Embed Size (px)
Citation preview

PHDTHESIS DANISHMEDICALJOURNAL
DANISH MEDICAL JOURNAL 1
ThisreviewhasbeenacceptedasathesistogetherwithfourpreviouslypublishedpapersbyUniversityofCopenhagen7thofAugust2015anddefendedon28thofAugustTutor(s):LarsNannestadJorgensen,HenrikHarling&PeerAndersWille-JørgensenOfficialopponents:IsmailGögenur,NielsQvist&PerJ.NilssonCorrespondence:DigestiveDiseaseCenter,BispebjergHospital,BispebjergBakke23,2400CopenhagenNV,Denmark E-mail:[email protected];63(1):B5190
THEFOURORIGINALPAPERSARE1. Nordholm-CarstensenA,Wille-JorgensenPA,JorgensenLN,
HarlingH.Indeterminatepulmonarynodulesatcolorectalcancerstaging:asystematicreviewofpredictiveparametersformalignancy.AnnalsofSurgicalOncology.2013;20(12):4022-4030[1].
2. Nordholm-CarstensenA,KrarupPM,JorgensenLN,Wille-JorgensenPA,HarlingH;onbehalfoftheDanishColorectalCancerGroup.Occurrenceandsurvivalofsynchronouspul-monarymetastasesincolorectalcancer:anationwidecohortstudy.EuropeanJournalofCancer.2014;50(2):447-456[2].
3. Nordholm-CarstensenA,JorgensenLN,Wille-JorgensenPA,HansenH,HarlingH.Indeterminatepulmonarynodulesincolorectal-cancer:doradiologistsagree?AnnalsofSurgicalOncology.2015;22(2):543-549[3].
4. Mismatchrepairandsynchronousmetastasesincolorectalcancer:anationwidecohortstudy.Nordholm-CarstensenA,KrarupPM,MortonD,andHarlingH,onbehalfoftheDanishColorectalCancerGroup.InternationalJournalofCancer.2015.doi:10.1002/ijc.29585.[4]
BACKGROUND
StagingCancerstagingistheshortdescriptionofacanceratapointinitsnaturalhistorythathassignificanceinguidingtreatment,inprog-nosis,andincomparisonofendresults[5].
This40-yearolddefinitionisstillvalidtodayandstagingre-mainsfundamentalintheassessmentofprognosis,intheplan-ningoftreatment,inthecommunicationbetweentreatinghealth
personnelandincomparisonofstudiesonpatientswithcancer.Cancerstaginghasbeencalled“thelanguageofcancer”[6].In1928thefirstknownattempttograderectalcancerwasmadebasedontheproportionofdifferentiatedcellsinthetumour[7].Morewell-knownis,however,theworkbyC.E.Dukes,whoin1932proposedDukes’classificationforrectalcancer[8].Thisclassificationwastheresultofobserveddifferencesinlengthofsurvivaldependingontheextentoftherectalcancerinvadingthroughthebowelwallandthepresenceoflymphaticmetasta-ses.AdecadelaterPierreDenoixbeganthedevelopmentofthetumour-nodemetastasis(TNM)systemthatcouldbeappliedtoallcancersites[6,9]resultinginthe1steditionoftheTNMclassifica-tionhandbook,“LivredePoche”,in1968[10].Todaythe7theditionoftheTNM(Table1and2)isinuseandstagingisbasedonthefurtherdevelopmentontheinitialTNMsystemwithin-formationonthetumour,regionalnodesandmetastases.Thedescriptionoftheanatomicextendofthediseaseisstillcentralindefiningcancerprognosis.Thisdescriptionprovidesthesolidfoundationforevaluationofthenumerousnewnon-anatomicalindependentprognosticfactorsofrecurrenceandoverallsurvivalunderstudyandisinadditiontohistologicalsubtypeandtopo-graphicsiteoneofthethreemainaxesoftumourclassification[6,11].Finally,aspointedoutbyComptonandGreene[12],afurtheradvantageoftheTNMsystemisitscontinuousimprove-mentbasedonon-goingexpertreviewsofexistingdata;ithasexhaustivedefinitionsensuringastringentuse;andisrelevanttoallmodernstagingevaluationtechniques[12,13].
Table1Classificationofcolorectalcancersaccordingtoextentoftheprimarytumour(Tstage),lymphnodeinvolvement(Nstage)anddistantmetastases(Mstage)T–Primarytumour Definition
Tis Tumourrestrictedtomucosa,noinfiltrationoflaminamuscularismucosae
T1 Infiltrationthroughlaminamus-cularismucosaeintosubmucosa,noinfiltrationoflaminamuscularispropria
T2 Infiltrationinto,butnotbeyond,laminamuscularispropria
T3 Infiltrationintosubserosaornon-peritonealisedpericolicorperirectaltissue,orboth.Noinfiltrationofserosaorneighbouringorgans
T4a InfiltrationoftheserosaT4b Infiltrationofneighbouring
organs
PulmonaryNodulesandMetastasesinColorectalCancer
AndreasNordholm-Carstensen

DANISH MEDICAL JOURNAL 2
N–Regionallymphnodes N0 NolymphnodeinvolvementN1a Cancercellsdetectablein1
regionallymphnodeN1b Cancercellsdetectablein2-3
regionallymphnodesN1c Tumoursatellitesinsubserosaor
pericolicorperirectalfattissue,regionallymphnodesnotinvolved
N2a Cancercellsdetectablein4-6regionallymphnodes
N2b Cancercellsdetectablein7ormoreregionallymphnodes
M–Distantmetastasis M0 NodistantmetastasesdetectableM1a Metastasisconfinedto1distant
organordistantlymphnodesM1b Metastasistomorethan1dis-
tantorganorperitonealmetasta-sis
Tablebasedon7thed.oftheUnionforInternationalCancerControlTumourNodeMetastasisclassification[18].
Table2UICCTNMStageGroupingofColorectalCancers7thed.
Stage T N M
5-yearsurvival(%)
I T1/T2 N0 M0 92.5II T3/T4 N0 M0 IIA T3 N0 M0 83.6IIB T4a N0 M0 76.3IIC T4b N0 M0 58.8III AnyT N+ M0 IIIA T1/T2
T1N1N2a
M0M0 83.1
IIIB T3/T4aT2/T3T1/T2
N1N2aN2b
M0M0M0
63.8
IIIC T4aT3/T4aT4b
N2aN2b
N1/N2
M0M0M0
35.2
IV AnyT AnyN M+ 10.4IVA AnyT AnyN M1a IVB AnyT AnyN M1b UICC,UnionforInternationalCancerControl;TNM,TumourNodeMetastasisSurvivaldatafromtheSurveillance,EpidemiologyandEndResults(SEER)programdatabaseaspublishedbyGaoetal.2013[17].“M”Bearingthefundamentalideaofstaginginmind,theintroductionofthe“M”totheclassificationofcancersisessential.Ahallmarkofcancer,towhichtheonesofcolorectaloriginarenoexception,isthecapabilityofinvasionandmetastasis[14].About20%ofpatientsnewlydiagnosedwithcolorectalcancer(CRC)willhavesynchronouscolorectalcancermetastases(SCCM),i.e.metastaticdiseaseatthetimeofdiagnosis[15,16].
Despiteaconsiderableimprovementofadjuvanttreatmentoverthepastfivedecades,themanagementofmetastaticspreadcontinuestobeasignificantchallenge,andthechangefromlocalizedtodistant,systemicdiseasehasgreatimplicationsfortheprognosis.The5-yearrelativesurvivalinpatientswithSCCMis10-13%,whichisconsiderablylowerthanforpatientswith
localizeddisease(Table2)[16,17].Thetreatmentofpatientswithdisseminateddiseaseisamultidisciplinarytaskandmostcasesarenotcandidatesforpotentialcurativeresection.However,itisofgreatimportancetoidentifythosepatientswhoaresuitableformetastasectomyandthoseinwhomthemetastasescouldbecomeresectableafterresponsetocombinationchemotherapy[19].PulmonarymetastasesThemajorityofsynchronousmetastasesarehepatic,[15]where-asthelungsremainthemostcommonextraabdominalmetastaticlocation[20].TheprevalenceofsynchronouspulmonaryCRCmetastases(SPCM)rangesfrom2%to18%[20-25]andinprevi-ousstudiestheyaremostoftenaccompaniedbyhepaticmetasta-ses[20,22].
Noteworthy,theriskofpulmonaryinvolvementdiffersac-cordingtothelocationoftheindextumourandhasbeenreport-edto10-18%forrectalcancersand2-6%forcoloniccancers[20-25].Theriskofpulmonary(andhepatic)metastasesincolonicandrectalcancershasbeenattributedtothedirectvascularandlymphaticcommunicationwiththeintestinaltract.Furthermore,thedensecapillarysysteminthelungsandliveractingasafilterforcirculatingtumourcellsincombinationwithanespeciallysuitablemicroenvironmentforimplantationandgrowthhavebeensuggestedasunderlyingmechanismsforthehepaticandpulmonarypredilection[26,27].
DespitebeingthesecondmostcommonmetastaticsiteinCRC,theepidemiologyandoptimaltreatmentofpulmonarymetastaseshavenotbeenasintensivelystudiedasforhepaticmetastases.Pulmonarymetastasectomyhasbeenacceptedasapotentiallycurativeoptioninthemultimodalmanagementofpulmonarymetastasesdespitethelackofresultsfromprospec-tiverandomizedclinicaltrials[28,29].Essentialforcurativeresec-tionistheearlydetectionofthesemetastasesandselectionofpatientswithlimitednumberofmetastases,as“completeresec-tionbasedintheanatomiclocationandextentofdiseasewithmaintenanceofadequatefunctionisrequired”[28,30,31].Uncertaintyconcerningthe“M”–indeterminatelesionsGiventheriskofmetastaticspreadtothelungsandthesubse-quentprognosticimpact,apreoperativestagingofthechestwithcomputedtomography(CT)isrecommendedinguidelinesonthemanagementofpatientswithCRC[30-33].Thoughtheoptimalstagingprocedureofthelungscanbediscussed,thehighsensitiv-ityforpulmonarymetastasesyieldedbyachestCTisundisputed[34].AconcernregardingthechestCT,however,isasomewhatlowerspecificityandindeterminatepulmonarynodules(IPNs)areafrequentfinding;insomestudiesdetectedinmorethan1/3ofpatientsintheCRCsetting[34,35].Alungnoduleisalesionbe-tween1and30mmsurroundedbynormallungparenchymaandnotassociatedwithadenopathyoratelectasis[36]Suchlesionsmayrepresentmetastaticdisease,[23,25,37-40]buttheneedforimmediatetreatmentoftheindextumourdoesnotallowforaprospectivesurveillanceforpotentialgrowthoftheselesionsonrepeatedCTscans.Theidealtestdistinguishinglesionsofbenignoriginfromthemalignantoneshasyettobediscovered;positronemissiontomography(PET)isoflimitedvalueinthesmallestofthelesions[34,41]andinvasiveproceduresarenotviableoptionsduetothevastnumberofpatientswithIPNandtechnicaldifficul-ties[35,42].Untilnowmanagementhasbeenbasedonguidelinesonmanagementoflesionsdetectedinlungcancerscreening[43].
TheclinicalsignificanceandoptimaldiagnosticapproachintheCRCsettingremainstoberesolved.Furtherdiagnostic

DANISH MEDICAL JOURNAL 3
workupmaydelaythetimetoresectionoftheindexcancer,andisassociatedwithincreasedradiationexposure,morbidity,costs,uncertaintyamongdoctorsandpatientanxiety.
HYPOTHESES
ThisthesiswassettoevaluatetheoverallhypothesisthattheinitialstagingchestCTinCRCpatientsdetectspulmonarylesionsinasubstantialnumberofthepatients.Lesionsclassifiedasdefi-nitepulmonarymetastaseshaveahighimpactonsurvivalprog-nosis,whereas“indeterminate”findingsmostoftenarebenignandcanbeignoredintheinitialdecision-makingontherapyfortheindextumourandothermetastaticsites.• Increasingnumbersofpulmonarynodulesaredetectedwith
theimplementationofcomputedtomographyinstagingofpatientswithcolorectalcancer.Manyofthesenodulescan-notreadilybeclassifiedasbeingbenignormalignant
• Pulmonarymetastasectomyand/oradjuvant/palliativechemotherapyimprovesurvivalinpatientswithpulmonarymetastases
• Clinicopathologicalfactorsandradiologicalcharacteristicsareusefulforevaluationofindeterminatepulmonarylesions
• Thecharacterizationofpulmonarylesionsdependsontheevaluatingradiologist
• Analysisofbiomarkershasimplicationsinthediagnosticstrategybyidentificationofpatientsinparticularriskofpul-monarymetastases
AIMSTheoverallobjectiveofthisthesiswastoinvestigatethepreva-lence,characteristicsandclinicalsignificanceofpulmonaryle-sionsdetectedattheinitialstagingofnewlydiagnosedCRCpa-tients.Lesionsofinterestcompriseddefinite,synchronouspulmonarymetastasesandindeterminatepulmonarynodules.Specifically,thethesisaddressed• existingevidenceontheprevalenceofIPNandspecificradio-
logicaland/orclinicopathologicalfactorsassociatedwithma-lignancyofIPN
• occurrenceofandriskfactorsforsynchronouspulmonarymetastases,howtheyaremanagedonanationalbasisandtheirimpactonsurvival
• variabilityinradiologists’assessmentofthestagingchestCT• potentialapplicabilityofmismatchrepair(MMR)status
analysisoftheindexcolorectaladenocarcinomainanevalu-ationoftheriskofsynchronouspulmonarymetastases
PRESENTATIONOFSTUDIES
STUDYIIndeterminatepulmonarynodulesatcolorectalcancerstaging:asystematicreviewofpredictiveparametersformalignancy
AimTheobjectivesofthisstudyweretoevaluatetheexistingevi-denceregarding
1. theprevalenceofindeterminatepulmonarynodulesattheprimarystagingCTscaninpatientswithcolorectalcancer
2. potentialclinicopathologicalfactorsandradiologicalcharac-teristicsassociatedwithamalignantnatureoftheIPN
3. clinicalimplicationsofIPN4. theoptimalfollow-upregimenofIPNMethodsThiswasasystematicreviewoforiginalstudiespublishedinEM-BASE,theCochraneLibraryandScienceCitationIndex,PubMeddatabases,GoogleScholar,relevantconferenceproceedings(UnitedEuropeanGastroenterologyWeek,AmericanSocietyofClinicalOncology,DigestiveDiseaseWeek,EuropeanSocietyofColoproctology,TheEuropeanCancerConference),trialregistries(clinicaltrials.gov,EUClinicalTrialsRegister,theWorldHealthOrganizationinternationalclinicaltrialsregistryplatform)andreferencelistsofrelevantretrievedarticles.Thereviewwascon-ductedinaccordancewiththePreferredReportingItemsforSystematicReviewsandMeta-analyses(PRISMA)guidelines[44].TheliteraturesearchwasperformedincooperationwiththetrialssearchcoordinatorfromtheCochraneColorectalCancerGrouptoensureathorough,objectiveandreproduciblesearchoftheavailablesources.InaccordancewiththeguidelinesoftheCochraneHandbook,[45]thesearchstrategywassettohavethreesetsoftermsdefining:1. Participants:Patientswithcolonicorrectalcancersubjected
tostaging2. Intervention:Primarystagingcomputedtomographyinclud-
ingthethoraciccavityandafollow-upintervention(notfur-therspecified)oftheprimarystagingfindings
3. Comparisonsandoutcomes:Definition,prevalence,charac-teristicsandoutcomeofindeterminatepulmonarynodulesdetectedatstaging
Incaseofmultiplepublicationsonthesamepatientpopulation,themostrecentorcompletestudywasselected.Recordswerethenscreenedbytitleandhereafterbyabstract.Finally,relevantarticleswereretrievedinfull-textforfurtherassessmentofeligi-bility.Studieshadtoreporttheoutcomeofpatientsdiagnosedwithindeterminatepulmonarynodulestobeincluded.
AllstudiesincludedforanalysisinthereviewwereassessedaccordingtotherecommendationsoftheOxfordCentreforEvidence-basedMedicine46andthemethodologychecklistsdevelopedbytheScottishIntercollegiateGuidelinesNetwork[47].Forsomeoftheincludedstudiesallassessmentpointsofthemethodologychecklistcouldnotbedirectlyapplied.
Weightedmeanofratios(WMR)takingthenumberofstudyparticipantsintoaccountwereusedfordataanalysis.Thenatureofthepublishedstudiesdidnotallowforastrictdiagnostictestaccuracymeta-analysis.
ResultsIntotal,3,485titleswerescreenedofwhich12studiesencom-passing6,222patientswereincluded.Thestudydesign,aimofstudy,levelofevidence,definitionofIPNandtypeofCTscannervariedamongthestudies.AssessmentofpulmonarystagingCTfindingswasreportedfor5,873(94.4%)patientsofwhom732(WMR=9.0%)hadoneormoreIPNs.
TheriskofIPNbeingmalignantincreasedwithseverityofUICCstage.Ameta-analyticalassessmentofclinicopathologicalfactorsassociationwithmalignancyofIPNwasdeemedimpossi-bleduetothelargeheterogeneityofthestudies.

DANISH MEDICAL JOURNAL 4
Intotal,10.8%ofIPNsprovedtorepresentCRCmetastases,whereas0.5%wereprimarylungcancers.Thevastmajoritywasconsideredtobebenignlesionsorremainedunclarified.
ConsistentfindingsofriskfactorsforIPNmalignancybetweenthestudieswerefewandlimitedtolymphnodemetastasis(n=5)[38,39,42,48,49],increasingnumberofIPN(n=3)[48-50]andirregularsize(n=2)[50,51],whereascalcificationindicatedbe-nignIPN(n=2)[50,51].
Finally,characteristicssuchassizeoftheIPN[51],intra-pulmonarylocation[50],locationoftheindextumour[50]andpresenceofextra-pulmonarymetastaticdisease[48]wereonlyreportedtobesignificantlyassociatedwithmalignancyoftheIPNinsinglestudies.
ConclusionInconclusion,9%ofpatientswithCRCsubjectedtoprimarystag-ingchestCThadIPN,butonlyonein100ofallchestCTstagedpatientshaveIPNultimatelyprovingmalignant.Mostpulmonarynoduleswereofbenignoriginorremainedunresolved.Noradio-logicalfeaturesforIPNcouldbeconcludedpathognomonicformalignancy.Mostcommonlyapositivenodalstatuswasassociat-edwithIPNrepresentingpulmonarymetastases.Basedonthesefindings,noadditionalwork-uptoIPNwasrecommendedinadditiontoroutinefollow-upregimens.
LimitationsDespitebeingasystematicandextensivereviewoftheavailableliterature,thisstudyhassomelimitations.Despitearestrictivesearchstrategy,thegreatheterogeneityoftheincludedstudiesisacentralchallenge.Thisheterogeneitywasduetodifferentdefi-nitionsofIPN(ifany),varyingdiagnosticmethods(typeofCTscanner,expertiseandnumberofevaluatingradiologists)andnostandardizedfollow-upregimenortimetofollow-up.Further-more,radiologicalandclinicopathologicalfactorsassociatedwithmalignancyofIPNwereinconsistentlyreported.Datafromthe12includedstudieswereunfortunatelysodisparateandinhomoge-neousthatthesolidityoftheconclusionisweakened.
Finally,amethodologicalcriticismcanbeexpressedregardingtheprocedureofdataextractionforthisstudy.Theextractionofstudyresultswasperformedsolelybythefirstauthor.Twootherauthorsverifiedtheaccuracyoftheextracteddata,buttheywerenotblindedtothefindingsofthefirstauthor.Optimally,allau-thorshadextractedthedataindependentlyallowingforacalcula-tionofthelevelofagreementinthedataextraction.
STUDYIIOccurrenceandsurvivalofsynchronouspulmonarymetastasesincolorectalcancer:anationwidecohortstudy
AimThisstudyaimedtoinvestigate1. theoccurrenceofsynchronouscolorectalcancermetastases
confinedtothelungsinanationwidecohortofDanishpa-tientswithCRC
2. toidentifyriskfactorsforthesepulmonarymetastases3. toanalysetheirprognosticimpactintermsofsurvivalin
relationtodifferenttherapeuticprocedures
MethodsAllpatientswithafirsttimediagnosisofcolonicorrectalcancerregisteredintheDanishColorectalCancerGroup(DCCG)data-
basebetween2001and2011wereassessedforinclusion.DatafromtheDCCGdatabaseweremergedwithdatafromtwootherpopulation-basedregistries,theNationalPatientRegistry(NPR)andtheDanishPathologyRegistry(DPR).Inadditiontodemo-graphicandclinicopathologicaldataonthepatients,dataonradiologicalexaminationsofthechestperformedfrom30daysbeforeCRCdiagnosisuntilendoffollow-upwereextractedfromtheNPR.
RiskfactorsforpulmonarymetastaseswereanalysedwithChi-squareandMann-Whitney-Wilcoxontests.Multivariablelogisticregressionwasusedtoadjustforpotentialconfounding.OverallsurvivalwasassessedbyKaplan-Meierplotsandstratifiedlog-rankanalysis.Furthermore,theimpactoftreatmentmeasuresandclinicopathologicalvariablesonsurvivalwasassessedinanextendedCoxregressionanalysistoallowfortime-varyingeffectsofthevariables[52].Atwo-tailedp-valueof0.01wasusedaslevelofsignificanceduetothelargestudycohort.
ResultsIntotal,40,425patientswereassessedforeligibilityofwhom26,200wereincluded.SCCMwerepresentin7,742(29.5%).AmongtheseSPCMwereregisteredin1970(25.4%).Mostcom-monlythediagnosisofSPCMwasbasedonradiologicalfind-ings,whereashistologicalconfirmationwasobtainedin182(9.2%).SCCMconfinedtothelungs(Pulmonary-onlysynchronousmetastases,POSM)accountedfor37%(736patients)oftheUICCstageIVpatients.TheprevalenceofPOSMincreasedduringthestudyperiod,asdidtheuseofstagingchestCTscans.Thedetec-tionrateofSPCMwas7.0%(1,160of16,508patients)inpatientsstagedwithatraditionalchestX-ray,and8.4%(810/9,692)inthosehavingachestCTstagingperformed.
RiskfactorsforPOSMwereadvancedage,rectalcancerandarecentyearofdiagnosisafteradjustmentforpotentialconfound-ersincludingamorewidespreaduseofCTscansinrectalcancerpatientsandrecentyears.
PatientswithPOSMhadanoverallsurvival(OS)ofmedian376days(IQR:95-956),andsurvivalwashighlycorrelatedtothetherapeuticproceduresperformed.InpatientsresectedfortheirPOSMmedianOSreached1470days(95%CI:600-1905days),however,apulmonarymetastasectomywasonlyperformedin28patients(3.8%).Intotal,485(66%)underwentresectionoftheindextumour,andchemotherapy(palliativeandadjuvant)wasadministeredin367patients(50%).Pulmonarymetastasectomy,resectionoftheindextumourandadjuvantchemotherapyincombinationhadonlybeenperformedin15patients(2.0%).Patientshavingtheirindextumourresected(adjustedHazardRatio(aHR)=0.50,95%CI:0.42-0.60,P<0.001)andreceivingpalliativechemotherapyhadafavourablesurvivalprognosis.AccordingtotheextendedCox-regressionmodel,theimpactofchemotherapywasmostnotablyfrom30-365daysaftertheinitialCRCdiagnosis(effectday30-365,aHR=0.58,95%CI:0.48-0.70,P<0.001),whereasthestatisticalsignificancedisappearedbeyondthefirstyearafterthediagnosis(effectyear1-2,aHR=1.20,95%CI:0.90-1.60,P=0.225).
ConclusionSPCMweredetectedin7.5%ofallnewlydiagnosedCRCpatients,whichisahigherprevalencethanpreviouslyreported,andin37%ofthecasesthemetastasesweresolelyconfinedtothelungs.Thepresenceofpulmonarymetastasessignificantlyimpairedsurvival,butbothresectionofthemetastasesandindextumourinaddi-tiontochemotherapywereassociatedwithaprolongedoverallsurvival.

DANISH MEDICAL JOURNAL 5
LimitationsTheuniquenessofthisstudylieswithintheepidemiologicalas-sessmentofsynchronouspulmonarymetastasesonanationalbasis.However,atthesametimethestudydesignisthemainlimitation-allowingonlyassociationsratherthancausalrelation-shipstobeexplored.Inparticular,thisimpairsthestrengthofconclusionsonthepotentialeffectofdifferenttherapeuticmeasures.Additionally,theseconclusionsarealsoweakenedbythelimitedavailabledataonthebasisforsurgicalintervention,adjuvant/palliativetreatmentandnumberofpulmonarymetasta-ses.Somedegreeofselectionbiasorconfoundingbyindicationmustbeexpectedregardingtheobservedeffectsofdifferenttreatmentmodalities.
Furthermore,fewpulmonarymetastaseswerehistologicallyconfirmed.Thiscouldberegardedasascientificshortcoming,bearinginmindthepotentialdifficultiesinassessingpulmonarynodules;thecentralissueofthisthesis.Someover-diagnosingmayoccur,asasubstantialnumberofpatientswithpulmonarymetastases,whowereonlysubjectedtoresectionoftheindexcancer,werestillalive5yearsafterdiagnosis.Inthesecases,benignandinsignificantpulmonarynodulescouldhavebeenwronglyregisteredinthedatabaseasmetastases.
STUDYIIIIndeterminatepulmonarynodulesincolorectal-cancer:Doradi-ologistsagree?AimThepurposeofthisstudywastoanalyse1. thevariabilityintheradiologists’detectionandcharacteriza-
tionofindeterminatepulmonarynodulesattheprimarypulmonarystagingCTscaninpatientswithnewlydiagnosedCRC
2. thepotentialassociationsbetweencertainradiologicalchar-acteristicsasassessedbyanexperiencedthoracicradiologistandamalignantnatureofIPN
MethodsInthesamecohortofpatientsasusedforstudyII,weidentifiedallpatientsreferredtoourcentrebetween2006and2011.Bytheinitialcut-offdateofthepresentstudyperiod,theuseofCTscansincludingthechesthadbeenfullyimplementedinthestagingofnewlydiagnosedCRCpatients.AsforstudyII,datawereextract-edfromtheDCCGdatabase,theNPRandtheDPR.Patientswerescannedwitha64-slicemultidetectorCTscannerandallscanswereassessedtwice.Aprimaryassessmentwasperformedpro-spectivelyaspartofthestagingprocedureandplanningoftreat-ment.Avastnumberofradiologistsperformedthisprimaryre-view.Secondly,anexperiencedthoracicradiologist,whowasblindedtotheprimaryassessment,reviewedthescansretrospec-tivelyforthisstudy.Thethoracicradiologistassessedthescansaccordingtoapreformeddataextractionsheet,andclassifiedscansintofourcategories:1)normalscan;2)benignpulmonarylesions;3)IPNor4)SPCM.IncaseofIPNorSPCM,thelesionsweredescribedindetailsregardingsize,number,location,calcifi-cation,ground-glassopacityandconsistencyandthedatawereenteredintoadedicateddatabase.AllreportsfromtheprimaryassessmentwereretrievedintheregionalPictureArchivingandCommunicationsSystemandmanuallysearchedforthesameinformationasreportedbythethoracicradiologist.Aresearch
assistant,blindedtothefindingsofthethoracicradiologist,ex-tracteddatafromtheprimaryscanreportstoadatabase,whichwasfinallymergedwiththedatafromthethoracicradiologist’sreviewanddatafromthenationalregistriesusingeachpatient’suniqueDanishcivilregistrationnumber.Additionally,allreportsonfollow-upradiologicalexaminationsincludingthechestfollow-ingtheinitialstagingCTwerereviewedinpatientswithIPNde-tectedateithertheprimaryorthoracicradiologist’sreport.SPCMdetectedattheseexaminationsweretobelocatedinthesamelocationastheinitialIPNtoconcludethattheSPCMoriginatedfromthisIPN.
Thelevelofinter-readeragreementbetweenradiologistswastestedwithKappastatistics.Radiologistperformancewascalcu-latedassensitivityandspecificity.MultivariablelogisticregressionwasusedtotestforassociationbetweenclinicopathologicalvariablesandamalignantnatureofIPN,whereasmultivariablelinearregressionwasusedtoassesstheimpactofadetectedIPNontimetosurgeryfortheCRC.
ResultsIntotal,841patientswereincludedofwhom8.7%(n=73)provedtohavepulmonarymetastaseseitherbyradiologicalfollow-uporhistologicalverification.IPNsweredetectedin82cases(9.8%)intheprimaryCTreviewascomparedto47(5.6%)bythededicatedthoracicradiologist.Inpatientssubjectedtoradiologicand/orinvasivefollow-up,IPNswereconcludedtobemalignantin20/73(27.4%,primaryassessor)and10/42(23.8%,thoracicradiologist).
ChestCTdiagnoseswereconsistentbetweentheprimaryandthoracicradiologistsin81.8%ofthecasesandoverallkappawas0.49(95%CI0.43–0.55),correspondingwithmoderateagree-ment[53].
Kappaforthecategories“IPN”and“SPCM”were0.31(fairagreement)(95%CI0.24–0.37;P<0.001,McNemar’stest)and0.65(95%CI0.58–0.71;P<0.001)(substantialagreement),re-spectively.
Timetoindextumourresectionwas13daysinpatientswithanormalscanorbenignnodulesonlycomparedwith20daysforpatientswithIPN.DiagnosisofIPNwasassociatedwithanaver-agesurgicaldelayof14days(95%CI2–27days;P=0.029)com-paredwithpatientswithnormal/benignfindings.NoneoftheevaluatedradiologicalfeaturesoftheIPNasassessedbythethoracicradiologistweresignificantlyassociatedwithmalignancyofthenoduleatfollow-up.
ConclusionAconsiderablenumberofradiologistsassessedtheprimaryCTscansandwithsomevariabilityinfindingswhencomparedtoadedicatedthoracicradiologist’sclassification.NoradiologicalfeaturesofIPNswerefoundpathognomonicformalignancyofthenodule.Notsurprisingly,thepresenceofsynchronouslivermetastaseswasassociatedwithahigherriskofmalignantnatureoftheIPN.Finally,timetoresectionoftheprimarytumourwasprolongedinpatientswithIPNcomparedtopatientswithnon-suspiciouspulmonaryCTfindings.
LimitationsTherearesomeimportantlimitationstothisstudy,mostofwhicharesharedwithotherpulmonarynoduledetectionstudies.Firstofall,theoutcomesoftheIPNsweredeterminedbyreviewingtheresultsoffollowupradiologicalexaminations,andonlyfewpatientsweresubjectedtothe“goldenstandard”histological

DANISH MEDICAL JOURNAL 6
verification.IPNshadtoincreaseinsizeand/ornumbertobeconcludedtobemalignantatfollow-up.
Potentially,pulmonarymetastasesinapatientsubjectedtoadjuvant/palliativetherapycouldremainstableinsize.ResultsareflawedifsuchmetastaseswereregisteredasIPNs.
Someofthedifferencebetweentheprimaryandexpertre-viewcouldbeattributedtotheimplicationoftheradiologicaldiagnosismade.Thus,theexpertreviewdiagnosisis“only”forstudypurposes,whereasthe“reallife”primaryassessmentshaveimplicationsforthepatient’streatment.
Theoretically,theprimaryradiologistmaythereforebereluc-tanttodesignatealesion“benign”or“malignant”definitively.
Furtherlimitationscanbeattributedtotheretrospectivede-signofthestudy.Notallpatientsweresubjectedtoastandard-izedfollow-upregimenortimetofollow-upradiologicalexamina-tion.Aprospectivedesigncouldhaveallowedforanassessmentoftheimpactofanindeterminatefindingandsubsequentexami-nationsonqualityoflifeandpotentiallyacostbenefitanalysisofsuchadditionalexaminations.
DuetolimitationsregardingbothradiologicalresourcesandnumberofCTscanswewerenotabletohaveanotherdedicatedthoracicradiologisttodoare-reviewoftheCTscans.Itwouldhavebeeninterestingandindeedscientificallyrelevanttocontrolforthe“expert”.Withanestimatedproportionofdisagreementbetweentwo“experts”of0.1thesamplesizeofscanstobereviewedbyasecond“expert”wouldbe1,603withasetkappaof0.8anda95%CIfrom0.75-0.85.
STUDYIVMismatchrepairandsynchronousmetastasesincolorectalcancer:anationwidecohortstudy
AimThisstudyaimedtoinvestigate,1. whethertheroutinelyassessedMMRstatusofthecolorectal
tumourwasassociatedwiththelocalizationofsynchronousmetastaticdiseaseasthiscouldbevaluableintheassessmentofIPNonthestagingCT
2. andtheimpactofMMRonsurvivalinpatientswithstageIVdisease
MethodsAsforstudyIIandIII,thepatientcohortwasidentifiedintheDCCGdatabase,anddatafromtheDCCGweremergedwithdatafromtheNPRandtheDPR.ThisstudyevaluatedallpatientswithafirsttimediagnosisofCRCbetween2010and2012forinclusion.Patientswithhistologicallyverifiedcolonicorrectaladenocarci-nomasinwhomMMRproteinexpression(MLH1andMSH2)analysiswasperformedbyimmunohistochemistry(IHC)wereeligible.
DataonhistopathologywereextractedfromtheDPR.TrainedpathologistsassessedallspecimensaccordingtotheTNM5thEdition.ThemismatchrepairanalysesusingIHCfollowedtheguidelinesfromtheNordicImmunohistochemicalQualityControl[54].
AssociationsbetweenvariablesandsynchronousmetastaticdiseasewereanalysedwiththeChi-squareandMann-Whitney-Wilcoxontestsforcategoricalandcontinuousvariables,respec-tively.
Multivariableandmultinomiallogistic-andCox-regressionandproportionalexcesshazardsanalyseswereusedforcon-
founderadjustmentandtoadjustforthegeneralpopulationmortality.
ResultsIntotal,6,692patientswithcompleteregistrationofMMRstatuswereincluded.AdeficientMMRoccurredin983ofthepatientsandwasmorecommoninfemales,inelderlypatients,inproximaltumoursandindistincthistologicalsubtypes.TheriskofvenousinvasionorlymphnodemetastasiswaslowerinpatientswithdeficientMMRcomparedwithaproficientstatus.
SCCMwerepresentin935patientsinthefinalstudycohort(14.0%).Liver(566/935,60.5%)andpulmonarymetastases(204/935,21.8%)werethemostcommonmetastaticlocations.Onehundredtwenty-fourpatientshadmultiplemetastases,themajorityhavinghepaticmetastasesaswell(117/124,94.4%).Metastasectomywasperformedin30(14.7%)withpulmonarymetastases.
PatientswithdMMRhadadecreasedriskofhavingSCCM,OR=0.54,95%CI:0.41-0.71,P<0.001.dMMRwasassociatedwithadecreasedriskoflivermetastasesinmultinomiallogisticregres-sion(OR=0.30,95%CI:0.18-0.49,P<0.001),butnostatisticalsignificantassociationwasfoundforeitherpulmonarymetastases(OR=0.71,95%CI:0.39-1.29,P=0.258)ormetastasesinbothliverandlung(OR=0.26,95%CI:0.26-1.77,P=0.436).
Finally,wefoundthatdMMRhadnosignificantimpactonsurvivalintheunivariableCoxregressionanalysis,HR=1.24(95%CI:0.91-1.70,P=0.166),orintheunivariableproportionalexcesshazardsanalysis,HR=1.26(95%CI:0.90-1.76,P=0.183).NordidMMRstatusinfluencesurvivalinthemultivariableanalyses.
ConclusionPatientswithdMMRhaddecreasedriskofsynchronousmetastat-icdisease,buttheassociationwaslimitedtohepaticmetastases.SurvivalinstageIVpatientswasnotinfluencedbyMMRstatus.
LimitationsDuetothemethodologicalsimilaritieswithstudyIIthepresentstudyhassomeofthesamelimitations.
Additionally,therecommendationsforMMRimmunohisto-chemistry(IHC)wererevisedduringthestudyperiodresultinginarelativelyyoungerpatientpopulationinthebeginningofthestudyperiod.Secondly,only75%ofthepatientseligibleforthestudywereMMRIHCtested.Thesetwopointsmayresultinsomedegreeofselectionbias.
DeficientMMRtumourswerepresentedasasingleentity.Thismaybeanoversimplification.
Itiswell-knownthattumourmorphologyandbehaviourde-pendontheetiologyoftheMMRdeficiencyandthesecondarymutationsresultingfrommicrosatelliteinstability[55].
ThenumberofdeficientMMRtumoursmaybeslightlyun-derestimatedduetotheIHCtestingapplied.IHCdetectsabout95%ofMMRdeficienttumours.AmissensemutationintheMLH1genecanresultinanon-functional,butIHCdetectableprotein[56].
Finally,theriskofatypeIIerrorregardingthesignificanceofMMRstatusonpulmonarymetastasisshouldbekeptinmind.Fewpatientshadconfinedpulmonarymetastasesrelativelytopatientswithhepaticmetastasesandonlyfewofthepulmonarymetastaseswerehistologicallyconfirmed.Oneshouldtakecau-tiontogivedefinitiveconclusionsontheimpactofMMRstatusonextra-hepaticmetastasis.

DANISH MEDICAL JOURNAL 7
METHODOLOGICALCONSIDERATIONS
ThisthesisislargelybasedonprospectivelycollecteddatafromtheDCCGdatabase.Inthissectionsomeaspectsofthemethodo-logicalapproachtohandlingthesedataforthisthesiswillbediscussed.TheapproachesweresimilarinstudiesII,IIIandIV,andwillbedescribedcollectively,thoughsmalldifferencesexist-edregardingtherelevantstudyperiodanddemographytosatisfytheindividualstudyobjectives,availabilityofCTscansanddatafromotherdatabases.
DatahavebeenprospectivelycollectedintheDCCGdatabasesincethe1stofMay2001onallnewlydiagnosedcolorectalcan-cercasesinDenmarktosurveythatthequalityofCRCtreatmentadherestothedesiredclinicalstandard[57].Furthermore,asthepatientcompletenessiscurrently>98%,[58]thecollectionofuniformandstandardizeddataenablestheconductionofna-tionwide,epidemiologicalstudiesrepresentativefortheDanishpopulationwithlowriskofselectionandreferralbias[59].Previ-ousrandomcheckshavefoundahighvalidityoftheDCCGdata[60].AmonthlylinkagetotheNPRservestovalidatethecom-pletenessofdata.
AllsurgicaldepartmentsregisterdataonpatientswithnewlydiagnosedCRCprospectivelyintothedatabaseanddepartmentsarenotifiedofmissingdataandlogicalerrorsinthedatareport-ing[61].
DataonallpatientsintheDCCGdatabasewereadditionallyretrievedfromtwoothernationwidepatientregistries:theNPR(registryofallpatientsadmittedtoDanishsomatichospitals,emergencyrooms,andoutpatientclinics)andtheDPR(registryofallindividualsinDenmarkwhohavehadahistologicalexamina-tionoftissue,cell,orautopsymaterial)[61].ThelinkbetweenthreenationwidedatabasesservedasasourceforidentificationofconfoundersnotregisteredintheDCCGdatabase.Importantly,thismergealsoservedasavalidationofvariablesregisteredintheDCCGdatabase.Incaseofamismatchbetweenthedatabasesonspecifickeyvariables,amanualsearchinthepathologyandpatientregistries,patientrecordsandradiologyreports(ifavaila-ble)wasconducted.ThekeyvariablesincludedthediagnosisofCRC,dateforthe(firsttime)diagnosisofCRC,UICCstageatthetimeofdiagnosisandcourseoftreatment.Themergeofdataacrossdifferentregistriesisuncomplicatedduetotheuniqueandpersonalcivilregistrationnumber,giventoallDanishcitizensatbirth.Themergeandmanagementofdatawasconductedcen-trallybytheDCCG’sdatabasemanagertoensurecleandatasetsforstatisticalanalyses.
ThoughtheDCCGdatabasehasbeenreportedsufficientquantitativelyaswellasqualitatively,theaccuracyofthemeta-staticcodingisnotknown.Potentialunder-andover-recordingofmetastaticspreadcouldleadtobiasedestimatesofassociation.Thereforeafurthervalidationontheregistrationofsynchronousmetastaticdiseasewasdeemedessentialtofulfiltheobjectiveofthethesis.
Additionally,thisvalidationsoughttoensurethatregisteredmetastaticdiseasewasactuallysynchronousandmostlikelydidoriginatefromacolorectalcancer.
TheprimarytumourItwasofparamountimportanceforinclusion,thatpatientshadahistologicalverificationoftheircolorectalcancer.HistologicalverificationonthediagnosiswasobtainedfromtheDPR.Ifapatienthadnotbeensubjectedtosurgeryoranyotherhistologi-calexamination,thediagnosisofamalignantcolorectaltumourhadtobeverifiedbyatrainedcolorectalsurgeonforthepatient
tobeincluded.InthesecasestheCRCdiagnosisintheDCCGdatabasehadtocorrespondtoaCRCdiagnosisintheNPR.
Onlypatientswithafirst-timediagnosisofCRCfromthecommencementofCRCregistrationintheDCCGdatabasefrom2001andonwardwereincluded.ThepatientwasexcludedinthecaseofapreviousregisteredspecimenintheDPRsuggestingCRCtominimizetheriskofanalysingdataonrecurrentCRCcasesormetachronousmetastaticdisease.Furthermore,thiswasdonetoensurethatdatafromtheregistriesconcernedtheprimarystag-ing.
MetastasesSynchronousmetastaticdiseasewasdefinedasanydetectedmetastaseswithinatimeframeof30dayspriortill120daysafterthediagnosisoftheindexcancer.Thereexistsnodefiniteconsen-susregardingthedefinitionofsynchronousandmetachronousmetastases.Thefourmonths’timerangeisinlinewiththe“timeofstagingdata”accordingtotheAmericanJointCommitteeonCancer[18].Intheliterature“synchronous”representslesionsdetectedbothatthetimeofresectionoftheindexcancer,andwithin3,6,or12monthsfromthediagnosisoftheindexcancer,butthetermisoftennotpreciselydefined[62-66].Accordingtomedicaldictionaries“synchronous”referstolesionsorconditionsattimesofaneventofinterest[67].Inthegivencase,theeventofinterestistheprimarystaging.Wedefinedtheprimarystagingasanydiagnosticwork-upperformed30daysprior-till120daysafterthediagnosisoftheindexcancer.Itistheassumptionthatanydetectedmetastaticspreadwithin120daysfromthediagno-siswaspresentatthetimeoftheCRCdiagnosiseventhoughitwasnotdetectedatthispoint.
Indeterminatehepaticand/orpulmonarylesionsdetectedatthestagingproceduresshouldnotberegisteredasmetastasesinthedatabaseaccordingtotheDCCGregistrationguidelines.Ap-plyingatimeframefordetectionof“synchronous”metastasesthereforeallowsforafollow-upCTscanforclarificationofsuchpotentialindeterminatelesionsatthreemonths,whichisclinicalpracticeinsomeDanishcolorectalcancercentres.Subsequentexaminationswereassumedtocontrolforrecurrentdiseaseinpatientsnotpreviouslyregisteredwithdisseminateddisease.TheDCCGdatabaseholdsnoinformationonrecurrent/metachronousdisease.The30-dayslimitpriortothediagnosisoftheCRCissomewhatarbitrarily,butensuredthatallrelevantdiagnosticproceduresinthestagingprocesscouldbeidentifiedintheNPR.
Noneofthepatientsinthedatabasehadmetastasesregis-teredpriortothese30days.Anepidemiologicalcriticismtothistimeframeisthediagnosisofsynchronousmetastasesinpatientswithafollow-upshorterthan120days.Potentially,somepatientsmaydiewithinthese120daysandtherebybeforethefinaldiag-nosisofsynchronousmetastaticdisease.
Avalidationofregisteredpulmonarymetastaseswasper-formedondataobtainedfromtheDCCGdatabaseastheaccura-cyofthe“pulmonarymetastases”diagnosisisofparamountimportanceforthisthesis.Asstatedabove,onlydefinitepulmo-narymetastasesonradiologicaland/orhistologicalevaluationaretoberegisteredintheDCCGdatabase–notindeterminatefind-ings.
TheDPRwasscrutinizedforanyhistologicalconfirmationofmetastaticdisease.Inmostofthecasesthis“goldenstandard”verificationcouldnotbeobtained.Thereforedataonallradiolog-icalproceduresperformedduringtheprimarystagingperiodwereextractedfromtheNPR.Patientswereexcludediftheyhadnohistologicalverificationofapulmonarylesionornorelevantradiologicalprocedure.

DANISH MEDICAL JOURNAL 8
TheDPRwasalsoreviewedfordataonothermetastasesthanpulmonaryregisteredintheDCCGdatabase,butnoequivalentrestrictionsondiagnosisoftheseextra-pulmonarymetastasesinrelationtoradiologicalorsurgicalprocedureswereapplied.
WeusedtheDPRtodetectsynchronousmetastaticdiseaseinthecaseswherenoinformationwasavailableintheotherregis-triesregardingthecancerstageatdiagnosis.Patientswhosecancerstageremainedundeterminedwereexcludedasthestageofthediseaseisessentialtoallaspectsoftheincludedstudies.
OthercancersthanCRCPatientswithothercancersthanCRC(exceptfornon-melanomaskincancers)fiveyearspriortillfiveyearsaftertheCRCdiagnosiswereexcluded.Ithasbeenarguedthatpatientswithmultiplemalignancieswillbecomeanincreasinglyimportanttopicincan-cerepidemiologyduetoanincreasingnumberofcancersurvivors[68].Liuetal.foundthat9%ofpatientswithaninitialCRCdevel-opasubsequentmalignantdisease.
Inanepidemiologicalperspectiveitwouldhavebeeninterest-ingtohavethecovariate“Othercancer”availableforthemulti-variableanalysis.Patientswithconcomitantcancerswere,how-ever,excludedforseveralreasons.InsomecasesothercancerformshadinitiallybeeninterpretedasCRCandfaultyenteredintheDCCGdatabase,typicallynon-CRCwithinvasiontotherectumorcolonandanalcancersregisteredasrectalcancers.Inothercaseshistologicalsamplingofwhatwasthoughttobedissemina-tionoftheCRCrevealedothercancers–e.g.histologicalsamplingofpulmonarymetastasesrevealingprimarylungcancers.
AreviewofallcaseswithspecimensregisteredintheDPRwasundertakenincooperationwithanexperiencedgastrointes-tinalpathologisttodeterminewhetherthehistologicalsubtypewasconsistentwithCRCineachcase.Additionally,areviewwasdoneinallcasesregisteredwithanothercancerthanCRCintheabdomenorthoraciccavitytoidentifycaseswherepotentialdirectinvasionormetastasesfromtheCRCerroneouslyhadbeenregisteredasanothercancer.Despitetheinitialintentiontoin-cludeallpatientsintheDCCGdatabaseandpotentialepidemio-logicalconcerns,itwasdeemednecessarytoexcludepatientswithevidentothercancerthanCRCafterthesereviewstoensurethat1)patientsactuallyhadCRC,2)metastasesdidoriginatefromtheCRCand3)thatdataononcologicaltreatmentextractedfromrelevantdatabasesconcernedtheCRC.
DISCUSSION
PrincipalfindingsPulmonarylesionsarecommonattheinitialstagingofcolorectalcancers,andthefrequencyhasincreasedwiththeintroductionofcomputedtomographyscans.Fewofthelesionswerehistologi-callyconfirmed.Theaccuracyoftheradiologicalcharacterizationisthereforeofparamountimportance.Survivalprognosisfortheincreasingnumberofpatientsregisteredashavingadefinitepulmonarymetastasiswasseverelyimpaired.However,thede-tectionofthesemetastasesisimportantassomepatientscanbecuredwithmetastasectomyandothersmaybenefitfrompallia-tivechemotherapyandresectionoftheindexcancer.Themeta-staticdiseasewasconfinedtothelungsinmorethan1/3ofthepatientswithpulmonarymetastases.
Unfortunately,asubstantialnumberofthepulmonarynod-ulescannotbeclassifiedasmetastasesorinsignificantbenignlesionsatthetimeofthestaging.Thenumberandclinicalsignifi-
canceoftheseindeterminatenodulesdependontheevaluatingradiologist.Theriskofmalignancywasabout10%inasystematicreviewofpreviousstudyresultscomparedwith20%ofIPNsdetectedataCTreviewbyanexperienced,thoracicradiologistofalocalcohortofmorethan800consecutivepatientswithnewlydiagnosedCRC.TheCTstagingscanhasahighspecificityforpulmonarymetastases,butthesensitivityisimpairedduetotheindeterminatelesions.Despitemultiplestudiesnopathognomon-icradiologicalfeatureformalignancyofanindeterminatepulmo-narynoduleexists.Arectalindexcancer,liverandlymphnodemetastases,tumourdepositsandvenousinvasionarefactorsassociatedwithpulmonaryspread,however,theiruseinthemanagementofIPNsremainsuncertain.Potentially,biomarkerscouldbeofsomevalueindeterminingthetruenatureoftheseindeterminatelesions.MismatchrepairstatushadnosignificantimpactontheoccurrenceofsynchronouspulmonarymetastasesandisthereforeunlikelytohavevalueintheclinicalmanagementofIPNs.
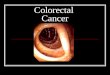
CRCandthemetastaticprocessColorectalcancer(CRC)isasignificantcauseofmorbidityandmortalityworldwide.In2012,GlobalCancerStatisticsestimatedmorethan1.3millionincidentcasesandalmost700,000deathsfromCRC[69].AccordingtotheDanishCancerRegistrymorethan4,400patientswerediagnosedwithcolorectalcancerinDenmarkin2011[70].HenceCRCwasthethirdmostcommonlydiagnosedcancerinDanishmenandsecondinDanishwomen,andthethirdmostcommoncauseofcancerdeathinbothgenders[70].Ap-proximately90%ofalldeathsinpatientswithCRCareduetometastaticdissemination[71].Earlydetectionisofparamountimportancewithregardstothechanceofcure,however,atpresentation15-25%ofthepatientswillhavemetastaticdisease[72].Figure1depicts5-yearsurvivalforpatientswithconfinedsynchronouspulmonarymetastasesincomparisontosurvivalforpatientswithUICCstageI-IIIdiseaseatthetimeofdiagnosis.
Figure1
SurvivalaccordingtoUICCstage(basedonstudyIIdata)[2] Colorectalcancersareheterogeneous.Despitebeingthebest-examinedtumourentitylittleisknownaboutthemoleculardeterminantsformetastasis[71].Stablefrequenciesfordissemi-nationtospecifictargetorganshasbeenarguedtosuggestforamolecularbackgroundofthemetastatictropism[72].Themajori-tyofcolorectalcancersareadenocarcinomasdevelopingfrombenignprecursors,adenomas,inamulti-stepprocessofmuta-

DANISH MEDICAL JOURNAL 9
tionsandepigeneticchangesintumoursuppressorgenesandoncogenes[73].Sincethefirstmodelofcolorectalcarcinogenesismorethan20yearsago,[73,74]ithasbecomeclearthatCRCdevelopsthroughseveralheterogeneousmolecularpathways[75-77].Awarenessofthisheterogeneityisimportant,asitmayhaveconsequencesforthemetastaticpotentialoftheCRC[78,79].
Theunderstandingofmetastasis,theshiftfromlocalizedtosystemicdisease,isessentialinCRCtherapyandisnecessarytoaddressforfutureinterventionandpreventionstrategies[6].MorethanacenturyagoPagetdescribedthemetastaticprocessinbotanicalterms,theso-calledseed-and-soiltheory,inwhichthedistributionofthemetastasesisnotsimplyamatterofchance[80].Theprimarytumouraswellasthepredilectionsiteformetastasescouldpossessspecificpropertiesthatpredisposesecondarygrowthatspecificlocations[72].Thoughtheunderly-ingmolecularabnormalitiesforCRCcarcinogenesishavebeenextensivelyinvestigated,littleisknownaboutthedeterminantsforthemetastaticformation[71].ThetraditionalperceptionofmetastasisinCRChasthereforeadheredtothecascadehypothe-sis,inwhichtheliverisaffectedfirstlyasmostofthevenousbloodfromthecolonenterstheportalveinandtherebytransferscancercellstothelivercapillaries[81-83].Subsequently,pulmo-narymetastasesarisefromlivermetastasesandfinally,arterialmetastasesdevelopfromthepulmonarymetastases[83,84].
PulmonarymetastasesBlalockisoftencreditedforperformingthefirstpulmonaryme-tastasectomyincolorectalcancerin1944[85].
Actually,thispaperreferstoapneumonectomyofalungco-incidentallyaffectedbyCRCmetastasis.Atthistimesurgeryinthetreatmentofpulmonarymetastaseswereregardedasobsoleteasthediseasehadescapedthe“first”hepaticfilterandtherebywassystemic[86].
Todaynationalandinternationalguidelinesrecommendpul-monarymetastasectomywhenpossible[30,31,87].AsurveyofthecurrentpracticeamongmembersoftheEuropeanSocietyofThoracicSurgeonsfoundthatpulmonarymetastasectomyrepre-sentsupto10%ofthesurgicalactivityandwasperformedby99.3%oftherespondersintheCRCsetting[88].Criteriaforsurgi-calinterventionadheretotheprinciplesintroducedin1965byThomfordetal.andrequirethatprimarytumourisundercontrol,noextrathoraciclesionsarepresent(exceptforresectablelivermetastases),themetastasesappeartechnicallyresectable,andthegeneralandfunctionalrisksaretolerable[89].Thepracticeofpulmonarymetastasectomyisbasedonmainlyretrospectivedataofhighlyselectedpatientseriesdespiteawidespreadconductionandguidelinerecommendationofsurgicalintervention[90].Thesestudiesreport5-yearsurvivalratesofupto40-60%[90].ThisprognosisisinlinewiththeresultsofstudyII,however,onlyasmallfractionofthepatientsweresubjectedtopulmonaryresectionandtheresultsaremostlikelyaffectedbyselectionbiasorconfoundingbyindication.Thefirstrandomizedtrial,Pulmo-naryMetastasectomyinColorectalCancer[PulMiCC]iscurrentlybeingundertaken[91].Anoptimalassessmentofthetherapeuticstrategyinthesepatientsnecessitatesfurtherclarificationoftheunderlyingepidemiologyandcontroversiesintheoptimaldiag-nosticapproach.
TrendsindetectionInconcordancewiththecascadehypothesisandpreviousfind-ings,thelungswerethesecondmostcommonlocationforsyn-chronousmetastaticspreadinCRC,onlysurpassedinnumberby
livermetastases[2,15,20].Itiswellestablishedthatthelungsarethemostcommonextra-hepaticlocationfordiseaserecur-rence,[92]butdataonsynchronouspresentationonpulmonarymetastasesaremorescarce[20,22,65].Inthisthesis,thepreva-lenceofsynchronouspulmonarymetastaseswasinvestigatedforthefirsttimeonanationwidebasis.Mitryetal.[20]investigatedtheepidemiologyandprognosisofcolorectalcancerinaFrenchregionalcohortfrom1976to2005anddiscoveredanearlythree-foldincrementintheestimatedprevalenceofSPCM.Despiteanearlierdiagnosisovertime,theoccurrenceofmetachronouspulmonarymetastases(inpatientsresectedforcureandfollowedwithayearlychestX-rayfor5years)didnotchangeduringthestudyperiod[20].ThesetrendswereattributedtoanincreasinguseofCT-scansovertimethoughdataonthestagingprocedurewerenotavailable.In2005pulmonarystagingwithCTscanswerenotfullyintegratedatallcentrestreatingCRCinDenmark.AsfoundintheFrenchstudythecontinuousimplementationofchestCTfollowingnationalguidelineswasassociatedwithanincreasednumberofregisteredSPCM.
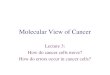
TheuseofpreoperativestagingwithCTofthechestincreasedsignificantlyfrom9%in2001–2004to63%in2009–2011withaconcomitantincreaseinthenumberofregisteredpulmonarySCCMfrom5.0%to9.3%(Figure2).TheincreasingapplicationofCTcanonlyexplaintheincreasedregistrationofpulmonaryme-tastasesinpart.Otherpotentialdeterminantscannotbeextract-edfromouravailabledata,butanincreasedawarenessandcon-comitantregistrationofpulmonarymetastases,increasingexperienceofevaluatingradiologistandimprovingscanningtechnology(e.g.theintroductionofmulti-slicescanners)maybeofimportance.
Figure2
NumberofstagingchestCTscansandsynchronouspulmonarymetastasesintheDanishCRCcohortfrom2001-2011
StagingchestCT-proetconThenecessityofasensitivepulmonarystagingmodalityisunder-linedbytheprognosticeffectofthedetectedpulmonarymetas-tasesandthefactthat>90%ofthesemetastasesaresolelybasedonaradiologicaldiagnosis.Furthermore,ahighaccuracyofthestagingisimportanttoavoidfirstlyunnecessarysurgeryinpa-tientswithnolungmetastases,andsecondlythepotentialexclu-sionofpatientswithasurgicallycurablediseasefromapotential-lybeneficialprocedure.

DANISH MEDICAL JOURNAL 10
TodayapreoperativestagingchestCTisrecommendedintheDCCG’sguidelines,[32]theNationalComprehensiveCancerNet-workguidelinesforbothcolonicandrectalcancer[30,31]andtheAssociationofColoproctologyofGreatBritainandIreland[33].InthepositionpaperfromtheEuropeanRegistrationofCancerCaremultidisciplinaryconsensusconferencein2012itisstatedforcoloniccancerstaging:“Chest-CTasroutinework-upisrecom-mended;althoughthereisevidencethatachestX-raymaybeusedforroutinework-up”andinthesectionforrectalcancerstaging“AbdominalCT,chestX-rayorCTaretheminimalre-quirementsforstagingofdistantmetastases.Thoracicandab-dominalCTarerecommendedaspartofthestagingprotocoltodetectdistantmetastases,especiallyforhighriskrectalcancer”[93].Despitebeingfullyintegratedinthediagnosticwork-up,thevalueofaroutinelyperformedstagingchestCThasbeensubjecttomuchdebate.ThisisalsothereasonwhychestX-rayisstillacceptedinthediagnosticwork-upaslistedabove.Itiswellestablishedthatthepick-uprateofpulmonarymetastasesishigherinCTthanconventionalchestX-ray[34].Thisisduetoahigherspatialresolutionandthelackofsuperimposition,andCTdetectssmallernodulesatanearliertime[94].
However,scepticsdoubtanybeneficialclinicalimplicationsofthehigherdetectionrate.Furthermore,concernisraisedregard-ingthepossibledelayedtreatment,prolongedanxietyandaddi-tionaldiagnosticprocedureswithaccompanyingcostandradia-tionexposureduetoavastnumberofindeterminatepulmonarylesionsonCT[24].AreviewofstudiescomparingchestCTandchestX-rayfoundlimitedevidenceforusingchestX-ray[34].TheimplicationsofthehigherdetectionratebyCTwere,however,unclear[34].Inthesettingofmetachronouspulmonarymetasta-sesearlydetectionbyCTaccompaniedbyaggressiveresectionhasbeenassociatedwithfavourablesurvivalprognosis,[95]whereasyearlychestX-rayisofquestionablevalue[96].ThesesurrogatemarkersfortheeffectsofchestCTandX-raymaynotbedirectlytranslatedtoastatementregardingtheirrelevanceinthedetectionandtreatmentofSPCM.SPCMmayimplyamoreaggressivediseasewithpoorersurvivalratesthaninpatientswithmetachronouslesions,[97]butasformetachronouslesionsearlydetectionbeforefurtherdisseminationmayimprovethechanceofcurativesurgery[90,98].SomeauthorsproposethatchestCT
shouldbereservedforhigh-riskpatients;i.e.patientswithrectalcancer,livermetastasesornodepositivedisease[21-24,99,100].Unfortunately,evenpatientswithearlystageCRCdeveloppul-monarymetastasesand37%ofpatients(asfoundinstudyII)withpulmonaryinvolvementwillhavenodetectableextra-thoracicdissemination.Tanetal.foundanincidenceof5.9%ofisolatedpulmonarymetastasesinpatientswithcoloniccancer[22].
ThetruevalueofachestCTcanonlybeassessedinapro-spectivestudywheretheinitialsurgicalintentisknownbeforefurtherinvestigationsareperformed.AvalueoftheinitialstagingCT(oftennotdiscussed)isitsuseasabaselinestudyintherou-tinefollow-upafter12and36months(accordingtoDanishguide-lines[101])fromtheradicalresectionoftheindextumour. AschestCTiscurrentlyfullyintegratedinournationalguide-linesandeverydayclinicalpracticeadiscussiononitsrelevanceinstaginginrelationtoCXRhasbecomeobsolete.Rather,futurefocusmaybeonthepotentialintroductionofPET/CTintopulmo-narystaging.Theidentificationofpatientsinhighriskforpulmo-narymetastasesmay,however,stillbeofgreatimportanceinrelationtothestagingCT;notforthepreclusionofscansinsomepatients,butforadditionalguidance,whenindeterminatelesionsareencountered.
IndeterminatePulmonaryNodulePulmonarymetastasesmaypresentinnumerouswaysonchestCT.Asimpleexhaustiveandcompletedefinitionofapulmonarymetastasesincolorectalcancerbasedonradiologicalfeaturescannotbegiven.Asmostoftheradiologicalfeaturesareunspecif-icformetastasesandnopathognomoniccharacteristicsexist,asubstantialnumberofthepulmonarynodulescannotreadilybeclassifiedaseitherbenignormalignantimpairingthespecificityoftheCT.Oftenthenodulesofmetastaticoriginareroundedlesionsofsofttissueattenuationvaryinginsize,well-circumscribedandlocatedintheperipheryandlowerpartsofthelungs[102].
Asforotheradenocarcinomas,pulmonarymetastasesofcolo-rectaloriginmaypresentassinglelesions.Thepresenceofmulti-plepulmonarynodulesinpatientswithaknownextra-thoracicmalignancytypicallyindicatespulmonarymetastasis,butradio-logicalcharacteristicsremainunspecific;especiallywhenonlysinglelesionsareencountered[102].Theradiologicalappearance
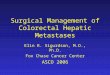
Figure3
SolitaryIndeterminatePulmonaryNodule(redarrow)detectedatstagingCTscan

DANISH MEDICAL JOURNAL 11
ofpulmonarymetastasesmayfurthermoredependontherouteofdissemination[103].
Mostmetastaticnodulesarelessthan1cmindiameter,butincreasingsizeofpulmonarynoduleshasbeenassociatedwithelevatedriskofmalignancy[51,104].Growthcharacteristicsofmetastaticnodulesvary(eveninthesamepatient)andvolumedoublingtimehasbeenreportedfrom11to150daysforcolorec-talcancer[105].Growthisafeaturethatcanbealteredwhenchemotherapyisadministered.Thisalsoappliestocalcificationandcavitationofthenodules,whichmaybetoounspecificfind-ingstodifferentiatemalignantnodulesfrombenignones[102].Furthermore,themetastasesmayhaveatypicalradiologicalmani-festationsmakingthediagnosisevenmoredifficult[106].Thediagnosticcriteriaforevaluatingandmanagingpulmonarynod-ulesadheretotherecommendationsdevelopedinlung-cancerscreeningtrials[43,107,108].Theaprioririskofpulmonaryma-lignancyinapatientwithacolorectalcancerisnotcomparabletoaparticipantinalung-cancerscreeningstudyandtheseguide-linesmaynotbedirectlyappliedtotheCRCsetting.Interestingly,inalung-cancerscreeningtrialtheprevalenceofsmall,non-calcifiedpulmonarynodulesdetectedonCTwas51%[108].
Recentlyadditionalstudiesinthecolorectalcancersettinghavebeenpublished[3,100,109-114].Resultsstillvaryandexter-nalvalidityofthesemainlyretrospective,single-centrestudiesareimpairedbydifferentdefinitionsofIPNs,typeofimagingperformed,patientcharacteristics,presenceofextra-thoracicmetastases,varyinginclusionofmetachronousnoduleswereincludedandexclusionofsomenoduleswithspecificmorphologi-calfeatures.Furthermore,resultsareimpairedbyvaryingfollow-upregimensanddefinitionsofamalignantoutcomeofthenod-ulesandrarelyincludeahistologicalverification.
ManagementofIPN–evaluationofexistingguidelinesSomestudiesonIPNintheCRCsettinghavestrivedtodevelopguidelinesonthemanagementofIPN.Gomezetal.[111]pre-sentedastrategyformanagementofpre-operativelydetectedIPNsinpatientsevaluatedforresectionoflivermetastases.Brief-ly,patientswithresectableliverdiseasewereresectedandre-assessedwithaPET/CTafterthreemonths.Ifpatientshadbor-derlineresectablelivermetastasestheywererecommendedtohaveaPET/CTpriortopotentiallivermetastasectomy.Baeketal.[115]failedtoestablishfollow-upguidelinesinpatientswithrectalcancerandIPNduetofewpatientshavingpulmonarymetastasesatfollow-up.Theysuggestedalongerfollow-upperi-odforpatientssubjectedtoFOLFOXtherapythanthosetreatedwith5-FUaloneornochemotherapy,asthetimetodevelopmentofpulmonarymetastaseswaslongerinpatientsinFOLFOXtreat-ment.However,thistimedifferencewasnotstatisticallysignifi-cantandtherecommendationisbasedonaverylimitedpatientcohort.NorcouldKimetal.[110]definitivelyconcludethatadju-vanttherapyhadimpactonthetimetoprogressionofIPNintodefinitemalignantlesions.Inthisstudyfiveriskfactorsformalig-nantprogressionwereidentifiedbeing:metachronousIPNs,arectalindexcancer,ahighernodalstage,bilaterallunginvolve-ment,andperineuralinvasion.Thesefactorswereusedtocon-structariskpredictionmodelaccordingtowhichthefollow-upofIPNcouldbeindividualisedfromnofurtherfollow-uptorepeatCTscanswith3monthsinterval.Unfortunately,perineuralinva-sionandnodalstatusmaynotnecessarilybeknowninthepre-operativeplanning.
Littleattentioninpreviousstudiesandguidelineproposalshasbeengiventotheexperienceoftheevaluatingradiologist,thoughexactlythisexperienceiscommonlylistedasoneofsev-
eralreasonsforvaryingresultsbetweenstudiesonIPN.InstudyIIItheinter-readervariabilityinthedetectionandcharacteriza-tionofpulmonarynodulesonCTscanswasfoundtobesubstan-tial.ThisisinlinewithresultsfromothersettingthanCRC[116-118].Apulmonarynoduleinitiallycharacterizedasindeterminatemaybereclassifiedaseitherbenignormalignantinasecondradiologicalreview[35,119].Evenbetweenexpertradiologiststhedefinitionof“truth”mayvary[116].Achallengeineverydayclinicistheinadequateaccessibilityofdedicatedthoracicradiolo-gistsforassessmentsofallstagingchestCTs.Thisissuecouldbereducedifasecondreview,byagroupofexperiencedthoracicradiologists,ofthescanswithIPNwasperformed.Intotal,only10%ofthestagingscansinthestudyIIIwouldhavehadtounder-goareviewbydedicatedthoracicradiologists.Ofcourse,thefeasibilityandvalueofthisapproachneedstobevalidatedinaprospectivetrial.
ManagementofIPN–proposalofnewguidelineBecauseIPNsaremostlikelyofbenignorigin,furtherdiagnosticworkupofthenodulesshouldnotpostponethetreatmentoftheindextumour;patientsshouldbetreated“inthebenefitofdoubt”.Preferablytreatmentplanningisbasedontheassump-tionthatIPNsarenotmalignantandarefollowedwithserialimaging.Additionalpre-operativework-uphasbeenproposedinpatientswithborderlineresectablelivermetastasesasstatedabove[111].ThelackofaconsensusinthedefinitionofIPNandvaryingCTtechniquesutilizedmakeitdifficulttomakeasingleomnipotentmanagementguidelinewithgreatexternalvalidityintheCRCsetting.Pre-operativelyknownclinicopathologicalfactors(besidessynchronouslivermetastases)andradiologicalcharac-teristicstobeusedintheriskassessmentofIPNareunconvinc-ing.Ithasbeenstated,thatnodulesizeistheonlymeasurablefactoronchestCT[110].
Bearingtheseresultsinmindandthefactthatthelevelofex-perienceoftheevaluatingradiologistisadecisiveparameterintheassessmentofIPN(asfoundinstudyIII),itmayberelevanttotaketheinter-observervarianceintoaccountwhenmanagementguidelinesofIPNsaresubmitted.InFigure4amanagementstrat-egyofIPNisputforward.
Itseemsclearthatsomenodulespossessobvioussignsofma-lignancyorbenignity.Thepatientshouldbesubjectedtothemultidisciplinaryteam(MDT)conferencewithrepresentativesfromabdominalandthoracicsurgery,oncology,pathologyandradiologyifthereisevidenceofpulmonarymetastases.Nofur-therfollow-upisnecessarybesidesroutineCRCsurveillanceifthenoduleisclearlybenign.InthecasewhereanIPNisencounteredintheprimaryCTreview,thescanistobeassessedbyagroupofdedicatedthoracicradiologists.Thiswillreservethelimitedavail-abilityofthoracicradiologicalexpertiseforasubsetofthestagedpatients.Thesecondaryreviewwilldeterminethefollowingwork-up.Ifpulmonarynodulesarestilldeemed“indeterminate”atthesecondreview,thepatientissubjectedtoalow-dosefol-low-upCTat3monthsintervaloraPET-CT,dependingonthesizeandpresenceofground-glassmorphology.Aground-glassnoduleis,accordingtotheFleischnerSociety,afocalnodularareaofincreasedlungattenuationthroughwhichnormalparenchymalstructurescanbevisualized,sometimesreferredtoasa“sub-solid”nodule[120].AsuspicionofmalignancymaypersistdespiteanegativeresultinsomeofthesmallestnodulesbeingPET-CTscanned.Thesepatientsmaybesubjectedtoalow-doseCTat3monthsintervalaswelltodeterminethepotentialgrowthrateofthenodule.Anodulethatappearsstableinsizeinsimilarprojec-tionsinaCTscanisconsideredmorelikelybenign[121].Inthe

DANISH MEDICAL JOURNAL 12
absenceofgrowthornewnodules,wesuggestthatthepatientcanbeallocatedtothestandardfollow-upregimenforthetreat-mentoftheindexcancer.
Figure4
ManagementofIndeterminatePulmonaryNodules.IPN,indeterminatepulmonarynodule;SPCM,synchronouspulmonarymetastases;GGN,ground-glassnodule;MDT,multidisciplinaryteamconference;CT,computedtomography
AccordingtotheDCCGthisincludesaCTofthechestandab-
domenat12and36monthsafteracurativeresection,[122]whichallowsfurtherassessmentofthenoduleformorethantherecommended2yearswithrespecttothetumourgrowthkineticsofadenocarcinoma[43,121,123].ThiswouldalsobesufficientforapotentialdelayintimetoprogressionofIPNinthecaseofadju-vantchemotherapy[110,115].InfewcasestheMDTcandecidetosubjectthepatienttoaCTguidedcorebiopsy.Thisisparticu-larlyusefulforperipherallesionsandhasbeenreportedtohaveamoderatespecificity,buthigh(>95%)sensitivityformalignantlesions[124].Theneedofatissuediagnosisshould,however,beweighedagainsttheriskofpneumothoraxandhemorrhage[121,124].Onceagain,itisofoutermostimportanceinanypro-posedguidelineforthemanagementofIPNdetectedatthepri-maryCRCstagingthatIPNandtherelevantdiagnosticwork-upshouldnotpersedelaythetreatmentandcaninitiallybedisre-gardedinthetreatmentofchoice.
ManagementofIPN–insearchforthefutureguidelineThemanagementstrategyasproposedaboveisrathersimpleandpragmatic.Optimally,reproducibleandobjectivepatientandnodulecharacteristicscouldaidtodeterminethefurtherwork-upandtreatmentofpatientswithIPNs[125].“PulmonaryNoduleMalignancyRiskcalculators”basedonBayesiananalysis,asde-velopedforeducationaluse,[126,127]aredesirable.ThediversityofradiologicalpresentationformsofpulmonarymetastasesandtheabsenceofradiologicalfeaturesinIPNofmalignantnaturelimittheuseofradiologicalcharacteristicsintheriskpredictionforamalignantnatureofIPN.
Notsurprisingly,characteristicsoftheCRCalreadyknowntobeassociatedwithmetastaticspreadtothelungsarealsofoundtobeassociatedwithanelevatedriskofanIPNbeingmalignantatfollow-up[38,39,42,48-50,100,109,110].Knownriskfactorssuchasrectalindexcancer,lymphnodespreadandhepaticin-volvementshouldwarrantahighdegreeofsuspicionofpulmo-
narymetastases.However,thesefactorsremainunspecificandtheirpotentialroleinthemanagementofIPNisyettobedefined.
Despitetheassociationbetweenarectalcancerandpulmo-narymetastasesinstudyIImorethan50%ofthepatientswithsynchronousmetastasesconfinedtothelungshadanindexcan-cerinthecolon.
Thedeterminantsformetastaticspreadrelatetoanatomicalfeaturesbutaremodulatedbytumour-hostinteractionsthatarecurrentlynotfullyunderstood,inlinewiththeseed-and-soiltheory.
Whethersuchtumour-hostinteractionsunderliesomeofthediscoveredassociationinstudyIIsuchasbetweenincreasingageandpulmonarymetastasisremainsspeculative.Interestingly,loweragewasassociatedwithhepaticmetastasesinbothstudyIIandIVandcontrastedthefindingsforpulmonarymetastases.Potentialmechanismscouldbeage-relatedchangesinlymphaticflow,declineinimmunologicalfunctionandalterationsinmuta-tionalstatus[128].Ageperseismostlikelynotatrueriskfactor.TheassociationbetweenageandpulmonarymetastasescouldsimplybeexplainedbyamoreadvancedtumourstageinelderlyatdiagnosisandtheassociationdisappearedinstudyIVaftertheadjustmentforrelevantpathologicalfeaturesoftheindexcancerincludingT-andN-stage.Nevertheless,pulmonarymetastasesdooccureveninearlytumourstagesoftheCRC[26].
InstudyIVitwasinvestigatedwhethersomeofthesediffer-encescouldbeassociatedwithfindingsatthepathologicalstag-ing,especiallyfocusingonthesignificanceofMMR.Previously,biomarkershavebeenassociatedwithdistantrecurrenceatspecificsites.Suchbiomarkerscouldthereforepotentiallybeusedinabiomarkerpanelforelucidationoftheclinicalsignifi-canceofIPNasseeninlungcancerscreening[129].KRASmuta-tionhasbeenassociatedwithpulmonarybutnotliverrelapse[130]andBRAFmutanttumoursareassociatedwithhigherratesofperitonealmetastases,distantlymphnodemetastases,andlowerratesoflungmetastases[131].Furthermore,areducedriskofmetastaticdiseasehasbeenreportedinpatientswithCRCanddeficientMMR[131-134].TheinvestigationofMMRasaprognos-ticbiomarkerinthecurrentsettingandinrelationtoorgan-specificmetastaseswaschosenforobviousreasons;MMRstatushasbeenanalysedroutinelysince2010andisinadditiontoareducedoverallriskofmetastasesknowntobeassociatedwithgender,age,locationoftheindextumour,lymphnodemetasta-sis,celltypeanddegreeofdifferentiationoftheCRC[131,132,134].However,despitethelarge-scalenationwidedataused,thereducedriskofsynchronousmetastasisindMMRtu-moursonlyappliedtopatientswithhepaticmetastases,whereasnostatisticallysignificantimpactwasfoundforpulmonarymetas-tases.Therationaleforthisdistinctpatternofmetastaticspread,associatedbyMMRstatus,isobscure.Unfortunately,basedonthepresentresultsMMRstatusaddsnovalueintheassessmentofIPNs.
CONCLUSION
Pulmonarymetastaseswereconfirmedtobethemostcommonextra-hepaticmanifestationforsynchronousmetastaticdiseaseinpatientswithCRC.TheoptimalapproachtotheinitialstagingwithregardtoSPCMisdebated.AnincreasingnumberofSPCMweredetectedwiththeimplementationofchestCTinstaging,however,asubstantialandvaryingnumberofpulmonarylesionsdetectedatchestCTcouldnotreadilybeclassifiedasbeingor

DANISH MEDICAL JOURNAL 13
malignant.InstudyIandIIIweassessedtheprevalenceofIPNandspecificradiologicaland/orclinicopathologicalfactorsassoci-atedwithmalignancyofIPNinpreviouspublishedstudiesandinalocalcohort.Inpreviouslypublishedseries,anaverageof9%ofallpatientswithCRCandstagedwithchestCThadIPN.However,thenumberofdetectedIPNsvariedgreatlybetweenthestudiesanddefinitionsofIPNdifferediftheyweregivenatall.Onein100ofallchestCTstagedpatientshadanIPNthatultimatelyprovedtobemalignant.MostpulmonarynoduleswereofbenignoriginandthefewIPNsprovingtobemalignantwerewithoutpathog-nomonicfeatures.InourlocalcohortthenumberofIPNsregis-teredintheprimarychestCTreviewwascomparabletotheaveragenumberformpreviousstudies.
However,thenumberofIPNswassignificantlyreducedwhenscanswerere-assessedbyadedicatedthoracicradiologist.Unfor-tunately,neitherinstudyIIIwefoundanyradiologicalfeaturesofIPNspathognomonicformalignancyandtimetoresectionoftheprimarytumourwasprolongedinpatientswithIPN.
SPCMweredetectedin7.5%ofallnewlydiagnosedCRCpa-tientsinstudyII,andtheirpresencesignificantlyimpairedsurviv-al.Resectionofthemetastasesandindextumourinadditiontochemotherapywasassociatedwithaprolongedoverallsurvival,thoughonlyfewpatientsweresubjectedtoallthreetreatmentmeasures.BasedontheprevalenceofSPCM,theirimpactonsurvivalandpotentialbenefitofearlydiagnosisandtreatmentwerecommendthatIPNshouldbefollowed-upinasystematicandpre-definedway.ThetotalnumberofIPNscanbereducedbyareviewofdedicatedthoracicradiologistsandtheremainingIPNsaftersuchareviewshouldbeallocatedtofurtherinvestigationsassuggested.Ofoutermostimportanceisthatthisfurtherfollow-updoesnotdelaytreatmentoftheindexcancer.Inthefuture,biomarkersforpulmonarymetastasescouldpotentiallybeim-plementedinthemanagementstrategiesofIPN.InstudyIVMMRdid,however,notprovetobeofanyvalueinevaluationoftheriskofSPCM.
PERSPECTIVESFORFUTURERESEARCH
Evenasthisthesisisbeingwrittenthetechniquesusedforstag-ing,theirapplicabilityandtheunderstandingofthemetastaticprocessarerapidlyevolving.Ithasbeenarguedthatcancertreatment,indevelopedcountries,isbecomingacultureofex-cesscharacterizedbyover-diagnosing,overtreatmentandover-promising[135].Asaresult,globaleconomicexpenditureoncancercareisincreasing[135].Theexpensesfortheimplementa-tionofnewandevolvingdiagnosticimagingmodalitiesarenoexception[136].Futureresearchandintroductionofnew(andpotentiallymoreexpensive)stagingmodalitiesneedtotakethecost-effectivenessaspectintoaccount.Inthiscontextfutureprospectivestudiesshouldseektoclarifythe“oncologicalbene-fit”fromfollowingIPNsandtheconcurrentconsequencesinclud-ingincreasedradiationandpatientanxiety.Somescepticsarguethatthepotentialharmfuleffectsoffollow-upoutweighthepotentialbenefit,whichiswhypatientswithIPNshouldnotbesubjectedtoanyfurtherdiagnosticwork-up;mostofthemprovetobebenignanywayandtheeffectivenessofpulmonarymetas-tasectomyisstilltoberesolved.However,asstatedbyMacMa-honetal.,[43]itisimpossibletoignorethemedicolegalconsid-erationswhendiscussingmanagementofIPNandthenodulescannotsimplybeignoredbecausesomeofthemdorepresentmetastaticdisease.Akeycomponentinfutureresearchshouldbe
thatreproducibleandobjectivepatientandnodulecharacteristicsdictatethefurtherwork-upandtreatment.Therebyensuringaveryselectiveuseofsurgeryalmostreservedformalignantnod-ules.FuturepredictivemodelcouldincludebiomarkerssimilartoplasmabiomarkerpanelsfordiscerningclinicalsignificanceofIPNasseeninnon-smallcelllungcancer[129].Thetranslationofbiomarkersandincreasingknowledgeondeterminantsforthemetastaticprocessintotheclinicaldecision-makingcouldberelevantforbothpatientandsocietycostbenefit.
SUMMARYPatientswithnewlydiagnosedcolorectalcancer(CRC)aresubjectedtoapreoperativethoraco-abdominalCTscantodeter-minethecancerstage.Thisstagingisofrelevancewithregardtotreatmentandprognosis.About20%ofthepatientshavedistantmetastaticspreadatthetimeofdiagnosis,i.e.synchronousmeta-stases.Mostcommonarehepaticmetastasesfollowedbypulmo-naryinvolvement. Theoptimalstagingmodalityfordetectingsynchronouspulmonarymetastasesisdebated.Ithasbeenargued,thatsynchronouspulmonarymetastases(SPCM)arerareinCRCandthattheconsequenceofdetectingSPCMisminimal. Furthermore,thecurrentstagingpracticeiscomplicatedbyahighnumberofincidentalfindingsonthethoracicCT,so-calledindeterminatepulmonarynodules(IPN).IPNcanpotentiallyre-presentSPCM. Thepurposeofthisthesiswastoestimatetheprevalence,characteristicsandclinicalsignificanceofIPNandSPCMdetectedattheprimarystaginginCRC. StudyIwasasystematicreviewofpublishedstudiesonIPNinCRCfocusingontheprevalenceandradiologicalcharacteristicsofIPNprovingtobemalignant.ThisknowledgewouldbeofvalueinmanagementstrategiesforIPN.Onaverage9%ofallpatientsstagedwithathoracicCThadIPN,however,theprevalenceva-riedsignificantlybetweenpatientsseries.Thiswasmainlyattri-butedtovarying/lackingdefinitionsonIPNandvariableradiologi-calexpertiseintheassessmentofthescans.DataweretooinconsistentlyreportedinthecaseseriesforarobuststatementtobemadeonpotentialradiologicalcharacteristicssuggestiveofmalignancyinIPN.LymphnodemetastasiswasthemostcommonclinicopathologicalfindingassociatedwithmalignancyofIPN.Inconclusion,1patientofevery100scannedpatientshadanIPNprovingtoaSPCMatfollow-up,butwefoundnoevidencethatIPNshouldresultinintensifieddiagnosticwork-upbesidesrouti-nefollow-upforCRC. StudyIIwasananalysisoftheprevalenceofandriskfactorsforSPCMinaDanishnationwidecohortofpatientswithnewlydiagnosedCRCfrom2001to2011.SPCMweredetectedin7.5%ofthepatientsandin37%ofthesecasesthemetastaticspreadwasconfinedtothelungs.TheprevalenceofSPCMincreasedwiththeimplementationofthoracicCTinCRCstaging.SPCMimpairedsurvivalsignificantlyandwasassociatedwithincreasingageandrectalcancer.Resectionoftheprimarytumour,resectionoftheSPCMandtreatmentwithchemotherapywereassociatedwithimprovedsurvival.Unfortunately,however,onlyveryfewpatientsweresubjectedtoallthreetreatmentmeasures,andtheimprovedprognosiscouldsimplybetheresultofaselectionbias. Theinter-observervariationinclassificationoffindingsatthoracicCTscanswasinvestigatedinstudyIIIandwasbasedonstagingCTscansfromalocalcohortofpatientswithnewlydiag-

DANISH MEDICAL JOURNAL 14
nosedCRC.Basedonanexperiencedthoracicradiologist’sasses-smentofthescans,wesearchedforradiologicalcharacteristicsofIPNthatcouldpredictmalignancyofthenodule.TherewasasignificantdifferenceinthenumberofIPNsdetectedbetweentheprimaryandthethoracicradiologist’sassessment.ThethoracicradiologistclassifiedfewernodulesasIPNandevenreportedwithhigherspecificityandsensitivityforSPCM.Morethan20%ofIPNs(asclassifiedbythethoracicradiologist)provedtobeSPCM.Unfortunately,noradiologicalcharacteristicscouldbeassociatedwithamalignantoutcome.IncontinuationofthesefindingswesuggestedasecondaryreviewofscanswithIPNbeagroupofdedicatedthoracicradiologists.Thisapproachmightreducetheneedforadditionalwork-upforIPNandcallsforclarificationinfutureprospectivestudies.IdentificationofpatientsinparticularriskofSPCMcouldbeofvalueintheassessmentofpulmonarynodules.SeveralbiomarkershavebeenproposedfordifferentialmetastaticpatternsinCRC. InstudyIVweinvestigatedthesignificanceofmismatchrepairstatus(MMR)forthelocationofmetastaticspreadinanationwideDanishcohortofpatientswithnewlydiagnosedCRCbetween2010and2012.DeficientMMRwasassociatedwithareducedriskofsynchronousmetastaticdisease,however,theriskreductiononlyappliedtohepaticmetastases.MMRhadnoim-pactonSPCMandisthereforecurrentlyofnouseintheasses-smentofIPN.
REFERENCES1 Nordholm-CarstensenA,Wille-JorgensenPA,JorgensenLN,HarlingH.
Indeterminatepulmonarynodulesatcolorectalcancerstaging:asys-tematicreviewofpredictiveparametersformalignancy.AnnSurgOncol2013;20:4022-4030.
2 Nordholm-CarstensenA,KrarupPM,JorgensenLN,Wille-JorgensenPA,HarlingH,onbehalfoftheDanishColorectalCancerGroup.Occurrenceandsurvivalofsynchronouspulmonarymetastasesincolorectalcancer:anationwidecohortstudy.EurJCancer2014;50:447-456.
3 Nordholm-CarstensenA,JorgensenLN,Wille-JorgensenPA,HansenH,HarlingH.Indeterminatepulmonarynodulesincolorectal-cancer:doradiologistsagree?AnnSurgOncol2015;22:543-549.
4 Nordholm-CarstensenA,KrarupPM,MortonD,HarlingH,onbehalfoftheDanishColorectalCancerGroup.Mismatchrepairstatusandsyn-chronousmetastasesincolorectalcancer:Anationwidecohortstudy.IntJCancerDOI:10.1002/ijc.29585
5 AndersonWA.Stageclassificationandendresultsreportingforcarci-nomaofthecolonandrectum.Cancer1974;34:suppl:909-911.
6 GreeneFL,SobinLH.Thestagingofcancer:aretrospectiveandprospec-tiveappraisal.CACancerJClin2008;58:180-190.
7 RankinFW,BrodersAC.Factorsinfluencingprognosisincarcinomaoftherectum.SurgGynecolObstet1928;46:660-667.
8 DukesCE.Theclassificationofcanceroftherectum.JPatholBacterial1932;35:323-332.
9 DenoixPF.Nomenclatureclassificationdescancers.BullInstNatHyg1952;7:743-748.
10 InternationalUnionAgainstCancer.TNMHistory,EvolutionandMile-stones.Available:http://www.uicc.org/sites/main/files/private/History_Evolution_Milestones_0.pdf.[accessedOctober14,2014]
11 PuppaG,SonzogniA,ColombariR,PelosiG.TNMstagingsystemofcol-orectalcarcinoma:acriticalappraisalofchallengingissues.ArchPatholLabMed2010;134:837-852.
12 ComptonCC,GreeneFL.Thestagingofcolorectalcancer:2004andbe-yond.CACancerJClin2004;54:295-308.
13 GospodarowiczMK,MillerD,GroomePA,GreeneFL,LoganPA,SobinLH.TheprocessforcontinuousimprovementoftheTNMclassification.Cancer2004;100:1-5.
14 HanahanD,WeinbergRA.Thehallmarksofcancer.Cell2000;100:57-70.
15 ManfrediS,LepageC,HatemC,CoatmeurO,FaivreJ,BouvierAM.Epi-demiologyandmanagementoflivermetastasesfromcolorectalcancer.AnnSurg2006;244:254-259.
16 HowladerN,NooneAM,KrapchoM,etal.(eds).SEERCancerStatisticsReview,1975-2010,NationalCancerInstitute.Bethesda,MD.Available:http://seer.cancer.gov/csr/1975_2010/[accessedDecember20,2014]
17 GaoP,SongYX,WangZN,etal.Isthepredictionofprognosisnotim-provedbytheseventheditionoftheTNMclassificationforcolorectalcancer?Analysisofthesurveillance,epidemiology,andendresults(SEER)database.BMCcancer.2013;13:123.
18 EdgeSB,ComptonCC.TheAmericanJointCommitteeonCancer:the7theditionoftheAJCCcancerstagingmanualandthefutureofTNM.AnnSurgOncol2010;17:1471-1474.
19 VanCutsemE,CervantesA,NordlingerB,ArnoldD,ESMOGuidelinesWorkingGroup.Metastaticcolorectalcancer:ESMOClinicalPracticeGuidelinesfordiagnosis,treatmentandfollow-up.AnnOncol2014;25Suppl3:iii1-9.
20 MitryE,GuiuB,CosconeaS,JoosteV,FaivreJ,BouvierAM.Epidemiolo-gy,managementandprognosisofcolorectalcancerwithlungmetasta-ses:a30-yearpopulation-basedstudy.Gut2010;59:1383-1388.
21 KirkeR,RajeshA,VermaR,BankartMJ.Rectalcancer:incidenceofpul-monarymetastasesonthoracicCTandcorrelationwithTstaging.JComputAssistTomogr2007;31:569-571.
22 TanKK,LopesGdeLJr.,SimR.Howuncommonareisolatedlungmetas-tasesincolorectalcancer?Areviewfromdatabaseof754patientsover4years.JGastrointestSurg2009;13:642-648.
23 McIntoshJ,SylvesterPA,VirjeeJ,CallawayM,ThomasMG.Pulmonarystagingincolorectalcancer--iscomputerisedtomographytheanswer?AnnRCollSurgEngl2005;87:331-333.
24 GrossmannI,AvenariusJK,MastboomWJ,KlaaseJM.Preoperativestag-ingwithchestCTinpatientswithcolorectalcarcinoma:notasaroutineprocedure.AnnSurgOncol2010;17:2045-2050.
25 HwangMJ,JungSH,KimJH,ShimMC.Diagnosticusefulnessofroutinelyperformedpreoperativechestcomputedtomographyforcolorectalcancer.JKoreanSocColoproctol2010;26:211-216.
26 KayserK,ZinkS,AndreS,etal.Primarycolorectalcarcinomasandtheirintrapulmonarymetastases:clinical,glyco-,immuno-andlectinhisto-chemical,nuclearandsyntacticstructureanalysiswithemphasisoncor-relationwithperiodofoccurrenceofmetastasesandsurvival.APMIS2002;110:435-446.
27 ComptonCC.Pathologyreportincoloncancer:whatisprognosticallyimportant?DigDis1999;17:67-79.
28 GonzalezM,PoncetA,CombescureC,RobertJ,RisHB,GervazP.Riskfactorsforsurvivalafterlungmetastasectomyincolorectalcancerpa-tients:asystematicreviewandmeta-analysis.AnnSurgOncol2013;20:572-579.
29 GonzalezM,RisHB,KruegerT,GervazP.Colorectalcancerandthoracicsurgeons:closeencountersofthethirdkind.ExpertRevAnticancerTher2012;12:495-503.
30 NationalComprehensiveCancerNetwork.NCCNClinicalPracticeGuide-linesinOncologyRectalCancer.2.2015Available:http://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf.[ac-cessedApril5,2015]
31 NationalComprehensiveCancerNetwork.NCCNClinicalPracticeGuide-linesinOncologyColonCancer.2.2015Available:http://www.nccn.org/professionals/physician_gls/pdf/colon.pdf.[ac-cessedApril5,2015]
32 DanishColorectalCancerGroup.Præoperativbilleddiagnostik.2010.Available:http://www.dccg.dk/retningslinjer/2010_praeopbill.pdf.[ac-cessedOctober14,2014]
33 AssociationofColoproctologyofGreatBritainandIreland.GuidelinesfortheManagementofColorectalCancer.3rded.2007.Available:http://acpgbi.mixd.co.uk/content/uploads/2007-CCManagement-Guidelines.pdf.[accessedOctober14,2014]
34 ParnabyC,BaileyW,BalasingamA,etal.Pulmonarystagingincolorec-talcancer:areview.ColorectalDis2011;14:660-670.
35 MaithelSK,GinsbergMS,D'AmicoF,etal.Naturalhistoryofpatientswithsubcentimeterpulmonarynodulesundergoinghepaticresectionformetastaticcolorectalcancer.JAmCollSurg2010;210:31-38.
36 AustinJH,MullerNL,FriedmanPJ,etal.GlossaryoftermsforCTofthelungs:recommendationsoftheNomenclatureCommitteeoftheFleischnerSociety.Radiology1996;200:327-331.
37 KronawitterU,KemenyNE,HeelanR,FataF,FongY.Evaluationofchestcomputedtomographyinthestagingofpatientswithpotentiallyresec-tablelivermetastasesfromcolorectalcarcinoma.Cancer.1999;86:229-235.
38 ChristoffersenMW,BulutO,JessP.Thediagnosticvalueofindetermi-natelunglesionsonstagingchestcomputedtomographiesinpatientswithcolorectalcancer.DanMedBull2010;57:A4093.
39 BrentA,TalbotR,CoyneJ,NashG.ShouldindeterminatelunglesionsreportedonstagingCTscansinfluencethemanagementofpatientswithcolorectalcancer?ColorectalDis2007;9:816-818.

DANISH MEDICAL JOURNAL 15
40 ChoYK,LeeWY,ParkCH,etal.TheroleofaroutinepreoperativechestCTinpatintswithcolorectalcancer.ColorectalDis2009;11:suppl2:44-44.
41 DeWW,MeylaertsL,DeCL,StroobantsS,VerschakelenJA.AdditionalvalueofintegratedPETCTinthedetectionandcharacterizationoflungmetastases:correlationwithCTaloneandPETalone.EurRadiol2007;17:467-473.
42 ChoiDJ,KwakJM,KimJ,WooSU,KimSH.Preoperativechestcomputer-izedtomographyinpatientswithlocallyadvancedmidorlowerrectalcancer:itsroleinstagingandimpactontreatmentstrategy.JSurgOn-col2010;102:588-592.
43 MacMahonH,AustinJH,GamsuG,etal.GuidelinesformanagementofsmallpulmonarynodulesdetectedonCTscans:astatementfromtheFleischnerSociety.Radiology2005;237:395-400.
44 MoherD,LiberatiA,TetzlaffJ,AltmanDG,PRISMAGroup.Preferredre-portingitemsforsystematicreviewsandmeta-analyses:thePRISMAstatement.PLoSMed2009;6:e1000097.
45 HigginsJ,GreenS.CochraneHandbookforSystematicReviewsofInter-ventions.2011;Available:http://www.cochrane-handbook.org.[acces-sedOctober14,2014]
46 PhillipsB,BallC,SackettD,etal.OxfordCentreforEvidence-basedMedicine-LevelsofEvidence.2009.Available:http://www.cebm.net/oxford-centre-evidence-based-medicinelev-elsevidence-march-2009/.[accessedOctober14,2014]
47 ScottishIntercollegiateGuidelinesNetwork.Sign50:aguidelinedevel-oper’shandbook.2011.Available:http://www.sign.ac.uk/pdf/sign50.pdf.[accessedJune22,2012]
48 PhillipsN,BhanC,MurphyJ,BeharN,AllenC,RowePH.T1178inde-terminatelunglesionsinpatientswithcolorectalcancer:dotheypro-gress?(Abstract)Gastroenterology.2009;136:A-517.
49 QuynAJ,MatthewsA,DanielT,AminAI,YalamarthiS.Theclinicalsignif-icanceofradiologicallydetectedindeterminatepulmonarynodulesincolorectalcancer.ColorectalDis2012;14:828-831.
50 VarolY,VarolU,KaracaB,KarabulutB,SezginC,UsluR.TheFrequencyandSignificanceofRadiologicallyDetectedIndeterminatePulmonaryNodulesinPatientswithColorectalCancer.MedPrincPract2012:1-5.
51 PomerriF,PucciarelliS,MarettoI,etal.Significanceofpulmonarynod-ulesinpatientswithcolorectalcancer.EurRadiol2012;22:1680-1686.
52 BelleraCA,MacGroganG,DebledM,deLaraCT,BrousteV,Mathoulin-PelissierS.Variableswithtime-varyingeffectsandtheCoxmodel:somestatisticalconceptsillustratedwithaprognosticfactorstudyinbreastcancer.BMCMedResMethodol2010;10:20.
53 LandisJR,KochGG.Themeasurementofobserveragreementforcate-goricaldata.Biometrics1977;33:159-174.
54 NordicimmunohistochemicalQualityControl,(NordiQC).NordiQCas-sessmentscheme2014.2014.Available:http://www.nordiqc.org/modules.htm.[accessedOctober23,2014]
55 HewishM,LordCJ,MartinSA,CunninghamD,AshworthA.Mismatchrepairdeficientcolorectalcancerintheeraofpersonalizedtreatment.NatRevClinOncol2010;7:197-208.
56 LindorNM,BurgartLJ,LeontovichO,etal.Immunohistochemistryver-susmicrosatelliteinstabilitytestinginphenotypingcolorectaltumors.JClinOncol2002;20:1043-1048.
57 HarlingH,NickelsenT.[TheDanishColorectalCancerDatabase].UgeskrLaeger2005;167:4187-4189.
58 DanishColorectalCancerGroup.Nationalårsrapport2013.Available:http://www.dccg.dk/03_Publikation/2013.pdf.[accessedOctober16,2014]
59 BoothCM,TannockIF.Randomisedcontrolledtrialsandpopulation-basedobservationalresearch:partnersintheevolutionofmedicalevi-dence.BrJCancer2014;110:551-555.
60 NickelsenTN,HarlingH,KronborgO,BulowS,JorgensenT.[Thecom-pletenessandqualityoftheDanishColorectalCancerclinicaldatabaseoncolorectalcancer].UgeskrLaeger2004;166:3092-3095.
61 UseofMedicalDatabasesinClinicalEpidemiology.In:SørensenHT,ChristensenT,SchlosserHK,(eds.)LP,eds.2.ed:SUN-TRYK,AarhusUni-versitet;2009.
62 MekenkampLJ,KoopmanM,TeerenstraS,etal.Clinicopathologicalfea-turesandoutcomeinadvancedcolorectalcancerpatientswithsyn-chronousvsmetachronousmetastases.BrJCancer2010;103:159-164.
63 MillerG,BiernackiP,KemenyNE,etal.Outcomesafterresectionofsynchronousormetachronoushepaticandpulmonarycolorectalmetas-tases.JAmCollSurg2007;205:231238.
64 TsoulfasG,PramateftakisMG,KanellosI.Surgicaltreatmentofhepaticmetastasesfromcolorectalcancer.WorldJGastrointestOncol2011;1-9.
65 NozawaH,SunamiE,NakajimaJ,NagawaH,KitayamaJ.Synchronousandmetachronouslungmetastasesinpatientswithcolorectalcancer:A20-yearmonocentricexperience.ExpTherMed2012;3:449-456.
66 PoultsidesGA,ServaisEL,SaltzLB,etal.OutcomeofprimarytumorinpatientswithsynchronousstageIVcolorectalcancerreceivingcombina-
tionchemotherapywithoutsurgeryasinitialtreatment.JClinOncol2009;27:3379-3384.
67 metachronous.(n.d.)McGraw-HillConciseDictionaryofModernMedi-cine.2002.Available:http://medical-dictionary.thefreedictionary.com/metachronous[accessedMay1,2015]
68 LiuL,deVriesE,LouwmanM,etal.PrevalenceofmultiplemalignanciesintheNetherlandsin2007.IntJCancer2011;128:1659-1667.
69 FerlayJ,SoerjomataramI,ErvikM,etal.GLOBOCAN2012v1.0,CancerIncidenceandMortalityWorldwide:IARCCancerBaseNo.Lyon,France:InternationalAgencyforResearchonCancer;2013.Availablefrom:http://globocan.iarc.fr.[accessedMarch15,2015]
70 EngholmG,FerlayJ,ChristensenN,etal.NORDCAN:CancerIncidence,Mortality,PrevalenceandSurvivalintheNordicCountries.2013;Versi-on6.0.Available:http://www.ancr.nu.[accessedJanuary8,2013]
71 ChristoforiG.Newsignalsfromtheinvasivefront.Nature2006;441:444-450.
72 SteinU,SchlagPM.Clinical,biological,andmolecularaspectsofmetas-tasisincolorectalcancer.Recentresultsincancerresearch.RecentRe-sultsCancerRes2007;176:61-80.
73 FearonER,VogelsteinB.Ageneticmodelforcolorectaltumorigenesis.Cell1990;61:759-767.
74 VogelsteinB,FearonER,HamiltonSR,etal.Geneticalterationsduringcolorectal-tumordevelopment.NEnglJMed1988;319:525-532.
75 JassJR.Classificationofcolorectalcancerbasedoncorrelationofclini-cal,morphologicalandmolecularfeatures.Histopathology2007;50:113-130.
76 ArendsMJ.Pathwaysofcolorectalcarcinogenesis.ApplImmunohi-stochemMolMorphol2013;21:97-102.
77 GoelA,ArnoldCN,NiedzwieckiD,etal.Characterizationofsporadicco-loncancerbypatternsofgenomicinstability.CancerRes2003;63:1608-1614.
78 MoranA,OrtegaP,deJuanC,etal.Differentialcolorectalcarcinogene-sis:Molecularbasisandclinicalrelevance.WorldJGastrointestOncol2010;2:151-158.
79 SamowitzWS,SweeneyC,HerrickJ,etal.PoorsurvivalassociatedwiththeBRAFV600Emutationinmicrosatellite-stablecoloncancers.CancerRes2005;65:6063-6069.
80 PagetS.TheDistributionofsecondarygrowthsincancerofthebreast.Lancet1889;1:571-573.
81 RadinskyR,EllisLM.Moleculardeterminantsinthebiologyofliverme-tastasis.SurgOncolClinNAm1996;5:215-229.
82 BiermanHR,ByronRL,Jr.,KelleyKH,GradyA.Studiesonthebloodsup-plyoftumorsinman.III.Vascularpatternsoftheliverbyhepaticarteri-ographyinvivo.JNatlCancerInst1951;12:107-131.
83 SadahiroS,SuzukiT,TanakaA,OkadaK,KamataH.HematogenousmetastaticpatternsofcurativelyresectedcoloncancerweredifferentfromthoseofstageIVandautopsycases.JpnJClinOncol2013;43:444-447.
84 WeissL,GrundmannE,TorhorstJ,etal.Haematogenousmetastaticpatternsincoloniccarcinoma:ananalysisof1541necropsies.JPathol1986;150:195-203.
85 BlalockA.Recentadvancesinsurgery.NewEnglJMed1944;231:26186 TreasureT,MilosevicM,FiorentinoF,PfannschmidtJ.Historyandpre-
sentstatusofpulmonarymetastasectomyincolorectalcancer.WorldJGastroenterol2014;20:1451714526.
87 JensenAR.DCCG’snationaleretningslinierfordiagnostikogbehandlingafkolorektalcancer-Lungemetastaser.2012.Available:http://www.dccg.dk/retningslinjer/2012_lungemets.pdf.[accessedMarch20,2015]
88 InternulloE,CassiviSD,VanRaemdonckD,FriedelG,TreasureT.Pul-monarymetastasectomy:asurveyofcurrentpracticeamongstmem-bersoftheEuropeanSocietyofThoracicSurgeons.JThoracOncol2008;3:1257-1266.
89 ThomfordNR,WoolnerLB,ClagettOT.SurgicalTreatmentofMetastaticTumorsinLungs.JThoracCardiovSur1965;49:357-363.
90 PfannschmidtJ,DienemannH,HoffmannH.Surgicalresectionofpul-monarymetastasesfromcolorectalcancer:asystematicreviewofpub-lishedseries.AnnThoracSurg2007;84:324-338.
91 TreasureT,FallowfieldL,LeesB,FarewellV.Pulmonarymetastasecto-myincolorectalcancer:thePulMiCCtrial.Thorax2012;67:185-187.
92 GalandiukS,WieandHS,MoertelCG,etal.Patternsofrecurrenceaftercurativeresectionofcarcinomaofthecolonandrectum.SurgGynecolObstet1992;174:27-32.
93 vandeVeldeCJ,BoelensPG,BorrasJM,etal.EURECCAcolorectal:mul-tidisciplinarymanagement:Europeanconsensusconferencecolon&rectum.EurJCancer2014;50:1e1-1e34.
94 DavisSD.CTevaluationforpulmonarymetastasesinpatientswithex-trathoracicmalignancy.Radiology1991;180:1-12.
95 IkeH,ShimadaH,OhkiS,TogoS,YamaguchiS,IchikawaY.Resultsofaggressiveresectionoflungmetastasesfromcolorectalcarcinomade-tectedbyintensivefollow-up.DisColonRectum2002;45:468-473.

DANISH MEDICAL JOURNAL 16
96 SchoemakerD,BlackR,GilesL,ToouliJ.Yearlycolonoscopy,liverCT,andchestradiographydonotinfluence5-yearsurvivalofcolorectalcancerpatients.Gastroenterology1998;114:7-14.
97 KobayashiK,KawamuraM,IshiharaT.Surgicaltreatmentforbothpul-monaryandhepaticmetastasesfromcolorectalcancer.JThoracCar-diovascSurg1999;118:1090-1096.
98 KimJY,KimNK,SohnSK,etal.PrognosticvalueofpostoperativeCEAclearanceinrectalcancerpatientswithhighpreoperativeCEAlevels.AnnSurgOncol2009;16:2771-2778.
99 KimHY,LeeSJ,LeeG,etal.ShouldPreoperativeChestCTBeRecom-mendedtoAllColonCancerPatients?AnnSurg2014;259:323-8
100 HoganJ,O'RourkeC,DuffG,etal.PreoperativestagingCTthoraxinpa-tientswithcolorectalcancer:itsclinicalimportance.DisColonRectum2014;57:1260-1266.
101 Wille-JorgensenPA.DCCG’snationaleretningslinierfordiagnostikogbehandlingafkolorektalcancer-Postoperativkontrol.2012.Available:http://www.dccg.dk/retningslinjer/2012_kontrol.pdf.[accessedMarch30,2015]
102 SnyderBJ,PugatchRD.Imagingcharacteristicsofmetastaticdiseasetothechest.ChestSurgClinNAm1998;8:29-48.
103 GooJM.PulmonaryNeoplasmsoftheLung.In:SabaL,SuriJS,eds.Mul-ti-DetectorCTImaging:Principles,Head,Neck,andVascularSystems.CRCPress;2013:503-528.
104 GrossBH,GlazerGM,BooksteinFL.Multiplepulmonarynodulesdetect-edbycomputedtomography:diagnosticimplications.JComputAssistTomogr1985;9:880-885.
105 StrausMJ.Thegrowthcharacteristicsoflungcanceranditsapplicationtotreatmentdesign.SeminOncol1974;1:167-174.
106 SeoJB,ImJG,GooJM,ChungMJ,KimMY.Atypicalpulmonarymetasta-ses:spectrumofradiologicfindings.Radiographics2001;21:403-417.
107 HenschkeCI,McCauleyDI,YankelevitzDF,etal.EarlyLungCancerAc-tionProject:overalldesignandfindingsfrombaselinescreening.Lancet1999;354:99-105.
108 SwensenSJ,JettJR,HartmanTE,etal.CTscreeningforlungcancer:five-yearprospectiveexperience.Radiology2005;235:259-265.
109 JessP,SeiersenM,OvesenH,etal.HasPET/CTaroleinthecharacteri-zationofindeterminatelunglesionsonstagingCTincolorectalcancer?Aprospectivestudy.EurJSurgOncol2014;40:719-722.
110 KimCH,HuhJW,KimHR,KimYJ.IndeterminatePulmonaryNodulesinColorectalCancer:Follow-upGuidelinesBasedonaRiskPredictiveModel.AnnSurg2014.
111 GomezD,KamaliD,DunnWK,BeckinghamIJ,BrooksA,CameronIC.Outcomesinpatientswithindeterminatepulmonarynodulesundergo-ingresectionforcolorectallivermetastases.HPB2012;14:448-454.
112 GriffithsSN,ShaikhI,TamE,WegstapelH.Characterisationofindeter-minatepulmonarynodulesincolorectalcancer.IntJSurg2012;10:575-577.
113 Downs-CannerS,BaharR,ReddySK,etal.Indeterminatepulmonarynodulesrepresentlungmetastasesinasignificantportionofpatientsundergoingliverresectionformalignancy.JGastrointestSurg2012;16:2256-2259.
114 OhBY,NohGT,HongKS,ChungSS,KimKH,LeeRA.Theavailabilityofcomputedtomographyforpulmonarystagingincolorectalcancer.AnnSurgTreatRes2014;86:212216.
115 BaekSJ,KimSH,KwakJM,etal.Indeterminatepulmonarynodulesinrectalcancer:arecommendationforfollow-upguidelines.JSurgOncol2012;106:481-485.
116 ArmatoSG,3rd,RobertsRY,KocherginskyM,etal.Assessmentofradi-ologistperformanceinthedetectionoflungnodules:dependenceonthedefinitionof"truth".AcadRadiology2009;16:28-38.
117 WormannsD,LudwigK,BeyerF,HeindelW,DiederichS.Detectionofpulmonarynodulesatmultirow-detectorCT:effectivenessofdoublereadingtoimprovesensitivityatstandard-doseandlow-dosechestCT.EurRadiol2005;15:14-22.
118 GieradaDS,PilgramTK,FordM,etal.Lungcancer:interobserveragreementoninterpretationofpulmonaryfindingsatlow-doseCTscreening.Radiology2008;246:265-272.
119 JeonKN,GooJM,LeeCH,etal.Computer-AidedNoduleDetectionandVolumetrytoReduceVariabilityBetweenRadiologistsintheInterpreta-tionofLungNodulesatLow-DoseScreeningComputedTomography.InvestRadiol2012;47:457-461.
120 NaidichDP,BankierAA,MacMahonH,etal.RecommendationsforthemanagementofsubsolidpulmonarynodulesdetectedatCT:astate-mentfromtheFleischnerSociety.Radiology2013;266:304-317.
121 FurmanAM,DitYafawiJZ,SoubaniAO.Anupdateontheevaluationandmanagementofsmallpulmonarynodules.FutureOncol2013;9:855-865.
122 TheDanishColorectalCancerGroup.GuidelinesfortheManagementofColorectalCancer.2010.Available:http://dccg.dk/03_Publikation/Retningslinier2009revOKT2010.pdf.[ac-cessedMarch8,2014]
123 DinkelE,MundingerA,SchoppD,GrosserG,HauensteinKH.Diagnosticimaginginmetastaticlungdisease.Lung1990;168:Suppl:1129-1136.
124 LacasseY,WongE,GuyattGH,CookDJ.Transthoracicneedleaspirationbiopsyforthediagnosisoflocalisedpulmonarylesions:ameta-analysis.Thorax1999;54:884-893.
125 Beigelman-AubryC,HillC,GrenierPA.Managementofanincidentallydiscoveredpulmonarynodule.EurRadiol2007;17:449-466.
126 MedCalc3000.SolitaryPulmonaryNoduleMalignancyRisk(MayoClinicmodel).Available:http://reference.medscape.com/calculator/solitary-pulmonary-nodule-risk.[accessedOctober20,2014]
127 GurneyJ.SPNcalculator.2014.Available:http://www.chestx-ray.com/index.php/calculators/spncalculator.[accessedMarch15,2015]
128 KimMJ,LeeHS,KimJH,etal.DifferentmetastaticpatternaccordingtotheKRASmutationalstatusandsite-specificdiscordanceofKRASstatusinpatientswithcolorectalcancer.BMCCancer2012;12:347.
129 DalyS,RinewaltD,FhiedC,etal.Developmentandvalidationofaplas-mabiomarkerpanelfordiscerningclinicalsignificanceofindeterminatepulmonarynodules.JThoracOncol2013;8:31-36.
130 TieJ,LiptonL,DesaiJ,etal.KRASmutationisassociatedwithlungme-tastasisinpatientswithcurativelyresectedcolorectalcancer.ClinCan-cerRes2011;17:1122-1130.
131 TranB,KopetzS,TieJ,etal.ImpactofBRAFmutationandmicrosatelliteinstabilityonthepatternofmetastaticspreadandprognosisinmeta-staticcolorectalcancer.Cancer2011;117:4623-4632.
132 HutchinsG,SouthwardK,HandleyK,etal.Valueofmismatchrepair,KRAS,andBRAFmutationsinpredictingrecurrenceandbenefitsfromchemotherapyincolorectalcancer.JClinOncol2011;29:1261-1270.
133 MullerCI,SchulmannK,Reinacher-SchickA,etal.Predictiveandprog-nosticvalueofmicrosatelliteinstabilityinpatientswithadvancedcolo-rectalcancertreatedwithafluoropyrimidineandoxaliplatincontainingfirst-linechemotherapy.AreportoftheAIOColorectalStudyGroup.IntJColorectalDis2008;23:1033-1039.
134 GryfeR,KimH,HsiehET,etal.Tumormicrosatelliteinstabilityandclini-caloutcomeinyoungpatientswithcolorectalcancer.NEnglJMed2000;342:69-77.
135 SullivanR,PeppercornJ,SikoraK,etal.Deliveringaffordablecancercareinhigh-incomecountries.LancetOncol2011;12:933-980.
136 DinanMA,CurtisLH,HammillBG,etal.ChangesintheuseandcostsofdiagnosticimagingamongMedicarebeneficiarieswithcancer,1999-2006.JAMA2010;303:1625-1631.