Embed Size (px)
Citation preview

743
PYLORIC STENOSIS IN ADULTSC. T. HOWE, B.M., B.CH.
Research Assistant, Department of Surgical Studies
M. P. SPENCE, M.B., B.CHIR., M.R.C.P.Senior Medical Registrar
Middlesex Hospital, London, W. i
Pyloric stenosis is defined as an obstruction togastric emptying due to any cause situated above.he biliary ampulla. This article is concernedwith the clinical features, metabolic disorder,assessment and treatment of patients with pyloricstenosis; anatomical narrowing of the pyloriccanal without delay in gastric emptying is notconsidered. In adults, symptoms due to theunderlying lesion may precede by weeks, monthsor years those due to obstruction and contributeto the clinical picture to a varying degree. Pyloricstenosis is unique among gastro-intestinal dis-orders which produce electrolyte disturbances inthe constancy with which it causes extracellularalkalosis and it is this aspect of the condition thathas received most attention in recent years.Clinical Features
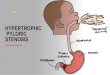
Benign peptic ulceration is the commonestcause of pyloric stenosis and was responsible for86% of 18 cases reviewed by Balint and Spence.'In 80% the ulcer was situated at or near thepylorus, but in 6% there was a remote gastriculcer with surrounding inflammatory and fibroustissue which shortened the lesser curve andextended to envelop the pylorus. Carcinoma ofthe pyloric region accounted for 11% of the casesin this series. Uncommon causes are cholecystitiswith involvement of the pylorus in adjacent in-flammatory tissue and carcinoma of the pancreasor duodenum. Rarely patients present in adultlife with congenital conditions such as hyper-trophic pyloric stenosis, duodenal diaphragmaticocclusion or compression of the pylorus bycholecysto-jejunal bands.
Earlier surgical treatment has reduced thenumber of peptic ulcers that progress to pyloricstenosis. It has been estimated to arise in about3% of patients with duodenal ulcers (includingpyloric and pre-pyloric ulcers), and in I% ofthose with lesser curve ulcers.
Benign duodenal ulceration causes cicatricial
narrowing of the pylorus, but in almost all casesof pyloric stenosis distortion by inflammatoryoedema is the precipitating cause of obstruction.This is why pre-operative preparation commonlyresults in relief of both pain and gastric retention.It is exceptional to find a healed ulcer in a patientwith unrelieved pyloric stenosis.Vomiting is the cardinal symptom and is rarely
absent. Usually it is preceded by a long history ofrecurrent dyspepsia and is sometimes episodic, theepisodes coinciding with active phases of the ulcer.In half the patients the vomit is copious, usuallyfree from bile and may contain undigested (andrecognizable) food taken many hours before.Typically the vomiting occurs in the late hours ofthe evening or in the early hours of the morning.Anorexia and weight loss are the rule. Diarrhoeaoccurs more frequently (20% of cases) than mightbe expected in an obstructive lesion of the upperalimentary tract. Offensive eructation is a diag-nostically helpful symptom when it occurs.
In approximately half the patients in whompyloric stenosis is diagnosed there are no abnormalphysical signs. A gastric succussion splash, onlysignificant if at least three hours have elapsedsince the last meal, is the commonest abnormalfinding. Visible waves of gastric peristalsis cours-ing across the abdomen from left to right are ofgreat diagnostic value, and occasionally it ispossible to see the outline of a grossly distendedstomach. Signs of fluid depletion or latent tetanymay be found. Gastric aspiration is the mostvaluable single diagnostic procedure. The normalstomach is empty three to four hours after a meal,but this time may be prolonged by such factorsas emotion, a fatty meal, or an attack of migraine.Nevertheless, the repeated presence of a largegastric residue, i.e. more than 250 ml. in patientson a normal hospital diet, four or more hoursafter the last meal, is an almost certain indicationof pyloric stenosis.
Barium-meal examination usually reveals pyloricG1
Protected by copyright.
on 23 Novem
ber 2018 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.422.743 on 1 Decem
ber 1960. Dow
nloaded from

4 POSTGRADUATE MEDICAL JOURNAL December 1960
·~:::::;i
:::....*:..::.:
· ':·::L:::i.
FIG. i.-Radiograph of the abdomen of a patient withpyloric stenosis one week after a barium meal.The whole lower abdomen is filled by a grosslydistended stomach still containing a large bariumresidue.
stenosis when it is present and is of additionalvalue in determining the underlying lesion. Pre-liminary fluoroscopy may show a dilated stomachand it is wise to empty this by aspiration beforegiving barium, otherwise it may be impossible todemonstrate the cause of the stenosis. Obstruc-tion may be intermittent in the early stages andcannot be excluded by the demonstration ofnormal emptying at one examination. A word ofcaution is necessary about barium-meal examina-tion in suspected cases. In severe pyloric obstruc-tion, barium, like food residues, may remain inthe stomach for many days, presenting a majorobstacle to the proper preparation and treatmentof the patient (Figs. i and 2).
Usually the diagnosis of pyloric stenosis iseasy, but it may remain unsuspected if thevomiting is mistakenly ascribed to uncomplicatedpeptic ulceration. The vomitus may resemblethat of exsanguinating haematemesis and diagnosismay be extremely difficult particularly as theconditions may co-exist. Significant blood losseven in the presence of pyloric obstruction isusually accompanied by melaena. If abdominalpain is severe its association with vomiting maymimic an acute surgical emergency. Diarrheoa
: ::..i...B-3s:::8::..-Hq;;
ffik,.
FIG. 2.-Further radiograph of the same patient afterrepeated gastric lavage. The stomach is smallerbut is still outlined by retained barium.
and vomiting in a patient with peptic ulcerationmay be attributed to food poisoning and thismay lead to omission of further investigation.The combination of body fluid depletion, vomitingand a raised blood urea may suggest chronicrenal disease, but the high specific gravity ofthe urine and the increased plasma bicarbonatelevel in pyloric stenosis make distinction easy.Rarely in the severely alkalotic patient the abdo-minal symptoms may be concealed by mentalconfusion or even coma.22 For this Hurst13 usedthe term 'coma dyspepticum', attributing it toVon Sakset.The pre-operative diagnosis of the underlying
lesion in a patient with pyloric stenosis is not ofparamount importance, but clinically a shorthistory of dyspeptic symptoms before the onsetof stenosis is suspicious of carcinoma. A mass israrely palpable in the abdomen nor is it certainevidence of malignancy. Even radiology may beinconclusive.
Metabolic ChangesMany patients with pyloric stenosis suffer from
the effects of loss of electrolytes and water pre-senting in its most severe form as gastric tetany.This was first described in I886 by Kussmauland in the early part of this century the disorder
Protected by copyright.
on 23 Novem
ber 2018 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.422.743 on 1 Decem
ber 1960. Dow
nloaded from

December I960 HOWE and SPENCE: Pyloric Stencsis in Adults 745
METABOLICNORMAL ALKALOSISpH 7 40 pH 7.54
,00 100A
50 50
URINNE
ACIN ALKALINEICI DECREASEDHCO,INCREASED
FIG. 3.-Typical changes in the extracellular electro-lytes in a patient with pyloric stenosis. (FromLe Quesne.'5)
was attributed to the secretion of toxins by thepylorus or obstructed stomach. McCallum andothers in I92016 demonstrated that the blood wasabnormally alkaline with an associated increase inneuromuscular excitability, and attributed thesechanges to loss of acid and chlorides in the vomit.Gamble and Ross"' demonstrated, in dog experi-ments, that an accompanying loss of sodium ionscaused the dehydration. They showed that wateror ammonium chloride solutions were ineffectivetherapy but that saline was curative. Subsequentworkers 4,6, 14, 17, 19 have demonstrated marked de-pletion of potassium in gastric alkalosis.The metabolic disturbance of pyloric stenosis
is caused by the loss of large amounts of acidgastric contents, probably as much as four litresper day in the worst cases. The magnitude ofthe losses of the important electrolytes can beseen from their mean concentrations in the gastricaspirate (Table I). The net effects of these losses
TABLE I
ELECTROLYTE CONCENTRATIONS IN THE GASTRIC CONTENTOF PATIENTS WITH PYLORIC STENOSIS, AT THE TIME OF
ADMISSION TO HOSPITAL
BenignUlceration Carcinoma
Sodium ..· ·· 50 55Potassium .. .... 11 IIChloride ...... I I 7.5 5I'Acid ' (by subtraction) .. 56.5
(All values as mEq./litre.)
are characteristic; the extracellular fluid and cir-culating blood volumes are reduced, the plasmachloride concentration is lowered with a corre-sponding increase in the plasma bicarbonate level
'-m: . ·'- :
: -.. ........ ·1
.;
r·.
CAUPY ANG ;Tr"T&I,R "X'IA,C:IBLI -Sa'....?-~....vine *~MU wet uinw
·tTIIiU.m S .. "'": -
ILC.F. E.F.
iC NCO3
c.:
ti HH+CO·: :' ,,,
'.· ,.K
E~.'' "
FIG. 4.-The intracellular-extracellular ionic shifts andtheir effects in potassium depletion. (FromLe Quesne.15)
and the plasma is more alkaline, i.e. a state ofhypochloraemic alkalosis (Fig. 3).The kidney normally excretes an acid urine,
but as a result of the extracellular alkalosis inpyloric stenosis the urine formed is alkaline inreaction. The sustained excretion of an alkalineurine represents a considerable departure fromnormal, entailing the loss of large quantities ofsodium or potassium in place of hydrogen ion,thus conserving the latter and limiting the degreeof extracellular alkalosis. By this increased urinaryexcretion of sodium and potassium the kidneysconvert a gastric loss of hydrochloric acid into atotal body loss of sodium and potassium chloride.
In the early stages of pyloric stenosis the gastricand urinary losses of sodium lead to considerabledepletion. Gamble and Ross1 have describedsodium as the skeleton of the extracellular fluidand its depletion is accompanied by a propor-tionate loss of water thus reducing the extracellularvolume. This process is limited by markedreduction in the sodium content of the urine,but potassium excretion continues undiminisheddespite a falling plasma level. It is the loss bythis route which is largely responsible for potas-sium depletion.21
It has long been known that the urine maybecome acid in the late stages of extracellularalkalosis.7, 13 This change in urinary reaction isconnected with internal rearrangements of theelectrolytes between the intracellular and extra-cellular fluids due to potassium depletion.8s, 9, 20Potassium is the principal cation of the intra-cellular fluid and, when it is lost from the body,sodium and hydrogen ions from the extracellularfluid enter the cells to replace it (Fig. 4). This
Protected by copyright.
on 23 Novem
ber 2018 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.422.743 on 1 Decem
ber 1960. Dow
nloaded from

746 POSTGRADUATE MEDICAL JOURNAL December 1960
aggravates the extracellular depletion of sodium.Furthermore, the migration of hydrogen ion notonly increases the extracellular alkalosis but alsomakes the intracellular fluid acid. The paradoxof an acid urine excreted in the face of increasingalkalinity of the plasma is in part explained bythese intracellular changes.2The electrolyte and fluid deficiencies are re-
flected in renal function. The blood urea rises,the urine is scanty, of high specific gravity andcontains little or no chloride. Initially alkaline, itbecomes acid in the later stages. Usually, adequaterenal function returns as soon as the circulatingblood volume and electrolyte deficiencies havebeen replenished, but slight impairment maypersist.5 Nephrocalcinosis has been reported as aresult of pyloric stenosis both in the experimentalanimal18 and in man.7
TreatmentThe aims of initial treatment of patients with
pyloric stenosis are threefold: to promote healingof the causative ulcer and alleviate pain, to relievethe effects on the stomach of long-standing ob-struction, and by replenishing the fluid andelectrolyte deficiencies to correct the metabolicdisturbance. The definitive treatment should besurgical. Bed rest and, possibly, antacids withsedatives promote healing of the ulcer and regres-sion of the surrounding inflammatory reaction,thus helping to overcome the obstruction andmaking subsequent operation easier. Atropineor other anti-cholinergic drugs should not begiven as any effects they may have in openingthe pylorus is offset by their depressant effect ongastric motility.
Local treatment of the stomach consists ofemptying it and preventing the accumulation ofstagnant contents. A large bore oesophageal tubemay be necessary for the initial lavage. Subse-quently, a small bore tube of the Ryle's type maybe used, but it is important to remember thatanything given by mouth may have to be with-drawn through the tube later. In the milder casea traditional ulcer diet may be given, but thestomach should be emptied each evening. Inmore severe cases with persistently large residuesthe tube may be left in place and a fortified milkfeed given through it during nine hours out ofeach twelve, the stomach being aspirated threehours after each feed ends. Pain is rapidly re-lieved, the pylorus opens up (as shown by asteadily decreasing aspirate), and the patient comesto operation with a clean stomach that can behandled and sutured with safety.
In all but the mildest cases water and electro-lytes should be given parenterally and an initialassessment of the patient's needs can be made
15Extracellula r
Volume in 10Litres 5
Hoemotocriti
38r / x X
Weight in Kg. t x36300 r
CSodium & CChloride N C
100
BGlance in
mEq.FIG. 5.-Changes resulting from infusion of normal
saline in a patient with pyloric stenosis due tocarcinoma. In the first I2-hour period sodiumand chloride are retained equally. In the secondperiod no further retention occurs, showing thatapproximate equilibrium has been achieved. Theextracellular volume rises, as demonstrated bydirect measurement using 82Br., and indirectlyby the fall in haematocrit level and the gain inweight.
without laboratory tests, although these makemanagement of a severe case much simpler. Theseverity of the vomiting and clinical signs of saltand water depletion or latent tetany will give anindex of the losses that have occurred. Thesimpler tests include the volume, specific gravity,chloride content and reaction to litmus of theurine. If there is an appreciable electrolytedeficiency an acid urine indicates severe potassiumdepletion. The blood urea, bicarbonate (or alkalireserve) and haemoglobin are the most usefullaboratory investigations. The plasma electrolytelevels are helpful in the more complicated cases.Low plasma levels of sodium or potassium indi-cate a body deficit of these ions, but normal levelsmay be found despite significant degrees ofdepletion. A raised blood urea is probably the
Protected by copyright.
on 23 Novem
ber 2018 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.422.743 on 1 Decem
ber 1960. Dow
nloaded from

December 1960 HOWE and SPENCE: Pyloric Stenosis in Adults 747
best indication for saline therapy and a raisedplasma bicarbonate for potassium therapy.
In the simple case where there is little dis-turbance of acid-base equilibrium the adminis-tration of normal saline will increase the extra-cellular volume with clinical improvement, gainin weight, the establishment of an adequateurinary flow and a fall in the haematocrit reading(Fig. 5). Where considerable disturbance ofacid-base balance has already occurred with signsof peripheral circulatory failure the overridingneed is for fluid and salt. Although over-hydrationis a danger, especially in cardiac disease, insuffi-cient infusion is a commoner error. Deficits of5oo-600 mEq. each of sodium and chloride repre-senting a need of 4 litres of normal saline forreplenishment are commonly encountered andcases occur with total body deficits of sodiumand chloride in excess of I,500 mEq. (io litres ofnormal saline).
In estimating the deficit the following rules arehelpful: if clinical signs of depletion are minimalbut chloride is absent from the urine, 2 litres ofsaline will be needed; if obvious clinical signs arepresent the loss equals 6% of the body weight(e.g. 4 litres in a 70-kg. man); if peripheral circu-latory failure is present it represents a loss of atleast 6 litres. In planning the intravenous treat-ment it is best to replace half the estimated deficitin the first I2 hours and then review the position,aiming at complete replenishment in 48 hours.The losses by aspiration over each I2-hour periodmust be measured and an equivalent volume ofnormal saline should be added to the intake forthe next period. These amounts are additionalto the basic requirements of a patient receivinglittle fi id by mouth.
In pyloric stenosis of any severity potassiumdepletion is invariably present and potassiumchloride should be given orally in all patients.In the mnore severely depleted patient excreting anacid urine despite severe extracellular alkalosis,it may be advisable to break the general rule andadminister potassium parenterally before there isan adequate urinary flow. The prolonged adminis-tration of saline alone in such a patient mayresult in a dangerous lowering of the concen-tration of potassium in the extracellular spaceboth by dilution and by increasing the renalexcretion of potassium.10, 17 Furthermore, salineadministration, although it may occasionally makethe urine alkaline in reaction, only partly correctsthe alkalosis.6, 8,14,23 Correction of potassiumdepletion with potassium chloride results in dis-placement of sodium and hydrogen ions from theIntracellular fluid, thus helping to correct boththe alkalosis and sodium depletion of the extra-cellular fluid (Fig. 6). Parenteral potassium may
Pl·.ner -p
9-...Urine pH' 7 -
umuti -
was administer ed and sodiumretained throughout
the period of study. The plasma electrolyte concen-
trations were restored almost to normal before the
mEq/L.
FIG. 6.-Plasma and urinary changes during correctionof the water and electrolyte deficit in a patientwith pyloric stenosis due to carcinoma. Salinewas administered and sodium retained throughoutthe period of study. The plasma electrolyte concen-trations were restored almost to normal before theurine became alkaline.
be administered conveniently by adding 40 ml. ofio% potassium chloride to each litre of intra-venous fluid, giving a concentration of approxi-mately 50 mEq. per litre. Not more than z litresof this should be given in 12 hours unless thereis a dangerous degree of hypokalaemia. If tetanyis present calcium gluconate can be given intra-venously. Ammonium chloride is contraindicatedas, apart from being inadequate replacementtherapy for the multiple deficiencies, it has aharmful diuretic effect. Re-expansion of theextracellular space often unmasks anaemia inpatients with pyloric stenosis and this should becorrected by blood transfusion before operation.Once the metabolic defects of a severe case
have been rectified and the stomach emptiedoperation should not be delayed. The procedureof choice is partial gastrectomy, but gastro-enterostomy has a limited place in irremovablecarcinoma of the stomach or in very ill patients.This operation has been advocated in the past forlong-standing cases where gastritis due to gastricretention has reduced acid section to a low level.Such advanced cases are now rarely seen nor is
Protected by copyright.
on 23 Novem
ber 2018 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.422.743 on 1 Decem
ber 1960. Dow
nloaded from

748 POSTGRADUATE MEDICAL JOURNAL December 1960
the associated hypochlorhydria necessarily per-manent.
Pyloric stenosis used to be a dreaded complica-tion of peptic ulceration, carrying a mortality ofsome i6.5%3 in patients submitted to operation.In a recent series' the overall mortality of casesdue to benign ulceration was 5%. This improvedprognosis is mainly due to the better under-standing of the metabolic problems involved andparticularly to the use of saline in treatment.
AcknowledgmentsWe thank Mr. D. H. Patey and Mr. L. P.
Le Quesne for their advice and help. The radio-active bromine assay was carried out by Mr.R. P. Ekins. Figs. 3 and 4 are reproduced bykind permission of Mr. L. P. Le Quesne and theEditor of' Surgery, Gynaecology and Obstetrics'.
REFERENCESI. BALINT, J. A., and SPENCE, M. P. (1959), Brit. med. J.
i, 890.2. BERLINER, R. W., KENNEDY, T. J., and ORLOFF, J.
(I95I), Amer. J. Med., II, 274.3. BERKMAN, D. M. (I92g), Med. Clin. N. Amer., 5, 41I.4. BLACK, D. A. K., and JEPSON, R. P. (I954), Quart. J. Med.,
23, 367.
5. BURNETT, C. H., BURROWS, B. A., and COMMONS,R. R. (1950), J. din. Invest., 29, Part I, 169.
6. BURNETT, C. H., BURROWS, B. A., COMMONS, R. R.,and TOWERY, B. T. (I950), Ibid., 29, Part I, I75.
7. COOKE, A. M. (I933), Quart. J. Med., 2, 539.8. COOKE, R. E., SEGAR, W. E., CHEEK, D. B., COVILLE,
F. E., and DARROW, D. C. (1952), J. din. Invest., 31, 798.9. DARROW, D. C., SCHWARTZ, R., IANUCCI, J. F., and
COVILLE, F. (1948), Ibid., 27, 198.Io. ELKINTON, J. R., and WINKLER, A. W. (1944), Ibid;,
23, 93.1. GAMBLE, J. L., and ROSS, S. G. (1925), Ibid., 1, 403.I2. HOBSLEY, M., HOWE, C. T., and LE QUESNE, L. P.
(1960). Unpublished observations.13. HOUGHTON, L. W., VENABLES, J. F., and LLOYD,
N. L. (1925), Guy's Hosp. Rep., 5, I47.14. LANS, H. S., STEIN, I. F., and MEYER, K. A. (1952),
Ann. Surg., 135, 441.x5. LE QUESNE, L. P. (1960), Surg. Gynaec. Obstet., in press.i6. McCALLUM, W. G., LINTZ, J., VERMILYE, H. N.,
LEGGETT, T. H., and BOAS, E. (1920), Bull. Johns Hopk.Hosp., 31, I.
17. NELSON, R. M., FRIESEN, S. R., and KREMEN, A. J.(1950), Surgery, 27, 26.
I8. PYRAH, L. N. (I949), Brit. J..uroi., 21, 27.I9. RITCHIE, J. B., and SMITH, A. N. (I959), Brit. J. Surg.,
46, 625.20. SAUNDERS, S. J., IRVINE, R. O. H., CRAWFORD, M. A.,
and MILNE, M. D. (1960), Lancer, i, 468.21. TARAIL, R., and ELKINTON, J. R. (1949), J. clin. Invest.;
28, 99.22. UNGLEY, H. G. (1948), Lancet, ii, 2z8.23. VAN SLYKE, K. K., and EVANS, E. I. (i947), Ann. Surg.,
126, 545.
RENAL DISEASE(Postgraduate Medical Journal, November 1959)
Price 6s. 6d. post free
RECENT DEVELOPMENTS IN THE STUDY HAEMODIALYSISOF THE KIDNEY
F. M. Parsons, B.Sc., M.B., Ch.B.A. A. G. Lewis, B.Sc., M.D., M.R.C.P.F. M. Parsons, B.Sc., M.B., Ch.B.
RENAL BIOPSY AND DIURETICSGLONMERULONEPHRITISGLOMEULONEPHITIS H. G. Lloyd-Thomas, M.A., M.B., M.R.C.P.J. H. Ross, M.D., M.R.C.P.
RECENT ADVANCES IN THE TREATMENT URINARY DIVERSIONOF RENAL DISEASE John Hopewell, F.R.C.S.A. G. Spencer, M.D., M.R.C.P.
AORTOGRAPHY RENAL ARTERY STENOSISI. H. Griffiths, F.R.C.S. Kenneth Owen, M.S., F.R.C.S.
Published byTHE FELLOWSHIP OF POSTGRADUATE MEDICINE
9, Gt. James Street, W.C.1
Protected by copyright.
on 23 Novem
ber 2018 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.422.743 on 1 Decem
ber 1960. Dow
nloaded from