Embed Size (px)
Citation preview

Joumal of Advanced Nurstng, 1993,18,1632-1639
Putting theory into practice: problems andprospects*
fiesook Suzie Kim PhD RNProfessor of Nursing, L White Hall 234, College of Nurstng, The Umversity of Rhode bland,Kingston, Rhode Island 02881-0814, USA
Accepted for publicahon 9 February 1993
KIM H S (1993) Joumal of Advanced Nursmg 18,1632-1639Putting theory into practice: problems and prospectsThe apparent gap between theory and practice in nursing seems to be wideningas it IS becommg mcreasmgly difficult for nurses to manage multiple theones andconflictmg knowledge claims for their use m practice Scientific pluralism innursmg provides, on the one hand, a nch array of knowledge about humanphenomena and ways of deaimg with nursmg problems, while on the other a setof theoretical choices available for knowledge-use m practice This paper presentsfour ideal-type modes of theory application as viable forms for nurses m practiceto deal with theoretical pluralism
INTRODUCTIONTbe progress m nursmg saence dunng tbe past decade isstaggenng as we compare the bnds and amount of saen-tific knowledge that were available to nursmg practitionersfor tbeir applicahon mto prachce durmg the 1960s and1970s with what are currently available As a saenhficdisaplme, nursing bas integrated tbe major saenhficmetbods of knowledge generation as tbe prime source forcumulatmg and revismg its knowledge base
At first glance, such development seems to giveassurance and confidence that nursing prachce is (or hasbecome) increasmgly grounded m saentific base and alsothat there is a positive linear relationship between theoreti-cal development and improvement m nursmg practice(Ingram 1991) However, many autbors (Craig 1980,Miller 1985 and Qarke 1986) bave pomted to the apparenttbeory/prachce gap, which is even referred to as a 'chasm'by Lewis (1988), refemng to tbe despondent nature of thegap m which theones and tbe results of saentific studies areseldom translated and integrated into nursmg prachceWhile there seems to be consensus among scholars andprachhoners witbm nursmg and otber disaplmes (see, forexample, Katz 1976, Miller 1985, Pbillips 1989 andSchneider 1990) that sucb a gap may be attnbutable to the
'Repaed versum ofthe poper which uias presented at the fourth Natumal Conference anMcMmg and Rok-Modebng Theory and Paradigm for Professionak, 4 Odober 1992
USA
differences m philosophies, onentations and mcxius operandtheld by saenhsts and practitioners, this issue appears to behed to the process of 'puthng theory into pradice' mcntical ways
The noted soaal psychologist Kurt Lewin was attnbutedas saying tbat 'there is nothing so practical as a goodtheory' (Sandelands 1990) While tbis is a truism that isaccepted by many applied scientists and professionalpractitioners, Sandelands offers a revised epigram that'there is nothing so prachcal about theory, but it may begood to bave around'
What tbese two statements (epigrams) note is tbe ground-ing of theory m tbe arena of prachce However, as PbiUips(1989) indicated for the case of dinical psydiology that thereare many obstades prevenhng 'a true confluence of saenceand prachce m psychology', all of tbe prachce disaplmesare faced with difficulhes m tbe groundmg of tbeory in prac-hce from two direchons, one in the produchon of tbeonesand research and tbe other m the applicahon of theones andresearcb m prachce Botb are mtertwmed to produce andsustam the apparent separahon of saentists fromprachhoners found in nursing and otber practice disaplmes
FOCUS OF THE PAPER
For tbis paper the focus is on the applicahon of tbeory mtoprachce exammed from two points of concem (a) putting
1632
Putttng theory into practice
theory into prachce mvolves transformmg symbohcknowledge mto actions in the sense of 'theory being theknowledge that explains thmgs, and practice being theknowledge that gets thmgs done' (Sandeland 1990), and (b)it also mvolves bemg selechve m bnnging certain theonesas relevant for such transformation from a vast array ofcompetmg, sometimes conflicting and sometimes comple-mentary theones While appbcation and mtegration oftheory mto practice involves accessibihty of theones topractihoners, which has been the major focus of cnh-asms regardmg theory/practice gap, selection of certaintheory(ies) among mulhple theones mvolves not onlyaccessibility but also preference for whatever reasons bypractitioners
Kurt Lewm suggested a way of bndgmg the gapbetween theory and prachce m terms of the accessibility oftheones by placing the work of saence concretely withinthe realm of practice and prachcal problems (Lewm 1947,1948) Phillips (1989) also suggests that bnngmg prac-htioners and researchers closer together m identifyingproblems and working m knowledge generation may behelpful m reducmg the inaccessibility of theones to prac-tihoners However, it has been found that these are notsimple solutions for nursmg (Lewis 1988)
Furthermore, theoretical pluralism presents a complexpicture for practice disaplmes m which complexities as-soaated with multiple and nval knowledge claims cannotjust be thought of as a defirung feature of saence butmust be addressed m terms of puttmg such claims mto thepractice framework For nursmg, hence, the reality of theor-ehcal pluralism means transmitting multiple knowledgeclaims to the arena of practice Not only would there benval explanahons regardmg human phenomena but alsocontradictory or competmg prescnptions for solvingnursing problems What this means is that 'choices' at theprachce level are required m applymg theory mto prachce
This two-pronged problem assoaated with puttmgtheory mto prachce, le the problem of translahon andchoice, IS considered as we discuss the process mvolvedm puttmg theory mto prachce and the modes of theoryapphcahon
THE PROCESS: THEORY INTO PRACTICE
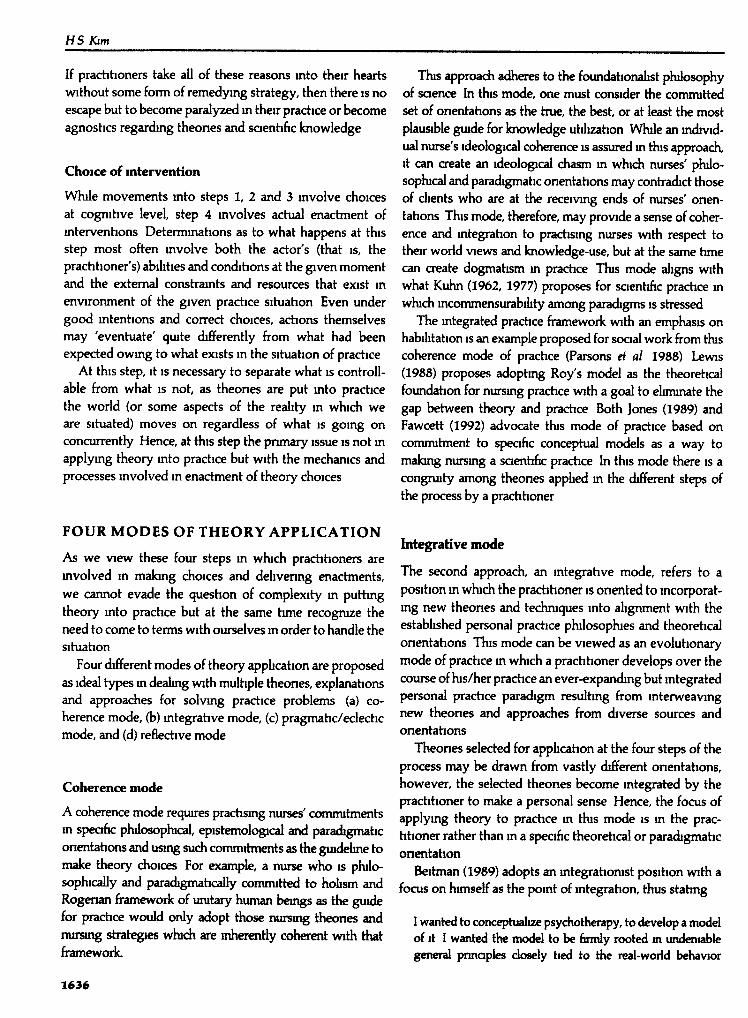
Putting theory mto practice mvolves a process that isembedded m the nature of practical work of nursmg Firstof all, this IS a matter that pertains to individuals m prachceSecond, it is a matter that pertams to a speafic situation ofprachce, mvolvmg a speafic client m a given nursmg caresituahon At an mstance of practice a practihoner confrontsthe situation of pradtice that is composed of a speaftc client
Preictice situation multiple phenomena
Step 1Knowied(]P -publ,c aonan
Practitioner's perception of situation
Step 2
Step 3
Practitioner's framing of situation
^ — • — "
/"^ Knowledge in ^ , ^V public domain /^
— • — K.,^.^.,^.
— \' ' ' '"-''---.^^^Knowledge i n - ^
f"^ pnvate domain^
r
Choice of intervention theories and strategies
Step 4Knowledge in •public domain ^' \^Krow'ea i ,e
•Vi" '*^ 3- \.a>e oor - j
T3- \.a>e oor-ji",
TEnactment of nursing interventions
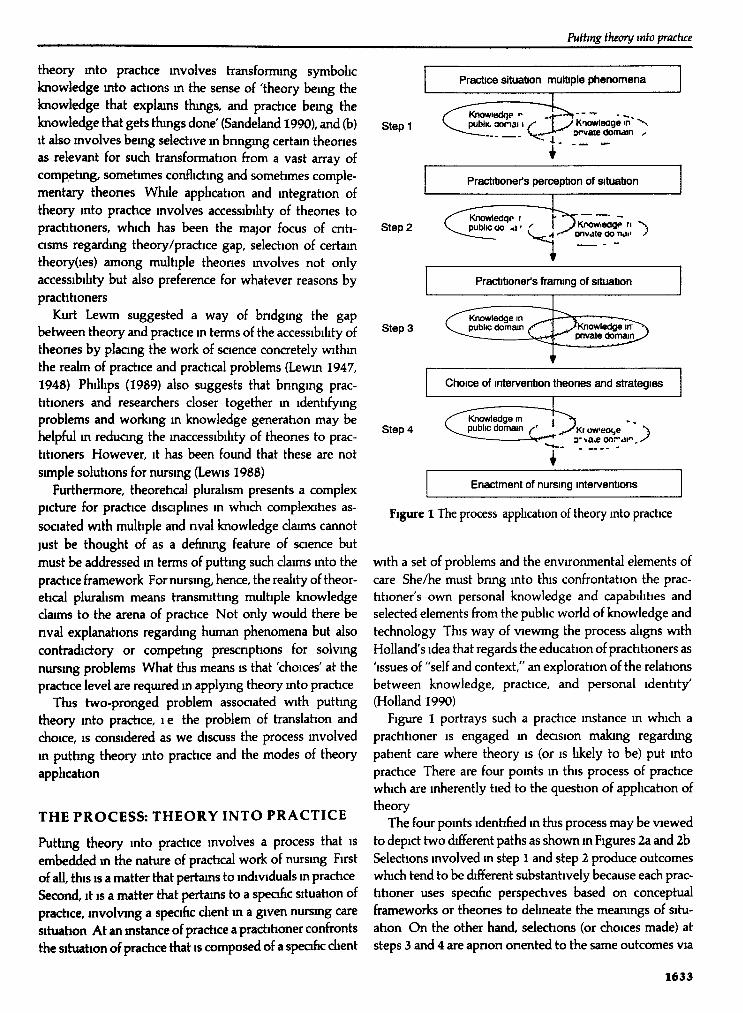
Figure 1 The process application of theory into practice
v«th a set of problems and the environmental elements ofcare She/he must bnng into this confrontahon the prac-titioner's ovwi personal knowledge and capabilihes andselected elements from the public world of knowledge andtechnology This way of viewing the process aligns withHolland's idea that regards the education of practihoners as'issues of "self and context," an explorahon of the relationsbetween knowledge, practice, and personal identity'(Holland 1990)
Figure 1 portrays such a practice instance m which apractitioner is engaged m decision making regardingpatient care where theory is (or is likely to be) put intopractice There are four points in this process of practicewhich are inherently tied to the question of appbcahon oftheory
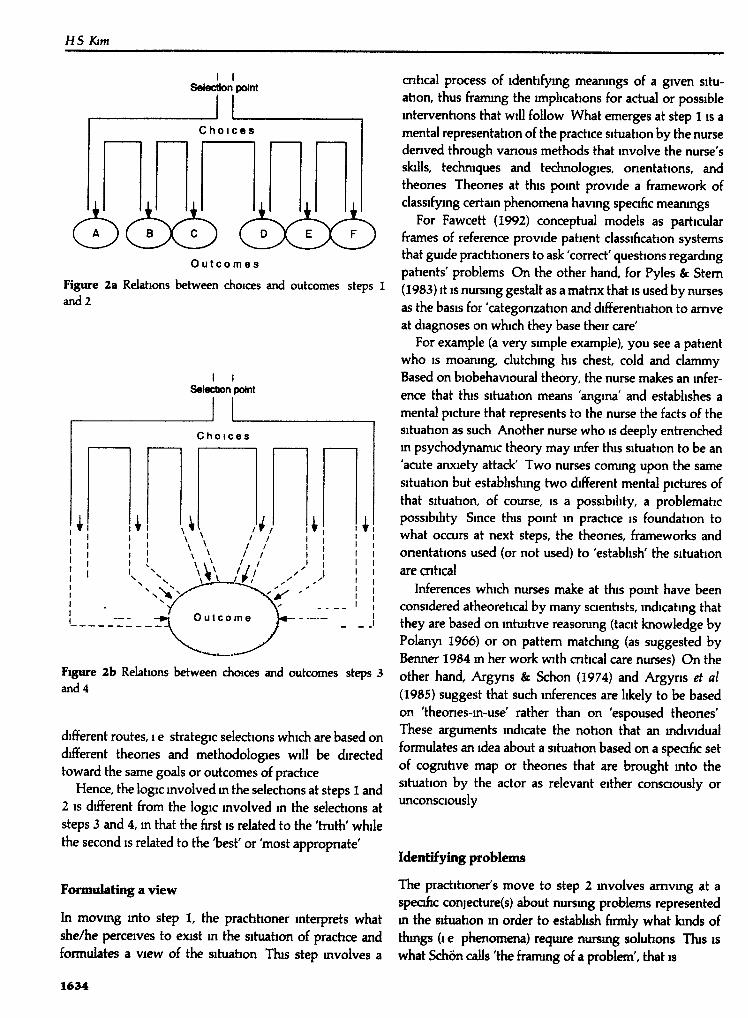
The four pomts ldenhfied in this process may be viewedto depict two different paths as shown m Figures 2a and 2bSelections mvolved m step I and step 2 produce outcomeswhich tend to be different substantively because each prac-titioner uses speafic perspechves based on conceptualframeworks or theones to delmeate the meanings of situ-ation On the other hand, selections (or choices made) atsteps 3 and 4 are apnon onented to the same outcomes via
1633
HSKim
Selection point
C h o i c e s
O u t c o m e s
Figure 2a Relahons between choices and outcomes steps 1and 2
I ISelection point
Figure 2b Relahons between choices and outcomes steps 3and 4
different routes, i e strategic selechons which are based ondifferent theones and methodologies will be dirededtoward tbe same goals or outcomes of prachce
Hence, the logic involved m tbe selections at steps 1 and2 IS different from the logic mvolved m the seledions atsteps 3 and 4, m that the first is related to tbe 'hiitb' whilethe second is related to the 'best' or 'most appropnate'
Formalating a view
In movmg mto step 1, tbe prachhoner mteiprets wbatshe/he perceives to exist m the situahon of prachce andformulates a view of tbe situation Tbis step mvolves a
cnhcal process of identifying meanings of a given situ-ahon, thus framing tbe imphcahons for actual or possiblemterventions tbat will follow What emerges at step 1 is amental representahon of tbe practice situation by tbe nursedenved through vanous methods that involve the nurse'sskills, tecbmques and technologies, onentahons, andtbeones Tbeones at this pomt provide a frameworic ofdassifying certain phenomena havmg speafic mearungs
For Fawcett (1992) conceptual models as particularframes of reference provide patient classification systemstbat guide practihoners to ask 'correct' queshons regardingpahents' problems On the other hand, for Pyles & Stem(1983) it IS nursing gestalt as a matnx tbat is used by nursesas the basis for 'categonzahon and differenhahon to amveat diagnoses on wbich tbey base their care'
For example (a very simple example), you see a patientwho IS moaning, dutcbmg bis chest, cold and clammyBased on biobehavioural theory, the nurse makes an infer-ence that this situahon means 'angina' and estabhshes amental picture tbat represents to tbe nurse the facts of tbesituahon as sucb Another nurse who is deeply entrenchedm psychodynamic theory may infer this situahon to be an'acute anxiety attack' Two nurses coming upon the samesituahon but establishing two different mental pictures oftbat situation, of course, is a possibility, a problematicpossibihty Since this pomt m practice is foundation towhat occurs at next steps, tbe theones, frameworks andonentahons used (or not used) to 'establish' the situahonare cnhcal
Inferences which nurses make at this point have beenconsidered atbeoretical by many saenhsts, indicahng tbattbey are based on intuitive reasoning (taat knowledge byPolanyi 1966) or on pattem matcbmg (as suggested byBenner 1984 m ber work with cnhcal care nurses) On tbeother hand, Argyns & Schon (1974) and Argyns et al(1985) suggest tbat such inferences are likely to be basedon 'theones-m-use' rather than on 'espoused tbeones'Tbese arguments indicate tbe nohon that an individualformulates an idea about a situahon based on a speafic setof cognitive map or tbeones that are brought mto tbesituahon by the actor as relevant either consaously orunconsaously
Identifying problems
Tbe practihoner's move to step 2 mvolves amvmg at aspeafic conjecture(s) about nursmg problems representedin the situahon in order to establish firmly what bnds ofthmgs (i e phencnnena) require nursu^ soluhons TTus iswhat Schon calls 'the fiammg of a problem', tbat is
1634
Putttng theory into practice
Whoi we set the problem, we select what we will treat as the'thmgs' of the situahon, we set the boundanes of our attentionto it, and we impose upon it a coherence which allows us tosay what is wrong and in what direchons the situation needsto be changed Problem setting is a process m which, inter-actively, we name the thmgs to which we will attend and framethe context m which we will attend to them
(Schon 1983)
The mental representation established at step 1 draws thenurse to consider selected aspects of the situahon to formu-late the type and nature of nursmg problems representedby the situation This involves discrimination as to whatare and what are not cntical, important and appropnateproblems presented in the situation that require nursingmtervenhon
Specific conjecture(s) about problems m a given situahonare denved as relevant ant requiring soluhon For example,the speafic conjectures about the patient represented withangina would be that he requires attention regardingarrythmia, pam, dyspnoea, and stress, while the specificconjectures about the patient represented with acuteanxiety attack would be that he requires attention regard-ing stress reduction and comfort At this point, speaficconjectures about the situation are formulated based onthe pnmary mental representahon established at step 1 mconjunction with other vanables noted by the nurse in thatsituation, such as, for example, the patient's age, his/heroverall demeanour and behaviours, and his/her personalhistory
Focus for applying theory
The movement mto step 3, the step most often identifiedas the focus for applying theory into practice, involvesselechon of nursmg mtervention to be appbed in a givenpractice situation Multiple theones and multiple solutionsthat exist m the public domain not only compete with eachother for selechon but also with those multiple soluhonsthat are integrated into the pnvate domam of knowledge ItIS espeaally so because this is the step m which the actualaction deasions are made At this step, a practitioner isfaced with two issues accessibihty and preference
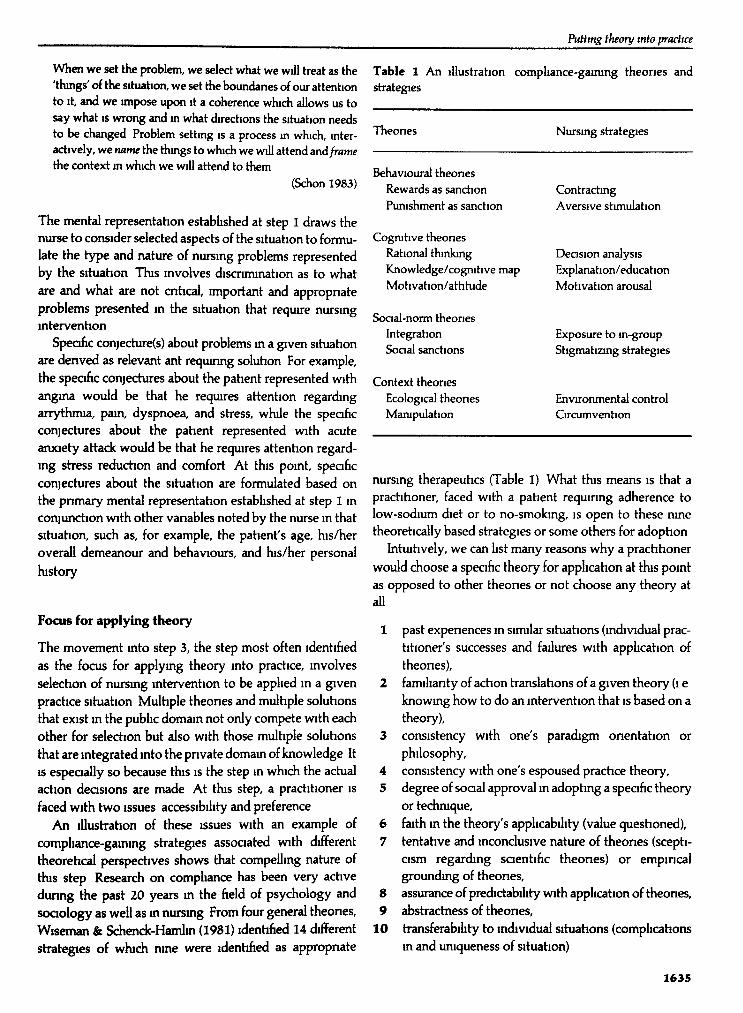
An lllustrahon of these issues with an example ofcompliance-gainmg strategies associated with differenttheoretical perspectives shows that compelling nature oftbs step Research on comphance has been very activedurmg the past 20 years m the field of psychology andsociology as well as m nursmg From four general theones,Wiseman & Schenck-Hamlm (1981) ldenhfied 14 differentstrategies of which nme were ldenhfied as appropnate
Table 1 An illustration compliance-gaming theones andstrategies
Theones Nursmg strategies
Behavioural theonesRewards as sanctionPunishment as sanction
Cognihve theonesRational thinkingKnowledge/cognitive mapMotivation/attitude
Social-norm theonesIntegrationSocial sanctions
Context theonesEcological theonesManipulation
ContractingAversive stimulation
Decision anedysisExplanation/educationMotivation arousal
Exposure to m-groupStigmatizmg strategies
Environmental controlCircumvention
nursing therapeutics (Table 1) What this means is that apractitioner, faced with a patient requmng adherence tolow-sodium diet or to no-smobng, is open to these nmetheoretically based strategies or some others for adophon
Intuitively, we can hst many reasons why a practitionerwould choose a specific theory for application at this pointas opposed to other theones or not choose any theory atall
1 past expenences m similar situations (mdividual prac-htioner's successes and failures with applicahon oftheones),
2 familianty of action translahons of a given theory (i eknowing how to do an intervention that is based on atheory),
3 consistency with one's paradigm onentation orphilosophy,
4 consistency with one's espoused prachce theory,5 degree of soaal approved m adopting a speafic theory
or technique,6 faith m the theory's applicabihty (value questioned),7 tentahve and inconclusive nature of theones (scepti-
cism regarding saentific theones) or empmcalgrounding of theones,
8 assurance of predictabdity with applicahon of theones,9 abstractness of theones,
10 transferabihty to individual situations (comphcahonsm and uniqueness of situation)
1635
HSKtm
If prachhoners take all of these reasons mto their heartswithout some form of remedying strategy, then there is noescape but to become paralyzed m their practice or becomeagnoshcs regarding theones and saenhfic knowledge
Choice of intervention
While movements mto steps 1, 2 and 3 mvolve choicesat cognihve level, step 4 mvolves actual enactment ofmtervenhons Determinations as to what happens at thisstep most often involve both the actor's (that is, theprachhoner's) abilities and condihons at the given momentand the extemal constraints and resources that exist menvironment of the given prachce situahon Even undergood mtentions and correct choices, achons themselvesmay 'eventuate' quite differently from what had beenexpected owmg to what exists m the situahon of practice
At this step, it IS necessary to separate what is controll-able from what is not, as theones are put into practicethe world (or some aspects of the reality in which weare situated) moves on regardless of what is going onconcurrently Hence, at this step the pnmary issue is not inapplymg theory into practice but with the mechanics andprocesses mvolved in enactment of theory choices
FOUR MODES OF THEORY APPLICATION
As we view these four steps m which prachhoners aremvolved m makmg choices and delivermg enactments,we carmot evade the queshon of complexity in puthngtheory mto practice but at the same time recognize theneed to come to terms with ourselves m order to handle thesituahon
Four different modes of theory apphcahon are proposedas ideal types m deabng with mulhple theones, explanahonsand approaches for solvmg prachce problems (a) co-herence mode, (b) mtegrahve mode, (c) pragmahc/eclechcmode, and (d) reflechve mode
Coherence mode
A coherence mode requires prachsmg nurses' commitmentsm speafic philosophical, epistemological and paradigmaticonentahons and usmg such commitments as the guideline tomake theory dioices For example, a nurse who is philo-sophically and paradigmahcally committed to hobsm andRogenan framework of urutary human beings as the guidefor prachce would only adopt those nursn^ theones andnuremg strategies wbch are inherently coha-ent with thatframework
This approadi adheres to the foundahonabst philosophyof saence In this mode, one must consider the committedset of onentahons as the true, the best, or at least the mostplausible guide for knowledge utilizahon While an mdivid-ual nurse's ideological coherence is assured m tbs approach,it can create an ideological chasm m wbch nurses' pblo-sopbcal and paradigmatic onentations may confradid thoseof dients who are at the receivmg ends of nurses' onen-tahons Tbs mode, therefore, may provide a sense of coher-ence and mtegrahon to prachsmg nurses with resped totheir world views and knowledge-use, but at the same hmecan create dogmatism m prachce Tbs mode abgns withwhat Kuhn (1962, 1977) proposes for scientific pradice mwbch mcommensurability among paradigms is stressed
The mtegrated prachce framework with an emphasis onhabibtahon is an example proposed for soaal woric from thiscoherence mode of prachce (Parsons et al 1988) Lewis(1988) proposes adoptmg Roy's model as the theorehcalfoundahon for nursmg pradice with a goal to eliminate thegap between theory and prachce Both Jones (1989) andFawcett (1992) advocate tbs mode of prachce based oncommitment to speafic conceptual models as a way tomakmg nursmg a saentific prachce In tbs mode there is acongruity among theones appbed m the different steps ofthe process by a prachhoner
bitegrative mode
The second approach, an mtegrahve mode, refers to aposihon m whidi the prachhoner is onented to mcorporat-mg new theones and techniques into aligrmient with theestabbshed personal pradice philosophies and theoreticalonentations Tbs mode can be viewed as an evolutionarymode of pradice m wbch a prachtioner develops over thecourse of bs/her prachce an ever-expandmg but mtegratedpersonal practice paradigm resulting from interweavingnew theones and approaches from diverse sources andonentahons
Theones seleded for appbcahon at the four steps of theprocess may be drawn from vastly different onentations,however, the selected theones become mtegrated by thepractitioner to make a personal sense Hence, the focus ofapplying theory to pradice m this mode is m the prac-hhoner rather than m a specific theorehcal or paradigmaticonentation
Beitman (1989) adopts an mtegrahonist position with afocus on himself as the point of mtegrahon, thus stahng
I wanted to conceptuabze psydiotherapy, to ckvelop a modelof it I wanted the mockl to be finnly rooted in undeniablegeneral prmapks dosely tied to the real-wodd behavior
1636

Puttmg theory into practice
of chents and counsellors I also wanted it to be flexibleenough to suit the speaal and varying arcumstances of themany practitioners I wanted to fend a way to embrace bothsimtUnties and differences
He then proposes for lntegrahve prachtioners to mcorporateinto practice such pnnaples as (a) the similanties and con-vergence among schools, (b) the heunstic value of stages mcounselling, (c) the interpersonal nature of counselling mboth its form and its major purposes, (d) the flexibilityrequired in matching approaches to speafic clients, and (e)the flexibihty m appreaating the role of new ideas andapproaches m the light of existmg ones
This mode supports the adoption of one aspect of whatBarlow et al (1984) suggested as the model for the saenhstpractitioner The usefulness of nval explanations andcontradictory knowledge can be verified or validated onlythrough their application mto prachce as a way of integrat-ing new theones and approaches to the practitioner'salready estabhshed framework for practice Hence, prac-htioners by applying 'applied research protocols' canengage in further testing of theones m speafic practicesituations without controls
Empmcal procedures such as single case, time-senesanalysis, deviant-case analysis and clinical replication aresuitable for testmg theones (strategies emerging fromtheones) m prachce situations in order to examine theirapplicability and validity in the light of all of the compli-catmg factors of the situation In this mode, nurses are notjust making choices about different theones but are teshngthe validity of chosen theones m order to cumulate knowl-edge, by finding out when certain theones work whileothers do not (for example, see Nolan & Grant 1992) So,each practice situation is a quasi-expenment in which sys-tematic data must be obtained and evaluated for saentificvalidity for the practitioner
In addihon, Messer (1989) suggests that an lntegrationistIS faced with the need to accept the 'different sorts andsources of data on which each therapy relies as an evidentialbase' Hence, an integrahonist has to know how to interpretempmcal findmgs that are produced with vanous methodsand to mtegrate them into one's prachce paradigm
Pragmatic/eclectic mode
The third approach, a pragmatic/edectic mode, refers toadopting a pragmahst's posture m knowledge-use, hence,the focus of theory use is not on the practihoner but onclient and client's problems Lazarus (1989) advocatessystematic, prescnptive (technical) edecticism as a way fora practitioner to combine the impacts of patient qualities,clinical sblls and speafic techniques He supports the idea
that 'a technically eclectic stance endeavors to use effechvetechniques from any persuasion, while also searching forguiding pnnaples and concepts, and tnes to avoid theneedless addition or multiplicahon of explanatory pnnaples'and further states that 'the hallmark of tedinical edechasmIS the use of prescnptive treatments based on empmcalevidence and client need, rather than theoretical andpersonal predisposition'
Since the objective of nursing practice is to solve chents'problems, a pragmatist's position aUows practihoners toselect those knowledge-claims and theones which are mostcapable or useful in solving given nursing problems Thisapproach allows nursing practihoners to circumvent thephilosophical differences underpinning compehng theonesand to disregard different philosophies and methodologiesadopted in knowledge generahon, but to focus only ontheones' ability to solve clinical problems Nurses can thusbe eclectic m selechng theones and strategies that arethought to be most useful, regardless of their onentahonsm given situations and at given steps of the process Thus,several theones with different orientations may be selectedfor apphcahon m any pahent care situahon or differenttheones may be selected for applicahon for different pahents
Knstjanson et al (1987) propose a meta-model that wiUguide the use of multiple theones m practice, rejechng theidea of the smgle-model approach for nursing prachce Thismeta-model requires the prachtioner to amve at applyingtheones through a process of inquiry that involves ideal,error and change m which a range of choices is formulatedfor application, rather than simply relying on habit andIgnorance
While this model is guided by the notion that 'the prac-titioner IS faced with the task of finding the best soluhon forthe particular client situation' (Knstjanson et al 1987), theguidmg pnnciple for deadmg what is best is based onstrong empmcal evidence supporting the application ofone theory of approach in contrast to others This modealigns closely with the model of professional practice that isbased on 'technical rationahty' by Schon (1983)
Reflective mode
The fourth approach is a reflective mode in which theorychoice IS entrenched m reflections by practitioners Newtheones and empmcal approaches are adopted for theircongruence with the view of the situation and themeanings of the problems gained from the practitioner'sreflections about own actions, reflections on situation, andreflections with the client
Achon saence advocated by Argyns et al (1985)considers reflection as the key to developmg effechve
1637
HS Ktm
functionmg of prachhoners, as prachhoners m general tendto be entrenched m a manner of practice that does notpromote new leaming Accordmg to action saence, reflec-hon of prachhoner's theones-m-use can lead to contmuousleammg of new theones-m-use, in that reBechcm allows theprachhoner to adopt advocacy, inquiry and joint enterpnseas the guidmg pnnaples of achon (Argyns et al 1985)
A nurse as an action scientist adopts the leammg-onented theones-m-use (Model II theones-m-use byArgyns et al 1985) and m domg so uses behaviouralstrategies that mvolves 'shanng control with those whohave competence and who partiapate m desigrung orimplementmg the achon' (Argyns et al 1985) Therefore,theory applicahon m the reflective mode with the actionscience perspechve mdicates 'redesignmg action' throughthe process of self-morutonng and reflection, reflechonwith the situahon, and reflechon with parhapants ofprachce
A reflechve mode encompasses not only reflection-m-achon by the prachhoner-self but also reflection-m-practice with those who are the reapients of practiceHabermas's (1971) cntical philosophy m which cnhcal selfand mterpersonal reflechons are considered the keys toshapmg the world we bve m provides the foundahon for areflechve mode This mode is an extension of Lewm's ideaof action research (1948) m which theones are developedand tested through prachce The essence of tbs mode isshared mquiry, selechon and control, with a goal of fusionamong the prachtioner's theorehcal onentahon, newtheones and approaches, and the dient's meanmgs andphilosophy
Schon (1983) asserts that the reflechve prachhoner isengaged m reflechve conversahons with the cbent as weUas v«th the situation Theory appbcahon at every step ofthe process mvolves a deasion that is denved from mutualunderstanding of the prachhoner's and the dient's per-spechves and of the values of different theones for thesituahon and parhapants The focus of the mode is then thepractihoner, situahon and dient as a urut
The four modes idenhfied m the foregoing are idealtypes for theory appbcahon and suggest different wayspractihoners may seek and use theones and strategies mpractice The consequences m practice m terms of problem-solving efificacy, cbent and prachtioner satisfaction, andorgamzahonal outcomes may vary accordmg to modesadopted by prachhoners
GOVERNING CRITERIA
While the four modes of theory applicahon emphasizepossible processes mvolved m juxtaposing a personal
world of knowledge with the public (world-at-large) one insituahons of prachce, theory application involves apnonacceptance of certam vahies by practihoners Regardless ofthe adoption one takes in terms of the modes, there arecertain cntena which are cnhcal m applymg theones mtopractice that must be used as guidebnes for assessingtheones, knowledge daims and tedmologies These follow
1 Rahonality supposes that practical deasions should bebased on the "best' tested theory, as Popper suggests,or at the least the well-tested theones One must beable to distmguish the best or well-tested theones fromthose that are not tested adequately However, it isalso necessary that ways m dealing with the pro-visional, uncertain nature of saence and theones mustbe developed by prachtioners Hence, as Phillips(1989) indicates, mformed judgement is cntical mapplying saence to practice Woodruff (1976) lllus-frates this sentiment by the followmg 'the prachcalman, if he has any scienhhc msight, knows full well thatthere is no way by which he can be certam of makmgcorrect deasions, but he wants nevertheless a guidewhich, if consistently followed, will enable him tomake deasions which tum out later to have beencorrect more often than would otherwise have beenthe case
2 Prachtioners must 'realize that practical appbcation is agambbng situation and that they need to gamble well,maximizmg the likelihood of gams and minimizing thepossibibty of losses from appbcahons of saence toprachce' (Phillips 1989)
3 Ethics of responsible action must guide the appbcahonof theory mto prachce Ethics of responsible actionrequire the practitioner to be comf>etent, consaous ofconsequences and morally committed to others as tooneself
4 The logic of prachce is m action's onentation to futurebut enactment that becomes a thmg of the past as it isenacted What it means is that one cannot reverseactions once they are enacted and that only recourse toremedymg practice is through cnhcal self-reflection
5 Premise of beneficence must be observed m practice asprachhoners are guided by goals that reside m thedients
CONCLUDING REMARKS
This analysis by no means depicts a complete picture oftheory appbcahon to nursing practice As theory gener-ahon must precede theory appbcation and smce theorygenerahon depends upon a well-frmctioning feedback pro-cess between scientists and prachhoners, many structural
1638
PtMtng theory tnto practice
facets beyond the processes associated with individual
practitioners will afifect the nature of theory use m
practice
Furthermore, since scientists can be considered to be
engaged m theory appbcahon to prachce, that is, m
saenhfic practice, the four modes of theory appbcahon are
applicable to scienhsts as well Scienhsts then would be
mvolved m producmg knowledge or research wbch are
quite vanant in terms of nature, type and onentation The
consequences of these on the discipline and practice would
be astoundmg
Nonetheless, what seems cntical at present for nursmg
IS to gam knowledge about the usual modes of theory
appbcahon by practiang nurses vis-d-vis the ideal types so
that we gam better msights regarding the dynamic process
of knowledge generation, knowledge appbcation and
consequences of pradice
References
Argyns C, Puhiam R & Smith D Me (1985) Action Saence
Jossey-Bass, San FranciscoArgyns C & Schon D (1974) Theory in Practtce Increasing
Professtonal Effecttveness Jossey-Bass, San Franasco
Barlow D H, Hayes S C & Nelson R O (1984) 77K SaenttstPracttttoner Research and Accountability tn Clinical and Edu-
cational Settmgs Pergamon Press, New YorkBeitman B D (1989) Why I am an integrationist (not an eclectic)
Bnttsh Joumal of Guidance and Counselltng 1 7 , 2 5 9 - 2 7 3
Benner P (1984) From Novtce to Expert Excellence and Power m
Cltmcal Nurstng Practtce Addison Wesley, Menlo Park,California
Clarke M (1986) Action and reflechon practice and theory mnursing Journal of Advanced Nursing 1 1 , 3 - 1 1
Craig SL (1980) Theory development and its relevance fornursmg Joumal of Advanced Nursing 5,349-355
Fawcett J (1992) Conceptual models and nursmg pradice thereaprocal relationship Joumal of Advanced Nursing 17,224-228
HabermasJ (1971) Knowledge and Human Interest Bacon, Boston
Holland R (1990) The paradigm plague prevention, cure, andmoculahon Human Relations 43 , 23-48
Ingram R (1991) Why does nursing need theory? Joumal ofAdvanced Nursing 16, 350-353
Jones S (1989) Is unity possible? Nursmg Standard 3, 22-23
Katz F (1976) Structuralism m Soaology An Approach to Knowl-
edge University of New York Press, Albany, pp 99-118Knstjanson LJ, Tamblyn R & Kuypers JA (1987) A model
to guide development and application of mulhple nursmgtheones Joumal of Advanced Nurstng 1 2 , 523—529
KuhnTS (1962) The Structure of Scientific Revolutions University
of Chicago Press, ChicagoKuhn T S (1977) The Essential Tension University of Chicago
Press, ChicagoLazarus A A (1989) Why I am an eclectic (not an mtegratiomst)
Bntish Joumal of Gutdance and Counselling 1 7 , 2 4 8 - 2 5 8
Lewin K (1947) Feedback problems m social diagnosis andaction Human Relations 1,147-153
Lewm K (1948) Action research and minonty problems InResolvtng Soaal Conflicts (Lewin G W ed), Harper, New York.
Lewis T (1988) Leaping the chasm between theory and practiceJoumal of Advanced Nursing 1 3 , 345 -351
Messer S B (1989) Integration and edectiasm m counselling andpsychotherapy cautionary notes Bnttsh Joumal of Gutdanceand Counselling 17 , 274-285
Miller A (1985) The relahonship between nursmg theory andnursing practice Joumal of Advanced Nursing 10, 417-424
Nolan M & Grant G (1992) Mid-range theory building and the
nursing theory-practice gap a respite care case shidy Joumalof Advanced Nursing 17 , 217-223
Parsons R J, Hernandez S H & Jorgensen J D (1988) Integratedprachce a framework for problem solvmg Soaal Work 37,417-421
Phillips B N (1989) Role of the practitioner m applymg science to
pradice Professtonal Psychology Research and Practice 20,3-8
Polanyi M (1966) The Tacit Dtmension Doubleday, Garden Qty,New York State
Pyles S H & Stem P N (1983) Discovery of nursmg gestalt mcntical care nursing the importance of the Gray Gonlla Syn-drome Image The Joumal of Nursing Scholarship 15,51—57
Sandelands L E (1990) What is so pradical about theory? Lewmrevisited Joumal for the Theory of Soaal Behaviour 20,235—262
Schneider SF (1990) Psychology at a crossroads Amencan
Psychologists 45, 521-529Schon D A (1983) The Reflective Practtttoner Basic Books, New
YorkWiseman RL & Schenck-Hamlm W (1981) A multidimensional
scaimg vaLdation of an lnduchvely-denved set of comphance-gaining strategies Communication Monographs 48,251-270
Woodruff M (1976) Problem-solvmg m science Research andMedtcal Practtce Their Interaction A Ciba Foundation Sympostum
44, 97-114
1639