinoids and oat cell carcinomas of lung. Am. J. Clin. Pathol., 69: 165-172, 1978.
25. Blondal, T., Grimelius, L., Nou. E., Wilander, E., and Aberg, T. Argyrophilcarcinoid tumors of the lung. Chest, 78: 840-844, 1980.
26. Baylin, S. B., Weisburger, W. R., Eggleston, J. C., Mendelsohn, G., Beaven,M. A., Abeloff, M. D., and Ettinger, D. S. Variable content of histaminase,L-dopa decarboxylase, and calcitonin in small-cell carcinoma of the lung. N.Engl. J. Med., 299: 105-110. 1978.
27. Knox, W. E. Enzyme Patterns in Fetal, Adult, and Neoplastic Rat Tissue.Basel: Karger AG, 1976.
28. Weber, G. Enzymology of cancer cells. N. Engl. J. Med., 290: 486-551,1977.
29. Charbit, A., Malaise, E. P., and Tubiana, M. Relation between the pathological nature and the growth rate of human tumors. Eur. J. Cancer, 7: 307-315, 1971.
30. Schwartz, M. A biomathematical approach to clinical tumor growth. Cancer(Phila.), 14:1272-1294, 1961.
31. Breur, K. Growth rate and radiosensitivity of human tumours. I. Growth rateof human tumours. Eur. J. Cancer, 2: 157-171, 1966.
32. Collins, V. P., Loeffler, R. K., and Tivey, H. Observations on growth ratesof human tumors. Am. J. Roentgenol., 76: 988-1000. 1956.
33. Mottram, J. C. On the origin of tar tumours in mice, whether from singlecells or many cells. J. Pathol. Bacteriol., 40:407-414, 1935.
34. Chahinian, P. and Israel, L. Prognostic value of doubling time and relatedfactors in lung cancer. In: L. Israel and P. Chahinian (eds.). Lung Cancer:Natural History'. Prognosis, and Therapy, pp. 95-106. New York: Academic
Press. Inc., 1976.35. Altschuler, M., Warner, R. R. P., and Kirschner, P. A. Resection of medias-
tinal metastasis of malignant bronchial carcinoid 32 years after pneumonec-tomy. NY State J. Med., 78: 2205-2210, 1978.
36. O'Grady, W. P., McDiritt, R. W., Holman, C. W., and Moore. S. W.Bronchial adenomas. Arch. Surg., 101: 558-561, 1970.
37. Borggreve, J. R. A bronchial adenoma of 33 years standing. Ned. Tijdschr.Geneeskd., 110: 1532-1535, 1966.
38. Okike, N., Bernal/. P. E., and Woolner, L. B. Carcinoid tumors of the lung.Ann. Thorac. Surg., 22: 270-277, 1976.
39. Mills, S. E., Walker, A. N., Cooper, P. H., and Krön,I. L. Atypical carcinoidtumor of the lung. A clinicopathologic study of 17 cases. Am. J. Surg.Pathol., fi: 643-654, 1982.
40. Balsón, J. F.. Gale, J. W.. and Hickey R. C. Bronchial adenomata. Arch.Surg., 92: 623-630, 1966.
41. Froelich. F. Die "Helle Zelle" der Bronchialschleimhaut und ihre Ziehungenzum Problem der Chemoreceptoren. Frankf. Z. Pathol., 60: 517-559, 1949.
42. Cutz, E. and Conen, P. E. Endocrine-like cells in human fetal lungs: anelectron microscopic study. Anal. Ree., 173: 115-122, 1972.
43. Feyrter, F. Zur Pathologie des argyrophilen Helle-Zellen-Organes im Bronchialbaum des Menschen. Virchows Arch. Pathol. Anat. Physiol. Klin. Med..525:723-732,1954.
2605
on June 27, 2020. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1986;46:2600-2605. Cancer Res Olga Greengard, Jonathan F. Head, Steven L. Goldberg, et al. Rate, and Early Age of InceptionPulmonary Carcinoid Tumors: Enzymic Discriminants, Growth
Updated version
http://cancerres.aacrjournals.org/content/46/5/2600
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/46/5/2600To request permission to re-use all or part of this article, use this link
on June 27, 2020. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from