Embed Size (px)
Citation preview

www.elsevier.com/locate/autrev
Autoimmunity Reviews 3 (2004) 313–320
Pulmonary hypertension in autoimmune rheumatic diseases
Patricia E. Carreira
Servicio de reumatologıa, Hospital 12 de Octubre, Avda. de Cordoba S/N, 28041 Madrid, Spain
Received 4 November 2003; accepted 8 November 2003
Available online 20 December 2003
Abstract
Arterial pulmonary hypertension (PH) might be a complication of some autoimmune rheumatic diseases, specially
systemic sclerosis. This form of arterial PH is indistinguishable from primary PH, characterised by the presence of plexiform
lesions. Although for many years plexiform lesions have been considered end-stage scarring lesions, they are composed by
actively proliferating endothelial cells that share many features with cancer cells. Endothelial cells within plexiform lesions
in all forms of arterial PH show a decrease in the expression of vasodilator and anti-proliferative factors, and an increase in
the expression of vasoconstrictor and angiogenic and mitogenic factors. These cells also show important alterations in
growth and apoptosis key regulatory genes. Plexiform lesions are surrounded by inflammatory cell infiltrates, probably
providing cytokines that may contribute to the endothelial cell proliferative process. All these data suggest that arterial PH
might be seen as a proliferative endothelial cell process, which would open new therapeutic approaches for this devastating
disease.
D 2003 Elsevier B.V. All rights reserved.
Keywords: Pulmonary hypertension; Systemic sclerosis; Endothelial cells
Pulmonary hypertension (PH) is present when current disease: arterial PH, PH with left heart
the median pulmonary artery pressure is higher
than 25 mmHg at rest or higher than 30 mmHg
during exercise [1]. Multiple classifications have
been developed for this disease, since PH can arise
primarily or secondarily to different pulmonary
pathologies. In 1998, a WHO expert meeting took
place in Evian, where a more descriptive classifi-
cation was proposed [2]. This classification has
been reviewed in a recent new WHO meeting, in
Venice in June 2003. The new proposal for PH
classification includes five main groups, according
to the presence or absence of additional or con-
1568-9972/$ - see front matter D 2003 Elsevier B.V. All rights reserved.
doi:10.1016/j.autrev.2003.11.004
E-mail address: [email protected] (P.E. Carreira).
disease, PH with lung disease and/or hypoxemia,
PH due to chronic thromboembolism and a mis-
cellaneous group (Table 1).
Rheumatologists are interested in this condition
because it can appear in some autoimmune diseases.
Arterial PH associated to autoimmune diseases is
clinically, hemodynamically and prognostically indis-
tinguishable from primary PH [3], and most therapeu-
tic strategies used in primary PH have confirmed its
efficacy in rheumatic diseases associated PH [4],
specially in systemic sclerosis (SSc) [5].
The normal lung vascular bed is a low-pressure
circuit, able to adapt to increased blood flow by
dilation of small arterioles, without increasing vascu-

Table 1
Proposal of clinical classification
(1) Pulmonary arterial hypertension (PAH)
(a) Idiopathic
(b) Familiala
(c) Related to collagen vascular disease, CHD, portal
hypertension, HIV, drugs and toxins, other
(d) PAH with significant venous and/or capillary
involvement
(e) Persistent PH in the newborn (PHN)
(2) PH with left heart disease
(a) Atrial ventricular heart disease
(b) Valvular heart disease
(3) PH with lung disease and/or hypoxemia
(a) Chronic obstructive pulmonary disease
(b) Interstitial lung disease
(c) Sleep disorders; alveolar hypoventilation;
chronic exposure to high altitude
(d) Developmental abnormalities
(4) PH due to chronic thromboembolism
(a) Thromboembolic obstructions of proximal
pulmonary arteries
(b) Thromboembolic obstructions of distal
pulmonary arteries
(c) Pulmonary embolism of other nature (tumour,
parasites, foreign material)
(5) Miscellaneous
(a) Sarcoidosis, histiocytosis X, lymphangiomatosis,
comprehension of pulmonary
vessels (adenopathies and tumours,
fibrosing mediastinitis), Type 1
glycogen storage diseases, lipid storage
diseases such as Gaucher’s disease
Third World Symposium on Pulmonary Hypertension, Venice, June
23–25, 2003.a Familial PAH is defined as a demonstrated familial presence of
PAH (at least one affected relative). In the future, a positive genetic
blood test (BMPR2 mutation?), may define this category.
P.E. Carreira / Autoimmunity Reviews 3 (2004) 313–320314
lar resistances. In arterial PH, the pressure in pulmo-
nary arteries is already high at rest, but has a dispro-
portionate increase during exercise, due to the
structural inability to accommodate the excessive
blood flow. This progressively stresses the right side
of the heart, leading to right ventricular hypertrophy
and eventually to right heart failure.
Most of the current knowledge on arterial PH
comes from studies done in primary PH, but many of
these findings have also been confirmed in PH asso-
ciated to autoimmune diseases. The aim of the present
work is to review the cellular and molecular mecha-
nisms implicated in arterial PH development, especial-
ly focused in the similarities and differences between
primary and autoimmune diseases associated PH.
1. Genetics in pulmonary hypertension
Genetic predisposition has been found in familial
PH, transmitted as an autosomal trait with low
penetrance. A heterozygous germ line mutation in
bone morphogenetic protein (BMP) receptor 2, a
member of the transforming growth factor h (TGF-
h) family, has been identified in 60% of familial cases
[6,7] and 25% of sporadic cases [8]. BMPs act
binding to BMPR1A and BMPR2 receptors,
expressed on cell surfaces adjacent to each other.
BMP binds to BMPR2 extracellular domain, which
activates BMPR1A intracellular domain. The activat-
ed BMPR1A phosphorilates the cytoplasmic signal-
ling protein Smad5, which binds to Smad4 and
migrates to the nucleus, where together with other
nuclear binding factors regulates DNA transcription.
The effect of activated BMP receptors depends on the
cell type and can result in either transcription activa-
tion or inhibition. Mutations in familial and sporadic
PH patients are found at highly conserved sites in
BMPR2, and predict either to alter the heterodimeri-
zation of this receptor with its co-receptor, BMPR1A,
or to inactivate the ligand-binding function of the
protein. Since PH only develop in 10–20% of
BMPR2 mutation carriers, it has been suggested that
some gene modifiers such as environmental factors,
hormones, immunologic mechanisms or mutations in
other regulatory genes may be necessary for the
clinical expression of the disease.
So far, these mutations have neither been found in
patients with PH associated with autoimmune diseases
nor in other secondary causes of PH [9].
2. Pulmonary hypertension in autoimmune rheu-
matic diseases
PH can appear mainly in SSc, and to a lesser
extent in other autoimmune diseases, such as sys-
temic lupus erythematosus, primary antiphospholipid
syndrome, mixed connective tissue disease (MCTD),

P.E. Carreira / Autoimmunity Reviews 3 (2004) 313–320 315
rheumatoid arthritis (RA), Sjoegren’s syndrome
(SS), polymyositis (PM) and dermatomyositis
(DM). It was also a prominent feature in two
scleroderma-like diseases: the Spanish toxic oil
syndrome (TOS), caused by ingestion of adulterated
rapeseed oil [10], and the eosinophilia myalgia
syndrome, caused by contaminated L-tryptophan
capsules [11].
In SSc, PH can appear secondary to severe
pulmonary fibrosis, or as a primary complication,
in the absence of interstitial lung disease. This
arterial PH has many similarities with all the
diseases included in the first group of PH classifi-
cation (Table 1). A third type of pulmonary vascu-
lar disease that reflects the vascular pathology of
SSc, with a more indolent course, has been recently
suggested [5]. It would include those patients with
limited SSc and slowly progressive arterial PH, and
also those who have a secondary pulmonary vas-
cular component in the context of mild interstitial
lung fibrosis. The overall incidence of PH, primary
or secondary, in SSc, varies largely depending on
the type of study, the diagnostic methods and the
criteria used for PH diagnosis [4]. Clinical studies
suggest an incidence between 2 and 30% in the
diffuse, and 10 and 60% in the limited form of the
disease, specially in patients with anti-centromere
antibodies. Transthoracic Doppler echocardiography
has shown high specificity and sensitivity to detect
PH in SSc patients, compared with the gold stan-
dard, right heart catheterisation [12]. On the basis
of the high incidence, current recommendations in
SSc include annual screening by transthoracic echo-
cardiography, even in the absence of PH symptoms
[3].
The incidence of this complication in other
autoimmune disease is still less well known. In
SLE, PH can be secondary to valvular or thrombo-
embolic disease, particularly in patients with anti-
phospholipid antibodies, rarely secondary to
interstitial lung fibrosis, and occasionally as primary
vascular disease. As in SSc, prevalence of PH in
SLE varies depending on the type of study. Retro-
spective studies estimate a prevalence of 0.5–6%
[4]. Prospective studies in asymptomatic patients
find a higher prevalence, from 9 to 14% [13], but
most cases have mild pulmonary artery pressure
elevation, whose clinical significance is unknown
[4]. PH has been rarely described in RA, as a
complication of interstitial lung fibrosis, pulmonary
vasculitis, thromboembolic or cardiac disease. One
prospective echocardiographic study shows a 6%
frequency of PH secondary to lung disease, and a
21% prevalence of mild arterial PH, in unselected
RA patients [14]. The clinical significance of this
finding is not known, since the prevalence of RA in
severe arterial PH is extremely low. Prevalence of
PH in MCTD patients varies between 23 and 50%,
although this is difficult to interpret, because many
patients are later diagnosed of SSc or other autoim-
mune rheumatic disease [4]. PH has also rarely
reported in SS and PM/DM. Given the low inci-
dence of severe arterial PH in all these autoimmune
diseases, current recommendations include Doppler
echocardiography only when patients have symp-
toms suggestive of PH [3].
When severe PH is diagnosed, patients with auto-
immune rheumatic diseases should follow the same
treatment strategy than primary PH patients. Immu-
nosuppressors have been suggested, as a possible
therapy, for this group of patients [3].
3. Endothelial lesion in pulmonary hypertension
3.1. Plexiform lesion as a primary event in PH:
endothelial cell tumour-like structure
Normal pulmonary arteries are composed by
three layers: endothelial cell monolayer, media of
smooth muscle cells and collagenous adventitia. In
PH, there is a wide range of morphologic changes
in the structure of small and large pulmonary
arteries, known as pulmonary vascular remodelling
[15]. Injury to endothelium is nowadays considered
the first step of vascular remodelling. Causes of
damage might include mechanical factors (shear
stress), hypoxia and other biochemical factors as
free radicals, some drugs, infections as HIV, and
immunologic factors, such as antibody binding,
immune complexes deposition, cellular infiltration
and inflammation. In TOS, where 20% of patients
developed severe plexogenic PH, direct endothelial
injury by the toxic agent has been proposed as the
initial trigger of PH, in specifically susceptible
patients [10].

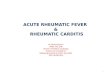
Fig. 1. Plexiform lesions in a pulmonary artery from the lung of a patient with arterial PH secondary to TOS. The vessel wall is engrossed by
smooth muscle cell proliferation in the median layer (white arrows). In some areas of the artery, the vessel lumen is almost completely occluded.
Around the vessel wall and filling also the arterial lumen can be seen numerous proliferative lesions, composed by endothelial cells (black
arrows). Lung tissue around the vessels shows a normal structure, without evidence of interstitial inflammation. (Image kindly provided by Dr
M. Teresa Sotelo, from the Pathology Department, Hospital 12 de Octubre, Madrid, Spain.)
P.E. Carreira / Autoimmunity Reviews 3 (2004) 313–320316
On the basis of classical pathological studies,
vasoconstriction has been considered the initial
cause of PH for many years [16,17]. Theoretically,
maintained vasoconstriction would lead to vascular
damage and the typical vascular remodelling seen in
PH. However, in contrast to the obligatory endothe-
lial cell monolayer seen in normal pulmonary arter-
ies, arterial PH vessels show intraluminal growth of

P.E. Carreira / Autoimmunity Reviews 3 (2004) 313–320 317
endothelial cells, forming intravascular tumourlets,
known as plexiform lesions (Fig. 1), even in early
PH patients [15,18]. The concept of excessive vaso-
constriction as the main mechanism in PH develop-
ment fails to provide explanation for this endothelial
tumour-like proliferation. As confirmed by cellular
markers [19,20], these lesions are composed of
proliferating endothelial cells, with an altered phe-
notype that share many features with cancer cells:
lost of mechanisms to stop proliferation and the
ability to differentiate, evasion of apoptosis, and
increased angiogenesis. Three-dimensional recon-
struction of plexiform lesions from PH of different
origins has also found that these lesions appear
either isolated or immediately distal to concentric-
obliterative lesions, which never appear isolated
[19]. This suggests that plexiform lesions are a
primary event, independent of a component of
vasoconstriction from medial smooth muscle cell
hypertrophy.
3.2. Angiogenic factors in PH: vascular endothelial
growth factor (VEGF) and angiopoyetin-1
Pulmonary endothelial cells are very stable, with
a very low replicative capacity ( < 0.02%), suggest-
ing that normal endothelial cells probably exert a
strong negative proliferative feedback on the adja-
cent cells to maintain a monolayer. Only two fam-
ilies of growth factors act specifically on blood
vessels: the VEGF family and the angiopoyetin
family [21]. Both are highly specific, because their
receptors are expressed almost exclusively by vas-
cular endothelium.
VEGF is an obligatory endothelial cell survival
factor, critical for vessel growth during development.
Since VEGF controls endothelial cell migration and
growth, and protects against apoptosis, it may also
be critical for the maintenance of lung endothelial
cells, and for the development of the angiogenic
plexiform lesions [15,20]. These lesions express
VEGF mRNA and protein [20], and primary or
secondary PH patients have increased VEGF serum
levels, compared to normal individuals [22]. The
protective role of VEGF for endothelial cells is
supported by several findings: first, experimental
VEGF overexpression produces glomeruloid struc-
tures resembling plexiform lesions [20]. Second,
VEGF receptor-2 blockade causes increased pulmo-
nary endothelial cell death, followed by increased
endothelial cell proliferation, probably due to a
selection of apoptosis resistant cell, and more severe
PH in hypoxic rats [23]. Finally, smooth muscle
VEGF gene transfer protects from monocrotaline-
induced PH in rats [24].
Angiopoyetin-1, a 70-kDa protein produced by
smooth muscle cells, is essential for lung devel-
opment. It recruits muscle cells and gives mature
structure to the developing arteries. After devel-
opment is completed, it is minimally expressed in
the human lung [21]. Nevertheless, in PH of
various origins, angiopoyetin-1 expression is high-
ly up-regulated in the lungs, and this expression
correlates with disease severity. In cultured human
pulmonary endothelial cells, angiopoyetin-1 upre-
gulation shuts off BMPR1A (BMPR2 co-receptor)
expression, required for BPM signalling. Also,
BMPR1A lung expression is severely reduced in
several forms of non-familial PH [25]. In an
experimental rodent model, targeted lung over-
expression of angiopoyetin-1 induces hyperplasia
of vascular smooth muscle cells and subsequently
PH [25], suggesting that angiopoyetin-1 overex-
pression may be cause and not consequence in
non-familial human PH. The findings also suggest
a shared pathway for primary and secondary PH:
An inactivation of the BMPR complex, either by
a mutation in BMPR2 in familial disease, or by
regulation of BMPR1A transcription in non-famil-
ial PH, should be a hallmark of the disease. By
contrast, a recent study has found that angiopoye-
tin-1 delivery to monocrotaline-treated rats dra-
matically protects against PH development in
these animals [26]. The model also shows in-
creased endothelial cell apoptosis, prevented as
well by angiopoyetin-1 gene transfer [26]. To
unify both studies, it has been suggested that,
perhaps, the increased angiopoyetin-1 expression
observed in the lungs of patients with PH of
different causes may reflect an insufficient com-
pensatory response [27]. Also, experimental
monocrotaline-induced PH in rats might have
different pathogenesis than human PH, since
angiopoyetin-1 expression is not increased in the
lung of these animals [26]. Interestingly, VEGF
gene transfer also prevent PH development in

P.E. Carreira / Autoimmunity Reviews 3 (2004) 313–320318
monocrotaline-treated rats [24], suggesting that, as
VEGF, angiopoyetin-1 could be another protective
factor for endothelial cells, essential for PH
development.
3.3. Vasoconstriction and vasodilation balance in
PH
There is an imbalance between vasodilator and
vasoconstrictor factors in PH. Endothelial cells in
PH have a significant reduction in expressed nitric
oxide synthase [28], and prostacyclin synthase
[29], responsible for the synthesis of nitric oxide
and prostacyclin, two potent vasodilators. This
reduction would promote smooth muscle hypertro-
phy, vasoconstriction and platelet aggregation. On
the basis of these findings, therapy with diverse
prostacyclin derivatives is currently used widely in
arterial PH [30]. Endothelial cells in plexiform
lesions also express 5-lypoxygenase (5-LO), and
its membrane partner 5-LO activation protein, that
may also contribute to vascular cell growth and
vasoconstriction, specially in pulmonary vessels
exposed to hypoxia [31]. In autoimmune diseases,
expression of nitric oxide is reduced in the
exhaled air of SSc patients with PH [32], and
in cultured dermal microvascular endothelial cells
from SSc patients [33]. Prostacyclin synthase is
also decreased in the pulmonary endothelium of
autoimmune disease PH patients [29]. Endothelin-
1, potent vasoconstrictor and smooth muscle mi-
togen, is increased in plasma and lungs of
patients with primary PH and SSc [34], and
treatment with endothelin-receptor antagonist has
proved beneficial for primary and secondary PH
[34].
A deficiency of vasoactive intestinal peptide
(VIP), potent systemic and pulmonary vasodilator,
has been very recently described both in serum and
in lung tissue of patients with primary PH [35]. VIP
vasodilator effects are mediated through the activa-
tion of cAMP and cGMP pathways, which also
mediate the action of prostacyclins, NO and phos-
phodiesterase inhibitors in PH. VIP has also shown
to inhibit in vitro the proliferation of pulmonary
artery smooth muscle cells. Treatment with aerosol-
ised VIP has shown to improve primary PH patients
[35].
3.4. Inflammation in PH development
Inflammation is a recognized feature of vascular
remodelling in PH lungs. Around remodelled pul-
monary arteries, there are perivascular infiltration of
lymphocytes, macrophages and mast cells [18].
These inflammatory cells express cytokines (inter-
leukin-1, interleukin-6) and growth factors (platelet-
derived growth factor, TGF-h, VEGF) that can also
contribute to vascular remodelling. Mast cells, pres-
ent in large amounts around pulmonary arterioles
from patients with PH, can release tryptase, which is
also a potent angiogenic factor. The expression of
macrophage inflammatory protein 1a (MIF-1a), a
chemokine that promotes the migration of monocytes
and T and B lymphocytes, is increased in PH lung
tissue [36], probably contributing to the recruitment
of inflammatory cells to the plexiform lesions.
3.5. Growth and apoptosis regulatory genes in PH
Several factors have been implicated in the ab-
normal endothelial proliferating cells in both primary
and secondary PH: downregulation of apoptosis
mediators expression, as TGFhR2 or Bax, and upre-
gulation of angiogenesis-related molecules expres-
sion, such as VEGF, angiopoyetin-1, and hypoxic
inducible factors (HIF) 1a and 1h. A complete
absence of apoptosis has been demonstrated in en-
dothelial cells of plexiform lesions [20]. Endothelial
cells from primary PH plexiform lesions also present
microsatellite instability in the pro-apoptotic Bax
gene [37]. This mutation confers growth advantage
to cells that escape from apoptotic cell death cas-
cades involved by Bax. It has been found an in-
creased expression of the anti-apoptotic Bcl-2 [38] in
plexiform lesions.
It has been proposed that the difference between
the primary and the secondary PH is that in
primary PH the disease is caused by somatic
mutations in key growth regulation genes, such as
TGFhR2 or Bax [38]. This loss of growth control
mechanism would allow for the clonal expansion of
a single endothelial cell after acquiring selective
growing advantages. On the other hand, different
factors, as immunologic mechanisms in autoimmune
diseases, or mechanical and biochemical factors in
other secondary forms of PH, would activate endo-

P.E. Carreira / Autoimmunity Reviews 3 (2004) 313–320 319
thelial cells to proliferate in a polyclonal way
[39,40].
Take-home messages
. Arterial PH, indistinguishable from primary PH,
can appear in some autoimmune rheumatic disease,
particularly in 5–15% of SSc patients.. Arterial PH, primary or secondary to autoimmune
rheumatic disease, is characterised by the presence
of plexiform lesions, composed by actively prolif-
erating endothelial cells, showing many features of
cancer cells.. There is an increase of vasoconstrictor factors and a
decrease of vasodilator factors in pulmonary vessels
of all cases of arterial PH.. There is an increase of proliferative endothelial cell
factors, and a decrease of anti-proliferative factors
in plexiform lesions of arterial PH.. Inflammatory cells are present around the plexiform
lesions, suggesting a role for inflammation in the
pathogenesis of this condition.. Endothelial cells in plexiform lesions of arterial
PH show alterations in key growth regulation
genes.
References
[1] Rubin L. ACCP consensus statement: primary pulmonary hy-
pertension. Chest 1993;104:236–50.
[2] Stuart, R, editor. Executive Summary from the World Sympo-
sium on Primary Pulmonary Hypertension 1998, Evian,
France, September 6–10, 1998. Co-sponsored by the World
Heart Organization.
[3] British Cardiac Society Guidelines and Medical Practice Com-
mittee, and approved by the British Thoracic Society and the
British Society of Rheumatology. Recommendations on the
management of pulmonary hypertension in clinical practice.
Heart 2001;86(Suppl I):i1– i13.
[4] Magliano M, Isenberg DA, Hillson J. Pulmonary hipertension
in autoimmune rheumatic diseases. Where are we now? Ar-
thritis Rheum 2002;46:1997–2009.
[5] Denton CP, Black CM. Pulmonary hypertension in systemic
sclerosis. Rheum Dis Clin N Am 2003;29:335–49.
[6] Deng Z, Morse JH, Slager SL, et al. Familial primary pulmo-
nary hypertension (gene PPH1) is caused by mutations in the
bone morphogenetic protein receptor-II gene. Am J Hum Gen-
et 2000;67:737–44.
[7] Lane KB, Machado RD, Pauciulo MW, et al. Heterozygous
germline mutations in BMPR2, encoding a TGF-beta receptor,
cause familial pulmonary hypertension. The International PPH
Consortium. Nat Genet 2000;26:81–4.
[8] Newman JH, Wheeler L, Lane KB, et al. Mutation in the gene
for bone morphogenetic protein receptor II as a cause of pri-
mary pulmonary hypertension in a large kindred. N Engl J
Med 2001;345:319–24.
[9] Morse J, Barst R, Horn E, Cuervo N, Deng Z, Knowles J.
Pulmonary hypertension in scleroderma spectrum of disease:
lack of bone morphogenetic protein receptor 2 mutations.
J Rheumatol 2002;29:2379–81.
[10] Gomez-Sanchez MA, Saenz de la Calzada C, Gomez-Pajuelo
FJ, Martınez-Tello FJ, Mestre de Juan MJ, James TN. Clin-
ical and pathologic manifestations of pulmonary vascular
disease in the toxic oil sındrome. J Am Coll Cardiol
1991;18:1539–45.
[11] Hertzman PA, Clauw DJ, Kauffman LD, et al. The eosin-
ophilia-myalgia syndrome: status of 205 patients and
results of treatment 2 years after onset. Ann Intern Med
1995;122:851–5.
[12] Denton CP, Cailes JB, Phillips GD, Wells AU, Black CM, Du
Bois RM. Comparison of Doppler echocardiography and right
heart catheterisation to assess pulmonary hypertension in sys-
temic sclerosis. Br J Rheum 1997;36:239–43.
[13] Winslow MW, Ossipov MA, Fazio GP, Simonson JS, Red-
berg RF, Schiller NB. Five year follow up study of the
prevalence and progression of pulmonary hypertension in
systemic lupus erythematosus. Am Heart J 1995;129:510–4.
[14] Dawson JK, Goodson NG, Graham DR, Lynch MP. Raised
pulmonary artery pressures measured with Doppler echocar-
diography in rheumatoid arthritis patients. Rheumatology
(Oxford) 2000;39:1320–5.
[15] Tuder RM, Lee SD, Cool CC. Histopathology of pulmonary
hypertension. Chest 1998;114:1S–6S.
[16] Bjornsson J, Edwards WD. Primary pulmonary hypertension:
a histopathologic study of 80 cases. Mayo Clin Proc
1985;60:16–25.
[17] Pietra GG, Edwards WD, Kay JM, et al. Histopathology of
primary pulmonary hypertension. A qualitative and quantita-
tive study of pulmonary blood vessels from 58 patients in the
National Heart, Lung and Blood Institute, Primary pulmonary
hypertension registry. Circulation 1989;80:1198–206.
[18] Tuder RM, Groves BM, Badesch DB, Voelkel NF. Exuberant
endothelial cell growth and elements of inflammation are pres-
ent in plexiform lesions of pulmonary hypertension. Am J
Pathol 1994;144:275–85.
[19] Cool CD, Stewart JS, Werahera P, et al. Three-dimensional
reconstruction of pulmonary arteries in plexiform pulmonary
hypertension using cell-specific markers. Evidence for a dy-
namic and heterogeneous process of pulmonary endothelial
cell growth. Am J Pathol 1999;155:411–9.
[20] Tuder RM, Chacon M, Alger L, et al. Expression of angio-
genesis-related molecules in plexiform lesions in severe pul-
monary hypertension: evidence for a process of disordered
angiogenesis. J Pathol 2001;195:367–74.
[21] Yancopoulos GD, Davis S, Gale NW, Rudge JS, Wiegand SW,

P.E. Carreira / Autoimmunity Reviews 3 (2004) 313–320320
Voelkel NF. Vascular-specific growth factors and blood vessel
formation. Nature 2000;407:242–8.
[22] Voelkel NF, Hoeper M, Maloney J, Tuder RM. Vascular en-
dothelial growth factor in pulmonary hypertension. Ann NY
Acad Sci 1996;796:186–93.
[23] Taraseviciene-Stewart L, Kasahara Y, Alger L, et al. Inhibition
of the VEGF receptor 2 combined with chronic hypoxia
causes cell death-dependent pulmonary endothelial cell prolif-
eration and severe pulmonary hypertension. FASEB J
2001;15:427–38.
[24] Campbell AIM, Zhao Y, Sandhu R, Stewart DJ. Cell-based
gene transfer of vascular endothelial growth factor attenuates
monocrotaline-induced pulmonary hypertension. Circulation
2001;104:2242–8.
[25] Du L, Sullivan CC, Chu D, et al. Signaling molecules in
nonfamilial pulmonary hypertension. N Engl J Med 2003;
348:500–9.
[26] Zhao YD, Campbell AIM, Robb M, Ng D, Stewart DJ. Pro-
tective role of angiopoyetin-1 in experimental pulmonary hy-
pertension. Circ Res 2003;92:984–91.
[27] Rudge JS, Thurston G, Yancopoulos GD. Angiopoyetin-1 and
pulmonary hypertension. Cause or cure? Circ Res
2003;92:947–9.
[28] Giaid A, Saleh D. Reduced expression of endothelial nitric
oxide synthase in the lungs of patients with pulmonary hyper-
tension. N Engl J Med 1995;333:214–21.
[29] Tuder RM, Cool CD, Geraci MW, et al. Prostacyclin synthase
expression is decreased in lungs from patients with severe
pulmonary hypertension. Am J Respir Crit Care Med
1999;159:1925–32.
[30] Paramothayan NS, Lasserson TJ, Wells AU, Walters EH.
Prostacyclin for pulmonary hypertension. Cochrane Database
Syst Rev 2003;2:CD002994.
[31] Wright L, Tuder RM, Wang J, Cool CD, Lepley RA, Voelkel
Tumor necrosis factor alpha blocking and rheumatoi
The effect of infliximab (a tumor necrosis factor-alpha
nodules was studied by Baeten et al. (Ann Rheu
immunopathological difference between the nodules be
had the classical structure with a central necrotic zone sur
tissue zone. Therefore, despite the improvement in articu
this therapy had no effect on the histopathology of rheum
mediate these 2 disease manifestations in rheumatoid ar
NF. 5-Lipoxygenase and 5-lipoxygenase activating protein
(FLAP) immunoreactivity in lungs from patients with primary
pulmonary hypertension. Am J Respir Crit Care Med
1998;157:219–29.
[32] Kharitonov SA, Cailes JB, Black CM, du Bois RM. Decreased
nitric oxide in the exhaled air of patients with systemic scle-
rosis with pulmonary hypertension. Thorax 1997;52:1051–5.
[33] Romero LI, Zhang DN, Cooke JP, et al. Differential expres-
sion of nitric oxide by dermal microvascular endothelial cells
from patients with scleroderma. Vasc Med 2000;5:147–58.
[34] Rubin LJ, Badesch DB, Barst RJ, et al. Bosentan therapy for
pulmonary arterial hypertension. N Engl J Med 2002;346:
896–903.
[35] Petkov V, Mosgoeller W, Ziesche R, et al. Vasoactive intesti-
nal peptide as a new drug for treatment of primary pulmonary
hypertension. J Clin Invest 2003;111:1339–46.
[36] Fartoukh M, Emilie D, Le Gall C, Monti G, Simonneau G,
Humbert M. Chemokine macrophage inflammatory protein-
1A mRNA expression in lung biopsy specimens of primary
pulmonary hypertension. Chest 1998;114:50S–1S.
[37] Yeager ME, Halley GR, Golpon HA, Voelkel NF, Tuder RM.
Microsatellite instability of endothelial cell growth and apo-
ptosis genes within plexiform lesions in primary pulmonary
hypertension. Circ Res 2001;88:e2–e11.
[38] Tuder RM, Voelkel NF. Angiogenesis and pulmonary hyper-
tension: a unique process in a unique disease. Antioxid Redox
Signal 2002;4:833–43.
[39] Lee SD, Shroyer KR, Markham NE, Cool CD, Voelkel NF,
Tuder RM. Monoclonal endothelial cell proliferation is pres-
ent in primary but not secondary pulmonary hypertension. J
Clin Invest 1998;101:927–34.
[40] Tuder RM, Cool CD, Yeager M, Taraseviciene-Stewart L, Bull
TM, Voelkel NF. The pathobiology of pulmonary hyperten-
sion. Endothelium Clin Chest Med 2001;22:405–18.
The World of Autoimmunity; Literature Synopsis
d nodules
blocker) on the immunopathology of rheumatoid
m Dis 2004;63:489). They found no manifest
fore and after infliximab treatment, as all nodules
rounding the palisade layer, and an outer connective
lar symptoms associated with infliximab treatment,
atoid nodules, suggesting that different mechanisms
thritis.


















![Autoimmune and rheumatic musculoskeletal diseases as a … · 1544 Rheumatology International (2020) 40:1539–1554 1 3 deservespecialmention.Myopathyandneuromyopathy canrarelyoccurfollowinglong-termtreatmentwithchlo-roquineandhydroxychloroquine[33].Favipiravircanlead](https://img.pdfslide.net/doc/110x75/602aaf537a8f1676737f1520/autoimmune-and-rheumatic-musculoskeletal-diseases-as-a-1544-rheumatology-international.jpg)